
Abstract
Objective
To systematically map registered interventional trials of traditional Chinese medicine (TCM) for asthenozoospermia and oligoasthenozoospermia across major international trial registries.
Methods
We systematically searched the Chinese Clinical Trial Registry (ChiCTR), the International Traditional Medicine Clinical Trial Registry (ITMCTR), the European Union Drug Regulating Authorities Clinical Trials Database (EudraCT), the University Hospital Medical Information Network Clinical Trials Registry (UMIN-CTR) and ClinicalTrials.gov from inception to December 31, 2025. We included all clinical trials evaluating TCM interventions (including Chinese herbal medicine, acupuncture, or their combinations) for asthenozoospermia or oligoasthenozoospermia. Two investigators independently screened records, extracted data, and cross-verified results.
Results
A total of 35 eligible trials were identified. Geographically, 32 trials (91.4%) were conducted in China, of which 30 (85.7%) were registered in ChiCTR or ITMCTR. Institutionally, Beijing (15 trials) and Shanghai (5 trials) led the distribution. Annual registrations showed a steady upward trend from 2020. Most trials (33, 94.3%) adopted randomized parallel-group designs, although single-center studies dominated (27 trials, 77.1%). Blinding was severely underreported, particularly among trials registered in ChiCTR and ITMCTR. Chinese herbal formulas/extracts were the most common intervention (25, 71.4%). The target population was predominantly males aged 22–45 years. Most trials (>80%) had planned sample sizes of 60-160 participants. Notably, more than half of the registered trials (19 trials, 54.3%) had not yet started recruitment, and only 4 trials (11.4%) had published protocols or results.
Conclusion
Clinical research on TCM for asthenozoospermia and oligoasthenozoospermia has reached a certain scale, predominantly employing randomized parallel-group designs. However, the evidence base remains geographically concentrated and largely incomplete, highlighting an urgent need to translate registered research into actionable clinical evidence.
Keywords
Introduction
Male infertility is often associated with reduced sperm motility.1,2 This study focuses on asthenozoospermia (isolated low motility with normal count) and oligoasthenozoospermia (low motility plus low count). While assisted reproductive technology (ART) has advanced, it remains costly and invasive. 3 Therefore, safe, effective, and accessible alternatives are of significant value. 4
Traditional Chinese medicine (TCM) has long been used to treat male infertility, particularly for improving sperm quality. Numerous studies suggest that TCM therapies may enhance sperm density, motility, morphology, and DNA integrity.5-9 However, the quality of clinical research is inconsistent, and higher-level systematic evidence is needed to support TCM’s efficacy and safety.10,11
Clinical trial registration improves transparency, reduces publication bias, and avoids duplication. 12 Registries offer a unique window to map the design landscape of ongoing and completed trials before results are formally published. However, no study has comprehensively reviewed registered TCM trials for asthenozoospermia and oligoasthenozoospermia from a global perspective. 13 Thus, it remains unknown whether existing trials have addressed methodological shortcomings (e.g., lack of blinding, small sample sizes, heterogeneous outcomes), or whether new trial designs are needed.
This study reviews registered TCM trials for asthenozoospermia and oligoasthenozoospermia on major global platforms. We depict the overall landscape (temporal trends, geographical distribution, platform characteristics) and analyze trial design, interventions, control types, and outcome measures. We then identify key gaps and provide actionable recommendations to foster high-quality, internationally recognized trials and advance evidence-based TCM.
Methods
This scoping review was conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) checklist. 14 The completed PRISMA-ScR checklist is provided as Supplementary File 1. The protocol was prospectively registered on INPLASY (INPLASY202640028).
Search Strategy
We systematically searched the following databases from inception to December 31, 2025: the Chinese Clinical Trial Registry (ChiCTR), the International Traditional Medicine Clinical Trial Registry (ITMCTR), the European Union Drug Regulating Authorities Clinical Trials Database (EudraCT), the University Hospital Medical Information Network Clinical Trials Registry (UMIN-CTR), and ClinicalTrials.gov. The search strategy used the following terms combined with “OR”: “asthenozoospermia”, “oligozoospermia”, “oligoasthenospermia”, and “oligoasthenozoospermia”. The study type was limited to interventional studies. Two investigators (Chen Z.X. and Jin Z.F.) independently performed the search.
