
Abstract
Background:
Automated insulin delivery (AID) improves glycemia in people with type 1 diabetes (T1D). However, concern remains about early worsening of diabetic retinopathy (EWDR) following rapid and large glycemic improvements. This study evaluated diabetic retinopathy (DR) outcomes in adolescents and young adults with T1D (aged 10-30 years) following AID initiation.
Methods:
This retrospective observational study included adolescents and young adults with T1D and hemoglobin A1c (HbA1c) ≥ 8.5% (69 mmol/mol) prior to AID initiation. Clinical data, continuous glucose monitoring (CGM) metrics, and retinopathy grading were collected from research and clinical databases before and after at least three months of AID initiation. Statistical analyses assessed outcomes.
Results:
A total of 95 adolescents/young adults (mean age 17.8 years, diabetes duration 9.7 years, 54.7% female) with a baseline HbA1c of 10.3% (89.5 mmol/mol) were included. Mean HbA1c improved by 2.1 percentage points (22.6 mmol/mol) following AID initiation. Retinopathy remained stable or improved in 72/95 (75.8%), while 23/95 (24.2%) experienced EWDR inclusive of diabetic macular edema (DME). While no one required treatment for DME, proliferative DR requiring treatment developed in three participants (3.2%); all had preexisting retinopathy and ≥1 additional diabetes-related complication/risk factor. Logistic regression identified age >18 years and preexisting retinopathy at AID initiation as the only significant risk factors for EWDR.
Conclusions:
Automated insulin delivery is associated with substantial glycemic improvement in adolescents and young adults with T1D. Despite these large glycemic improvements, diabetic retinal disease remains stable or improves in most cases. Risk factors for deterioration include age >18 years and preexisting DR.
Introduction
Automated insulin delivery (AID) is the gold standard for the management of type 1 diabetes (T1D). Automated insulin delivery combines an insulin pump, a continuous glucose monitor (CGM), and an algorithm modulating insulin delivery based on real-time CGM data and predicted glucose levels.1 -3 It has demonstrated significant improvements in glycemic outcomes, enhanced quality of life, and reduced diabetes-related complications.3 -6 These benefits are greatest in those with markedly elevated glucose levels at initiation.1,7 -10
Improving glycemia is essential to reduce the risk of diabetes-related short- and long-term complications. This includes diabetic retinal disease, where both proliferative diabetic retinopathy (PDR) and diabetic macular edema (DME) can threaten vision.11 -14 However, it has been clinically recognized with robust data from the Diabetes Control and Complications Trial (DCCT) that rapid improvement in glucose can temporarily lead to early worsening of diabetic retinopathy (EWDR) 14 that is generally characterized as a transient progression of retinopathy following rapid reductions in glucose over a period of 3 to 12 months.14 -17 The fact that this transient is important, as the DCCT demonstrated those with EWDR had overall improved eye outcomes in subsequent years.14,17 Early worsening of diabetic retinopathy has also been observed in other intensive interventions, such as commencing glucagon-like peptide-1 receptor agonists (GLP-1RAs), more intensive diabetes management in pregnancy, or bariatric surgery.18 -25 Although the mechanisms remain unclear, associated risk factors include hypertension, longer duration of diabetes, preexisting diabetic retinopathy (DR), and/or other diabetes-related microvascular complications.16,17,19,21 -24,26
Recent early data on risks of EWDR following AID in young people and adults appear reassuring, with only 3% of participants requiring retinal treatment after initiation. 27 This aligns with the 3% to 19% background EWDR rate reported in the general T1D population. 28 Data from an adult population have shown similar findings. 29 In these studies, the average hemoglobin A1c (HbA1c) reductions were 1.0 percentage points (11 mmol/mol) in an adolescent and adult cohort 27 and 0.4 percentage points (4.7 mmol/mol) in an adult-only cohort. 29 This leaves a lack of data on the risks associated with larger reductions in HbA1c. Therefore, we aimed to evaluate EWDR including impacts on DME in adolescents and young adults with a higher baseline HbA1c who experienced large and rapid glycemic improvements following AID initiation, and to identify associated risk factors.
