
Abstract
Background
Maternal mirror syndrome is a rare pregnancy complication causing maternal edema that mirrors that of a hydropic fetus. Isolated fetal ascites is also uncommon and has multiple possible etiologies, and has not traditionally been associated with maternal mirror syndrome.
Case report
We present a case of “atypical maternal mirror syndrome” in a fetus with isolated abdominal ascites to illustrate the possibility of mirror syndrome without fetal hydrops. A 32-year-old G1P0 had an ultrasound revealing significant fetal abdominal ascites with incompletely visualized fetal bladder dome. The patient developed pulmonary edema with oxygen requirements and underwent preterm delivery due to concern for mirror syndrome. The neonatal ascites was suspected to be secondary to bladder outlet obstruction due to hydrometrocolpos from an imperforate hymen. Although the fetus was not hydropic, our patient developed pulmonary edema, hemodilution, and maternal weight gain, and recovered quickly after delivery, many features of maternal mirror syndrome.
Conclusion
This case illustrates an atypical presentation of maternal mirror syndrome in the setting of isolated fetal ascites rather than fetal hydrops. With the significant maternal and fetal morbidity associated with maternal mirror syndrome, clinicians should consider maternal mirror syndrome as a possible diagnosis even in the absence of fetal hydrops.
Introduction
Maternal mirror syndrome (MMS) describes maternal edema that “mirrors” edema of a hydropic fetus, and may occur with immune- and non-immune-mediated hydrops.1–3 Although not well-elucidated, the pathogenesis appears related to trophoblastic damage and maternal vascular endothelial dysfunction leading to fluid extravasation, possibly representing a form of preeclampsia with preeclampsia reported in up to 50% of cases.2,4 Increases in placental growth factor (PIGF) and soluble Fms-like tyrosine kinase 1 (sFlt-1) has also been proposed as a cause of MMS similar to in preeclampsia, leading to the endothelial and vascular dysfunction; however, further investigation of these markers as diagnostic tools is needed. 1 MMS is likely underdiagnosed due to the similarities to preeclampsia and ill-defined diagnostic criteria, and the incidence is unclear1,2; however, a 2010 systematic review reported 56 cases between 1956 and 2009.3,4 MMS has traditionally been associated with fetal hydrops, with a majority reported to be secondary to severe rhesus isoimmunization (29%), 3 and has not been reported in the setting of isolated fetal abdominal ascites, which alone does not meet the diagnostic criteria for fetal hydrops. (In this patient case, we use the term “isolated fetal ascites” to describe the abnormal presence of fluid within the fetal abdomen alone, as opposed to fluid collections in the abdomen in addition to other compartments, which would be indicative of fetal hydrops. Our use of “isolated fetal ascites” does not preclude the presence of other abnormal findings. We also use the term “atypical MMS” as MMS is associated with fetal hydrops rather than isolated fetal ascites).
We present a case of atypical MMS with a fetus with isolated ascites, and urge providers to consider MMS even in atypical clinical scenarios given the increased fetal mortality and maternal morbidity associated with MMS. The patient provided both verbal and written informed consent prior to preparation of this manuscript.
