
Abstract
Background:
The experience of childbirth is accompanied by a mix of excitement and apprehension, due to concerns about pain management and the health of the newborn. The aim of this study is to evaluate the effects of prenatal acupuncture on childbirth preparation, focusing on maternal childbirth outcomes, among multigravida women in Indonesia.
Methods:
Using consecutive sampling, 34 multigravida women aged 25–40 years and at least 36 weeks’ gestation were recruited and allocated to the intervention or control group. The intervention group received manual acupuncture with 0.25 mm × 40 mm stainless steel at ST-36, SP-6, and LI-4 for 20 min. Acupuncture was scheduled once weekly (<38 weeks’ gestation) and twice weekly (>38 weeks’ gestation) until labor. The control group received standard prenatal care. Outcomes assessed included onset of labor, labor pain, duration of the active phase, the second stage of labor, perineal tear, Apgar scores, and colostrum production. Data were analyzed using t-test or Mann–Whitney depending on the distributions.
Results and Discussion:
The average age of participants was 30.88 ± 3.68 years in the intervention group and 33.23 ± 4.20 years in the control group. Significant differences were observed between the two groups, particularly in labor pain (p = 0.000), duration of the active phase (p = 0.000), second stage of labor (p = 0.000), and colostrum production (p = 0.002). There were no significant differences (p ≥ 0.005) in onset of labor, Apgar scores, or perineal outcomes. In the safety outcomes, no adverse events were reported.
Conclusion:
This study suggests that prenatal acupuncture is an effective and safe method for childbirth preparation.
INTRODUCTION
The experience of childbirth can be accompanied by a mix of excitement and apprehension, largely due to concerns about pain and the health of the newborn. 1 Many women have opted for medical interventions such as cesarean sections (CSs) to alleviate fears associated with vaginal birth. However, the increasing rate of CS, which has reached alarming levels in Indonesia, raises serious public health concerns. The 2018 Basic Health Research reported a national CS prevalence of 17.6%, 2 which rose to 25.9% according to the 2023 Indonesia Health Survey. 3 This far exceeds the World Health Organization’s recommendation that CS should constitute no more than 10–15% of all births.4,5 Elevated CS rates are concerning because they are linked to higher maternal and neonatal morbidity and mortality as well as increased health care costs.6–8
To facilitate a safer and more positive childbirth experience, there is a growing interest in complementary therapies that can enhance physiological and psychological preparedness for labor. Among these, acupuncture has gained attention as a nonpharmacological intervention that may offer benefits during the antenatal period and labor. 9 Research suggests that acupuncture has potential in improving outcomes for both mothers and their newborn. 10
Acupuncture may contribute to a smoother labor process by reducing labor pain, shortening the length of labor by enhancing uterine contractions for a more efficient labor, 11 and reducing the need for artificial oxytocin.12–14 Acupuncture is associated with increased maternal satisfaction with pain relief and reduced use of pharmacological analgesia during labor.15,16 Moreover, acupuncture has been suggested as a safe and effective method to support women during the antenatal period, labor preparation, and the birth process. 17 As acupuncture becomes more integrated into maternity care, it has shown minimal adverse effects, accessible and effective complementary method, making it an appealing option for women seeking nonpharmacological support and alternative pain management techniques during pregnancy and childbirth, including in Indonesia.13,15,18–20
The aim of this quasi-experimental study is to evaluate the effects of prenatal acupuncture on childbirth preparation, focusing on maternal childbirth outcomes, including onset of labor, labor pain, duration of active phase, second stage of labor, perineal tear, and colostrum production among multigravida women in Indonesia.
METHODS
Ethical Clearance
The research received approval from the Ethics Board of Kusuma Husada University (Number: 1606/UKH.L.02/EC/VIII/2023) in August 2023, and informed consent was obtained from all patients.
Participants
This quasi-experimental study involved 34 multigravida pregnant women beyond 36 weeks’ gestation who were aged between 25 and 40. Maternal age was categorized as <35 years or ≥35 years based on the Indonesian national guidelines for antenatal care, which define pregnancy at age 35 or above as high risk due to increased likelihood of maternal and perinatal complications.21,22 The following inclusion criteria included the following: single fetus, vertex presentation, and healthy vital signs. Exclusion criteria included the following: preeclampsia, gestational diabetes, thrombocytopenia, cardiovascular disease, and previous CS.
