
Abstract
Importance
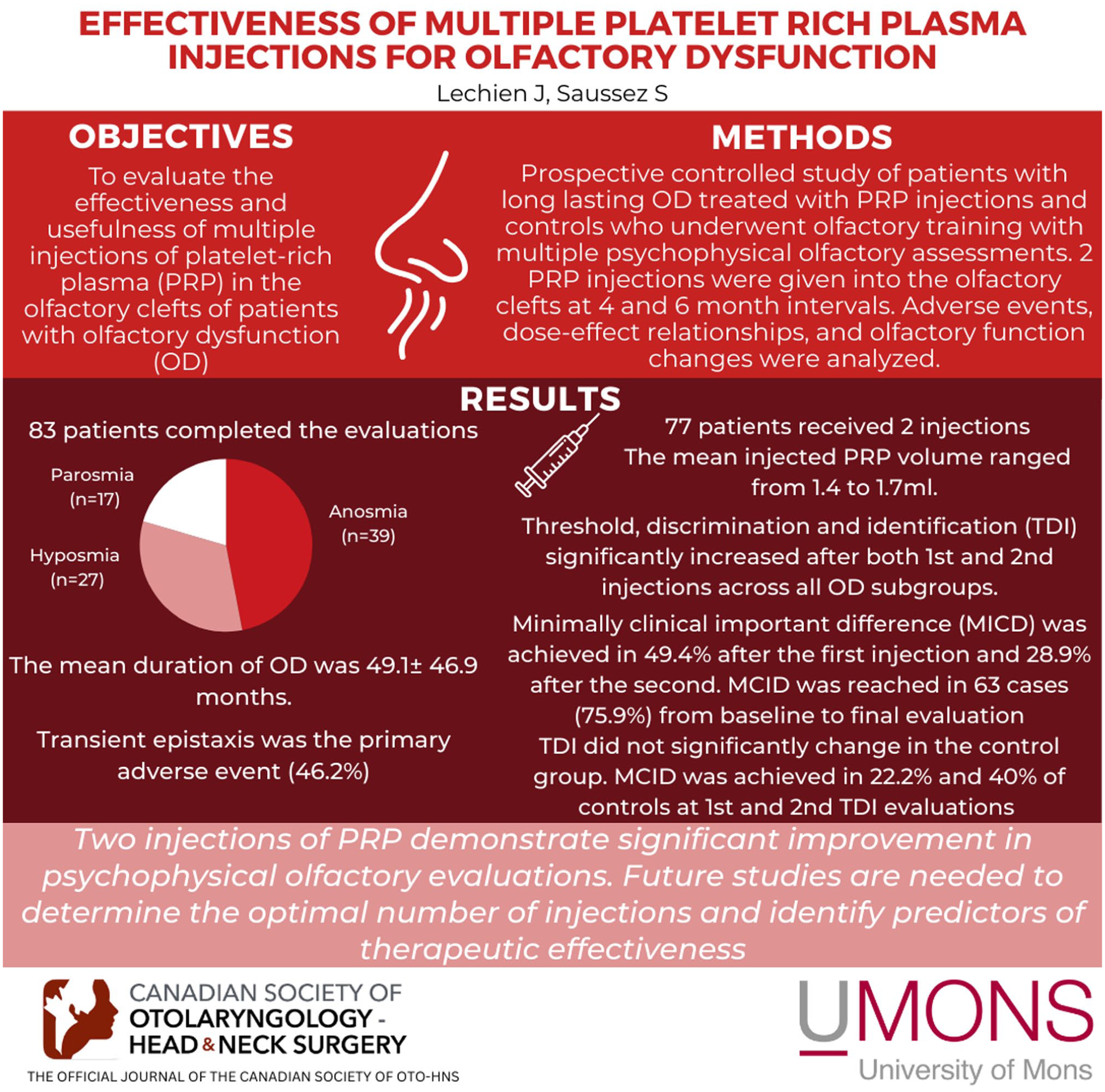
The injections of platelet-rich plasma (PRP) in the olfactory clefts of patients with olfactory dysfunction (OD) is an emerging treatment. To date, no study investigated the effectiveness of multiple PRP injections.
Objective
To evaluate the effectiveness and usefulness of multiple injections of PRP in the olfactory clefts of patients with OD.
