
Abstract
The purpose of this study is to examine (a) the association between cancer diagnosis and psychological distress and (b) the extent to which this association is moderated by perceptions of neighborhood social cohesion. Data are drawn from the 2013 wave of the National Health Interview Survey (NHIS), a nationally representative survey on broad health topics. We employ ordinary least squares (OLS) regression to examine the links between cancer, neighborhood cohesion, and distress. Findings reveal no statistically significant difference in psychological distress between women with breast and cervical cancer. However, neighborhood social cohesion does moderate the effect of cancer on distress. While perceptions of neighborhood cohesion do not affect levels of psychological distress among women with breast cancer, perceived connectedness with neighbors translates into significantly lower levels of mental distress among women diagnosed with cervical cancer.
Introduction
Extensive research documents the psychological health consequences of where we live (Galea et al. 2007; Hill and Maimon 2013). A bulk of this inquiry focuses on distress associated with undesirable neighborhood characteristics, including neighborhood structural disadvantage and signs of neighborhood physical and social disorderliness, such as dilapidated buildings, vandalism, violence, noise, and pollution (Cohen-Cline et al. 2018; Galea et al. 2007; Mair, Diez Roux, and Galea 2008; Richardson et al. 2015). What remains relatively underassessed is the extent to which positive features of a neighborhood impact levels of psychological distress (Diez Roux and Mair 2010). In this study, we assume this task by examining the extent to which neighborhood social cohesion—a positive neighborhood characteristic—moderates the association between cancer—a chronic stressor—and psychological distress.
Cancer and Psychological Distress
Cancer as a chronic disease is enormously stressful as it often is accompanied by feelings of fatigue and uncertainty and fears of relapse and mortality (Brown and de Graaf 2013; Hodgkinson et al. 2007; Waldrop, O’Connor, and Trabold 2011). As such, despite the headways in cancer research and treatments, those suffering from it often report feelings of depression, anxiety, and anger (Bernad, Zysnarska, and Adamek 2010; Culver et al. 2002). Adverse psychological reactions to the often unexpected and life-threatening chronic stressors, such as cancer, are attenuated by social support (Applebaum et al. 2014; Dunkel-Schetter 1984). For instance, both quality of support and size of social network are linked with reduced distress and improved longevity among cancer patients (Lehto et al. 2018; Nausheen et al. 2009; Pinquart and Duberstein 2010). When grappling with the enormous personal, financial, and psychological burden of cancer, individuals often rely on family and friends who become their source of emotional, informational, and/or instrumental support (Lehto et al. 2018). While we know that informal support provided by family and friends alleviates distress among cancer patients (Nausheen et al. 2009), what is surprising is the underassessment of the role played by those outside of one’s immediate social network. In this study, we look at the extent to which psychological distress reported by cancer patients is conditioned by perceptions of connectedness with neighbors or neighborhood social cohesion.
Why Neighborhood Social Cohesion Matters?
Neighborhood social cohesion generally is considered as the perception of trust, connectedness, and camaraderie among residents of a particular neighborhood (McNeill, Kreuter, and Subramanian 2006; Sampson 2003). In a way, neighborhood social cohesion can be one of the many forms of social support. Those who live in close proximity to us, our neighbors, are just as likely as our family and friends to become a source of emotional, informational, or/and instrumental support (Robinette et al. 2013). Perceived connectedness with neighbors may translate into good health by reducing susceptibility to the day-to-day stressors and mitigating the otherwise noxious effects of stress on health (Robinette et al. 2013). Neighbors, like family members, can act as agents of social control by encouraging individuals to shun risky health habits and engage in behaviors that promote good health (Zhang et al. 2017), including problem-focused coping.
Several existing studies find associations between neighborhood cohesion and a variety of health outcomes, including depression, self-rated health, cardiovascular health, disability, and even mortality (Ahern and Galea 2011; Bjornstrom, Ralston, and Kuhl 2013; Cramm and Nieboer 2013; Kim, Hawes, and Smith 2014; Murayama, Fujiwara, and Kawachi 2012). Supportive neighbors may minimize distress by providing health-related information or/and facilitating access to health clinics for the purposes of prevention, treatment, and rehabilitation (Kim and Kawachi 2017; Ryvicker, Gallo, and Fahs 2012). Depending on the degree of closeness, neighbors may also become a source of instrumental or tangible support by providing help with child/elder care, housekeeping, and transportation (Cramm, Van Dijk, and Nieboer 2013). Put simply, a strong sense of connectedness with those who live in close proximity may translate into both emotional relief and practical help needed to cope with serious chronic stressors, such as cancer (Yamasaki, Geist-Martin, and Sharf 2016). Whether or not the perception of neighborhood connectedness or cohesion moderates the link between cancer and psychological distress remains to be tested empirically.
