
Abstract
Background:
Currently, there is no effective treatment for vascular cognitive impairment (VCI), a range of cognitive disorders that occur locally or globally, solely resulting from vascular issues in the brain. The aim of this review is to summarize the potential mechanisms involved in acupuncture treatment for VCI.
Methods:
PubMed and Google Scholar were searched for randomized controlled trials and systematic reviews/meta-analyses from the date of their inception to December 2024.
Results:
Out of 2,331 studies screened, 6 studies met the inclusion criteria. These studies suggest that acupuncture may have a positive impact on improving symptoms of VCI. The proposed mechanisms include enhancement of neuroplasticity, increased release of acetylcholine and neurotrophic factors, and inhibition of post-ischemic inflammatory responses and oxidative stress in cerebral regions, which may collectively contribute to improved cognitive function.
Conclusion:
Overall, our findings provide a basis for future research into the effects of acupuncture on VCI.
INTRODUCTION
Vascular cognitive impairment (VCI) refers to the entire spectrum of cognitive disorders that manifest locally or globally, solely caused by brain vascular disturbances. This condition includes mild cognitive impairment (MCI) to the most severe form, which is dementia.1,2 All systemic disease risk factors that can cause issues with brain vascularization are associated with increased occurrence of VCI. 3 The prevalence of VCI increases with age.
According to the report from the Vascular Impairment of Cognition Classification Consensus Study, VCI is divided into vascular mild cognitive impairment (VMCI) and major VCI (vascular dementia). 4 In 2018, it is estimated that 50 million people, worldwide, were living with dementia. The prevalence of dementia in developing countries, after the age of 65, is estimated to be 5–8% (though underreported) and 7–10% in developed countries. Vascular dementia accounts for 17–30% of all dementia cases, second only to Alzheimer’s dementia (AD). Prevalence of vascular dementia for age >65 is 1.5–4.5%. The incidence is approximately 0.1/1,000 for ages 60–64 and rising to 7/1,000 for ages >90, with males having a higher risk. VMCI is more prevalent than vascular dementia among individuals 65–84 years of age. Approximately 25% of stroke survivors develop new-onset dementia within 1 year post cerebrovascular accident (CVA). The prevalence of VMCI is 44–74% within 6 months of CVA, worsening quality of life. Due to the anticipated increase in world population and the rising prevalence of dementia, it is estimated that the number of individuals with dementia will triple by the year 2050, resulting in annual medical costs of approximately 4 trillion USD.2,4–10
To determine the classification of VCI, clinical data are required, including the use of cognitive screening instruments and brain imaging for cerebrovascular abnormalities. 4 To diagnose major VCI, the dementia diagnostic criteria in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders can be used. In addition, evidence is needed to determine the presence of comorbid non-vascular dementia causes, such as AD and Lewy body dementia (LBD). If cerebrovascular abnormalities are present along with diagnostic evidence of AD or LBD, the resulting dementia is classified as a mixed type. 11
The process of VCI onset begins with the damage to nerve function in areas such as the hippocampus, prefrontal cortex-basal ganglia network, and possibly the periventricular white matter. The hippocampus in mammals is one of the most vulnerable organs to hypoxia due to its high activity, requiring substantial energy. Like AD and other memory disorders, the core issue in vascular dementia is the impairment of the ability to form synapses and/or communicate through synaptic connections in the hippocampus and cortex, which are essential for cognitive function. 12 Local tissue damage caused by ischemic infarction can lead to neurodegenerative changes in small areas of the brain. Secondary neurodegeneration that occurs after subcortical ischemic infarction is mediated by the degeneration of nerve tissue connecting the initial vascular injury site to the substantia nigra, resulting in focal or widespread loss of white matter along with cortical thinning. The underlying mechanisms of secondary substantia nigra loss are not well understood, but they may involve transsynaptic effects and inflammatory responses. Brain atrophy is one of the strongest predictors of cognitive impairment in patients with pure vascular disease, and growing evidence suggests that the effects of subcortical ischemic lesions on cognitive function are mediated by the loss of cortical substantia nigra.2,12
Vascular risk factors play a role in the development of VCI. These risk factors include non-modifiable factors (age, sex, race, and genetics) and modifiable factors (hypertension, diabetes mellitus, obesity, and dyslipidemia). In managing VCI risk factors, controlling the modifiable factors is one of the preventive measures that can be undertaken.13,14 To date, there is no specific pharmacological treatment recommended by the U.S. Food and Drug Administration for the management of vascular dementia symptoms. Therapies used for AD have not been clinically proven to significantly improve vascular dementia. Pharmacological therapies targeting underlying conditions, such as hypertension, dyslipidemia, and/or diabetes mellitus, are expected to help prevent the worsening of vascular dementia.
