
Abstract
Research has shown that acupoint therapy can be a viable, evidence-based treatment for treating sleep, anxiety, and pain symptoms among children, adolescents, and adults. This article provides a framework to translate acupoint therapy into formalized programs in outpatient and inpatient pediatric settings. The lead author and her team worked together with children and adolescents in urban school-based health centers and a pediatric tertiary care hospital within a large academic urban medical center using different forms of acupoint therapy to support patients in managing a variety of symptoms. We describe the process of developing patient-centered, evidence-based programs with a strong foundation in research, administration, clinical care, and education, and demonstrate how this model can be effective through teamwork, training, and innovation.
Keywords
INTRODUCTION
The use of integrative health is growing in many fields of medicine, including pediatrics, internal medicine, family medicine, and oncology. Multiple studies have confirmed that acupoint therapies such as acupressure and acupuncture can have a positive impact on managing sleep,1–4 anxiety,5,6 pain, 7 and other symptoms8,9 among children and adolescents,5,8 as well as adults. This article focuses specifically on the development and growth of a program focused on acupoint therapy in pediatric settings. Given the efficacy of acupoint therapies demonstrated through randomized controlled trials for symptom management, efforts are needed to expand access to acupoint therapies for pediatric populations. Over 10 years, a Pediatric Integrative Medicine team established acupoint therapies in outpatient and inpatient settings in New York City (NYC). There are few published accounts of the development of pediatric outpatient and inpatient integrative medicine programs or services. To support future programming, this article describes the evolution and expansion of an integrative acupoint therapy program in pediatrics in outpatient and inpatient programs.
GUIDING FRAMEWORK FOR THE PROGRAM
What centers this program framework are four key elements—clinical care, research, teaching, and administration—that are overlapping and strengthened by a focus on building relationships. While clinical care and the care of patients are at the center of the program, focusing on simultaneously nurturing research, training, and administrative support functions was key to successful program development. Our program is guided by goals that are explicitly articulated and SMART-EST 9 : Specific, Measurable, Attainable (or achievable), Relevant, Time-bound, Evidence-based, and STrategic. The intersecting relationships of team members in roles across the key elements (clinical, research, teaching, administration) have a shared articulation of these SMART-EST goals (Fig. 1). Most frameworks for clinical program development follow a linear process. The framework for building this program (Fig. 1) was not linear. Being wedded to a linear process may stand in the way of building a successful program. Many of the program components—such as founding the outpatient program and building a research base—occurred simultaneously. Other program development steps were revisited as the program grew gradually over time (Fig. 2).

Framework for SMART-EST goals. SMART-EST, Specific, Measurable, Attainable (or achievable), Relevant, Time-bound, Evidence-based, and STrategic.
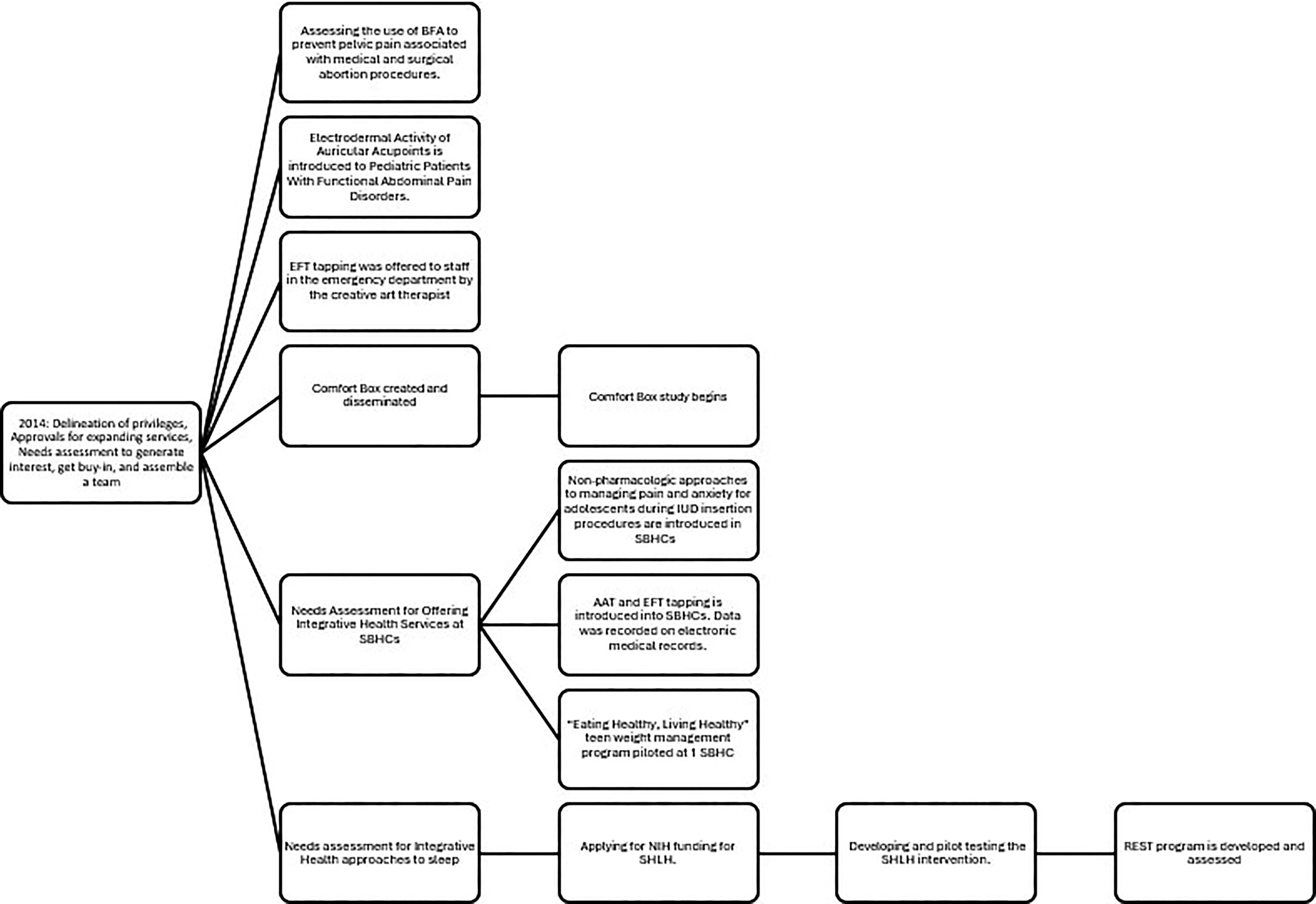
