
Abstract
Background:
Use of automated insulin delivery (AID) systems has increased in people with type 1 diabetes (T1D); however, real-world data in preschool-age children remain limited. In this multicenter analysis, we assess real-world glycemic outcomes in preschool-age children using AID systems compared with those using multiple daily injections (MDIs).
Methods:
This retrospective, multicenter, cross-sectional analysis assessed current usage of AID systems and glycemic outcomes in preschool-age children ≤6 years across 37 pediatric sites in the T1D Exchange Quality Improvement Collaborative (T1DX-QI). Differences in AID use and HbA1c were evaluated using t tests and χ² tests, with multivariable logistic and linear regression models adjusting for age, race/ethnicity, diabetes duration and insurance type to assess associations between AID use and glycemic outcomes.
Results:
In this cohort of 3521 youth ≤6 years, the mean age was 4.6 (1.4), 47% female, 53% non-Hispanic white, 12% non-Hispanic black, and 14% Hispanic, and 31% with public insurance. Of these, 48% were using AID for insulin management with a mean HbA1c of 7.9% (1.7), compared with 52% using MDI with a mean HbA1c of 8.8% (2.2), P < .0001. In this cohort, 25% had an HbA1c <7%. AID use was associated with a greater odds of achieving HbA1c <7% (OR 1.91, 95% CI 1.57 to 2.33, P < .001).
Conclusions:
Real-world use of AID systems in preschool-age children (≤6 years of age) is associated with lower A1c levels and greater potential to achieve the American Diabetes Association (ADA) A1c target range of <7%.
Keywords
Introduction
Current trends demonstrate increasing use of automated insulin delivery (AID) systems for the management of type 1 diabetes (T1D) across the lifespan. 1 Clinical trials and real-world outcomes show that AID systems significantly improve glycemic outcomes with improvements in time in range (TIR) and reductions in hemoglobin A1c (HbA1c), while also reducing acute complications of hypoglycemia and diabetic ketoacidosis.2-5 The American Diabetes Association (ADA) recommends AID as the preferred method of insulin delivery for children and adults with T1D who can safely use them. 6
A recent meta-analysis of studies in children and adolescents (ages 6-18 years) with T1D found that AID use is associated with improvements in multiple glycemic outcomes, reducing the risk of both hyperglycemia and hypoglycemia. 7 Furthermore, participants with the highest baseline HbA1c levels experienced the greatest improvements in TIR and HbA1c. 8 Clinical trials of AID use in preschool-age children (≤6 years), including the LENNY trial of MiniMed 780G, the PEDAP trial of Tandem Control-IQ system, and the Omnipod 5 system, have shown similar benefits.9-11 Particularly for young children, insulin pumps can be helpful due to the small amounts of insulin administered that are challenging to give precisely with a syringe or insulin pen. In addition, reducing the need for multiple daily injections (MDIs) can alleviate needle phobia and in general reduce distress in both children and their caregivers. 12 The aforementioned trials contributed to subsequent regulatory approvals and broader clinical adoption of AID systems in young children, although commercial availability for older children and adults (MiniMed in 2016, Control IQ in 2018, and Omnipod 5 in 2022) may have preceded regulatory approvals for preschool-age children, and there may have been off-label use in this young population.
There is limited data on real-world outcomes of preschool-age children (≤6 years) using AID systems, and across different racial and ethnic cohorts. In this multicenter analysis, we sought to assess real-world glycemic outcomes in preschool-age children using AID systems compared with those using MDI.
Methods
This retrospective, multicenter, cross-sectional analysis was conducted as part of the T1D Exchange Quality Improvement Collaborative (T1DX-QI), engaging over 60 diabetes clinics in the United States, evaluating the current state of diabetes care and sharing data and best practices to improve care delivery in T1D. 13 A total of 37 pediatric sites contributed data for this cross-sectional analysis assessing current usage of automated insulin delivery systems in preschool-age children ≤6 years.
