
Abstract
Background:
Severe headaches, including migraines, have been reported in 4.5% of preschool children, with prevalence increasing to 27.4% in older teenagers. Patients with intractable headaches, including status migrainosus, may be admitted to the hospital if outpatient treatments are unsuccessful. Intravenous dihydroergotamine (DHE) is commonly prescribed for the management of pediatric inpatients with status migrainosus.
Aim:
The primary objective of this study is to determine if acupuncture is as effective as a complementary treatment to intravenous DHE in treating status migrainosus in the pediatric population. The primary outcomes assessed were pain, nausea, and length of stay in the hospital.
Methods:
This is a retrospective chart review. We performed electronic keyword searches of patient records between January 2005 and January 2022 for patients younger than 18 years and with a chief complaint of intractable headache who received acupuncture treatment at our center. We compared these records against data from an equal number of recent admissions to our hospital who fit the same criteria, but who did not receive acupuncture.
Results:
Patients who received acupuncture experienced a significantly lower rate of nausea (61.1% (66/108) versus 77.8% (84/108), odds ratio = 0.45, 95% confidence intervals: 0.25–0.81, p = 0.008). There were no significant differences observed in level of pain or length of stay.
Conclusion:
Acupuncture significantly mitigates the nausea caused by DHE treatment for status migrainosus in pediatric patients and can serve as a complementary therapy.
INTRODUCTION
Intractable headaches in the pediatric population are a major cause of disability and decreased quality of life. 1 The prevalence of severe headaches, including migraines, increases with age throughout childhood, with the most recent national data estimating that 4.5% of 4- to 6-year-olds and 27.4% of 16- to 18-year-olds experience severe headaches. 2 Intractable headaches are headaches that do not respond to standard treatment, including rest, hydration, and medication. Status migrainosus is a type of intractable headache, defined as a severe migraine that has continued for greater than 72 h and has not responded to the usual treatments for migraines. Status migrainosus is associated with both pain and nausea, and it is the most common form of intractable headache that we treat at our center.
Patients with status migrainosus are typically admitted to the hospital if outpatient treatment regimens fail. Intravenous dihydroergotamine (DHE) is one of the most common medications for the treatment of pediatric patients with status migrainosus. 3 At our institution, pediatric patients can elect to receive acupuncture as part of a complementary treatment to DHE. In this retrospective chart review, we evaluated the effectiveness of acupuncture in treating pediatric status migrainosus. We hypothesized that integrating acupuncture into the clinical care of pediatric patients with severe headaches would result in lower pain scores, lower rates of nausea, and shorter lengths of hospital stay.
METHODS
The Medical Acupuncture Service at Boston Children’s Hospital was established in September 2000. We conducted a retrospective review of records from January 2005 to January 2022 for patients (1) 18 years old or younger and (2) who received acupuncture treatment for the chief complaint of status migrainosus. We excluded patients over 18 years, patients with complex comorbidities, patients for whom the headache was a symptom accompanying other non-neurological medical issues, postoperative patients, or patients who were hospitalized for more than a week. A total of 108 patient records met the search criteria and were included in the study. The Institutional Review Board at Boston Children’s Hospital approved this research project.
These inpatient acupuncture consultations were initiated by the patient’s pediatrician, neurologist, or family. We provided the patients with acupuncture treatment one to two times a week. The acupuncture treatment plans were formulated according to the Traditional Chinese Medicine syndrome pattern.4–11
The main acupuncture points from the protocol set up by our Medical Acupuncture Service include the following:
Local Points: GB 20 (Feng Chi), GV 20 (Bei Hua), Ex-KH 5 (Tai Yang)
Distal Points: LI 4 (Ho Gu), TE 5 (Wai Guan), LR 3 (Tai Chung)
Acupuncture treatment according to pain location:
Yang ming: EX-HN3 (Yintang), LI 4 (Ho Gu), ST 44 (Nei Ting)
Shao yang: Ex-KH 5 (Tai Yang), TE 5 (Wai Guan), GB 41 (Zu Lin Qi)
Tai yang: GB 20 (Feng Chi), BL 60 (Kunlun), SI 3 (Hou Xi)
Acupuncture points to treat symptoms:
Menstruation-associated headache: SP 6 (San Ying Jiao), SP 10 (Xue Hai)
Severe nausea and/or vomiting: CV 12 (Zhong Wan), PC 6 (Nei Guan)
Stress-associated headache: GV 20 (Bai Hua), LR 3 (Tai Chung), LR 5 (Li Gou)
Exhaustion: ST 36 (Zu San Li), CV 6 (Ji Zhong), BL 20 (Pi Shu), BL 23 (Shen Shu)
The acupuncture treatment followed standard guidelines and procedures. We used SEIRIN® sterilized acupuncture needles. The acupuncture treatment was provided by either Dr. Yuan-Chi Lin or Dr. Cynthia S. Tung. Both clinicians have more than 15 years’ experience in providing acupuncture care.