Sampling
This study used a consecutive sampling method. A total of 34 eligible women were assigned to intervention and control groups, based on their willingness to undergo acupuncture. Those who consented received the intervention, whereas those who declined were assigned to the control group.
Participants were informed about prenatal acupuncture treatment and the study. Acupuncture sessions involved needle insertion, two to six sessions: once a week for pregnancies under 38 weeks’ gestation and twice a week from 38 weeks until the onset of labor. The treatment schedule is modified based on research by Betts. 23 No acupuncture was given for pain relief during labor, and no additional birth preparation classes or psychosocial interventions were provided. The rationale for applying prenatal acupuncture in this study is to improve maternal experiences during labor by physiologically promoting pain modulation, uterine readiness, and early postpartum lactation. 24
Intervention and Control Group
The intervention group (n = 17) received prenatal acupuncture treatment with 0.25 mm × 40 mm stainless-steel C-type needles (Huanji, China) at the acupoints Zusanli ST-36, Sanyinjiao SP-6, and Hegu LI-4 for 20 min until the De-qi sensation was reported. Acupuncture sessions were scheduled once a week for those under 38 weeks’ gestation and twice a week for those over 38 weeks’ gestation before the day of labor. Although the exact timing between the last session and the onset of labor was not recorded, it is estimated that participants gave birth within 1–4 days after their last acupuncture session. During the labor, there were no interventions regarding to acupuncture treatment or pharmacological intervention to induce labor. In contrast, the control group (n = 17) continued standard antenatal care without acupuncture at Cawas Islamic Hospital in Klaten and Familia Primary Health Clinic in Karanganyar, along with routine assessments. These assessments included the evaluation of vital signs and general antenatal care.
Intervention Procedures
