
Abstract
Objective
To evaluate the effects of salacinol on stool levels of putrefactive products and intestinal function in healthy adults.
Methods
We conducted a double-blind, randomized, parallel-group comparative study to examine changes in stool characteristics and defecation-related symptoms associated with salacinol intake in healthy adults aged 55 to 70 years living in Japan. The salacinol group received salacinol supplementation (1 mg/day for 28 days), whereas the placebo group received placebo. We collected stool samples before the start of the study, after 14 days of intake, and on designated days or the day after the study completion date. We assessed stool pH and water content, bowel movement frequency, subjective stool odor score, subjective defecation score, stool putrefactive products (ammonia, phenols, paracresol, indole, skatole, 4-ethylphenol, and total putrefactive products) and safety outcomes. We analyzed these data using the chi-square test or Fisher’s exact test for qualitative variables and the Mann–Whitney U test and the Jonckheere–Terpstra test for quantitative variables.
Results
Thirty-nine participants consented to participate. After exclusion of those who met the exclusion criteria or withdrew consent, 24 participants (70.8% female, mean age 60.3 years, 12 in the salacinol group and 12 in the placebo group) were included in the analysis. The salacinol group showed a significant reduction in stool ammonia levels (approximately 40% from baseline), beginning at day 14 and continuing through day 28, and stool water content increased. These results suggest that salacinol may help regulate intestinal levels of ammonia and other putrefactive products.
Conclusions
The observed decrease in putrefactive products is consistent with salacinol’s proposed effect on microbial fermentation, which is thought to occur through inhibition of carbohydrate absorption in the small intestine. These findings suggest that salacinol has potential as a new functional compound that promotes intestinal health through microbiota-mediated mechanisms.
Keywords
Introduction
According to the most recent clinical guidelines for chronic constipation, approximately 10–15% of the Japanese population report symptoms of constipation, with a higher prevalence among women and a gradual increase with age. 1 Chronic constipation is a risk factor for a variety of conditions, including colorectal cancer,2,3 hemorrhoids, 4 and intestinal obstruction. 5 In the elderly population, constipation is further associated with reduced quality of life 6 and has been suggested to contribute to the risk of developing dementia. 7
To relieve constipation, lifestyle changes are necessary, particularly dietary modifications. Consuming foods that promote intestinal health is one effective strategy. These properties are commonly attributed to probiotics, 8 prebiotics, 9 or synbiotics, 10 with the latter being a combination of both. Although salacinol does not fall into these conventional categories, studies have suggested that it has beneficial effects on intestinal function.11,12 Salacinol is a bioactive compound extracted from Salacia, a plant in the family Hippocrateaceae that has been traditionally used in Ayurvedic medicine to treat diabetes.13-15 Salacinol acts as an α-glucosidase inhibitor, thereby reducing the absorption of disaccharides in the small intestine.16-18 Consequently, undigested disaccharides and oligosaccharides reach the large intestine, where they are presumed to promote the proliferation of Bifidobacterium and Lactobacilli species, while concurrently suppressing the growth of Escherichia coli. In studies of the rat intestinal microbiota, salacinol increased the relative abundance of Bacteroides and decreased that of Firmicutes. 19 In human studies, salacinol increased Bifidobacteria levels while decreasing the prevalence of Clostridium species. 20
While the health benefits of common functional foods, such as yogurt and probiotics, have been extensively documented, there is a significant lack of human clinical data regarding salacinol, and further additional studies are needed.
Based on these findings, we hypothesized that oral salacinol intake would act as an α-glucosidase inhibitor, thereby reducing stool putrefactive products and improving intestinal function. To test this hypothesis, we conducted a randomized, placebo-controlled study in healthy adults.
Methods
Study Design
This study utilized a double-blind, randomized, parallel-group comparative design and was conducted in Matsumoto City, Nagano Prefecture, Japan. The intervention group received tablets containing salacinol, while the placebo group received placebo tablets without salacinol. The study period was from November 1 to December 4, 2018.
Study Participants
We recruited healthy adults aged 55–70 years through local bulletin-board postings and from members of the Matsumoto Health Lab, a public–private partnership organization that aims to foster a healthy community through resident participation. The recruitment period for this study was from September 1 to October 16, 2018.
