
Abstract
Much of the research on the social determinants of health has been done at national or international comparative levels. Findings from these studies highlight the importance of macro social factors that affect health outcomes, such as limited and unequal access to health care and the effects of racial discrimination, economic inequality, and patriarchy. However, such macro-level research provides limited information about how applied and clinical sociologists can address local social determinants of health and improve the well-being of individuals and community residents. Results from a county-level public health survey shed more specific light on how interpersonal networks, social activities, and neighborhood characteristics affect people’s physical and mental health. The results can be utilized by clinical and applied sociologists who counsel individuals and work to invigorate neighborhoods, and by public health officials who develop and reform community-level health policies and programs.
Since the late nineteenth century, some medical researchers conducted empirical studies of how day-to-day living conditions affect health (Carey and Crammond 2015). By the middle of the twentieth century, this supra-individual area of medical research had an official name, “social epidemiology” (Yankauer 1950). Over the past 68 years, social scientists have joined medical researchers in investigating how social environmental conditions and patterns of social interactions affect the health of individuals. One area of social epidemiology that sociologists have greatly contributed to has come to be known as the social determinants of health, or SDH (Cassel 1976; Cobb 1976).
As research accumulated that showed statistical associations between social factors (such as poverty, racial injustice, and gender inequality) and health outcomes, national and international agencies began to publish reports and to hold conferences on the SDH. For example, in 2011, the World Health Organization (WHO) held the World Conference on Social Determinants of Health in Rio de Janeiro, Brazil (WHO 2015). Within the United States, research on how broad social factors, such as race, class, and neighborhoods, affect health led to a three-part seminar series on the Social Determinants of Health, Law, and Policy at Brown University in 2012 (De Maio, Mazzeo, and Ritchie 2013). The social ecological approach to improving health also has a central role in the federal government’s Healthy People 2020 initiative (Office of Disease Prevention and Health Promotion 2015).
While national and international research and conferences that draw attention to macro-level political and economic issues are essential, they tend to produce broad action plans and general goals. The five action areas defined at the 2011 WHO conference focused on macro-level changes, such as broadening participation in health care policy formation and reducing economic inequalities in access to quality care. Similarly, the five key areas of SDH identified during the Brown University seminars included macro-level issues of income inequality, racial discrimination, housing inadequacy, and food insecurity.
All sociologists know that reducing social problems, including public health problems, requires attention to institutional-level political economic factors. However, large structural analyses and the broad policy and action themes that they produce do not provide much guidance for how local public health officials, social services personnel, and applied and clinical sociologists can take action to address negative social factors and to improve people’s health (Baum et al. 2013). What Krumeich and Meershoek (2014:7) describe as “the unproblematic introduction of global [SDH] standards in local context” is likely one reason that “examples of effective, sustainable intervention and policy explicitly inspired by SDH frameworks are difficult to find.”
As Droomers et al. (2014:122) note, neighborhood and area-based interventions “are one possible way to . . . tackle the social determinants of health” (see also Baum et al. 2013; Keyes 1998). The “localism approach” (Crowley, Balaram, and Lee 2012:2) supplements macro-level analyses of the SDH and provides more specific information that can be applied in community and neighborhood contexts by sociologists. Our study, thus, adds to the small but growing literature on local SDHs, and it sheds light on which specific SDHs have the strongest association with health and well-being in one community.
Below, we describe the methodology that we utilized, explain some key research findings, provide suggestions for moving research on the local SDH forward, and discuss how the findings can be used by applied and clinical sociologists to improve local public health.
Survey Method and Sample
During the summer of 2014, a draft questionnaire was developed by the authors in collaboration with four officials from the county public health department. Pre-tests showed that the instrument needed to be shortened, and a revised 71-item survey was developed (available on request from the authors). During the fall of 2014, telephone surveys were conducted with a random sample of 391 adults ages 18 to 64 (a separate sample not used in this paper was of individuals ages 65 and older).
The average age of respondents was 51 years old. The sample was ethnically homogeneous, as 91.8 percent of respondents identified as white, 2.8 percent were Hispanic/Latino, and 2.3 percent were black/African American. This homogeneity is representative of the county’s population, which is 91.3 percent white (U.S. Census Bureau 2014). As with many surveys, more women participated than men. Two-thirds of respondents were female, and one-third were male. One in 10 county residents ages 25 and older had not graduated from high school, whereas 3.1 percent of sample respondents were high school dropouts (U.S. Census Bureau 2014). Nineteen percent of respondents had a household income between $40,000 and $60,000, and 38 percent of respondents reported a household income more than $60,000. Thus, 57 percent of our sample had household incomes of $40,000 or more, while the median income of the county was $40,337 (U.S. Census Bureau 2014). Thus, sample respondents were somewhat better educated and had a slightly higher income than county residents as a whole.