To facilitate a comparison with the 108 patient records we were analyzing, we searched the electronic record for the most recent cases of status migrainosus admitted to Boston Children’s Hospital as of January 2022 who did not receive acupuncture treatment. We then selected the 108 most recent cases that met all of our original search criteria for the retrospective chart review so as to have an equal number of patients for comparison. The two cohorts were comparable in age (Fig. 1) and gender (Fig. 2). We analyzed admission pain score, discharge pain score, length of hospital stay, and nausea or vomiting in both sets of patient data.
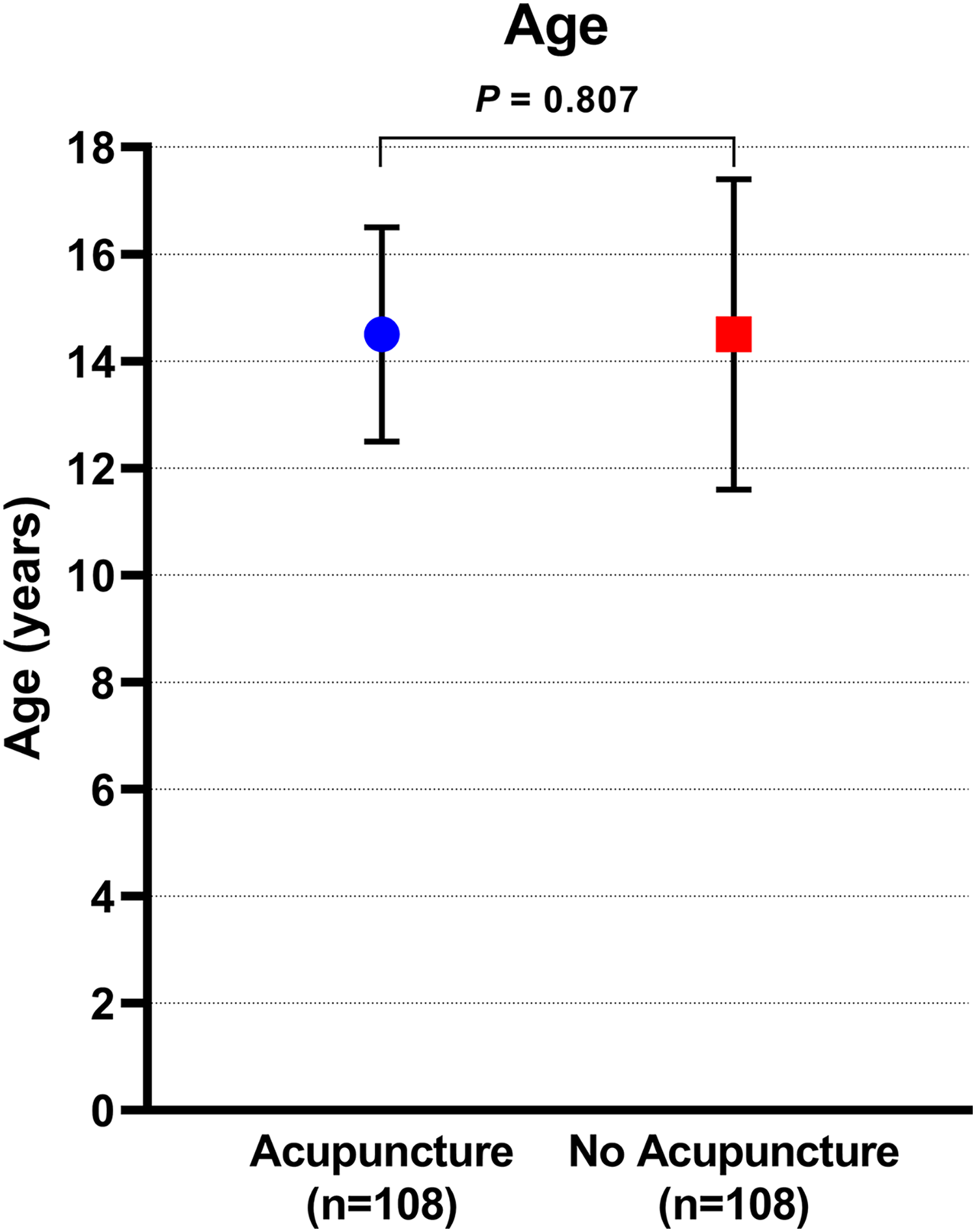
Age difference between the acupuncture and non-acupuncture groups.