Study Allocation
An individual not involved in this study served as the allocation manager and used a stratified permuted block method to generate a random allocation table based on height, weight, age, and sex. Participants were assigned to either the salacinol group or the placebo group. The allocation officer sealed the assignment list and stored it securely. The officer who enrolled and allocated participants to interventions had no access to the random allocation sequence. Participants and outcome assessors were blinded to group assignment, and neither knew whether participants were receiving salacinol or placebo.
Study Criteria
Inclusion and Exclusion Criteria

Test Foods
We prepared the salacia plant extract powder as follows. The trunk and root parts of the S. reticulata plant were dried and chipped. After thorough drying, the chips were placed in hot water for 1 h to facilitate extraction and then removed by filtration. The liquid was then cooled, and the extract was powdered using an ADL-310 spray dryer (Yamato Science Co., Tokyo) and stored at 4°C. The powder consisted of 61% carbohydrates, 17% polyphenols, 12% ash, 5% moisture, 4% protein and 0.6% fat. The salacinol content of the salacia plant extract powder was 4.20 μg/mg; this confirmed that salacinol content and its contribution to α-glucosidase inhibition were higher than those of the other ingredients. For the salacinol group, the test food contained 60.00 mg S. reticulata extract, 6.00 mg of calcium carbonate, 172.75 mg of crystalline cellulose, 7.50 mg of sucrose fatty acid ester and 3.75 mg of silicon dioxide per 250 mg. For the placebo group, the test food contained 175.00 mg of crystalline cellulose, 2.50 mg of silicon dioxide, 50.00 mg of erythritol, 2.50 mg of calcium stearate, and 20.00 mg of color adjuster per 250 mg. Aliment Industry Co. (Yamanashi, Japan) produced the test foods. Japan Food Research Laboratories (Ibaraki, Japan) analyzed the components of salacia powder and the test foods, and the salacinol content was confirmed by liquid chromatography–mass spectrometry.
We prepared tablets containing 0.25 mg of salacinol for the salacinol group and administered them according to the following schedule: 1 tablet before breakfast, 1 tablet before lunch, and 2 tablets before dinner, for a total daily salacinol dose of 1 mg. In determining the salacinol dosage, we referred to a previous study that evaluated changes in the intestinal microbiota after salacinol intake, because the production of putrefactive products is associated with alterations in the intestinal microbiota. Since a previous study in healthy adults (15 participants per group) showed changes in the intestinal microbiota at the same salacinol dose as in the present study [20], we selected this dose to evaluate its effects on stool putrefactive products and intestinal function. The placebo group followed the same schedule. Excipients that did not affect the intestinal environment were used for tablet manufacturing, along with color and flavor modifiers in the placebo. The test foods were indistinguishable in appearance, taste, and color.
Outcome Measures
The primary outcomes were stool pH, stool water content, subjective stool odor score using a 5-point scale (1: excellent to 5: very poor), and stool putrefactive products, including ammonia, phenols, paracresol, indole, skatole, and 4-ethylphenol. The secondary outcomes were bowel movement frequency, subjective defecation score assessed using a 5-point scale (1: excellent to 5: very poor), and safety assessments. In addition, participants completed a self-administered questionnaire on medication use, carbohydrate intake, and test tablet consumption, all of which could affect the intestinal microbiota or the effects of salacinol.
The following items were assessed via questionnaire at both the beginning and end of the survey period: sex and age (assessed only at baseline), height, weight, allergies, intake of fermented foods, lactic acid bacteria, dietary supplements, alcohol consumption habits, smoking habits, exercise habits, dietary patterns, and carbohydrate intake. The following items were evaluated through a daily questionnaire: tablet intake, carbohydrate intake, subjective stool odor score, and subjective defecation score. No special diets or dietary restrictions were imposed.
Participants were required to maintain a daily diary throughout the study period to record their physical condition, medication use, and any changes in lifestyle. The researchers monitored these diaries to ensure that all participants in both the salacinol and placebo groups maintained their healthy status. To ensure data integrity, participants who showed significant changes in their health or who met the exclusion criteria were excluded from the final analysis.
We defined an adverse event as any unwanted or unintended injury, illness, or related symptom occurring in a study participant, regardless of whether it was causally related to the research. If an adverse event occurred, the principal investigator or co-investigator immediately took appropriate measures, recorded the event in the case report form, and, if necessary, took appropriate action, such as discontinuing the participant’s involvement in the study.