Our study population of interest was patients aged 0 to 6 years, 14 diagnosed with T1D, with data available on insulin management and glycemic outcomes. Data are submitted from the individual sites through electronic medical records (EMR) data mapping on an ongoing basis. Data were collected from January 16, 2018, to December 23, 2025, with available data analyzed from the most recent clinic visit associated with their device. All patients with a data point from the above-mentioned study time frame were included in the analysis if their latest visit was within that period. Of these, 11 patients were reported from 2018 to 2020, 21 reported in 2021, and the remaining patient data points from 2022 onward. The main outcome of interest was the absolute number and percentage of preschool-age children using AID systems.
Institutional review board approval was obtained by a central review board (Western Institutional Review Board) as an exempt study, and each site obtained local IRB approval as needed, with a waiver of consent.
Statistical Analysis
Descriptive statistics were used to summarize data. The primary outcome was use of an AID system, and the secondary outcome was HbA1c. The most recent HbA1c level from the latest encounter coinciding with their device date during the study period was collected. Mean and median HbA1c for each group were calculated. The percentages of youth with HbA1c
Results
Patient Clinical Characteristics and Demographics
In this cohort of 3521 youth, the mean age was 4.6 (1.4), 47% women (female), 53% non-Hispanic white, 12% non-Hispanic black, and 14% Hispanic, and 31% with public insurance (Table 1).
AID Users Versus MDI Users Among Preschool-Age Children Less Than 7 Years Old.
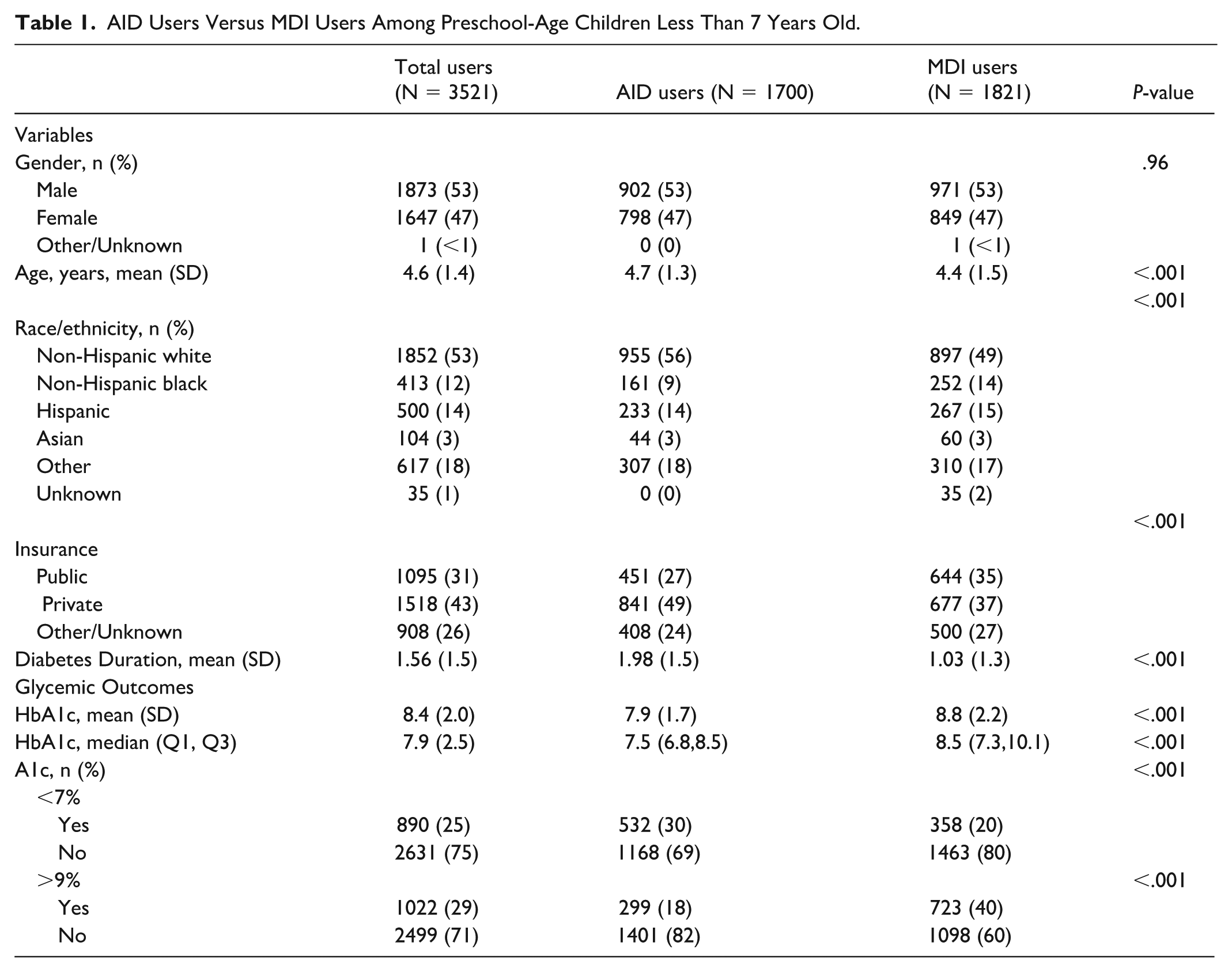
Of these, 48% were using AID for insulin management with a mean HbA1c of 7.9% (±1.7), compared with 52% using MDI with a mean HbA1c of 8.8% (±2.2), P < .001 (Figure 1). The median time from diagnosis to initiation of AID was 0.86 years (IQR 0.29, 1.70).