Cancer Type—Breast Versus Cervical Cancer
As the most frequently diagnosed cancer and the second leading cause of death among women, breast cancer affects about one in eight women in the United States (American Cancer Society 2017). Following breast, lung, and colorectal cancer, the fourth most common cancer found in women across the globe is cervical cancer affecting over one million women worldwide. The demographics of breast and cervical cancers differ in that women with cervical cancer are more likely to be younger at diagnosis, lower socioeconomic status (SES), and Hispanic or African American (Newmann and Garner 2005).
Beyond demographics, several studies demonstrate that there are significant differences between women with breast cancer and gynecological cancers concerning unmet informational and supportive care needs (Beaver and Booth 2007; Faller et al. 2017; Faller et al. 2019). In addition, a study by Awadalla and colleagues (2007) finds that there is a significant disparity in physical and psychological health, as well as overall quality of life, between patients with breast cancer and other gynecological cancers, such as cervical cancer. To date, very few studies have compared breast cancer to cervical cancer, specifically Awadalla et al. (2007), Greimel et al. (2002), Marlow, Waller, and Wardle (2010), and Vigod et al. (2011). When included in analyses compared to breast cancer, some studies use gynecological cancers as an umbrella term to include cervical, endometrial, vulvar, or ovarian cancers (Awadalla et al. 2007; Beaver and Booth 2007; Faller et al. 2017; Faller et al. 2019). A systematic review by Maguire and colleagues (Maguire et al. 2015) concluded that women with cervical cancer, compared to other gynecological cancers, have increased distress and unmet informational needs. This significant disparity, coupled with the stressors of being younger at diagnosis, of lower SES, and a racial minority, lends itself to the need for a direct comparison between individuals with cervical cancer and breast cancer when looking at the relationships between cancer, neighborhood cohesion, and mental distress.
Methods
For this study, we use cross-sectional data from the 2013 National Health Interview Survey (NHIS) collected by the National Center for Health Statistics, which is a part of the Center for Disease Control and Prevention (CDC). These data are collected annually since 1957 and includes multilevel samples (household, family, person, sample adult, and sample child). The NHIS focuses on observing health behaviors and health statuses of individuals who are civilians who are not institutionalized within the United States.
The 2013 NHIS collected data from 41,335 households with 104,520 individuals in 42,321 families. For the purposes of this project, we merged the household, family, person, and sample adult levels to obtain access to a variety of indicators of SES and neighborhood characteristics. Our main independent, moderating, and dependent variables were taken from the adult-level sample, which includes a random adult (18 years and older) from each household (n = 34,557). However, our analyses only include the cases that identified as having a previous breast or cervical cancer diagnosis (n = 775). For the 2013 NHIS data, the response rate was 61.2% for the adult sample. Individuals who identified as black, Hispanic, or Asian and aged 65 years or older were oversampled to provide a more accurate sample of those populations. The NHIS includes sample weights to adjust for the oversampling of these populations.
Dependent Variable
The variables we use to create the distress variable are all items taken from the abridged version of the Kessler Psychological Distress Scale (K6) (Kessler et al. 2003). The K6 is commonly used in research as a global measurement of psychological distress and is considered a reliable and valid screening measurement (Keller et al. 2013; Rios, Aiken, and Zautra 2012). The K6 questionnaire includes six questions that ask the participants how often they felt the following emotions in the last 30 days: so sad that nothing could cheer you up, nervous, restless or fidgety, hopelessness, that everything was an effort, or worthlessness. The responses were reverse coded, summed, and averaged on a 5-point scale so that a higher score on the K6 indicates higher levels of psychological distress: none of the time (a), a little of the time (b), some of the time (c), most of the time (d), and all of the time (e). The Cronbach’s alpha score for the scale in this study is 0.87.
Independent Variable
The main independent variable, cancer type, has two categories for the analysis: breast cancer (0) and cervical cancer (1). In the NHIS questionnaire, participants were asked, “Have you ever been told by a doctor or other health professional that you had cancer or a malignancy of any kind?” For the participants that responded, “Yes,” they were then asked to indicate what type of cancer it was by selecting an option from a broad list. As majority of breast cancer cases deal with women and because cervical cancer only concerns women, the breast cancer cases of men (n = 9) were eliminated from the analyses which results in a total of 575 women with breast cancer. For cervical cancer, there were a total of 200 women.