Acupuncture therapy was administered by licensed acupuncturists using disposable stainless-steel needles measuring 1 and 1.5 cun. The specific acupuncture points targeted included Zusanli ST 36, Sanyinjiao SP6, and Hegu LI4. According to Traditional Chinese Medicine, pregnancy represents a yin-dominant state, and labor initiation requires the transformation of yin into yang to activate qi movement, promote uterine contractions, and support birth progression. 25 Hence, the three acupoints used in this study exerts a strong descending action, generating effective and sustained uterine contractions.25,26 The acupuncture points used are shown in Figure 1.
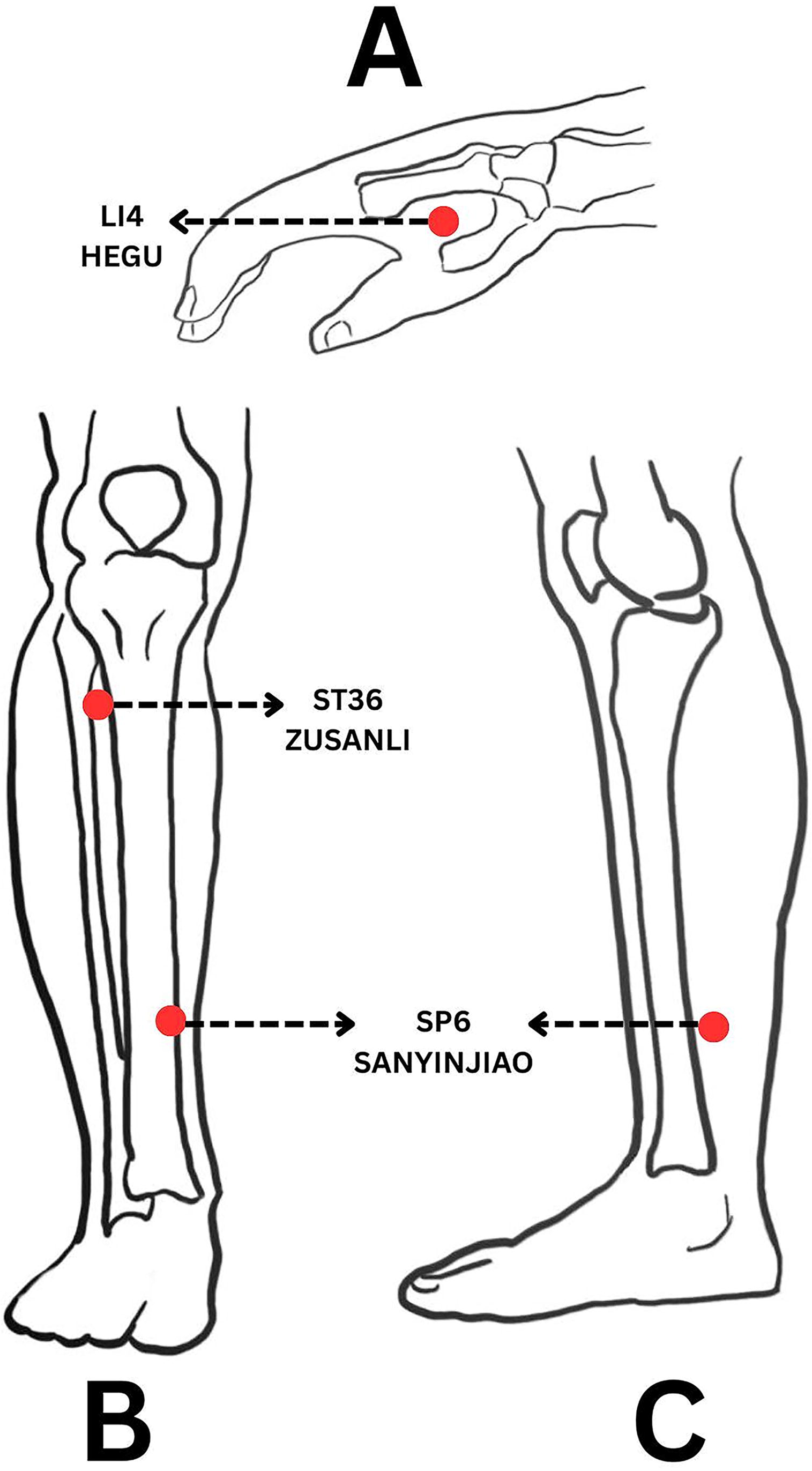
The location of acupuncture points used in this study, which are Hegu LI4
Clinical Assessment and Measurement Tool
Onset of labor
Onset of labor in this study was determined based on documentation in medical records and partographs and was categorized as either spontaneous or induced. Spontaneous labor was defined as the natural initiation of uterine contractions without pharmacological or medical intervention, whereas induced labor referred to the initiation of contractions through artificial techniques or medical agents to stimulate birth.33,34
Labor pain
Labor pain was evaluated using the Visual Analog Scale (VAS), based on mother’s subjective pain assessments during active phase, with a scale of 0–10. Score 0 represents no pain, and 10 represents the worst pain imaginable. Participants were asked to mark the point on the line that represents their current level of pain intensity. Pain assessments were conducted every 1 h during the active phase before second stage of labor. VAS scoring is categorized as mild (0–4), moderate (4–7), and severe (7–10). Patients report their pain using the VAS, which is illustrated in Figure 2.
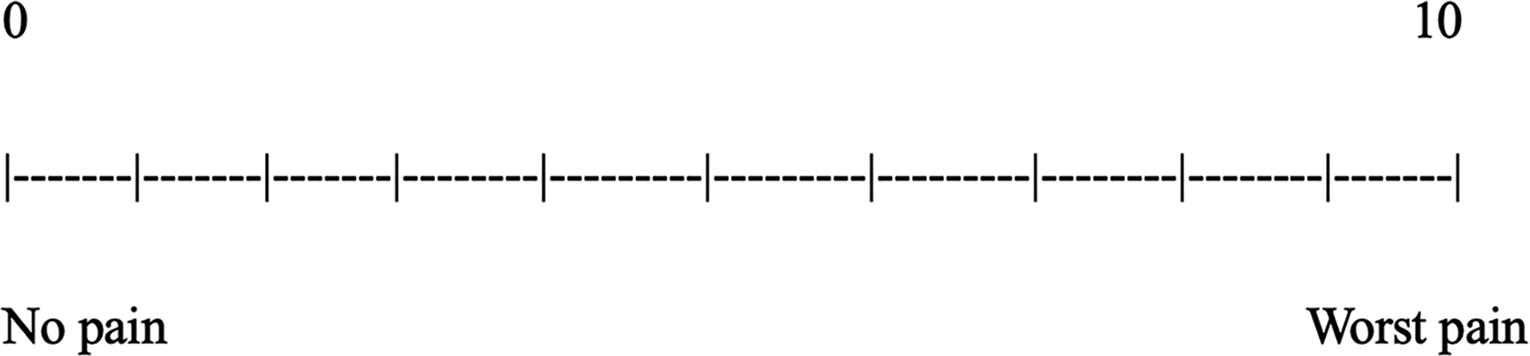
The Visual Analog Scale used in this study, using the number between 0 and 10. Zero score indicates no pain, and 10 represents the worst pain. The higher number (to the right side) means an increase levels of pain.