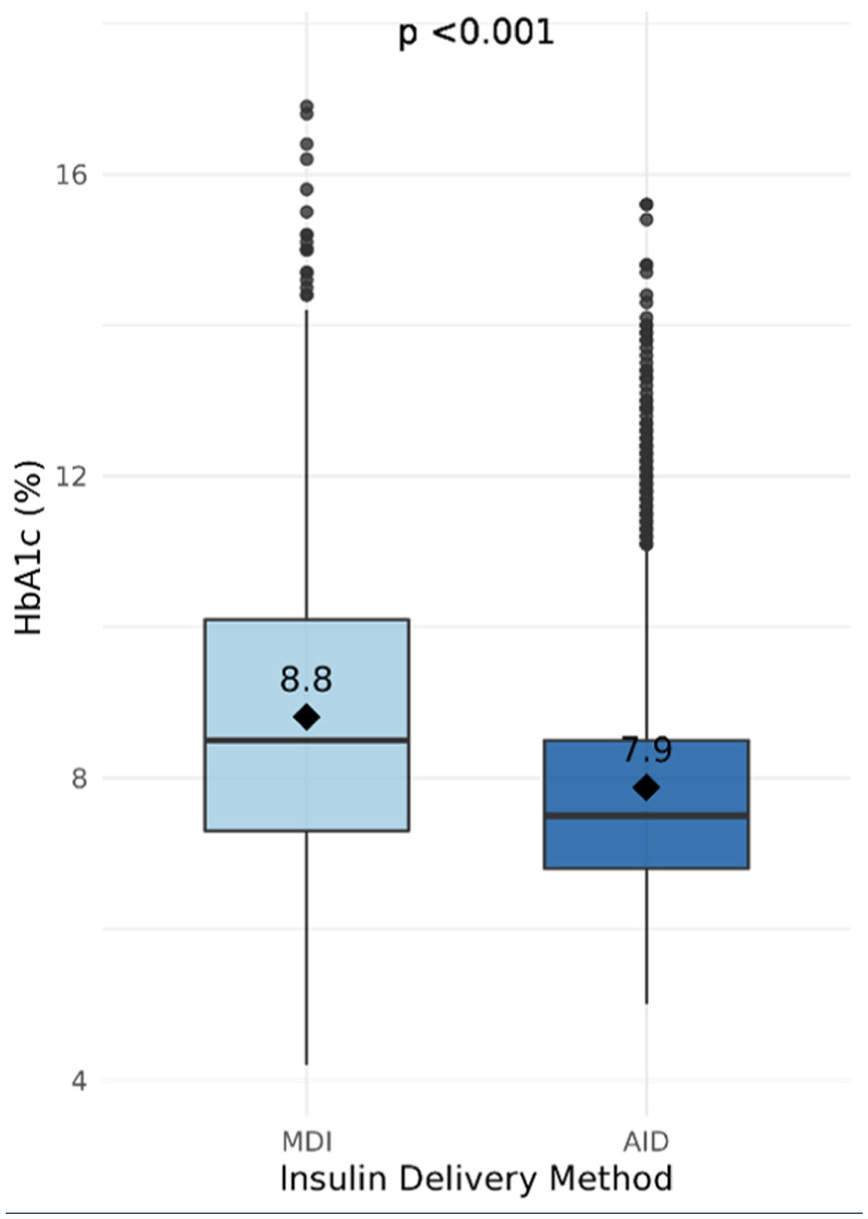
HbA1c by insulin delivery modality (MDI vs AID).