Design
Prospective controlled study.
Setting
Monocentric medical center.
Participants
Patients with long-lasting OD treated with PRP injections and controls who underwent olfactory training with multiple psychophysical olfactory assessments.
Intervention
Two PRP injections into the olfactory clefts at 4- to 6-month intervals.
Main Outcomes
Outcomes included adverse events, dose-effect relationships, and olfactory function changes measured by threshold, discrimination, and identification (TDI) testing with minimal clinically important difference (MCID).
Results
Eighty-three subjects completed the evaluations. Patients had anosmia (n = 39), hyposmia (n = 27), and parosmia (n = 17). The mean duration of OD was 49.1 ± 46.9 months. Seventy-seven patients received 2 injections. Transient epistaxis was the primary adverse event (46.2%). The mean injected PRP volume ranged from 1.4 to 1.7 mL. TDI significantly increased after both first and second injections across all OD subgroups. MCID was achieved in 49.4% after a first injection and 28.9% after a second. MCID was reached in 63 cases (75.9%) from baseline to final evaluation. Baseline TDI strongly predicted post-second injection TDI (rs = .919; P = .001), but the first PRP response didn’t significantly predict second response (rs = −.201; P = .069). TDI did not significantly change in the control groups. MCID was achieved in 22.2% and 40% controls at the first and second TDI evaluations.
Conclusion and Relevance
Two injections of PRP demonstrate significant improvement in psychophysical olfactory evaluations. Future studies are needed to determine the optimal number of injections and identify predictors of therapeutic effectiveness.
Key Messages
TDI significantly increased after both first and second injections of PRP in patients with a long-lasting OD, with 49.4% and 28.9% patients achieving MCID after the first injection and the second injection.
TDI MCID was reached in 63 cases (75.9%) from baseline to the final evaluation, while MCID was achieved in 22.2% and 40% controls at the first and second TDI evaluations.
Baseline TDI strongly predicted post-second injection TDI, but the first PRP response did not significantly predict the second response.
Introduction
The injection of platelet-rich plasma (PRP) in the olfactory clefts is an emerging therapeutic option for patients with a long-lasting olfactory dysfunction (OD). 1 The procedure is safe 2 and recent studies demonstrated superiority over placebo or olfactory training protocol in patients with a long-lasting post-COVID-19 OD,3,4 while a very recent preliminary controlled study supported its effectiveness in patients with post-traumatic OD. 5 To date, the studies investigating the PRP injection effectiveness reported olfactory change results after a single injection.2-6 It is therefore unclear whether multiple injections can be safely administered and whether they are associated with continuous improvement of olfactory function.
The aim of this preliminary study was to evaluate the effectiveness and usefulness of multiple PRP injections in the olfactory clefts of patients with long-lasting OD.
Methods
Ethical Statement
The study protocol was approved by the Institutional Ethics Committee (CHU Saint-Pierre Hospital-2102028). Electronic informed consent was obtained for patients. This study adhered to the STROBE guidelines for observational studies to ensure transparency and replicability of our findings. 7
Patients and Setting
Patients with a long-lasting (>6 months) post-viral or post-traumatic OD were consecutively recruited from March 2022 to July 2024 in the Dour Medical Center (Belgium). The OD lasted for more than 6 months, and included quantitative and qualitative disorders (eg, anosmia, hyposmia, parosmia). These 2 etiological OD were chosen in the present study because the PRP injections demonstrated a potential benefit for the recovery of olfaction.1-3,5 Note that the post-traumatic OD was defined as a total loss of smell after a head trauma.
The definitions of anosmia and hyposmia were based on the threshold, discrimination, and identification (TDI) test. 8 Normative studies reported that anosmia was defined as a TDI score ≤16 points and hyposmia was defined as a TDI ≤30.75. TDI >30.75 was considered normosmia.8,9 Patients were included for TDI score below 30.75 or if they reported qualitative OD independent of the TDI score consisting of parosmia. To date, there is no objective 10 or psychophysical olfactory testing available for the assessment of parosmia in our country. The parosmia definition was therefore based on a qualitatively validated structured questionnaire consisting of the parosmia subscore of the French version of the olfactory disorder questionnaire (ODQ) >8/12. 11 A control group was composed of patients with long-lasting OD who were followed at CHU Saint-Pierre hospital with multiple TDI assessments conducted at intervals ranging from 4 to 6 months. The control group adhered to an olfactory training protocol. 12
Subjects had no sinus or olfactory region abnormalities on nasofibroscopy or imaging, ongoing acute, recurrent, or chronic rhinosinusitis with or without nasal polyps, olfactory or nasal tumor. Consistent with previous research, 13 patients with the following conditions were excluded: idiopathic OD before the pandemic; nasal obstruction related to rhinitis; history of nasal chemo/radiation, severe neurological or psychiatric comorbidities, and chronic rhinosinusitis. Only patients completing the follow-up evaluations were included.
