
Abstract
Keywords
Background
Obesity is the most common medical condition that affects women of reproductive age around the world.1–3 Recently, an inverse relationship between pregestational body mass index (BMI) and breastfeeding (BF) has been established.1–3 The benefits of lactation on short- and long-term maternal and infant health have been clearly documented.4–6 Specifically, exclusive breastfeeding (EBF) or partial BF during birth hospitalization and through the first postpartum year are important for healthy women as well as for those with comorbidities such as diabetes, severe obesity, hypertension, or other conditions.7–10 Regrettably, few studies on perinatal outcomes that included EBF or partial BF in women with Class 3 obesity (morbid BMI 40–49 kg/m2 and extreme BMI ≥ 50 kg/m2) have been published.1,11–14 Women with higher BMI and delayed lactogenesis II are less likely to initiate skin-to-skin contact, BF within the first hour, or EBF at hospital discharge. 11 Previously, we compared perinatal outcomes including BF of 84 women with Class 3 obesity and lower BMI (40–44 kg/m2) with 82 others with higher BMI (≥ 45 kg/m2). 10 Despite the small sample size, we observed greater prevalence of CHTN and lower EBF and BF rates at discharge in the higher BMI group. 10 In the present investigation we have expanded the comparison of BF outcomes to a larger number of women with Class 3 obesity separated into those with morbid or extreme obesity.1,10
Objective
The objective of this study was to compare BF initiation rates and related outcomes of 890 women with morbid and 890 with extreme obesity matched by race, parity, and year of delivery.
Subjects and methods
This retrospective cohort investigation was approved by the Institutional Review Board of The Ohio State University Wexner Medical Center (IRB 2010H0198). Electronic maternal and neonatal records (2013–2021) were reviewed. According to their prepregnancy BMI, women were classified as normal (BMI 18.5–24.9 kg/m2), overweight (BMI 25–29.9 kg/m2), obese Class 1 (BMI 30–34.9 kg/m2), Class 2 (BMI 35–39.9 kg/m2), or Class 3 (morbid BMI 40–49.9 kg/m2 and extreme BMI ≥ 50 kg/m2).1,2
Morbid and extreme obesity groups were matched electronically by race, parity, and year of delivery from 1780 women with Class 3 obesity who delivered live singletons at ≥ 34 weeks gestation in our institution. Not included were women who had bariatric surgery and others whose infants had major malformations. Gestational diabetes mellitus (GDM), Type 1 and Type 2 DM, chronic hypertension (CHTN), preeclampsia, anemia, polycystic ovary syndrome (PCOS), obstructive sleep apnea (OSA), and gastroesophageal reflux disease (GERD) were diagnosed and treated following established guidelines.15–17 Gestational weight gain (GWG) was categorized as adequate, inadequate, or excessive. 18 Clinical and demographic data from some women included in this investigation have been reported previously.9,10,13,14,19
During their prenatal visits and on arrival to Labor and Delivery women were asked about their prior BF experiences, if applicable, and their anticipated feeding preference (BF, formula, or partial) for their infants.10,13,14,19 Women were also informed of our maternal practices that encourage BF including early BF, formula supplementation only if medically indicated, rooming in and availability of fulltime lactation consultants and post-discharge BF support.10,13,14,19 As required for hospital accreditation, our institution reports BF data to the Joint Commission. 7
Following delivery, symptomatic infants were transferred directly to the neonatal intensive care unit (NICU) for further care. Holding, skin-to-skin contact and BF were encouraged depending on the mother-infant dyad condition. Asymptomatic infants able to feed were taken to the Newborn Nursery with their mothers for routine care and glucose monitoring if indicated.10,13,14,19 Using intrauterine growth charts, infants were identified as appropriate for gestational age (AGA), small (SGA), large (LGA), or macrosomic (birthweight ≥ 4000 g). 19
Blood glucose was assessed with Accu-Chek® or by plasma glucose measurements starting during the first hour of life. Infants with hypoglycemia (glucose < 40 mg/dl) were treated with glucose gel, BF or formula feeding and those with persistent hypoglycemia were transferred to the NICU for further care.10,13,14,19
EBF was defined as direct feedings from the breast, expressed breast milk, or donor human milk (DHM). Partial BF was defined as direct BF, expressed breast milk, or DHM supplemented with formula.13,14,19 BF was considered initiated if, during the 24 h preceding hospital discharge, infants were EBF or BF partially.13,14,19 Due to the study design, information on post-discharge infant feeding was not available.