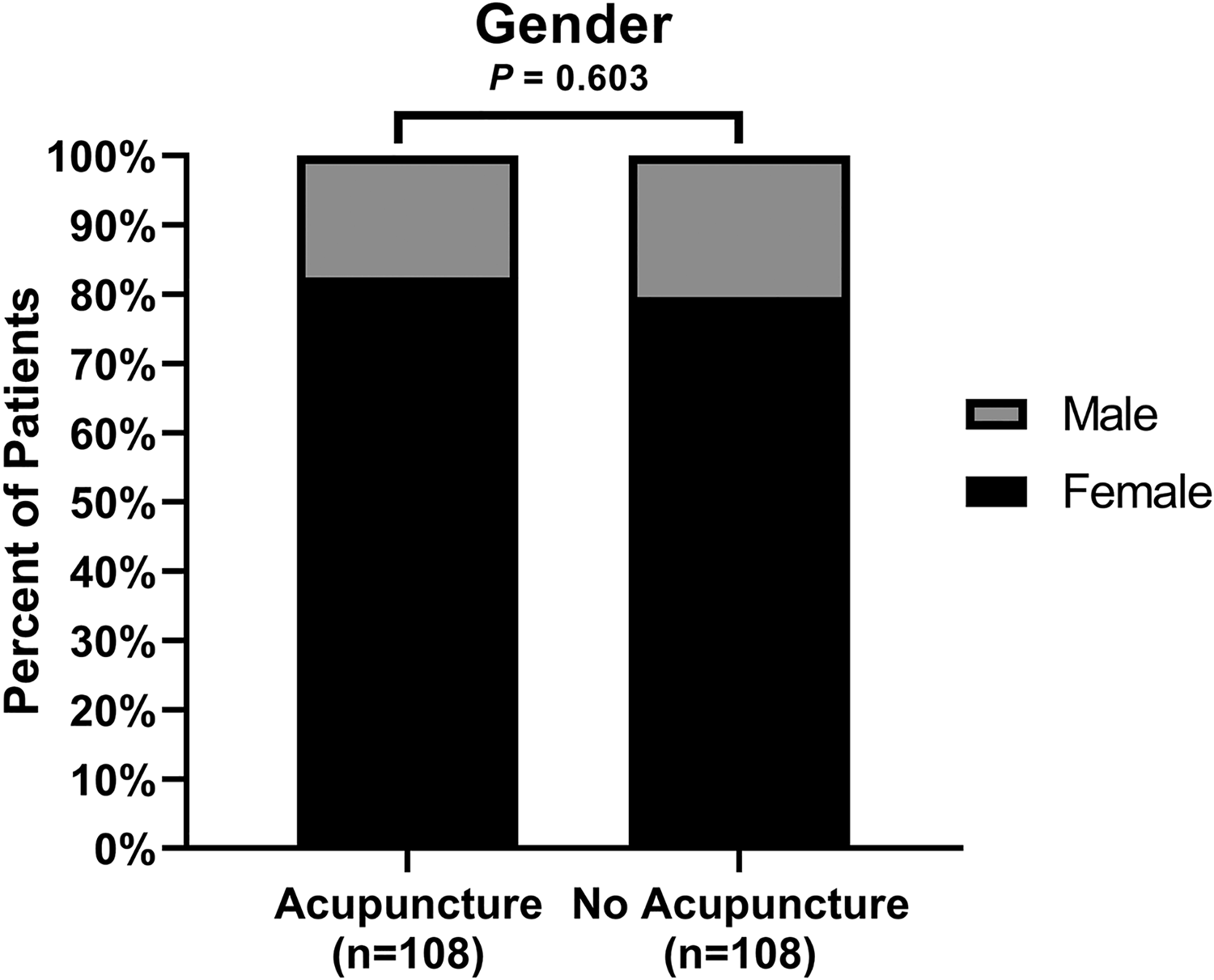
Gender difference between the acupuncture and non-acupuncture groups.