Demographic, Clinical, and Olfactory Outcomes
The following outcomes were prospectively collected: age, gender, comorbidities, allergies, tobacco history, and origin of OD. Moreover, details about previous interventions for the management of OD were carefully collected, including olfactory training protocols, medications (eg, nasal and oral corticosteroids), and dietary supplements (eg, alpha lipoic acid, vitamins A, B12, zinc).
The baseline impact of OD on quality-of-life (QoL) was evaluated in PRP group with the French version of the ODQ. 11 The ODQ is a validated patient-reported outcome questionnaire composing of parosmia (0-12 points), QoL (0-57 points), and sincerity (0-18 points) subscores. 11 The ODQ total score ranges from 0 (no OD impact on QoL) to 87 (severe impact of OD on QoL). 11 Psychophysical evaluations were conducted using the TDI test (Medisense, Groningen, Netherlands) for both patients and controls throughout the follow-up. In our center, the TDI is administrated by a speech therapist trained in olfaction. The recommendations of the manufacturer are followed for performing the TDI, with a complete TDI duration ranging from 25 to 30 minutes. The cost of TDI is not reimbursed by the healthcare system.
Injection Procedure
The injections were performed by the same practitioner (J.R.L.). 14 The blood was extracted into a 20 mL tube with sodium citrate anti-coagulant (PRP-Tubes, RegenLab®, Lille, France) by an experienced nurse. The blood collection time varied depending on the difficulty in finding an adequate vessel for blood collection. PRP isolation was carried out with a 5 minute centrifugation at 3500 RPM. The centrifuge (Horizon 6FA) was provided by the tube manufacturer (RegenLab). The centrifuge was not cold. The supernatant was drawn up into a 10 mL syringe, and the nurse transferred it into a 1 mL syringe. The final volume of PRP varied depending on the initial blood collection volume. The red blood cells were isolated in the back of the tube from the PRP through a specified gel. The practitioner performed the nasal anesthesia with Xylocaine 10% spray after the use of xylometazoline hydrochloride drops. Injections were performed with a bent 27-G needle (10 cm) guided by a 30° rigid endoscope. Bilateral 4 to 6 injections of 0.2 mL were performed in the upper septum of the olfactory cleft. The access and the length of the olfactory cleft determined the number of injections and the volume of injected PRP. Indeed, in contrast to initial studies, 5 practitioners administered more than 1 mL of PRP in each nasal cavity when the patient’s anatomical configuration permitted such volumes. Patients were monitored for 15 minutes post-procedure, while potential adverse events and bleeding were carefully documented.
Discharged patients were instructed to adhere to an olfactory training protocol for 3 months despite a history of unsuccessful olfactory training before injection. The olfactory training was similar to those proposed to control individuals and consisted of sniffing daily odors every day a few minutes (including fragrance, spicy, soap, coffee, food odors, essential oils). Patients and controls were recommended to do the olfactory protocol at least 2 times a day. A second injection was carried 4 to 6 months after the first one. Consistent with previous studies,2,5 the TDI scores was recorded at 4 months post-PRP injections in all patients. The 3 days after the injections, patients were recommended to avoid anti-coagulant/anti-platelet, physical activity, and any activity increasing the blood pressure.
The volume of injected PRP, the time of centrifugation and preparation of PRP, anesthesia, and potential adverse events were collected.
