
Abstract
Fungal infections in preterm infants are uncommon but serious infections that carry a high mortality rate. Preterm infants who are extremely low birth weight are at high risk for fungal infections due to immaturity of their immune system and skin barrier. Factors which further reduce host immunity in premature infants include prolonged use of broad-spectrum antibiotics and corticosteroids. Our case presentation involves an extremely low-weight 23-week preterm infant diagnosed with primary invasive cutaneous aspergillosis (PCA) confirmed by skin biopsy and cultures obtained from skin debridement. His inoculation was thought to be secondary to either a thermal burn or macerated skin from prolonged incubation. This case highlights the importance of keeping fungal infections at the forefront of one’s differential diagnosis when an extremely low-weight infant presents with cutaneous lesions, as disseminated fungal infections carry a high mortality rate.
Introduction
Environmental factors that compromise the integrity of the epidermal layer may increase the risk of inoculation of opportunistic species such as fungal infections. 1 Most opportunistic fungal infections in very low to extremely low birth weight premature infants are caused by Candida species. Primary cutaneous aspergillosis is a rare but potentially fatal infection for a preterm infant due to the organism’s ability to easily invade blood vessels and spread systemically.2,3 Therefore, it is important to maintain a high index of suspicion for a fungal etiology when non-specific cutaneous lesions present in a preterm newborn. We present a case of a preterm male infant who had eruption of cutaneous lesions at day of life seven thought to be due to a primary cutaneous fungal infection due to a thermal burn or macerated skin from incubation. Skin biopsies ultimately proved the diagnosis to be primary invasive aspergillosis due to Aspergillus fumigatus. Early diagnosis is paramount to successful treatment due to the high mortality rate of this infection, and treatment will involve prolonged use of systemic antifungal agents and the possibility of surgical debridement.
Case presentation
A male preterm infant present at 1 week of life as transfer from an outside hospital. The patient was born at 23 weeks 6 days of gestation with a birth weight of 690 g to a 23-year-old African American mother via C-section due to preterm labor and breech presentation. His APGAR scores were 1, 3, and 5, at 1, 5, and 10 minutes, respectively. He was intubated after birth and received a dose of surfactant. He had severe hypoxia and hypotension for the first 12 hours of life requiring oscillator, inhaled nitric oxide, fluid resuscitation, blood products, and vasopressors. He required insulin for the first 2 days of life due to hyperglycemia. His early onset sepsis workup was negative and had received empiric treatment with ampicillin and gentamicin for 48 hours. He remained on prophylactic fluconazole due to prematurity and presence of a central line. He was on hydrocortisone due to presumed adrenal insufficiency. Late onset sepsis work up was initiated at 7 days of life due to worsening respiratory status and eschar-like plaque lesion on the posterior trunk [Figure 1]. He was transferred to our NICU for further management. Eschar-like plaque noted on day of life 8.
The initial working diagnosis for cutaneous lesion at our NICU was pressure or decubitus ulcers or thermal burns from prolonged contact with the thermal mattress. Burn surgery and wound care team followed the patient with regular cleaning and application of bacitracin with transient improvement in the lesion. He completed his second course of empiric antibiotics after his late-onset sepsis evaluation was unremarkable. He also remained on Tylenol treatment for patent ductus arteriosus (PDA) closure. Fluconazole was not continued at our NICU as per unit guidelines due to low fungal infection rate.
On day of life 13, he developed acute evolution of the lesion with breakouts of vesiculopustular lesions on the back, discrete crusted lesions on the right side of the abdomen, and sharply demarcated darkened perianal lesions [Figure 2(a)–(c)]. The initial clinical suspicion was that the evolution of lesions represented disseminated herpes or bacterial sepsis. Biopsy of the lesion was performed, and infectious work up including blood cultures, herpes simplex virus (HSV), varicella zoster virus (VZV) surface cultures, urine cytomegalovirus (CMV), and cerebrospinal fluid (CSF) studies were sent and started on cefotaxime, vancomycin, and acyclovir. Abdominal ultrasound obtained showed a large hepatic fluid collection. The preliminary result of the skin biopsy noted ribbon-like hyphae in the epidermis, necrotic tissue, lymphohistiocytic infiltrate, and edema, concerning for opportunistic fungal infection. CSF studies, blood and other cutaneous cultures were negative. On day of life 13—new pustular lesions surrounding plaque (a), eruption of erythematous vesicles on abdomen/chest (b), and darkened perianal lesion (c).
