
Abstract
Background
Umbilical venous catheterization provides essential vascular access in neonates, particularly in premature and low-birth-weight neonates. Conventional confirmation using radiography may delay accurate placement and increase radiation exposure.
Aim
To compare catheter placement confirmation using conventional radiography versus real-time bedside ultrasonography, while evaluating diagnostic performance, procedural efficiency, radiation exposure, and short-term complications.
Patients and Methods
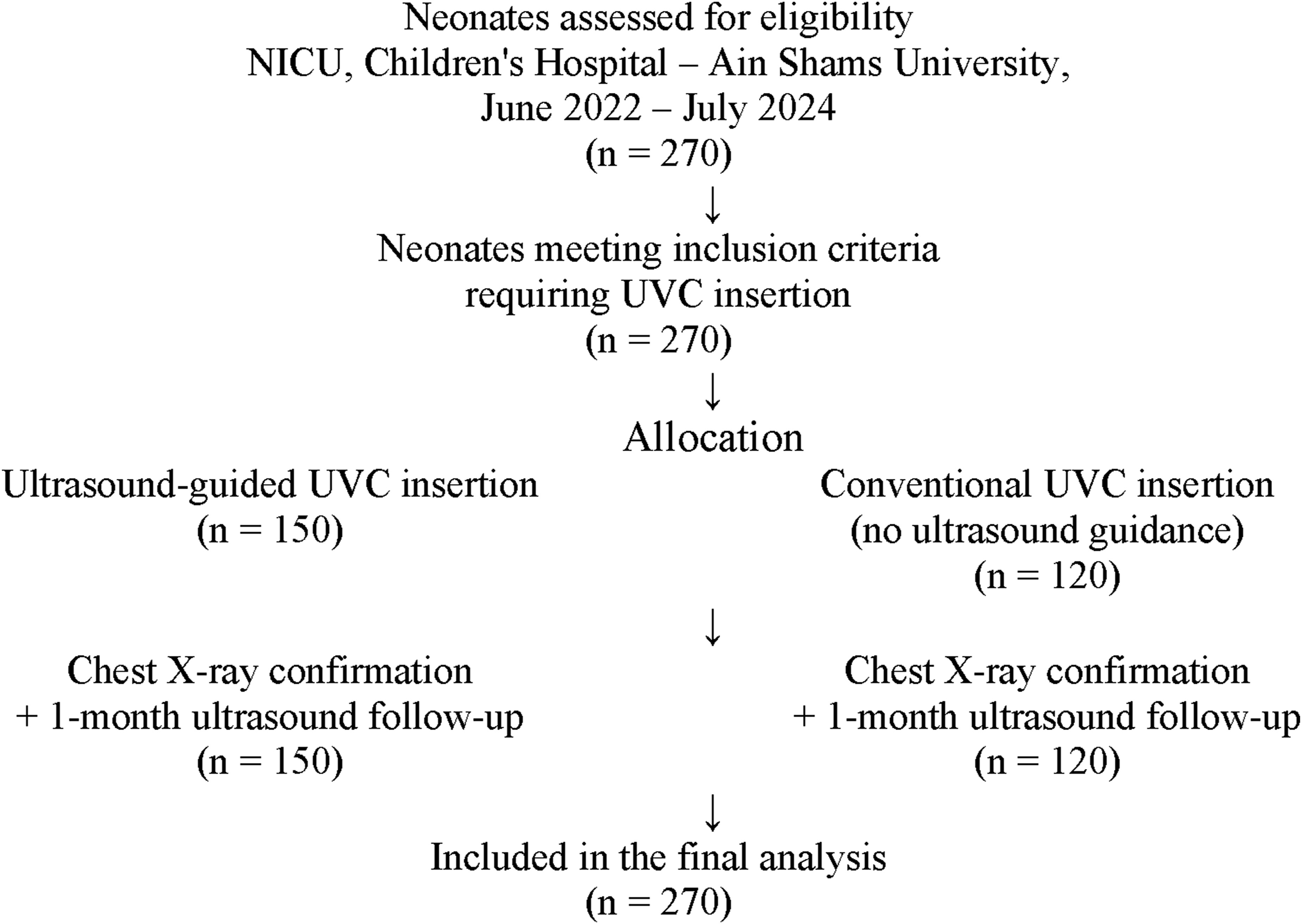
A prospective cohort study was conducted on 270 neonates (150 with ultrasound guidance and 120 without) who required umbilical venous catheterization in the neonatal intensive care unit at Children’s Hospital, Ain Shams University, from June 2022 to July 2024.
