
Abstract
Background:
Asthma is a chronic obstructive pulmonary disease characterized by episodic airway obstruction, hyperresponsiveness, and inflammation, leading to symptoms such as shortness of breath, wheezing, chest tightness, and cough. Complementary and alternative medicine, including acupuncture and moxibustion, is increasingly used to manage asthma symptoms. There is a lack of studies pertinent to lung-specific points such as BL 13 (a back shu point of the lung) and LU 9 (source point of the lung meridian). This study evaluates the impact of acupuncture and moxibustion at BL 13 and LU 9 on pulmonary function in patients with bronchial asthma.
Methods:
In this single-blinded randomized controlled trial, a total of 60 participants with bronchial asthma will be recruited and randomly assigned into two groups. The study group will receive acupuncture and moxibustion at BL 13 and LU 9 for 20 min a day, 5 days a week for 2 weeks, while the control group will receive placebo acupuncture for the same period. Pulmonary function tests (PFT) and quality of life (QoL) will be assessed at baseline and after 14 days.
Results:
Acupuncture and moxibustion at BL 13 and LU 9 acupuncture points might significantly improve PFT and QoL than the placebo acupuncture points in patients with bronchial asthma.
Conclusion:
Two weeks of acupuncture and moxibustion at BL 13 and LU 9 may improve pulmonary function and quality of life in patients with bronchial asthma. These findings may help to support the integration of these techniques into standard asthma care.
INTRODUCTION
Asthma is an obstructive pulmonary disease characterized by episodic airway obstruction and hyperresponsiveness usually accompanied by airway inflammation. It presents as shortness of breath, wheezing, chest tightness, and cough, which can occur in relation to triggers but may also occur spontaneously. 1 These episodes are usually associated with widespread but variable mild or severe symptoms that are often reversible either spontaneously or with treatment. 2 The prevalence of people affected with asthma worldwide accounts for 262 million in 2019 3 and caused 455,000 deaths. India is a home for 6% of children and 2% of adults suffering from this chronic disease. 4 The global burden of disease estimated the total burden of asthma in India as 13.09% compared to the global percentage. 5 The exact cause of asthma is not known. The risk factors include infections, air pollution, allergens, or irritants such as smoke, sprays, diet, seasonal variation, and occupational exposure. 6 The development of asthma involves an interplay between risk factors and exposures and genetic predisposition. 1 Patients with untreated asthma are prone to exacerbation and deterioration of lung functions, affecting day-to-day activities and quality of life. 7 Pharmacological management of the disease comprises bronchodilators such as beta-2 agonists and muscarinic antagonists (salbutamol and ipratropium bromide, respectively) and anti-inflammatories such as inhaled steroids. 8 However, long-term use of medicines brings about a slew of adverse reactions, including disturbed mood and physical symptoms. 9 Nonpharmacological management includes weight loss, smoking cessation, occupational change, and self-monitoring. 8
Complementary and Alternative Medicine (CAM) is increasingly used in the management of asthma. 10 Acupuncture and moxibustion are divisions of traditional Chinese medicine (TCM) involving the stimulation of certain points in the skin with the use of needles and external heat using moxa sticks for preventive and therapeutic purposes.11,12 It is widely used in the treatment of asthma and has certain advantages in reducing the recurrence rate, relieving symptoms, and improving the pulmonary function variables. 13 Previous studies have shown the efficacy of acupuncture solitarily or in combination with moxibustion14–16 involving several acupuncture points from different meridians. However, there is a lack of studies pertinent to lung-specific points such as BL 13 (a back shu point of the lung) and LU 9 (source point of the lung meridian) that address both the organ-level (BL13) and channel-level (LU9) dysfunction according to TCM in bronchial asthma, making them a synergistic and focused point combination for targeting respiratory symptoms and improving pulmonary function.
OBJECTIVE
Primary Objective
To study the effect of acupuncture with moxibustion at BL 13 and LU 9 on pulmonary function in patients with bronchial asthma.