10
Currently used pharmacological therapies for VCI, such as cholinesterase inhibitors and N-methyl-
Acupuncture therapy can be considered a non-pharmacological treatment option for managing VCI, given that existing conventional treatments have not shown satisfactory results and are accompanied by the side effects of pharmacological therapies. Acupuncture can play a role in controlling modifiable risk factors for VCI, as well as serving as a therapy after VCI has occurred. A meta-analysis has shown that acupuncture therapy, whether as a stand-alone treatment or in combination with conventional therapy, can improve cognitive function and daily activities in patients with VCI, with minimal side effects. 15 Acupuncture therapy can influence the process of VCI through several aspects, such as protecting cerebral neurons from oxidative stress, apoptosis, and neural inflammation; regulating glucose metabolism; and modifying neurotransmitters.16–21
METHODS
A comprehensive literature search was conducted using PubMed and Google Scholar from the date of their inception until December 2024. The search aimed to identify randomized controlled trials (RCTs) and systematic reviews/meta-analyses that investigated the effects of acupuncture on VCI, vascular dementia, or VMCI. The search was restricted to studies published in English and limited to those involving human participants. Eligible studies were required to employ acupuncture as a therapeutic intervention, which included various modalities such as body acupuncture, ear acupuncture, electroacupuncture, laser acupuncture, and scalp acupuncture. Key search terms included acupuncture, ear acupuncture, electroacupuncture, laser acupuncture, scalp acupuncture, VCI, vascular dementia, and VMCI.
During the screening process, several exclusion criteria were applied. Studies were excluded if they were non-English publications, involved non-human subjects, or did not employ an evidence-based clinical design. In addition, non-clinical publications such as narrative reviews, editorials, commentaries, conference abstracts without full texts, and protocol-only articles were not considered. Studies that did not specifically address VCI or related diagnoses were also excluded. Furthermore, duplicate studies or those presenting overlapping data from the same population without providing additional or distinct findings were removed from the final selection. Figure 1 shows the search strategy scheme.
