
Abstract
Background
Hyperoxia-induced lung injury is a key contributor to the development of bronchopulmonary dysplasia in preterm infants, primarily through oxidative stress and impaired antioxidant defense mechanisms.
Objective
To evaluate the protective effects of N-acetylcysteine (NAC) and combined vitamin E and C therapy on oxidative stress, antioxidant capacity, and lung histopathology in a neonatal rat model of hyperoxia-induced lung injury.
Methods
A total of 36 neonatal rats were randomly assigned to four groups: control (room air, n = 9), hyperoxia (n = 9), hyperoxia + NAC (n = 8), and hyperoxia + vitamin E + C (n = 10). Hyperoxia exposure (90% ± 10% O2) was maintained from postnatal days 3–14. Treatments were administered intraperitoneally (NAC 150 mg/kg/day, vitamin E 25 IU/day, vitamin C 1 mg/kg/day). Oxidative stress parameters (TOS, OSI, and LOOH), antioxidant markers (TAS, paraoxonase, and arylesterase), and histopathological findings were evaluated in serum and lung tissue.
Results
Hyperoxia significantly increased oxidative stress markers, with higher TOS levels observed in both serum and lung tissue compared to the control group (p < 0.001). NAC and vitamin E + C treatments significantly increased TAS levels compared to the hyperoxia group (p < 0.05). Serum OSI levels were significantly reduced in both treatment groups (p = 0.002 and p = 0.032). Additionally, arylesterase levels were significantly higher in the vitamin group compared to all other groups (p < 0.001). Histopathological evaluation demonstrated reduced inflammatory cell infiltration and lower fibrosis scores in the treatment groups.
Conclusion
N-acetylcysteine and combined vitamin E and C therapy attenuate hyperoxia-induced lung injury by reducing oxidative stress and improving lung histopathology in neonatal rats. These findings support antioxidant strategies as adjunctive approaches for BPD-related lung injury.
Introduction
Bronchopulmonary dysplasia is a major cause of morbidity and mortality in preterm infants, with a global incidence ranging from 17% to 75% among infants born before 28 weeks of gestation.1–3 The pathogenesis of BPD is multifactorial and includes immature lung development, oxygen therapy, mechanical ventilation, infection, and inflammation. Recent studies have demonstrated that oxidative stress, prolonged exposure to high oxygen concentrations (hyperoxia), and inflammation contribute to lung injury and airway reactivity and play a critical role in the development of BPD.4–6 Although oxidative stress is widely recognized as a key mechanism in the pathogenesis of BPD, effective therapeutic strategies targeting this pathway remain limited. In this context, the evaluation of antioxidant agents with distinct mechanisms of action in experimental models is important for a better understanding of potential therapeutic approaches to hyperoxia-induced lung injury.
Preterm infants are particularly vulnerable to oxidative stress due to frequent exposure to supplemental oxygen, immature enzymatic antioxidant systems, reduced glutathione availability, and concomitant inflammation or infection. 7 Experimental models of hyperoxia-induced lung injury reproduce many pathological features of BPD, including impaired alveolarization, inflammation, and fibrotic remodeling, making them valuable tools for evaluating potential therapeutic interventions. Neonatal rats are in the saccular stage of lung development at birth, which corresponds to the lung maturity of extremely preterm infants, supporting the translational relevance of this model.8,9
N-acetylcysteine (NAC) is a precursor of glutathione and also acts as a direct free radical scavenger (10). 10 Experimental studies have demonstrated that NAC attenuates hyperoxia-induced lung injury by reducing oxidative stress and modulating inflammatory responses.11,12 Vitamins E and C are potent antioxidants that act synergistically to inhibit lipid peroxidation and regenerate oxidized tocopherol, thereby strengthening cellular antioxidant defenses.13,14 Vitamin E acts as a lipid-soluble chain-breaking antioxidant, while vitamin C regenerates oxidized vitamin E, thereby enhancing its antioxidant capacity and providing more effective protection against oxidative damage.15,16 However, comparative data evaluating different antioxidant strategies with distinct mechanisms of action in hyperoxia-induced neonatal lung injury remain limited. Although clinical studies in preterm infants have yielded inconsistent results, experimental data suggest that antioxidant therapies may mitigate hyperoxia-induced lung injury during critical periods of lung development.17,18
The present study aimed to evaluate the effects of NAC and combined vitamin E + C treatment on oxidative stress parameters and lung histopathology in a neonatal rat model of hyperoxia-induced lung injury.
Materials and methods
Study design and outcomes
This study was designed as an experimental animal study investigating the effects of antioxidant therapies in a neonatal rat model of hyperoxia-induced lung injury. The primary outcomes of the study were oxidative stress parameters (TOS, TAS, OSI, and LOOH) measured in serum and lung tissue. Secondary outcomes included antioxidant enzyme activities (paraoxonase and arylesterase) and histopathological findings, including inflammation and fibrosis.
Animals and experimental design
This study was conducted on 3-day-old Wistar albino rats in which a hyperoxia model was established. Ethical approval was obtained from the Institutional Animal Ethics Committee of Çukurova University Faculty of Medicine (Project number: TF2010LTP7).
The animals were maintained under a 12-h light/12-h dark cycle, with room temperature kept constant at 21–23°C and humidity maintained between 40 and 60%. Adult breeding rats were fed standard laboratory rat feed.
Rat pups were enrolled at postnatal day 3 and randomly assigned to study groups. The experimental protocol was initiated on postnatal day 3 and continued until postnatal day 14, during which a total of 36 neonatal rat pups were included. The rats were divided into four groups. Group 1 (n = 9) served as the control group and was not exposed to supplemental oxygen; these animals were maintained in room air. Groups 2, 3, and 4 were housed in a closed plexiglass chamber and continuously exposed to hyperoxia (90% ± 10% O2) throughout the experimental period.
For the hyperoxic lung injury model, a hyperoxia-induced bronchopulmonary dysplasia (BPD) rat model was used. 19 Rat pups, together with their dams, were continuously exposed to hyperoxia in a closed plexiglass chamber from postnatal day 3 to day 14, for a total duration of 10 days. Oxygen concentration was monitored three times daily using an anesthetic gas monitor (Type 1304, Brüel & Kjær, Denmark). Carbon dioxide was removed using soda lime.
On postnatal day 14, the rats were euthanized by intraperitoneal injection of pentobarbital sodium (200 mg/kg). Following thoracotomy, intracardiac blood samples were collected, after which the left lung lobe was harvested for biochemical analyses and the right lung lobe for pathological examination.
Study groups
A formal sample size calculation was not performed due to the exploratory nature of the study; however, group sizes were determined based on previous experimental studies using similar hyperoxia models.8–19 Control group (n = 9): Control rats maintained in room air, not exposed to supplemental oxygen, and administered saline.
Hyperoxia group (n = 9): Rats exposed to hyperoxia and administered saline.
NAC group (n = 8): Rats exposed to hyperoxia and treated with N-acetylcysteine (NAC).
Vitamin group (n = 10): Rats exposed to hyperoxia and treated with vitamin E and vitamin C.
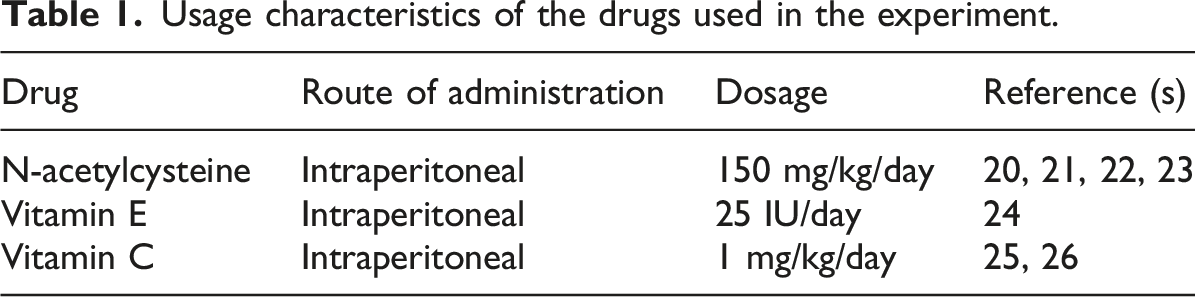
Drug administration
Usage characteristics of the drugs used in the experiment.