Results
Standard catheter positioning (T7–T9) was achieved in 97.9% of ultrasound-guided cases compared with 70.4% in the non-guided group (p < 0.001). Procedure time until suturing and radiographic confirmation was significantly shorter in the ultrasound group (5.87 ± 1.37 and 14.14 ± 2.15 min) than in the non-ultrasound group (6.90 ± 1.99 and 16.90 ± 3.46 min) (p < 0.001). Ultrasound guidance reduced catheter manipulations and the number of radiographs required. Diagnostic performance of ultrasound showed high sensitivity (95.2%) and accuracy (94.0%). One-month follow-up demonstrated minimal complications.
Conclusion
Ultrasound-guided umbilical venous catheter insertion provides accurate and efficient catheter localization, reduces procedure time and radiation exposure, and offers reliable diagnostic performance. These findings support its routine use in neonatal intensive care units.
Introduction
Umbilical vein catheterization utilizes the exposed umbilical stump in a neonate as a site for emergency central venous access up to 7 days old. Umbilical vein catheterization can provide a safe and effective route for the intravenous delivery of medications and fluids during resuscitation. While most commonly used in the delivery room for resuscitation, the umbilical vein provides a viable site of venous access for a trained provider. While peripheral intravenous access is the preferred route of medication administration in neonates, providers who care for neonates should be skilled in multiple techniques for IV access, including intraosseous lines, peripheral IVs, central venous catheters, and umbilical vein access. While intraosseous (IO) access has been shown to be more quickly attainable than an umbilical vein catheter in a neonate, difficulty placing an IO in a neonate and the risk of dislodgement during a code make umbilical vein catheterization an attractive modality for intravenous access by personnel trained in the procedure
1
An umbilical venous catheter generally passes directly superiorly and remains relatively anterior in the abdomen. It passes anterosuperiorly through the umbilicus, umbilical vein, left portal vein, ductus venosus, and the middle or left hepatic vein, and terminates in the suprahepatic inferior vena cava. The tip of the catheter is the most important factor in the development of hepatic injury (Figures 1–4).
2
Schematic representation of the umbilical venous catheter (UVC) pathway through the umbilical vein (UV), ductus venosus (DV), inferior vena cava (IVC), and right atrium (RA), illustrating the ideal catheter tip position at the IVC–RA junction. Adapted from D'Andrea et al. (2022). Flow diagram of neonates included in the study comparing ultrasound-guided versus conventional umbilical venous catheter insertion. Comparison between US-Guided Group and non-US-Guided Group, according to the number of CXR needed. Level of UVC in CXR (thoracic vertebrae number) in both US-Guided Group and non-US-Guided Group.


Path of the umbilical venous catheter
Previous studies conducted in neonatal intensive care units have reported considerable variability in the number of radiographs performed during hospitalization, with some infants undergoing multiple imaging examinations. This variability raises concerns about cumulative radiation exposure in premature and critically ill neonates and highlights the need for alternative imaging methods that reduce radiation use. 3
Traditionally, the position of the umbilical venous catheter tip is confirmed using chest and abdominal radiography after catheter insertion. However, this approach may delay confirmation of correct catheter placement and frequently requires repeated radiographs when malposition occurs. Catheter malposition is relatively common and may lead to serious complications such as arrhythmia, thrombosis, hepatic injury, or cardiac tamponade. In addition, repeated radiographic examinations increase radiation exposure in premature and critically ill neonates, who often require multiple imaging procedures during their NICU stay. Although ultrasound has emerged as a promising alternative for real-time catheter visualization, further studies are needed to evaluate its diagnostic accuracy, procedural efficiency, and clinical outcomes compared with conventional radiographic confirmation.
Aim of the work
To compare the accuracy of conventional radiography and real-time bedside ultrasonography in confirming umbilical venous catheter placement in neonates, while also evaluating the diagnostic performance of ultrasound (sensitivity and specificity), procedural efficiency, radiation exposure, and short-term complications during follow-up.
Patients and methods
This prospective cohort study was conducted on 270 neonates who required umbilical venous catheter placement, admitted to the neonatal intensive care unit (NICU) at Children’s Hospital, Ain Shams University, from June 2022 until July 2024.
Study population
Neonates who required umbilical venous catheter placement were recruited after obtaining informed consent from their guardians and after approval from the ethics committee of Ain Shams University.
