
Abstract
Keywords
Introduction
An estimated 15 million infants are born prematurely every year and preterm birth is a major cause of morbidities and mortality during the first 5 years of life.1,2 Importantly, the main causes of global neonatal mortality are highly remediable, particularly respiratory distress syndrome. 3 Indeed, it is estimated that hospital care of small and sick infants can prevent ∼750,000 deaths per year and require simple therapies such as continuous positive airway pressure (CPAP), which can further reduce mortality even in infants born with birth weight between 500 g and 1.8 kg.3–5 Several methods to provide CPAP are widely available but a persistent problem in low-middle income countries (LMIC) is the use of low-cost systems without proper gas conditioning. In highly industrialized areas this problem has been efficiently solved by the systematic use of heater-humidifiers with closed-loop control of temperature & relative humidity of mixed gases and wired-heated circuits.
Under normal circumstances, the upper airway and respiratory tract are responsible for humidification and heating of the inspired air. 6 In patients receiving invasive mechanical ventilation via endotracheal tube this physiological process is impossible, making artificial heating and humidification of medical gases a standard of care. During non-invasive respiratory support, the upper airway is not totally by passed as the gas is offered at the nasal area. However, neonates have narrow nostrils and nasal fossae, with the first centimeter of the nasal cavity playing a main role on thermal conditioning by warming 66% of the air. 7 Consequently, the administration of cold and dry medical gases at high flow rates (5–12 lpm) in this area, may damage the nasal mucosa epithelium leading to increased nasal bleeding. Inadequate humidification may lead to ciliary dysfunction, inflammation and necrosis of the pulmonary epithelium, dried secretions, atelectasis, bacterial infiltration and/or pneumonia. 7 Hence, gas conditioning is also recommended during non-invasive support by adjusting the heater temperature to provide a gas at 36.5–37°C and by maintaining proper water level of the humidifier.7,8 Unfortunately, closed-loop control of temperature & relative humidity and wired-heated circuits are expensive and not available in our unit. Consequently, a high rate of nasal bleeding during non-invasive support was noted in preterm infants receiving non-invasive respiratory support. Thus, a policy for manual close control of gas temperature & relative humidity (T&RH) was developed and implemented. The main objective of this study was to assess the impact of this intervention on rates of nasal bleeding.
Methods
A single center retrospective study including all preterm neonates (<37 weeks) admitted to our unit between June 2019 and June 2020 and managed with non-invasive respiratory support during hospitalization was conducted. A policy for close control of gas T&RH was implemented in Dec 2019 to be used in any patient receiving non-invasive respiratory support. Therefore, two groups of infants were selected for analysis based on how medical gases were offered: no T&RH control and close T&RH control. Infants never submitted to non-invasive respiratory support were excluded. The study was approved by the Ethics Committee of the Institution (CAAE: 33747320.9.0000.5305) and followed the resolution 466/2012 of the Brazilian Health Care Council.
Intervention (policy for close T&RH control)
During the study period, T&RH of the gas mixture was provided with the use of 2 devices produced in Brazil: Misty 3 (Intermed®, São Paulo - Brazil) and GT-5000 (Globaltec Med, São Paulo, Brazil). Before the new policy, temperature of the gas was not checked, and the heater was set at the number 2 constantly, without any change during the therapy (Figures 1(a) and (c)). The new policy included a close control of the gas temperature by starting with the heater set at number 3 (Figures 1(b) and (d)) and adjusted based on intermittent checking of the gas temperature (every 6 h), which was performed with a water resistant thermometer (G-Tech, TH1027) using an operating temperature range of 32.0°C–42.9°C (precision of +/− 0.2°C) and indication of “low” or “high” for temperatures below or above the range. The thermometer is approved by Brazilian Health Regulatory Agency and The National Institute of Metrology, Standardization, and Industrial Quality. It was inserted into the inspiratory limb of the circuit (Figure 2) and has a reading time of 1 minute for the display of the temperature. The target temperature of the gas mixture was between 36.5°C and 37°C, i.e., close to body temperature to prevent heat loss and nasal mucosal damage.