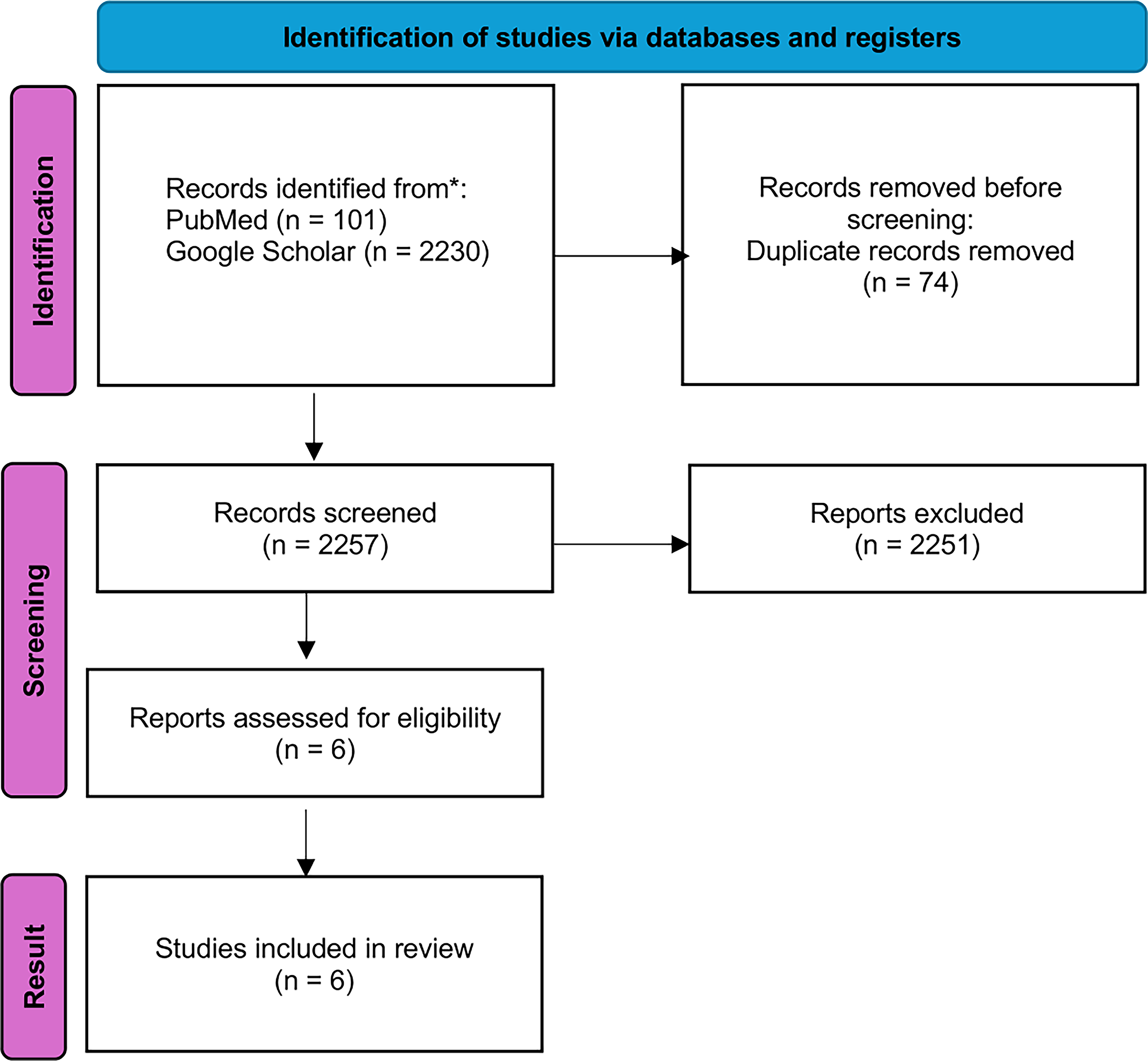
Search strategy scheme.
RESULTS
The literature search described in the section “Methods” yielded 2,331 studies in the initial search. After screening, six studies met the inclusion criteria for this narrative review. Table 1 provides details on the six included studies.