Secondary Objective
To study the effect of acupuncture with moxibustion at BL 13 and LU 9 on quality of life measured using the Asthma Quality of Life Questionnaire (AQLQ).
TRIAL DESIGN: A RANDOMIZED CONTROLLED TRIAL
A single-blinded randomized controlled study design will be adopted for this study. All the eligible subjects will be randomly divided into two groups, a study group and a control group, after an interview and obtaining informed consent. Institutional ethical committee (IEC) approval was taken, vide letter number (RES/IEC-GYNMC/2023/191). This study was prospectively registered at the Clinical Trial Registry India (CTRI) (CTRI registration no: REF/2023/12/076946. The study group will undergo acupuncture with moxibustion at BL 13 and LU 9 for 20 min once 5 days a week for 2 weeks. The control group will receive placebo acupuncture for 20 min for the same duration as the study group. Outcomes will be assessed at baseline and on day 14 after intervention. The trial profile is shown in Figure 1.
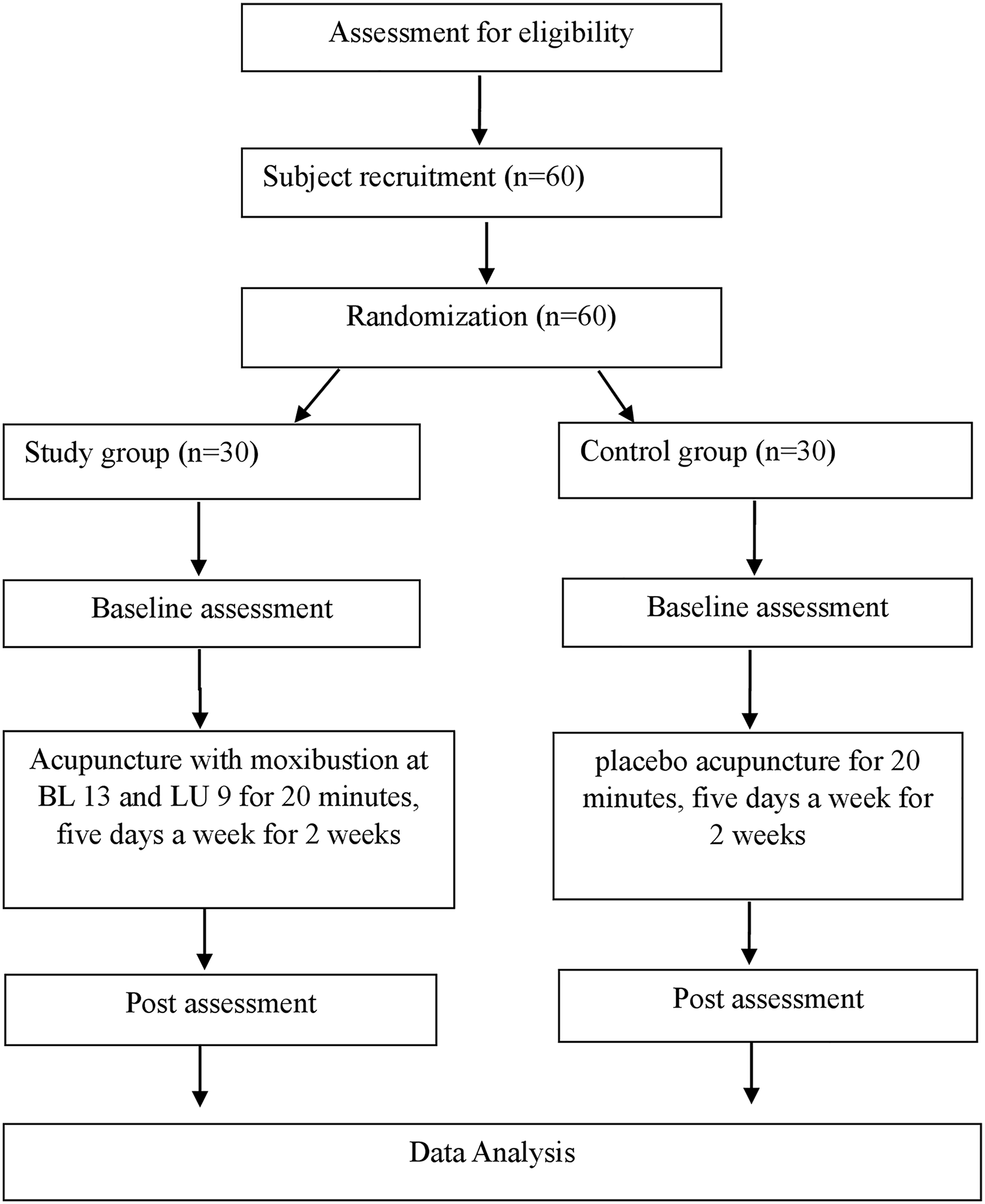
Trial Profile. This figure displays the flow of participants through the study, including screening, randomization into intervention and control groups, the number of sessions received, and assessment points. It outlines the structure and stages of the clinical trial.