8
Before the policy, humidity was not controlled, and the water level was checked randomly. After, humidity was closely controlled by checking and adjusting the water level of the humidifier every 6 h and for the presence of circuit condensation. All nurses and respiratory therapists were trained in the new policy during a period of 1 month prior to its implementation. Training consisted of awareness of all details of the policy including starting the humidifier using the correct set levels, constant checking of water levels and condensation, and measurements of temperature of the gas at the interface level. KS assured that all professionals working at the NICU were trained and familiar with the policy before its final implementation. Physicians were also made aware of the policy and supported its implementation. Heater and humidifiers used and the set levels. Legend: (a) and (c) display the set temperature of the two humidifiers before close the T&RH control policy. Note that the temperature was set at numbers two or three without any change during therapy. (b) and (d) show the same humidifiers set temperature during close T&RH control; note that the required set levels to achieve the target air temperature of 37°C were only achieved at numbers 8 and 10, respectively. Temperature control during non-invasive respiratory support. Legend: Close control of the gas mixture temperature was achieved by intermittent checking with a thermometer inserted on the inspiratory limb of the circuit, close to the patient. The target temperature was between 36.5°C and 37°C.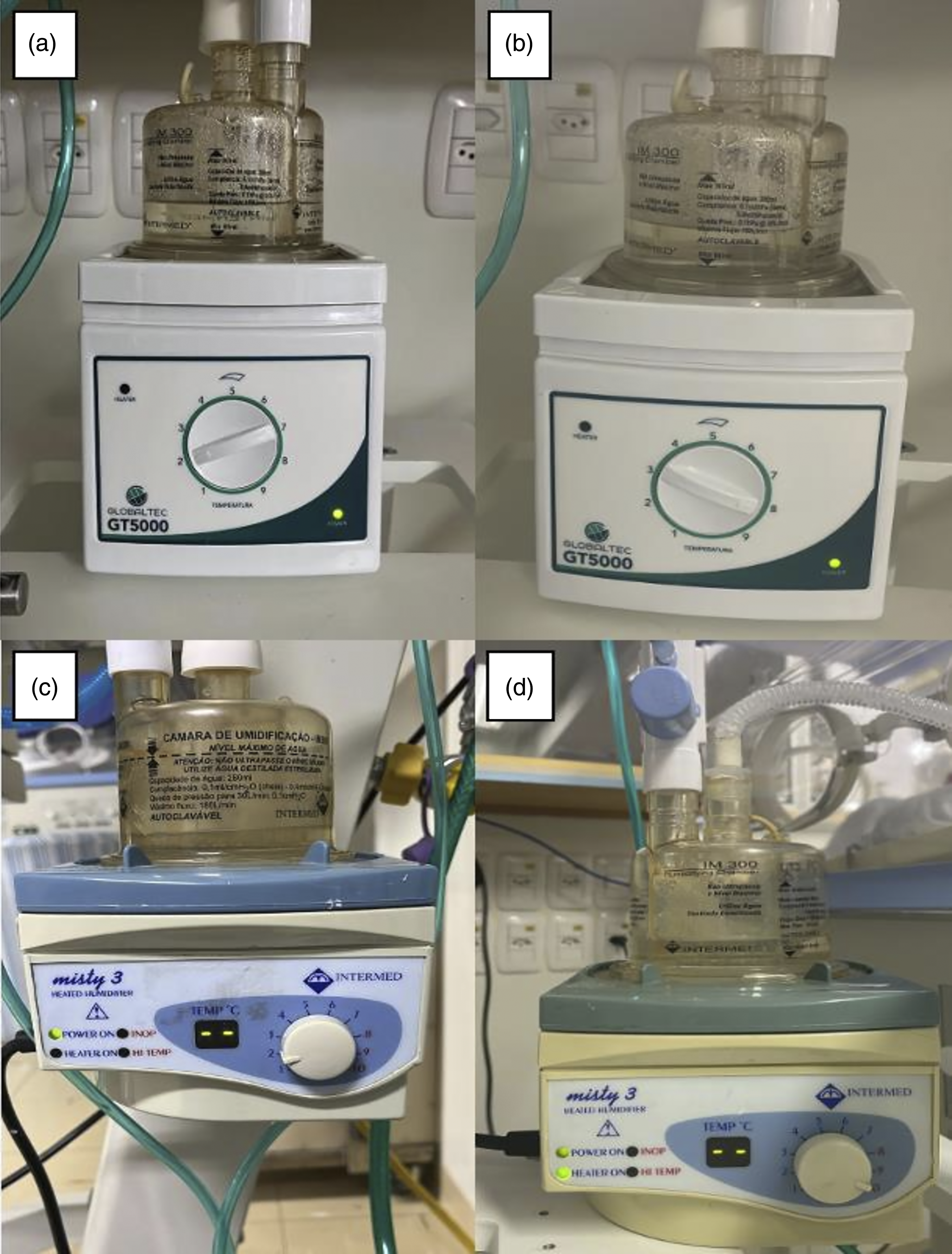

Respiratory management
Non-invasive respiratory support was initiated in infants with respiratory distress, frequent episodes of apnea (>6 episodes/6h), severe apnea requiring bag & mask ventilation, or after extubation from MV. This was provided by using either the bubble (Babypap 150-S, Fanen, Sao Paulo, Brazil) or ventilator CPAP systems (Servo-I; Maquet Critical Care AB, Solna, Sweden) or NIPPV (Servo-I, Maquet Critical Care AB, Solna, Sweden) with nasal masks