Continuous variables are presented as mean ± standard deviation, and categorical variables are presented as n (%). The comparisons of acupuncture and non-acupuncture patient groups were performed using Student’s t-test for continuous data and using the chi-square test or Fisher’s exact test for categorical data. Logistic regression was implemented to calculate odds ratios with 95% confidence intervals (CI) and p values. A two-tailed p < 0.05 was considered statistically significant. Statistical analyses were performed using Stata software (version 17.1, StataCorp LLC, College Station, TX).
RESULTS
The comparison between pediatric patients with status migrainosus who received acupuncture and those who did not is summarized in Table 1. There were no significant differences observed in the age (Fig. 1), gender (Fig. 2), length of hospital stay (Fig. 3), or pain scores (Fig. 4) between the two cohorts. However, patients who received acupuncture experienced a significantly lower rate of nausea (61.1% (66/108) vs. 77.8% (84/108), odds ratio = 0.45, 95% CI: 0.25–0.81, p = 0.008) (Fig. 5) than patients who did not. In addition, Figure 6 compares the rate of DHE infusion between acupuncture versus non-acupuncture groups.
Comparison of Patients Receiving Versus Not Receiving Acupuncture
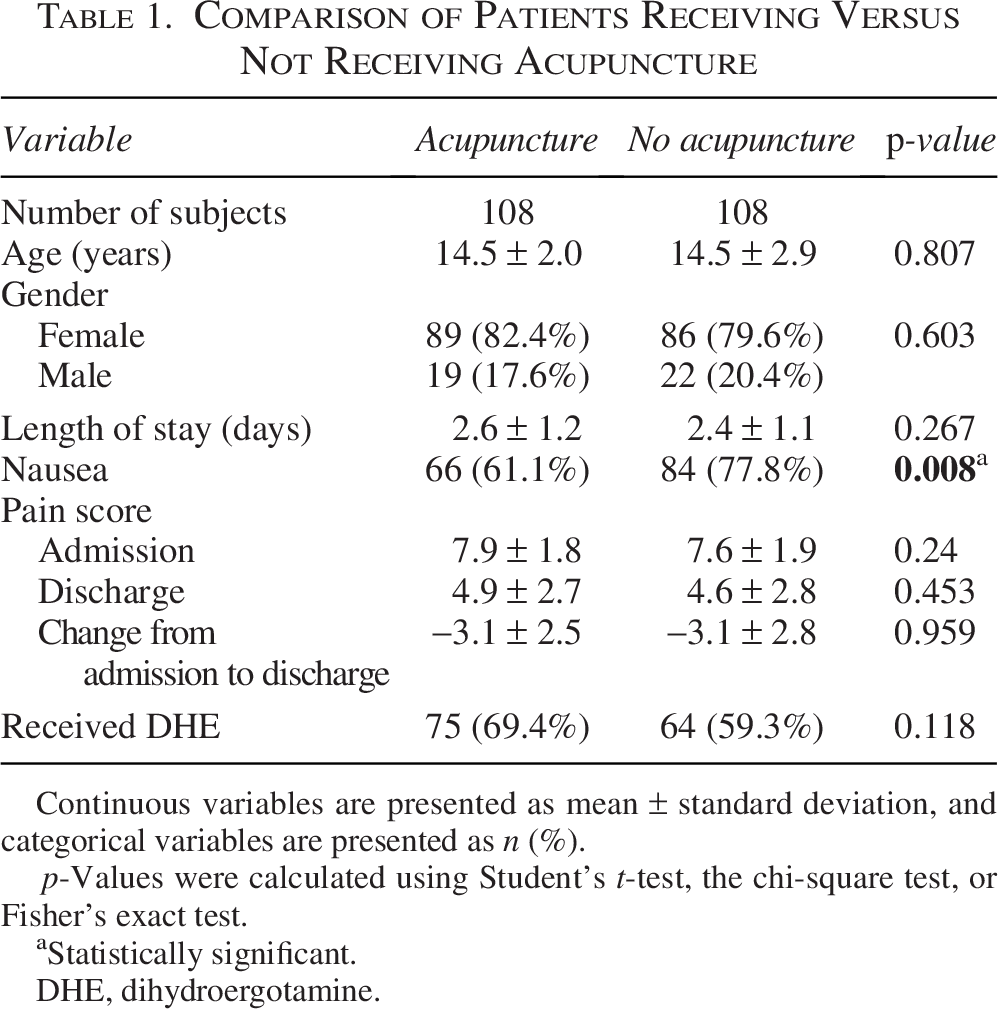
Continuous variables are presented as mean ± standard deviation, and categorical variables are presented as n (%).
p-Values were calculated using Student’s t-test, the chi-square test, or Fisher’s exact test.