Inclusion Criteria
Registered trials were eligible if they included male participants diagnosed with asthenozoospermia or oligoasthenozoospermia. We did not impose a standardized definition a priori, as our primary objective was to map the existing registered trials and their characteristics. Instead, we accepted the diagnostic criteria as defined by each individual trial protocol, recognizing that diagnostic standards may vary across studies, regions, and time periods. Diagnostic criteria for asthenozoospermia and oligoasthenozoospermia varied across registered trials. The majority of trials adopted thresholds from WHO laboratory manuals (e.g., WHO 2010, 5th edition: <32% progressive motility and <15×106/mL sperm concentration). The intervention or treatment was TCM, including Chinese herbal medicine (decoction, granules, pills, tablets, powder, capsules, extracts, etc.), acupuncture (electroacupuncture) and moxibustion.
Exclusion Criteria
Trials focusing on azoospermia or isolated oligozoospermia (reduced sperm count without impaired motility) were excluded. Trials that exclusively used other forms of complementary and alternative medicine (e.g., yoga, manual therapy, Thai traditional massage) were also excluded.
Data Extraction
Data extraction was performed independently by two investigators (Chen Z.X. and Jin Z.F.) using a standardized form that included: registration number, location, registration date, design type, blinding, age range, sample size, intervention, primary outcome measures, number of centers, and trial status. For each registry entry, we first extracted all available information as directly reported. When critical fields (e.g., blinding method, sample size calculation, diagnostic criteria) were not explicitly stated, we checked the “detailed description” section or any attached study protocols within the registry entry to supplement missing information. If a field remained unmentioned after this process, we recorded it as “not reported (N/A)”. No assumptions were made about missing data. The complete data extraction form is provided as Supplementary File 2.
Statistical Analysis
Characteristics of the Registered Clinical Trials
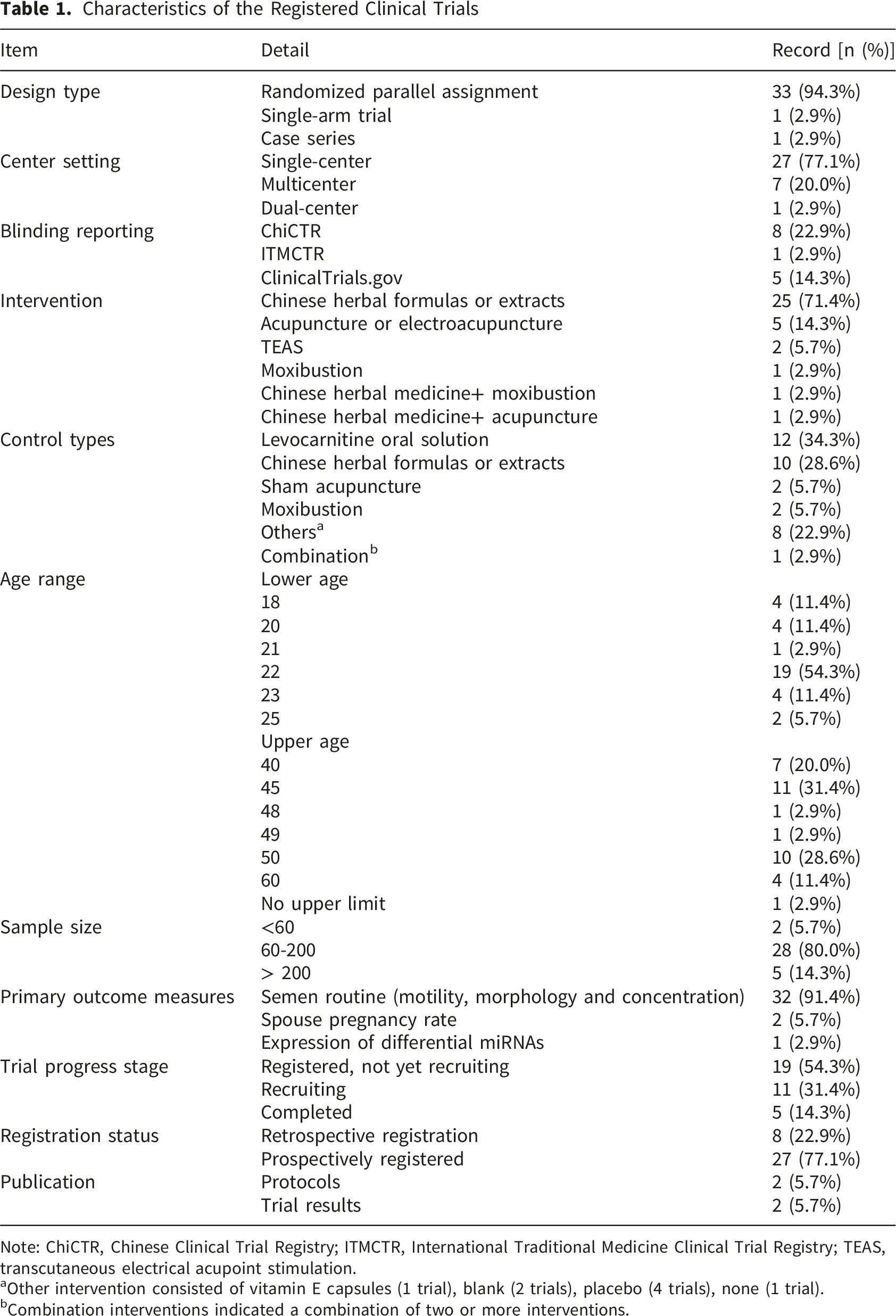
Note: ChiCTR, Chinese Clinical Trial Registry; ITMCTR, International Traditional Medicine Clinical Trial Registry; TEAS, transcutaneous electrical acupoint stimulation.