In summary, the randomly drawn sample was representative by age and ethnic group for the county as a whole, and similar proportions of people from low- and high-income categories participated. However, more women than men answered survey questions. These sample characteristics should be considered when interpreting the results presented below.
Concepts and Operationalizations
Socioeconomic Status
There is strong evidence in the sociological literature that individuals’ social standing affects their life chances, including their chance to be healthy (Wilkinson and Pickett 2009). We constructed a measure of individuals’ socioeconomic status (SES), which was measured as a combination of people’s income category and their highest level of education completed (see appendix for survey questions used to operationalize all variables discussed in this section).
Behaviors Affecting Health
We measured nine individual behaviors that affect people’s health, including number of sodas, glasses of water, and alcoholic drinks consumed per day, eating habits, sleep patterns, frequency of using stress relief techniques, how often people practice a positive outlook, hours spent watching TV, and days of exercise per week. 1
Well-Being
Human health and well-being is a complex concept. Early social epidemiology medical researchers typically viewed physical health narrowly as the absence of diagnosed chronic physical illnesses, while psychologists most often utilized broad measures of life satisfaction or happiness to investigate mental and emotional well-being (Keyes 1998). We used six measures of well-being, including subjective assessments of mental and physical health and the presence or absence of four chronic illnesses (high blood pressure, high cholesterol, diabetes, and a respiratory or lung illness such as asthma, chronic obstructive pulmonary disease [COPD], chronic bronchitis, or emphysema). The composite operationalization of well-being goes beyond the lack of physical illnesses and includes the presence of good physical and mental health. The multidimensional variable that we established is consistent with current “wellness” models that understand that physical and mental health are highly interrelated and mutually reinforcing aspects of well-being.
Community-Level Social Determinants of Health
As was previously mentioned, most studies of the SDH have focused on associations between national-level factors (such as income inequality, poverty and violence rates, and access to health care) and macro-level public health measures (e.g., national infant mortality and chronic illness rates, and longevity).
To investigate social factors that affect health and well-being within a community, we developed a three-dimensional conceptualization of the local SDH (see Figure 1). The structural component was respondents’ network size and degree of social isolation. The social interactional dimension was the frequency and positive nature of people’s social activities. And the social environmental aspect was how safe people felt in their area and how comfortable they were asking a neighbor for help.
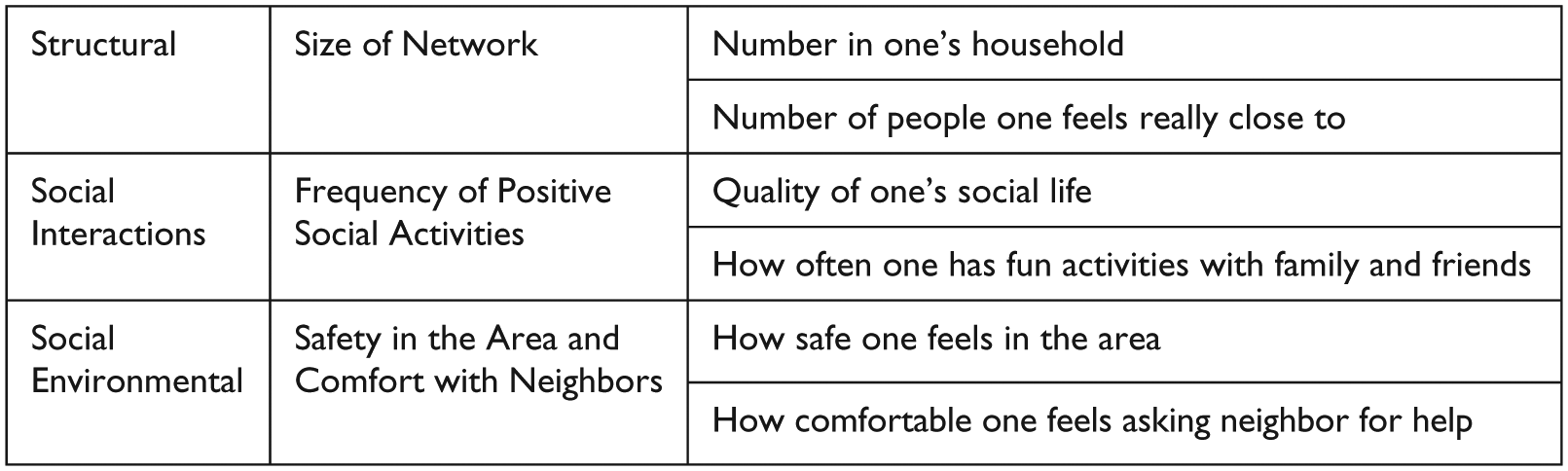
Community-level social determinants of health.