Case report
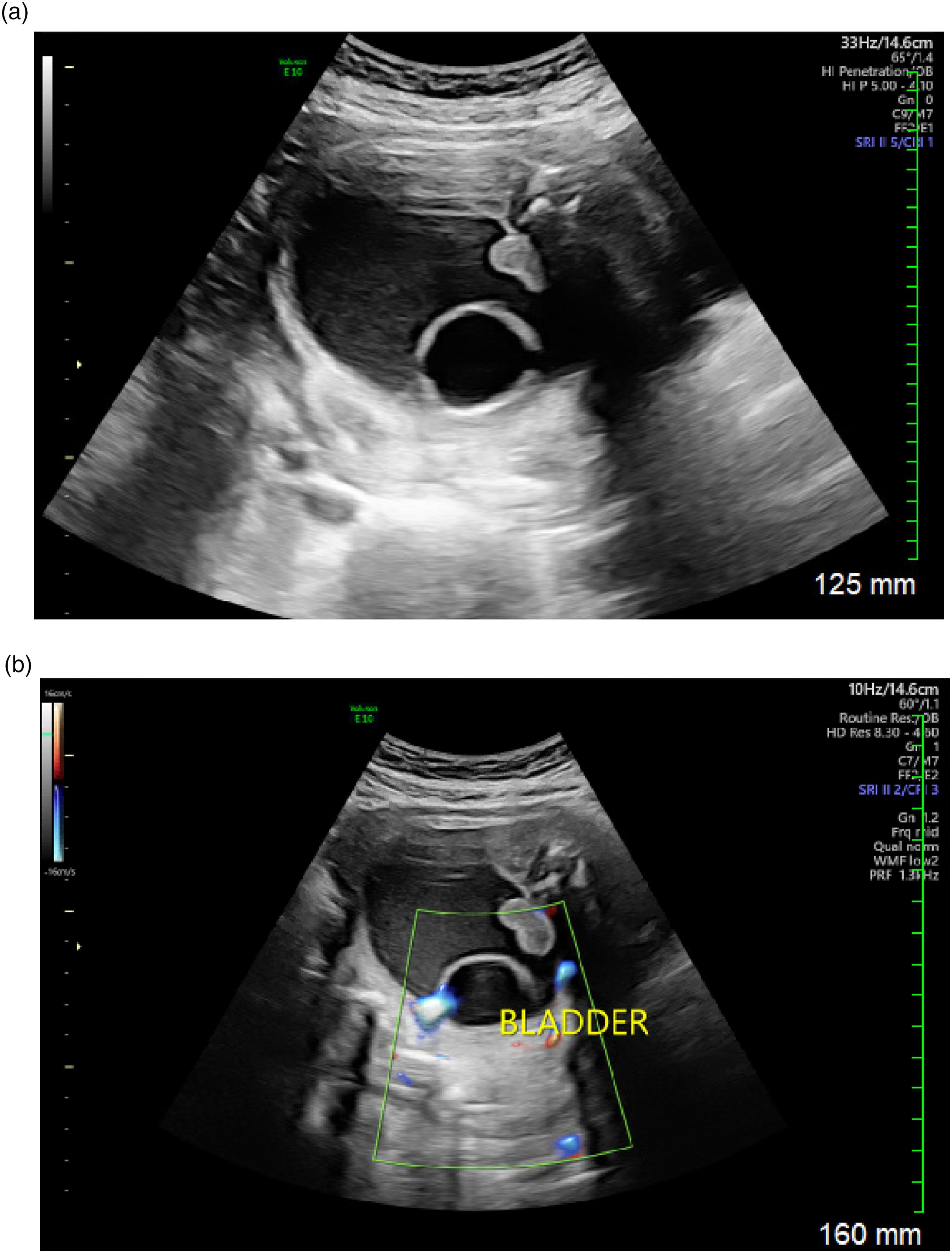
A 32-year-old G1P0 with a female fetus was referred to our institution for a detailed anatomical survey at 20 weeks gestation, indicated for elevated alpha-fetoprotein (3.05 MoM) and single umbilical artery. The patient was healthy without other notable medical history or family history of genetic disorders. Ultrasound revealed normal anatomy, estimated fetal weight of 329 g, and maximum vertical pocket (MVP) of 4.39 cm. At 28 weeks, the patient was re-referred following a growth scan with new fetal ascites at 27 weeks, 6 days. Repeat ultrasound revealed fetal abdominal ascites with oligohydramnios (MVP 1.39 cm). Abdominal circumference was greater than the 98th percentile (Figure 1), with other biometry measurements 50–65th percentile. Middle cerebral artery Doppler peak systolic velocity was normal (1.47 MoM). No scalp edema, skin thickening, or placentomegaly were present. Despite lack of hydronephrosis and hydroureter, flow was seen through the fetal bladder wall and an incompletely visualized bladder dome, suspicious for partial bladder rupture (Figures 2(a) and (b)). Bladder not decompressed, with the bladder wall thickened and echogenic, further supporting concern for partial fetal bladder rupture. Amniocentesis