aOther intervention consisted of vitamin E capsules (1 trial), blank (2 trials), placebo (4 trials), none (1 trial).
bCombination interventions indicated a combination of two or more interventions.
Results
Trial Selection Process
A total of 162 records were retrieved from five registries. After deduplication and screening, 35 trials met the eligibility criteria and were included. The detailed screening process was presented in Figure 1. Flowchart of retrieval of registered clinical trials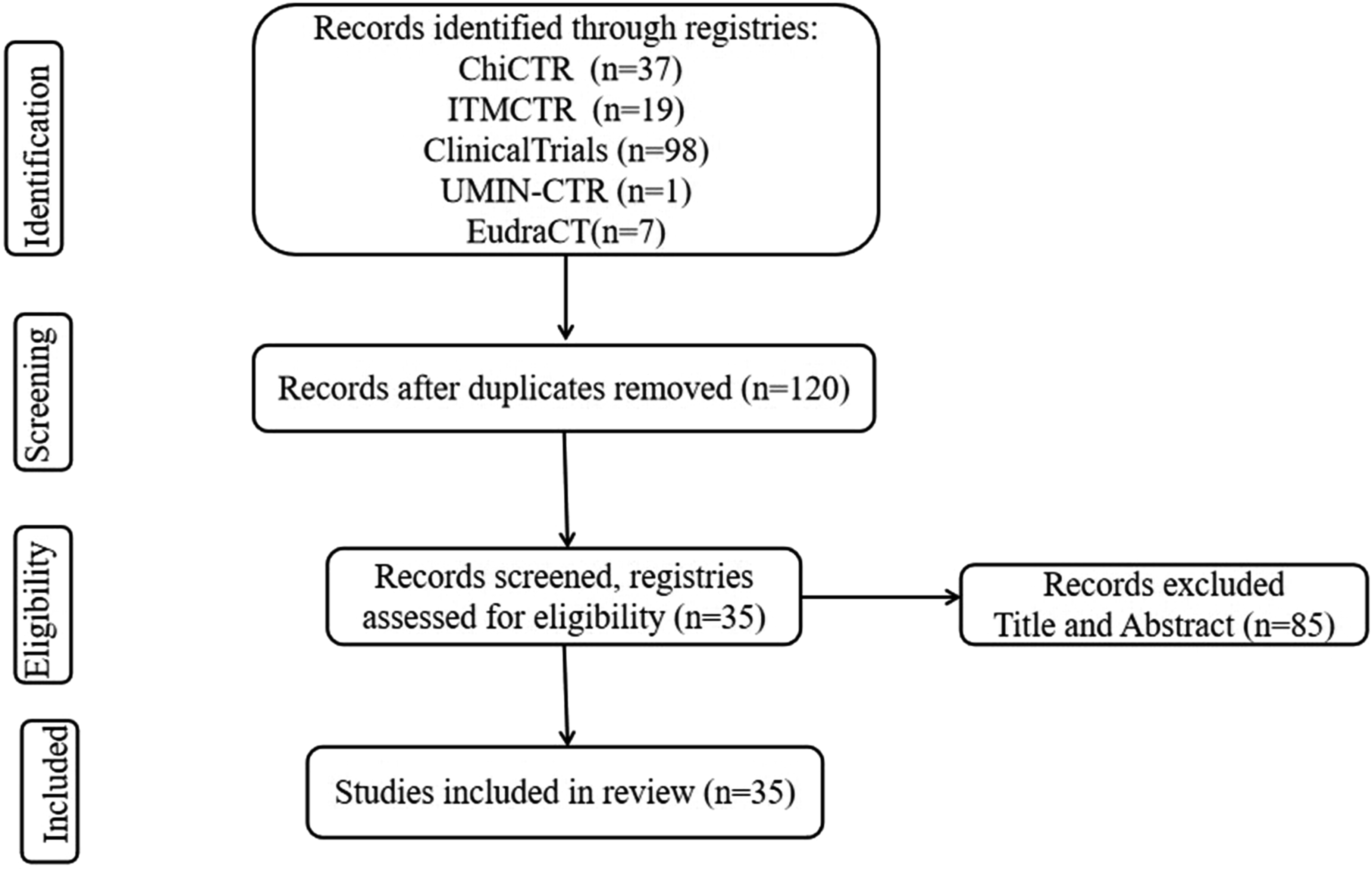
Basic Characteristics of Included Trials
Registry and Geographic Distribution
Table 1 showed the characteristics of the included trials. Among the 35 included trials, 30 trials (85.7%) were registered on Chinese registries (ChiCTR and ITMCTR), and 5 trials (14.3%) on ClinicalTrials.gov. Of these, 32 trials (91.4%) were conducted in China, and 3 trials (8.6%) were international collaborations or conducted in other countries. Domestic trials were geographically concentrated: Beijing (15 trials, 42.9%), Shanghai (5 trials, 14.3%), and Henan and Shandong (3 trials each, 8.6% each). The remaining provinces (Jiangsu, Sichuan, Shanxi, Hubei) accounted for 6 trials (17.1%). Geographic distribution was shown in Figure 2. Geographic distribution of the registered clinical trials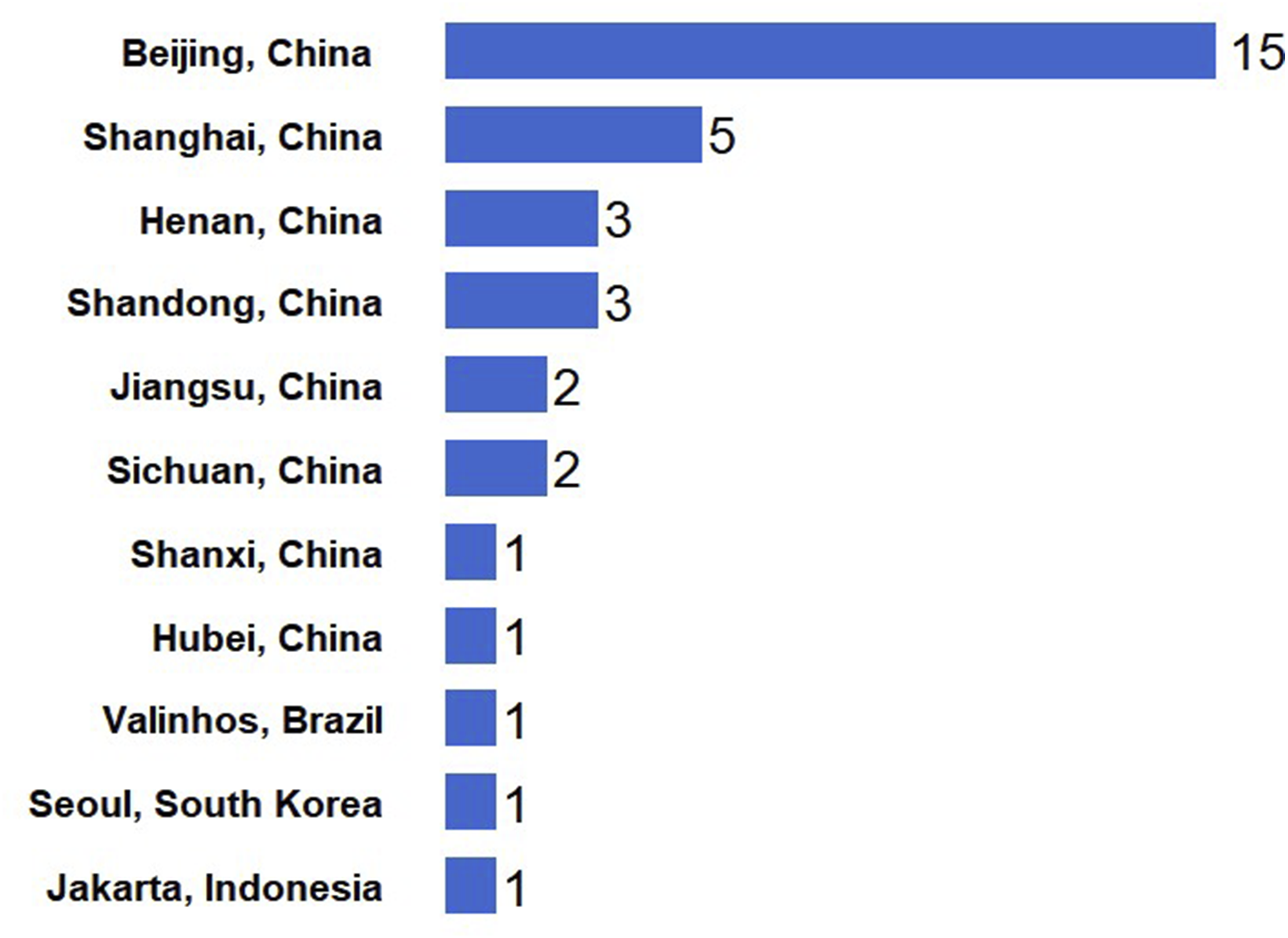