Growth model of pediatric integrative program development. AAT, aroma acupoint therapy; BFA, battlefield acupuncture; EFT, emotional freedom techniques; REST, resident education in sleep techniques; SBHC, school-based health center; SHLH, sleeping healthy living healthy.
SCOPE OF THE PROGRAM
The program implemented five types of acupoint therapy over 10 years: aroma acupoint therapy (AAT), acupressure, emotional freedom techniques (EFT) tapping, acupuncture, and auriculotherapy (including using needles, electrical stimulation, adhesive beads, seeds, or magnets) for battlefield acupuncture (BFA) or National Acupuncture Detoxification Association protocols. A published evidence-base and a long clinical practice history support these integrative therapies for conditions frequently seen in pediatric outpatient and inpatient settings; these integrative therapies are easily implemented with children and adolescents. Research has demonstrated that children and adolescents are receptive to integrative therapies during hospital admissions and outpatient medical visits.10–12
ADMINISTRATIVE AND LEADERSHIP SUPPORT
The program’s institution is composed of two universities and one affiliated hospital system, a common structure for academic institutions and affiliated hospitals. The first step in founding the program in 2014 was to address the fact that there were no acupuncture privileges in either pediatric department. Because there were two academic departments of pediatrics, approval was needed from both departments to credential two pediatric faculty at one university who wanted to offer acupuncture. These two faculty members wrote the delineation of privileges (DOP) themselves, adapted from those from other departments, and submitted the DOP to the credentialing committees for approval. This process took 6 months.
Administrative approval and buy-in were needed to support the program lead’s initial assessment of the need for acupoint therapies in the outpatient (SBHC) and inpatient hospital settings, as well as to make it a viable evidence-based treatment option, to allow expansion of clinical services to include acupoint therapies, and to allot staff time to receive training and supervision in providing acupoint therapies to patients. When the SBHC teams met together at the beginning of staff meetings, everyone learned and practiced different integrative or acupoint therapies. This included weekly, monthly, and quarterly all-staff meetings. Integrative therapies were taught by the program lead (M.A.G.), coauthors (M.B. and K.M.), SBHC staff, or outside trainers who were brought in to work with the team. Support was garnered from hospital leadership and from the SBHC leadership, which resulted in allocating discretionary funds to purchase supplies needed for clinical acupoint therapy services (e.g., essential oils, diffusers, acupuncture needles and electrical stimulators, ear point finders, adhesive beads) The majority of student–patients at the SBHCs are uninsured, underinsured, or receive medical assistance, which does not cover integrative or acupoint therapies in New York. SBHC leadership supported requests to allocate time for SBHC staff to learn integrative therapies and allowed time to integrate these services into patient clinical flow. They allowed staff time to create innovative programs or to participate in clinical research, all of which took time. The SBHC administration also supported staff time to teach regionally in Years 4 and 5, leading to local recognition of staff expertise and boosting staff morale.