Selection criteria for cases
Group allocation
Neonates were allocated to either the ultrasound-guided group or the conventional group according to the catheter insertion technique used during the study period. During the initial phase of the study, UVC insertions were performed using the conventional technique without ultrasound guidance. Following training in neonatal ultrasonography and the implementation of ultrasound-guided practice in the NICU, subsequent UVC insertions were performed under real-time ultrasound guidance.
Study tools and procedures
Part 1: Prospective evaluation of current umbilical venous catheter placement practices
During a 3-month period, the following pre-procedural data were gathered: maternal data (age, gravida, para, diabetes mellitus, hypertension, delivery type, and multi/single gestation), gender, race, APGAR at 5-min, newborn gestational age, length, umbilical stump length, birth weight, umbilical catheter type/size, indication for placement, and respiratory support at birth. Using a stopwatch, we measured procedure time for catheter placement with suturing/fixation. Procedure time was started with the cutting of the umbilical vessel and measured at 2 endpoints. The first endpoint was when the operator completed suturing. The second endpoint was X-ray confirmation of the proper placement of the UVC. Success rate, number of manipulations, Complications including bleeding, arrhythmia, thrombosis, and infection were documented. In this study, bleeding was defined as clinically evident hemorrhage from the umbilical catheter insertion site occurring during or after catheter placement that required local pressure, additional suturing, or other medical intervention. Failure of the procedure and the number of chest radiographs needed to confirm proper placement of the UVC were noted.
Part 2: Prospective observation of real-time ultrasound guidance for UVC placement
After being trained and gaining experience in ultrasound skills for UVC insertion, and after attending certified courses to perform neonatal echocardiography, we proceeded with UVC insertion using real-time ultrasound guidance according to the research protocol.
The ideal position of the umbilical venous catheter tip was defined differently according to the method of confirmation. For radiographic confirmation, the correct catheter position was defined as the catheter tip located between the seventh and ninth thoracic vertebrae (T7–T9), corresponding to the inferior vena cava–right atrium junction. For ultrasound confirmation, the ideal position was defined as direct visualization of the catheter tip at the junction of the inferior vena cava and the right atrium.
Part 3: Follow-up after one month for complications
During the one-month follow-up period, neonates were evaluated for complications related to UVC insertion, including hepatic injury, portal venous air, thrombosis, splenic abnormalities, and catheter-related infection.
Study outcomes
The primary outcome was accurate positioning of the UVC tip in the standard central venous location (T7–T9) as confirmed by chest radiography. Secondary outcomes included the procedure time until suturing of the catheter, the procedure time until chest X-ray confirmation, the number of manipulations, meaning any additional adjustment of the catheter after initial insertion, including advancement, withdrawal, or repositioning prior to final confirmation, required during catheter insertion, the number of chest radiographs required to confirm catheter position, and procedure-related complications.
Ethics consideration
Informed consent was obtained from parents or legal guardians of patients before enrollment in the study. The study protocol was approved by the local ethics committee of the Faculty of Medicine, Ain Shams University (FWA 000017585).
Statistical analysis
Recorded data were analyzed using the Statistical Package for social sciences, version 23.0 (SPSS Inc., Chicago, Illinois, USA). The quantitative data were presented as mean ± standard deviation and ranges when their distribution was parametric (normal) while non-normally distributed variables (non-parametric data) were presented as median with interquartile range (IQR). Qualitative variables were presented as number and percentages. Data were explored for normality using the Kolmogorov–Smirnov and Shapiro–Wilk tests.
The following tests were done
Independent-samples t-test was used when comparing between two means. The Mann–Whitney U test: for two-group comparisons in non-parametric data. The comparison between groups with qualitative data were done using the chi-square test and Fisher’s exact test instead of the chi-square test only when the expected count in any cell was less than 5.





Results
Maternal data for both the US-Guided Group and the non-US-Guided Group.