Methods
Study Design
This retrospective observational study included adolescents and young adults with T1D (Figure 1). Participants were initially selected from participation in previous research trials on AID conducted by the investigators, where elevated baseline HbA1c was present at study entry by design.7,8,10,30,31 For the majority, subsequent observational data regarding diabetes complications and retinopathy were drawn from usual clinical care databases after study completion. Retinopathy assessment was not an outcome in these trials, except for 30 participants where these data were captured as part of the original trial. 10 Follow-up data were collected between April and October 2025 (original trials commenced between 2020 and 2023).
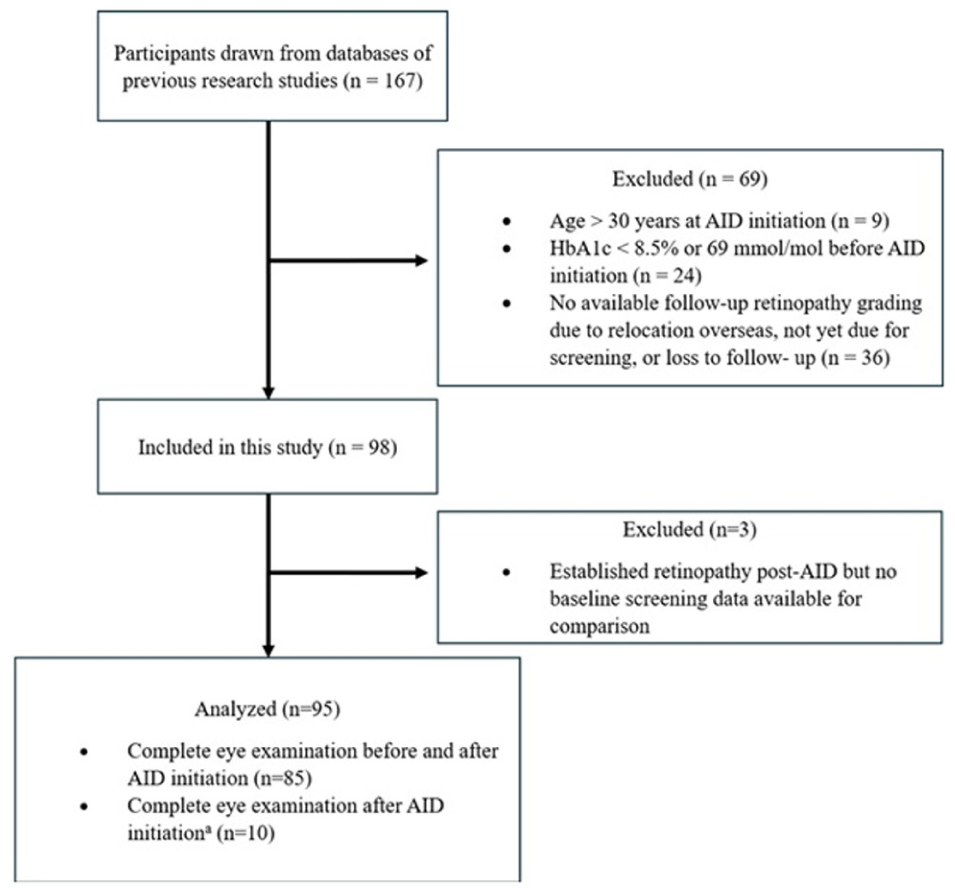
Participant flow diagram.
Selection of Participants
Participants were adolescents and young adults, aged 10 to 30 years, with a confirmed diagnosis of T1D for at least one year prior to AID initiation, a most recent HbA1c ≥ 8.5% (69 mmol/mol), and a minimum of three months of AID system use at the time of data collection. No pregnancies or use of GLP-1 RAs or SGLT2 inhibitors were recorded. These inclusion criteria were selected pragmatically to correspond with young people potentially experiencing the greatest improvements in glycemia following AID, and the period following AID initiation where EWDR is most likely to develop. 23 Participants who did not meet the above criteria or had not yet received a retinopathy assessment following commencement of AID were excluded. Notably, we also included ten individuals who lacked a baseline eye examination but had a documented follow-up of R0M0 after AID initiation. For these ten participants, we conservatively assumed a normal baseline status (R0M0) and classified them as “non-worsening” (see classification of retinopathy below).