Duration of active phase
The duration of cervical dilation during labor was measured from ≥4 cm until 10 cm, based on the partograph. The cervical dilation measurements were determined by standard vaginal examination conducted by attending midwives, as part of routine labor monitoring based on standard care. In standard care, vaginal examinations are conducted every 4 h during active labor or as needed based on clinical signs. Examinations are performed under aseptic conditions by midwife, and findings are recorded in the partograph directly in the labor room. During this time, patients remained in the labor room and were allowed to choose their preferred position—lying down, sitting, or walking around the room—as per their comfort.
Second stage of labor
The second stage of labor was assessed from the time of complete cervical dilation until the birth of the baby, as recorded on the partograph.
Perineal tear
The elasticity of the perineum is evaluated based on perineal tears, classified into four degrees. The first degree involves only superficial tears of the vaginal mucosa, whereas second degree extends to vaginal mucosa and perineal muscles. The third degree includes tears to the anal sphincter, and the fourth degree extends further to involve the rectal mucosa.
In this study, we did not specifically assess the rate or indication of episiotomy. According to the national midwifery care guidelines used in Indonesia, routine episiotomy is not recommended for all vaginal births. Episiotomy should only be performed based on clinical indications, such as rigid perineum, fetal distress, or instrumental childbirth, and not as a routine procedure. 35
Apgar score
The Apgar score was used as a standardized clinical tool to assess the immediate postnatal condition of the newborns. It was measured at 1-, 5-, and 10-min following labor and birth by trained midwives who were blinded to the group assignments. The Apgar score comprises five vital physiological functions, including: Appearance, Pulse, Grimace, Activity, and Respiration. Each component is scored from 0 to 2, yielding a total score ranging from 0 to 10. A score of 7–10 is interpreted as normal, whereas scores below 7 indicate neonatal distress and require further observation or intervention. 36 Assessment at 1 and 5 min is standard in clinical practice, while the 10-min score provides additional insight into neonatal adaptation.37,38 In Indonesia, the Apgar score remains a routine part of neonatal evaluation, endorsed in national midwifery guidelines and obstetric protocols. 39
Colostrum production
Colostrum production is assessed through medical records, specifically noting how many minutes elapse before breast milk or colostrum is released after the completion of the fourth stage of labor. This assessment is conducted either before or after the 24-h mark postlabor and birth.
Statistical analysis
The statistical analysis used SPSS for Windows version 22.0 (SPSS Inc., Chicago, IL, USA). The significance level was set at p < 0.05. The data were analyzed using the Shapiro–Wilks to assess the normality and continued with an independent t-test if the data were parametric or using the Mann–Whitney test if the data were nonparametric.
RESULT
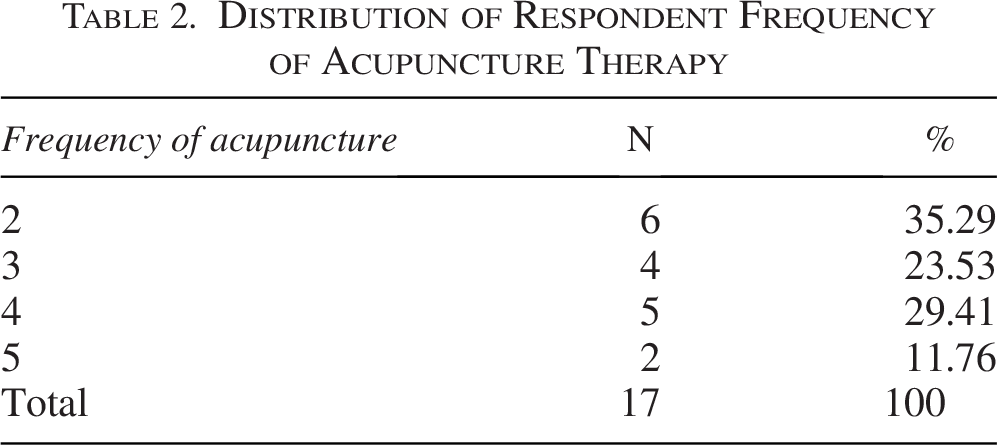
The maternal childbirth outcomes are presented in the tables below. Table 1 presents the average age for women in the intervention and control groups, which were 30.88 ± 3.68 and 33.23 ± 4.20, respectively. No significant difference for all characteristics participants between both groups was found in this study (p > 0.05). Table 2 concludes that most participants received either two or four sessions of acupuncture therapy, with two sessions being the most common.
