
Abstract
Introduction
This study aimed to evaluate the possible associations between specific fetal vascular malperfusion (FVM) findings—beyond standard high- and low-grade criteria—and fetal and neonatal clinical complications in a tertiary high-complexity hospital.
Methods
We conducted a retrospective, observational, descriptive cohort study of 706 placentas, correlating routine histological findings with maternal conditions and fetal and neonatal outcomes. Bivariate and multivariate logistic regression analyses were performed to explore potential associations between detailed microscopic features and clinical variables.
Results
A high frequency of FVM was observed in this high-risk population. Several histologic features were found to be associated with adverse perinatal outcomes, including cases classified as low-grade FVM. Similar patterns of association were observed between FVM and maternal pre-pregnancy conditions as well as gestational complications.
Discussion
Because FVM is typically diagnosed only after delivery, its clinical impact may be underrecognized. Our findings suggest a potential increased risk of neonatal and fetal complications in both low- and high-grade FVM. We highlight the importance of considering the temporal progression of fetal circulatory obstruction, from leukocyte stasis to calcified thrombi.
Introduction
Fetal vascular malperfusion (FVM) is a recently recognized placental pathological entity characterized by lesions affecting the fetal-placental circulation. 1 Given the direct vascular connection between the placenta and the fetal cardiovascular and neurological systems through the umbilical cord, alterations in this axis may have important clinical consequences. FVM has been associated with serious fetal and neonatal outcomes, primarily related to fetal hypoxia,2,3 including death, low Apgar score, fetal growth restriction (FGR), non-reassuring fetal status, low IQ, and both short- and long-term adverse neurological outcomes.4–7 In high-income countries, FVM has been implicated as a causal or contributing factor in approximately 15% of stillbirths. 8 However, its true prevalence remains uncertain. 9 At the histopathologic level, these clinical outcomes are thought to arise from impaired or obstructed fetal blood flow within the placental vascular tree, resulting in a heterogeneous spectrum of lesions. The distinction between high- and low-grade FVM is based on the extent and combination of these findings (detailed below). While high-grade FVM has been more clearly associated with adverse outcomes, the clinical significance of lower-grade or partial manifestations remains less well defined and may be underrecognized in routine placental evaluation. In this context, this study aimed to examine the associations between specific FVM findings and short-term fetal and neonatal clinical outcomes in a large cohort, with particular emphasis on the potential clinical relevance of FVM even when full high-grade criteria are not met.
Methods
Study design and ethical approval
We conducted a retrospective, observational, descriptive cohort study approved by the Institutional Research and Ethics Committee (FM-CIE0131-21). The study analyzed maternal and neonatal clinical data together with gross and microscopic placental findings from 706 consecutive cases recorded as part of routine clinical care and placental pathology evaluation at a single tertiary hospital. These data had been entered into REDCap, a secure web-based data capture platform, and were retrospectively analyzed for the present study.
Eligible cases included placentas obtained at delivery at HUSI and submitted for histopathologic evaluation in the Department of Pathology. Specimens without sufficient placental tissue for histopathologic diagnosis (e.g., products of conception/ovular remains) were excluded.
Study setting and population
The study population comprised high-risk pregnancies, as all patients were referred to our center for specialized high-risk obstetric care. The entire population of fetuses and newborns with available placental histopathology during the study period, thereby minimizing potential case selection bias. Because the full population was analyzed rather than a sample, a formal sample size calculation was not required.
Gestational age was categorized as follows: <20 weeks; 20–21 weeks (miscarriages); 22–23 weeks (extremely preterm births); 24–36 weeks (viable preterm births); 37–40 weeks (term births); and >40 weeks (post-term births). Term neonates (37–40 weeks) were used as the reference group for analysis.
Outcomes assessed
(1) Neonatal outcomes
Neonatal outcomes were grouped into the following categories: mortality, congenital anomalies, respiratory morbidity, adaptation and metabolic disorders, infectious outcomes, bilirubin disorders, and hematologic abnormalities. -Mortality: Neonatal death. -Congenital anomalies: Major congenital anomalies were defined as anomalies requiring medical or surgical treatment, associated with significant adverse effects on health or development, or resulting in major cosmetic impact. These conditions typically require early—sometimes urgent—management and may carry psychosocial consequences. Congenital anomalies were classified according to the coding guidelines of the European Surveillance of Congenital Anomalies (EUROCAT)
10
and ECLAMC (Latin American Collaborative Study of Congenital Malformations).
11
-Respiratory morbidity: Neonatal respiratory disorders was defined as a clinical condition characterized by impaired ventilation and increased work of breathing, identified by signs of respiratory effort and compromised gas exchange, including surfactant deficiency and disorders of neonatal cardiopulmonary transition.
12
-Adaptation and metabolic disorders: Low Apgar score was defined as a value <7. Neonatal hypoglycemia was operationally defined as a plasma glucose concentration ≤47 mg/dL (≤2.6 mmol/L).
13
-Infectious outcomes: Perinatal infection (neonatal sepsis) was defined by the presence of systemic signs and a documented bloodstream infection within the first 4 weeks of life.
14
-Bilirubin disorders: Abnormal neonatal jaundice was defined as neonatal hyperbilirubinemia meeting age-in-hours–specific thresholds for clinical intervention based on total serum bilirubin levels, according to the American Academy of Pediatrics.
15
-Hematologic abnormalities: This category included newborns with thrombocytopenia, disseminated intravascular coagulation, and other hematologic abnormalities.