Temporal Trend
The registration dates ranged from 2011 to 2025. The earliest registrations occurred in 2011 (2 trials), with subsequent registrations in 2016 (1 trial), 2017 (1 trial), and 2019 (2 trials). The number of registrations increased from 2020 onward: 2020 (4 trials), 2021 (3 trials), 2022 (3 trials), 2023 (8 trials), 2024 (2 trials), 2025 (9 trials). Temporal trend was shown in Figure 3. Numbers of registered clinical trials from 2011 to 2025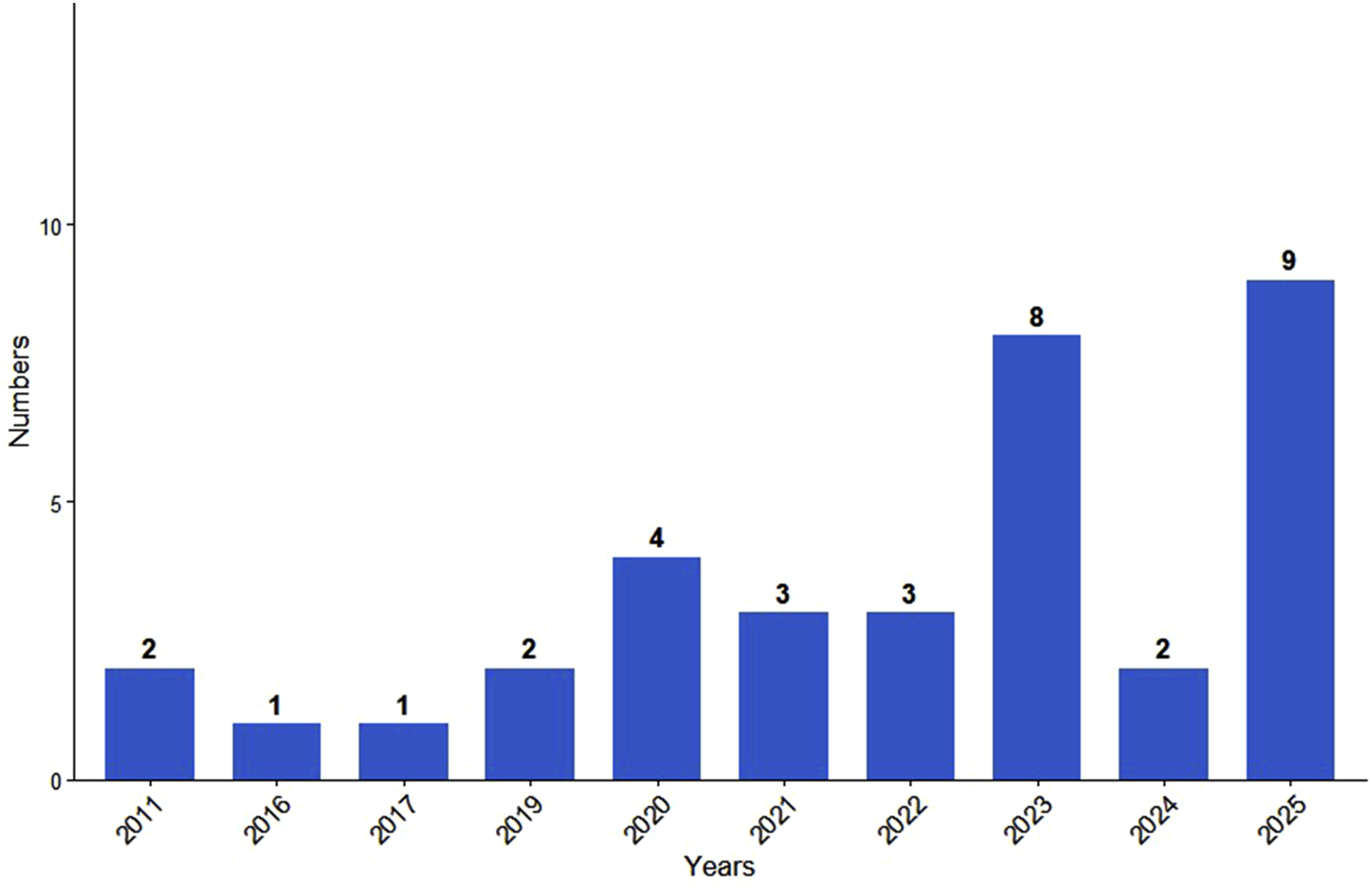
Design Type and Center Setting
The majority of trials (33 trials, 94.3%) employed randomized parallel-group designs. The remaining two trials were non-comparative: one single-arm trial and one case series. Regarding center setting, single-center studies were dominant (27 trials, 77.1%), followed by multicenter studies (7 trials, 20.0%) and dual-center studies (1 trial, 2.9%).
Blinding, Interventions and Primary Outcome Measures
Among trials registered on ChiCTR and ITMCTR, only 9 trials explicitly described their blinding design. All 5 trials registered on ClinicalTrials.gov explicitly described blinding. Chinese herbal formulas or extracts (25 trials, 71.4%) were the most common intervention, followed by acupuncture or electroacupuncture (5 trials, 14.3%). Other interventions included transcutaneous electrical acupoint stimulation (TEAS) (2 trials, 5.7%), moxibustion (1 trial, 2.9%), Chinese herbal medicine combined with acupuncture (1 trial, 2.9%) and Chinese herbal medicine combined with moxibustion (1 trial, 2.9%). Notably, 91.4% of the primary outcomes were semen routine parameters, while only two trials used pregnancy rate as an outcome.
Participant Characteristics and Sample Size
Age Range
The most common lower age limit was 22 years (19 trials, 54.3%). The most frequently set upper age limit was 45 years, adopted by 11 trials (31.4%), followed by 50 years in 10 trials (28.6%).
Sample Size
The mean planned sample size was approximately 124 participants (range: 10-360). Most trials (28 trials, 80%) had a planned sample size of 60-200 participants. Five trials (14.3%) had a sample size exceeding 200 participants.
Trial Status and Output
Trial Progress Stage
Among the 35 registered trials, 19 trials (54.3%) were “registered, not yet recruiting”; 11 trials (31.4%) were “recruiting”; and 5 trials (14.3%) were “completed”.