Demographic and Clinical Variables
Baseline demographic and clinical data collected included date of birth, date of diabetes diagnosis, date of AID initiation, sex, smoking status, ethnicity, socioeconomic status using the New Zealand deprivation index, 32 body mass index (BMI), BMI z-score (for individuals aged 10-19 years), and type of insulin therapy prior to AID. Automated insulin delivery systems, including both investigational and approved commercial devices, spanning multiple algorithms, have intentionally not been provided as study was not designed to compare different systems. Hemoglobin A1c values and glycemic metrics including sensor glucose (SG), time below range (%TBR), time in range (%TIR), time in normal glucose (%TING), time above range (%TAR), coefficient of variation (%CV), and glucose management indicator (GMI) were obtained at AID initiation and after three months or the closest available data.
History of diabetes-related risk factors or complications were recorded prior to starting AID. These included nephropathy (an elevated albumin-to-creatinine ratio [ACR] or a formal diagnosis and/or treatment), neuropathy (a formal diagnosis), dyslipidemia (as defined by the American College of Cardiology/American Heart Association Practice guidelines or a formal diagnosis and/or treatment), 33 and hypertension (a formal diagnosis and/or treatment). Retinopathy gradings were obtained from the clinical records closest to the periods before and after the start of AID therapy. Variation in collection time points was seen and is described in the results. This variation was considered acceptable according to the one-year time frame for diagnosis of EWDR. 23
Assessment of Diabetic Eye Disease
All retinopathy assessments were conducted by health professionals, and in New Zealand, all data were extracted from routine retinopathy screening programs. In New Zealand, DR and DME gradings are based on “New Zealand National Diabetes Retinal Grading System,” 34 which is adapted from the “Airlie House Classification Scheme of the Early Treatment Diabetic Retinopathy Study” 35 and comparable with the “International Clinical Disease Severity Scale” (ICDSS). 36 This system is characterized by a discrete alphanumeric scoring system for DR and DME grading. Classification of DR consists of seven grades: no DR (R0), minimal (R1), mild (R2), moderate (R3), severe (R4), proliferative (R5), and previously treated proliferative retinopathy (RT). Diabetic macular edema grading also consists of seven grades: no macular disease (M0), minimal (M1), mild (M2), mild (M3), moderate (M4), severe (M5), and stable, treated macular disease (MT). Diabetic retinopathy assessments from Perth were performed using the ICDSS, but as all demonstrated no apparent DR, comparison between scales was straightforward.
Data Analysis and Statistical Methods
Demographic and clinical characteristics were described using means and standard deviations for continuous variables, and numbers and percentages for categorical variables. Self-identified prioritized ethnicities were used. Diabetic retinopathy and DME data were divided into subgroups (determined by the worst grade of the worst eye): nil (R0 and M0), minimal (R1 and/or M1), mild (R2 and/or M2/M3), moderate (R3 and/or M4), severe (R4 and/or M5), proliferative (R5), or previously treated DR (RT and/or MT). Proportions were determined for improvement, stability, or worsening. While separate analyses were conducted, due to the sample size, for the main analyses, a combined score for DR and DME was used to determine EWDR. For these analyses, improvement was defined as both DR and DME grades decreasing or one decreasing with the other remaining stable, stability as no change in both grades, and worsening as any rise in either DR or DME grade (or both). When M and R grade changes were inconsistent, the overall classification was based on the grade showing the largest change.
Retinopathy status was then categorized as either non-worsening (improvement or stability) or EWDR based on clinical characteristics. Diabetic retinopathy and DME grading at baseline were determined for each group using the previously defined classification system (nil, minimal/mild, moderate/severe, proliferative, and previously treated). For the individuals whose retinopathy progressed to proliferative disease requiring treatment, their characteristics were further described to highlight distinguishing features including baseline characteristics, degree of HbA1c improvement, change in CGM-derived glycemic metrics after AID initiation and DR outcomes.