Statistical Analyses
The statistical analyses were performed with Statistical Package for the Social Sciences for Windows (SPSS version 29.0; IBM Corp, Armonk, NY, USA). According to the data features and distribution, Mann-Whitney and chi-square tests were used to compare outcomes between PRP and control groups at baseline. The evolution of TDI scores across multiple injections was assessed with Wilcoxon rank tests, with additional consideration given to the minimal clinically important difference (MCID) in TDI scores (5.5 points) 9 and the effect size (Cohen-d). Spearman correlation coefficient was used to evaluate demographic, procedure, and olfactory outcome associations. The outcome association was considered as low, moderate, and strong for k < 0.40, 0.40 to 0.60, and k > 0.60, respectively. A level of significance of P < .05 was used.
Results
Of 118 eligible patients, 83 completed follow-ups with multiple PRP injections (mean age: 51.2 ± 14.6 years). A total of 35 patients were excluded: 30 for incomplete TDI, 5 for COVID-19 during follow-up. The patients lost to follow-up were primarily non-Belgian citizens who came from other European countries to benefit from PRP, which was not available in their countries. In this regard, the follow-up of these patients was difficult due to travel distance and associated costs. There were 53 (63.9%) females and 30 (36.1%) males (Table 1). OD was related to the following etiologies: coronavirus disease 2019 (COVID-19; n = 61, 73.5%), non-COVID-19 infection occurring before the pandemic (n = 16, 19.3%), head trauma (n = 5; 6.0%), and undetermined sudden smell loss (n = 1, 1.2%). According to the TDI and the qualitative evaluation, there were 39 patients with anosmia, 27 patients with hyposmia, and 17 patients with parosmia, respectively. The mean duration of OD was 49.1 ± 46.9 months. Comorbidities and previous interventions are reported in Appendix Table A1. Patients with anosmia, hyposmia, and parosmia were comparable for mean age, gender ratio, and mean duration of OD (Table 1). Because the definition of anosmia and hyposmia was based on TDI, subgroups demonstrated significant differences for TDI. Moreover, patients with parosmia exhibited a lower proportion of non-COVID-19 post-viral and post-traumatic etiologies compared to those with anosmia and hyposmia (Table 1).
Features and Clinical Scores of Patients and Controls.

Abbreviations: COVID, coronavirus disease 2019; NS, non-significant; OD, olfactory dysfunction; PRP, platelet-rich plasma; TDI, threshold, discrimination, and identification.
Patients and controls were comparable in terms of gender ratio, mean age, mean duration of OD and etiologies of OD, while subgroup analyses reported significant differences between anosmia versus control groups for TDI (Table 1).
Injection Outcomes
The following adverse events were reported: transient post-injection epistaxis (46.2%), significant pain (11.8%), vasovagal malaise (2.4%), repetitive sneezing during the procedure (2.4%), and anxiety (1.2%). In 3 cases, an ipsilateral nasal deviation limited injection to only one side. The preparation of PRP, including blood collection, centrifugation, and local nasal anesthesia, required 8.0 ± 3.2 minutes per patient. The injection procedure following anesthesia took 3.2 ± 0.6 minutes per patient. The mean volumes of PRP administered in right and left olfactory clefts for initial injections were 1.4 ± 0.5 and 1.4 ± 0.4 mL, respectively. For the second injection, mean volumes increased to 1.7 ± 0.4 mL for both right and left olfactory clefts, with a cumulative administration time of 3.4 ± 0.4 minutes.
Multiple Injection Olfactory Outcomes
Seventy-seven patients received 2 injections. The baseline mean TDI was 15.3 ± 9.3 (95% CI: 13.3-17.3) and significantly increased to 20.4 ± 9.8 (95% CI: 18.3-22.5) after the first injection and 23.5 ± 10.0 (95% CI: 21.3-25.7) after the second one. The effect size of pre- to post-treatment (2d injection) TDI change reported a Cohen’s d of 1.17, which demonstrated a large effect.
Following the first injection, TDI scores increased in 71 patients (85.5%), with 41 patients (49.4%) achieving the MCID. Between the first and second injections, 58 patients (69.9%) demonstrated increased TDI scores, though only 24 patients (28.9%) reached the MCID threshold. Among patients without significant response (MCID) after the first injection (n = 42), 15 (35.7%) subjects achieved a significant increase of TDI at the second injection.
When comparing baseline TDI scores to those after 2 injections, MCID was achieved in 63 cases, yielding a double injection success rate of 75.9%. TDI scores failed to increase in 9 patients (10.8%). Mean TDI scores significantly improved from baseline to post-first injection (P = .001) and from first to second injection (P = .001; Table 2). The baseline ODQ was 38.8 ± 14.9.