Tissue preparation and blood collection
On postnatal day 14, intracardiac blood samples were collected using an insulin syringe following thoracotomy. The collected blood was centrifuged at 3000 rpm for 10 min to separate the serum, which was then stored at −80°C for subsequent biochemical analyses.
The lungs were excised, and the right lung lobe was fixed in 10% formalin for 24 h. After fixation, one lobe of the lung tissue was placed into separate cassettes and processed routinely, followed by paraffin embedding. Sections of 4 μm thickness were cut from the paraffin blocks and evaluated in a blinded manner by a single pathologist. The left lung lobes were snap-frozen in dry tubes and stored at −80°C for biochemical analyses.
Histological evaluation of fibrosis
Paraffin-embedded lung sections were stained with hematoxylin and eosin (H&E). Five randomly selected fields per section were evaluated under light microscopy at ×200 magnification. Fibrosis was semi-quantitatively scored as 0 (absent), 1 (mild), 2 (moderate), or 3 (severe and diffuse). Masson’s trichrome staining was used to assess collagen deposition. Histopathological evaluation was performed by a single experienced pathologist who was blinded to group allocation. Fibrosis scores were statistically compared between groups.20–27
Preparation of lung tissue for biochemical analyses
One gram of fresh lung tissue was taken and 9 ml of working solution (a solution containing 140 mmol KCl in deionized water) was added. The mixture was crushed using a mechanical homogenizer (blender). After centrifugation at 3000 rpm for 5 min, the resulting supernatant was used for biochemical analyses.
Biochemical analyses
Measurement of serum paraoxonase and arylesterase activities
Serum paraoxonase (PON) activity was measured using paraoxon as the substrate, and the absorbance of the hydrolysis product was recorded at 412 nm at 37°C (27). PON activity was determined as basal activity and expressed as U/L.
Phenyl acetate was used as the substrate for arylesterase activity. One unit of arylesterase activity was defined as the amount of enzyme that generates 1 μmol of phenol per minute, and results were expressed as U/L. 28
Measurement of serum total antioxidant status
Serum total antioxidant status (TAS) was determined using an automated colorimetric method based on the decolorization of the 2.2′-azino-bis(3-ethylbenzothiazoline-6-sulfonic acid) (ABTS) radical by antioxidants present in the sample. 29 Results were expressed as mmol Trolox equivalent/L.
Measurement of serum total oxidant status
Serum total oxidant status (TOS) was measured using an automated method. 30 Oxidants in the sample oxidize the ferrous ion–o-dianisidine complex to ferric ions, which form a colored complex with xylenol orange in an acidic medium. The color intensity, measured spectrophotometrically, is proportional to the total oxidant concentration in the sample. The assay was calibrated with hydrogen peroxide (H2O2), and results were expressed as μmol H2O2 equivalent/L.
Measurement of oxidative stress index
The oxidative stress index (OSI) was defined as the percentage ratio of total oxidant status (TOS) to total antioxidant status (TAS). For calculation, TAS values were converted to mmol/L. OSI was calculated using the following formula 31 :
OSI (arbitrary units) = TOS (μmol H2O2 equivalent/L)/TAS (mmol Trolox equivalent/L).
Measurement of lipid hydroperoxide levels
Serum lipid hydroperoxide (LOOH) levels were measured using the ferrous ion oxidation–xylenol orange (FOX-2) assay. 32
Statistical analysis
Statistical analyses were performed using SPSS software version 18.0. Continuous variables were summarized as mean ± standard deviation or, where appropriate, as median (minimum–maximum). For comparisons of continuous variables among more than two groups, one-way analysis of variance (ANOVA) was used when assumptions were met, and the Kruskal–Wallis test was applied when assumptions were not met.
For pairwise group comparisons, Sidak or Tamhane’s T2 post hoc tests were used according to the homogeneity of variances. A p value <0.05 was considered statistically significant. Fibrosis scores were compared between groups using the chi-square test.
Results
Body weight gain
Group averages of rat weights at the end of the experiment, according to groups.
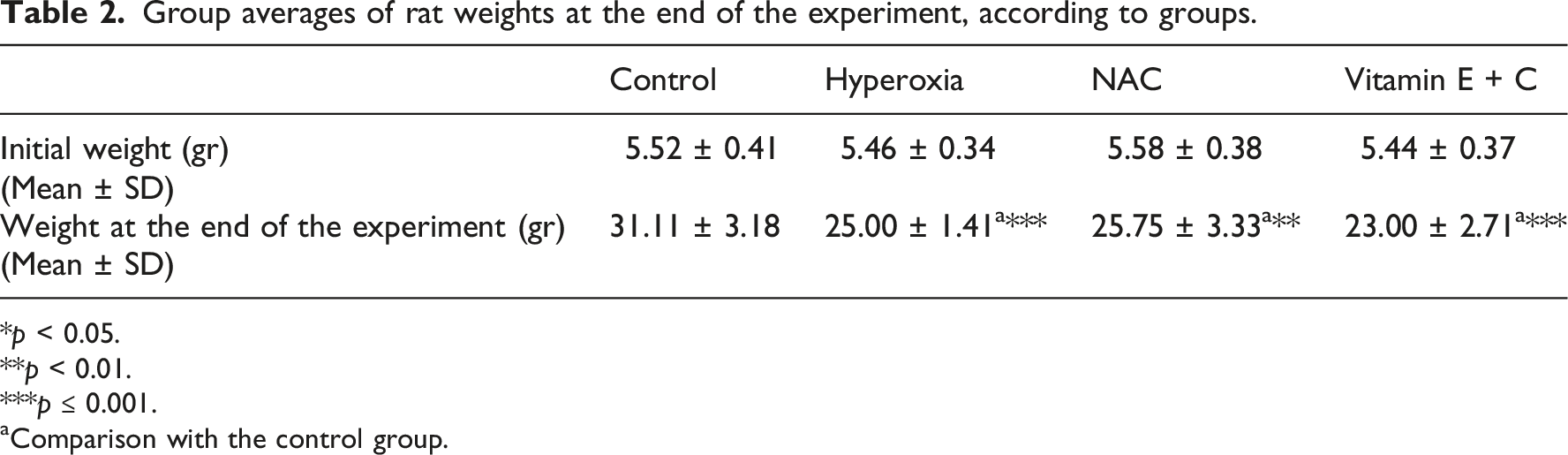
*p < 0.05.
**p < 0.01.
***p ≤ 0.001.
aComparison with the control group.
Serum antioxidant enzyme levels
Comparison of serum antioxidant enzyme levels between groups. (mean ± SD).
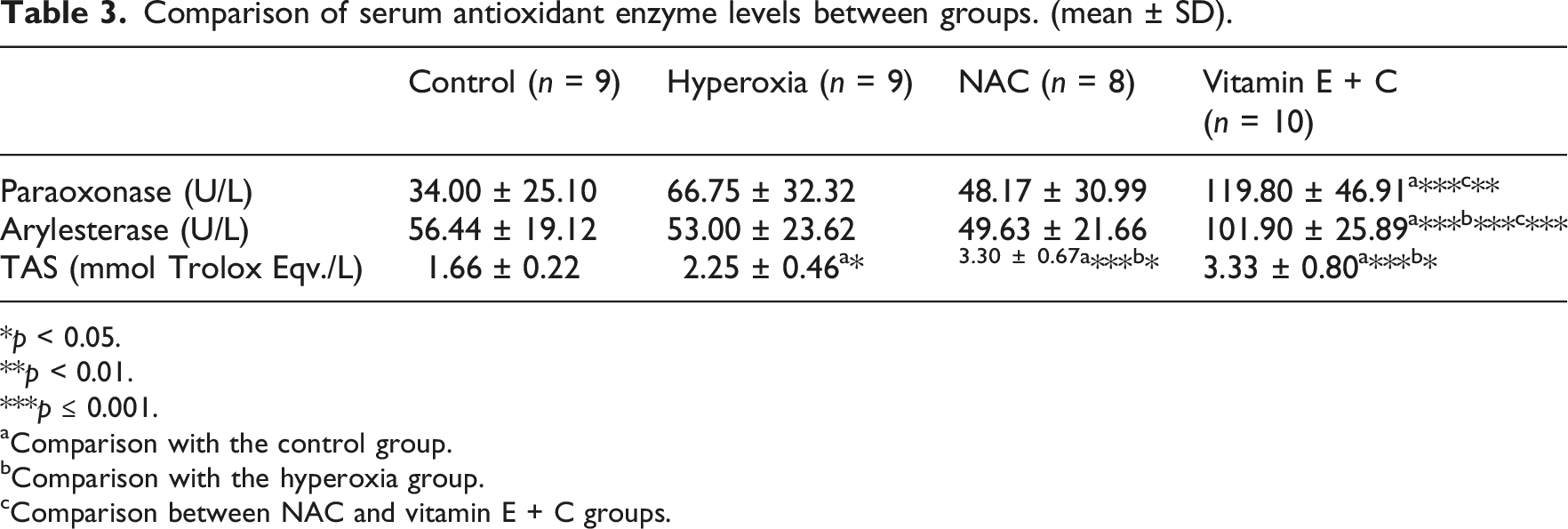
*p < 0.05.