Summary of the Six Included Studies
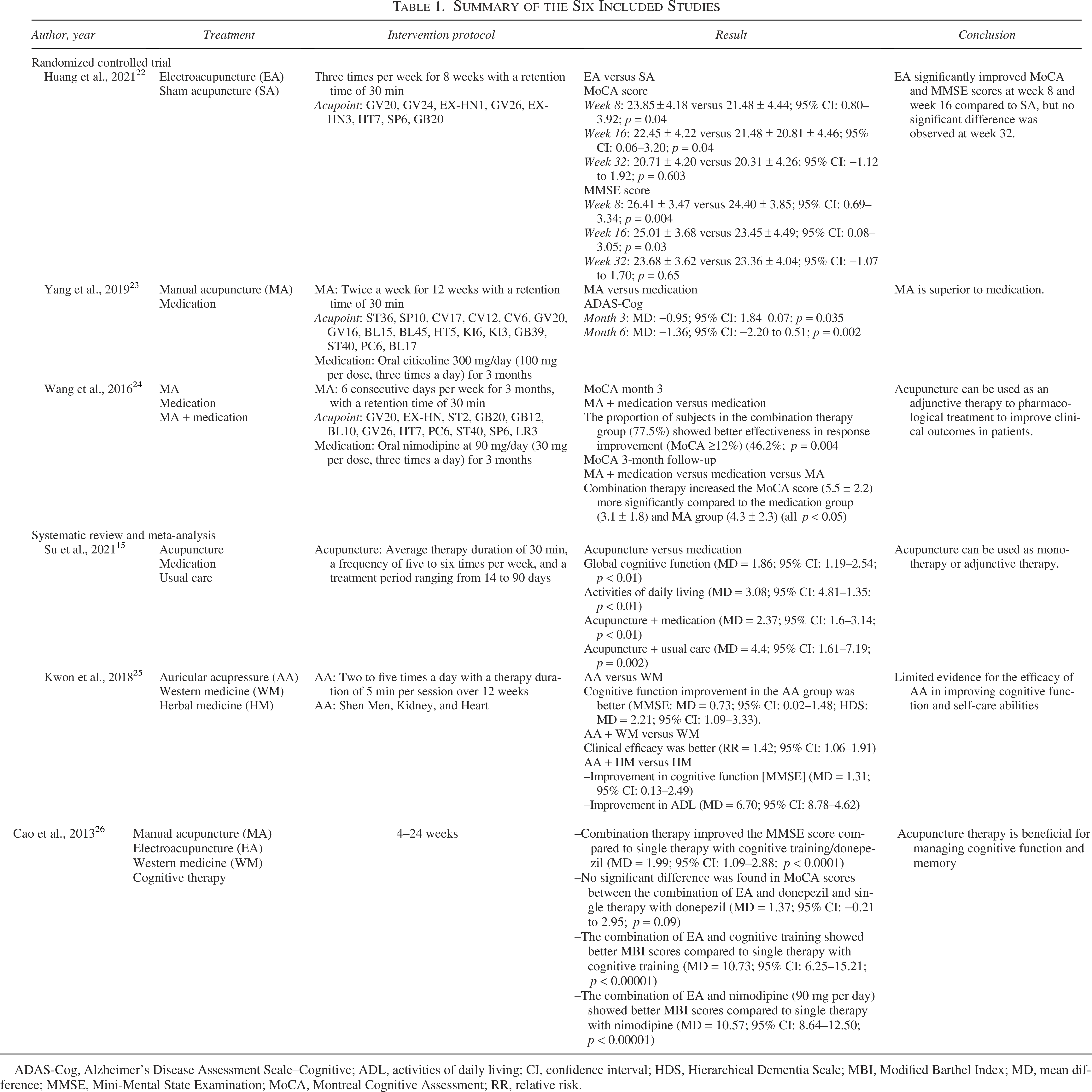
ADAS-Cog, Alzheimer’s Disease Assessment Scale–Cognitive; ADL, activities of daily living; CI, confidence interval; HDS, Hierarchical Dementia Scale; MBI, Modified Barthel Index; MD, mean difference; MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment; RR, relative risk.