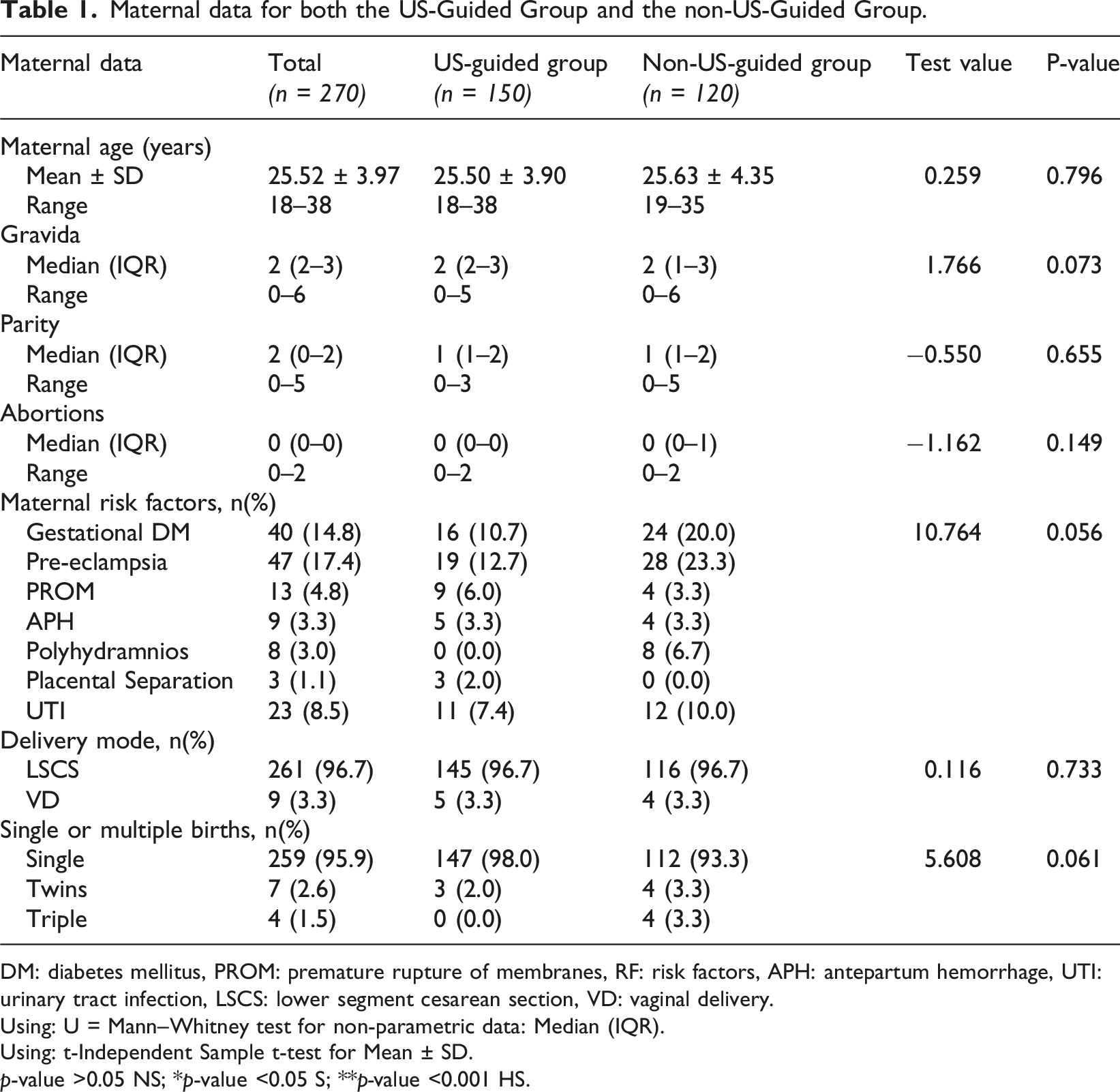
DM: diabetes mellitus, PROM: premature rupture of membranes, RF: risk factors, APH: antepartum hemorrhage, UTI: urinary tract infection, LSCS: lower segment cesarean section, VD: vaginal delivery.
Using: U = Mann–Whitney test for non-parametric data: Median (IQR).
Using: t-Independent Sample t-test for Mean ± SD.
p-value >0.05 NS; *p-value <0.05 S; **p-value <0.001 HS.
Neonatal data for both the US-Guided Group and the non-US-Guided Group.

GA: gestational age.
Using: t-Independent Sample t-test for Mean ± SD.
Using: x2: Chi-square test for number (%) or Fisher’s exact test, when appropriate.
p-value > 0.05 NS; *p-value <0.05 S; **p-value < 0.001 HS.
Procedure-related characteristics in ultrasound-guided and non–ultrasound-guided groups.