Retinopathy outcomes were further analyzed according to diabetes duration (DD) with participants categorized into two groups: DD ≥ 10 years and DD < 10 years. Given the observational nature of the data, retinopathy grading and HbA1c measurements were performed at varying time points. For transparency, median and interquartile range (IQR) values before and after AID initiation are reported, and categorical variables were analyzed using chi-square (χ2) tests. Relative risks (RRs) were calculated by comparing the incidence of EWDR (combined DR and DME scores) among participants with large HbA1c improvement with that among those without large improvement. Binary logistic regression was performed to adjust for potential confounders that may have influenced the outcomes of interest including age at AID initiation, BMI, prior insulin therapy (MDI or CSII), and duration from AID initiation to DR grading assessment. Baseline HbA1c was not included in the analysis due to collinearity with large HbA1c improvement. All statistical analyses were performed using R, version 4.5.2 (R Core Team, Vienna, Austria). 37
Ethical Considerations
Ethics approval was obtained from the University of Otago (HD24/015). Ethnicity data were collected and managed in a culturally appropriate way, with consultation undertaken with Māori communities (indigenous people of New Zealand).
Results
Baseline Demographic and Clinical Characteristics
Data were included from 95 adolescents and young adults with T1D who had commenced AID and used it for ≥3 months. Overall, EWDR occurred in 23 participants (24.2%). Figure 1 shows participant flow into and out of the study. Demographic characteristics are provided in Table 1. At baseline, both age and duration of diabetes at AID initiation were higher in those who subsequently experienced EWDR. Participants who developed EWDR were more likely to have preexisting DR and prior treatment with multiple daily injections (MDI) before AID initiation. The mean interval from AID initiation to HbA1c measurement was 3.0 ± 0.5 months and to DR assessment was 9.5 ± 7.2 months. There was no difference in time from AID initiation to DR assessment between the EWDR and non-worsening groups (9.7 ± 6.5 vs 9.4 ± 7.5 months; P = .882).
Study Population Baseline Demographic and Clinical Characteristics Including Grouping by Change in Combined Diabetic Retinopathy Score.

Abbreviations: AID, automated insulin delivery; BMI, body mass index; CSII, continuous subcutaneous insulin infusion; DME, diabetic macular edema; DR, diabetic retinopathy; EWDR, early worsening of diabetic retinopathy; MDI, multiple daily injections; NZE, New Zealand European; SD, standard deviation.
Ten participants lacked baseline DR grading but since their follow-up showed R0M0 after AID initiation, they were classified as having “Non-worsening.”
P value indicates statistically significant difference (<.05).
Total includes 30 participants identified as “Australian” for whom specific ethnicities were unclear.
Including nine Pacific and one Asian.
BMI z-scores for 10 to 19 years old, mean ± SD are 1.1 ± 1.1 (overall), 1.2 ± 1.0 (non-worsening), and 1.0 ± 1.4 (EWDR).
Including 17 participant who had one complication, two participants who had two complications, and one participant who had three complications.
One participant in this study who had baseline severe DR (R4) before AID initiation (P2).
One participant with previously treated proliferative diabetic retinopathy had received panretinal photocoagulation (PRP) prior to AID initiation, and the disease remained stable during follow-up.
Impact of Glycemia on DR Outcomes
The mean HbA1c improvement after AID initiation was 2.1±1.9 percentage points (22.6 ± 20.9 mmol/mol), with a maximum reduction of 9.7 percentage points (106 mmol/mol). Stratification by HbA1c reduction (>1% vs ≤1%) showed no significant difference in DR or DME outcomes (RR 0.88, 95% confidence interval [CI] 0.77-1.00; P = .174 and RR 0.88, 95% CI 0.72-1.06; P = .225, respectively).
Figure 2 shows the progression of both DR and DME grades after AID initiation in all participants. A total of 25 participants (26.3%) had HbA1c reductions of ≤1 percentage point (≤10.9 mmol/mol). Mean baseline HbA1c in this group was 9.7% (82.7 mmol/mol). In this subgroup, DR progression occurred in one participant (4%) and DME progression in three participants (12%). No additional retinopathy treatment was required in this subgroup. Two participants (8%) demonstrated a one-grade improvement in DR (R2 to R1 and R1 to R0). One participant (4%) showed improvement in DME grade from M3 to M2.