Automated insulin delivery users were more likely to be older (4.7 vs 4.4, P < .001), non-Hispanic white race (56% vs 49%, P < .001), have a longer duration of diabetes (1.9 vs 1.0 years, P < .001), and have private insurance (49% vs 37%, P < .001). Logistic regression adjusting for age, insurance type, HbA1c, and diabetes duration showed that compared with non-Hispanic white individuals, non-Hispanic black individuals had significantly lower odds of AID use (OR 0.61, 95% CI 0.47 to 0.79, P < .001) (Table 2).
Association Between AID Use and Race/Ethnicity.
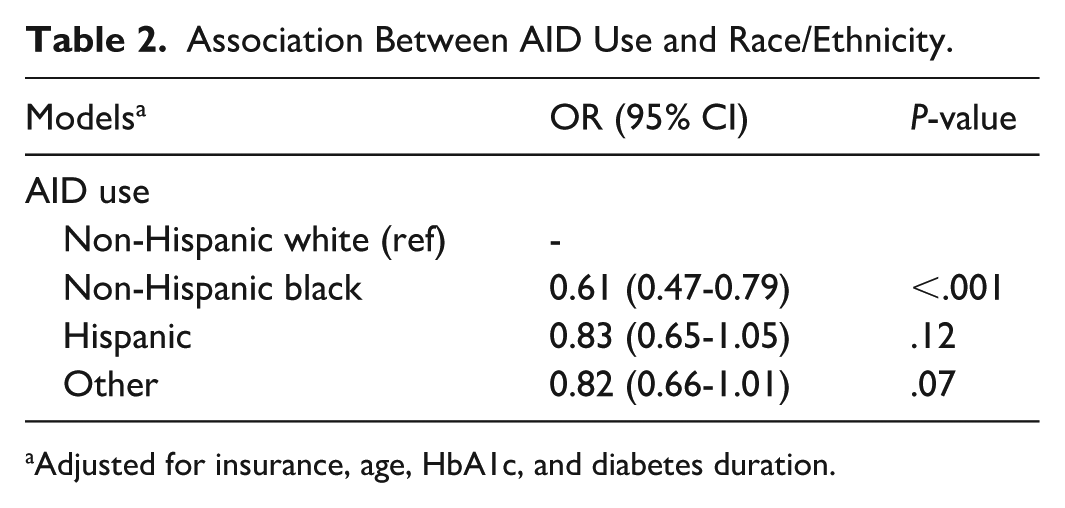
Adjusted for insurance, age, HbA1c, and diabetes duration.
Glycemic Outcomes
Overall, 25% of this cohort had an HbA1c meeting the ADA target of <7%. More children using AID achieved an HbA1c <7% (30% vs 20%, P < .001), and fewer had an HbA1c >9% (18% vs 40%, P < .001) compared with those using MDI. There was a difference in HbA1c values by race/ethnicity with a mean HbA1c of 8.5% in non-Hispanic white, 9.3% in non-Hispanic black, and 8.4% in Hispanic youth (P < .001). When evaluating HbA1c levels for only youth on AID systems, mean HbA1c was 7.8% in non-Hispanic white, 8.8% in non-Hispanic black, and 8% in Hispanic youth (P < .001). Similarly, patients with AID with private insurance had a lower mean HbA1c compared with those with public insurance (7.6% vs 8.4%, P < .001). As shown in Table 3, logistic regression models adjusting for age, race/ethnicity, insurance, and diabetes duration showed that AID use is associated with a greater odds of achieving HbA1c <7% (OR 1.91, 95% CI 1.57 to 2.33, P < .001).
Association Between AID Use and Glycemic Outcomes.