(2) Pre-pregnancy maternal conditions
Pre-pregnancy maternal conditions included chronic hypertension, endocrine disorders (including diabetes mellitus, hypothyroidism, and hyperthyroidism), and obesity, defined according to body mass index (BMI) classification.
(3) Pregnancy complications
Pregnancy complications included hypertensive disorders of pregnancy, gestational diabetes, gestational hypothyroidism, intra-amniotic infection, premature rupture of membranes, and urinary tract infection.
Placental pathology evaluation
-Gross examination and routine reporting
Placental pathology reports were based on fixed placentas, most of which were processed within 12 h of delivery. Reports included detailed descriptions of umbilical cord (UC) features, including insertion type (e.g., velamentous, furcate, marginal, or paramarginal [within 1 cm of the placental edge]), coiling index (normal range 0.07–0.3 turns/cm), coiling direction (counterclockwise [left twist], clockwise [dextro-rotatory], or bidirectional), number of vessels (two, three, or more), cord entanglements involving fetal body parts, true UC knots, and other macroscopic and microscopic placental abnormalities. The presence of cord entanglement was determined from delivery records documented at the time of birth. Diagnoses followed the criteria proposed by the Amsterdam consensus conference.
1
-Histologic sampling protocol
For histological examination, three routine placental sections were consistently obtained in a standardized sequence: one near the cord insertion, one from the area of greatest placental thickness, and one from the area of least placental thickness, plus one section from the basal plate. When gross lesions were identified in these regions, they were specifically sampled, and additional sections were taken when indicated. Two membrane sections and two umbilical cord sections were also routinely obtained. -Fetal vascular malperfusion (FVM) assessment
A descriptive analysis was performed to characterize microscopic features within the FVM spectrum. Any qualifying histological lesion within this spectrum was considered indicative of FVM. Key histological features included thrombosis, stem vessel obliteration, fibromuscular sclerosis, segmental avascular villi, villous stromal vascular karyorrhexis, intramural fibrin deposition, and vascular ectasia.1,2,16,17 To avoid interpretive artifacts, chorionic surface vessel ectasia was not assessed in samples obtained near the UC insertion.
High-grade FVM was defined as more than one focus of avascular villi (cumulative assessment of ≥45 avascular villi across three sections examined, or an average of >15 villi per section), with or without thrombus; or two or more occlusive or non-occlusive thrombi in chorionic plate or major stem villi; or multiple non-occlusive thrombi.
1
Cases not meeting full criteria for high-grade FVM but showing selected features were classified as low-grade FVM. -Placental Data Collection and Recording
Placental histological findings were obtained as part of consecutive routine clinical evaluation. To minimize interpretive bias, placentas were initially assessed without prior review of the primary clinical diagnosis or neonatal outcomes. After completion of the histopathologic evaluation, the clinical history was reviewed for clinicopathologic correlation, and both placental pathology and clinical data were subsequently entered into the REDCap® database.
Leukocyte vascular stasis assessment
Leukocyte vascular stasis, defined as “vessels with a fibrin network containing trapped leukocytes,” is the first step for thrombus formation and its formation implies the presence of chemical mediators involved in thrombus formation; it is not recognized in the Amsterdam criteria but considered a potential marker of thrombi in other vascular areas, was also classified for us as FVM; thrombus formation is gradual and is often described as involving leukocytes in fibrin traps.18,19 Finally, we conducted a categorical analysis comparing “Amsterdam-defined FVM” and “early or partial FVM features,” excluding leukocyte stasis from the former category.
Statistical analysis
Statistical analysis included bivariate and multivariate binary logistic regression models, with odds ratios (ORs) and 95% confidence intervals (CIs) reported as effect estimates. Because multiple neonatal outcomes were analyzed, multiple comparisons were addressed using the Benjamini–Hochberg false discovery rate (FDR) procedure to reduce the likelihood that significant findings were due to chance while preserving statistical power. A backward selection approach was used to derive the final multivariable model, retaining variables with p values <0.05. Analyses were performed using Stata version 17.
Results
Demograpic information.