**p < 0.01.
***p ≤ 0.001.
aComparison with the control group.
bComparison with the hyperoxia group.
cComparison between NAC and vitamin E + C groups.
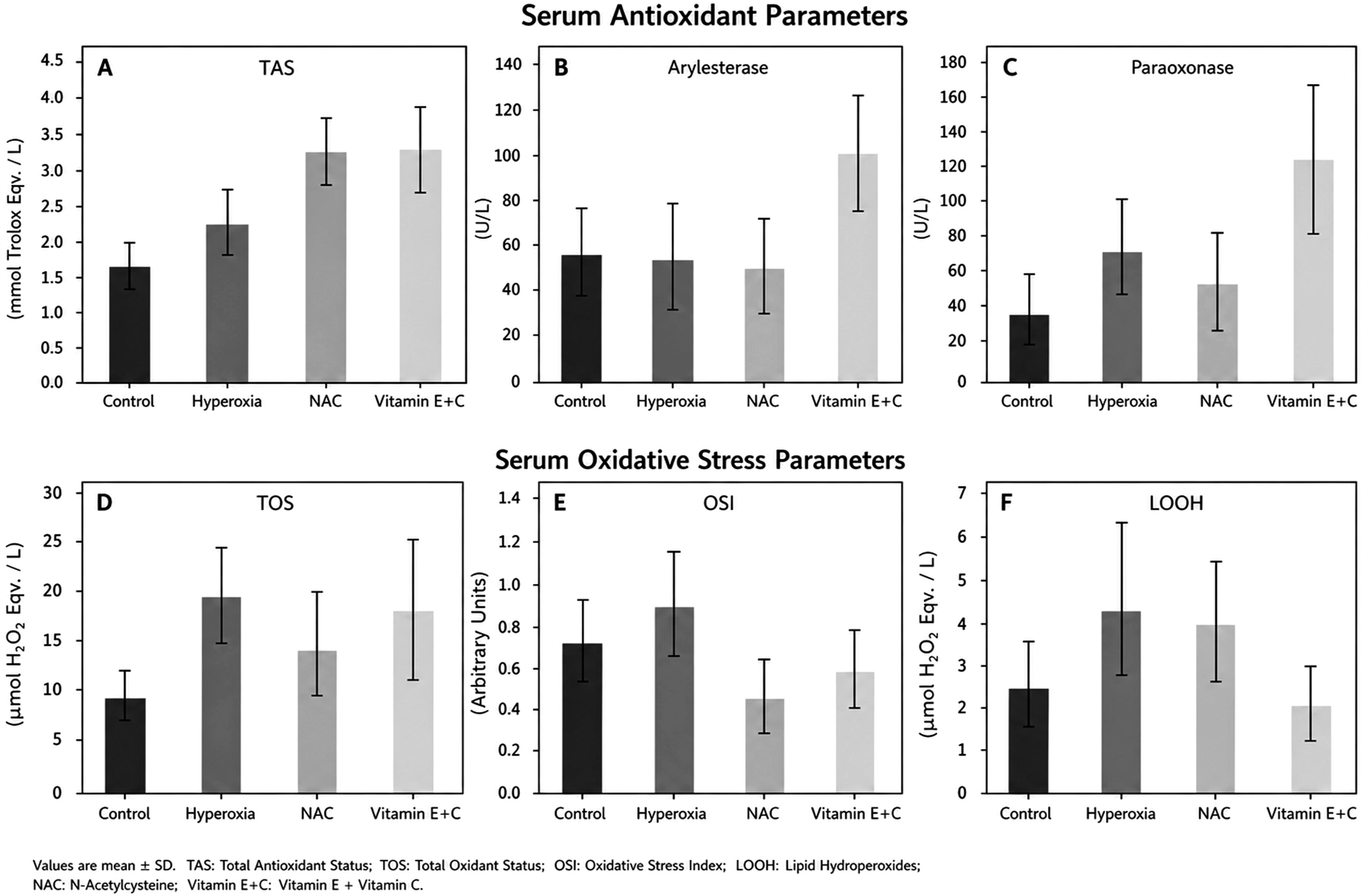
Serum antioxidant and oxidative stress parameters across study groups. (a) Total antioxidant status (TAS), (b) arylesterase activity, (c) paraoxonase activity, (d) total oxidant status (TOS), (e) oxidative stress index (OSI), and (f) lipid hydroperoxide (LOOH) levels. Data are presented as mean ± SD. Detailed statistical comparisons are provided in Tables 3 and 4.
Serum oxidative stress parameters
Comparison of serum oxidative stress parameters levels between groups. (mean ± SD).
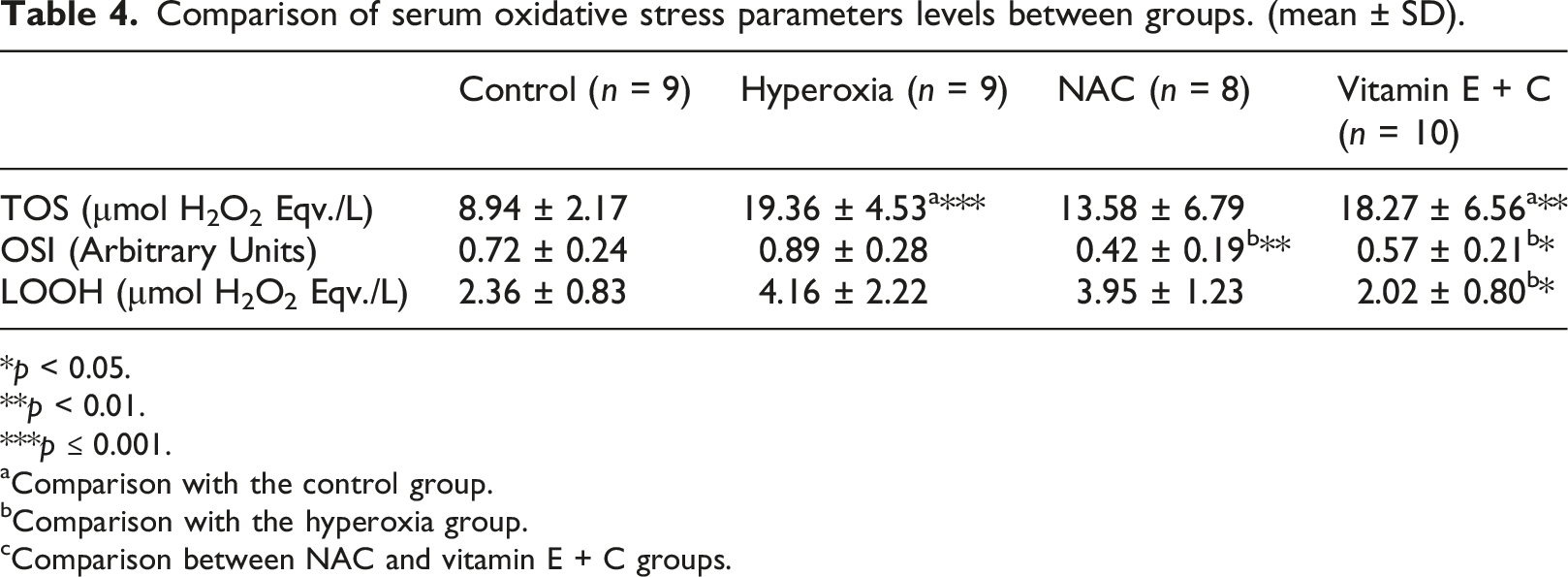
*p < 0.05.