The Characteristics of Respondents

Statistical significance was set at p < 0.05. All statistical results were insignificant.
p-Value calculated using chi-square test.
p-Value calculated using Fisher’s exact test due to expected frequencies less than 5 in one or more cells.
SD, standard deviation.
Distribution of Respondent Frequency of Acupuncture Therapy
As shown in Table 3, this study found that all participants had spontaneous onset of labor and no participants received any medical induction during the labor in both groups (p = 1.00). Prenatal acupuncture significantly reduces labor pain (VAS scores 5 ± 0.707 vs. 6.12 ± 0.928; p = 0.000) and shortens both the active phase (4.80 vs. 6.50 h; p = 0.000) and second stages of labor (18 vs. 31 min; p = 0.000) compared with those in the control group. Regarding perineal tearing, most women in both groups experienced second-degree perineal tears (52.94% in the intervention group, 64.71% in the control group) that was not significantly different between groups (p = 0.261). In terms of colostrum production, a greater percentage of participants in the intervention group began producing milk within 24 h, whereas a higher proportion in the control group commenced production after 24 h (p = 0.002).
Effects of Prenatal Acupuncture on Onset of Labor, Labor Pain, Duration of the Active Phase, Second Stage of Labor, Perineal Tears, and Colostrum Production
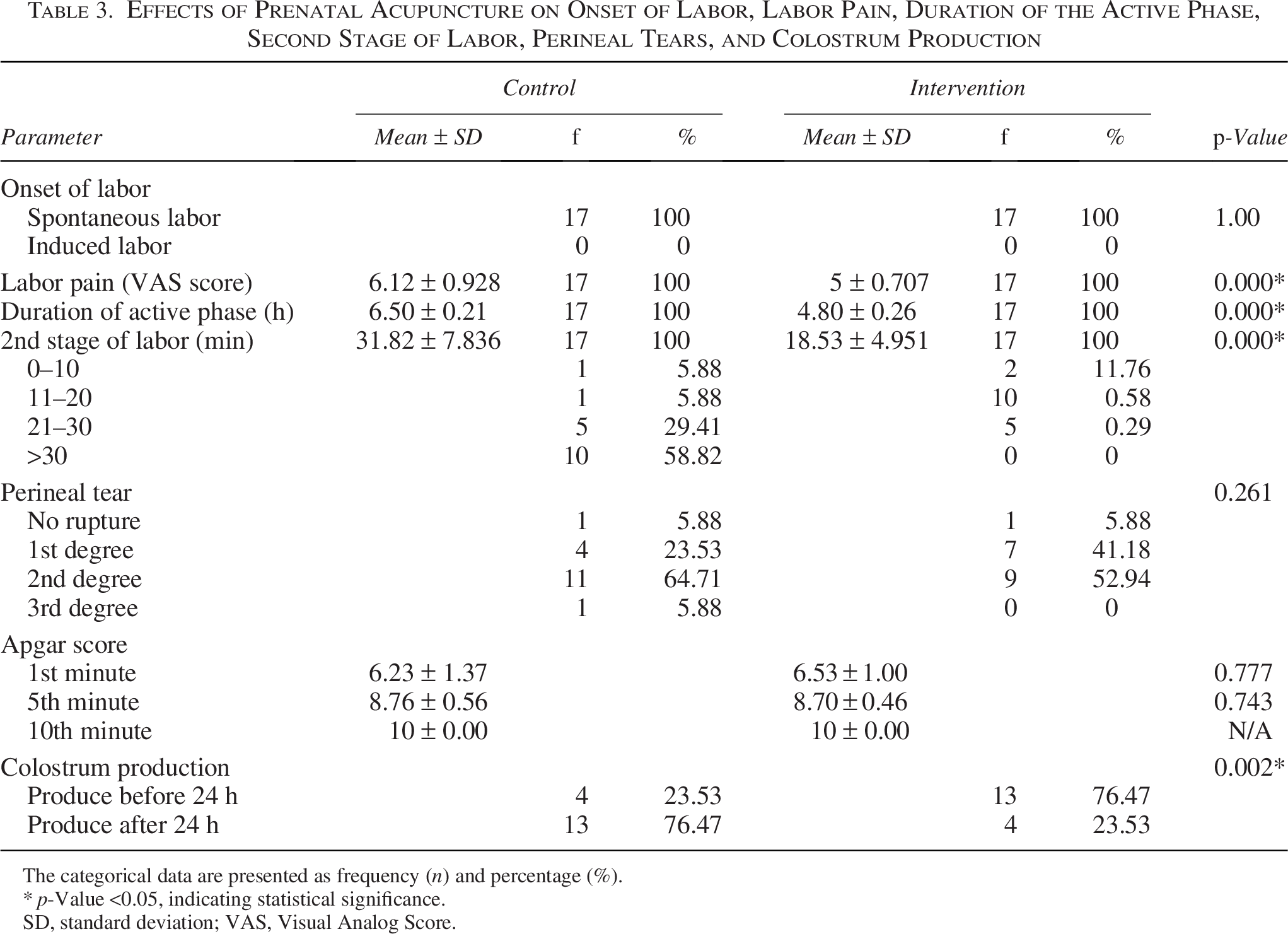
The categorical data are presented as frequency (n) and percentage (%).