was offered to evaluate aneuploidy, inborn errors of metabolism, and fetal TORCH infections. Fetal paracentesis was also considered for evaluation of fetal ascitic fluid. Both were deferred due to patient desire to instead pursue less invasive initial testing. Ultrasound performed at 28w0d with significant fetal abdominal ascites. (a) Ultrasound performed at 28w0d with possible partial fetal bladder dome rupture, (b) Ultrasound performed at 28w0d with possible flow through the partial fetal bladder dome rupture.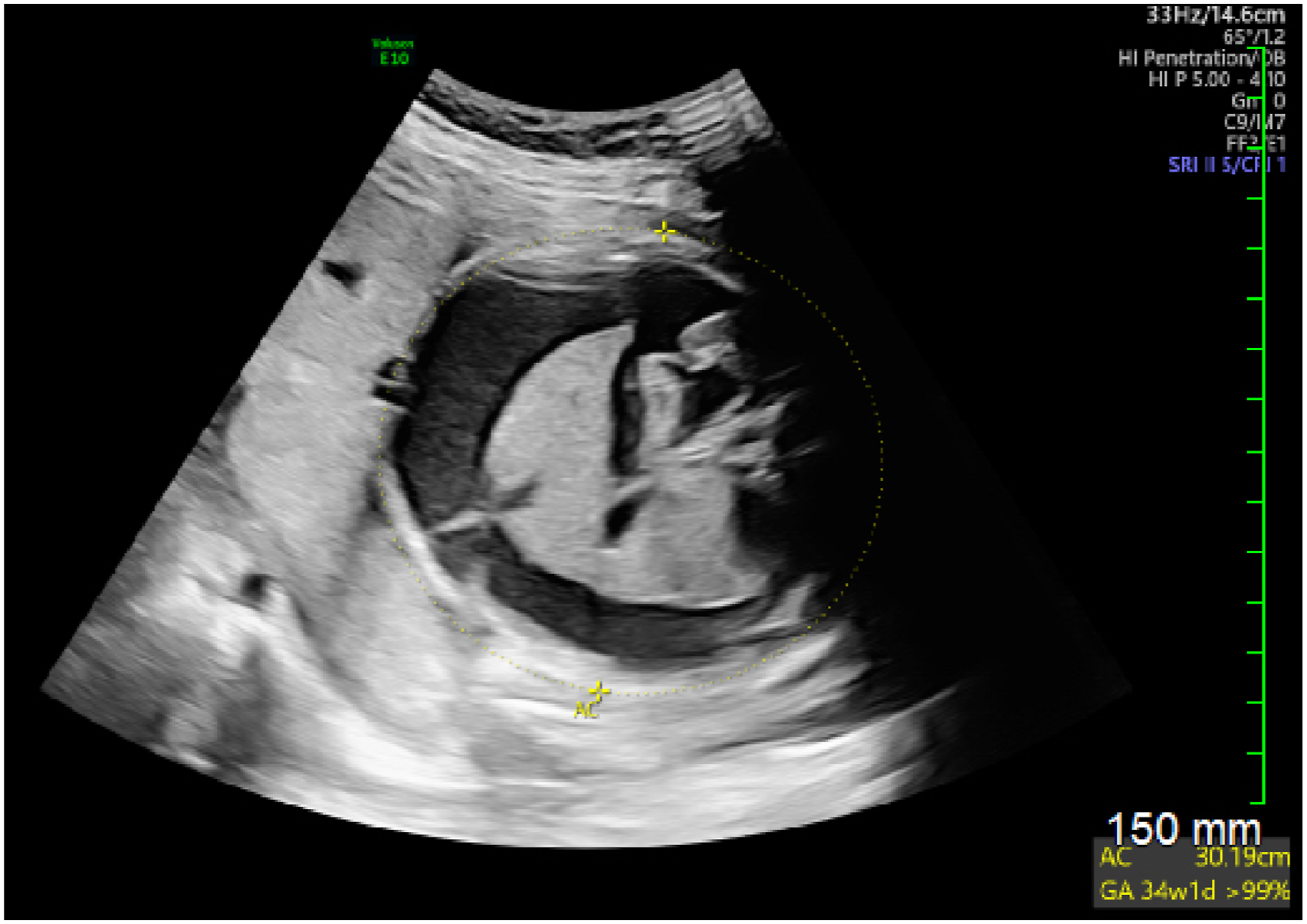
At 28 weeks, 0 days, the patient was admitted for fetal monitoring and hydrops workup, which was negative for infections (maternal serum testing for parvovirus, syphilis, rubella, toxoplasmosis, cytomegalovirus) and alloimmunization (maternal blood type A+, negative antibody screen, negative direct Coombs). Her blood pressure was 119/60 on admission and remained normotensive. Admission labs were notable for a low hemoglobin of 9.9 g/dL and hematocrit of 30.4%. Other serum preeclampsia labs were normal (platelets 193 × 103/mcL, AST 14 IU/L, ALT 27 IU/L, creatinine 0.50 mg/dL). She weighed 84.05 kg. She received betamethasone for fetal lung maturity and was discharged on hospital day 3 at 28 weeks, 2 days.