**p < 0.01.
***p ≤ 0.001.
aComparison with the control group.
bComparison with the hyperoxia group.
cComparison between NAC and vitamin E + C groups.
Antioxidant enzyme levels in lung tissue
Comparison of antioxidant enzyme levels in lung tissue between groups. (mean ± SD).
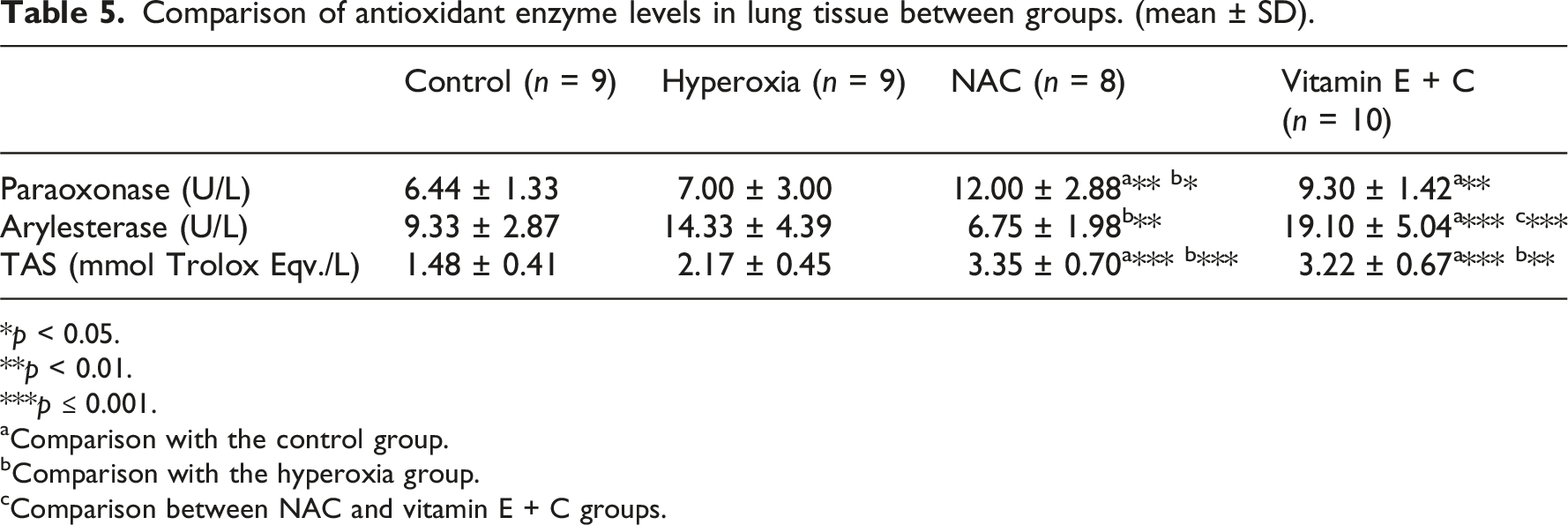
*p < 0.05.
**p < 0.01.
***p ≤ 0.001.
aComparison with the control group.
bComparison with the hyperoxia group.
cComparison between NAC and vitamin E + C groups.
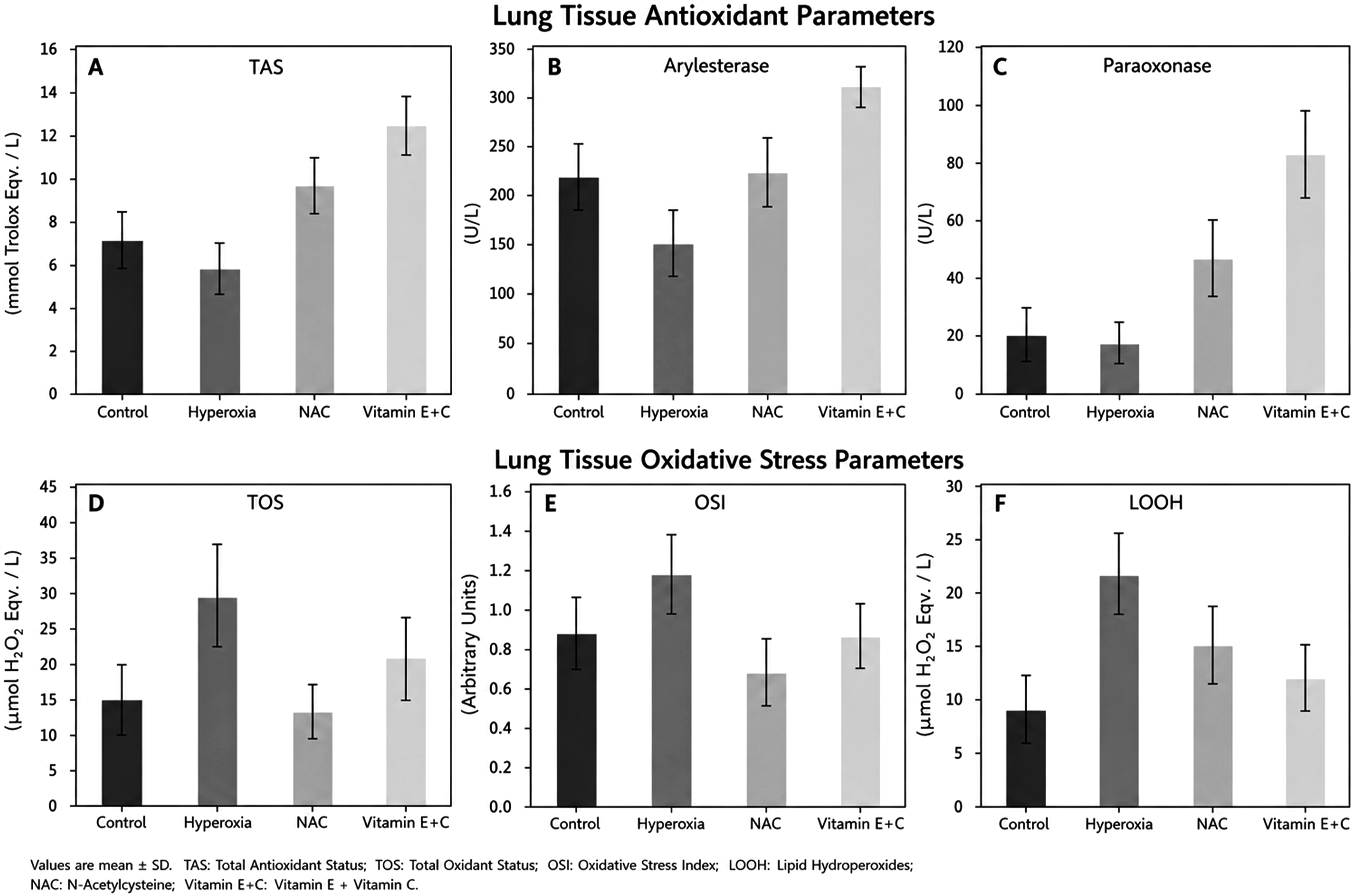
Lung tissue antioxidant and oxidative stress parameters across study groups. (a) Total antioxidant status (TAS), (b) arylesterase activity, (c) paraoxonase activity, (d) total oxidant status (TOS), (e) oxidative stress index (OSI), and (f) lipid hydroperoxide (LOOH) levels. Data are presented as mean ± SD. Detailed statistical comparisons are provided in Tables 5 and 6.
Oxidative stress parameters in lung tissue
Comparison of oxidative stress parameters in lung tissue between groups. (mean ± SD).