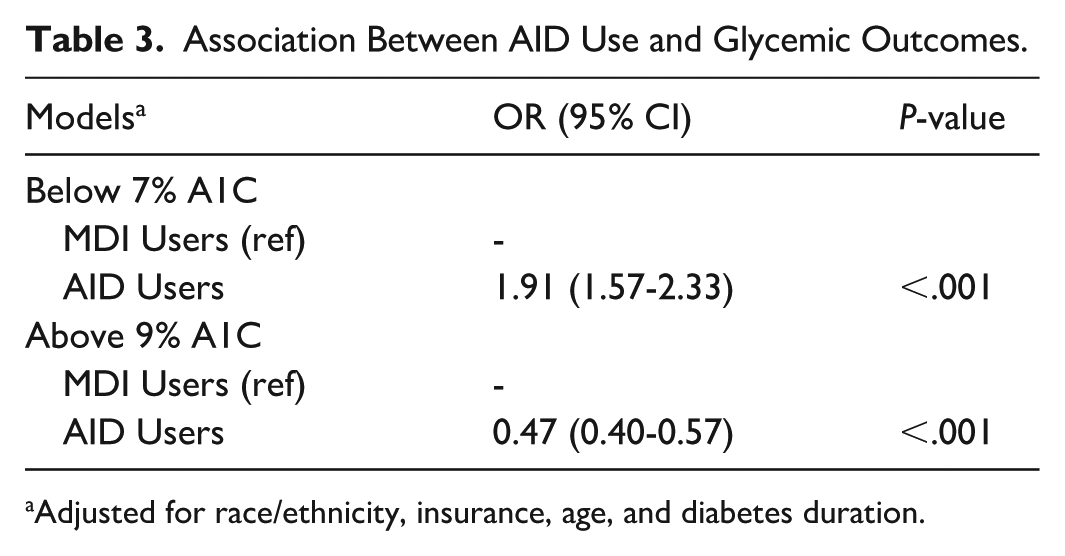
Adjusted for race/ethnicity, insurance, age, and diabetes duration.
A linear regression model adjusting for age, race/ethnicity, diabetes duration and insurance type showed that AID use is associated with a −0.63 difference in HbA1c compared with those using MDI (95% CI −0.77 to −0.49, P < .001).
Discussion
In this large, multicenter, real-world cohort of preschool-age children less than 7 with T1D, use of AID systems was associated with lower HbA1c compared with MDI. To our knowledge, this represents the largest multicenter real-world study of AID use in preschool-age children to date, addressing an important evidence gap in a population often underrepresented in clinical trials. Overall, 25% of children in this cohort achieved an HbA1c meeting the ADA target of <7%, with a greater proportion of children using AID achieving this goal compared with those using MDI. Together, these findings support the real-world effectiveness of AID systems in helping young children achieve glycemic outcomes closer to recommended targets in routine clinical practice.
Our findings are consistent with clinical trial data demonstrating improved glycemic outcomes in preschool-age children using AID systems. In the Omnipod 5 pivotal trial, the proportion of participants achieving HbA1c <7% increased from 31% at baseline to 54% during the study period, while mean HbA1c improved from 7.4% to 6.9%, reflecting a cohort close to meeting glycemic goals at baseline. 11 Similarly, in the PEDAP trial, 48% of participants achieved an HbA1c <7% after 13 weeks of Control-IQ use. 10 A large registry study from the European Diabetes Prospective Follow-up Database [DPV] demonstrated that young children (<7 years) have the highest AID use rates, and 43.6% achieve an HbA1c <7%, perhaps due to better access to care and diabetes technologies.15,16 In this study, 30% of children using AID in this real-world cohort achieved an HbA1c <7%. Although this proportion is lower than that observed in clinical trials, it likely reflects broader clinical heterogeneity, greater patient diversity, and less selective baseline glycemic control typical of real-world populations. Our cohort also included more patients from minoritized racial and ethnic populations (12% non-Hispanic black and 14% Hispanic) compared with the randomized controlled trials mentioned above, which highlights the real-world glycemic improvements seen in all children with T1D using AID systems. However, consistent with prior studies, while children using AID systems experience improvements in HbA1c, racial and ethnic disparities in HbA1c persist despite use of these advanced diabetes technologies.17-19
Several factors likely contribute to these persistent disparities in both AID use and glycemic outcomes. Structural barriers, such as differences in insurance coverage and access to routine pediatric diabetes care, may limit uptake of AID technologies among minoritized populations. 20 In addition, variability in clinician prescribing practices may influence which families are offered or supported in initiating AID. 21 At the patient and caregiver level, differences in health literacy, language barriers, competing socioeconomic demands, and trust in medical technology may further impact AID adoption and sustained use. 20 Disparities in HbA1c outcomes despite AID use suggest that access alone is insufficient and that differences in device utilization, training, and ongoing support may also play a role.22,23 Addressing these gaps requires multifaceted interventions, including efforts to improve patient and caregiver education, increase clinician awareness and equitable prescribing practices, expand insurance coverage and affordability, and provide ongoing support for technology use in the patient’s primary language.24,25