Statistical analysis
Comparisons of the Class 3 morbid and extreme obesity groups were made with t-tests for continuous variables following a normal distribution, and Wilcoxon Two-Sample tests for continuous variables that were not normally distributed. Chi-square analysis was used for categorical variables. Multivariate logistic regressions were used to determine the probability of BF initiation and the probability of EBF at discharge. Explanatory variables in both logistic models included BMI, DM, CHTN, race, public healthcare assistance, mode of delivery, prior BF, infant feeding intention, fetal growth, preeclampsia, late prematurity, macrosomia, hypoglycemia, and admission to the NICU. Logistic models used backward elimination method for variable selection, although forward and stepwise selection methods produced the same results. Significance was established at a p-value < 0.05. Analyses were performed with SAS version 9.4 (Cary, NC).
Results
Maternal clinical and demographics in the morbid and extreme obesity groups
Maternal clinical and demographics in the morbid and extreme obesity groups.

Analysis: † Fisher’s Exact Test, ^ Chi-square, * T-Test, ‡ Wilcoxon Two-Sample test.
The prevalence of A1 GDM (6 vs 4%) was similar while that of A2 GDM (11 vs 7%) was greater in the extreme obesity group. Treatment of the 168 women with A2 GDM combined from both groups included: 25 on glyburide, 67 on insulin, and 76 on metformin. Although the prevalence of Type 1 was similar (2 vs 2%) that of Type 2 DM was greater in the extreme obesity group (10 vs 4%).
Hypertensive disorders were more common among women in the extreme obesity group: CHTN (23 vs 11%) and CHTN on medication (18 vs 6%). The most common medications in the morbid obesity group were labetalol (55%), nifedipine (20%), lisinopril (5%), amlodipine (5%), and miscellaneous (15%). For women in the extreme obesity group, the most common medications were labetalol (63%), nifedipine (22%), lisinopril (4%), and miscellaneous (11%). All patients with preeclampsia with severe features were treated with magnesium sulfate during the intrapartum period and post-delivery. OSA (12 vs 3%), and asthma (22 vs 16%). PCOS (7 vs 5%), GERD (10 vs 10%), and anemia (17 vs 17%) were similar. There were 152 women in the morbid and 154 in the extreme obesity group reported to have anemia. These groups represent a combination of postpartum hemorrhage (2 vs 3%), intraoperative bleeding (2 vs 1%), and iron deficiency anemia (13 vs 13%).
Vaginal delivery was more frequent in the morbid group (57 vs 38%) while primary and repeat cesareans were greater in the extreme obesity group (31 vs 22% and 31 vs 21%, respectively). As expected, mean pregestational weight (102 vs 134 kg) and weight at delivery (116 vs 149 kg) were different; however, the prevalence of excessive (73 vs 76%), adequate (21 vs 18%), and inadequate GWG (6 vs 6%) were similar in both groups.
Neonatal outcomes in the morbid and extreme obesity groups
Neonatal outcomes in the morbid and extreme obesity groups.