Registration Status and Publication of Results
Of the 35 trials, 8 trials (22.9%) were retrospectively registered and 27 trials (77.1%) were prospectively registered. Using the registration numbers as search terms in the CNKI and PubMed databases, only 4 trials (11.4%) were found to have published related articles, of which 2 were study protocols and 2 were trial results.
Discussion
This scoping review identified 35 registered trials of TCM for asthenozoospermia and oligoasthenozoospermia. Clinical research in this field has reached an initial scale, with randomized parallel assignment being the predominant design. However, registered trials are geographically concentrated in China, and a substantial proportion remain incomplete or have not reported results. The core bottleneck is the insufficient translation of trial registration into clinical application.
Chinese herbal formulas were the main intervention (>70%), aligning with mainstream TCM practice. Non-pharmacological therapies (e.g., acupuncture) also accounted for a notable proportion, reflecting therapeutic diversity. Future research should report formula composition, dosage, and treatment course in greater detail to enhance reproducibility. 15 Most trials had sample sizes of 60-160 participants, appropriate for exploratory studies, while five trials with more than 200 participants may provide more reliable efficacy estimates.
Prospective randomized parallel-group designs have become mainstream, indicating improved methodological awareness. A prominent issue was the underreporting of blinding. Over two-thirds of trials registered in ChiCTR and ITMCTR did not explicitly describe blinding methods. Inadequate blinding can introduce performance bias (participants modifying behavior based on perceived treatment assignment) and detection bias (outcome assessors influencing measurements). This is particularly problematic when outcome measures include subjective assessments such as sperm motility and morphology. Both biases tend to overestimate treatment effects, with empirical evidence showing that unblinded or inadequately blinded trials yield measurably larger effect sizes compared to properly blinded trials.16,17 This severely compromises the internal validity of the evidence base.
A more critical challenge is the severe “funnel effect” and low output translation. Over half of registered trials remain “not yet recruiting” (54.3%), and only 4 trials (11.4%) have published related articles.18-21 This “recruitment-to-publication gap” results in two forms of evidence waste. First, resources are invested in registered but never initiated trials. Second, completed but unpublished results fail to inform clinical practice or future research, which perpetuates unnecessary duplicate studies and exposes patients to research without generating usable knowledge. Establishing a “registration-implementation-publication” tracking mechanism is essential to overcoming this bias.22,23
Although semen parameters are commonly used as surrogate outcomes in male infertility research, their correlation with patient-centered outcomes such as live birth rate or pregnancy rate remains controversial. Over-reliance on semen parameters may overestimate clinical efficacy. A further source of heterogeneity is the variation in diagnostic criteria for asthenozoospermia and oligoasthenozoospermia across included trials. Although most studies referred to WHO standards, the specific versions adopted varied according to the trial registration date (e.g., 5th or 6th edition). Differing threshold ranges give rise to differing baseline prognoses and treatment responses. Consequently, pooling such heterogeneous trials in future meta-analyses would produce unreliable summary estimates unless subgroup analyses stratified by diagnostic criteria are performed. Future studies should prioritize pregnancy or live birth rate as primary outcomes, adopt standardized reporting of herbal interventions,24,25 and explicitly report diagnostic thresholds using the most recent WHO criteria (currently the 6th edition, 2021).
Several methodological limitations should be acknowledged. First, trial quality varied considerably; many trials, especially those registered in ChiCTR and ITMCTR, did not explicitly describe blinding, which may introduce performance and detection bias. Second, the lack of standardized outcome measures and a core outcome set for TCM trials in male infertility limits cross-study comparability and synthesis. Third, most trials had small sample sizes (60-160 participants), limiting statistical power and generalizability. These gaps should be addressed in future research to strengthen the evidence base for TCM interventions. Finally, diagnostic criteria for asthenozoospermia and oligoasthenozoospermia varied substantially across trials, limiting direct comparisons and complicating future meta-analyses. Researchers are encouraged to adopt the most recent WHO criteria to standardize future studies.