Stool Samples
Before collecting a stool sample, we gave participants the following instructions: (1) Place the special stool collection sheet in the toilet. (2) Scoop the stool into the collection container while preventing contamination from urine. (3) Place the stool in a polystyrene container along with a cooling pack, and record the date and time of collection as well as the intensity of the stool’s odor. (4) Submit the refrigerated stool sample and self-report form promptly.
We collected stool samples before the study began, after 14 days of intake, and on the designated day or the day after the study concluded. The samples were frozen and stored within 24 hours and then analyzed by an external laboratory. We measured stool pH, water content, and levels of putrefactive products (ammonia, phenols, paracresol, indole, skatole, 4-ethylphenol, and the total amount).
Sample Size
We conducted this study as an exploratory investigation to evaluate the preliminary feasibility of salacinol and assess outcome trends. Because of its exploratory nature, we did not perform a formal power analysis to determine the sample size. Instead, we aimed to recruit 30 participants, which we considered sufficient to provide a basis for future larger-scale confirmatory trials and to estimate effect sizes for subsequent power calculations. This sample size was based on a previous randomized placebo-controlled trial showing changes in the gut microbiome and suppression of inflammation with 30 participants. 20
Statistical Analysis
In the basic tabulation, percentages were calculated for qualitative variables, and summary statistics were calculated for quantitative variables. As prespecified, the chi-square test or Fisher’s exact test was used for qualitative variables. In addition, because we considered it important to assess between-group differences and temporal changes in quantitative variables, including test food intake, bowel movement frequency, subjective stool odor score, subjective defecation score, and stool analysis results, we performed post-hoc analysis using the Mann–Whitney U test and the Jonckheere–Terpstra trend test within each group. Statistical analyses were conducted using IBM SPSS Statistics for Windows, version 29 (IBM Corp., Armonk, N.Y., USA). Two-tailed tests were used for comparisons between subjects, and p values less than 0.05 were considered statistically significant. Missing data were excluded from the analysis.