Statistically significant.
DHE, dihydroergotamine.
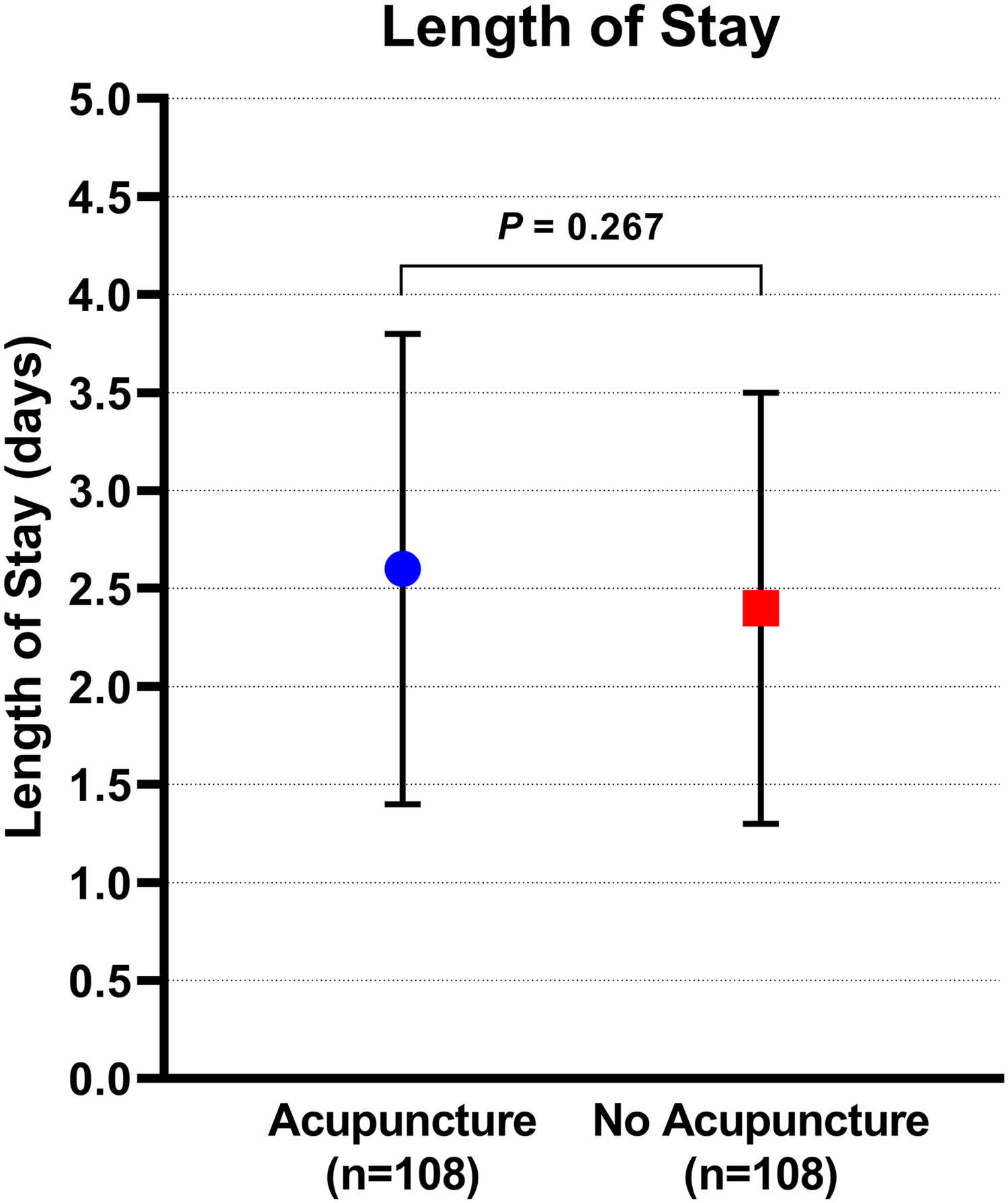
Length of stay difference between the acupuncture and non-acupuncture groups.