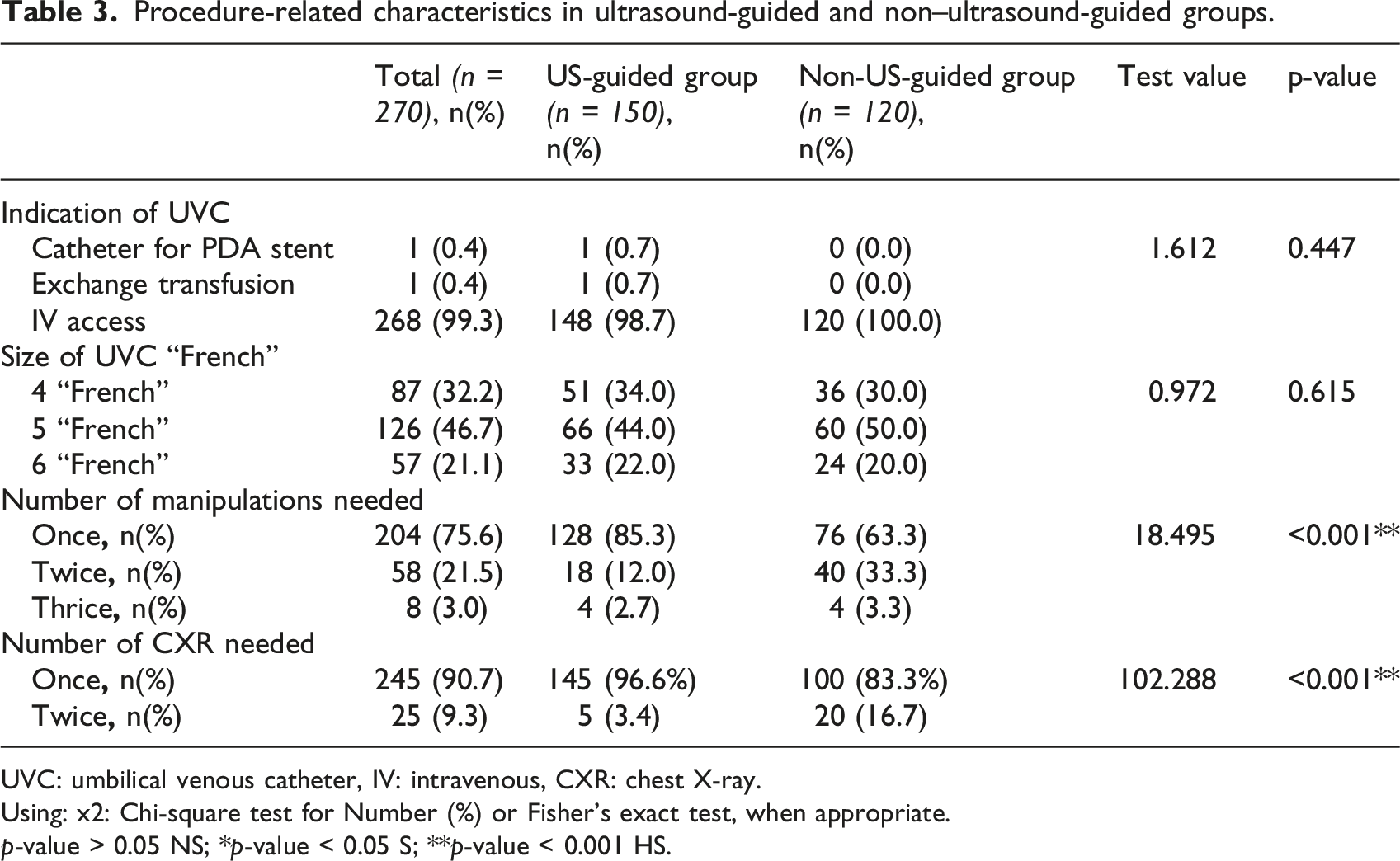
UVC: umbilical venous catheter, IV: intravenous, CXR: chest X-ray.
Using: x2: Chi-square test for Number (%) or Fisher’s exact test, when appropriate.
p-value > 0.05 NS; *p-value < 0.05 S; **p-value < 0.001 HS.
Procedure time comparison between groups.