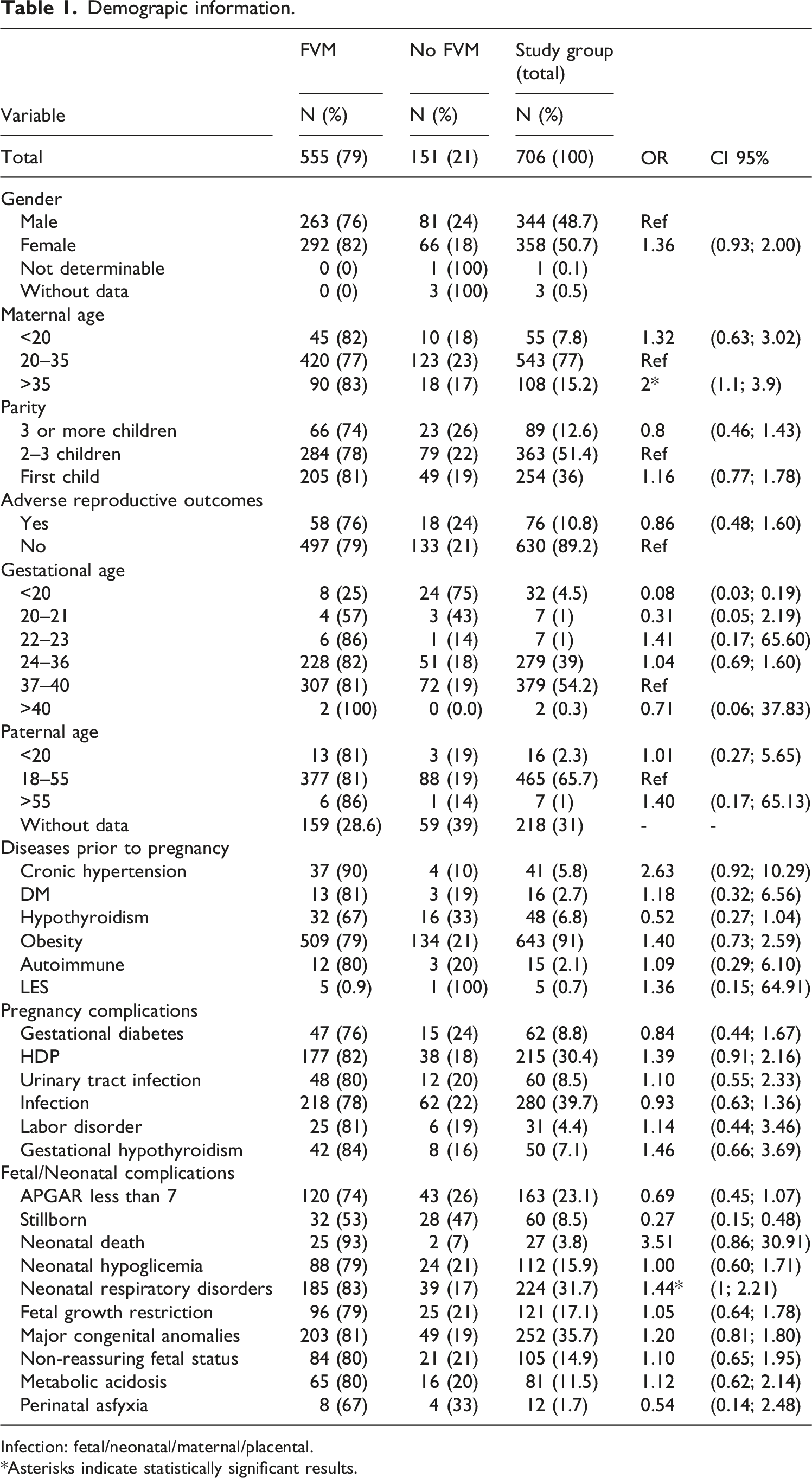
Infection: fetal/neonatal/maternal/placental.
Asterisks indicate statistically significant results.
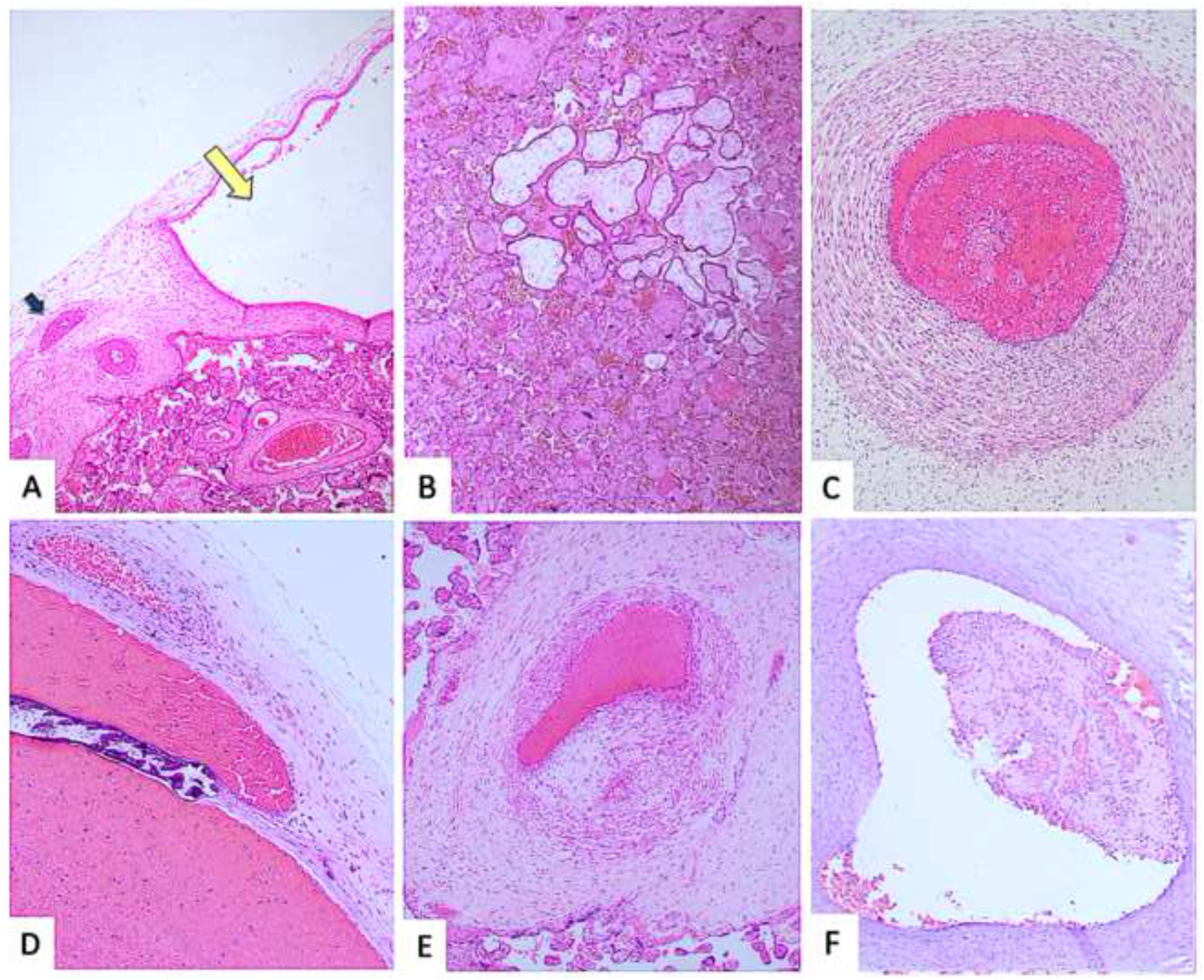
The histological images of fetal vascular malperfusion (FVM) shown in our results include: (a) Vascular ectasia of chorionic plate vessels—marked dilation of placental surface vessels, defined as a luminal diameter at least four times greater than that of a nearby comparable vessel (yellow arrow: dilated vessel; blue arrow: reference vessel) (H&E, 4×). (b) Large avascular villi—clusters of terminal villi showing complete loss of capillaries, meaning these exchange units no longer contain visible blood vessels, involving areas with more than 10 villi (H&E, 4×). (c) Leukocyte stasis in the umbilical vein—intravascular accumulation of white blood cells with surrounding fibrin deposition, reflecting slowed blood flow and an early stage of thrombus (clot) formation. (d) Calcified thrombus in a chorionic plate vessel—an intravascular blood clot with calcium deposits, indicating a long-standing or chronic lesion (H&E, 4×). (e) Organized thrombus—a blood clot showing structural remodeling and tissue incorporation, consistent with temporal evolution (H&E, 4×). (f) Non-occlusive fibrin thrombus—a fibrin-rich intravascular clot that partially, but not completely, obstructs the vessel lumen (H&E, 10×).