Social network theory was first applied to health outcomes by physicians in the mid-1970s (Cassel 1976; Cobb 1976). Since then, social scientists increasingly have studied the mechanisms through which social networks affect health (Smith and Christakis 2008). Our measure of the structural dimension of the local SDH is the size of individuals’ personal networks. This is operationalized by combining how many people lived in respondents’ households with how many people respondents felt really close to and could discuss a personal problem with. The structural component, thus, measures how many people an individual is physically close to (in the same household) and feels emotionally close with (can discuss a personal problem with).
One common finding is that the relationship between network size and health outcomes may not be linear. The primary negative effects come from social isolation. As Steve Cole noted (quoted in Dobbs 2013:9), “social isolation is the best-established, most robust social or psychological risk factor for disease out there. Nothing can compete.” We therefore utilized both a scale and a categorical measure of social isolation to investigate the connection between the structural dimension of local SDH and well-being. It is important to recognize that the association between social isolation and well-being is multidirectional. Social isolation may worsen well-being, and poor physical and mental health may result in more social isolation. As we discuss in a later section, clinical sociological practitioners need to intervene in this possible cyclical relationship.
What the social interaction component of local SDH adds is how often individuals actually spend time with others (Cacioppo and Cacioppo 2014; Shor and Roelfs 2015). Since the 1980s, many studies have documented that social relationships and social activities are associated with a variety of health outcomes (Holt-Lunstad and Smith 2012; Shor and Roelfs 2015). Our measure of the social interaction dimension of the local SDH combines respondents’ assessment of the quality of their social life with how often they do fun activities with family and friends. As is shown below, it is important conceptually and analytically to distinguish between people’s social interactions with others, and their personal actions, such as eating habits or time spent watching television.
The quality of the neighborhood in which people live, which is the social environmental dimension of local SDH, also affects their well-being (Carpiano 2007). For example, E. S. Kim, Hawes, and Smith (2014:1020) reported that “a growing body of literature suggests that neighborhood characteristics impact cardiovascular health,” which is the leading cause of death among adults in the United States. Most researchers have focused on how negative neighborhood characteristics (such a high poverty, crime, and violence rates) harm the health of residents. As Catherine Lucey noted, “whether or not someone becomes ill has a lot to do with the society in which they live.” If children “live in a violent neighborhood, . . . they are much more likely to develop diabetes, high blood pressure, obesity, and many other chronic illnesses, because of their social environment” (quoted in Dembosky 2015:2).
Droomers et al. (2014) noted that a residents’ perception of safety and their sense of social cohesion were key features of neighborhoods that were associated with positive health outcomes. We combined the level of safety that participants felt in their neighborhood with their comfortableness asking a neighbor for help if they had a health problem as our measure of the social environmental dimension of the local SDH.
While our three-dimensional operationalization captures an important subset of the local SDH, we did not include several commonly recognized SDHs in our analysis. Ward et al. (2014) found that nonheterosexuals reported lower levels of mental and physical health than did heterosexuals, and the American Medical Student Association (2017) noted that transgender people face barriers to care and experience some health disparities compared with cisgender individuals. Our survey instrument did not ask respondents about their gender identity or sexual orientation, so we were unable to include these SDHs in our analysis.
Respondents did identify their race and gender. Our sample was 92.8 percent white, so we combined racial minority groups to create a white/nonwhite variable. However, this measure of race did not have a statistically significant association with our measure of well-being. Gender (female or male) also did not have a significant association with well-being. So, four local SDHs that have been identified in some research could not be used in our investigation.
There are no perfect operationalizations for the complex concepts of local SDH and human well-being. However, we feel that the multifaceted definitions that we utilize do have substantial construct and face validity as measures of those important social science concepts.
The Structural Component of Local SDH and Well-Being
Initial correlation analyses showed that the structural component of local SDH, network size, did not have a statistically significant association with the well-being composite variable (reported in column 8 of Table 2). More detailed analyses showed that network size had only a moderate positive correlation with mental and emotional health (Rho = .127, p < .05). The structural aspect of local SDH did not have a statistically significant association with self-reported physical health or with four chronic illnesses. However, as was explained above, previous research suggests that network size may be related to health primarily at the low end of the scale. We, therefore, established a categorical social isolation variable to better measure the relationship between the structural element of local SDH and well-being.
No numerical threshold of social isolation has been identified in previous network studies (Holt-Lunstad and Smith 2012:46). However, as Dobbs (2013) noted, the impact of social isolation on health outcomes may be strongest at the extreme low end of network size. To test this idea, we designated individuals with three or fewer people in their social network as being socially isolated, and all other participants were viewed as not being socially isolated. Social isolation was associated with five of the six elements of our composite measure of well-being.