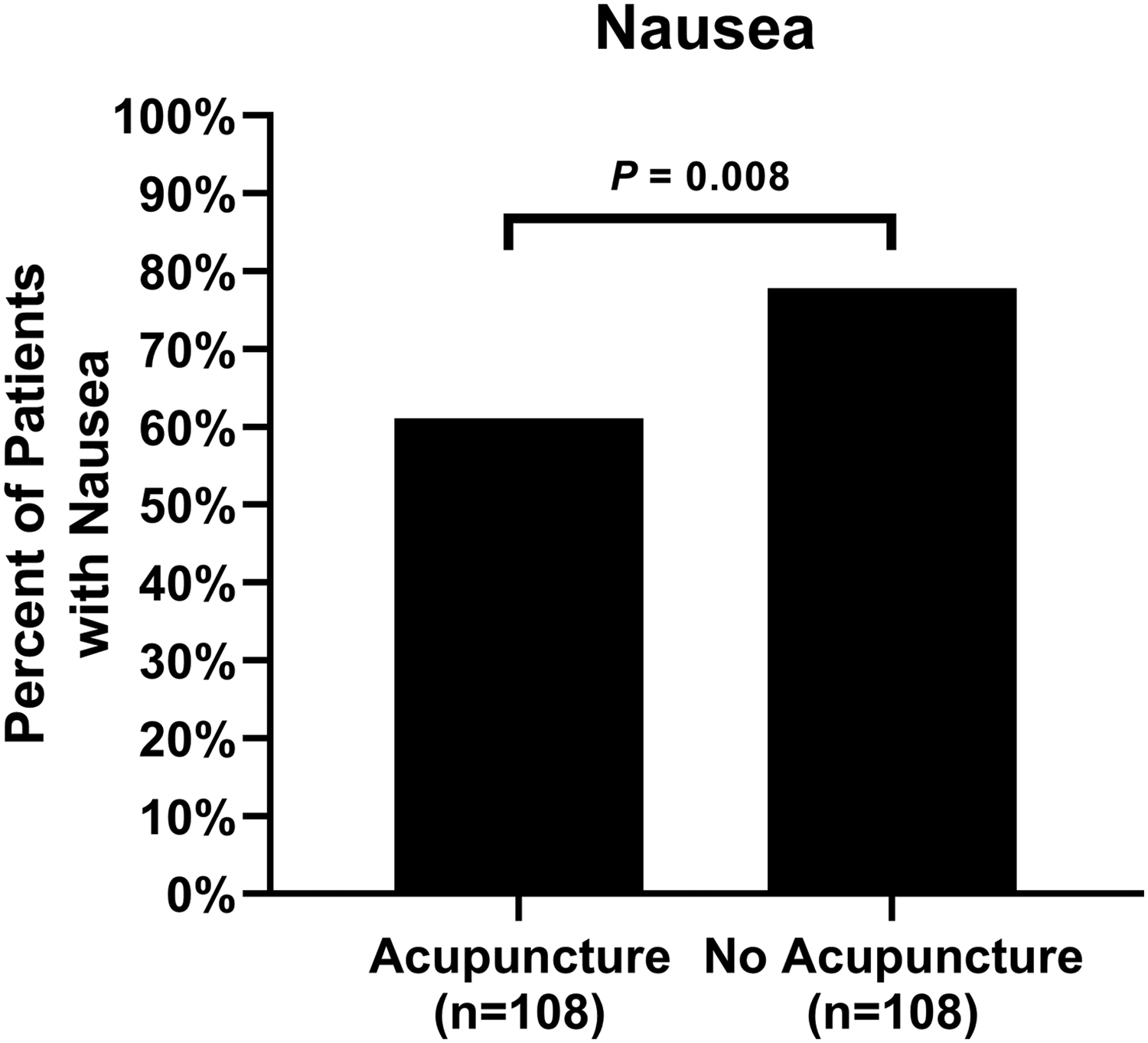
Incidence of nausea difference between the acupuncture and non-acupuncture groups.