as the interface (Miniflow Neonatal, Medin Medical Innovations GmbH, Olching, Germany). All attempts were made to fix the masks tightly to promote optimal sealing and prevent leaks. Nasal suction was done by nurses and/or RTs when secretions were noted or suspected, using a 6 or 8 Fr PVC catheter (Mark Med Inc., São Paulo, Brazil) and a wall mounted suction source at a pressure of −50 mmHg. If secretions were deemed thick, normal saline solution was instilled during the suction to facilitate removal. As suction equipment and technique can influence the risk of damage, the procedure was not changed after the T&RH policy implementation. Non-invasive support was discontinued in infants receiving 21% O2 at a corrected gestational age between 31 and 32 weeks and body weight >1000 g, or if the presence of an important nasal injury or abdominal distention affecting progression of the enteral feeds.
CPAP or NIPPV failure was defined: (a) consistent increase in oxygen requirement >50% or (b) PCO2 > 65 mmHg with a pH < 7.20 in two consecutive blood gases, (c) 1–2 episodes of apnea requiring bag and mask ventilation, and (d) frequent episodes of apnea and/or bradycardia (>6 episodes in 6 h). Apnea was defined as a respiratory pause longer than 20 seconds, or less if associated with desaturation (SpO2 < 88%) and/or bradycardia (<100 bpm). If any of these criteria were present the non-invasive support was escalated from CPAP to NIPPV or from NIPPV to MV.
Data collection
A pre-defined data collection form was used for extraction of the following data: admission date, gender, gestational age, birth weight, admission diagnosis, length (days) of CPAP and nasal intermittent positive pressure ventilation (NIPPV) use, adherence to the close T&H control policy, nasal bleeding, need to change the mode of respiratory support from CPAP to NIPPV or need of intubation and MV.
Primary outcome
The primary outcome was the occurrence of nasal bleeding. Nasal bleeding was defined as the presence of any pink or red secretions spontaneously or during suction, and all episodes were recorded.