Results
Figure 1 shows the flow diagram of this study. Thirty-nine participants consented to participate in the study; 7 were excluded due to hypertension (n=4), diabetes (n=2), or hyperuricemia (n=1), and 1 withdrew informed consent just before participation. This left 31 participants (15 in the salacinol group and 16 in the placebo group), from whom all necessary data for analysis were collected during the intake period, resulting in a 100% follow-up rate. There was no significant difference in the baseline characteristics between the salacinol and placebo groups. Seven participants (3 in the salacinol group and 4 in the placebo group) were excluded from the analysis because they did not regularly consume carbohydrates at least once a day or met other exclusion criteria. The final analysis included 24 participants (12 in the salacinol group and 12 in the placebo group). There were no serious adverse events in this study. Flow diagram of this study
Characteristics of the Placebo and Salacinol Groups
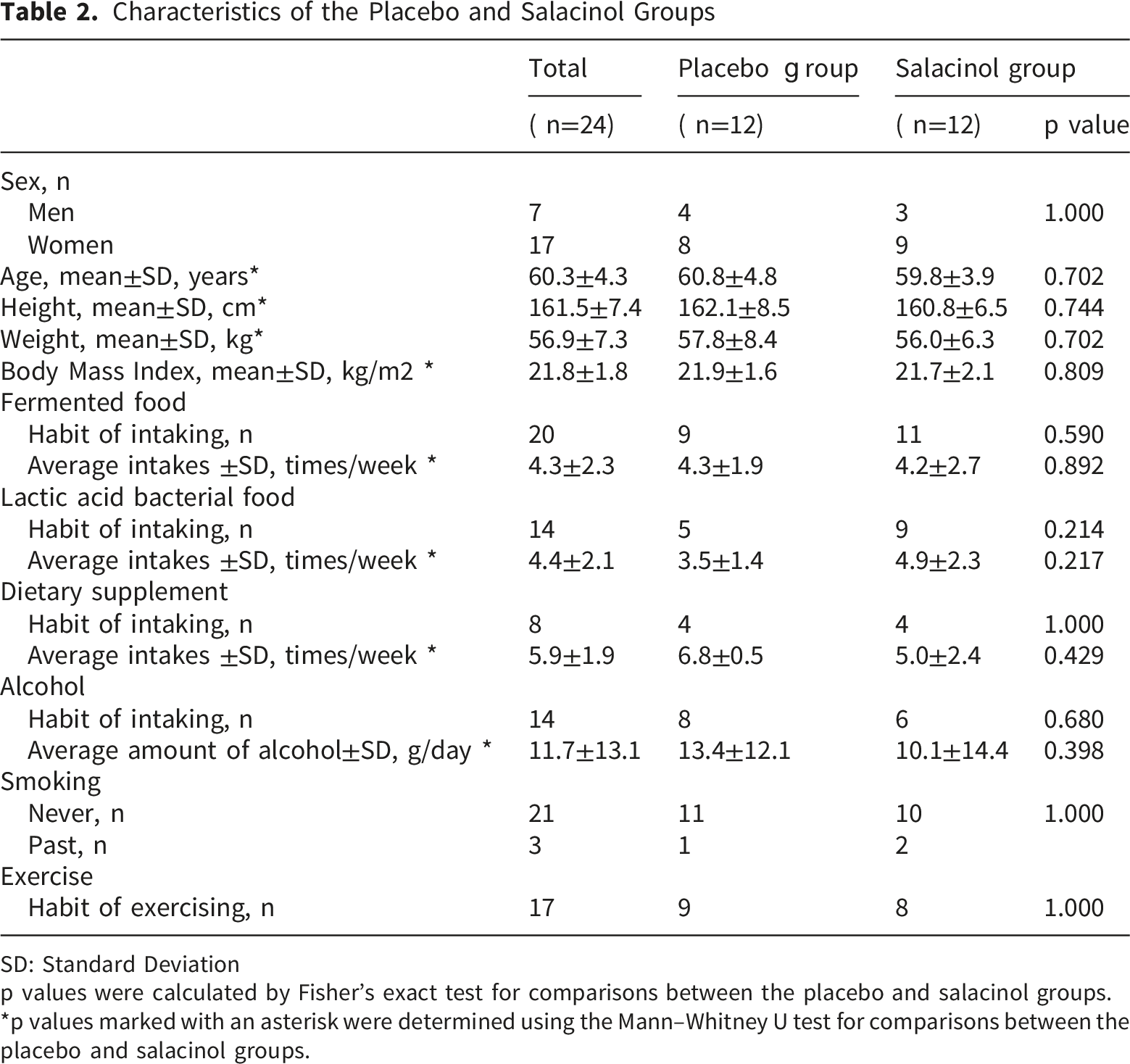
SD: Standard Deviation p values were calculated by Fisher’s exact test for comparisons between the placebo and salacinol groups.
*p values marked with an asterisk were determined using the Mann–Whitney U test for comparisons between the placebo and salacinol groups.
Average of Tablet Intake, Carbohydrate Intake, Bowel Movement Frequency, and Subjective Scores

SD: Standard Deviation p values were calculated using the Mann–Whitney U test or Fisher’s exact test for comparisons between the placebo and salacinol groups. p for trend:The Jonckheere–Terpstra test was performed in each group.
Stool Analysis in the Placebo and Salacinol Groups
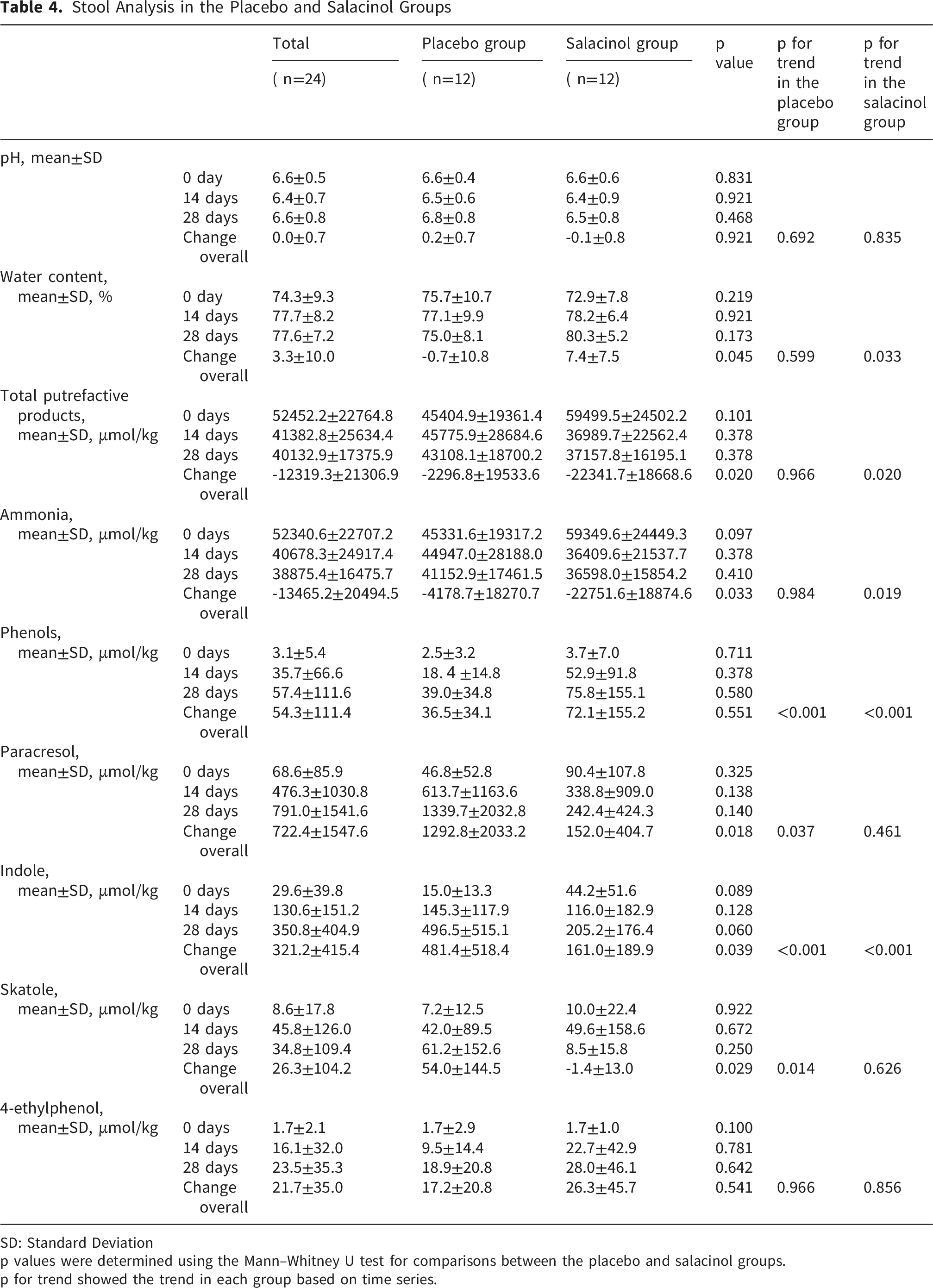
SD: Standard Deviation p values were determined using the Mann–Whitney U test for comparisons between the placebo and salacinol groups. p for trend showed the trend in each group based on time series.
Discussion