We were fortunate in that our leadership embraced the introduction of integrative therapies and, in particular, acupoint therapies in our settings. Thus, we did not experience significant barriers in the incorporation of these therapies. The lead frequently offered integrative therapies to leaders and administrators so they had a better understanding of the value of integrative therapies, which went a long way in garnering their support in introducing these modalities within clinical care, education, and research.
CLINICAL CARE
A case vignette is presented in Supplementary Appendix S1 to exemplify the patient-centered care focus of the program and illustrate the range of program components. While awaiting DOP approval, efforts were dedicated to assessing and building interest in integrative health among colleagues and potential collaborators within and outside the Department of Pediatrics. Building partnerships and teams to support clinical services began in the outpatient setting by assessing awareness among the SBHC staff about integrative approaches to school-based health. SBHCs are clinical entities that provide health services to student–patients in collaboration with, but operated independently of, the school system. SBHCs reduce barriers to care that children and adolescents often face when accessing traditional health care, such as transportation or parental availability, and they provide comprehensive, age-appropriate health care to student–patients who may otherwise be unable to access care.13–15 Services at SBHCs include primary care, including immunizations, and often mental health and reproductive health care, including contraceptive services of all adolescent-appropriate methods. Parental consent was required for any student–patient to receive primary care services. SBHC medical providers called parents to inform them of treatment plans, including acupoint therapies. Parents expressed great interest in these practices, so the SBHC offered educational sessions about acupoint therapies to parents.
Essential in this phase was listening carefully to what others saw as areas that needed or could support integrative therapies. An informal needs-assessment phase was carried out in conjunction with expanding other clinical services. Integrative acupoint therapies were offered to manage student–patients’ common conditions (Table 1). Once needs were assessed through these informal partnerships, the program lead met regularly to encourage the four disciplines at the SBHC (medical, mental health, health education, patient financial advisors) to champion a specific integrative health modality. The specific integrative health modality was chosen based on each discipline’s scope of practice and staff interest. The patient financial advisors (registration clerks who assist patients in scheduling appointments and getting insurance) chose to learn aromatherapy for the waiting areas. The health educators chose mindfulness meditation and later requested to receive small group training on aromatherapy. The mental health providers asked to learn clinical hypnosis, followed by AAT, 16 and then EFT tapping. The nurse practitioners (NPs) expressed interest in acupressure. Later they requested training on AAT and hypnosis to manage student–patient anxiety and discomfort around procedures such as vaccinations, phlebotomy, and insertion and removal of intrauterine devices (IUDs) and contraceptive implants. The SBHC staff embraced these practices and incorporated them with the support of the administration and program lead.
Common Conditions Treated With Acupoint Therapies in Outpatient Setting Such As School-Based Health Centers
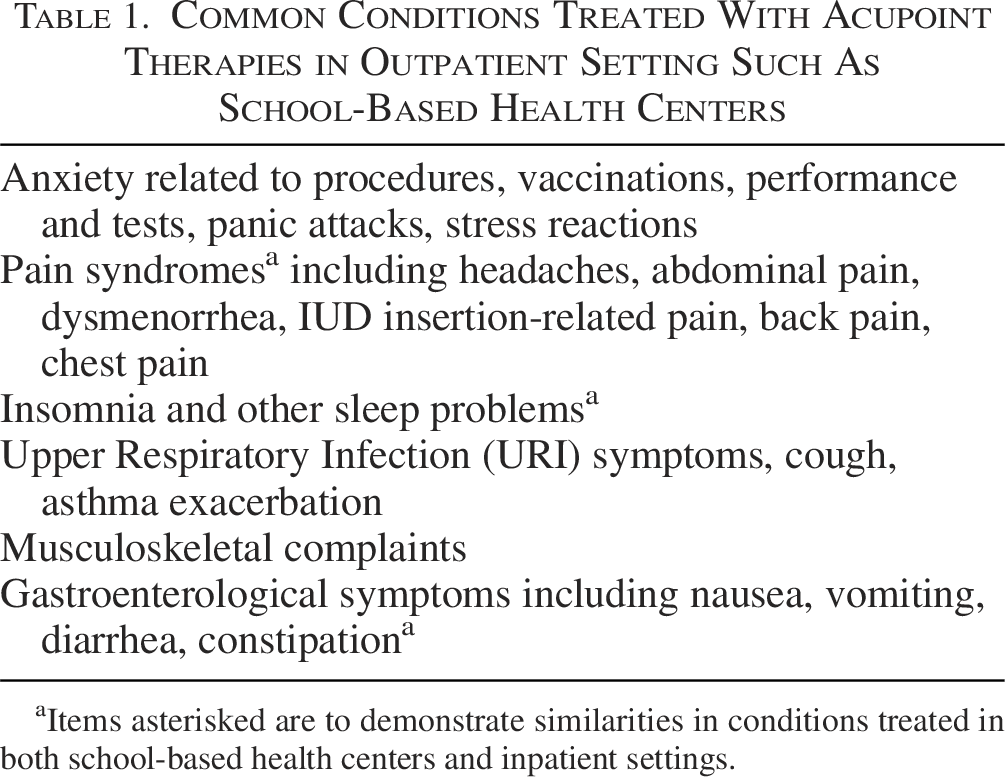
Items asterisked are to demonstrate similarities in conditions treated in both school-based health centers and inpatient settings.