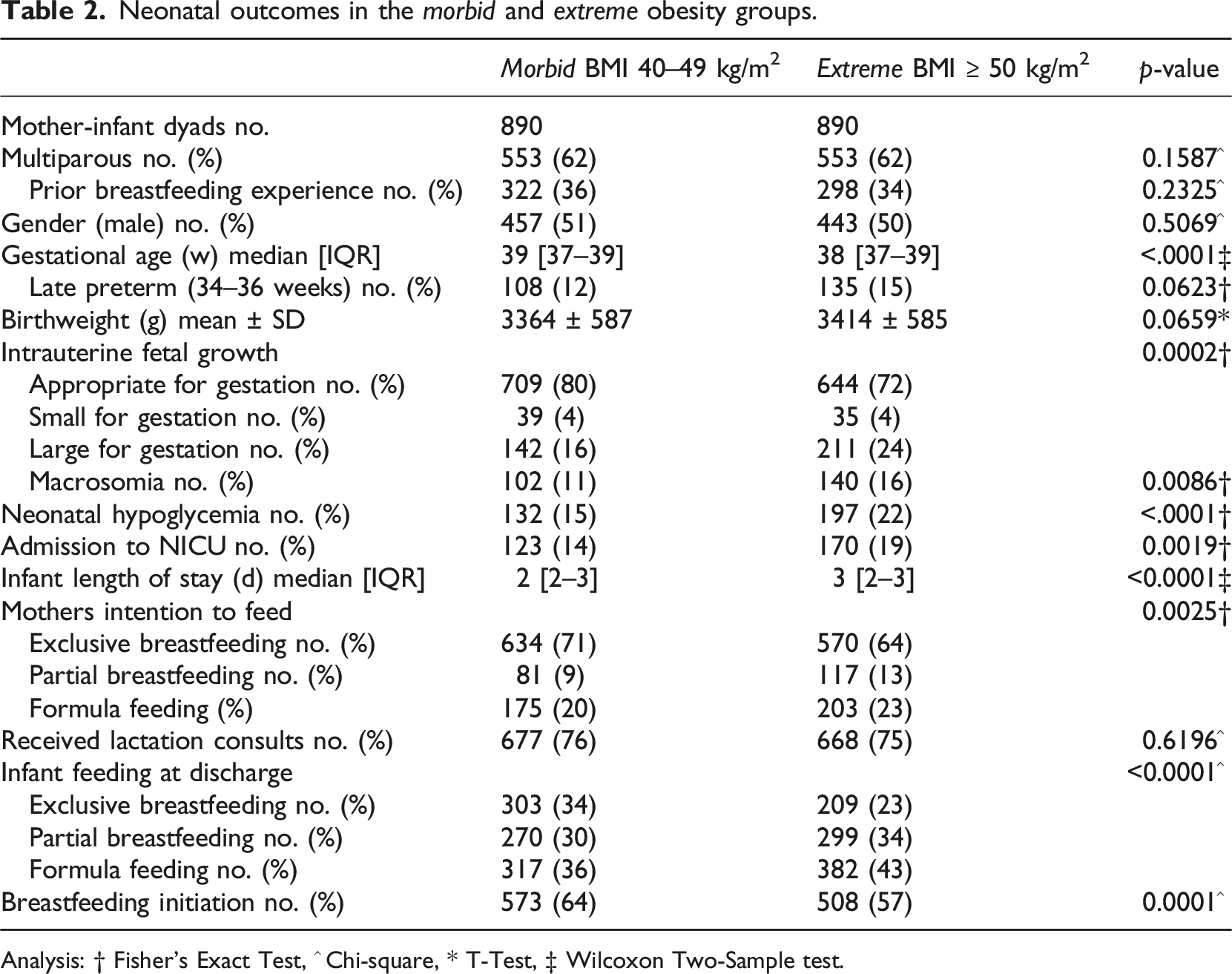
Analysis: † Fisher’s Exact Test, ^ Chi-square, * T-Test, ‡ Wilcoxon Two-Sample test.
According to their gestational age, the prevalence of late prematurity was similar at 34 (25 vs 22%), 35 (31 vs 31%), and 36 weeks (44 vs 47%). In the morbid obesity group, 50% of the 108 late premature infants required NICU care. In comparison, in the extreme obesity group, of the 135 late premature infants, 82 (61%) were transferred to the NICU.
Hypoglycemia affected 132 (15%) of the morbid obesity group and of them, 78 (59%) were treated successfully in the Newborn Nursery while the remaining 54 (41%) required admission to the NICU. Of the 197 (22%) infants from the extreme obesity group who had hypoglycemia, 98 (50%) were treated successfully in the NN while the remaining 99 (50%) required admission to the NICU.