METHODS
Study Setting
It is a single-centered study, which will be conducted at Government Yoga and Naturopathy Medical College and Hospital (GYNMCH), Chennai-600106. The eligible bronchial asthma patients will be selected using a convenient sampling method from the above-mentioned institution. All the assessments will be carried out in the research department.
Participants
The participants will be recruited from the GYNMCH, Chennai, based on the following eligibility criteria:
Inclusion criteria
(1) Age between 18 and 50 years.
(2) Both males and females.
(3) Participants with a known history of asthma under conventional medications or diagnosed under the guidelines of the Global Initiative for Asthma. 17
(4) Accept to undertake all the procedures by signing the written consent form.
Exclusion criteria
(1) Habits of tobacco chewing, smoking, and alcoholism.
(2) Women who are known to be pregnant and menstruating.
(3) Acupuncture contraindications include open or infected skin and hemorrhagic diseases (including thrombocytopenic purpura and hemophilia).
(4) Participants with systemic illness and other respiratory diseases.
(5) Participants with an acute exacerbation of asthma in the past 1 month.
(6) Participation in other clinical trials.
Intervention
All participants will receive either real acupuncture or sham acupuncture for 5 days a week for 2 weeks. The intervention will be provided for 20 min in the sitting position by a trained acupuncture physician who has a master’s degree in a relevant field and with significant clinical experience in a controlled environment free from noise, with lighting adjusted to create a calming atmosphere. The acupuncture points will be selected based on TCM (given lung-related special points). The details of the intervention for the acupuncture group and the sham-acupuncture group have been given below.
Acupuncture group
Acupuncture needling will be given at BL 13 (1.5 cun lateral to the spinous process of the 3rd thoracic vertebra, and LU 9 (in the crease of the wrist, just lateral to the radial artery) bilaterally. Filiform copper needles (TX-PinPai Acupuncture Needle Acupuncture for Single Use, manufactured by Suzhou Tianxie Acupuncture Instruments Co., Ltd, China) of size 0.25* 25 mm will be inserted into the points with a depth of 0.5 cun, penetrated obliquely at BL 13 and vertically at LU 9. Moxibustion will be given to each point in close proximity to the neck of the needle till the patient feels the sensation of warmth. The needle will be retained for 20 min (5 min of moxibustion to each point). No electrical or manual stimulation will be given. The treatment will be provided for 5 days a week for 2 weeks.
Control group
The control group subjects will receive acupuncture with moxibustion on non-acupuncture points (superficial insertion at 1 cun lateral to BL 13 and 1.5 cun lateral to LU 9). The same procedure will be followed as that of the acupuncture group (Fig. 2).