Training led to creative innovations by staff. At one SBHC, they wanted to address obesity and better support overweight adolescents. The team at this site created a multidisciplinary “Eating Healthy, Living Healthy” teen weight management program with small groups of student–patients who received auricular acupressure seeds for appetite control and tranquility points to diminish appetite and manage anxiety (as student–patients’ commonly reported anxiety and worry about eating). Student–patients were also taught mindfulness meditation and were offered aromatherapy. They journaled, practiced 4:7:8 breathing, received dietary education, and completed weigh-ins with NPs. 17
The team also created a Stress Relief Kit (Figs. 3 and 4) for AAT with four essential oils (chamomile, lavender, bergamot, and atlas cedarwood) and instructions for use. 18 AAT entails applying essential oils on acupuncture points and is hypothesized to stimulate bioenergy channel flow. “The principle involved rests on creating an energetic resonance between [the essential oil and acupuncture point], sympathetic vibration or frequency… a positive mutual resonance between oil and point creates a synergy, a combined quantum effect that obtains therapeutic results.” 16 This is further described in our article “The theoretical concept proposed is that the natural bioenergetic frequency of an essential oil provides information to an acupoint. In the principle of resonance, the synergy between a certain oil and a particular point can trigger a specific type of therapeutic action in a patient.” 11
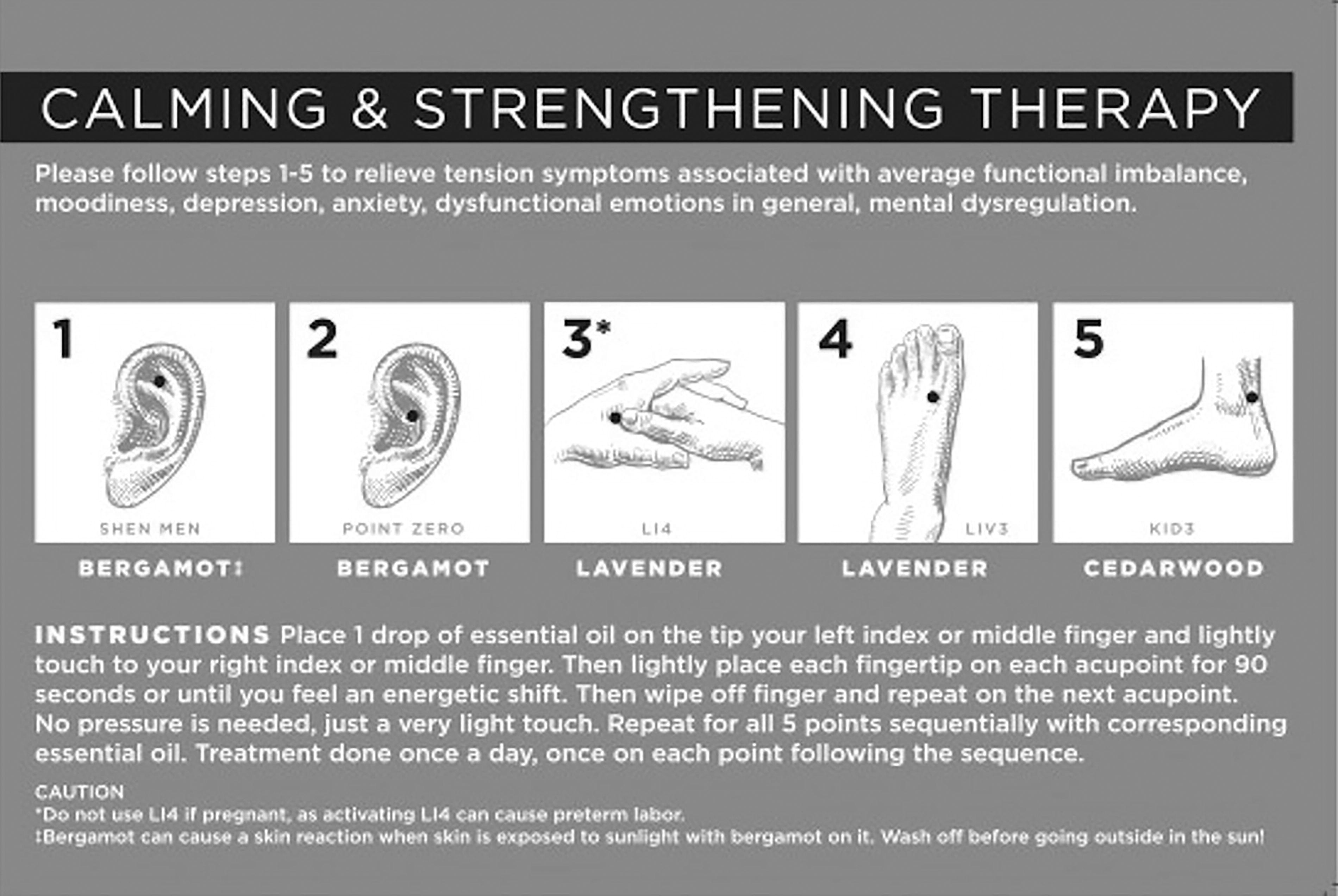