FVM findings were observed across all gestational age groups and were more frequent among mothers younger than 20 years and older than 35 years compared with those aged 21–34 years, reaching statistical significance in the older maternal age group (p = 0.02; OR 2.0, 95% CI 1.1–3.9).
Among maternal clinical variables, certain pregestational conditions were more frequent in the FVM group than in the group without FVM, including chronic hypertension (6.7% vs 2.7%) and systemic lupus erythematosus (five cases). FVM findings were also more common among patients with hypertensive disorders of pregnancy (32% vs 25.2%).
With respect to neonatal outcomes, neonatal respiratory disorders were positively associated with FVM (OR 1.4, 95% CI 1–2.1), as were neonatal death (4.5% vs 1.3%) and major congenital anomalies (36% vs 32.5%).
Histological features of fetal vascular malperfusion and associations.

aThrombosis included: thrombi, calcified thrombi, vascular intramural fibrin deposition, karyorrhexis and recanalized thrombus.
Umbilical cord abnormalities.
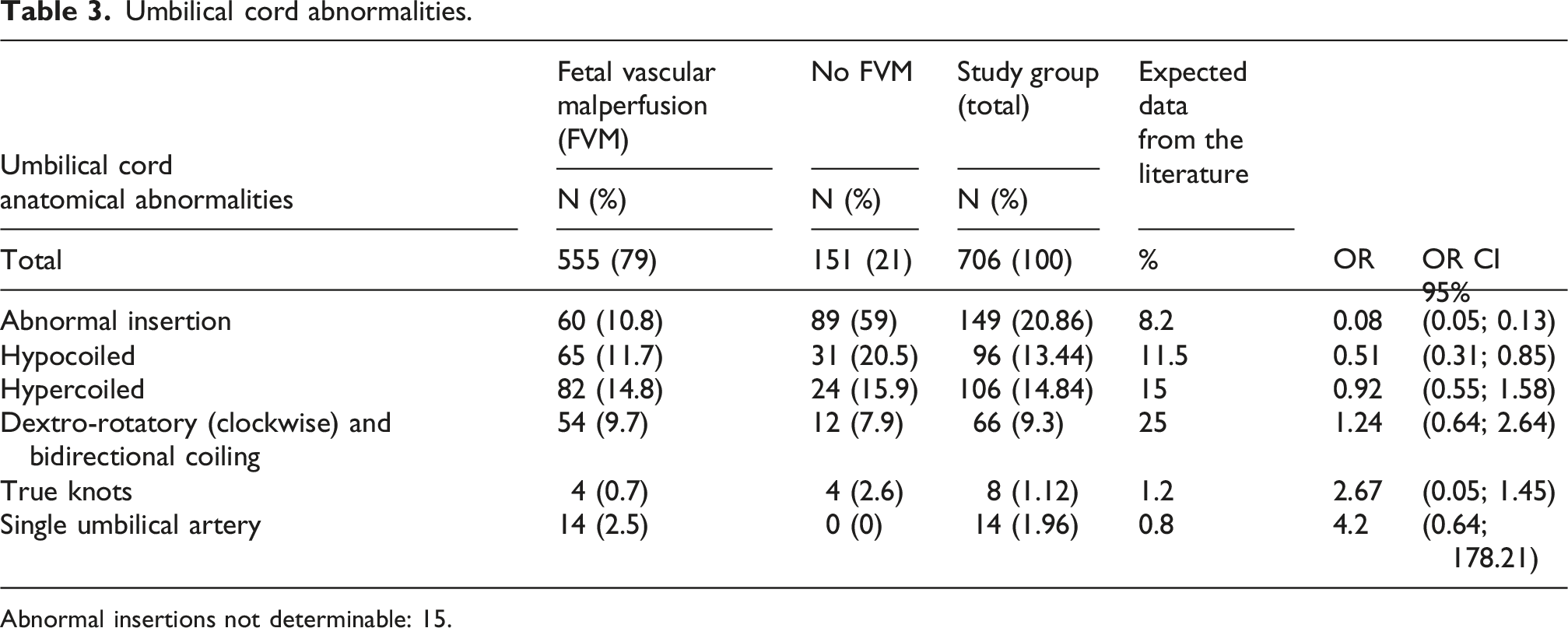
Abnormal insertions not determinable: 15.