Progression of diabetic retinopathy (DR) and diabetic macular edema (DME) grading after AID initiation. Y-axis shows the percentage of participants (before, n = 75; after, n = 85 including ten post-AID R0M0 cases conservatively classified as “Non-worsening”). Diabetic retinopathy grading includes: no DR (R0), minimal (R1), mild (R2), moderate (R3), severe (R4), proliferative (R5), and previously treated proliferative retinopathy (RT). Diabetic macular edema grading includes: no macular disease (M0), minimal (M1), mild (M2 and M3), moderate (M4), severe (M5), and stable, treated macular disease (MT).
A larger magnitude of glycemic improvement (>1 percentage point [>10.9 mmol/mol]) was observed in 70 participants (73.7%) with a mean reduction of 2.7 ± 1.7 percentage points (29.9 ± 19 mmol/mol). Mean baseline HbA1c in this group was 10.5% (91.7 mmol/mol). In this subgroup, EWDR occurred in 11 individuals (15.9%), including three participants who developed PDR without vision loss after AID initiation, as shown in Table 2. In addition, this cohort included 54 participants with CGM-derived glycemic metrics available both before and three months after AID initiation (data shown in Supplemental Table 1).
Characteristics of Participants Who Progressed to Proliferative Retinopathy Requiring Treatment.

Abbreviations: AID, automated insulin delivery; BMI, body mass index; CGM, continuous glucose monitoring; CV, glucose coefficient of variation; DR, diabetic retinopathy; GMI, glucose management indicator; isCGM, intermittently scanned continuous glucose monitoring; MDI, multiple daily injections; NZE, New Zealand European; PDR, proliferative diabetic retinopathy; SG, sensor glucose; TAR, time above range; TBR, time below range; TING, time in normal glucose; TIR, time in range.
P2 was diagnosed with microalbuminuria three months after AID initiation but before the diagnosis of PDR.
DR Progression to Proliferative DR Requiring Therapeutic Management
Three participants developed clinically significant EWDR requiring treatment (Table 2). All had a DD of ≥10 years; preexisting DR at baseline; and at least one additional diabetes-related complication. Two participants (P1 and P3) with baseline mild DR (R2) had HbA1c levels >11.3% (100 mmol/mol) prior to AID initiation while the third participant (P2) with severe DR (R4) at baseline had a baseline HbA1c of <11.3% (100 mmol/mol). All three had improvements in TIR greater than 40 percentage points. None required treatment of DME.
Additional Analysis of Risk Factors for EWDR
Logistic regression analyses are presented in Table 3. Significant risk factors associated with early worsening included age over 18 years at AID initiation (odds ratio [OR] 14.88, 95% CI 3.00-99.48; P = .002) while the absence of preexisting DR prior to AID initiation was a significant protective factor against early worsening (OR 0.08, 95% CI 0.01-0.38; P = .002). Stratified analyses for EWDR by DR and DME components are presented in supplemental tables. All six participants who experienced progression to moderate/severe DR or PDR had a DD of ≥10 years, HbA1c reduction >1 percentage point (>10.9 mmol/mol), and ≥1 additional diabetes-related complication/risk factor other than DR.
Logistic Regression Analysis of Risk Factors Associated With Early Worsening of Diabetic Retinopathy (EWDR a ).