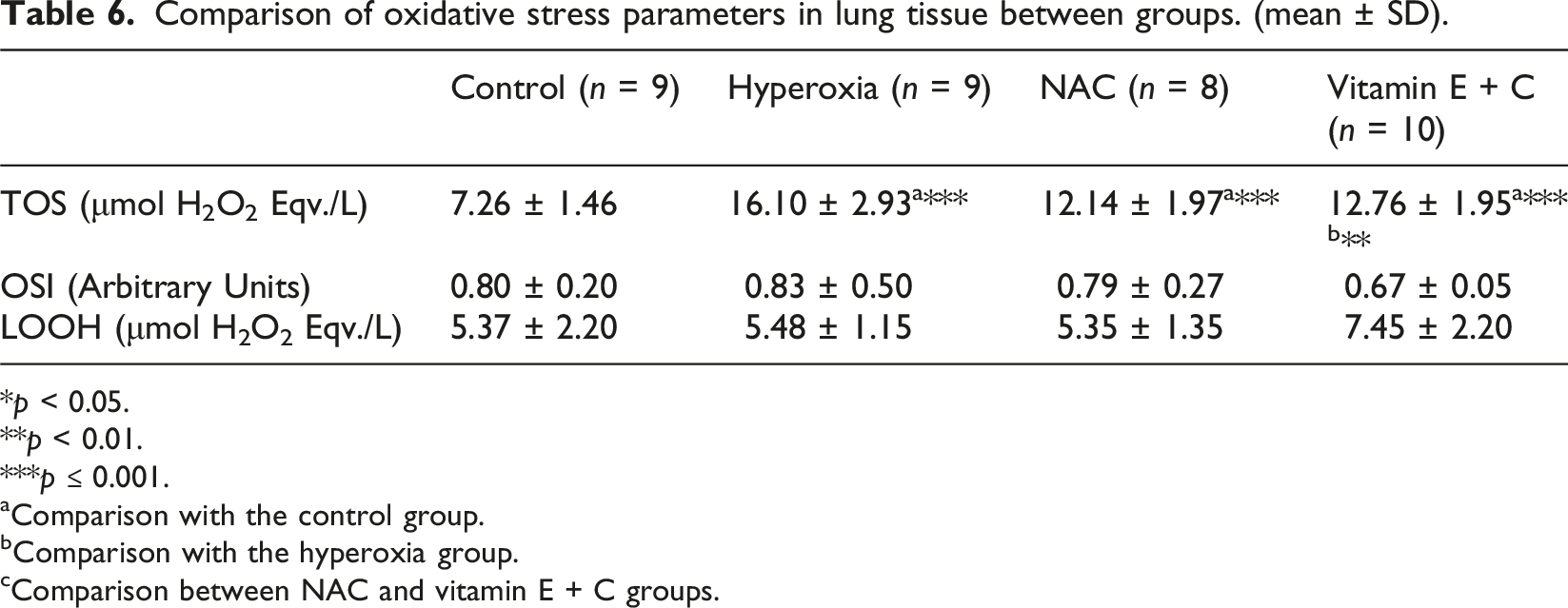
*p < 0.05.
**p < 0.01.
***p ≤ 0.001.
aComparison with the control group.
bComparison with the hyperoxia group.
cComparison between NAC and vitamin E + C groups.
Histopathological evaluation
Fibrosis was significantly more frequent in all hyperoxia-exposed groups compared with the control group (p = 0.002). No fibrosis was observed in the control group, whereas it was present in nearly all animals in the hyperoxia group.
In the NAC group, fibrosis was absent in a subset of animals and was predominantly mild in the remaining rats. Similarly, in the vitamin E + C group, fibrosis was absent in approximately half of the animals, while the remaining rats showed mostly mild and occasional moderate fibrosis. No severe fibrosis was observed in any group.
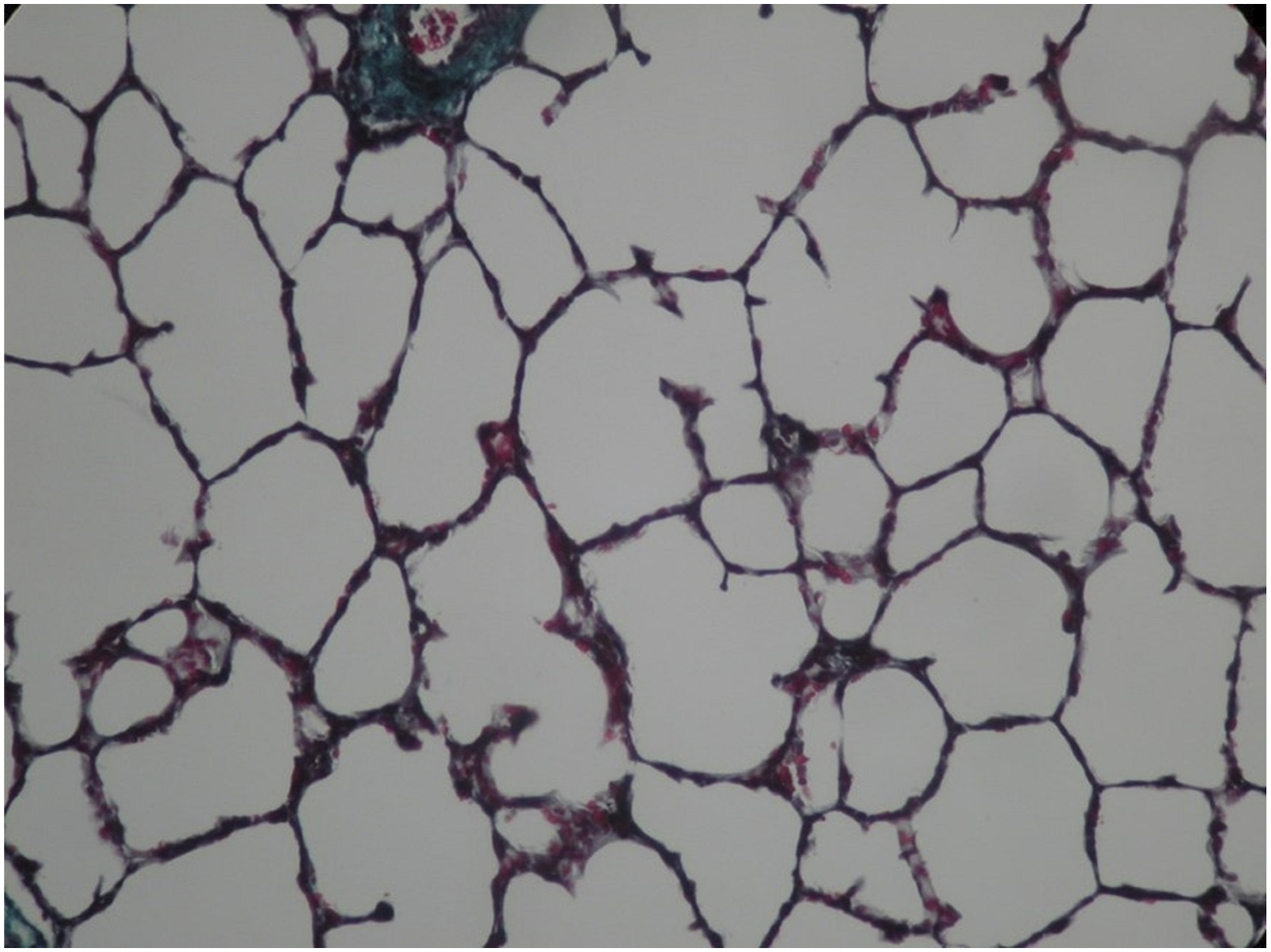
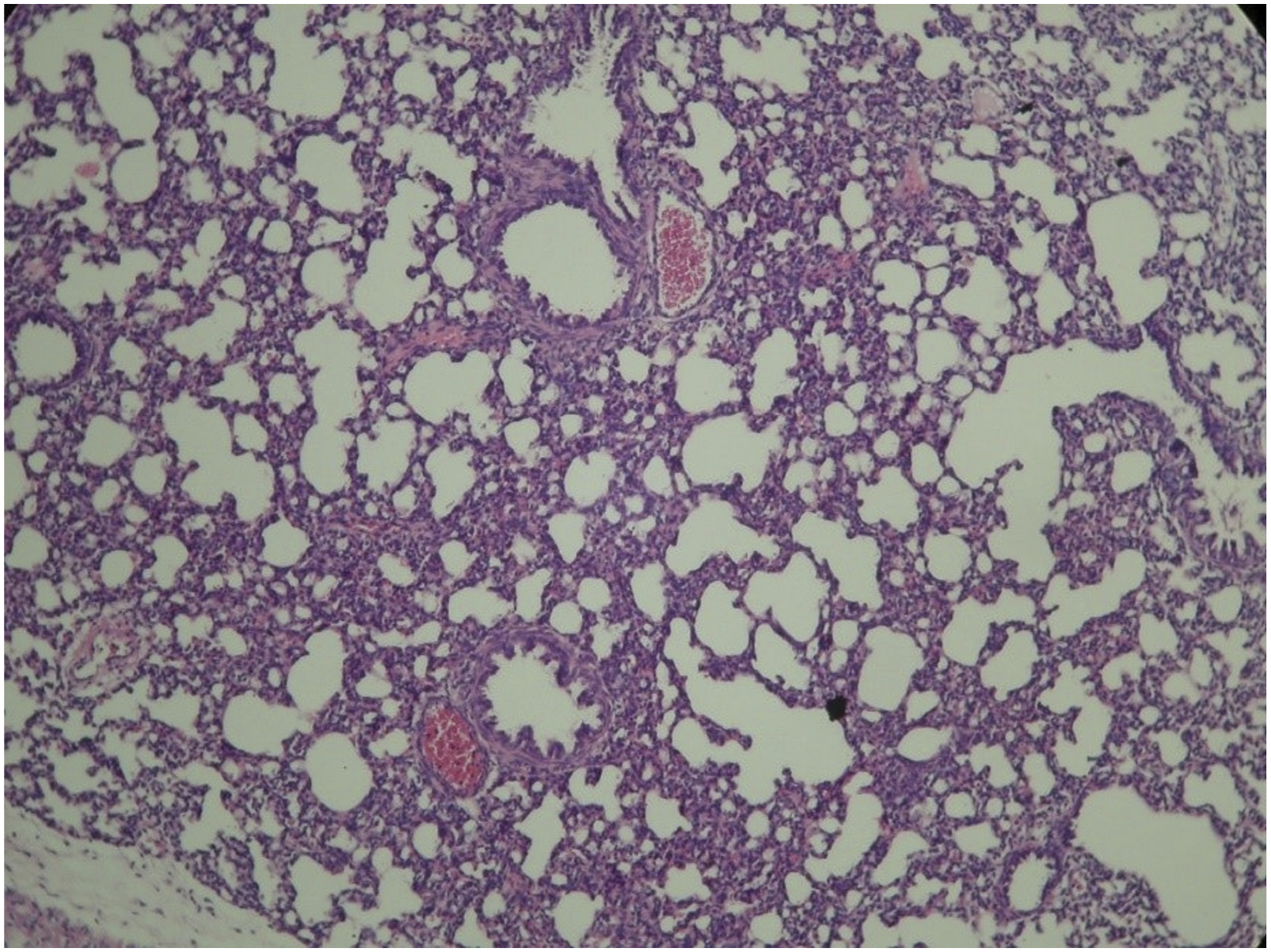
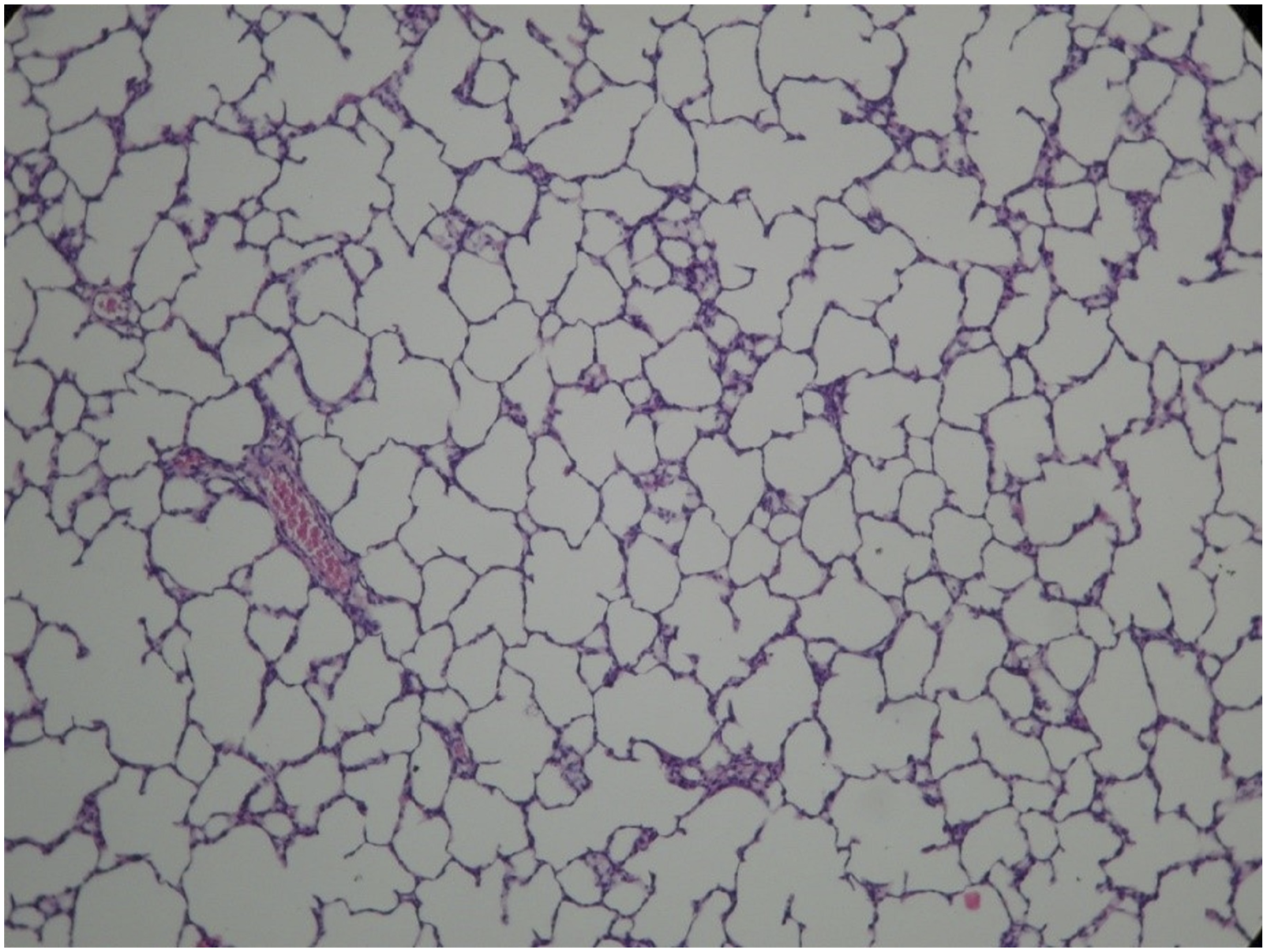
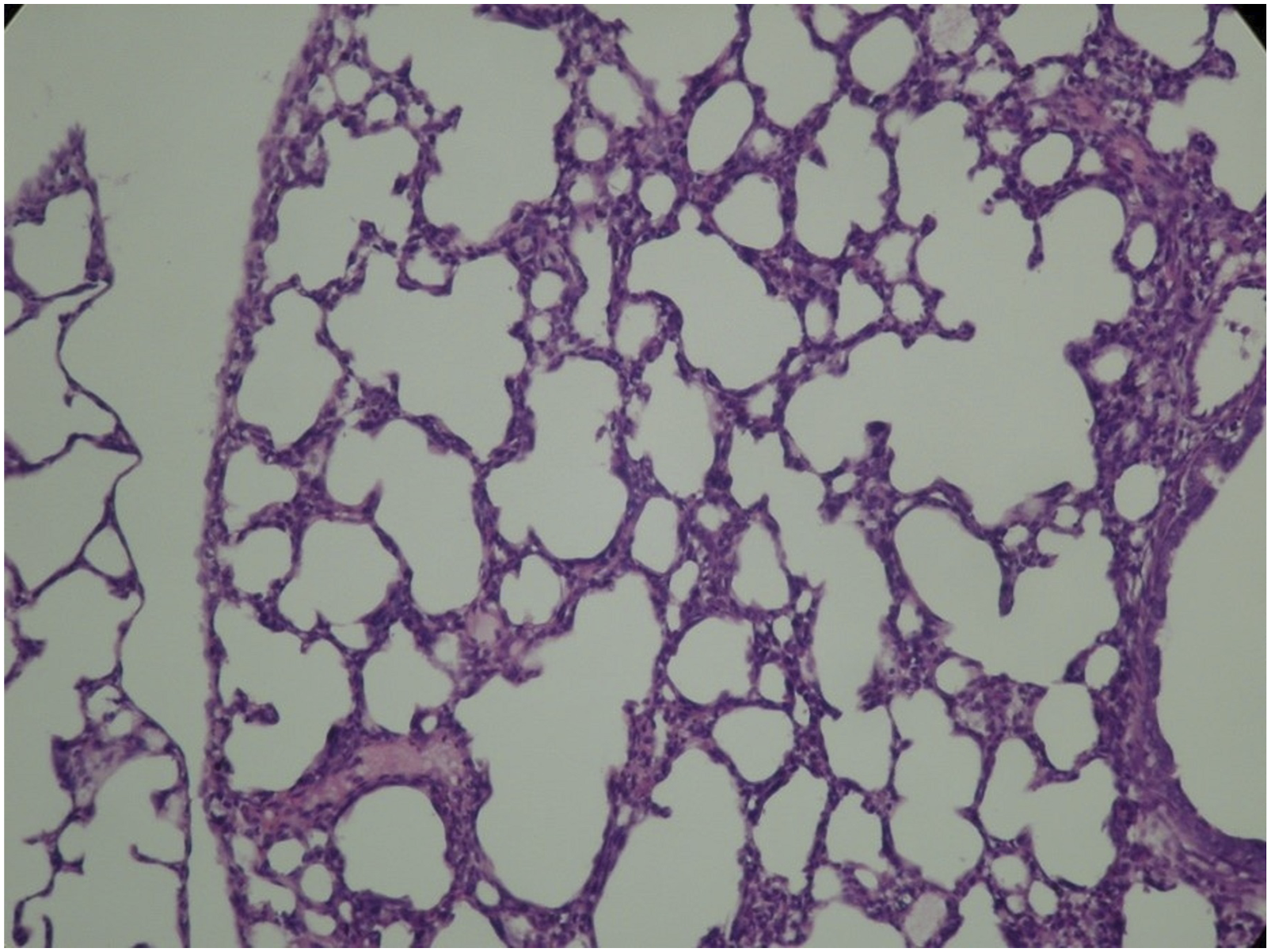
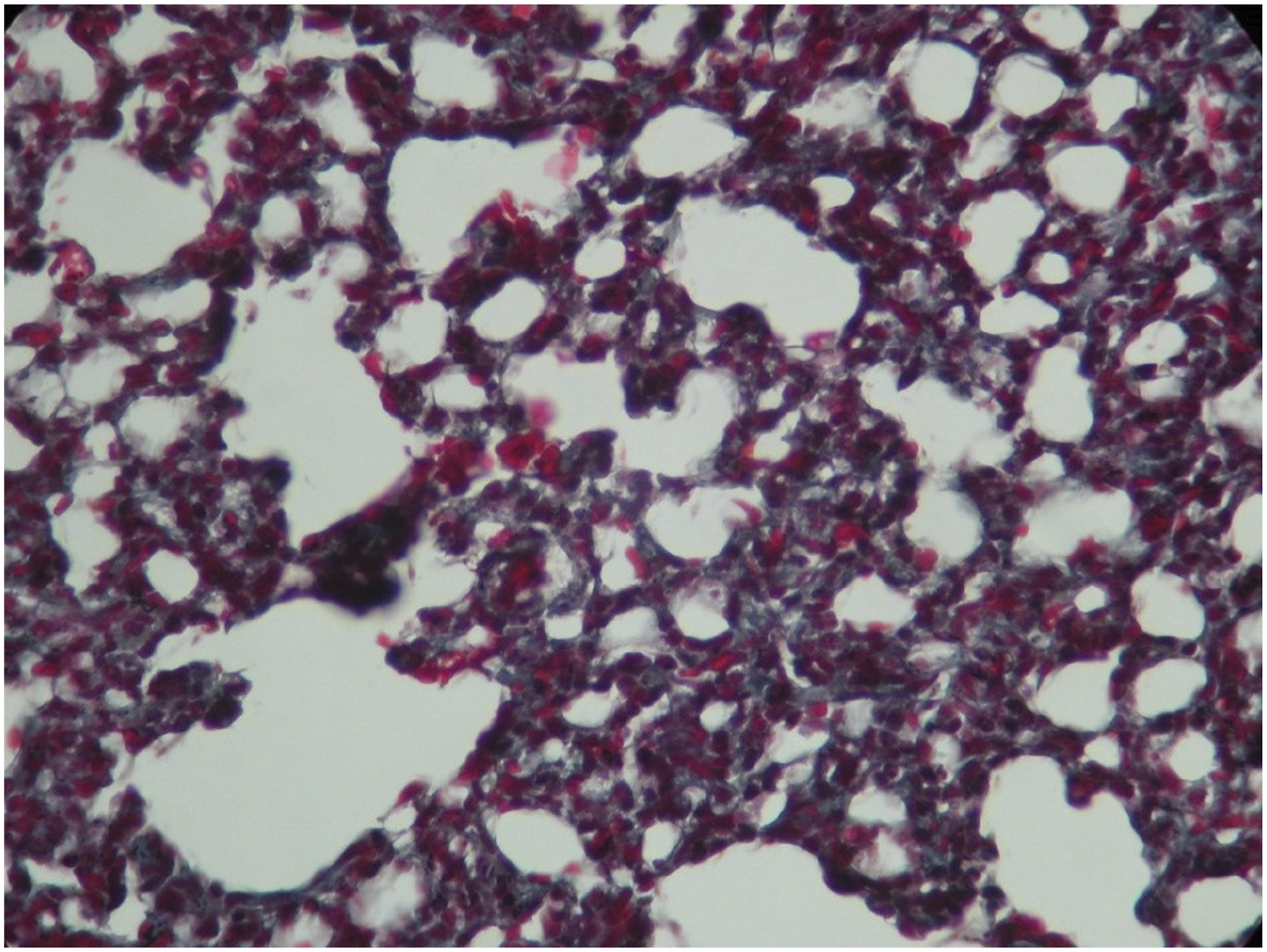
Histopathological examination demonstrated findings consistent with hyperoxia-induced lung injury, including alveolar simplification, septal thickening, inflammatory cell infiltration, and increased collagen deposition in the hyperoxia group. In contrast, both NAC and vitamin E + C treatment groups showed features suggestive of improved alveolar architecture, reduced inflammatory infiltration, and decreased collagen deposition compared with the hyperoxia group (Figures 3–8). Representative H&E-stained section of control lung showing normal alveolar architecture without inflammatory infiltration (original magnification ×200). Masson’s trichrome staining of control lung tissue demonstrating absence of collagen deposition (original magnification ×200). Hyperoxia group showing dense inflammatory infiltration, septal thickening, decreased septation, and distal airspace enlargement (H&E, ×200). Representative H&E-stained section showing reduced inflammatory infiltration and improved alveolar architecture in the NAC-treated group (original magnification ×200). Representative H&E-stained section showing reduced inflammation and near-normal lung architecture in the vitamin-treated group (original magnification ×200). Masson’s trichrome staining demonstrating increased collagen deposition and fibrosis in the hyperoxia group (×200).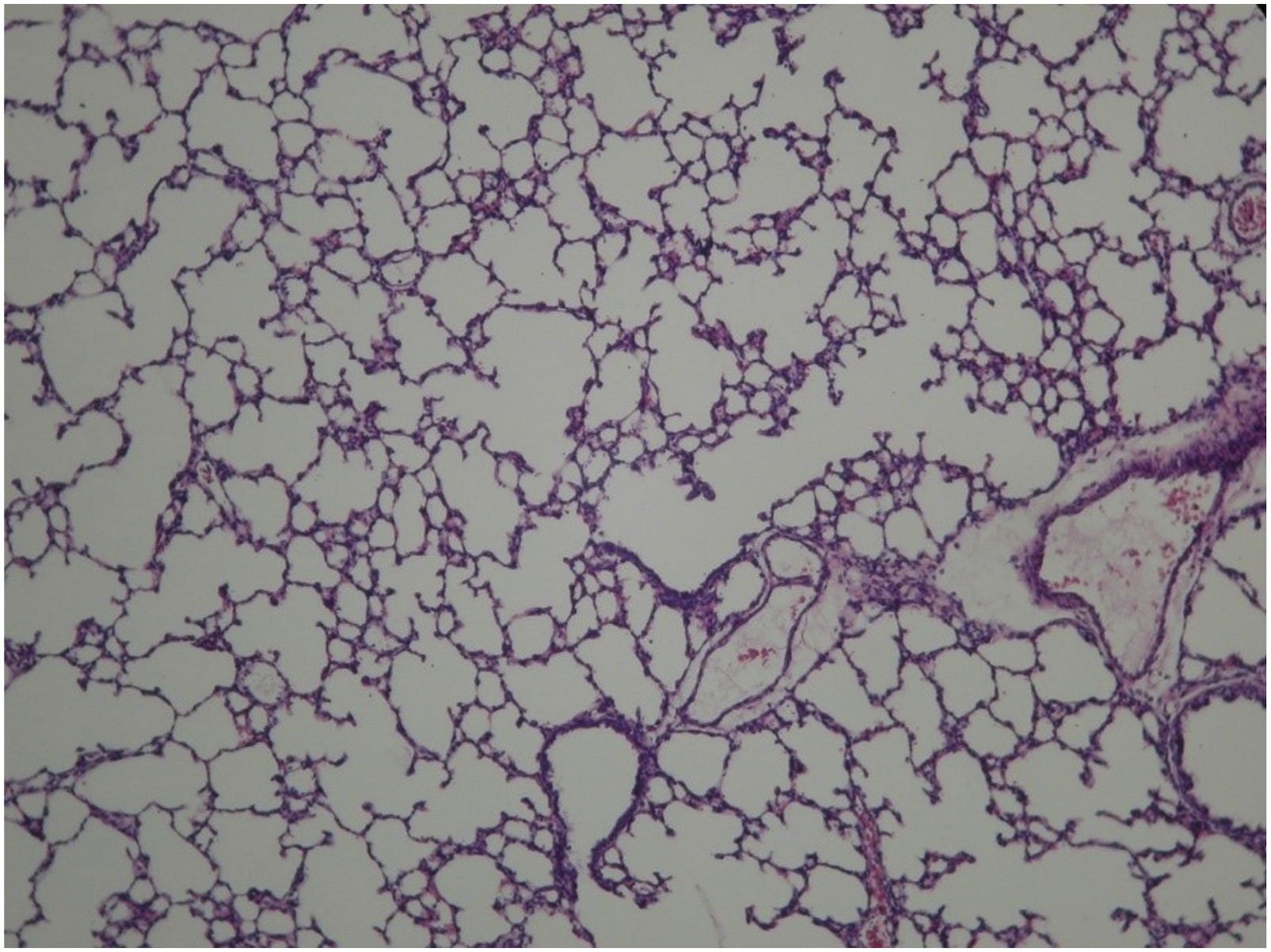
Discussion