Socially isolated people were 70 percent more likely to have high blood pressure, and two and one-half times more likely to have diabetes or a respiratory illness compared with those who were not socially isolated (see Table 1). Socially isolated people also were twice as likely to report their physical health as poor or fair, and three times more likely to report poor or fair mental health compared with individuals who were not socially isolated.
Health Impacts of Social Isolation.
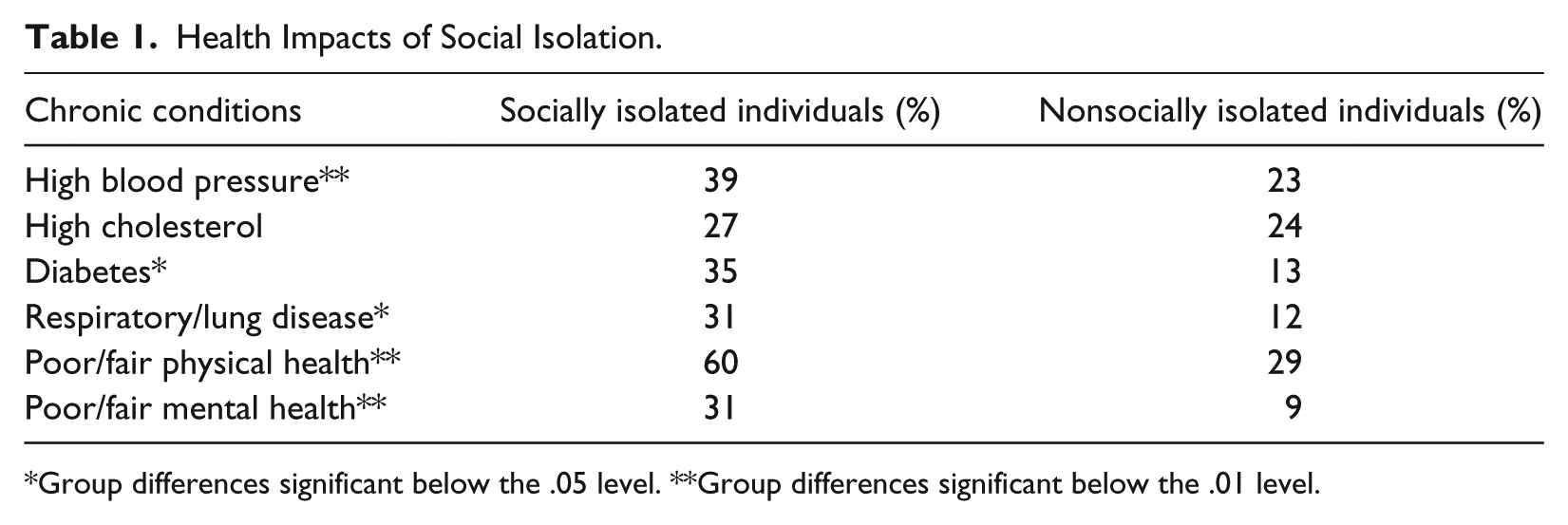
Group differences significant below the .05 level. **Group differences significant below the .01 level.
SES, Local SDH, Personal Behaviors, and Well-Being
We analyzed associations between well-being and two social factors: SES and the local SDH. The right-hand column of Table 2 shows that SES is positively correlated with well-being (Rho = .482; p < .01).
Correlates with Well-Being.