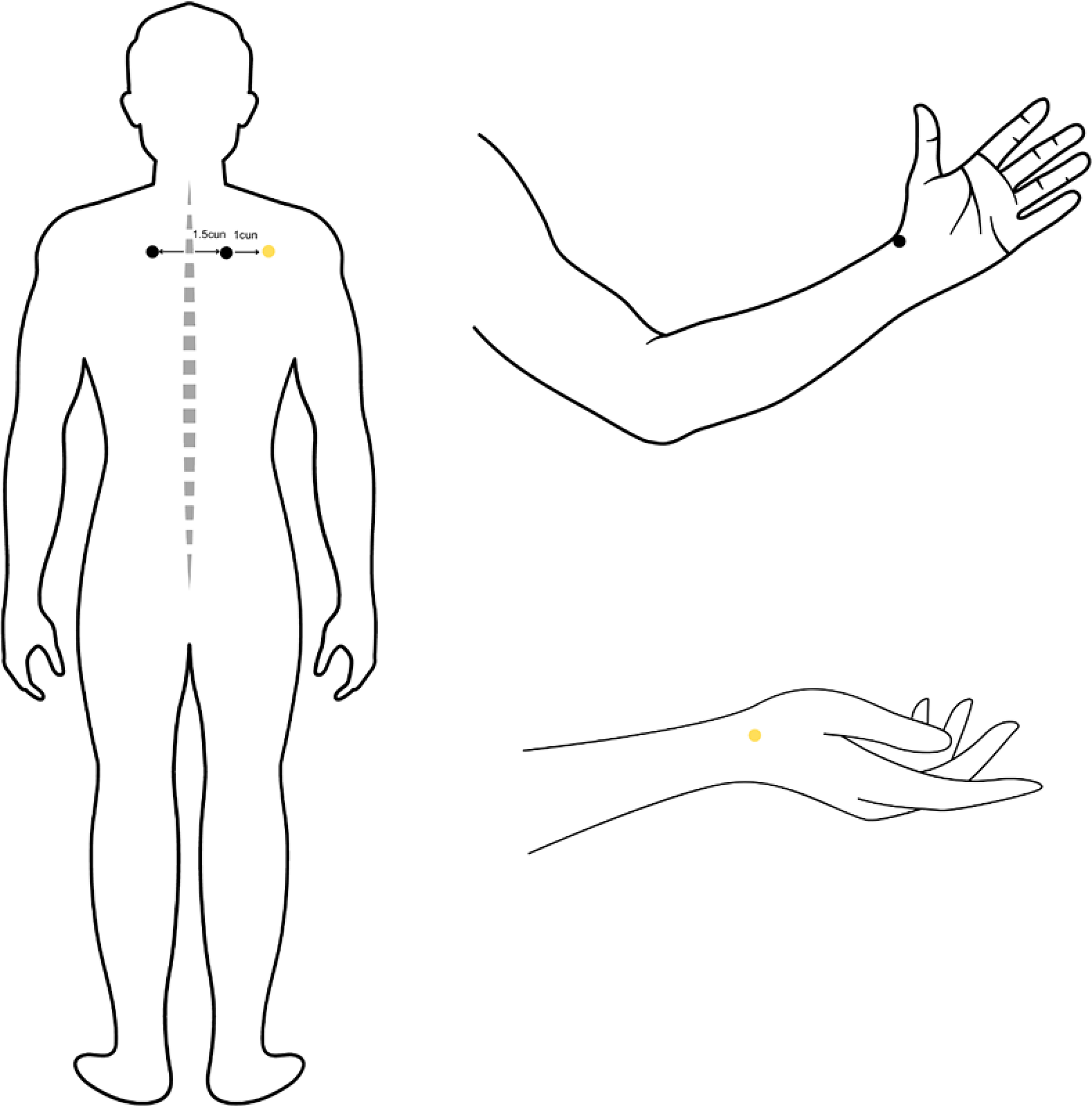
Location of acupuncture and non-acupuncture points. This figure illustrates the anatomical positions of the acupuncture points and non-acupuncture points used in the intervention group. Black points indicate the BL13 (located 1.5 cun lateral to the lower border of the spinous process of the T3 vertebra), and LU9 (located at the wrist crease, lateral to the radial artery). Yellow points indicate non-acupuncture point UB 13 (located 1 cun lateral to UB 13), and non-acupuncture point LU 9 (located 1.5 cun lateral to LU 9).