Bronchopulmonary dysplasia (BPD) remains a major cause of morbidity in preterm infants, with oxidative stress playing a central role in its pathogenesis. 1 Despite advances in neonatal care, effective therapeutic strategies specifically targeting oxidative injury remain limited. In this context, evaluating antioxidant therapies in experimental models of hyperoxia-induced lung injury is of considerable importance.
In the present study, both N-acetylcysteine (NAC) and combined vitamin E + C therapy attenuated hyperoxia-induced lung injury in neonatal rats; however, they demonstrated differential effects in terms of magnitude and mechanism. Hyperoxia exposure resulted in increased oxidative stress parameters and the development of inflammatory and fibrotic changes in lung tissue, findings that are consistent with established experimental models of BPD.33–35 In contrast, both treatment strategies were associated with reduced oxidative stress, enhanced antioxidant capacity, and improved histopathological findings.
Our findings support the concept that hyperoxia induces oxidative stress, as reflected by increased TOS levels, although no significant differences were observed in OSI and LOOH levels. Interestingly, TAS and antioxidant enzyme activities were also elevated in the hyperoxia group. This increase likely represents a compensatory upregulation of endogenous antioxidant defenses in response to increased oxidative burden rather than effective protection against oxidative injury.17,18 This interpretation is consistent with previous studies demonstrating adaptive antioxidant responses under conditions of oxidative stress.
NAC treatment reduced oxidative stress parameters and significantly improved antioxidant capacity, particularly TAS and paraoxonase activity. These findings are consistent with experimental studies demonstrating that NAC attenuates oxidative stress and inflammation through glutathione replenishment and direct free radical scavenging.11,12,36 In our study, NAC reduced TOS, OSI, and LOOH levels in both tissue and serum; however, statistical significance was primarily observed for serum OSI levels. These results suggest that NAC may provide partial protection against hyperoxia-induced oxidative injury. Similarly, previous clinical studies have reported that NAC did not consistently reduce the incidence or severity of BPD when used alone.37,38 Taken together, these observations suggest that NAC predominantly enhances intracellular antioxidant defense through glutathione-dependent mechanisms but may have limited efficacy as a single-agent strategy.