Secondary outcomes
Adherence to the close T&RH control policy, duration of all modes of respiratory support, and the association between nasal bleeding with the need to change the mode of respiratory support and need of intubation were also recorded. A change was considered if infants at a maximum CPAP level of 8 cm H2O were changed to NIPPV or intubated. A change on the mode of respiratory support was always recorded on the medical chart and decided at the discretion of the medical team. As for the nasal suction, this approach was also the same during the 2 periods. Endotracheal intubation and MV was indicated in the presence of one of the following: (a) Severe apnea requiring positive pressure ventilation; (b) Multiple episodes of apnea: >6 within 6 h; (c) Hypoxemia: FiO2 >50% to maintain SpO2 >88%; (d) Hypercapnia: PCO2 (partial pressure of carbon dioxide) >60 with pH <7.25, and (e) Excessive work of breathing with severe retractions.
Sample size and statistical analysis
Based on a rate of nasal bleeding in our unit of 30% and hypothesizing a clinically relevant decrease to 10% with the implementation of close the T&RH control policy, a sample size of 59 infants on each group were estimated to obtain a power of 80% with a confidence level of 95%. Categorical variables are expressed as counts and percentages and continuous variables as mean ± standard deviation (SD) or median (confidence intervals). Results were compared between groups of infants managed with or without the close T&RH control policy by using the Chi-square test and the Fischer exact test for categorical variables and the Student t-test for continuous variables. Statistical analysis was performed using the software Stata/MP 16.1 (StataCorp, College Station, TX, USA). A p value <0.05 was considered as statistically significant.
Results
Population characteristics.
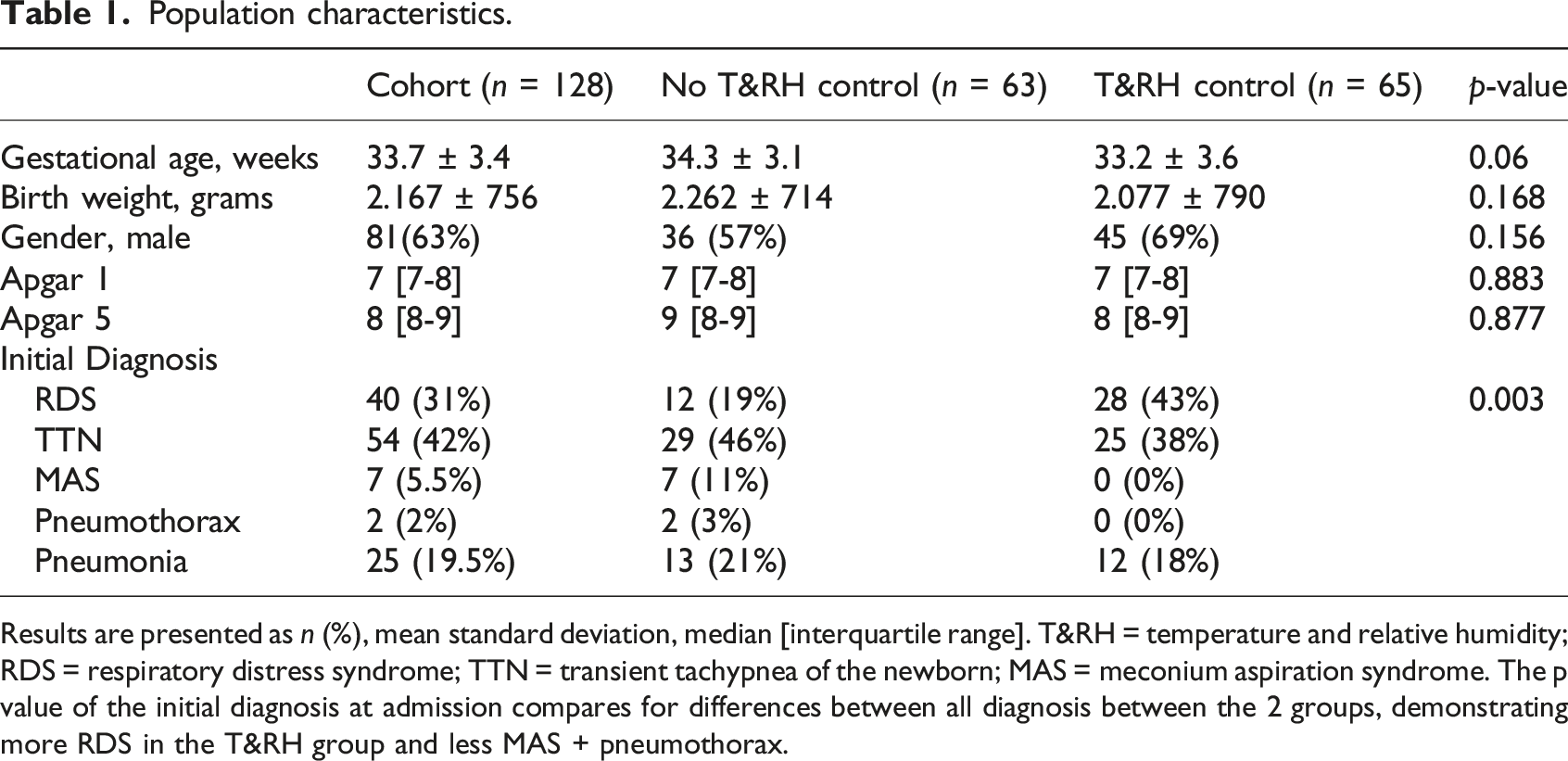
Results are presented as n (%), mean standard deviation, median [interquartile range]. T&RH = temperature and relative humidity; RDS = respiratory distress syndrome; TTN = transient tachypnea of the newborn; MAS = meconium aspiration syndrome. The p value of the initial diagnosis at admission compares for differences between all diagnosis between the 2 groups, demonstrating more RDS in the T&RH group and less MAS + pneumothorax.