His antimicrobial regimen was switched to amphotericin B to treat fungal infection and meropenem due to concerning hepatic abscess. On day of life 17, debridement of the lesions and draining of hepatic abscess was performed by burn and pediatric surgery. The cultures obtained from cutaneous lesions speciated to Aspergillus fumigatus. All other cultures including several fungal blood cultures sent during the hospitalization remained negative. His lack of clinical improvement on amphotericin B and elevated Aspergillus galactomannan levels up to 1.34 prompted switch to voriconazole, which he was ultimately discharged with. After debridement and continuation of IV antifungal medication and wound care, the lesions slowly started improving [Figure 3(a) and (b)]. Improvement of lesions noted of 2 days post-surgical debridement (a). Evolution of posterior trunk lesion into a hypopigmented scar tissue at 2 months (b).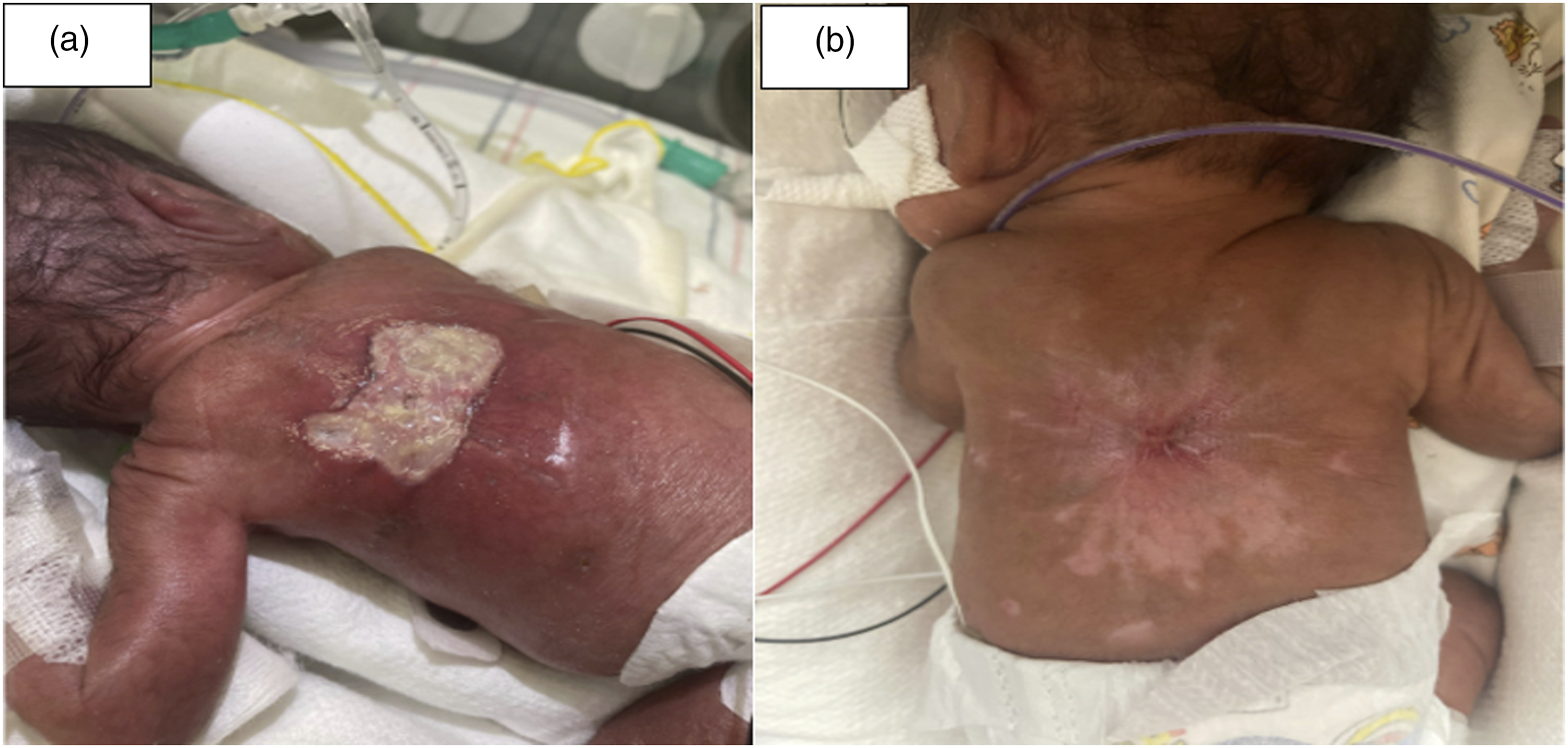
Literature review and discussion
Aspergillus is a common fungal organism with Aspergillus Fumigatus being the most common species causing invasive disease in humans. This infection may cause severe sepsis and multiorgan failure.4,5 Aspergillus spores easily become airborne due to their small size (2.5–3 µm in diameter) and may spread via the respiratory tract from common NICU objects such as adhesive tapings used for securing endotracheal tubes, non-sterile gloves, oximeter sensors, and humidified incubators.6,7 The risk factors for Aspergillus to become an invasive infection include neutropenia, and use of glucocorticoids or antibiotics. 8 The use of glucocorticoids has been shown to decrease the quantity of neutrophils and macrophages, as well as diminish their fungicidal activity against Aspergillus.3,8
Cutaneous aspergillosis is a rare infection with premature infants being at higher risk due to their impaired cutaneous and immunologic defenses. The mean gestational age for infection in the NICU is 25 weeks, mean birth weight 720 g, and mean age of onset of lesions at 10 days of life. The diagnosis is made with tissue biopsy and culture which shows septate hyphae with branching at 45°, and if invasive may show extension into dermal blood vessels.2,4 Intact keratin and epidermal layers prevent the inoculation of the small 3–5 um conidial spores of Aspergillus species in healthy hosts. 