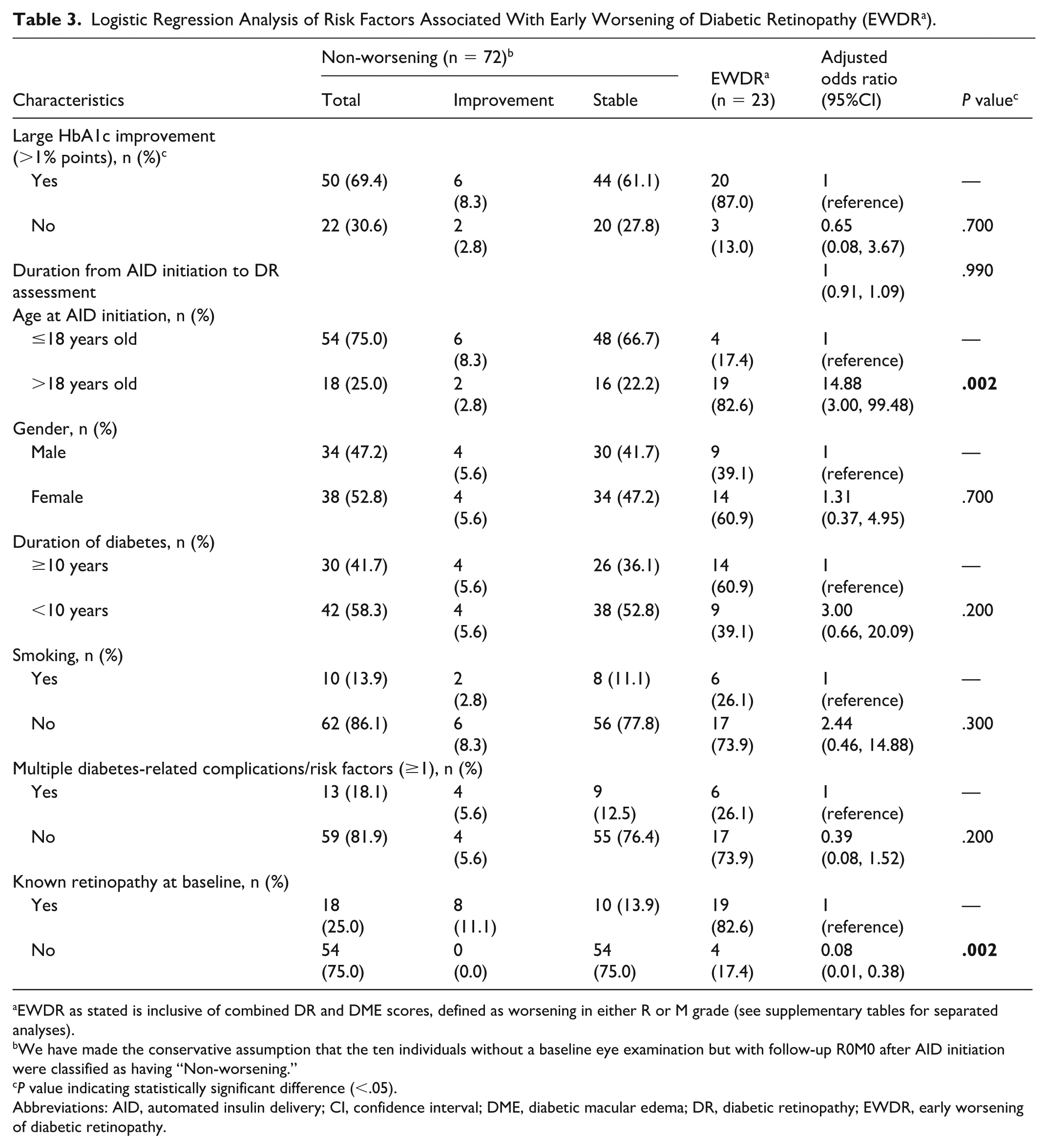
EWDR as stated is inclusive of combined DR and DME scores, defined as worsening in either R or M grade (see supplementary tables for separated analyses).
We have made the conservative assumption that the ten individuals without a baseline eye examination but with follow-up R0M0 after AID initiation were classified as having “Non-worsening.”
P value indicating statistically significant difference (<.05).
Abbreviations: AID, automated insulin delivery; CI, confidence interval; DME, diabetic macular edema; DR, diabetic retinopathy; EWDR, early worsening of diabetic retinopathy.
Discussion
We report retinopathy status and EWDR in adolescents and young adults experiencing large improvements in HbA1c following initiation of AID. This subpopulation under 30 years of age often has above-target glycemia,38,39 making the risk and significance of EWDR in this group an important consideration for people with diabetes and health care providers. Similar to previous studies with smaller HbA1c changes (0.43%-1.0%),27,29 the majority of people (≥75%) experienced improved or stable retinal findings over a mean AID duration of 9.5 months. However, just as previously reported for AID, and for other forms of intensive diabetes treatment, approximately 3% developed EWDR requiring treatment.17,27,28,40,41 Taken together with previously reported risk factors for DR, the key risk factors for EWDR and need for treatment following AID appear to include longer DD, longer-term uncontrolled hyperglycemia, magnitude but not speed of HbA1c reduction, baseline retinopathy severity, and comorbid diabetes complications/risk factors such as nephropathy and hypertension.11,23,28 These data provide confidence in the relative retinal safety of treating young people <18 years of age with markedly elevated glycemia using AID, but highlight the need for focused DR screening in higher-risk individuals.