Combined vitamin E and C therapy demonstrated a more pronounced effect on antioxidant defense mechanisms. The synergistic interaction between these vitamins enhances antioxidant capacity by inhibiting lipid peroxidation and regenerating oxidized vitamin E.15,16 In our study, this combination significantly increased TAS, paraoxonase, and arylesterase levels and was associated with reductions in oxidative stress parameters, particularly OSI. This effect may be particularly relevant for protecting cellular membranes from lipid peroxidation, which plays a critical role in hyperoxia-induced lung injury. In addition, the significantly increased arylesterase activity observed in the vitamin-treated group further supports the enhancement of antioxidant defense systems.39,40 Considering the reduced levels of antioxidant vitamins in preterm infants, this combination may offer a physiologically relevant approach to mitigating oxidative damage. 41
These findings highlight that NAC and vitamin E + C therapy exert complementary and mechanistically distinct effects. NAC appears to primarily enhance intracellular antioxidant mechanisms, whereas the vitamin combination more effectively targets lipid peroxidation and membrane stability. This distinction may have important implications for optimizing antioxidant strategies in neonatal lung injury and supports the concept that combination therapies may be more effective than single-agent approaches.15,16,36 The doses used in this study were based on previously published experimental studies demonstrating efficacy and acceptable safety profiles; however, different dosing regimens may yield variable effects.
The biochemical improvements observed in this study were supported by histopathological findings. Hyperoxia exposure was associated with findings consistent with alveolar simplification, septal thickening, inflammatory cell infiltration, and increased collagen deposition. In contrast, both NAC and vitamin E + C treatment groups demonstrated findings suggestive of improved alveolar architecture, reduced inflammatory infiltration, and decreased collagen accumulation compared with the hyperoxia group. These findings indicate that antioxidant therapies may provide protective effects not only at the biochemical level but also at the structural level.