The next day, at 28 weeks, 3 days, the patient re-presented with chest pressure. She had a nonreactive NST and 6/10 biophysical profile (−2 for nonreactive tracing, −2 for oligohydramnios), and was admitted for further evaluation. Hemoglobin was 8.7 g/dL, hematocrit 27.4%, platelets 167 × 103/mcL, and the patient weighed 85 kg on admission. She had a normal electrocardiogram, negative troponin level, and was normotensive.
At 28 weeks, 4 days, she developed an oxygen requirement (92% on room air) of 1 L/min to maintain 95% oxygen saturation. Chest X-ray revealed bilateral pleural effusions with pulmonary vascular congestion (Figure 3), without evidence of pulmonary embolism on computed tomography pulmonary angiogram. Repeat bedside pregnancy ultrasound by two separate maternal fetal-medicine specialists noted a similar degree of fetal ascites and oligohydramnios unchanged from the prior ultrasound from 28 weeks. However, it was noted that the patient had gained 3.81 kg from the day prior, now weighing 88.81 kg. The patient also had worsening hemodilution with hemoglobin 8.6 g/dL and hematocrit 26.1%. The patient had increasing oxygen requirements (3 L/min of oxygen) with, and elevated brain natriuretic peptide of 661 pg/mL (normal <100 pg/mL). Bedside echocardiography performed by cardiology demonstrated mild mitral regurgitation without ventricular dysfunction, pulmonary hypertension, or wall motion abnormalities, ruling out peripartum cardiomyopathy. The elevated brain natriuretic peptide was attributed to non-cardiogenic pulmonary edema and fluid overload. The patient received 40 mg of IV furosemide with output of 2450 cc (300 cc/hr) to treat pulmonary edema without improvement in dyspnea or oxygen saturation. Despite a mild increase in ALT (55IU/L, laboratory upper limit of normal 40IU/L), other preeclampsia labs remained normal (creatinine 0.51 mg/dL, AST 19IU/L, platelets 155 × 103/mcL, urinary protein:creatinine undetectable before furosemide) and the patient remained normotensive. Given the lack of clinical improvement in respiratory function despite diuresis, there was increased concern for atypical preeclampsia versus MMS and the decision was made to proceed with delivery. With the rapid change in clinical presentation of the patient despite stable fetal ultrasound findings, it was determined that a therapeutic paracentesis to treat MMS would have delayed reversal of her pulmonary edema, putting the patient at further risk. She was started on magnesium sulfate for fetal neuroprotection and underwent an uncomplicated primary cesarean at 28 weeks, 5 days gestation. Maternal chest X-ray performed at 28w5d with persistent bibasilar airspace disease with central pulmonary vascular congestion.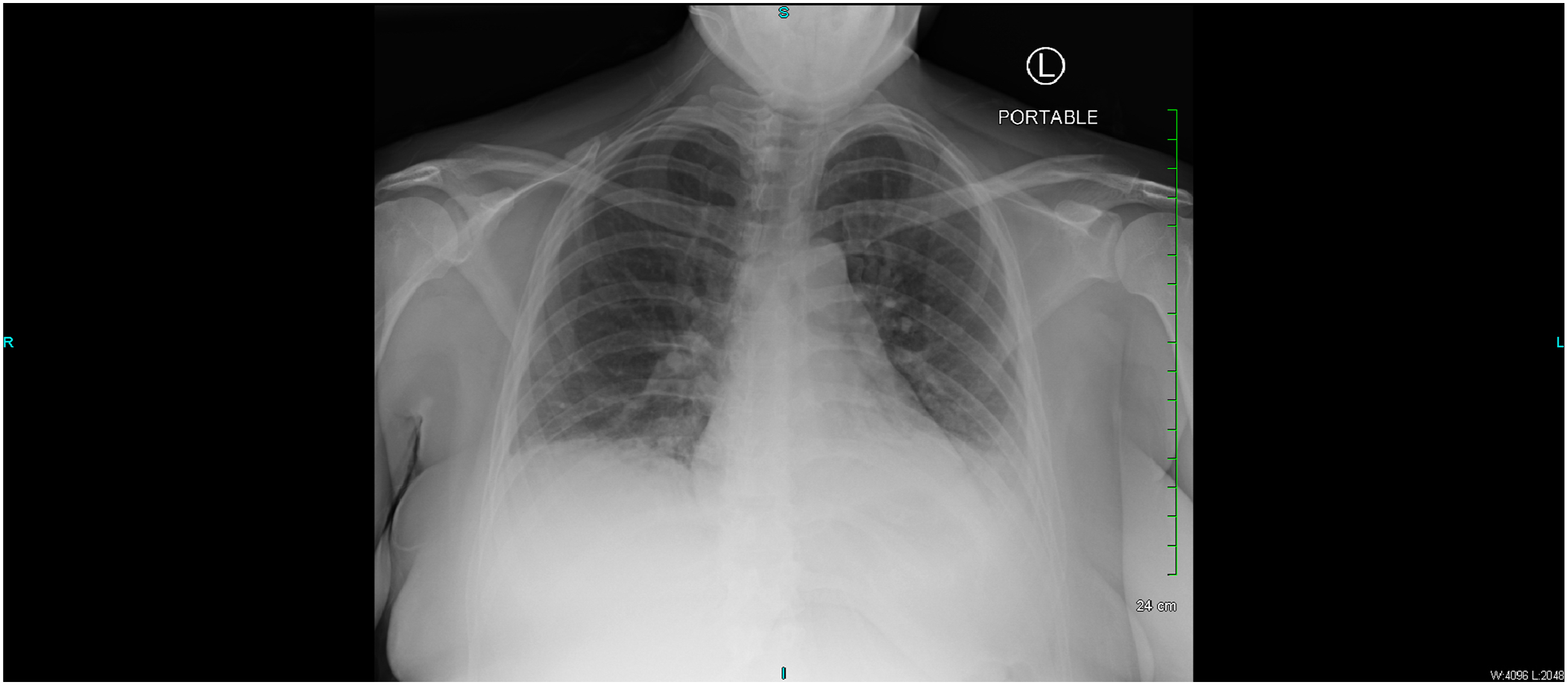