Criteria for Discontinuing or Modifying Allocated Interventions
Participants are free to withdraw from the study at any point of time, for any reason, with or without prior intimation to investigators. Participants can also discontinue if there are any inconveniences or severe adverse events (feeling of discomfort, nausea, redness or any other skin changes, muscle twitching, or heightened nerve sensation in the area) reported in the study group and also in the control group.
Strategies to Improve Adherence to Interventions
Participants will be contacted by the investigators periodically to attend the OPD on a daily basis for 10 days. The participants will be given access to contact the investigator throughout the study period to clarify doubts. Primary outcome data will be collected from patients who discontinue or deviate from the intervention protocol if consent is granted.
Relevant Concomitant Care Permitted or Prohibited during the Trial
Concomitant care, along with routine activity, will be provided to both groups. All participants will be restricted from participating in other clinical studies.
Outcomes
Primary outcome measure
Pulmonary function tests (PFT) will be performed using spirometry (RMS Helios 401, India). Calibration will be done before each testing session. Spirometry test will be performed in a sitting position with their nose closed by nose clips. A minimum of three trials will be performed, and the average of the three is used for the analysis. The spirometry parameters measured are: forced vital capacity (FVC), forced expired volume in 1 s (FEV1), FEV1 to FVC ratio (FEV1/FVC), peak expiratory flow rate, during the middle half of FVC (FEF 25–75%).
Secondary outcome measure
Quality of life will be measured using the AQLQ (32-item scale), a disease-specific health-related quality of life instrument that focuses on both the physical and emotional impact of the disease.
Participant Timeline
The participant timeline is shown in Figure 3 for your information.
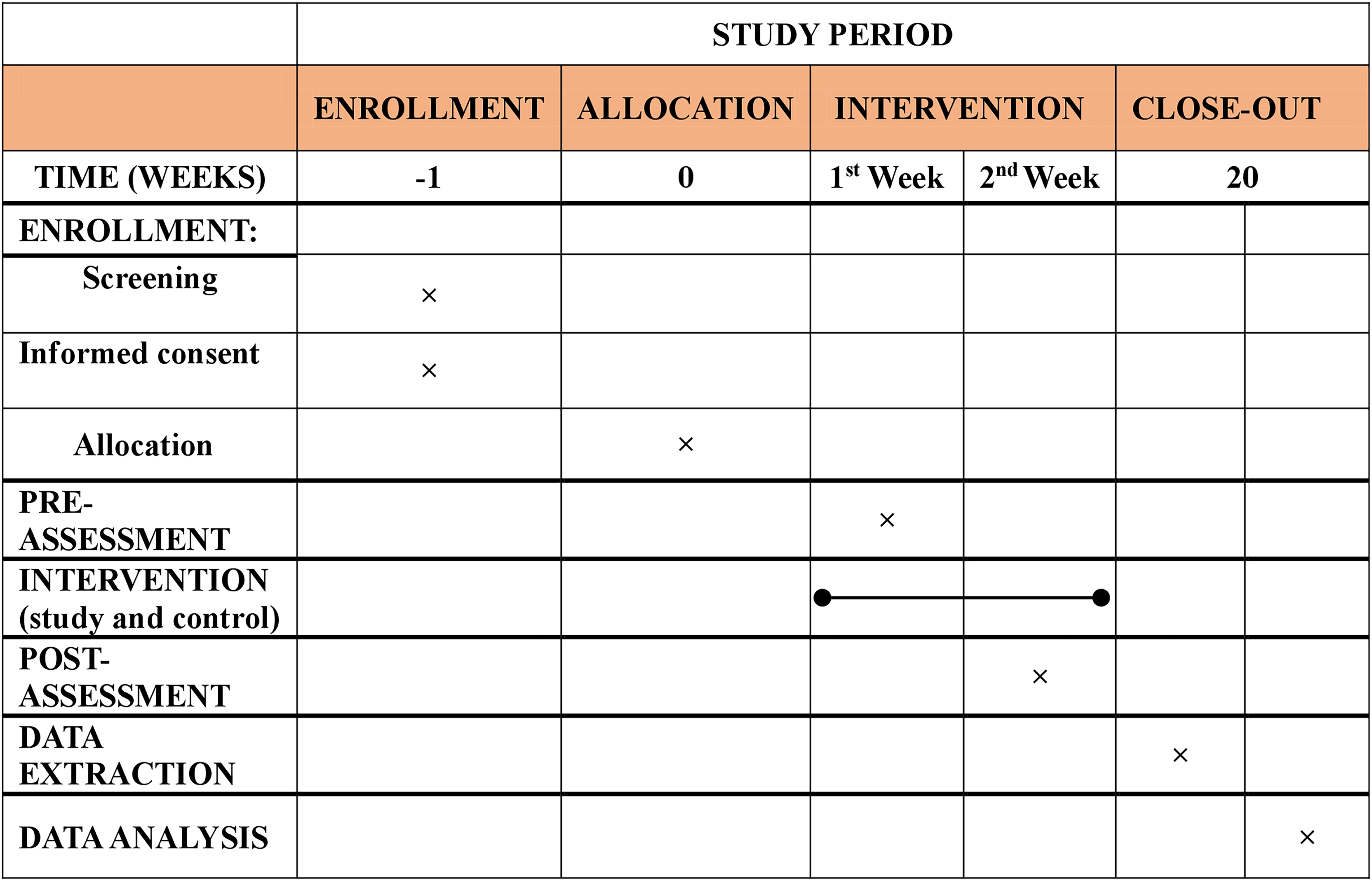
Participant timeline. This figure presents the timeline of study events from enrolment, baseline assessment, intervention for 2 weeks (5 days/week), to post-treatment assessment and data analysis. It is a visual map of the participant’s procedure throughout the entire trial course.
Sample Size
Sixty eligible participants will be recruited from the GYNMCH by using a convenient sampling technique.