Psychophysical Olfactory Evolution.
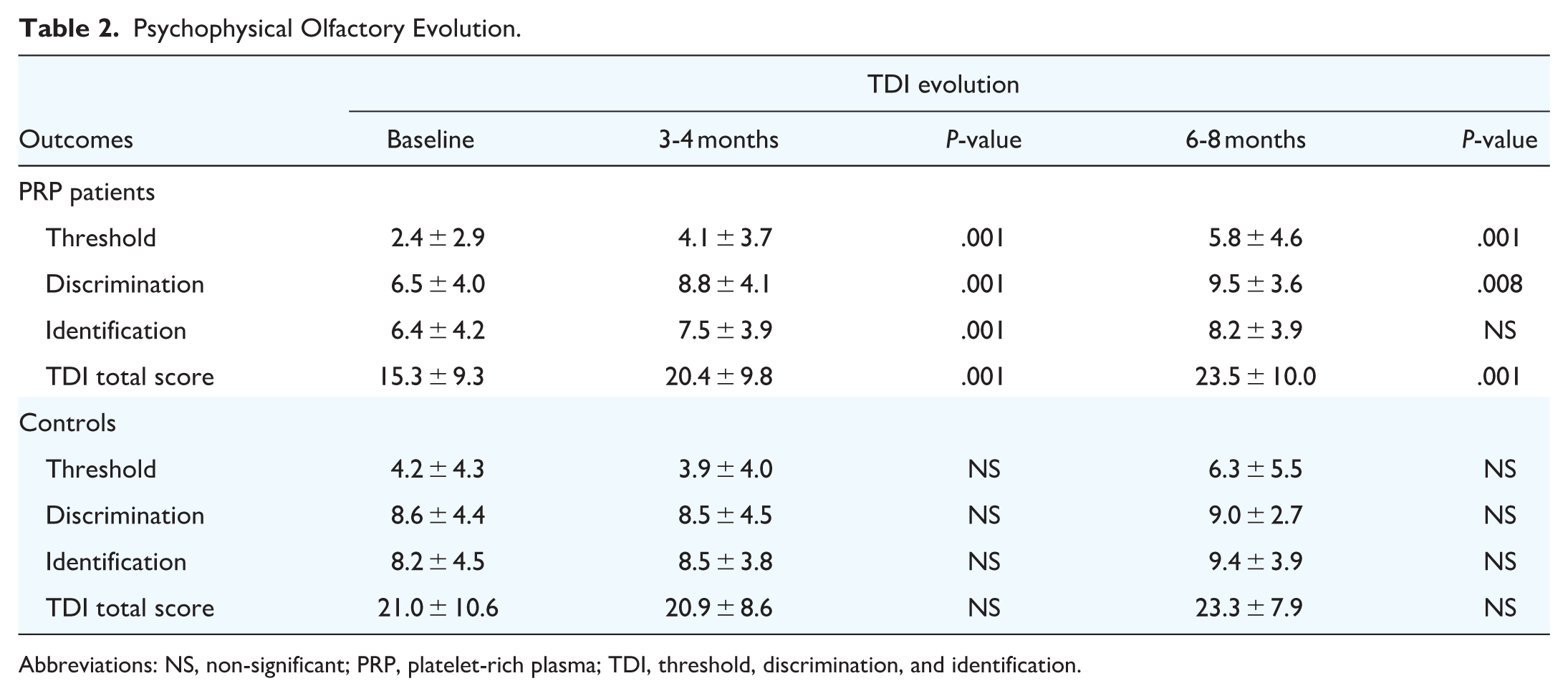
Abbreviations: NS, non-significant; PRP, platelet-rich plasma; TDI, threshold, discrimination, and identification.
In the control group, TDI scores increased in 13/27 patients (48.1%) at first follow-up assessment, with MCID achieved in 6 cases (22.2%). At second follow-up, MCID was achieved in 40% of controls. However, mean TDI scores in the control group did not demonstrate statistically significant changes throughout the follow-up period (Table 2).
Subgroup analyses were summarized in Table 3. TDI total score and the threshold subscore similarly increased in anosmia, hyposmia, and parosmia groups. The increase of discrimination and identification subscores varied from 1 group to another (Table 3).