Postoperatively, the patient’s oxygen requirement was resolved immediately after delivery and she remained stable on room air. On postoperative day 0, she had a single elevated non-severe range blood pressure of 148/84 but was otherwise normotensive. With the immediate resolution of respiratory distress after delivery with preceding unexplained pulmonary edema, hemodilution, and maternal weight gain, and without meeting criteria for preeclampsia, the patient was diagnosed with MMS. On postoperative day 1, hemodilution had improved with hemoglobin of 9.2 g/dL, hematocrit of 27.2%, and platelets of 208 × 103/mcL. Postpartum course was otherwise uncomplicated and she was discharged on postoperative day 4.
The viable female infant was delivered weighing 1640g with APGAR score of 7 at five minutes of life. The infant was intubated immediately after delivery for respiratory distress. On day of life (DOL) 0, the infant underwent an abdominal paracentesis, draining 70 mL of clear yellow ascites, with improvement in respiratory function. Urinary foley was placed with return of clear yellow urine, and imperforate hymen with purple vaginal bulge was noted on physical exam. Abdominal ultrasound revealed hematometrocolpos, which had not been previously visualized on prenatal ultrasound. Hymenectomy was performed with drainage of 6 mL of clear fluid. Voiding cystourethrogram (VCUG) was delayed until the infant was stabilized on day of life 7, and showed no signs of bladder rupture or fistula. Urinary creatinine resulted at 6.4 mg/dL, ascitic creatinine 0.8 mg/dL, and hydrocolpos creatinine 3.7 mg/dL. Given that the ascitic creatinine was lower than vaginal creatinine, it is suspected that the bladder ruptured remote to delivery, with low ascitic creatinine due to absorption of creatinine through the small bowel similar to peritoneal dialysis. With the intentional delay in obtaining the VCUG, the pediatric urology team suspected that the early bladder rupture likely healed before the exam.
The infant underwent additional testing including cultures (blood, hydrocolpos fluid, and ascitic fluid) which were negative and a complete blood count to screen for infection and anemia, which were normal. Genetic microarray screening was normal, with expanded renal panel revealing one pathogenic variant in CYP11B2 (associated with autosomal recessive aldosterone synthase deficiency; infant is a carrier), a variant of uncertain significance in LMX1B (associated with autosomal dominant nail-patella syndrome and focal segmental glomerulosclerosis), and a variant of uncertain significance in SLC4A1 (associated with autosomal dominant distal renal tubular acidosis, autosomal recessive distal renal tubular acidosis with hemolytic anemia, autosomal dominant Southeast Asian ovalocytosis, and autosomal dominant hereditary stomatocytosis). Both echocardiography and cranial ultrasound was performed for the infant to rule out congenital anomalies. Echocardiography was performed on DOL 1 revealing a small patent ductus arteriosus and mildly elevated right ventricular pressures, with repeat echocardiography at DOL 40 without abnormal findings. Cranial ultrasound was also performed on DOL 1 and repeated on DOL 7, both of which were normal.