p-Value <0.05, indicating statistical significance.
SD, standard deviation; VAS, Visual Analog Score.
DISCUSSION
Effect of Prenatal Acupuncture on Onset of Labor
In this study, all participants in both the intervention group and the control group experienced spontaneous onset of labor, and no differences were observed between the groups. The uniformity of spontaneous onset across groups may indicate that other physiological or maternal factors played a more dominant role in triggering labor. Similar results have been reported in previous studies where acupuncture showed limited effect on the spontaneous onset of labor, emphasizing that while acupuncture may provide benefits for maternal comfort and other perinatal outcomes, its role in stimulating onset of labor remains inconclusive. 40
Effect of Prenatal Acupuncture on Labor Pain, Duration of Active Phase, and Second Stage of Labor
This study found that prenatal acupuncture significantly reduces labor pain and shortens both the active and second stages of labor compared with those in the control group. This aligns with earlier findings that acupuncture can be effective in managing labor-related pain, 16 improved cervical ripening, 41 and reduced the duration of the first stage of labor42,43 and second stages of labor. 43
Previous studies indicated that acupuncture administered in the late stages of pregnancy—typically between 35th and 39th weeks—may contribute to more efficient labor. While previous studies focus on acupuncture administered during labor itself, our study focuses on investigating the prenatal acupuncture before childbirth. This treatment may influence labor outcomes through direct analgesic effects, enhancing cervical ripening, promoting spontaneous onset of labor, and modulating maternal physiology in advance of birth.41,44
No acupuncture was administered on the day of labor, and acupuncture was completed within 1–4 days before labor, yet analgesic benefits persisted and had longer lasting effects. Studies reported that acupuncture induces pain-inhibitory effects that last up to 6 days after a single treatment. 45 These sustained effects may involve multiple interacting mechanisms, including neurophysiological, hormonal, and psychological components.
Acupuncture stimulates the release of endogenous opioids (e.g., β-endorphins), calcitonin gene-related peptide, and adenosine. Functional MRI studies demonstrate that acupuncture activates brain regions involved in the processing and modulation of pain, including the periaqueductal gray, anterior cingulate cortex, and prefrontal cortex, 46 leading to pain inhibition and relaxed emotion during labor.
Acupuncture enhances oxytocin and prostaglandin release, improving uterine contractility and cervical readiness. Improved uteroplacental blood flow through sympathetic inhibition may optimize labor progression. 47 The acupuncture points, namely Hegu LI4, Zusanli ST36, and Sanyinjiao SP6, are recognized for their roles in pain modulation and labor. Hegu LI4 stimulation activates descending inhibitory pathways and promotes the release of endogenous opioids, thereby reducing pain intensity. Zusanli ST36 contributes to improved gastrointestinal function and immune modulation, indirectly supporting the body’s response to stress and pain during labor. In addition, Sanyinjiao SP6, which is an intersection point of the spleen, liver, and kidney meridians, is implicated in hormonal regulation, parasympathetic activation, and circulating catecholamines reduction, which may indirectly decrease pain and prepare the reproductive tract for labor. These mechanisms are further supported by the review by Levett et al., 16 outlining how acupuncture and acupressure can effectively modulate pain pathways and improve labor outcomes.