Moderating Variable
In order to operationalize perceived neighborhood social cohesion, we created a scale from four items measuring perceptions neighborhood social cohesion. The NHIS asked participants or how much they disagreed or agreed with the following four statements: (a) “People in this neighborhood help each other out”; (b) “There are people I can count on in this neighborhood”; (c) “People in this neighborhood can be trusted”; and (d) “This is a close-knit neighborhood.” Responses were reverse coded, summed, and averaged on a 4-point scale so that high values reflect high neighborhood social cohesion, while low values indicate low cohesion (1 = Definitely disagree, 2 = Somewhat disagree, 3 = Somewhat agree, 4 = Definitely agree). These same items have been used to measure neighborhood social cohesion in previous literature (Rios et al. 2012; Sampson, Raudenbush, and Earls 1997), with Cronbach’s alpha for the scale in this study being 0.89.
In addition, when we incorporate perceptions of neighborhoods social cohesion in Models 2 and 3, we include two control variables for neighborhood characteristics. First, we measure housing status, indicating whether a person is renting/has another arrangement (0) or owns their own home (1) because of the significant effect that owning a house has on perceptions of neighborhoods cohesion and psychological distress (Cairney and Boyle 2004; Ellaway, Macintyre, and Kearns 2001). We also indicate length of time at residence, which is correlated with neighborhood social cohesion and psychological distress (Austin and Baba 1990; Schulz et al. 2006). Length of time at residence has five categories: (a) “Less than 1 year”; (b) “1–3 years” (c) “4–10 years”; (d) “11–20 years”; and (e) “More than 20 years.”
Control Variables
We control for a variety of sociodemographic characteristics in our analyses. We measure race-ethnicity, indicating whether a person identifies as white (0) or non-white (1) because of the differences between whites and non-whites for perceptions of social cohesion (Echeverría et al. 2008) and psychological distress (D. R. Williams, Neighbors, and Jackson 2003). We include a measure of marital status that indicates if the respondent was not married/not living with their partner (0) or married/living with their partner (1) because marriage and cohabitation, as a form of informal support, can impact perceptions of neighborhood social cohesion (Wen, Hawkley, and Cacioppo 2006) and psychological distress (K. Williams, Frech, and Carlson 2010). We control for age (measured continuously in years), which is associated with perceptions of neighborhood social cohesion (Diez Roux and Mair 2010) and psychological distress (Mirowsky and Ross 2010). In addition, we control for age of onset of the cancer diagnosis. This allows us to address the difference in age of onset for women with breast cancer compared to women with cervical cancer (American Cancer Society 2017). Next, health status can influence an individual’s mental health (Mirowsky and Ross 2010). We include the respondent’s reported health status, which ranges from poor health (1) to excellent health (5). Finally, we also include measures of SES, including income (“$0–$34,999” (1), “$35,000–$74,999” (2), “$75,000–$99,999” (3), and “$100,000 and over” (4)), a continuous measure of education (ranges from 0–21), and whether a person is employed (a) as being employed full-time, with high income and education contributing to being more integrated in the neighborhood and perceiving your neighborhood as close-knit (Adams and Serpe 2000; Dassopoulos and Monnat 2011) and also experiencing less distress (Culver et al. 2002; Epping-Jordan et al. 1999).
Analytical Strategy
For this study, we first calculated summary statistics using means and standard deviations for the total sample, which includes all merged levels (Table 1). The observations differ based on the level at which the variable was measured. We then compared the means (or proportions) and standard deviations using t-tests and proportion tests for women with a previous diagnosis of breast cancer or cervical cancer for the dependent variable and independent variables (Table 1). Next, shown in Table 2, we used ordinary least squares (OLS) regression to investigate the effect of a specific cancer diagnosis on psychological distress. Model 1 shows the effect of cancer diagnosis on psychological distress while including demographic and SES variables. Model 2 assesses if controlling for neighborhood social cohesion and neighborhood characteristics impacts the effect of a cancer diagnosis on psychological distress. Model 3 includes the interaction term of a cancer diagnosis and perceptions of neighborhood social cohesion while controlling for sociodemographic and neighborhood characteristics. The interaction term will illustrate if the effect of a cancer diagnosis on psychological distress is moderated by perceptions of neighborhood social cohesion. Regression coefficients for Model 3 are shown in Table 2. All analyses were weighted and were completed using STATA 13. This study was reviewed and approved by Kent State University’s Institutional Review Board.