Final suspected diagnosis was bladder outlet obstruction and rupture, due to hydrometrocolpos secondary to imperforate hymen, causing subsequent fetal ascites and oligohydramnios. Spontaneous resolution occurred during the infant’s first 7 days of life with urinary foley in place which allowed for bladder decompression and healing. The neonate recovered well postnatally and was discharged home in stable condition on day of life 86.
Discussion
Isolated fetal ascites with oligohydramnios is a rare finding on prenatal ultrasound, and the etiology is most predictive of outcome. It is important to consider a wide differential when investigating the cause of isolated fetal ascites as it may not be evident even postnatally. In a 2021 systematic review of 315 cases of isolated fetal ascites, 93.4% did not progress to hydrops, and the most common etiologies were genitourinary (24%) and gastrointestinal (20%), which have the best prognosis. 1 When assessing isolated fetal ascites, the causes of fetal hydrops should also be explored due to the small but potential possibility of progression to hydrops. Fetal hydrops is defined as the presence of pathological fluid collection in at least two areas (i.e., ascites, pleural effusions, pericardial effusions, and skin edema). Non-immune causes of fetal hydrops are diverse and include cardiovascular abnormalities (20% of cases) and chromosomal abnormalities (13%) amongst the most common. When fetal hydrops is suspected, several etiologies may be diagnosed at the time of diagnosis of hydrops based on ultrasound findings (i.e., twin-to-twin transfusion syndrome, cardiac arrhythmias, and structural anomalies). In an otherwise structurally normal fetus, alloimmunization must be ruled out as well as infectious causes (syphilis, cytomegalovirus, and toxoplasmosis).2,5
In this case, the cause was suspected to be bladder rupture secondary to an outlet obstruction due to a distended uterus caused by an imperforate hymen. The infant recovered appropriately after drainage of the ascites and hydrometrocolpos, and hymenectomy. Prenatal diagnosis remains challenging; there was no clear evidence of bladder rupture antenatally without prior hydronephrosis or hydroureter, which may have resolved before additional imaging, and thus the diagnosis of hydrometrocolpos causing urinary obstruction leading to bladder rupture and ascites is presumptive.
This case was also significant for atypical MMS. Common maternal syndrome symptoms include weight gain/edema (89%), hypertension (61%), proteinuria (43%), elevated uric acid/creatinine (25%), elevated liver enzymes (20%), and headache/visual disturbances (14%), with major morbidity from pulmonary edema (21%). 3 Given these symptoms, it may be difficult to distinguish between preeclampsia and MMS. MMS has been posited to be secondary to vascular endothelial dysfunction; however, it is not well understood why certain patients develop MMS while others do not in the setting of fetal hydrops, and further research is required to elucidate the underlying pathophysiology. MMS also resolves soon after treatment of fetal hydrops, or after delivery. 3 Thus, it is prudent to weigh the risks and benefits of an iatrogenic preterm birth or urgent treatment of fetal hydrops, with maternal symptom management.
In regards to our patient, atypical preeclampsia was excluded as the patient remained normotensive aside from a single elevated non-severe range blood pressure, and had no laboratory evidence of preeclampsia. Despite the mild increase in ALT and decrease to low-normal platelet levels, these lab values did not meet diagnostic criteria for preeclampsia, and remained in a normal range after delivery. Although the fetus was not hydropic, the patient developed rapid onset, progressive pulmonary edema in addition to hemodilution (as evidenced by the progressively decreasing hemoglobin and hematocrit, with hematocrit at a nadir of 27.4% which meets prior proposed hemodilution definitions of hematocrit below 35% in MMS 2 ) as well as maternal weight gain (with a maximum of 4.76 kg over the course of 4 days, greater than the 1 kg per week previously proposed as a criteria for MMS2,4), both of which are commonly associated with MMS rather than preeclampsia. Notably, hemodilution has been proposed as a differentiating characteristic of MMS when compared to preeclampsia, as preeclampsia is typically associated with hemoconcentration. 2 Thus, MMS was determined to be the most likely cause of progressive pulmonary edema rather than atypical preeclampsia. Our patient had rapidly increasing oxygen requirements, increasing her risk of worsening morbidity, thus necessitating urgent delivery. Ultimately, her symptoms resolved immediately after delivery, as is typical with MMS, and her neonate had an uncomplicated hospital course with treatment of imperforate hymen, the suspected primary etiology of the ascites.