Randomization and Blinding
Eligible participants will be randomly divided (1:1 ratio) into two groups: study group (n = 30) and control group (n = 30) using simple random methods with the use of computerized randomization. Randomization will be done by a research consultant who will not participate either in the data collection or statistical analysis of the trial.
Allocation Concealment Mechanism
Sealed envelopes will be prepared in advance, indicating each participant’s allocation based on their recruitment number. During the recruitment process, these envelopes will be handed to the researcher responsible for enrolling participants. Participants who meet the inclusion and exclusion criteria and provide informed consent will be assigned a unique recruitment number in chronological order. The corresponding sealed envelope for that recruitment number will then be opened, and based on its contents, participants will either begin the intervention or be assigned to the control group. A member of the study, who is not involved in participant recruitment, will generate the allocation sequence for assigning participants according to generated random numbers.
BLINDING
All the participants will be blinded in this study.
Data Collection
Data collection will be performed after getting approval from the IEC and after registration of the Clinical Trials Registry—India (CTRI). The study protocol will be explained to the subjects, and a signed consent will be obtained from each subject. PFT will be measured using spirometry (RMS Helios 401, India) before and after the intervention.
Data Management
All the data will be entered in Microsoft Excel 2011 and kept confidentially under the custody of the research department.
Statistical Analysis
Data will be entered in Microsoft Excel, 2011 and analysis will be done using Statistical Package for the Social Science Software (SPSS), Version 16.0. Kolmogorov–Smirnov test will be done to check the normal distribution of the data. Based on the data distribution, within-group analysis will be done using a paired-samples t-test or Wilcoxon signed rank test, and between-group analysis will be done using an independent samples t-test or Mann–Whitney U test. For data pertaining to dropouts, the last observation carried forward will be used for statistical analysis. A p-value <0.05 will be considered significant.