While EWDR can occur in a minority of cases, it is important to emphasize that the long-term benefits of improving glycemic control with AID systems greatly outweigh the temporary and relatively small risk associated with EWDR. This was demonstrated in the DCCT with even those who experienced EWDR, experiencing substantially reduced longer-term risks of diabetes complications including retinopathy.12,14,17 Relevant to AID, speed of improvement (as anticipated with AID) was not seen as an additional risk for EWDR in the DCCT. 17 Importantly, the 3% risk of DR requiring treatment after AID therapy appears comparable with the documented background risk of retinopathy progression that occurs irrespective of diabetes treatment modality.17,27,28,40,41
In this cohort, the majority (93%) of individuals aged 18 or younger had either stable or improved DR, and no one under 18 years developed PDR. These findings underscore the importance of using advanced technology such as AID as early in age as possible to lessen the burden of diabetes complications (the concept of “metabolic memory”).14,42,43 This is similar to and builds on previous evidence on EWDR and AID.27,29 In contrast to the above protective factor of age, it is well recognized that key risk factors for worsening DR include long-term uncontrolled hyperglycemia, longer DD, out-of-target baseline glycemic control, and preexisting DR.11,23 These factors are not specific to EWDR but are key determinants of the development and progression of retinopathy at any stage. Finally, although the previous studies involving older populations identified magnitude of HbA1c reduction as a risk factor for EWDR, this remains unclear for this younger cohort. This likely reflects the natural course of DR progression in older individuals with a long-standing history of above-target glycemia.
These findings should be interpreted in the context of several limitations. Although the cohort represents a large real-world dataset of young people initiating AID, the retrospective design, small sample size, short follow-up, absence of a comparison group, and limited ethnic diversity may limit generalizability and introduce bias. Stratified analyses by DR and DME involved small event numbers, which may limit model stability (hence only combined EWDR analyses are provided in the main text). Multiple comparisons in this exploratory analysis raise the risk of type I error. Furthermore, metabolic data such as lipid profiles and CGM metrics were only available for a subset of participants, limiting interpretation. HbA1c and ophthalmologic data were also collected at routine clinical assessments and thus varied in timing. Offsetting this, the mean interval from AID initiation to retinopathy assessment was appropriate for investigating EWDR (9.5 months). Given variability in the timing of eye assessments relative to AID initiation, retinopathy progression may have occurred irrespective of AID during this interval; therefore, the risk may be overestimated.
Conclusions
Automated insulin delivery is the gold standard therapy for young people with T1D. Our data, especially when combined with prior evidence, confirm overall retinal safety of AID, with most showing stable or improved retinopathy after initiation. Although the risk of EWDR and vision loss is low, it can be further mitigated in higher-risk individuals through timely retinal screening and intervention. Concerns about EWDR should not delay access to AID.