A daily intake of 1 mg of salacinol for 28 days significantly reduced total stool putrefactive products and stool ammonia levels in the salacinol group compared to the placebo group. Quantitatively, the mean stool ammonia concentration in the salacinol group decreased by approximately 40% from baseline and differed significantly from that in the placebo group. This effect was maintained from day 14 through day 28. Although stool water content increased notably in the salacinol group compared with the placebo group, stool pH remained unchanged, with no significant difference between the groups. Additionally, bowel movement frequency, subjective stool odor score, and subjective defecation score did not differ significantly between the groups. These results suggest that salacinol may help improve the intestinal environment and may have potential clinical relevance.
The findings obtained in this study are considered to be attributable to the α-glucosidase inhibitory activity of salacinol. Salacinol inhibits the breakdown and absorption of carbohydrates in the upper small intestine through its α-glucosidase inhibitory effect.11,12 As a result, undigested oligosaccharides and monosaccharides reach the large intestine, where they serve as fermentable substrates for gut microbiota. 21 This promotes the proliferation of specific bacterial groups, leading to alterations in the composition and balance of the intestinal microbiota. 22 The α-glucosidase inhibitory activity of salacinol may exert its intestinal modulatory effects through a mechanism distinct from that of probiotics and prebiotics.
The observed reduction in ammonia concentration of stool is likely attributable to the fermentation of undigested carbohydrates that reach the colon as a result of α-glucosidase inhibitor administration. These carbohydrates are metabolized by colonic microbiota, leading to increased production of short-chain fatty acids (SCFAs). The accumulation of SCFAs lowers the colonic pH, thereby suppressing the growth and enzymatic activity of bacteria that produce ammonia. This mechanism is consistent with previous findings linking colonic acidification to reduced ammonia levels of stools.23,24
In addition to reducing ammonia in stool, α-glucosidase inhibitors such as salacinol may increase stool water content. This effect is thought to be due to the osmotic activity of undigested carbohydrates reaching the colon, which helps to retain water within the intestinal lumen. 25 Furthermore, enhanced colonic fermentation and shortened transit time may also contribute to a reduction in water reabsorption and softer stools.