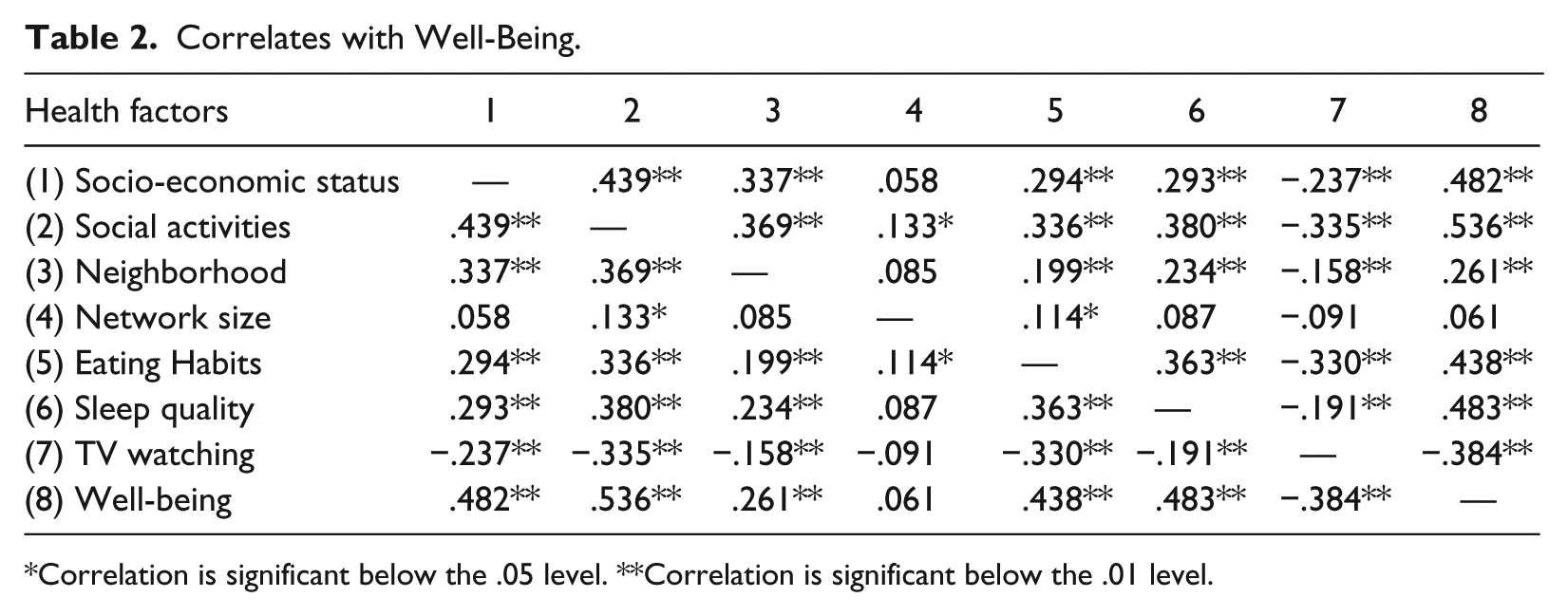
Correlation is significant below the .05 level. **Correlation is significant below the .01 level.
Further analyses suggested that among people in our sample, this association stems in part from how SES affects peoples’ access to health insurance, their use of regular health screenings, and their health-related behaviors. We collapsed the scale measure of SES used in correlations into a separate two-category, low- and high-SES variable (see appendix) to test for an association between SES and nominal measures of insurance coverage, health screenings, and smoking. More than 90 percent of high-SES individuals had health insurance, compared with 70 percent of low-SES people (see Table 3). And, among those with health care coverage, more high-SES participants than low-SES persons had insurance that covered annual medical screenings. Fewer low-SES than high-SES respondents had had a physical in the past year, probably because they were less likely to have comprehensive health insurance. Thus, SES is related with unequal access to high-quality insurance and differences in preventative health care practices that likely affect well-being.
SES, Insurance, and Health-Related Behaviors.

Group differences significant below the .05 level. **Group differences significant below the .01 level.
SES = Socio-economic status.
SES also was related to the three behaviors in Table 2 that are correlated with well-being. Low-SES individuals were over twice as likely to report poor or fair eating habits compared with high-SES persons. Those who were lower on the social status ladder also were nearly twice as likely to say that they had poor or fair sleep quality compared with higher-status people. Three times as many low-SES individuals than high-SES people watched seven or more hours of TV daily.
In addition, low-SES individuals are four times more likely than high-SES people to use tobacco regularly. Although the nominal tobacco use variable was not included in correlations, a separate cross table analysis using an ordinal well-being measure showed that 39 percent of regular tobacco users reported high well-being, while 68 percent of nonusers of tobacco did so (p < .01). Thus, SES indirectly affects well-being through its association access to and quality of health insurance, frequency of medical screenings, and health-related behaviors.
As Table 2 showed, network size did not have a linear association with well-being. However, the neighborhood quality and social interaction components of local SDH had relatively strong associations (Rho = .261, p < .01, and Rho = .536, p < .01, respectively) with our composite measure of well-being. This suggests that beyond social isolation, it is not how many people individuals know and feel close with that most affects their well-being. Rather, it is how often individuals engage with others in fun activities and how safe and comfortable they feel in their immediate social environment that matters most.
Among the seven variables that we tested, the social interaction dimension of the local SDH had the strongest correlation with well-being (column 8 of Table 2). The social environmental dimension, neighborhood quality, had a somewhat weaker but statistically significant connection with well-being. Both interaction and environmental components of the local SDH also were interrelated with eating habits, sleep quality, and TV watching. It makes sense that people with more active social lives and who live in safe neighborhoods would watch less TV. The association between the social interaction and environmental aspects of local SDH and eating patterns and sleep quality is less intuitive.
Overall, our survey results suggest that along with SES status and some health-related behaviors, all three dimensions of local SDH have a significant impact on well-being.