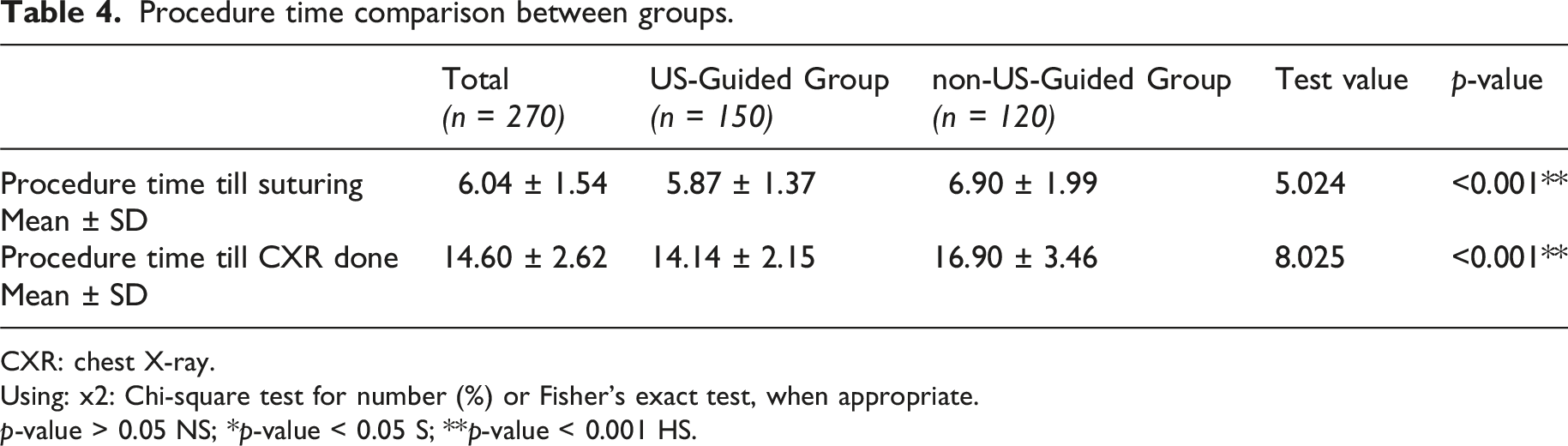
CXR: chest X-ray.
Using: x2: Chi-square test for number (%) or Fisher’s exact test, when appropriate.
p-value > 0.05 NS; *p-value < 0.05 S; **p-value < 0.001 HS.
Level of UVC in CXR (thoracic vertebrae number) in both US-Guided Group and non-US-Guided Group.
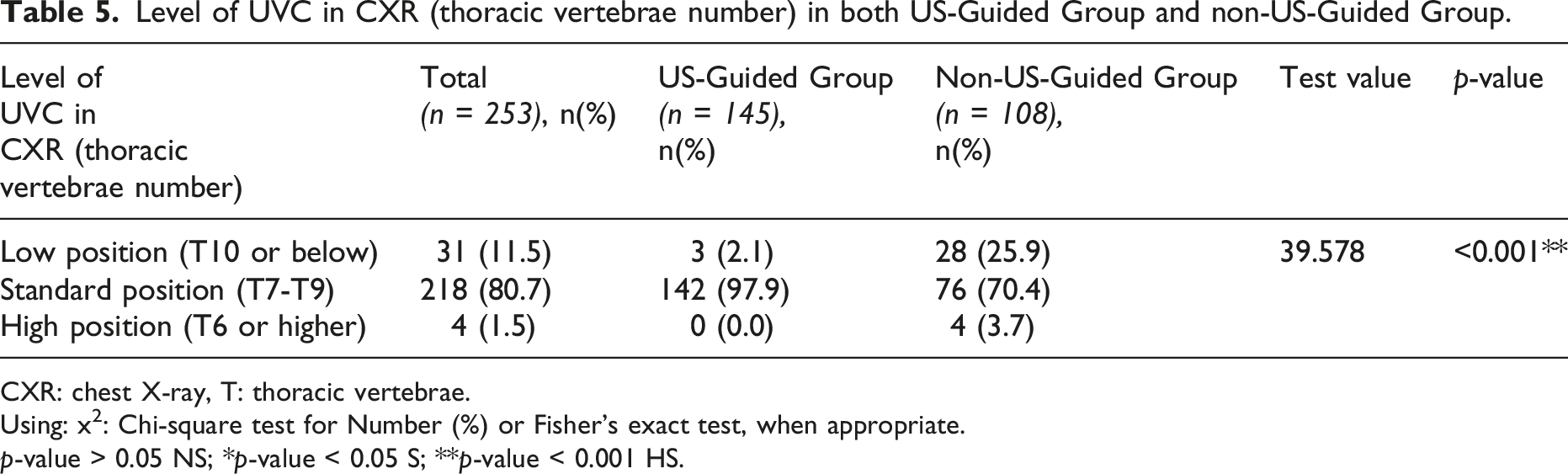
CXR: chest X-ray, T: thoracic vertebrae.