In human studies, administration of the α-glucosidase inhibitor acarbose has been shown to increase SCFA-producing bacteria while suppressing ammonia-producing bacterial populations. 26 Specifically, acarbose has been reported to increase the abundance of Lactobacillus spp., Faecalibacterium prausnitzii, and Prevotella spp. in humans, suggesting enhanced microbial glycolysis and fermentation and increased SCFA production in the colon. 27 In the present study, one participant with frequent diarrhea was excluded from the analysis (Figure 1). Because diarrhea has been reported as a side effect of α-glucosidase inhibitors, 28 we cannot rule out the possibility that salacinol intake contributed to this event. Taken together, these findings indicate that salacinol may exert similar modulatory effects on the gut microbiota.
A major strength of this study is its design as a double-blind, randomized controlled trial involving human participants. This approach minimizes bias and ensures a high level of evidence in clinical research. The study also evaluated parameters—specifically putrefactive products, moisture content, and pH—that are presumed to reflect changes in the gut microbiota. Furthermore, the effects of salacinol were explained in comparison with previously reported findings on acarbose, a known α-glucosidase inhibitor.
This study has several limitations. First, the number of participants included in the analysis was small (twenty-four), which limits the generalizability of the findings. As an exploratory study, it may not reflect the broader population, and larger studies including more diverse participants are needed to confirm these preliminary results. Second, diet was not standardized among participants. Because putrefactive products are generated during the breakdown of dietary proteins and diet substantially affects the intestinal microbiota, dietary differences may have influenced the results. Although we attempted to minimize this issue by excluding participants with markedly unbalanced diets and by monitoring diet during the study period, some residual dietary imbalance may have remained. These first two limitations, together with individual differences and lifestyle differences, may have increased variability and reduced our ability to detect the true effects of salacinol. Third, selection bias may have been present because the study population consisted of high-conscious individuals, and the findings may therefore not be fully generalizable to the broader population. Finally, we did not directly analyze gut microbiota composition. Although putrefactive products, stool water content, and pH may indirectly reflect changes in the gut microbiota, direct microbiota analysis would allow a more complete assessment of salacinol’s effects on microbial composition.
Conclusion
In conclusion, this exploratory study suggests that salacinol intake regulates intestinal ammonia-containing putrefactive product levels and stool water content through α-glucosidase inhibition. However, because of the small sample size and exploratory design, these findings should be interpreted cautiously as hypothesis-generating. Further large-scale studies are needed to confirm these effects.
Footnotes
Acknowledgements
The authors wish to thank all participants and the relevant institutions for their cooperation in this study.
Ethical Considerations
Participants who indicated willingness to enroll were provided with a full explanation of the study protocol, after which written informed consent was obtained. Our study was CONSORT compliant and well conducted. Participants who indicated willingness to enroll were provided with a full explanation of the study protocol, after which written informed consent was obtained. Our study adhered to the “Ethical Guidelines for Epidemiological Surveys” and the “Ethical Guidelines for Clinical Research.” The methods and measurement items were examined and approved by the Medical Ethics Committee of Shinshu University School of Medicine (#4132) and the Fujifilm Life Science Ethics Review Committee (#130). We conducted the study with the approval of the ethics review committee with no changes made. We registered this study in the UMIN Clinical Trials Registry under the number UMIN000034522 (![]() . Date of registration: Oct 16, 2018.).
. Date of registration: Oct 16, 2018.).
Consent to Participate
The study protocol was fully explained to participants who wished to participate, and written informed consent was obtained before the study was conducted. We explained to participants that no personally identifiable information would be released, and written consent was obtained for publication.
Author contributions
The authors’ contributions are as follows:
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The grant was received by the authors, M.M, T.T and T.N. The grant number is GAY123. This study has been funded by FUJIFILM Corporation. (![]() ). The funder was involved in the study design and preparation of the manuscript.
). The funder was involved in the study design and preparation of the manuscript.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: This study has been funded by the FUJIFILM Corporation.
Data Availability Statement
The dataset supporting the findings of this study is available at Zenodo. DOI: 10.5281/zenodo.20437220
Trial Registration
Statement of Human and Animal Rights
All procedures in this study were carried out according to the protocol described above. The research was a collaborative effort between Matsumoto City, Shinshu University, and FUJIFILM Corporation.