Implications for Theory
Theories try to explain how one factor affects another, and why relationships between variables exist. Our research was not designed to test social epidemiological theories that explain how social factors affect health and well-being. Nonetheless, a brief discussion of those theories is warranted to inform future studies of the local SDH. Currently the exact pathways through which social factors affect health remain a “black box” (Shor and Roelfs 2015:77). No one knows precisely how external factors in the social world get through peoples’ skin to trigger biological processes inside of individuals that affect their health. However, researchers in three fields (neuroscience, epigenetics, and endocrinology) are investigating the social-physiological mechanisms that might account for how the SDH affect health. First, neuroscientists are focusing on how social experiences affect brain and nervous system development. For example, researchers have demonstrated that early life experiences of poverty affect the structural development of children’s brains (Badger 2013; Hanson et al. 2013; Landau 2013). Next, epigeneticists have come to realize that social experiences act as dimmer switches that reduce or intensify the expression of genetic health or illness predispositions. As Dobbs (2013:5) explained, “our social life can change our gene expression with a rapidity, breadth, and depth previously overlooked.” Third, medical researchers have noted that the human body responds to negative social experiences by generating high levels of cortisol and other stress-related hormones that are associated with a range of health problems. This is a chemical pathway through which negative social conditions and experiences “get under the skin” of individuals and adversely affect their mental and physical well-being (Wilkinson and Pickett 2009:31). Most likely, the SDHs impact a mix of neurological, genetic, and chemical processes within the body to affect health and well-being.
Our results do help explain why some of the relationships found in the sociological and health literature occur. For example, the Moving to Opportunity program from the mid-1990s provided vouchers for some low-income families (chosen by lottery) to move to better neighborhoods. Early evaluations showed that living in a better neighborhood had little to no effect on the physical and mental health of people (Parry 2012). Our SDH results shed new light on this finding. First, geographical mobility may have severed local supportive social network ties for low-income people, which worsened their physical and mental health. Second, the individuals had not lived in a new neighborhood long enough to feel safe, build trusting relationships with neighbors, and begin to engage in regular social activities. It is interesting to note that a recent study found much stronger positive health outcomes of people who had been children during the Moving to Opportunity program (Leonhardt, Cox, and Miller 2015). Thus, it is possible that there is a lag effect between moving to a better neighborhood (and improving the local SDH) and better health outcomes for individuals.
Implications for Future Research
The questionnaire used to generate our data was part of a public health survey that was constructed in collaboration with officials from the county health department. To keep the instrument short, we had to limit the number of questions pertaining to local SDH and health outcomes. The collaboratively constructed questionnaire also generated various levels of measurement of key variables. Investigating associations among the limited number of variables with different levels of measurement required us to utilize different analytical processes. When possible, index variables (such as the local SDH and well-being) were created to allow for correlation analysis. When key variables were nominal, then responses for some constructs were collapsed to create categorical variables, which allowed cross-tabulation to be used.
Even given the data restrictions noted above, our study made several methodological contributions that can be built on in future research to provide more specific information on the local SDH. First, our three-part measurement of well-being, which consisted of respondents’ subjective evaluations of their physical and mental health and presence or absence of four chronic illnesses, was more comprehensive than most operationalized definitions used by previous researchers. However, well-being is a complex, multidimensional concept, and cross-disciplinary teams of medical, behavioral, and social science researchers are needed to continue to refine measures of wellness. Studies that combine multiple subjective evaluations of physical and mental health with a broad array of objective medical health measures would be an advancement in operationalizing well-being.
Our tripartite conceptualization of SDH that included structural, social interactional, and social environmental dimensions also was an advancement on local area studies of social factors that affect health. However, more work needs to be done to capture the richness of the local SDH concept. In addition to including sexual orientation and gender identity as SDH variables, future studies could improve on our structural, interactional, and neighborhood measures.
Our structural SDH variable only measured the size of people’s networks. But, as Smith and Christakis (2008) noted, thorough measures should account for the size, density, and heterogeneity or homogeneity of networks. Qualities of personal networks other than social isolation also likely affect health and wellness.
A more multifaceted measure of social interactions is needed to identify which types of activities with which groups of people (family members or friends, for example) have the strongest association with health. One possible advancement would be to build on the variety of measures of social relationships used by Holt-Lunstad and Smith (2012:46). Their “multi-faceted measurement” of social relationships utilized functional measures of social support interactions and structural measures of activities that bring a sense of integration.
Previous research on neighborhood quality (which is the social environmental aspect of local SDH) and health outcomes has relied largely on secondary socioeconomic, demographic, and urban geography data. Crime and poverty rates, school test scores, median income, racial group composition, quality of sidewalks and number of abandoned buildings have been used as measures of neighborhood quality (Mast 2010; Rollings, Wells, and Evans 2015). More direct assessments of the social environment of neighborhoods could be added to strengthen measures of neighborhood quality. One possible improvement would be to utilize survey measures of local social capital (Mohnen et al. 2015). Chi and Carpiano (2013) operationalized four types of neighborhood-based social capital: social support (connections and activities that help people meet regular challenges), social leverage (sharing information on health-related issues), informal social controls (to maintain safety), and participation in neighborhood organizations (to create a sense of integration and improve the local quality of life). Those or similar direct measures of the social environment of neighborhoods would improve our understanding of the local SDH.