Subgroup Psychophysical Olfactory Evolutions.
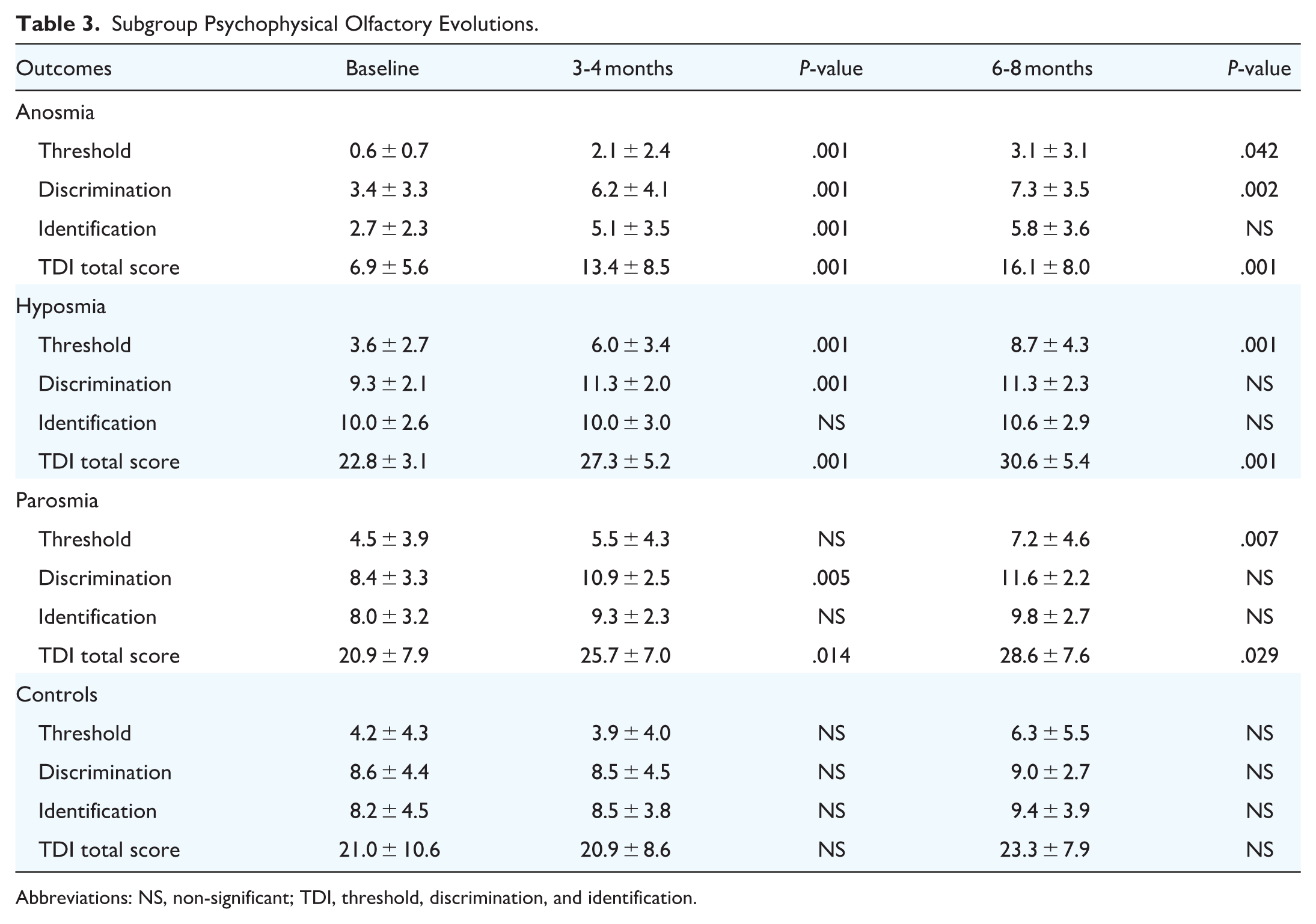
Abbreviations: NS, non-significant; TDI, threshold, discrimination, and identification.