Admission to the NICU (19 vs 14%) was more prevalent in the extreme obesity group. Of the 293 (16%) infants from both groups combined admitted to the NICU, 24% were transferred directly from the delivery room (DR) while the remaining 76% remained in the Newborn Nursery until they developed the need for specialized care. Primary NICU admission diagnoses for both obesity groups were similar in respiratory distress (32 vs 32%), apnea-hypotonia-temperature instability (14 vs 12%) and other miscellaneous conditions (13 vs 10%). Regardless of morbidities or place of care, all infants as well as their mothers were discharged home in good condition.
Infant feeding preference, exclusive breastfeeding, and breastfeeding initiation
Six hundred and thirty-four women (71%) in the morbid obesity group and 570 women (64%) in the extreme group intended EBF (Table 2). Although 92% and 91% of them received lactation support, at discharge 18% from the morbid and 23% of the extreme obesity group fed formula, 36% and 42% BF partially and 46 and 34% EBF. Direct BF only was more common in the morbid obesity group (78 vs 72%). In contrast, direct BF combined with DHM was not different between groups (18 vs 16%).
Eighty-one (9%) of the morbid and 117 (13%) of the extreme obesity group intended partial BF. Although 85% in the morbid and 88% of those in the extreme obesity group received lactation support, at discharge 44% in the morbid and 46% in the extreme obesity group fed formula, 42 and 45% BF partially and only 14 and 9% EBF.
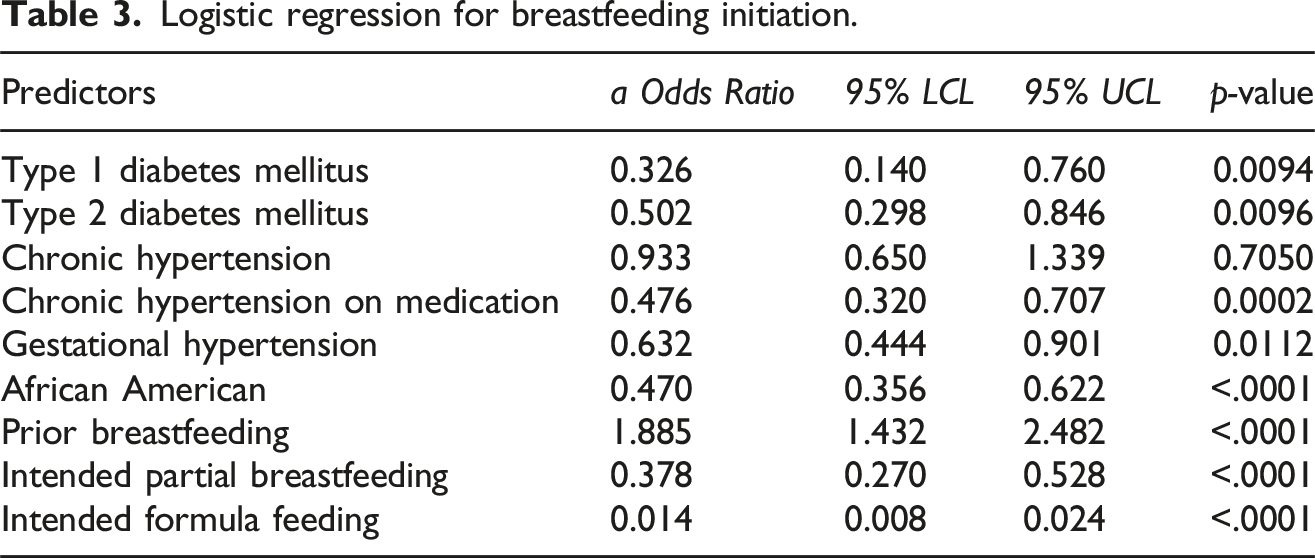
One hundred and seventy-five women (20%) in the morbid and 203 (23%) in the extreme obesity group prenatally intended to feed formula and 85% and 82% of them respectively declined lactation support (Table 2). At the time of discharge, 95% of those in the morbid and 97% of the extreme obesity group fed formula while the remaining BF partially. Regression analysis confirmed that intention to FF was likely to predict EBF or BF initiation failure (a OR 0.016 CI 95% 0.005, 0.050 and a OR 0.0140 CI 95% 0.008, 0.024, respectively) (Figure 1 & Table 3). Exclusive breastfeeding at discharge. Logistic regression for breastfeeding initiation.