According to Max Weber ([1917] 1946:138), it is our duty as sociologists to disseminate the results of our research, and then hope that others soon will do better: “Every scientific ‘fulfilment’ raises new ‘questions’; it asks to be ‘surpassed’ and outdated . . . We cannot work without hoping that others will advance further than we have, . . . for it is our common fate, and, more, our common goal.” Improved future research designs and methods will produce more specific findings that will, in turn, allow for more effective, evidence-based policies and programs to be implemented.
It is a daunting task to better understand the many SDHs and the complex pathways through which they affect health, for as Krumeich and Meershoek (2014:4) point out, “everything can be related to everything in an endless number of ways.” However, a mix of future area-based studies across different regions and types of communities (urban/rural, low SES/high SES, ethnically diverse/ethnically homogeneous, etc.) should allow for patterns to emerge concerning what SDHs affect which health and well-being outcomes. If researchers developed scale measures of key SDHs and of well-being and utilized multivariate analyses, then at least some elements of the complex processes may come into focus and provide information for incremental improvements in policies and programs. While such a “localism approach” (Crowley et al. 2012:2) will take time, merely amassing still more national and international data holds very little promise of untangling the web of factors and pathways through which the SDHs affect well-being. While more research is needed, we can utilize our findings and results from existing small-area studies to inform and improve sociological practices to better the health of people in many neighborhoods.
Implications for Sociological Practice
Because most SDH research has been conducted at national and international levels, it is not surprising that the policy and practice recommendations usually are at those same levels. As research results have mounted over the last 40 years, “evidence on the social determinants of health has prompted calls for widespread political action at both a national and global level” (Carey and Crammond 2015:134; Wilkinson and Pickett 2009). The 2008 and 2011 WHO conferences on the social determinants of health produced action plans that center on multinational and national-level institutional reforms to establish equal access to high-quality health care for all (WHO 2008, 2015).
We sociologists should never take our eye away from institutional inadequacies and widespread inequalities that are leading causes of poor health outcomes in many neighborhoods. Advocating for “upstream change” in the nation’s health care institution is vital (Carey and Crammond 2015). However, while macro institutional reforms are essential, downstream changes in the communities where people actually live also are needed.
Droomers et al. (2014:122) pointed out that “area-based interventions that target deprived neighborhoods are one possible way to deliver the complex interventions needed to tackle the social determinants of health.” In fact, several countries have experimented with community-based public health programs in the past two decades. These include England’s Health Action Zones and the broader New Deal for Communities Program, and The District Approach in the Netherlands. In these programs, emphasis was placed on creating greater access to medical care, improving education, housing and employment, and promoting healthy lifestyles (Judge and Bauld 2006:342). While such efforts are necessary, they seem to be insufficient, as only modest and inconsistent health gains occurred through these small-area programs (Batty et al. 2010; Leonhardt et al. 2015). As Droomers et al. (2014:122) state, “Experiences thus far have . . . failed to come up with conclusive empirical evidence showing positive health impacts of area-based interventions.” Our research suggests that there is a need to refocus area-based programs and place more emphasis on strengthening individuals’ social networks, creating more opportunities for positive social interactions and relationships, and improving the social environment in neighborhoods. In short, programs to alter the local SDH and improve health outcomes need to be more sociological.
Distinctions between the work of applied and clinical sociologists are somewhat blurred, and considerable overlap in their efforts exists. One way to think about sociological practice to address the local SDH and improve well-being is that clinical sociologists may focus on changes at the micro level of individuals and households. Applied sociologists would help implement changes at the meso neighborhood or community levels.
The position of community health case manager provides an opportunity for both types of sociological practice. At the micro level, individuals or household members are the cases to be managed. Presently, most community health case managers are either nurses or social workers with a background in counseling who work at the micro level (K. Kim et al. 2016). Both groups of community health case managers likely have some familiarity with the SDH literature. However, as Holt-Lunstad and Smith (2012) maintain, many public health officials simply do not know how to strengthen protective social factors and reduce risk-magnifying social factors. For instance, an online training module for community health social workers does acknowledge “the central importance of human relationships”; however, building strong interpersonal networks and establishing opportunities for positive interactions are not mentioned as steps in the case management process (Zralek 2012:6). Clinical sociologists as community health case managers would place extending and strengthening the networks of individuals and household members and establishing reoccurring opportunities for positive social interactions at the core of their micro-level practice.