DISCUSSION
The exact neuropathology of VCI remains unclear due to the various factors that may contribute to it. Key factors in VCI seem to include microinfarcts, microvascular alterations linked to blood–brain barrier disruption, focal neuronal atrophy, and neurodegenerative processes.4,27–29
Huang et al. (2021) conducted an RCT involving 120 subjects with vascular cognitive impairment without dementia (VCIND), aged between 40 and 80 years. The subjects were divided into two groups: the intervention group, which used electroacupuncture (EA) at a frequency of 2.5 Hz and an intensity of 2–3 mA depending on the subject’s comfort, and the control group, which used sham acupuncture (SA) with Streitberger needles. The acupuncture points used in this study were GV20, GV24, EX-HN1, GV26, EX-HN3, HT7, SP6, and GB20. Acupuncture therapy was administered three times per week for 8 weeks with a retention time of 30 min. The primary outcome of this study was the Montreal Cognitive Assessment (MoCA), measured at weeks 0, 8, 16, and 32, while the secondary outcome was the Mini-Mental State Examination (MMSE), measured at the same time points as the primary outcome. The EA group showed superior results in the MoCA and MMSE assessments compared to the SA group up to the evaluation at week 16, but there was no significant difference noted between the two groups at week 32. 22
The RCT research with a VCIND population was also conducted by Yang et al. in 2019 on 216 subjects aged 55–85 years. The subjects were divided into two groups: the intervention group, which received manual acupuncture (MA), and the control group, which received oral citicoline at 300 mg/day (100 mg per dose, three times a day) for 3 months. The acupuncture points used in this study were ST36, SP10, CV17, CV12, CV6, GV20, GV16, BL15, BL45, HT5, KI6, KI3, GB39, ST40, PC6, and BL17. Acupuncture therapy was performed twice a week for 12 weeks with a retention time of 30 min. Assessment using the Alzheimer’s Disease Assessment Scale–Cognitive subscale (ADAS-Cog) at 3 months and follow-up at 6 months showed that acupuncture therapy has comparable efficacy and even superior effects in improving cognitive function and daily living activities. 23
In 2016, Wang et al. conducted an RCT involving 126 subjects with MCI following a cerebral infarction, aged 50–80 years. The subjects received treatment for 3 months and were divided into three groups: a group receiving MA, a group receiving oral nimodipine at 90 mg/day (30 mg per dose, three times a day), and a group receiving both MA and nimodipine. The acupuncture points used in this study were GV20, EX-HN1, ST2, GB20, GB12, BL10, GV26, HT7, PC6, ST40, SP6, and LR3. Acupuncture therapy was performed 6 consecutive days per week for 3 months, with a retention time of 30 min. The results of the study showed that the combination therapy of acupuncture and nimodipine increased the MoCA scores at the end of the therapy at 3 months and at the 3-month follow-up compared to the other groups. 24
Su et al. (2021) conducted a systematic review and meta-analysis (SR-MA) of 48 RCTs involving 3,778 VCI subjects to assess the effects of acupuncture on VCI, either as a stand-alone intervention or in combination with conventional therapy. The primary outcomes of this SR-MA focused on global cognitive function assessment using MoCA, MMSE, ADAS-Cog, and Hasegawa’s Dementia Scale. The acupuncture methods used included MA and EA, with an average therapy duration of 30 min, a frequency of —five to six times per week, and a treatment period ranging from 14 to 90 days, with 95% of the studies in this SR-MA lasting at least 4 weeks. The data collected indicated that acupuncture was more beneficial for global cognitive function (mean difference [MD] = 1.86; 95% confidence interval [CI]: 1.19–2.54; p < 0.01) and activities of daily living (ADL; MD = 3.08; 95% CI: 4.81–1.35; p < 0.01) compared to Western medicine (WM). Favorable outcomes were also observed when acupuncture was combined with WM (MD = 2.37; 95% CI: 1.6–3.14; p < 0.01) or usual care (UC) (MD = 4.4; 95% CI: 1.61–7.19; p = 0.002) compared to the control group. Meanwhile, the subgroup analysis did not show any statistically significant differences between MA and EA. 15