9 Direct skin inoculation of Aspergillus spores may occur when skin barrier defenses become further damaged by surgery, burns, or by skin maceration (prolonged exposure to heat and moisture in a confined environment) caused by the humid environments of incubators. The use of corticosteroids further decreased the tensile strength of epidermal and dermal tissue. The use of antibiotics is purported to decrease potentially protective skin flora. The initial lesions of PCA begin as erythematous plaques or papules and evolve to pustules and yellow crusted ulcerated lesions and finally into necrotic black eschars.8,9
The final diagnosis for our patient was primary cutaneous aspergillosis with Aspergillus fumigatus. The lesions upon transfer were non-specific and had been amenable to bacitracin ointment. Eschar-like lesions were the presenting skin finding upon transfer, and the clinical suspicion for fungal infection occurred after the development of vesiculopustular lesions with overlying yellow crusting lesions extended to the abdomen. The diagnosis was made a day after skin biopsies and culture from surgical debridement confirmed that the lesions were fungal. In our case, the etiology of inoculation was thought to be secondary to skin breakdown from skin maceration from thermal incubation or from burned skin from ECG leads. There was no formal epidemiological investigation into the true source of the infection at the referring unit.
Our patient had several risk factors which strongly predisposed him to a fungal infection. His 23-week prematurity and birth weight of 690 grams were non-modifiable risk factors. The most obvious additional risk factor for inoculation involved a large surface area of compromise of skin integrity from presumed skin erosion. Additionally, he received broad-spectrum antibiotics in his hospital course and corticosteroids potentially compromising his skin microbiome and integrity.