Iron deficiency anemia, postpartum hemorrhage or intraoperative bleeding were not independent predictors of BF success or failure. Similarly, excessive, adequate, or inadequate rates of GWG observed in women of either group were not independent predictors of EBF or any BF in this investigation.
The occurrence and timing of the first BF showed that in the morbid obesity group 317 (50%) BF during the first 2 hours, 161 (25%) between 3 and 6 hours, 94 (14%) BF later, and 62 (10%) never BF. On the other hand, of women in the extreme obesity group 232 (41%) BF during the first 2 hours, 144 (25%) between 3 and 6 hours, 121 (21%) BF later, and 73 (13%) never BF.
At discharge, the rates of EBF (23 vs 34%) and BF initiation (57 vs 64%) were significantly lower in the extreme obesity group. Regression analysis showed that women who were African American, received public healthcare assistance, diagnosed with DM, gestational or severe CHTN, delivered by cesarean, and whose infants had hypoglycemia were less likely to EBF or to initiate BF at discharge (Figure 1). More women in the extreme obesity group received public healthcare assistance and of them only 18% had EBF at discharge as compared with those from the morbid obesity group who had 25% EBF, however, both groups had similarly low rates of BF initiation (52 vs 51%). In contrast, among women who did not receive public healthcare assistance, rates of EBF (46%) and BF initiation (80%) in the morbid group were significantly better than those of women in the extreme obesity group (EBF 34% and BF initiation 71%).
Among women in the morbid obesity group, 322 (36%) had prior BF experience and at discharge, 48% EBF and 84% initiated BF. In comparison, of women in the extreme obesity group, 298 (34%) had prior BF experience and at discharge 30% EBF and 74% initiated BF. Regression analysis corroborated the importance of prior BF experience on successful EBF (a OR 1.512 CI 95%1.155, 1.981) (Figure 1) and BF initiation rates (a OR 1.885 CI 95% 1.432, 2.482) (Table 3) at the time of hospital discharge.
Discussion
Given that race, parity, and year of delivery could affect outcomes, we matched women with these variables to highlight any differences between the morbid and extreme obesity groups. Of the many morbidities that alone or in combination with morbid and extreme obesity could affect BF initiation and other perinatal outcomes, diabetes, hypertension, preeclampsia, fetal growth, prematurity, and hypoglycemia are prominent.9,10,13,14,19,20
While many studies have addressed perinatal outcomes, their results have often been confounded by small sample size, the definition of obesity used (BMI ≥ 25 kg/m2, BMI ≥ 30 kg/m2), and the absence of information on BF.20–22 Although without providing specific BF data, several authors have reported increased rates of adverse perinatal outcomes among women with extreme obesity (BMI ≥ 50 kg/m2).20,23,24 The overall rate of severe maternal morbidity at the time of delivery is lowest among women with normal prepregnant weight and is the highest among women with extreme obesity. 20 The greater prevalence of GDM, PGDM, CHTN, and preeclampsia superimposed in the extreme obesity group is a significant concern because the absence of BF deprives mother and infants of short- and long-term health benefits.4–6,25
OSA was twice as common in the extreme than in the morbid obesity group. This is not surprising because OSA is a common sleep disorder in obese adults estimated to affect up to one billion people worldwide. 26 The prevalence of GERD in both study groups, although similar, remained a comorbidity of clinical importance. 27 Obesity has been recognized as an important comorbidity in patients with asthma or asthma-like symptoms. 28 Adults with Class 3 obesity, especially those with BMI ≥ 50 kg/m2 have over twice the risk of asthma as compared to adults of normal weight. 29 Furthermore, the increased prevalence of asthma and OSA in combination with GERD in the extreme obesity group is worrisome because their common inflammatory pathways could further the development of asthma or worsen asthma control. 30 Another concern is the high prevalence of asthma in children born to women who were obese and had asthma during pregnancy. 28 Fortunately, weight reduction following bariatric surgery may improve asthma outcomes or may decrease the need for asthma medications. 29
PCOS is the most common endocrine disorder associated with obesity among women of reproductive age; however, its prevalence in this study is in line with other reports. 31