Highlighted umbilical cord anatomical abnormalities in our results include: (a) Abnormal insertion: paramarginal (1 cm or less from the placental margin); (b) Abnormal insertion: velamentous (cord insertion where the cord reaches the membranes); (c) Abnormal insertion: marginal (at the placental margin); (d) Abnormal insertion: furcate (vessels lacking Wharton’s jelly before reaching the placenta); (e) Abnormal coiling: contrary coiling and hypercoiling; (f) Abnormal coiling: hypercoiled (coiling index >0.3 coils/cm); (g) Abnormal coiling: bidirectional (top: dextro-rotatory, bottom: levo-rotatory, as highlighted by the blue lines); and (h) Abnormal coiling: contrary coiling (dextro-rotatory/clockwise).
Comparison between Amsterdam-defined FVM and early/partial FVM features
To preserve adherence to the Amsterdam consensus criteria, we performed a secondary analysis comparing Amsterdam-defined FVM with our proposed category of early or partial FVM features. In this analysis, leukocyte stasis was excluded, and the models were reassessed using bivariate analysis. Significant associations were observed between Amsterdam-defined FVM and obesity (OR 2.02, 95% CI 1.1–3.7), and between early/partial FVM features and major congenital anomalies (OR 1.45, 95% CI 1.0–2.15). In contrast, the previously observed associations with maternal age and neonatal respiratory disorders were no longer retained.
Discussion
Fetal vascular malperfusion (FVM), a term introduced by the Amsterdam Placental Working Group in 2016, was previously known by various names, including fetal thrombotic vasculopathy, hemorrhagic endovasculitis, fetal vessel thrombosis, fibrinous vasculosis, thromboesclerosis placentitis, and extensive avascular villi, among others.1,9,20 The significance of FVM lies in its association with stillbirths21,22 and adverse neurological outcomes. 23 Accumulating evidence links FVM to a wide range of fetal and neonatal complications, including intrauterine fetal death,9,24 systemic thromboembolic events involving multiple fetal organs such as the liver, renal vessels, pulmonary circulation, and myocardium,3,25 and central nervous system injury, including thrombotic and hemorrhagic lesions such as lenticulostriate vasculopathy, occipital infarctions, venous sinus thrombosis, cortical vein thrombosis, intracranial hemorrhages, neonatal encephalopathy with subsequent degenerative brain changes, cerebral palsy, and long-term neurological disorders.3,9,26 FVM has also been associated with fetal growth restriction, likely related to hypoperfusion,27–29 as well as with developmental disruptions such as limb deficiencies and intestinal atresia. 16
The diagnosis of FVM is based exclusively on placental histological evaluation, which confirms fetal blood flow obstruction.1,5 In this study, we focused on the analysis of histological findings and their relevance to pathological reporting, as well as their impact on short-term neonatal prognosis, particularly when they do not meet criteria for high-grade involvement.
The Amsterdam Consensus describes two patterns of fetal vascular malperfusion (FVM): segmental and global, each of which may be classified as low- or high-grade. Segmental FVM includes thrombotic occlusions of chorionic or stem villous vessels and stem vessel obliteration. Global FVM is characterized by partial or intermittent obstruction of umbilical blood flow, venous ectasia, intramural fibrin deposition in large vessels, and small, diffusely distributed foci of avascular or karyorrhectic villi within the placenta.1,16 In this study, high-grade FVM was associated with neonatal death (p = 0.04; OR 3.5, 95% CI 1–12), consistent with prior reports. However, our primary focus was on findings suggestive of fetal circulatory obstruction that did not meet high-grade criteria. We examined the observed frequencies and statistical associations between pregestational maternal conditions and fetal outcomes. Although the Amsterdam Consensus describes multiple histological alterations within the FVM spectrum, the individual clinical significance of these features remains uncertain. It is also not yet clear whether alternative grouping strategies beyond the established high-grade classification may provide additional interpretive value. Accordingly, we explored the potential analytical value of individual histological findings as well as grouped patterns.
We observed a higher frequency of FVM than that reported in series of uncomplicated deliveries. This likely reflects the high-risk profile of our study population, in which FVM would be expected to occur more frequently given its association with multiple adverse maternal, fetal, and placental conditions, as discussed below.
Impact on the fetus and newborn
In our study population, we observed a substantial short-term clinical impact on fetuses and neonates. FVM diagnoses were statistically associated with neonatal complications, including death and neonatal respiratory disorders. In addition, several specific histologic features showed associations with fetal growth restriction (FGR), major congenital anomalies, and neonatal hypoglycemia. Moreover, the association with major congenital anomalies was also observed in the combined analysis including all FVM criteria (OR 1.45, 95% CI 1.0–2.15). Similarly, Ravikumar et al. 30 in a cohort of 110 patients, reported a significantly higher frequency of adverse neonatal outcomes in cases with FVM, including poor neonatal survival, non-reassuring fetal status, neurological abnormalities, neonatal sepsis, asphyxia, low Apgar scores, FGR, and increased need for respiratory support.