Counseling individuals and households to reduce unhealthy behaviors (tobacco use, alcohol abuse, and many hours spent watching TV) and to promote healthy behaviors (good sleep patterns, regular exercise, and healthy eating habits) is necessary. Our results suggest that those actions need to be augmented by sociological interventions with individuals and households to avoid social isolation, especially for those whose mental or physical illnesses may already limit their social ties, and to enhance their social activities. Many senior living centers offer communal meals and regular group activities. Younger individuals living independently might be encouraged to eat meals with family members or close friends, and to interact with others through neighborhood association meetings, community programs, and local events.
At the meso-level of community health case management, the neighborhood itself becomes the case to be managed by applied sociologists. The social conditions of the community need to be improved. The failure by current practitioners to acknowledge the importance of improving the local social environment as a step to bettering health outcomes is demonstrated by the Assertive Community Treatment (ACT 2009) practice. In this program, teams of behavioral and health care officials engage in assertive outreach to and treatment of individuals in the community. ACT focuses on providing effective diagnoses and services to individuals where they live, not on improving the community itself.
Although such programs are important, they reproduce a bias toward psychological and medical models of health that downplay the significance of the SDH. As Crowley et al. (2012) noted, most existing programs to help disadvantaged people attain better health outcomes without addressing conditions where they live have shown limited effectiveness. One reason for the limited success is that there has been an imbalance between initiatives to change individuals and efforts to improve neighborhoods. In other words, programs to help people have taken priority over efforts to improve place.
Our study suggests that community development efforts to increase safety, to support strong neighborhood associations that build cohesion through public actions and social events, and to strengthen neighborhood social capital are needed to address the local SDH. Meso-level applied sociologists are well-trained to lead place-improving programs that will improve the local SDH and contribute to better health outcomes.
Conclusion
Krumeich and Meershoek (2014) discussed five interrelated contexts of the SDH: superordinate, global, domestic [national], community, and household. While macro- and policy-oriented sociologists must continue to research and advocate for change at the first three levels, the latter two contexts are the focal areas of applied and clinical sociologists.
A substantial research literature has been amassed over the past four decades on the national- and international-level SDH. However, relatively few studies have been done at subnational levels. To overcome this shortage of information, researchers should improve on our survey methods and conduct more area-based studies that focus specifically on the SDH. As more community-level studies are completed, patterns of similar findings can be used to guide more effective, evidence-based strategies to address the SDH in small areas.
Practicing sociologists do not have to wait until the literature on local SDHs accumulates to be more effective in their efforts to improve health. It might be useful for clinical sociologists to focus on micro-level programs to identify individuals and household members who are socially isolated, and to work with them to expand and strengthen their social network and to increase the number and frequency of their social activities.
However, health outcomes for individuals depend not just on their personal characteristics and actions but also on aspects of their social environment. Therefore, “collective and not just individual interventions become salient” (Smith and Christakis 2008:420). Applied sociologists could take a meso-level approach and focus on improving safety and strengthening social capital within neighborhoods as a means to improving health.
In 2015, the Association of American Medical Colleges added a new lengthy social science section to the Medical College Admissions Test (Dembosky 2015). Better training on social environmental and social psychological factors that affect health should improve medical practices. However, we sociologists also need to deepen our understanding of the local SDH and improve our clinical and applied practices to help individuals make adjustments in their social lives and to strengthen communities, which should lead to better health outcomes.
Related Resources
The World Health Organization has descriptions of its international goals and programs, analyses of case studies from several countries, and training manuals related to macro-level social determinants of health on its website: http://www.who.int/social_determinants/en/.
The social determinants of health is one of the major topic areas of the U.S. Department of Health and Human Services’ Healthy People 2020 Program. Of the five key domains within the social determinants of health area, two are most closely related to the work of applied and clinical sociologists: social and community context, and neighborhood and built environment. https://www.healthypeople.gov/2020/topics-objectives/topic/social-determinants-health/interventions-resources.
The National League of Cities is working to create healthier communities, especially for kids. The organization’s “resources–general” tab has information on community commons and community gardens programs. It also contains a Roadmap for Healthier General Plans that includes tips for improving the social and physical environment of communities. http://www.healthycommunitieshealthyfuture.org/learn-the-facts/social-determinants-of-health/.
The Springfield-Greene County Health Department participated in this research. The Department’s Community Health Advocates program utilizes frontline public health workers who are trusted members of their community to bridge gaps and reduce barriers to better health. Advocates build individual and community capacity by increasing health knowledge and self-sufficiency through a range of activities such as outreach, education, social support, and advocacy. https://www.springfieldmo.gov/3062/Community-Health-Advocate.
Footnotes
Appendix
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by a grant from the Springfield-Greene County Health Department.