Unweighted Descriptive Statistics.
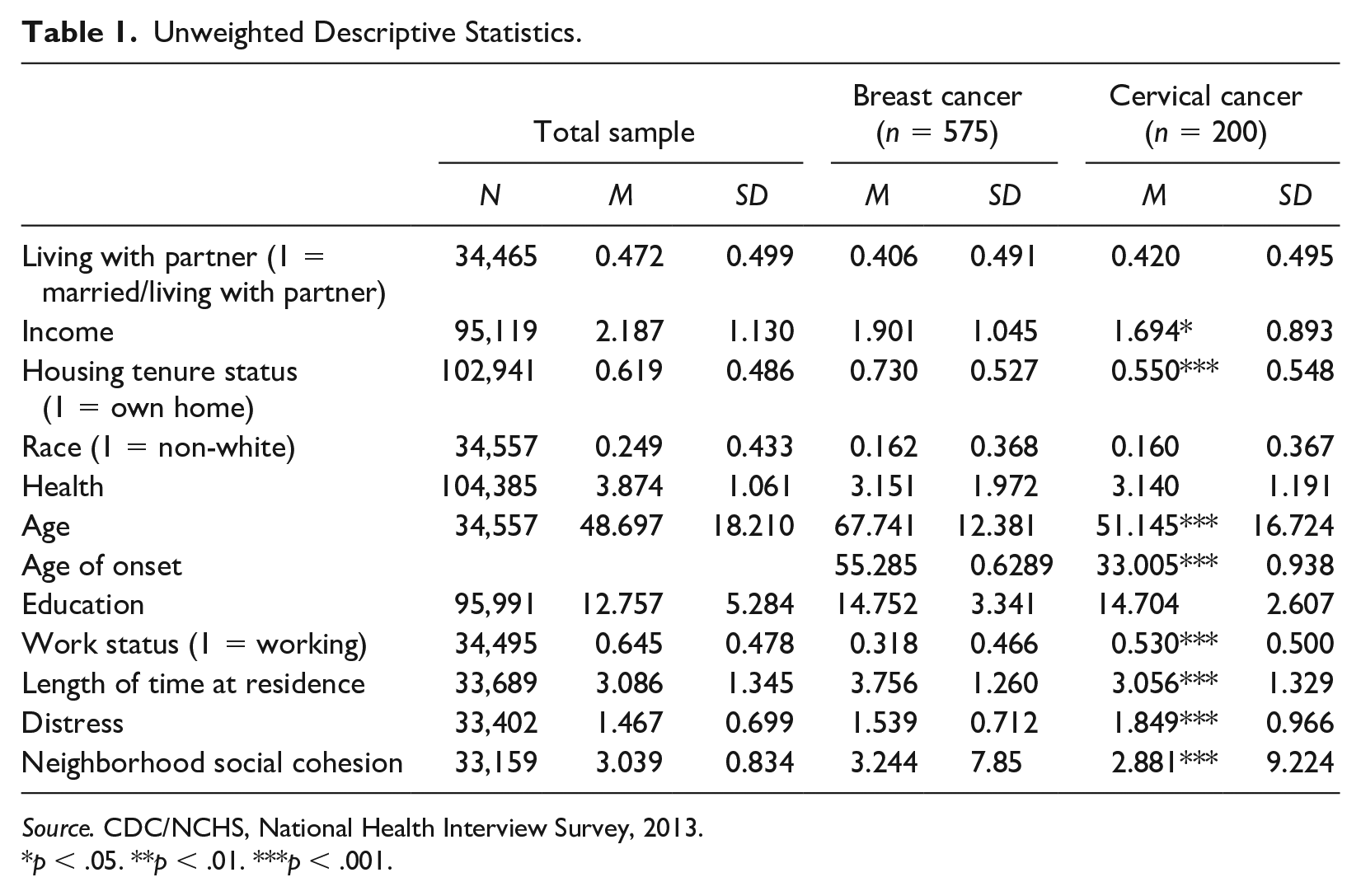
Source. CDC/NCHS, National Health Interview Survey, 2013.
p < .05. **p < .01. ***p < .001.