Calming and strengthening therapy. LI4—also known as Hegu, located on the back of the hand between the base of the thumb and index finger. LIV3—also known as Tai Chong, located on the top of the foot between the big toe and the second toe. KID3—also known as Taixi, located in the depression between the tip of the medial malleolus and Achilles tendon.
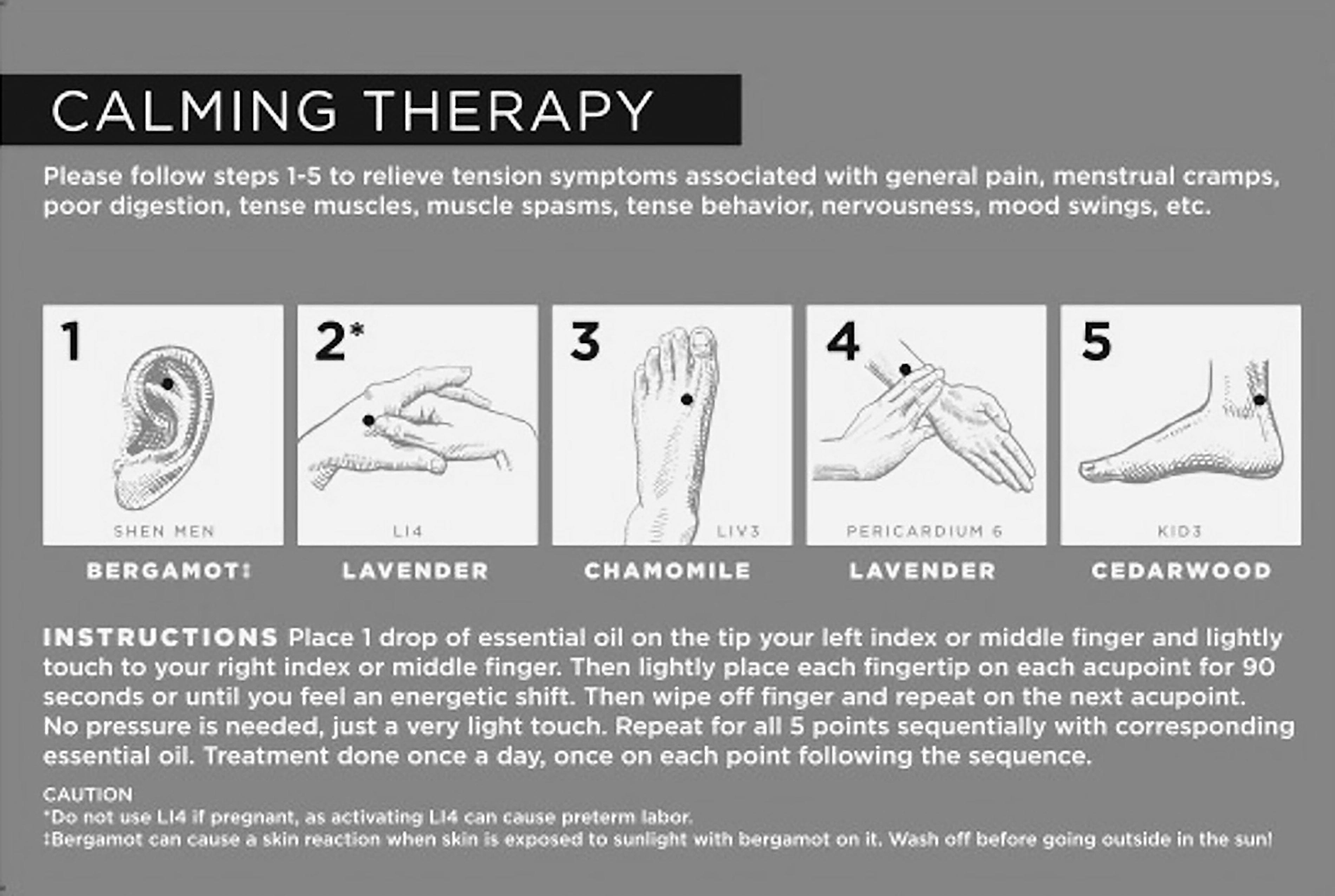
Calming therapy. Pericardium 6—also known as “Nei Guan” (inner gate), located on the inner wrist.
They taught the NPs in the SBHCs how to provide AAT to patients using the Stress Relief Kit for common conditions (Table 1). AAT use was recorded in the electronic medical records (EMR). The team collected and compiled EMR data for a case series describing the use of AAT in the SBHC setting, the first publication on the use of AAT in the pediatric literature. 11
Simultaneously, the SBHC staff were taught EFT tapping for self-care. EFT tapping was used during staff team meetings as a break during lengthy meetings to enhance energy and recharge staff motivation. As the staff became familiar with these therapies, they became more invested in sharing these techniques with student–patients and student–patients’ families.
Years 5–8: Outpatient
EFT tapping was taught to the SBHC Peer Educators during their summer orientation beginning in 2019. SBHC Peer Educators are high school student–patients who are hired as volunteers by the affiliated hospital. In addition to EFT tapping, peer educators learned acupressure and mindfulness meditation. During the training, the youth were shown each of the acupressure points, and they practiced locating the points by placing adhesive star stickers on their skin. During the training, the program lead (M.A.G.) and coauthor (M.B.), a licensed acupuncturist, worked with other SBHC staff to ensure that the peer educators’ point locations were correct.