Data Monitoring
Data monitoring in the proposed study will be carried out by the primary investigator, and the quality control of the entire project will be monitored by the Head of the Department and research guide to identify problems in the project implementation process in a timely manner and to implement the corresponding countermeasures. The researchers will be handling the control bias by examining and supervising the acquired data.
DISCUSSION
The present study investigates the effect of acupuncture with moxibustion at BL 13 and LU 9 on pulmonary function in patients with bronchial asthma. The results could have significant implications for the management of asthma. According to traditional Chinese medicine, Lung Qi moves downward, and the kidneys hold it down. The lungs control inhalation and the kidneys control exhalation. Liver Qi usually ascends, which coordinates with the downward direction of Lung Qi. Asthma occurs when the descending of Lung Qi is defective, due to Lung Qi deficiency or kidney deficiency (failure to receive the descending Lung Qi), or obstructed by the ascending excessive Liver Qi (liver Yang rising) or obstructed by phlegm (spleen deficiency) or wind. 18 LU 9 is a source point for the lung, which is used to tonify the lung qi in case of deficiency of the lung and BL 13 is a back shu point of the lung, which affects the organs directly by transporting Qi to the relevant organ. It also stimulates the diffusing and descending of Lung-Qi. 19 Acupuncture suppresses airway hyperresponsiveness and inhibits the elevation of total leukocytes, neutrophils, lymphocytes, and eosinophils. It would regulate the immune system and restore the equilibrium between Th1 and Th2 activity by reducing the production of Th2-specific cytokines, such as interleukin (IL)-4, IL-5, and IL-13, reducing the levels of pro-inflammatory cytokines and IgE. 20 This study has a few limitations that including a limited sample size and a single-blind design, where only participants are blinded, which may reduce the statistical power and generalizability of the findings. In addition, it is a single-center trial, limiting its external validity. The short duration of the intervention (2 weeks) and lack of long-term follow-up restrict the ability to assess sustained effects. Placebo acupuncture may still induce mild physiological effects, potentially minimizing the observed difference between groups, and inflammatory or immunological biomarkers are not measured to understand the actual mechanism of the intervention on lung function. Therefore, future studies should consider larger, multicenter trials with long-term follow-up, a more rigorous blinding, along with measurement of inflammatory markers to substantiate the evidence.
Harms
According to recent investigations, significant adverse reactions connected to needles were uncommon among practitioners of acupuncture and were linked to adverse occurrences. In rare instances, there are still mild side effects following acupuncture; these include syncope (fainting or feeling ill), exhaustion, light-headedness or blurred vision, pain and bruises, sleepiness, and bleeding. Regardless of how they relate to the research intervention, any unexpected symptoms or indications that arise throughout the course of treatment must be reported. These can be successfully treated with targeted care in the GYNMCH’s outpatient department.
Auditing
Auditing will be done in a timely manner.
Ethics and Dissemination
The study protocol was approved by the Institutional Ethics Committee (IEC) (RES/IEC-GYNMC/2023/160) of GYNMCH, Chennai. The study protocol will be explained to the subjects, and a signed consent will be obtained from each subject.
Protocol Amendments
In case of any changes, it will be informed to the department and IEC.
Confidentiality
GYNMCH will protect the confidentiality of your records to the extent provided by law. You understand that the study sponsor and the institution have the right to review your records.
ACCESS TO DATA
The data will be available in the department, and it can be accessed by request with a valid reason.
DISSEMINATION POLICY
The results of the study will be disseminated through conference presentations and publications in peer-reviewed indexed journals.
PROTOCOL AVAILABILITY
The protocol is freely available at CTRI for the public.
AUTHORS’ CONTRIBUTIONS
Idea and conceptualization: V.S. Review and editing: M.A. Supervision and monitoring: M.N.
Footnotes
AUTHOR DISCLOSURE STATEMENT
No competing financial interests exist.
FUNDING INFORMATION
No funding was received for this article.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.