In 2018, Kwon et al. conducted an SR-MA of 9 RCTs involving 677 subjects to examine the effects of auricular acupuncture (AA) on cognitive dysfunction. The primary outcomes of this SR-MA focused on global cognitive function assessment using MoCA, MMSE, ADAS-Cog, Hierarchical Dementia Scale (HDS), Global Deterioration Scale, and Clinical Dementia Rating. The secondary outcome of this study was the ability to perform ADL. The most commonly used AA points in this study were AA point Shen Men, AA point Kidney, and AA point Heart. The acupuncture method used was self-acupressure, performed two to five times a day with a therapy duration of 5 min per session over 12 weeks. Vaccaria seeds were used as the acupressure material in seven of the studies included in this SR-MA. The conclusion of this SR-MA indicates that the evidence on the AA in patients with cognitive impairment and/or dementia is mixed and inconclusive. Although some studies suggest potential benefits in improving cognitive function and self-care abilities, the overall findings are limited by the small number of studies and poor methodological quality of the included studies. 25
Cao et al. (2013) conducted an SR-MA of 12 RCTs involving 691 subjects to examine the effects of acupuncture therapy on VMCI. The primary outcomes of this SR-MA focused on global cognitive function assessment, which must include at least one internationally recognized scale such as MMSE, MoCA, Modified Barthel Index (MBI), Wechsler Memory Scale, or similar. The results of the study showed that the combination therapy of acupuncture with cognitive function exercises/donepezil (0.25 mg per day) improved MMSE scores compared to the single therapy of cognitive function exercises/donepezil (MD = 1.99; 95% CI: 1.09–2.88; p < 0.0001). The combination of EA and cognitive function exercises showed better MBI scores compared to the single therapy of cognitive function exercises (MD = 10.73; 95% CI: 6.25–15.21; p < 0.00001). The combination of EA and nimodipine (90 mg per day) showed better MBI scores compared to the single therapy of nimodipine (MD = 10.57; 95% CI: 8.64–12.50; p < 0.00001). The conclusion of this study is that acupuncture therapy is beneficial for managing cognitive function and memory in patients with VMCI. 26
Recent neurophysiological studies have provided insight into the potential mechanisms by which acupuncture may exert therapeutic effects on VCI, particularly through its modulation of brain activity. As an external stimulation modality, acupuncture has been shown to influence central nervous system (CNS) functions, with electroencephalography (EEG)-based monitoring systems revealing measurable changes in brain dynamics during acupuncture intervention. Specifically, acupuncture enhances power spectral density in the alpha (8–12 Hz) and delta bands, particularly in parietal, occipital, and central-frontal regions. These changes are accompanied by a decrease in the aperiodic exponent of the EEG power spectrum, suggesting a reduction in background neural noise and greater cortical excitation efficiency. In addition, EEG studies demonstrate that acupuncture increases phase synchronization in the delta and alpha bands and enhances long-range connectivity between hemispheres, as reflected in changes in graph theory metrics. Functional brain networks during and after acupuncture exhibit small-world network properties with improved efficiency, indicating enhanced functional integration and communication across brain regions. These findings suggest that acupuncture may improve cognitive function in VCI by promoting neuroplasticity, optimizing functional connectivity, and modulating both oscillatory and non-oscillatory neural activity.30,31 Functional magnetic resonance imaging (fMRI) studies have demonstrated that acupuncture exerts modulatory effects on multiple brain regions implicated in cognitive processes, offering potential benefits for individuals with VCI. Acupuncture has been shown to activate brain areas associated with cognition, perception, and sensory integration. For example, resting-state and task-based fMRI revealed that acupuncture at KI3 in elderly individuals with MCI activated over 20 cerebral regions, including the bilateral anterior cingulate gyrus (BA 32, 24), medial and superior frontal gyri (BA 9, 10, 11), cuneus (BA 18, 19), lingual gyrus (BA 18), inferior frontal gyrus (BA 47), and superior temporal gyrus (BA 38). These regions are involved in attention, memory processing, and executive function, which are often impaired in