Using: x2: Chi-square test for Number (%) or Fisher’s exact test, when appropriate.
p-value > 0.05 NS; *p-value < 0.05 S; **p-value < 0.001 HS.
Figure 5 shows that ultrasound had a sensitivity of 95.2%, a specificity of 60.0%, PPV 98.6%, NPV 30.0%, and an accuracy of 94.0% in determining the UVC tip position. The sensitivity and specificity of USG compared with CXR for localization of the tip position of UVC.
UVC insertion was attempted in all 270 neonates. In some cases, initial catheter advancement resulted in malposition within the portal venous system, and repositioning or reinsertion was performed until the desired catheter position was achieved.
Discussion
Umbilical venous catheterization remains one of the most commonly used methods for central venous access in the neonatal intensive care unit. Accurate catheter tip positioning is critical to minimize complications such as thrombosis, arrhythmia, hepatic injury, and cardiac tamponade. Traditionally, catheter position is confirmed using radiography; however, this approach may delay confirmation, require repeated imaging, and expose neonates to cumulative radiation. Therefore, alternative methods that allow rapid, accurate, and radiation-free confirmation are of significant clinical importance. 4
Although previous studies have demonstrated the utility of ultrasound in confirming UVC position, the present study provides additional clinically relevant insights. In addition to comparing ultrasound and radiographic confirmation, this study evaluated diagnostic performance parameters, including sensitivity, specificity, positive predictive value, and negative predictive value. Furthermore, procedural efficiency was assessed through procedure time, number of manipulations, and number of radiographs required. Importantly, a one-month follow-up ultrasonographic assessment was performed to evaluate potential complications, which is less frequently addressed in similar studies. These elements collectively provide a more comprehensive evaluation of both the diagnostic accuracy and the short-term clinical impact of ultrasound-guided UVC placement.
Our study compares catheter insertion using the standard technique with the ultrasound-guided technique. One hundred and twenty in the non-US-guided group and 150 cases in the US-guided group. Both groups were comparable regarding maternal and neonatal characteristics.
The present findings demonstrate that the time to suturing and the time to chest X-ray confirmation were significantly shorter in the ultrasound-guided group than in the non–ultrasound-guided group. This finding may be explained by the higher rate of optimal catheter positioning on the first attempt in the ultrasound group, which reduced the need for repeated catheter manipulations and repositioning.
Our findings, demonstrating improved catheter positioning and reduced procedure time with ultrasound guidance, are consistent with the results reported by Kaur et al. This improvement may be explained by the ability of real-time ultrasound to directly visualize the catheter tip during insertion, allowing operators to adjust catheter advancement immediately and reducing the need for repeated manipulations. Consequently, the procedure becomes more efficient, and the likelihood of optimal catheter placement on the first attempt increases. 5
In contrast, Mishra et al. conducted a recent study in which the mean procedure time in the ultrasound-guided group and the blind insertion group was 8.9 and 8.3 min, respectively, with no statistically significant difference between the two groups (p = 0.56). 6 Unlike that study, our results demonstrated a statistically significant reduction in procedure time when ultrasound guidance was used.
Moreover, 85.3% of neonates in our study required only one attempt to insert UVC in the ultrasound-guided group, whereas it was 63.3% in the non–ultrasound-guided group, with P-value 0.012. Similarly, in Patel et al., Study (2022) 71% of umbilical venous catheters were inserted using a single attempt in the non–ultrasound-guided group. 7
Regarding the number of X-rays required to confirm catheter position, 96.6% of cases in the US-Guided Group needed only one X-ray compared to 83.3% needed one X-ray in the non-US-Guided Group, with a p-value (p = 0.004), in similar study, ultrasound use led to a reduction in additional X-ray exposure in the US group (n = 11) compared to the non–ultrasound group (n = 20) (p = 0.020). 5
Regarding catheter tip position, 97.9% of catheters guided by ultrasound were in the normal position (central venous) compared with 90% in the non-US-guided Group, although this difference was not statistically significant.
Additionally, US-guided UVC insertion showed that 98% of catheters were in the standard position (from T7 to T9), 2% were in the low position (T10 and below) and none were in the deep position (T6 and above), whereas in the non–ultrasound-guided UVC insertion group, 70.3% of catheters were in the standard position, 26% were in the low position, and 3.7% were in the deep position. On the other side Goh et al., study (2021) the UVC was in an ideal position in 25.0%, deep in 12.0% and low in 32.4% of neonates.