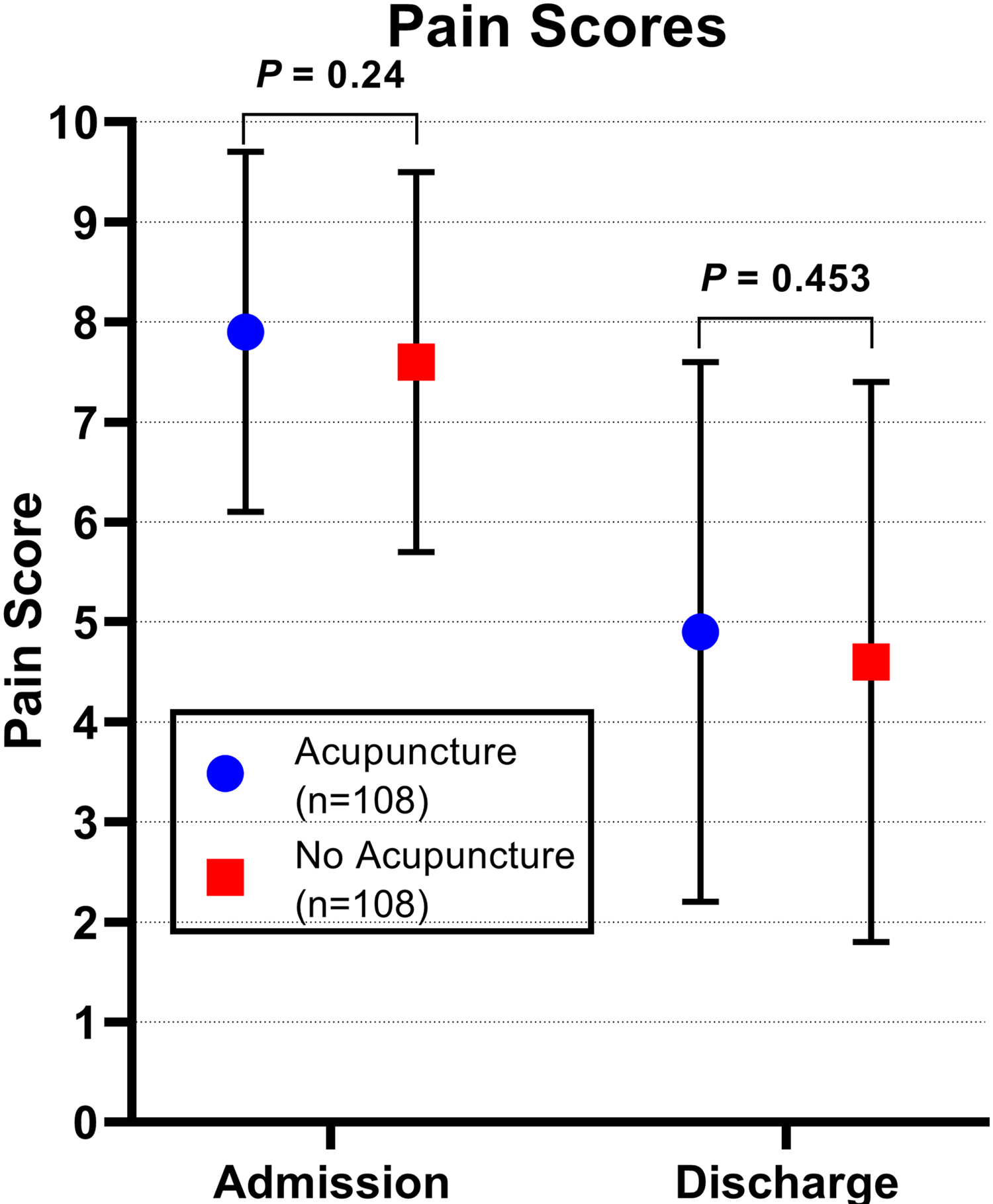
Comparison of headache pain scores on admission and discharge between the acupuncture and non-acupuncture groups.
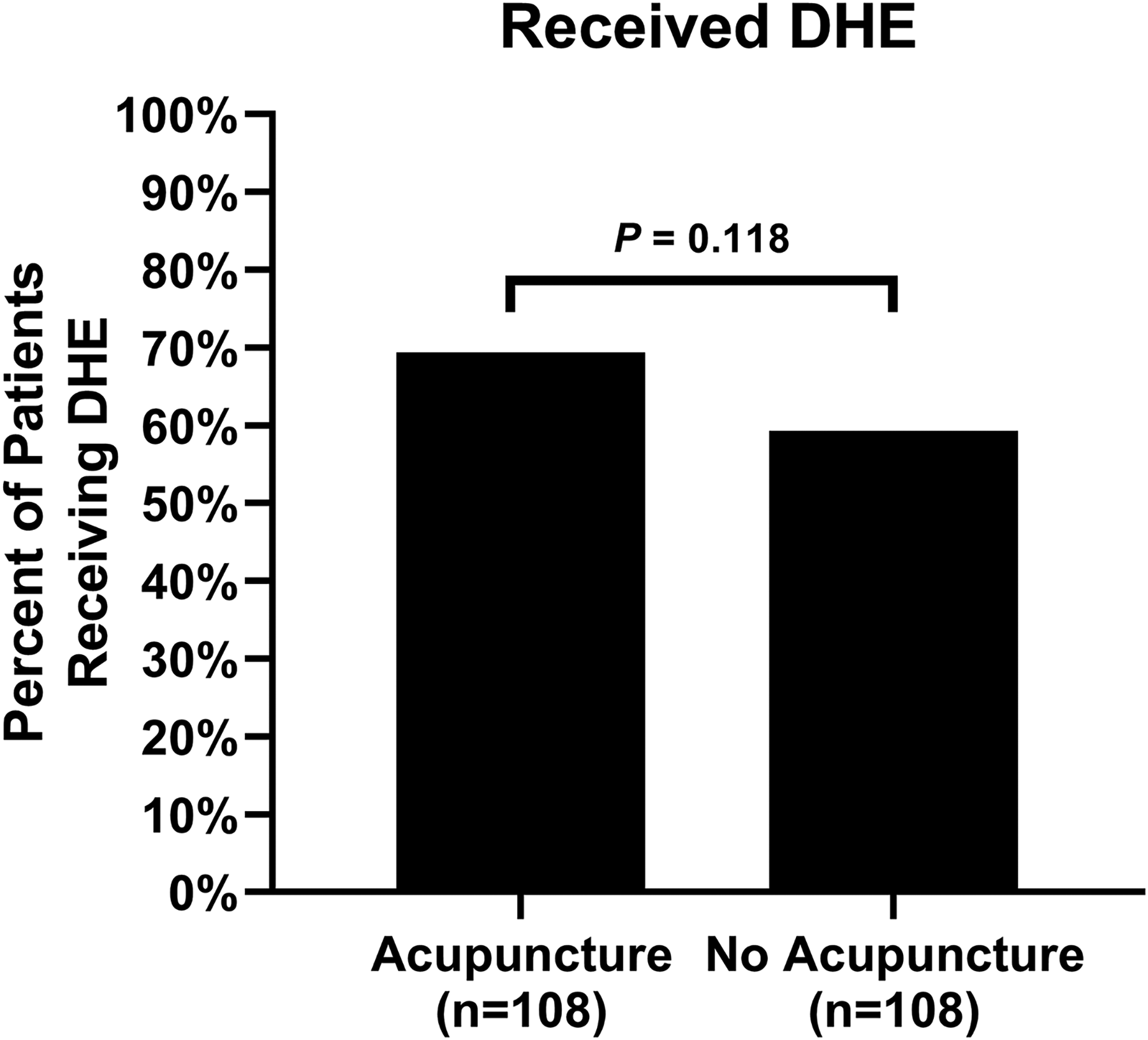
Incidence of receiving DHE infusion compared between the acupuncture and non-acupuncture groups. DHE, dihydroergotamine.
Overall, 139 patients received DHE, and 117/139 (84%) had nausea. There were 77 patients not receiving DHE, and 33/77 (43%) had nausea (p < 0.001). When we look only at patients with acupuncture, there is a statistically significant association between nausea and receiving DHE (odds ratio = 6.8, 95% CI: 2.74–16.8, p < 0.001). Similarly, when looking at patients without acupuncture, there is a significant association between nausea and receiving DHE (odds ratio = 18.6, 95% CI: 5.1–68.2, p < 0.001). Acupuncture can be used as an adjunctive treatment for hospitalized pediatric patients with status migrainosus, especially for alleviating nausea related to DHE.
DISCUSSION
The primary finding of this retrospective chart review was that acupuncture was effective as a complementary treatment to intravenous DHE for the management of nausea experienced by patients with status migrainosus but did not appear to have an effect on the patients’ pain or length of hospital stay.
This study has several limitations, including a retrospective design, reliance on data from a single institution, and the involvement of multiple pediatric neurologists with varying approaches to treating status migrainosus.
More studies are needed to fully determine the effectiveness of acupuncture as a complementary treatment for status migrainosus. Several other studies have shown the efficacy of acupuncture therapy for migraine headaches. Existing studies suggest that acupuncture can be as effective as prophylactic medications for the prevention of migraine headaches 12 and is also a viable treatment option for patients with frequent episodic or chronic tension-type headaches. 13
Acupuncture is increasingly being utilized for managing pediatric pain in outpatient settings. 14 Our analysis indicates that acupuncture can serve as an effective complementary treatment for hospitalized pediatric patients with status migrainosus, particularly in reducing nausea. More research is needed to determine the full scope of its effectiveness in mitigating the symptoms of status migrainosus.
Footnotes
ACKNOWLEDGMENTS
The authors thank Ms. Jennani Durai for her thoughtful review of this article.