In addition to these evidence-level limitations, several review-level limitations should be acknowledged. This scoping review did not formally assess the methodological quality or risk of bias of the included registered trials, consistent with PRISMA-ScR guidelines (quality assessment is optional). However, the lack of quality appraisal means that the completeness and accuracy of individual registry entries were not systematically evaluated. Our search was limited to major Chinese and English trial registries and did not include unpublished or non-Chinese/English grey literature, which may have introduced publication bias. Also, we did not impose a standardized definition of asthenozoospermia or oligoasthenozoospermia for trial inclusion. As a result, included trials may have used different diagnostic thresholds or may not have reported their criteria explicitly. This heterogeneity limits comparability and generalizability. Future systematic reviews should consider applying standardized diagnostic criteria (e.g., WHO criteria) when selecting trials.
To address the issues identified in this review, we propose three feasible measures. First, we recommend adopting a minimum reporting standard for TCM infertility trials that requires explicit specification of: (a) blinding methods (e.g., triple-blind with centralized outcome assessment); (b) sample size calculation, including effect size assumptions and statistical power; and (c) WHO-based diagnostic criteria, with the edition and thresholds reported. We recommend following the CONSORT statement extension for non-pharmacologic interventions and TCM-specific reporting guidelines. 26 Second, a core outcome set for TCM male infertility research should be developed through a formal Delphi consensus process involving clinicians, researchers, and patient representatives. The core outcome set should include at least one patient-centered outcome (e.g., clinical pregnancy rate or live birth rate) alongside standard semen parameters. 27 Third, researchers should shift from small single-center studies to adequately powered multicenter trials. Specifically, we propose a pragmatic multicenter randomized trial with 200-300 participants across 4-6 geographically diverse sites in China, comparing a standardized TCM regimen (fixed formula or acupuncture protocol) with an active control (e.g., conventional Western medicine) or placebo. This design would enable subgroup analyses by region and severity, improve generalizability, and provide high-level evidence acceptable to international regulatory bodies. Collectively, these steps would substantially improve evidence quality and accelerate the translation of TCM research into clinical practice guidelines.
Conclusion
This scoping review systematically mapped the interventional trials of TCM for asthenozoospermia and oligoasthenozoospermia registered on major trial platforms (ChiCTR, ITMCTR, and ClinicalTrials.gov). The findings indicate that clinical research in this field has reached an initial scale, with randomized parallel-group design being the predominant type. However, the registered trials are geographically highly concentrated, and a substantial proportion remain incomplete or have not reported their results, which severely limits the completeness and transparency of the evidence base. Consequently, the core bottleneck is the insufficient translation of research registration into clinical application. Future research should focus on promoting mandatory prospective registration and result reporting, facilitating multicenter and cross-regional international collaboration, and developing standardized diagnostic criteria and core outcome sets to accelerate the translation of high-quality evidence into clinical practice guidelines.
Supplemental Material
Supplemental Material - Traditional Chinese Medicine for Asthenozoospermia and Oligoasthenozoospermia: A Scoping Review of Registered Intervention Trials in Major Trial Registries
Supplemental material for Traditional Chinese Medicine for Asthenozoospermia and Oligoasthenozoospermia: A Scoping Review of Registered Intervention Trials in Major Trial Registries by CaiYuZhu Wen, ZhiXu Chen, ZhenFei Jin, LiNa Zhao, YaFei Liu and JianShe Chen in Natural Product Communications.
Supplemental Material
Supplemental Material - Traditional Chinese Medicine for Asthenozoospermia and Oligoasthenozoospermia: A Scoping Review of Registered Intervention Trials in Major Trial Registries
Supplemental material for Traditional Chinese Medicine for Asthenozoospermia and Oligoasthenozoospermia: A Scoping Review of Registered Intervention Trials in Major Trial Registries by CaiYuZhu Wen, ZhiXu Chen, ZhenFei Jin, LiNa Zhao, YaFei Liu and JianShe Chen in Natural Product Communications.
Footnotes
Author Contributions
CaiYuZhu Wen conceived the manuscript idea. ZhiXu Chen and ZhenFei Jin filtered the articles and performed data extraction. LiNa Zhao and YaFei Liu analyzed the data and completed the graphs. JianShe Chen provided a critical version of the manuscript. All authors contributed to the revision of the manuscript and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was supported by Jointly Established Research Project of Traditional Chinese Medicine Scientific Research Special Project in Henan Province (2025LHZX2008).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.