Predictor of Outcomes
The duration of OD is negatively correlated with the baseline TDI (rs = −.338; P = .006), the post-injection TDI (month 4; rs = −.255; P = .044). The baseline ODQ was negatively associated with the duration of OD (rs = −.276; P = .028). The baseline TDI was a strong predictor of the TDI post-second injection (rs = .919; P = .001). However, considering the MCID for the PRP responsiveness, there was no significant association between the first PRP response and the second PRP response (rs = −.201; P = .069).
Discussion
The adequate number of PRP injections required for treating OD is currently unknown. Most studies of the literature included the placebo-randomized controlled trials, 3 report findings of a single injection in patients with long-lasting post-viral or post-traumatic OD.1-3,5,6,15
The primary findings of the present study suggest a potential benefit of 2 PRP injections, while insufficient data are provided to conclusively determine the usefulness of more than 2 injections. Importantly, association analysis revealed that responsiveness to the first injection is not predictive for responsiveness to the second one, with baseline TDI score identified as a significant predictor of therapeutic response. The rationale for performing multiple injections derives from orthopedics and plastic surgery literature.16-18 In orthopedics, the administration of 3-to-5 injections of PRP is safe and substantially more effective than single injections, leading to significant clinical improvement in chronic inflammatory disorders.17,18 Similar observations have been documented for hair and skin tissue regeneration. 16
The physiological mechanisms underlying the effectiveness of PRP in the long-lasting post-viral (COVID-19 and non-COVID-19) OD remain unknown. 19 Growth factor release from PRP—including platelet-derived growth factor, transforming growth factor-β, vascular endothelial growth factor, epidermal growth factor, and fibroblast growth factor—along with plasma proteins, could promote tissue regeneration while reducing chronic inflammatory responses in persistent OD.20,21 The pathophysiology of long-lasting OD likely involves persistent transcriptomes or viral antigens within the mucosa/neuroepithelium that trigger immune system reactivation and premature apoptosis of differentiating stem cells during recovery.22,23 This therapeutic mechanism is supported by Yasak et al, who demonstrated superior olfactory recovery and epithelial healing following PRP injection into the olfactory region compared to saline controls in a murine model of chronic OD. 24 Both anti-inflammatory and regenerative mechanisms may be sustained through repeated PRP injections; however, optimal injection frequency and intervals for OD remain undefined. In the present study, the authors selected a 4-month interval between injections based on their clinical experience (more than 1400 procedures), during which they empirically observed PRP benefits and olfactory improvements typically persisting for approximately 4 months, with some patients reporting maximal satisfaction following a single intervention.
To the best of our knowledge this study is the first investigating the usefulness and effectiveness of multiple PRP injection into the olfactory cleft of patients with OD. The use of validated psychophysical olfactory testing and the recruitment of a control group are the primary strengths of the paper. The inclusion of heterogeneous patients with variable OD etiologies is the primary limitation of the study. However, despite heterogeneity across OD etiologies, the 3 types of included patients (post-viral non-COVID-19, post-COVID-19, and post-traumatic OD) are 3 conditions reporting significant response to PRP injections. In addition to the literature dedicated to post-viral OD,1-3 our group very recently published that PRP can be effective in 66.7% of post-traumatic patients with TDI scores demonstrating significantly higher increases in injected post-traumatic patients compared to controls. 5
The lack of sample size calculation, and the lack of prospective recruitment of subjects of the control group matched for age and gender proportion are additional limitations. While COVID-19 and non-COVID-19 post-viral OD patients can share similar responses to PRP.13,19,25,26 Several confounding factors may influence group comparability, including prevalence of parosmia, disproportionate representation of post-traumatic patients, and potential selection bias due to loss to follow-up. Indeed, only patients completing both pre- and post-evaluations were included in the analysis. In practice, more than 50% of patients originated from remote regions or foreign countries and consequently did not complete post-injection TDI assessments. Similarly, some patients failed to complete post-injection evaluations due to either self-perceived high or low PRP response following 1 or 2 injections, resulting in an inability to return for consultation. Such a risk is inherent in the nature of the study reporting data of a new procedure, but these factors potentially limit the generalizability of the present study’s findings to the broader population. Finally, the control group was designed to reflect a typical population of patients suffering from long-lasting OD, including individuals with anosmia, hyposmia, or parosmia, which can be associated with psychological distress. 27 We did not create separate control subgroups based on specific OD (ie, parosmia, anosmia, or hyposmia). This approach prevented us from determining which OD might be most responsive to PRP injections when compared to the broader population of long-lasting OD patients. The lack of quantification of PRP is an additional limitation. From a physiological standpoint, future basic science studies are needed to understand the effect of PRP on the stem cells in the regeneration of the olfactory neurons, 28 considering potentially the septum and middle turbinate neuroepithelium that are both important for olfaction. 29
Conclusion
Multiple injections of PRP demonstrate significant improvement in psychophysical olfactory evaluations. Future studies are needed to determine the optimal number of injections, intervals between injections, the consideration of additional injection points into the middle turbinate and identify predictors of therapeutic effectiveness.