Among the 27 postnatal deaths after 24 weeks’ gestation, more than half (55%) occurred in term neonates. Placental examination in these cases revealed FVM-spectrum lesions in 81.5%, a markedly higher proportion than the 31.1% reported in viable fetuses, 24 underscoring a potential association with adverse outcomes. In contrast, in stillbirths—particularly those with maceration—placentas more frequently exhibited features suggestive of chronic and evolving vascular compromise, including thrombi at different stages of organization, intramural fibrin deposition, and vascular ectasia.
Although fetoplacental circulatory alterations may have long-term consequences, in our cohort we observed associations primarily with early outcomes, including neonatal death. In some cases, placental findings appeared to reflect underlying fetal conditions; for example, congenital heart disease was identified in several patients, in whom altered hemodynamics may favor thrombosis. This is consistent with previous reports describing turbulent or reduced flow and its association with thrombotic lesions and structural umbilical cord abnormalities.31,32 Additionally, FVM has been reported in association with chromosomal disorders, which were also present in a subset of our patients.
Other components of FVM have been associated with the placental microenvironment and the fetal–maternal interface, particularly hypertensive disorders of pregnancy,26,27 which are known to involve increased prothrombotic factors, 33 a relationship discussed in detail below.
Maternal factors
When assessing the association between FVM and pregnancy complications, concomitant maternal vascular malperfusion increased the risk of FVM (p = 0.007; OR 1.7, 95% CI 1.2–2.6), consistent with previous reports. 16 In our setting, preeclampsia—a clinical condition closely associated with maternal vascular malperfusion—has an incidence of approximately 14%, well above that reported in most regions, and accounts for 30% of the placentas submitted to our pathology laboratory (see below and Table 1). According to the literature, in neonates born to mothers with PE, erythrocytes have been reported to show a reduced elongation index, indicating impaired deformability and reduced aggregability, which may explain these findings. This reduced aggregability may represent an adaptive response to endothelial dysfunction and increased vascular resistance, potentially helping to preserve blood flow. 33 Environmental factors during pregnancy—collectively referred to as the “maternal exposome”—may also influence neonatal erythrocyte properties. For example, maternal smoking during pregnancy has been associated with increased oxidative stress, with neonatal red blood cells showing elevated levels of peroxynitrite (ONOO−), a toxic oxidant formed by the reaction of superoxide anion (O2−) with nitric oxide, along with increased lipid peroxidation. 33
FVM was associated with obesity, nulliparity, and long interpregnancy intervals. These factors may coexist with advanced maternal age and are often encountered in clinical settings with a higher prevalence of PE.34,35 PE and obesity have also been associated with variety of anatomical umbilical cord abnormalities, 36 as well as vascular alterations within the placental bed and microcirculation, reflected in morphometric and histological changes in the umbilical vessels. 37 These findings may be interpreted within the broader placental environment of chronic hypoxia, hypercoagulability, and endothelial dysfunction.
In our highly specialized referral center, a substantial proportion of mothers entered pregnancy with a BMI greater than 24. Obesity may contribute to the occurrence of FVM and has also been associated with anatomical abnormalities of the umbilical cord, as noted above. These abnormalities appear to confer a higher risk of stillbirth among obese women than among women of normal weight. 38 Obesity has also been associated with oxidative stress-related alterations in the fetal circulation. 39
Numerous studies have reported associations between obesity, carbohydrate intolerance, and gestational diabetes and adverse perinatal outcomes, including increased miscarriage rates, congenital anomalies, and macrosomic fetuses. 40 Although obesity is not among the most consistently emphasized classic clinical associations of FVM, recent evidence supports its relationship with altered placental vascular development, and a statistically significant association with FVM was observed in our study population (OR 2.02, 95% CI 1.1–3.7). Additionally, previous research on FVM has noted delayed villous maturation. 41 Beyond obesity, some patients had chronic hypertension, and FVM was more frequently observed in their placentas.
In contrast to preeclampsia, the incidence of pregestational and gestational diabetes was low in our study population, as shown in Table 1. Even so, diabetic pregnancies have been associated with structural alterations in the umbilical vessels, including constriction, endothelial discontinuity of the intima, and extravasation of arterial blood into Wharton’s jelly in the umbilical artery, and wall thinning with luminal enlargement in the umbilical vein, 42 all of which may contribute to a vascular environment conducive to FVM.
We consider it important to highlight the association between maternal vascular malperfusion (MVM) and the increased risk of fetal vascular malperfusion (FVM). While frequently discussed in the context of preeclampsia, MVM is also observed in other maternal conditions such as diabetes, obesity, and related disorders. 43 Its relatively high frequency is consistent with prior reports, including large population-based series of more than 20,000 births reporting an incidence of 32.8% at term. 44 Similarly, Freedman et al. reported MVM in 35.6% of 728 cases of preeclampsia, 45 similar to the 30.4% observed in our cohort of 706 patients.
The umbilical cord
The umbilical cord, the primary conduit for fetal blood, provides critical information in placental examination. Associations between FVM and umbilical cord anatomical abnormalities (UCAAs), such as those described above, are well established.46,47 In our high-risk population, the incidence of umbilical cord alterations was higher than typically observed in the general population. We identified an association between hypercoiled cords and vascular ectasia of the chorionic plate vessels (OR 1.6) (Table 3). Compared with frequencies reported in the literature, our cohort showed a higher prevalence of several umbilical cord abnormalities, consistent with the high-risk profile of the study population. The reported prevalence of abnormal cord insertions is generally around 7.8–12% of pregnancies, 48 in our study, they were observed in 20.9% of cases. Likewise, single umbilical artery (SUA) in the general obstetric population is typically below 1%, whereas in our cohort it was observed in 1.96% of cases, 49 and all of these cases occurred in the FVM group.