Supplemental Material
sj-docx-1-dst-10.1177_19322968261446654 – Supplemental material for Diabetic Retinopathy Outcomes and Early Worsening of Diabetic Retinopathy in Adolescents and Young Adults With Type 1 Diabetes Following Rapid and Large Glycemic Improvements After Commencing Automated Insulin Delivery
Supplemental material, sj-docx-1-dst-10.1177_19322968261446654 for Diabetic Retinopathy Outcomes and Early Worsening of Diabetic Retinopathy in Adolescents and Young Adults With Type 1 Diabetes Following Rapid and Large Glycemic Improvements After Commencing Automated Insulin Delivery by Wipa Warunyuwong, Alisa Boucsein, Kate M. B. Sneddon, Francesc March de Ribot, Mary-Jane Sime, Yongwen Zhou, Tom Wilkinson, Martin I. de Bock, Esko J. Wiltshire, Ryan G. Paul, Craig A. Jefferies, Ashleigh Brown, Mary B. Abraham, Timothy W. Jones and Benjamin J. Wheeler in Journal of Diabetes Science and Technology
Supplemental Material
sj-docx-2-dst-10.1177_19322968261446654 – Supplemental material for Diabetic Retinopathy Outcomes and Early Worsening of Diabetic Retinopathy in Adolescents and Young Adults With Type 1 Diabetes Following Rapid and Large Glycemic Improvements After Commencing Automated Insulin Delivery
Supplemental material, sj-docx-2-dst-10.1177_19322968261446654 for Diabetic Retinopathy Outcomes and Early Worsening of Diabetic Retinopathy in Adolescents and Young Adults With Type 1 Diabetes Following Rapid and Large Glycemic Improvements After Commencing Automated Insulin Delivery by Wipa Warunyuwong, Alisa Boucsein, Kate M. B. Sneddon, Francesc March de Ribot, Mary-Jane Sime, Yongwen Zhou, Tom Wilkinson, Martin I. de Bock, Esko J. Wiltshire, Ryan G. Paul, Craig A. Jefferies, Ashleigh Brown, Mary B. Abraham, Timothy W. Jones and Benjamin J. Wheeler in Journal of Diabetes Science and Technology
Supplemental Material
sj-docx-3-dst-10.1177_19322968261446654 – Supplemental material for Diabetic Retinopathy Outcomes and Early Worsening of Diabetic Retinopathy in Adolescents and Young Adults With Type 1 Diabetes Following Rapid and Large Glycemic Improvements After Commencing Automated Insulin Delivery
Supplemental material, sj-docx-3-dst-10.1177_19322968261446654 for Diabetic Retinopathy Outcomes and Early Worsening of Diabetic Retinopathy in Adolescents and Young Adults With Type 1 Diabetes Following Rapid and Large Glycemic Improvements After Commencing Automated Insulin Delivery by Wipa Warunyuwong, Alisa Boucsein, Kate M. B. Sneddon, Francesc March de Ribot, Mary-Jane Sime, Yongwen Zhou, Tom Wilkinson, Martin I. de Bock, Esko J. Wiltshire, Ryan G. Paul, Craig A. Jefferies, Ashleigh Brown, Mary B. Abraham, Timothy W. Jones and Benjamin J. Wheeler in Journal of Diabetes Science and Technology
Footnotes
Acknowledgements
None.
Abbreviations
ACR, albumin-to-creatinine ratio; AID, automated insulin delivery; BMI, body mass index; CGM, continuous glucose monitoring; CI, confidence interval; CSII, continuous subcutaneous insulin infusion; %CV, coefficient of variation; DCCT, Diabetes Control and Complications Trial; DD, diabetes duration; DME, diabetic macular edema; DR, diabetic retinopathy; EWDR, early worsening of diabetic retinopathy; GLP-1RA, glucagon-like peptide-1 receptor agonist; GMI, glucose management indicator; HbA1c, hemoglobin A1c; ICDSS, International Clinical Disease Severity Scale; IQR, interquartile range; isCGM, intermittently scanned continuous glucose monitoring; MDI, multiple daily injections; NZE, New Zealand European; OR, odds ratio; PDR, proliferative diabetic retinopathy; PRP, panretinal photocoagulation; RR, relative risk; SD, standard deviation; SG, sensor glucose; T1D, type 1 diabetes; %CV, coefficient of variation; %TAR, time above range; %TBR, time below range; %TING, time in normal glucose; %TIR, time in range.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AB discloses consultancy services for i-SENS. TW discloses speaker honoraria, travel support, and research funding from Tandem Diabetes Care, Dexcom, Insulet, and Beta Bionics. MIDB discloses research funding from Novo Nordisk, Medtronic, Ypsomed, Dexcom, Beta Bionics, and Insulet; speaker honoraria, travel support, or other honoraria from Novo Nordisk, Sanofi, Pfizer, Medtronic, Boehringer Ingelheim, Ypsomed, Dexcom, and Insulet; and advisory board roles for Tandem and Dexcom. RGP discloses speaker honoraria, advisory roles, and research support from Dexcom, Abbott, Novo Nordisk, Lilly, Boehringer Ingelheim, and Sanofi. BJW discloses research funding and speaker honoraria from Dexcom and Medtronic. The remaining authors disclose no conflicts of interest.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.