Primary outcome
Primary and secondary outcomes.

Results are presented as n (%). T&RH = temperature and relative humidity.
Respiratory management.
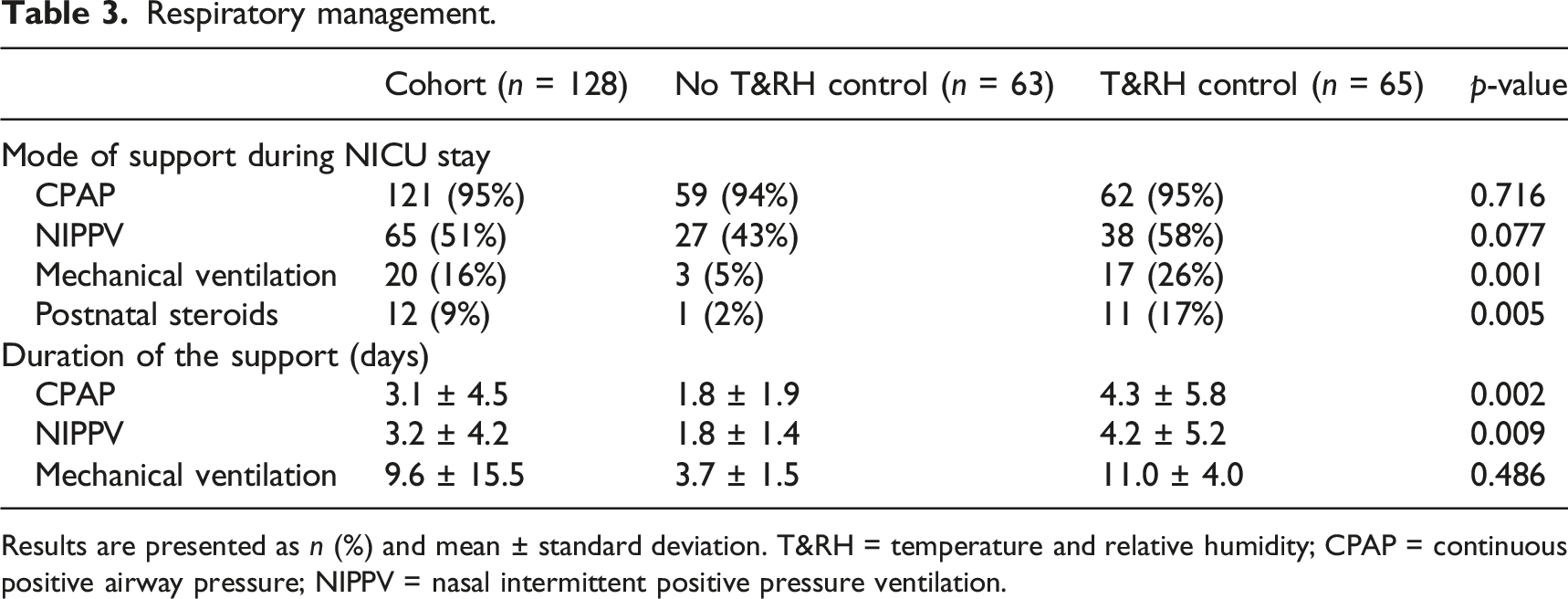
Results are presented as n (%) and mean ± standard deviation. T&RH = temperature and relative humidity; CPAP = continuous positive airway pressure; NIPPV = nasal intermittent positive pressure ventilation.
Secondary outcomes
After the policy implementation five infants were not managed with the T&RH control by the treating team, making an overall adherence to the protocol of 93%. These five infants were admitted closely after the policy implementation and had similar BW and GA as the infants treated with the policy. All five infants did not have the temperature checked and in one the water level was not checked. The following 59 consecutive admissions had 100% adherence to the protocol. The need for change of the original mode of respiratory support also decreased significantly with the close T&RH control (14% vs 3%; p = 0.024). No difference was noted for the need to intubate because of nasal bleeding, which was overall very low.
Discussion
In this retrospective study, the successful implementation of a close T&RH control policy during non-invasive respiratory support had a positive and significant impact on short-term outcomes of very and late preterm infants. Indeed, this simple and low-cost intervention was associated with a 60% drop on the rates of nasal bleeding (from 30% to 14%; p = 0.026), 80% decrease on the need to change the original non-invasive support mode (from 14% to 3%; 0.024), and no need of endotracheal intubation secondary to nasal bleeding. In LMIC, the successful use of non-invasive respiratory support has been demonstrated to reduce the need for mechanical ventilation without an increase in mortality. 9 The low certainty of evidence for decreased mortality and adverse events seems to be dependent on the environment and hospitals must optimize safety, numbers of staff trained, promote close monitoring and supervision, and use equipment that is suitable and accessible. 10