With the lack of diagnostic criteria surrounding MMS, we propose a possible set of diagnostic criteria: hemodilution (with either a new hematocrit of <35% with previously normal hematocrit, or progressively decreasing hematocrit with previously low hematocrit), maternal edema (with weight gain >1 kg per week or evidence of fluid retention such as pleural effusions, pulmonary edema, skin edema, or pathologic accumulation of fluid in other body cavities), and fetal hydrops (with pathologic fluid accumulation in at least two fetal compartments). We propose expanding this definition to include atypical MMS with hemodilution and maternal edema, without fetal hydrops and instead with pathologic fluid accumulation in one fetal compartment. Overlap with preeclampsia may occur with elevated blood pressures or other lab abnormalities; however, this is not required for diagnosis of MMS. Other suggestive findings may include preeclampsia as well as placental edema or placentomegaly.
Fetal therapy may have a role in prolonging pregnancies affected by MMS and decreasing perinatal morbidity associated with significant hydrops and iatrogenic preterm delivery. Sichitiu et al. describes use of fetal intervention with fetal shunt placement, laser ablation for TTTS, and intrauterine blood transfusion for treatment of underlying causes of fetal hydrops and/or placentomegaly as a method of preventing and treating MMS. In this study, 38% of cases treated with fetal intervention led to resolution of MMS symptoms, with a mean time to resolution of 13.1 days. 6 For a stable patient with slowly progressing MMS symptoms, fetal intervention can be considered. In our case, the patient had rapidly progressive pulmonary edema refractory to treatment with diuretics, making delivery rather than fetal therapy the more appropriate treatment.
Strengths of the approach to this case including close monitoring and comprehensive work up after initial diagnosis of fetal ascites. This allowed for early diagnosis of suspected MMS and management, as well as optimization with betamethasone for fetal lung maturity prior to preterm delivery. There was close collaboration of the maternal fetal-medicine team with the neonatology team as well as involvement of pediatric urology to determine likely etiology of fetal ascites. Limitations include the speculative nature of the diagnosis of bladder rupture as there was no official antenatal diagnosis nor evidence of rupture postnatally in the setting of the intentionally delayed VCUG. Furthermore, therapeutic paracentesis of the fetus was not considered antenatally given stability and patient desires; however, this may have potentially delayed onset of MMS symptoms.
There have not previously been published cases of MMS secondary to fetal ascites with an attributable cause. Hamdeh et al. reported a case of MMS secondary to idiopathic isolated fetal ascites. 7 Notably, outcomes of fetal ascites are most favorable for chylous ascites (100% survival) and idiopathic ascites (90%), with survival dropping to 77% for both gastrointestinal and genitourinary ascites. 8 Fortunately, the infant in our case recovered well postnatally without long-term sequelae or recurrence.
Conclusion
This case of MMS in the setting of isolated fetal ascites illustrates an atypical presentation as this is the first reported case of MMS secondary to isolated fetal ascites secondary to suspected fetal bladder rupture to our knowledge. This patient presented with isolated fetal ascites at 28 weeks gestation, with ultrasonic findings suggestive of bladder rupture and no other attributable cause antenatally. Due to rapidly progressing pulmonary edema in the setting of suspected MMS, delivery was performed via cesarean at 28 weeks, 5 days. Extensive postnatal examination was performed without other proposed causes of ascites, with suspected bladder rupture spontaneously healing by DOL 7. Both the patient and infant did well after delivery without long-term complications, with reversal of MMS and treatment of the infant’s ascites without recurrence. Given the significant potential complications as a result of MMS (including but not limited to ICU admission, cardiac failure, and renal or liver dysfunction), it is prudent to consider MMS as a diagnosis even in the absence of multicompartment fetal hydrops.
Footnotes
Consent to participate
Written informed consent was obtained from the patient prior to the preparation of this manuscript and all patient identifiers have been removed.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.