Hyperoxia-induced lung injury involves complex interactions between oxidative stress, inflammation, and fibrotic pathways. Increased reactive oxygen species (ROS) production leads to activation of inflammatory cascades, cytokine release, and disruption of normal alveolar development. 42 In addition, interactions between oxidative stress and endoplasmic reticulum stress may further amplify lung injury through self-perpetuating mechanisms. 43 Our findings are consistent with these pathophysiological processes and suggest that modulation of oxidative stress may interrupt this cycle.
Although hyperoxia models reproduce several key features of BPD, they do not fully reflect the complex developmental arrest characteristic of the “new BPD” phenotype observed in preterm infants. Therefore, the findings of this experimental model should be interpreted within this limitation.
Limitations
This study has several limitations. First, the sample size was relatively small, which may have limited statistical power for some parameters. Second, quantitative morphometric analyses such as mean linear intercept or radial alveolar count were not performed. In addition, immunohistochemical markers associated with inflammation and fibrosis were not evaluated. Finally, long-term lung development and functional outcomes were not assessed. This limitation should be considered when interpreting the histopathological findings.
Conclusion
In conclusion, in a neonatal rat model of hyperoxia-induced lung injury, both NAC treatment and combined vitamin E + C therapy demonstrated protective effects. These findings support the concept that targeted antioxidant strategies may serve as adjunctive approaches alongside current interventions aimed at minimizing oxidative lung injury in preterm infants. However, further well-designed experimental and clinical studies are required to define their optimal therapeutic role.
Footnotes
Acknowledgments
The authors would like to thank Yaşar Sertdemir for statistical analysis.
Ethical considerations
The ethical approval for the study was obtained from the ethics committee established at the Medical Experiments Research and Application Center of Çukurova University Faculty of Medicine.
Author contributions
Narli N and Mutlu B designed and conducted the study. Mutlu B performed the experimental procedures. Gumurdulu D performed the pathological examination. All authors read and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data is contained within the article.