The association between maternal obesity and fetal/neonatal macrosomia has been reported consistently.9,23,24 Although the prevalence of macrosomia among the extreme obesity group was greater, regression analysis revealed that macrosomia was not a main predictor of EBF or BF initiation. Late prematurity was similar between both study groups while hypoglycemia was more common among infants in the extreme obesity group. Furthermore, as confirmed by abundant literature, hypoglycemia is more common among infants born to women with Class 3 obesity, diabetes, hypertensive disorders, SGA, LGA, macrosomia, late prematurity, cesarean delivery, and admission to the NICU.9,10,13,14,19,23
The American Academy of Pediatrics and the Academy of Breastfeeding Medicine recommend EBF for all healthy infants during their birth hospitalization.7,8 In the US, in 2019 the mean in-hospital EBF rate in the general population was 62.6% and for those in the most BF supportive hospitals was 64.7%.7,8 These rates are quite different from the 19 to 35% EBF range reported for women with severe obesity, pregestational diabetes, preeclampsia, or CHTN.9,10,13,14,19 Considering that the comorbidities affecting both groups were similar to those described above, the low EBF rate reported here was not surprising. The even lower EBF rate observed in the extreme obesity group clearly suggests the significant influence of the elevated pregestational weight.
Intention to BF is a strong, albeit not absolute, predictor of BF initiation and BF duration in healthy as well as in high-risk obstetrical populations.9,10,13,14,19 Intention to BF, EBF, and BF initiation rates were all lower in the extreme obesity group. It is likely that the higher prevalence of comorbidities and other obstacles to BF that characterized the extreme obesity group played a significant role in these results.
Nine percent of women in the morbid and 13% of those in the extreme obesity groups intended to BF partially. Despite receiving lactation support, about 40% fed formula at discharge, 50% had partial BF and only 10% EBF. Twenty percent of women in the morbid and 23% of those in the extreme obesity group intended to feed formula at discharge. Most of these women declined lactation assistance, and as expected, almost all formula fed at discharge. The rate of women who did not intend to BF has been consistent through many studies.13,14,19
The few articles that included BF information among women with Class 3 obesity have corroborated the negative association of severe obesity with low BF initiation and BF duration.9–14 Unfortunately, none of these studies separated women with Class 3 obesity by severity until Ramji et al. reported decreasing rates of any BF at discharge for Classes 1 and 2 combined (BMI 30–39.9 kg/m2) and for Class 3 divided into morbid and extreme obesity. 1 Regrettably, their definition of BF was limited to “any” BF and their sample size included 535 women with morbid and only 71 with extreme obesity. 1
Another predictor of BF duration, BF initiation (EBF or partial) at hospital discharge, was reported to be 83.2% in 2019 for the general US population. 8 In comparison, BF initiation rates among women with comorbidities such as those described above ranged from 54 to 82%; thus, the 64% BF initiation rate in the morbid and the 57% in the extreme obesity group reported here is of concern.7,8,19
Prior BF experience even among women with obesity and other comorbidities is also a good predictor of successful BF in subsequent pregnancies.32,33 It is of concern that at discharge of 298 women with prior experience in the extreme obesity group only 30% had exclusive BF as compared to the 48% among 322 women with prior BF experience in the morbid obesity group. It is established that women who do not BF their first child are unlikely to BF their next. 32 Regardless of the difficulties that led to an unsatisfactory BF experience, it is important for health providers to comfort, educate, and encourage these women and their families to expect better outcomes in future pregnancies. 33
In addition to the comorbidities described above, there are several other obstacles to BF including race, advanced maternal age, smoking, and public healthcare assistance that should be recognized.34–36 The lower success of EBF and BF initiation of African American women compared to white women in our study is similar to that reported by others. 34 Women of advanced age and smokers are less likely to initiate BF or to BF longer than non-smokers. 35 In this investigation, almost one fourth of women in both BMI groups have been smokers prior to the current pregnancy. There is ample evidence that smoking in obese and non-obese women is associated with low BF and BF duration.1,10,11,19,35 In the present study, the high rate of former smokers before their pregnancy compared to the 10% still smoking through delivery may reflect some success, at least temporarily of smoking cessation programs. Promoting BF initiation and duration in smokers and non-smokers could have cascading health benefits for mothers and infants. 35