While our focus is on preschool-age children, the clinical impact of AID systems in older children and adolescents has demonstrated similar improvements. A recent meta-analysis evaluating clinical trials outcomes in youth ages 6 and older on AID systems showed that of 901 participants (median age 12 years), TIR increased an average of 11.5% (from a baseline of 50%), and HbA1c decreased by 0.41% from a baseline average of 8.5%. 7 Although clinical trials and real-world data demonstrate improvements in TIR and reduction in hypoglycemia with initiation of AID therapy that persists beyond 1 year after initiating AID therapy, there are some limitations to its usage in very young children.9-12 These systems often require a minimum total daily dose of insulin (e.g. Omnipod 5 requires 6 units, MiniMed 780G requires 8 units, and Tandem CIQ requires 6 units daily minimum for AID) to initiate automated mode. Young children in this age range may not consistently utilize enough insulin to initiate or sustain automated mode, and thus may not realize the full benefits of AID therapy, although pump use in manual mode still allows for smaller and more precise dosing increments than MDI. In addition, young children often have highly variable insulin requirements due to unpredictable eating patterns, activity, growth, and illness, which may challenge algorithm performance despite overall improvements in safety, glycemic stability, and glycemic outcomes. Finally, consistent with guidance from the ADA and the International Society for Pediatric and Adolescent Diabetes, 14 successful AID use in this population requires high caregiver engagement, frequent sensor wear, and access to diabetes technology support, all of which may contribute to variability in real-world effectiveness.
Strengths and Limitations
To our knowledge, this study represents the largest analysis of real-world data in preschool-age children to date, with a multicenter and representative sample across racial/demographic groups and from across the United States. Limitations of this study include the cross-sectional nature representing one point in time and it does not examine improvements over time. In addition, we did not have available continuous glucose monitoring data parameters and could not evaluate TIR as a main outcome, nor hypoglycemia. In addition, we did not have data on time spent in automated mode, which may influence the effectiveness of the AID system. Finally, although unlikely, there is no data available on whether any of the AID users used diluted insulin. Future real-world longitudinal trials may elucidate the true real-world impact of these technological advances.
Conclusions
In conclusion, real-world use of AID systems in preschool-age children (≤6 years of age) is associated with lower HbA1c levels and greater potential to achieve ADA target range of <7%. These findings underscore the importance of initiatives to increase patient awareness of AID benefits, enhance physician knowledge of AID management, and expand equitable access to increase uptake of AID technologies in this young age group.
Footnotes
Abbreviations
AID, automated insulin delivery; T1D, type 1 diabetes; T1DX-QI, T1D Exchange Quality Improvement Collaborative.
Author Contributions
RMW conceived of the study. All authors collected the data. EO analyzed the data. RMW wrote the manuscript. All authors reviewed, edited, and approved the final version of the manuscript. RMW and EO had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Helmsley Charitable Trust funds the T1D Exchange QI Collaborative. The funding organization had no role in the design and conduct of the study, collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: RMW reports receiving research support from Lilly Diabetes, Novo Nordisk, and Sanofi outside the submitted work, and is a consultant for Sanofi and Mannkind. JCW receives research support from Abbott Diabetes Care, outside the submitted work. NM and JCW serve as medical advisors to T1D Exchange and receive compensation from T1D Exchange. The other authors declare no conflicts of interest.
Data Availability Statement
All data generated or analyzed in this study are included in this article. Further enquiries can be directed to the T1D Exchange QI Collaborative.