Furthermore, regular acupuncture during pregnancy may reduce maternal anxiety, enhance coping abilities, and increase labor self-efficacy; thus, these could influence the perception of pain and labor duration. 16 Hence, even in the absence of direct analgesic administration during labor, a well-prepared psychological state may enhance pain tolerance and improve birth experience.
Acupuncture is believed to exert its effects by enhancing the frequency and coordination of uterine contractions, facilitating cervical ripening, and reducing maternal pain perception. These outcomes are mediated through the stimulation of specific acupoints, which promote the release of endogenous opioids such as endorphins and increase oxytocin secretion—both of which contribute to more efficient uterine activity, including enhancing uterine contractility. 48 In addition, the analgesic effects of acupuncture, mediated by neuropeptide release and modulation of the central nervous system, may help reduce maternal stress and muscular tension during labor, thereby facilitating cervical dilatation and baby descent. 49 The reduction in perceived pain and anxiety may help improve maternal cooperation and physical endurance during the second stage of labor, thus enabling a smoother and more effective birthing process.
Impact on Perineal Outcomes
No significant differences were observed in perineal tear rates between the intervention and control groups. Most existing research addressing perineal integrity has focused on perineal massage, which has been shown to improve elasticity and reduce trauma.50–53 In contrast, acupuncture has rarely been evaluated for its impact on perineal outcomes, highlighting a notable gap in the literature. Future studies that specifically assess perineal integrity in relation to acupuncture are needed to clarify its potential role.
Neonatal Outcomes: Apgar Score
No significant differences were observed in Apgar scores between both groups, suggesting that prenatal acupuncture is not associated with adverse neonatal outcomes. Thus, this finding supports the safety profile of prenatal acupuncture.
A study reported higher Apgar scores in the intervention group receiving auricular acupuncture combined with doula support. 54 While improved maternal comfort and reduced labor stress may indirectly benefit neonatal outcomes through enhanced uteroplacental circulation, the evidence of acupuncture contributing to these outcomes remains limited. Future studies with well-controlled designs and standardized acupuncture regimens are warranted to evaluate potential subtle or long-term effects on neonatal outcomes.
Colostrum Production
In this study, women in the acupuncture intervention group began producing colostrum within 12 h after labor and birth, whereas those in the control group required more than 24 h. To our knowledge, only a limited number of studies have examined colostrum production in relation to prenatal acupuncture, and most previous research has focused instead on outcomes such as labor induction, pain relief, or duration of labor. Our findings therefore provide new evidence in this area. Acupuncture is thought to promote the release of prolactin and oxytocin—hormones crucial for milk synthesis and ejection. Stimulation of points, including ST18, SI1, and CV17, is associated with increased serum prolactin levels. 55 These hormonal responses facilitate mammary gland activation and accelerate transition from colostrum to mature milk.
Study Limitations
This study is limited by the lack of randomization and data regarding the exact timing of the last acupuncture session.
CONCLUSION
These findings suggest that prenatal acupuncture serves not only as a nonpharmacological pain relief in labor but also as an intervention that can optimize physiological labor processes, particularly shortening the active phase and second stage of labor, with no significant effect on neonatal outcome. Nevertheless, future studies with larger cohorts and biochemical assessments are warranted to explore its mechanisms and optimize treatment protocols.
AUTHORS’ CONTRIBUTIONS
S.H. conceptualized the study, designed the methodology, and secured ethical approval. N.J.W. and H.P. were responsible for data collection and clinical assessments. R.P. conducted the data analysis. D.N.P. contributed to the literature review and initial drafting of the article. I.N. supervised the research process and critically reviewed the article. All authors contributed to data interpretation, revised the article critically for important intellectual content, and approved the final version.
Footnotes
ACKNOWLEDGMENTS
The authors thank Dr. Syaiful Huda, Dr. Abi, and their team, as well as the Familia Primary Health Clinic team, for their invaluable support and assistance.
AUTHOR DISCLOSURE STATEMENT
The authors declare no conflicts of interest. No interests to disclose.
FUNDING INFORMATION
This study was supported by a grant from LPPM UNS under the Hibah Kolaborasi Perguruan Tinggi Dalam Negeri program (Contract No: 1496/UN27.22/PT.01.03/2023).
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.