After the lesions erupted, the differentials included infectious and non-infectious etiologies. From an infection standpoint, there were concerns for disseminated herpes and bacterial sepsis. Prior to Aspergillus speciation on culture, additional fungal considerations included Candida, Fusarium, and Mucormycosis. Non-infectious etiology was originally the leading diagnosis upon transfer as we thought the patient had iatrogenic pressure ulcers. Epidermolysis bullosa simplex is a blistering disorder that was also considered because it involves eroded or ulcerated skin with overlying crusting. Pyoderma gangrenosum was not discussed as a differential due to its rarity in neonates, but may present with sharply demarcated ulcers of the groin and buttocks of infants. 4 Additional non-infectious sources included nutritional/vitamin deficiencies such as a zinc deficiency with acrodermatitis enteropathica, although this would typically have a perioral rash. Immunological deficiencies such as complement deficiency were considered. Hematologic considerations included protein C/protein S deficiency and Langerhans cell histiocytosis.
The standard of treatment for most cases of cutaneous aspergillosis is systemic deoxycholate amphotericin B at a dose of 1 mg/kg/day. 8 While on amphotericin B, there is close monitoring for myelotoxicity, nephrotoxicity, and electrolyte derangements. Our patient was eventually switched to 6 mg/kg twice daily voriconazole due to its efficacy in treating invasive aspergillosis and because of slowly healing lesions and high galactomannan level on amphotericin B.1,5 Voriconazole is an effective fungicidal against Aspergillus molds and is becoming the standard of treatment for invasive Aspergillus infections in both children and adults. 4 Voriconazole acts by inhibiting synthesis of the fungal plasma membrane. 1 In a large comparative trial in immunocompromised adult patients with invasive aspergillosis, voriconazole proved a better clinical response and survival than compared to amphotericin B. 10
Serum Aspergillus galactomannan levels were traced throughout inpatient and outpatient management to determine response to antifungal treatment and to determine length of treatment. Our case was presumed disseminated disease with an initial galactomannan level of 1.34. Fortunately, brain MRI never showed CNS disease, the hepatic abscess remained culture negative, and chest X-rays never showed any consolidations concerning invasive pulmonary aspergillosis. Close discussions between the primary team, infectious disease, burn and pediatric surgery, and dermatology determined that the best chance at reducing morbidity and mortality included surgical debridement of lesions and close monitoring of new lesions for possible re-debridement. Some of the literature reports that surgery is not indicated when lesions are extensive due to the risk of poor post-operative tolerance. In our case, surgical debridement complimented intravenous systemic antifungal therapy. After surgery, burn surgery recommended daily wound care with daily cleansing of wounds with infant soap, bacitracin ointment 3 times daily, and coverage with Telfa dressing.
Our patient was eventually discharged on oral voriconazole 6 mg/kg/dose three times daily. There was routine monitoring of hepatic function, voriconazole levels, and galactomannan levels by the infectious disease team. His previous necrotic skin lesions have healed completely with formation of hypopigmented scar tissue. Voriconazole was stopped after 7 months of treatment when monthly galactomannan level remained low (0.07). The patient is currently 9-month-old and is being followed outpatient by pediatric infectious disease every 3 months.
Conclusion
Preterm infants are particularly susceptible to environmental fungal infections given their immature immune systems and thin epidermal layer. Multiple cases show that it is important to consider primary cutaneous Aspergillus in extremely low birth weight neonates with rapidly progressing non-specific lesions given the need for prolonged antifungal treatment and possible surgical debridement. Before diagnostic testing with skin biopsies, empiric antifungal treatment should be started. While the previous standard of treatment was amphotericin B, voriconazole is becoming a more viable treatment option for immunocompromised patients.
Statements and declarations
Footnotes
Acknowledgements
I would also like to acknowledge Dr Erica Peak, MD and Dr William Koch MD who were part of our infectious disease team. They helped aid in the diagnosis and management of our patient, and whom continue to monitor his progress after his NICU discharge.
Conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.