During the use of non-invasive respiratory support the upper airway is anatomically not “bypassed”, but the prolonged and repeated exposure of the mucosa to inadequately heated and humidified gas at high flow rates (5–12 lpm) may dry out the epithelial surface of the nasopharyngeal cavity affecting the mucociliary transport system.11,12 Dry inspired gas stimulates a cascade of events such as changes on the viscosity gradient, mucus dehydration, and cilia beat frequency. Moreover, after 3 hours of exposure it may lead to permanent interruption of cilia activity with consequent inflammation, sloughing of the mucosa and nasal bleeding. 13 In a study in Malawi, the efficacy of a low cost bCPAP without a heater and humidifier (H&H) was evaluated on 54 neonates born at gestational age similar to our study. 14 Because there was no H&H, nursing care included the use of sterile nasal saline drops every 4 hours to reduce mucosal drying, and low flow rates (typically between 1 and 2 L/min). Nevertheless, 11% of the infants had mild nasal bleeding. Standards on minimum required levels of inspired gas humidity during artificially supported respiration have been published. 15 More recently, the International Organization for Standardization (ISO) specified 12 mg H2O/L as the minimum level of humidification required during non-invasive respiratory support. 16 Specifications for the neonatal age group have not been issued but much higher humidity levels, close to 44 mg H2O/L at body temperature (36.5°C), is recommended. 17 Noticeably, this may lead to condensation and accumulation of water inside an unheated circuit which is a sign of proper humidification and should not lead into reduction of the temperature. Rainout, however, should be avoided by close monitoring and water drainage, as condensate may become contaminated or be flushed down the upper airways with risks of water aspiration. The opinions of health care providers on barriers to implement a non-invasive respiratory support system (bCPAP) have been reported.18,19 All-inclusive and comprehensive training were factors identified as facilitators. In our study, training on the use of a strict T&RH policy led to a 93% adherence and clinical improvements.