Public healthcare assistance was reported for 57% women in the morbid and 67% in the extreme obesity group. At the same time, EBF (25 vs 18%) and BF initiation (52 vs 51%) were low in both groups. On the other hand, among women who had private insurance, rates in the morbid obesity group were 46% EBF and 80% BF initiation compared with those in the extreme group where rate of EBF was 34% and of BF initiation was 71%. Regression analysis revealed that women receiving public healthcare assistance were less likely to EBF (a OR 0.521 CI 95% 0.403, 0.675) (Figure 1) or to initiate BF (a OR 0.484 CI 95% 0.362, 0.646) (Table 3). We agree with Greiner et al. that more research is needed to identify risk factors for comorbidities and find ways to improve perinatal outcomes for women with severe obesity who receive public healthcare assistance. 36
Lactogenesis II occurs normally between 50 and 72 hours postpartum and is recognized by the start of a copious milk secretion, beyond that period it is considered delayed.37,38 Delayed lactogenesis II is associated with obesity, diabetes, excessive weight gain during pregnancy, primiparity, advance maternal age, operative delivery, labor medications, and breast and nipple morbidities.11,37,38 Women who experience delayed lactogenesis II often have low BF initiation and early BF cessation.11,37,38
Self-confidence in women’s capacity to BF successfully (self-efficacy) is a modifiable factor that may improve BF rates. 39 Lack of information about the health benefits of BF and exposure to friends or relatives who never BF may contribute to low self-confidence. Furthermore, inadequate milk supply, poor latching, breast size, nipple problems, and the inability to satisfy their infants often lead to milk supplementation. 39 Poor self-efficacy with BF could be improved by social support (family, friends, or healthcare providers) together with educational interventions that need to be provided during and after the hospital stay. 40 In the present study, there was no information available on self-efficacy; however, lower intention to BF among multiparous women without prior BF experience in the extreme obesity group suggests that lack of self-confidence with BF may have played a role. 40
A limitation of this investigation is that the definition of exclusive BF and BF initiation at discharge used here may be applicable only to women with high-risk obstetrical conditions and to the absence of follow-up information on BF after hospital discharge. The strength of this investigation is that it highlights the differences in BF initiation and related comorbidities between women with Class 3 obesity separated by pregestational weight into morbid and extreme. In addition, the obstetrical and neonatal data presented here was obtained directly from electronic medical records and not from post-delivery maternal questionnaires.
In conclusion, the division of women with Class 3 obesity into subgroups according to severity revealed significant differences in BF initiation and related perinatal outcomes. Women in the extreme obesity group had a greater incidence of maternal and neonatal comorbidities that were associated with lower rate of prenatal intention to BF, EBF, and BF initiation at discharge. Recognition of the difference between morbid and extreme obesity groups highlights the need for specific perinatal interventions if BF initiation is to be improved in this uniquely challenging patient population.
Statements and declarations
Footnotes
Authors’ contributions
All authors participated in planning and research design; data analysis and manuscript preparation: LC; and manuscript revisions: LC, CAN, MRS, MBL, BJN, and SN. The author(s) read and approved the final manuscript.
Conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Human research statement
This research was approved by The Ohio State University Wexner Medical Center and followed all federal regulations. All methods were performed in accordance with the relevant guidelines and regulations of the Declaration of Helsinki.
Data availability statement
The data sets generated during and analyzed during the current study are not publicly available due to limitations of ethical approval involving the patient data and anonymity but are available from the corresponding author on reasonable request.