Footnotes
Appendix
Comorbidities and Interventions of Patients.

| Outcomes | PRP patients | Total (n = 83) | P-value | ||
|---|---|---|---|---|---|
| Anosmia (n = 39) | Hyposmia (n = 27) | Parosmia (n = 17) | |||
| Age (mean, range) | 50.2 ± 17.1 | 55.5 ± 12.5 | 48.4 ± 11.6 | 51.2 ± 14.6 | NS |
| Comorbidities | |||||
| Reflux | 6 (15.4) | 8 (29.6) | 1 (5.9) | 15 (18.1) | NS |
| Thyroid disorder | 4 (10.3) | 2 (7.4) | 2 (11.8) | 8 (9.6) | NS |
| Hypercholesterolemia | 5 (12.8) | 6 (22.2) | 2 (11.8) | 13 (15.7) | NS |
| Hypertension | 2 (5.1) | 4 (14.8 | 4 (23.5) | 10 (12.0) | NS |
| Arthrosis | 4 (10.3) | 2 (7.4) | 2 (11.8) | 8 (9.6) | NS |
| Depression (mild) | 0 (0) | 1 (3.7) | 2 (11.8) | 3 (3.6) | NS |
| Asthma | 2 (5.1) | 1 (3.7) | 1 (5.9) | 4 (4.8) | NS |
| Mellitus diabetes | 1 (2.6) | 3 (11.1) | 2 (11.8) | 6 (7.2) | NS |
| Cardiologic affections | 2 (5.1) | 0 (0) | 0 (0) | 2 (2.4) | NS |
| Respiratory insufficiency | 2 (5.1) | 0 (0) | 1 (5.9) | 3 (3.6) | NS |
| Renal insufficiency | 0 (0) | 0 (0) | 1 (5.9) | 1 (1.2) | NS |
| Hepatic insufficiency | 1 (2.6) | 2 (7.4) | 0 (0) | 3 (3.6) | NS |
| Psoriasis | 1 (2.6) | 0 (0) | 1 (5.9) | 2 (2.4) | NS |
| Allergy | 3 (7.7) | 3 (11.1) | 0 (0) | 6 (7.2) | NS |
| Tobacco consumption | 3 (7.7) | 2 (7.4) | 3 (17.6) | 8 (9.6) | NS |
| Intervention pre-injection | |||||
| Olfactory training (12 weeks) | 25 (64.1) | 20 (74.0) | 13 (76.5) | 58 (69.9) | NS |
| Alpha lipoic acid | 1 (2.6) | 2 (7.4) | 3 (17.6) | 6 (7.2) | NS |
| Nasal corticosteroids | 13 (33.3) | 8 (29.6) | 10 (58.8) | 31 (37.3) | NS |
| Oral corticosteroids | 8 (20.5) | 1 (3.7) | 3 (17.6) | 12 (12.5) | NS |
| Vitamin B12 | 5 (12.8) | 9 (33.3) | 4 (23.5) | 18 (21.7) | NS |
| Vitamin A | 2 (5.1) | 5 (18.5) | 1 (5.9) | 8 (9.6) | NS |
| Zinc | 7 (17.9) | 14 (51.9) | 8 (47.1) | 29 (34.9) | NS |
| Omega 3 | 2 (5.1) | 5 (18.5) | 4 (23.5) | 11 (13.3) | NS |
Abbreviations: NS, non-significant; PRP, platelet-rich plasma.
Acknowledgements
Roxane Geerts and the Audiology team for the Sniffin-stick tests. S. Soylu for the database of controls.
Ethical Considerations
The study was approved by the institutional review board of CHU Saint-Pierre (CHUSP-2102028).
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.