The length of the umbilical cord could not be recorded, as it is not routinely measured in the delivery room. A potential limitation in interpreting the ectasia observed in umbilical cord vessels—and its extension into chorionic and stem villus vessels—is its known dependence on fixation time. 50 In our hospital, all placental samples were obtained after fixation, with most processed within the first 12 h; however, some samples, particularly those processed over weekends, had longer fixation times of up to 3 days. Fixation-related overestimation of vascular changes has been described mainly in specimens subjected to prolonged fixation exceeding 2 weeks, a scenario not applicable to our placental samples. In such settings, reported frequencies of vascular ectasia differ markedly between promptly processed specimens and those subjected to prolonged fixation (3% vs 61%). In our high-risk cohort, the observed frequency was 21%, suggesting that our findings are unlikely to be solely explained by fixation-related artifacts.
Significant associations were observed between bidirectional cords and large foci of avascular villi (OR 6), as well as between abnormal cord insertions and thrombus formation (OR 2). In contrast, Stanek established analytical groups for distal and large vessel obstruction without reporting an association with umbilical cord abnormalities. 51
Leukocyte stasis
Our primary concern in analyzing routine cases was the following: “What should be done when only a few microscopic lesions are present, or when multiple lesions are identified but do not meet high-grade criteria? How should we report frequent leukocyte stasis when it does not form an adherent thrombus recognized by the pathologist? Leukocyte stasis is considered an ‘early thrombus’—but is it accompanied by fully developed thrombi upstream or downstream? Are the chemical mediators that trigger leukocyte migration and fibrin formation already producing vascular changes that may be harmful to the fetus? If so, should leukocyte stasis be disregarded?” Although we adhered to Amsterdam Consensus guidelines, we decided to include leukocyte stasis as an exploratory criterion. We defined leukocyte stasis as the presence of a fibrin network containing entrapped leukocytes within fetal-placental vessels. Because placental-specific literature addressing leukocyte stasis and the earliest stages of fetal-placental thrombus formation is limited, interpretation of this finding currently relies in part on broader concepts from thrombosis pathophysiology. Accordingly, to evaluate its potential significance, we considered Virchow’s triad as a conceptual framework, encompassing endothelial or vessel wall injury, flow stasis, and hypercoagulability. In our study, the first two components were frequently observed in placental vessels showing FVM-spectrum lesions. To address concerns regarding the inclusion of leukocyte stasis, we examined the number of cases in which it was the sole finding, in order to assess the potential for overdiagnosis of FVM. Out of a total of 555 cases, 65 cases (11.7%) met this criterion alone, indicating that leukocyte stasis is frequently accompanied by other FVM criteria (88.3%), suggesting that its inclusion is unlikely to result in overdiagnosis. However, association analyses were performed comparing “Amsterdam-defined FVM” with “early or partial FVM features”; in the former category, leukocyte stasis was excluded. Some associations emerged, including major congenital anomalies and obesity, as expected. Other associations were not observed, such as those with maternal age >35 years or neonatal respiratory disorders.
Leukocyte stasis is thought to occur during delivery and may represent an early stage of thrombus formation, potentially triggered by endothelial injury, prothrombotic factors, or reduced blood flow. Although the process of thrombus formation in the fetal and placental circulation remains poorly defined, the histological features observed resemble those described in recent and older thrombi across age groups. Neonates also exhibit reduced fibrinolytic activity, largely due to low plasminogen levels and elevated plasminogen activator inhibitor concentrations, which may contribute to an increased susceptibility to thromboembolic events. Congenital thrombophilias may further predispose to thrombosis, particularly in the presence of additional precipitating factors.52,53 Hypercellularity and hyperviscosity may also contribute to this prothrombotic milieu. In particular, neonates exposed to chronic or acute fetal hypoxia have an increased incidence of polycythemia and the associated hyperviscosity. 54 In patients with transient abnormal myelopoiesis (TAM)—an illustrative condition marked by pronounced hypercellularity in some individuals with trisomy 21—myeloid cell thrombi (MCT) were frequently identified, and a high incidence of FVM was observed in association with TAM. However, the available evidence remains limited. 55
Temporal interpretation of lesions
FVM analysis may reveal either a single catastrophic event or the coexistence of lesions at different stages of evolution, suggesting repeated or cumulative occurrences of FVM. 56 In medico-legal contexts, establishing both the chronicity and severity of placental injury is essential. Chronic lesions—such as vascular recanalization and calcified thrombi—reflect prior vascular obstruction and are not attributable to intrapartum events. These findings serve as markers of fetal vessel compromise and have been associated with adverse outcomes, including metabolic acidosis and fetal growth restriction; in our series, they were also linked to hypoglycemia and major congenital anomalies (Table 2). Additional features of chronicity include stem vessel obliteration, fibromuscular sclerosis, organized thrombi, and intramural fibrin deposition. More recent lesions include vascular ectasia and newly formed thrombi, whereas leukocyte stasis represents an early microscopic stage of vascular obstruction. Histological patterns may provide etiopathogenic insight, 56 for example, FVM associated with congenital heart disease often shows thrombi at different stages of organization, while delivery-related compromise (e.g., cord compression) tends to exhibit recent thrombi, vascular ectasia, and leukocyte stasis. In our cohort, among major congenital anomalies, 13 cases of congenital heart disease were identified, of which 12 occurred in the FVM group and 1 in the non-FVM group, a distribution consistent with the expected pathophysiological framework.