D'Andrea et al., 2024 compared real-time ultrasound and traditional X-ray methods for assessing umbilical venous catheter tip location in 461 cases and showed that ultrasound-guided tip location was found to be more reliable and efficient, demonstrating a significantly lower incidence of primary malpositioning compared with X-ray assessments (9.6 vs 75.9%). The multiple logistic regression showed a high probability of the central safe position of the umbilical venous catheter tip using real-time ultrasound tip location (odds ratio 29.5, 95% confidence interval: 17.4–49.4). 8
These results indicate that ultrasound-guided insertion of UVC had a sensitivity of 95.2% (90.4%–99.9%), a specificity of 60.0% (57.0%–63.0%), a PPV 98.6% (96.6%–100.0%), a NPV 30.0% (28.5%–31.5%), and an accuracy of 94.0% (89.3%–98.7%) in determining the UVC tip position. In Michel et al., (2012) study conducted on 60 neonates reported a sensitivity and specificity for ultrasound in localizing the UVC tip of 96.4% and 93.9% for US. 9
In another study, it showed that out of 112 enrolled neonates, 58 were in the ultrasound-guided group and 54 in the blind group, the sensitivity and specificity of ultrasound in detecting the correct position of the catheter tip were 96.9 and 46.8%, respectively. 10
The present findings demonstrate that the mean time of UVC duration was 8.64 ± 2.31days. In Hess et al. study comparing dwell time of umbilical venous catheters in 63 neonate, 31 with umbilical venous catheter dwell time between 1 and 7 days (control group) and 32 patients with umbilical venous catheter dwell time (intervention group) between 8 and 14 days. The results showed that longer UVC dwell time of up to 14 days significantly decreased the number of painful invasive vascular procedures and radiation exposure, and shortened the length of the hospital stay. 11
In this study, one-month follow-up pelvi-abdominal ultrasonography was normal in 98% of cases, while 3 cases showed complications (hepatic and splenic air foci, portal vein air foci, and splenomegaly). Unlike Mutlu et al. (2016) conducted a study on 974 newborns with umbilical venous catheters, UVC related complications developed in 198 patients (20.3%). He related this relatively high percentage of complications to the lack of ultrasound guidance. Similar to Mutlu et al., in other study, in which 108 patients had UVC insertions without using ultrasonography, complications occurred in 25% of patients; venous thrombosis occurred in 1.9%. 12
Although several previous studies have evaluated the role of ultrasound in confirming the position of umbilical venous catheters, the present study provides additional clinical insights. First, this study included a relatively large prospective cohort of neonates and evaluated multiple procedural and diagnostic parameters simultaneously. Second, the diagnostic performance of ultrasound was assessed using sensitivity, specificity, positive predictive value, and negative predictive value, in comparison with conventional radiography. Third, our study incorporated a one-month follow-up ultrasonographic evaluation to identify possible complications related to catheter placement, which is less frequently reported in similar studies. These aspects provide further evidence regarding not only the accuracy of ultrasound for catheter localization but also its clinical impact on procedural efficiency, radiation exposure, and short-term safety outcomes in neonates. Despite moderate specificity, the high sensitivity and PPV suggest that ultrasound is reliable for confirming correct placement, though caution is needed when ruling out malposition.
Limitations of the study
This study has some limitations. First, it was conducted in a single tertiary center, which may limit the generalizability of the results. In addition, inter-observer variability for ultrasound interpretation was not formally assessed. Although ultrasound examinations were performed by a neonatologist trained in neonatal echocardiography, evaluation of agreement between independent observers would further strengthen the reproducibility of ultrasound in determining the UVC tip position.
Conclusion
This study demonstrates that ultrasound-guided umbilical venous catheter insertion provides accurate catheter localization with high diagnostic sensitivity while reducing procedure time, catheter manipulations, and the need for repeated radiographic confirmation. In addition to confirming previously reported advantages, this study contributes further clinical evidence by evaluating diagnostic performance and short-term safety outcomes through follow-up assessment. These findings suggest that ultrasound may be a reliable adjunct for UVC placement, though further multicenter studies are warranted.
Footnotes
Acknowledgments
The authors are deeply grateful to the guardians of the neonates who agreed to participate in the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Human research statement
The Declaration of Helsinki’s guiding principles were followed in the conduct of this investigation. Approval was granted by the Research Ethics Committee (REC) at the Faculty of Medicine, Ain Shams University (Reg. No. FWA 000017585).