In a small single center trial, infants with birthweight <2,500 g and a gestational age of <37 weeks received CPAP or NIPPV with nasal prongs. 20 Nose bleeding was defined as blood in the cavity causing obstruction and occurred in 12.5% of infants treated with CPAP and none with NIPPV. The control of the T&RH used on both modes of support was not described. In a convenience sample study in Malawi, 62 infants with average birth weight of 1.370 g were treated with a low cost bCPAP system for an average of 6.9 days. The system did not have a H&H and normal saline drops were instilled by the nurses in the nostrils every 2–4 hours. Mild epistaxis was reported in 11% of the cases. 21 In a randomized control trial in Tanzania, 48 infants with a mean gestational age of 33 weeks were treated with oxygen via nasal cannula (n = 23) or the Pumani bCPAP system® (n = 25); a system also without H&H. 22 Despite normal saline drops were instilled in the nostrils every 2–4 hours, rates of nasal bleeding were 40%. In our center, infants treated with the close T&RH control policy had rates of nasal bleeding of 14%, which was significantly lower than before the policy, and similar to studies using H&H. Certainly, mucosal edema, secretions, or bleeding may create airway obstruction, which is more serious in newborns as they are obligate nose breathers with a small cross-sectional diameter of the nares, responsible for up to 50% of total lung resistance. Therefore, even partial nasal obstruction can significantly increase work of breathing, decrease tidal and minute ventilation, causing episodes of apnea leading to therapy failure. Importantly, after the implementation of the policy, changes on the original mode of respiratory support significantly due to bleeding causing obstruction decreased from 14% to 3%, and no infant required intubation.
Due to financial constrains the equipment used for H&H of the medical gases in the unit had important limitations. The circuits did not have a temperature probe (close-loop system) and were not wired. Therefore, it was no possible to continuously monitor the gas temperature close to the patient and the circuit was prone to condensation. The Globaltec GT 5000 does not have a display to monitor gas temperature and adjustments are done by turning a knob with numbers going from 1 to 9. The Misty 3 also has a knob that goes from 1 to 10 but can display the temperature if used with the circuit with a temperature sensor, which was not available due to the costs (Figure 2). To overcome these issues, we performed a few measurements of gas temperature using a simple digital thermometer inserted close to the patient. After a few trials we realized that heating should be initiated at a minimum level of 3 for both systems but frequent adjustments up to 8-10 based on manual temperature measurements performed each 6 h (Figure 1) were required.