Although leukocyte stasis does not by itself establish a diagnosis of FVM, its presence—particularly in large vessels—should prompt careful clinicopathologic correlation.
Interpretation and reporting of early or partial FVM lesions
The interpretation of early or partial FVM lesions remains challenging, particularly in cases that do not meet established criteria for high-grade involvement according to the Amsterdam consensus. In routine practice, pathologists frequently encounter isolated or limited histologic findings suggestive of altered fetal circulation, raising questions regarding their diagnostic weight and clinical relevance.
Based on our findings, we suggest that such lesions should not be disregarded, but rather reported using cautious and descriptive language. When present in isolation or in limited number, these findings may be best interpreted as features suggestive of early or partial fetal vascular malperfusion, without assigning a definitive diagnosis of FVM. This approach allows recognition of potential fetal circulatory disturbance while avoiding overdiagnosis.
In this context, we propose that pathology reports may include phrases such as “features suggestive of early or partial fetal vascular malperfusion” or “isolated findings within the FVM spectrum,” particularly when the full criteria for high-grade FVM are not met. These descriptors may be accompanied by a comment highlighting the importance of clinical correlation, especially in cases with adverse neonatal outcomes or relevant maternal conditions.
Based on our findings, a conceptual framework may be proposed in which maternal conditions (e.g., hypertensive disorders), together with fetal susceptibility factors and umbilical cord abnormalities, contribute to alterations in fetoplacental circulation. These disturbances may lead to progressive vascular compromise within the placenta, ranging from early or partial changes—such as leukocyte stasis—to more advanced lesions, including thrombosis and features of high-grade FVM. Within this continuum, the interaction between maternal, fetal, and placental factors ultimately determines the severity of vascular malperfusion and its clinical expression in adverse perinatal outcomes.
Consistent with our findings, in which early or partial FVM features were associated with adverse outcomes, these data support the potential clinical relevance of reporting such lesions, even when full diagnostic criteria are not met. Notably, our study extends current evidence by specifically evaluating non-high grade FVM lesions, leukocyte stasis, and partial vascular features, highlighting their potential role within the spectrum of fetal vascular malperfusion. Further studies are needed to better define the prognostic significance of these lesions and to determine whether alternative classification or grading approaches may provide additional clinical value.
Conclusions
Fetal vascular malperfusion (FVM) is a largely silent condition, typically diagnosed only after delivery, yet it reflects obstruction within the neuro–cardio–placental axis with potential consequences for fetal development and neonatal outcomes. In this study, we identified maternal risk factors and associations with umbilical cord abnormalities, supporting current concepts in neuroplacentology. We also propose leukocyte stasis as a potential stage in the progression of circulatory obstruction, emphasizing its temporal evolution toward more advanced lesions, including calcified thrombi.
Importantly, our findings indicate that even low-grade FVM may be associated with an increased risk of adverse fetal and neonatal outcomes. From a diagnostic perspective, placental lesions within the FVM spectrum should not be dismissed solely because they do not meet full high-grade criteria. Although caution is warranted to avoid overinterpretation, early or partial vascular lesions may still provide clinically meaningful information when integrated with the broader placental and perinatal context.
Overall, these findings underscore the clinical value of detailed placental histopathological evaluation, which may aid obstetricians in identifying maternal conditions associated with placental dysfunction and support pediatricians and neonatologists in understanding the risks and underlying mechanisms of neonatal compromise.
Limitations and strengths
This study has limitations and potential biases related to sample selection, as it focuses on a hospital population at increased obstetric risk, with higher rates of maternal, fetal, and neonatal complications, and consequently a higher incidence of fetal vascular malperfusion (FVM). Strengths of the study include the large sample size, the comprehensive assessment of macroscopic and microscopic placental findings, and the availability of detailed maternal and neonatal clinical data.
Footnotes
Acknowledgments
We wish to thank the Pontificia Universidad Javeriana-Hospital Universitario San Ignacio (HUSI) in Bogotá, Colombia for its indispensable support and participation in this study. We also like to thank the Staffs of the Departments of Pathology and Obstetrics and Gynecology.
ORCID iDs
Ethical considerations
The present study was performed in line with the principles of The Code of Ethics of the World Medical Association (Declaration of Helsinki) and all procedures were approved by the Ethics Committee of the Pontificia Universidad Javeriana and the Hospital Universitario San Ignacio (FM-CIE0131-21).
Consent to participate
The research involving human subjects complies with all relevant national regulations and institutional policies and adheres to the principles of the Helsinki Declaration. The study was approved by the authors’ institutional review board, as specified above. Consent to participate was waived by the Institutional Review Board (IRB) because the cases do not include patient identifiers, and the placentas were obtained through routine histological examination.
Author contributions
NFC: Writing—Original Draft, Writing—Review and Editing, Visualization. AMV: Resources, Writing—Original Draft, Writing—Review and Editing. MAR: Methodology, Formal Analysis. MOC: Conceptualization, Project Administration, Resources, Writing—Original Draft, Writing—Review and Editing, Supervision, Investigation, Visualization.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Pontificia Universidad Javeriana Bogota and Hospital Universitario San Ignacio.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The authors declare that the data are available without unnecessary restriction, including histological slides and paraffin blocks.