Outpatient Research
Outpatient research was conducted with gynecologists at the same institution and at the SBHCs.
Gynecology Research Years 2–6
The lead author taught gynecologists an adapted BFA protocol for auricular therapy. The original BFA protocol was modified for research to test its effectiveness in preventing pain associated with gynecological procedures. Three studies were conducted with the gynecology team assessing the use of adapted BFA to prevent pelvic pain associated with medical and surgical abortion procedures.19–21 Other research with public health students and gynecology faculty describes barriers that patients face in accessing acupuncture, both due to state-specific acupuncture licensing requirements and due to lack of insurance coverage for acupuncture.22,23
SBHC Research Year 2
In 2015, as SBHCs began to introduce integrative therapies into the clinical setting, a needs assessment was conducted in collaboration with master’s in public health students from the affiliated university to assess what SBHC student–patients knew about acupoint therapy and other integrative therapies. The assessment explored student–patients’ awareness, interest, experience with integrative therapies, and their health goals. Their primary health goal was improving sleep.
SBHC Research Years 3 and 4
The first needs assessment led to a second needs assessment on SBHC student–patients’ sleep quality and interest in participating in Mind Body Integrative Health sleep interventions. 24 The pilot data were used to apply for NIH grant funding to develop and test an integrative sleep intervention at the SBHC.