The study has some limitations. This was a single center experience including very or late preterm infants, a population under lower risk of nasal injury when compared to smaller and more immature infants. The retrospective nature design might have affected the results as they depend on review of charts and some information is inevitable missing. Also, the study populations are not completely balanced. In the T&RH control group patients were sicker than the group without T&RH control, stayed longer on non-invasive support, and had a higher use of MV and postnatal steroids. For the primary outcome of the study, this would probably increase their chances of nasal bleeding, but our findings were the opposite, reinforcing the message of the beneficial effect of the new policy. We did not measure RH which was assessed by the presence of condensation of the system during the T&RH period. Furthermore, temperature measurements relied on manual checks instead of continuous monitoring which was not possible given the available technology. We recognize that the presence of pink or red secretions is somewhat subjective to assess nasal bleeding. However, this was the assessment used prior to the policy implementation and given the retrospective nature of the study, the only information available for comparisons. Therefore, readers need to carefully interpret the results. Nevertheless, a simple and low-cost T&RH control policy is important for LMIC countries given the constraints of the devices available. Apart from preventing nasal bleeding, heated and humidified gases can also help on body temperature maintenance, especially when high gas flow rates are being used. A large number of preterm infants were included with good adherence to the intervention and a significant clinical impact on important outcomes. Therefore, other centers challenged with similar problems with their T&RH systems might benefit from our experience. Thus, in adverse situations where the equipment available has limitations for the provision of adequate temperature and RH control some interventions are recommended on Box 1.
Test the available devices for the delivery of adequate gas temperature and RH at the patient level, i.e., close to the nares. The air temperature checking can be done by using a simple thermometer inserted in the inspiratory limb of the system, close to the patient interface. If air temperature <36°C, the temperature of the gas mixture offered is low and can damage the nasal mucosa causing nasal bleeding. In this case, increase the temperature of the available device until the gas temperature reaches 36.5–37°C. Annotate the knob position of the device that provides this gas temperature to always start the system at this position. During the use on non-respiratory support check the temperature at each care. Usually this is done every 4–6 h. If the circuit is not wired be sure there is water condensation. The absence of water condensation is a sign of inadequate temperature/humidity. If there is condensation, as water in the system may create pressure oscillations or enter the nasal cavity, be sure to drain this water frequently. If too much condensation is ongoing, try to decrease the distance between the humidifier and the patient by placing the system closer to the incubator. By doing that, only a shorter length of the system is outside of the incubator, i.e., exposed to the temperature of the unit (usually 20–22°C). Develop a protocol for the unit highlighting the critical importance of adequate temperature and humidity control. Provide adequate training to all health care professionals working in the unit during day and night shifts. Plan an audit of the policy use and patients’ outcomes after its implementation.
Future directions
As non-invasive respiratory support is a promising and safe technology for neonates with respiratory distress it has been increasingly adopted in developing countries. However, factors like costs, availability of consumables, and additional equipment such as wired circuits and proper humidifiers, can prevent its success and has limited its use for a more immature population of infants with respiratory distress syndrome. Recently, a national scale study done in Malawi demonstrated improved survival with the use of CPAP in much smaller neonates, with birth weight between 1.0 and 1.3 kg. 23 These promising results require larger investigations. Also, studies on the impact of such intervention in patients with meconium aspiration syndrome, perinatal asphyxia, pneumothorax or pneumonia are need. In all these clinical conditions, it is paramount to best utilize any available system, overcoming issues related to their limited technology such as adequate provision of temperature and humidity.
Conclusion
A simple and low-cost intervention to optimize gas T&RH during non-invasive respiratory support is feasible and associated with decreased rates of nasal bleeding in very and late preterm infants.
Footnotes
Authors’ note
The study has been conducted at the Tacchini Hospital NICU in Bento Gonçalves, RGS, Brazil.
Author contributions
KS conceptualized and designed the study, collected data, drafted the initial manuscript, and critically reviewed and revised the manuscript. RMW, MFS, FF, KS, and SCS designed the close control policy, assisted on implementation, and critically reviewed and revised the manuscript for important intellectual content. STMM assisted on the study design, supervised the statistical analyses, and critically reviewed and revised the manuscript for important intellectual content. GSA analyzed collected data, performed statistical analyses, drafted the initial manuscript, and critically reviewed and revised the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.