VCI. In addition, comparisons between real acupuncture and SA show significant alterations in both amplitude of low-frequency fluctuation (ALFF) and regional homogeneity (ReHo) values. Acupuncture led to increased ALFF in areas such as BA10, BA39, and the cerebellum posterior lobe and increased ReHo in BA10, BA37, and the cerebellum pyramis. Conversely, decreased ALFF and ReHo were observed in visual and association cortices like BA18, BA19, and BA31, suggesting selective modulation of sensory and associative processing. Notably, these brain regions also overlap with areas commonly affected in VCI, including the temporal and prefrontal lobes—key hubs for cognitive control and memory encoding. Taken together, fMRI evidence suggests that acupuncture may facilitate cognitive improvement in VCI by enhancing activity in neural circuits responsible for attention, memory, and executive functioning.32–34
Several preclinical studies using animal models of VCI have explored the underlying neurobiological mechanisms through which acupuncture may exert its therapeutic effects. In a study with rats having cognitive impairment, acupuncture stimulation at the GV20 point significantly improved the rats’ memory and restored the expression of messenger RNA (mRNA) molecules involved in memory function in the hippocampus, such as cAMP-response element-binding protein (CREB). 24 The increase in CREB and phosphorylated CREB expression may enhance memory function in vascular dementia.35,36 Research with EA demonstrated therapeutic effects in reducing cerebral ischemia–reperfusion injury and providing neuroprotection by disrupting the expression of several apoptosis-related genes, such as c-fos, heat shock protein 70 (HSP70), and even neurotrophin family (NT) genes. Acupuncture therapy can have beneficial effects on the CNS by increasing the mRNA expression levels of brain-derived neurotrophic factor (BDNF) in the hippocampus of rats following cerebral ischemia–reperfusion injury, which protects neurons from damage and inhibits hippocampal cell apoptosis. Acupuncture can enhance BDNF expression through the PI3K/Akt (phosphatidylinositol-4,5-bisphosphate 3-kinase) and MEK/ERK1/2 (extracellular signal-regulated kinases) signaling pathways by activating tropomyosin receptor kinase B (TrkB), a high-affinity catalytic receptor for several neurotrophins that induce the activation of survival signaling pathways. 37 In a rat model of vascular dementia, AA was shown to increase the expression of bcl-2 in brain tissue, suggesting that AA may have neuroprotective effects by modulating the apoptosis process. Short-term AA therapy has been proven to enhance antioxidant capacity in individuals at high risk for diabetes, potentially reducing the risk of dementia through indirect neuroprotective effects by controlling antioxidant capacity in the body. AA can also directly influence the expression of beta-amyloid proteins. In a rat model of vascular dementia, AA significantly improved learning and memory capacity through mechanisms that inhibit the excessive production of beta-amyloid protein in the hippocampal area. In addition, AA has a mechanism of action that can prevent or repair cognitive impairment and/or dementia either directly or indirectly through the “ear-vagus nerve reflex.” EA stimulation at the auricular branch of the vagus nerve can improve ADAS-Cog and MMSE scores in AD patients. Based on these findings, it is suggested that AA may be effective in preventing and treating neurodegenerative diseases through mechanisms that activate the vagal nucleus in the brainstem. 25 Acupuncture stimulation can enhance neuroplasticity, increase the release of acetylcholine and neurotrophic factors, and inhibit postischemic inflammatory reactions and oxidative stress in cerebral regions. 38
CONCLUSIONS
Acupuncture therapy is potentially an effective non-pharmacological treatment for VCI. Commonly used acupuncture points include GV20, GV26, GB20, EX-HN1, PC6, and SP6, with a 30-min retention time. Treatment is given—five to six times per week for 4–9 weeks. Acupuncture is effective, safe, and has minimal side effects when used as primary or adjunctive therapy for VCI.
AUTHORS’ CONTRIBUTIONS
D.R. and A.S. conceived the study and designed the methodology, collected, and analyzed the data. D.R. drafted the manuscript. Both authors reviewed and approved the final version of the manuscript.