SBHC Research Years 5–8
After the second grant application round, the team received funding from the National Institute of Minority Health and Disparities for an R21, a 2-year development grant, to create and pilot test the Sleeping Healthy Living Healthy (SHLH) intervention.25,26 As part of the development phase of the first year of the grant, the team published a literature review on integrative approaches to sleep interventions for adolescents and conducted formative research. 27 For the intervention study, student–patients were recruited from two SBHCs to participate in a randomized controlled trial (RCT). The SHLH intervention included acupoint therapies such as acupressure and EFT tapping, as well as several forms of mindfulness. Outcomes assessed at baseline, immediately postintervention, and 10-week postintervention included: Sleep quality (Pittsburgh Sleep Quality Index [PSQI]); PROMIS (Patient Reported Outcomes Measurement Information System) sleep-related impairment, stress, and anxiety; and perceived stress (Perceived Stress Scale). Actigraphy data were collected at each assessment. Generalized linear mixed-effects models with a random subject effect tested effects on outcomes following the intent-to-treat principle. 28
Additional Outpatient Research Year 9
In 2022, the team received donor funding to modify the SHLH curriculum for pediatric residents and fellows to address sleep deficiency. The Resident Education in Sleep Techniques (REST) program taught residents and fellows a variety of integrative approaches to improve their own sleep. Modules include sleep tips and instructional videos. REST also taught trainees integrative approaches to help their patients’ sleep, with resources and handouts for adolescent patients and their parents.
Inpatient Year 1
The timeline for introducing integrative therapies to the inpatient pediatric program began in 2014. The program began with acupoint therapies to manage common symptoms experienced by children and adolescents related to hospitalization, including anxiety around being in the hospital, having procedures (surgical, chest tube placement, intravenous lines, phlebotomy, etc.), receiving a diagnosis, medication administration, pain syndromes, disturbed sleep, and gastroenterological complaints, including nausea and vomiting (Table 2). Care for adolescents regularly addressed nausea, vomiting, and bloating for eating disorder patients and those with cannabis hyperemesis syndrome. Collaborations with psychiatry offered acupoint therapies and were anecdotally well received by patients and their families.
Common Conditions Treated With Acupoint Therapies In Inpatient Settings

These items demonstrate similarities in conditions treated in both school-based health centers and inpatient settings.
Inpatient Years 2–4
While on the consult service, the lead author taught hospital medicine, adolescent medicine, and other subspecialty faculty, adolescent medicine fellows, pediatric residents, and medical students acupoint therapies such as auriculotherapy, acupressure, EFT tapping, and AAT to address common conditions experienced by pediatric patients in the hospital (Table 2).
Inpatient Years 4 and 5
The lead author taught inpatient pediatric hospitalists several nonpharmacologic therapies, including AAT and BFA (using an ear point finder), to manage pain for hospitalized children and adolescents.
Inpatient Years 5–8
Teaching and clinical exposure in acupoint therapies led to a second-year pediatric gastroenterology fellow conducting mentored research on auricular acupoint mapping for functional abdominal pain. The research identified electrodermally active auricular acupoints to develop intervention and control auriculotherapy protocols to be used to conduct an RCT. 29
Inpatient Years 6–9
A multidisciplinary inpatient team partnered together at the start of the COVID-19 pandemic to address isolation among hospitalized pediatric patients and their families. Representatives from integrative therapies (acupuncturists), creative arts therapy, pastoral care, nursing, psychology, psychiatry, hospital medicine, and adolescent medicine joined together to share resources, discuss integrative service provision, identify overlaps, and learn from each other. From these interactions, the team created and disseminated a well-being resource. 30 To address staff stress during COVID-19, EFT tapping was offered to staff in the emergency department by the creative art therapist as part of this initiative, and its effectiveness was evaluated in partnership with public health and nursing research partners. 31
For pediatric inpatients, the team developed a “Comfort Box” project where integrative medicine materials were distributed to hospitalized patients to use during their admission and at home after discharge. Each Comfort Box includes three types of aromatherapy (lavender, peppermint, and orange oil); laminated cards with QR codes linking patients and their families to audio recordings or websites on self-hypnosis and EFT tapping; and cards describing acupressure points for common symptom management. The box also contains finger labyrinth cards, a mandala coloring book, a fidget spinner popper, and two types of stress balls that are helpful when children and adolescents have anxiety or are waiting to have procedures or scans. The Comfort Boxes are donor-funded, and once a patient receives a box, it belongs to them, and they take it home. A semi-structured interview guide (combining qualitative and quantitative data collection) was used to assess adolescent patients’ use of and satisfaction with the Comfort Box. Analysis is complete, and the article describing the study findings is being submitted to a peer-reviewed journal.
The SBHC team was asked to teach staff from other SBHCs in NYC about how they successfully incorporated providing IUD and contraceptive implant services into SBHC services. The trainings were funded and coordinated by the New York City Department of Health, Office of School Health. The lead author proposed to the director of the program that they include training on the use of integrative therapies to help staff manage their own anxiety and to help patients deal with anxiety and pain, as this was part of the SBHC team’s success. The director of the Office of School Health was very supportive, and this resulted in two 8-h trainings in 2018 and in 2019, of which the last 2 h of the training focused on teaching how to use integrative therapies with SBHC staff from around NYC. The training focused on dealing with staff anxiety related to providing IUD services and also on how to manage patient anxiety and pain related to procedures. Staff were taught how to apply bergamot oil on the auricular point Shen Men so that they would stay calm and focused while doing procedures, especially when situational stressors occur. Staff were also taught how to do self-acupressure for stress relief of their own heads and necks. Materials were created in English and Spanish for patients with the help of public health students and included videos teaching acupressure use on Sanyinjiao (Spleen-6) for IUD-related pelvic pain and dysmenorrhea management. Nonpharmacological interventions, such as the use of acupressure and mind–body elements, have been recommended to reduce patient anxiety and discomfort during IUD placement. 32 This led to one of the public health students coauthoring a book chapter with the lead author on nonpharmacologic approaches to managing pain and anxiety for adolescents during IUD insertion procedures. 33
BUILDING RELATIONSHIPS AND PROGRAM LEADERSHIP
The work described above was made possible by having a program lead with training and experience—as well as a commitment to foster accountability, transparency, and collegiality. Centering the building of relationships requires collaborative and supportive multidisciplinary relationships.
DISCUSSION
This is a description of one team’s experience utilizing acupoint therapies in a pediatric tertiary care environment in NYC. Thus, this may not be generalizable to rural or suburban environments or other fields of medicine. Of note, the team did not hire new staff to implement integrative acupoint therapies. The model used involved training existing staff in acupoint therapies. Donor funding was critical to the success of pilot programs and initiatives (e.g., Comfort Box and REST curriculum). Health care professionals were not able to bill for the costs associated with providing acupoint therapies, and services were integrated into routine services provided in the outpatient and inpatient settings. The majority of student–patients at SBHCs receive medical assistance or are uninsured and are not charged for any health care services. Visits where acupoint therapies were provided were billed by time and for the ICD-10 diagnosis.
When research was funded, specific metrics were used to measure impact, such as the R21 for SHLH. However, much of the clinical care and education around acupoint therapies did not include metrics to measure impact. If other researchers and clinicians want to implement such a program, having metrics in place from the start would be extremely valuable. BraveNet, a practice-based research network of integrative medicine clinics across the United States, provides a model for this kind of structured evaluation. Examples of how this can be done and metric selection are illustrated by the publications supported by BraveNet. 34
CONCLUSION
Acupoint therapies can be integrated seamlessly into both inpatient and outpatient settings to support management of common symptoms experienced by children and adolescents from a variety of health conditions. Codeveloping clinical, teaching, research, and administrative aspects of programming can result in overall success. There are innumerable ways to be creative in applying this model of pediatric acupoint therapy to other healthcare settings.
AUTHORS’ CONTRIBUTIONS
I.K. drafted the initial article in collaboration with M.A.G., which was based on a transcript of the plenary session Dr. Gold presented at the AAMA Symposium on April 15, 2023, in Dallas, TX. M.B., S.G., I.K., K.M., and M.A.G. reviewed and revised the article. All authors approved the final article as submitted.
Footnotes
ACKNOWLEDGMENTS
The authors thank their patients for participating in this new model, sharing their experiences, and allowing the authors to partner with them. The authors thank all the SBHCs and hospital staff, as well as hospital administration leadership, especially Janet Garth, MPH, without whom this work would have been impossible. The authors thank the donors for supporting the Comfort Box and REST curriculum development projects. The authors particularly thank Susan Rosenthal, PhD, for her many years of mentorship and support.
AUTHOR DISCLOSURE STATEMENT
M.A.G. has been a member of the Scientific Advisory Board of the Tapping Solution App since 2020 (uncompensated role) as well as a consultant for Bayer, Policy & Research Group, and 5 Points App. She was a consultant for the Tapping Solution, LLC, and Tapping Solution Foundation from March through August 2024. M.A.G. and S.G. received funding for their investigator-initiated research on the Telehealth-Supported Long-Acting Reversible Contraception in School-Based Health Centers study from Merck/Organon. I.K., M.B., and K.M. have no conflicts of interest.
FUNDING INFORMATION
No funding was provided for this work.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.