Ordinary Least Squares Regression Results. a
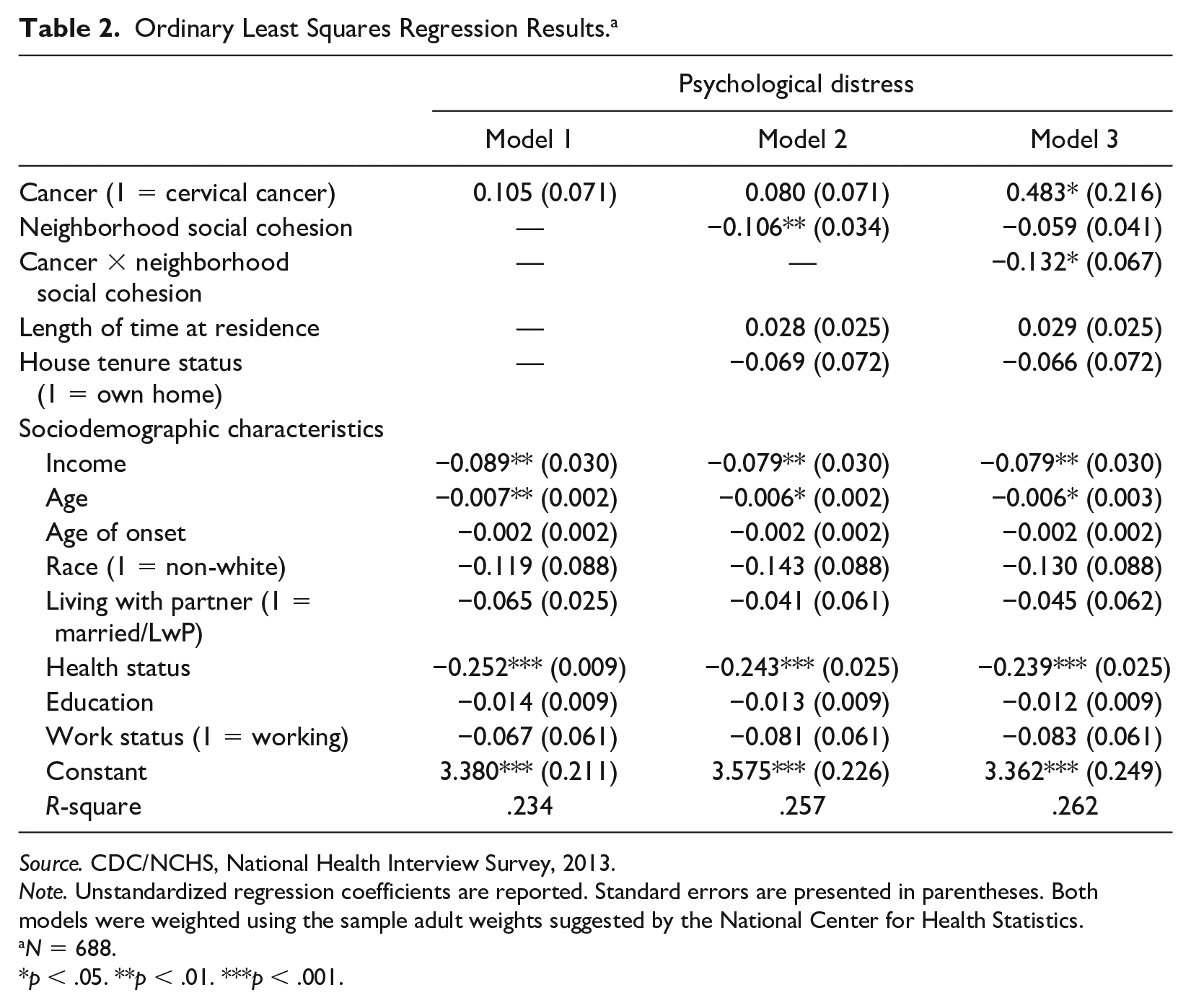
Source. CDC/NCHS, National Health Interview Survey, 2013.
Note. Unstandardized regression coefficients are reported. Standard errors are presented in parentheses. Both models were weighted using the sample adult weights suggested by the National Center for Health Statistics.
N = 688.
p < .05. **p < .01. ***p < .001.
Results
Bivariate Analyses
Table 1 shows the total sample with the mean and standard deviations of all variables in the study. Within the overall sample, the majority of people indicated that their race is white, are not married or living with a partner, have a job, and own a home. In addition, the individuals in this sample are on average about 49 years old, have an income within the range of $35,000 to $75,000, report very good health, have completed about 13 years of education, and have lived at their residence with the range of 4 to 10 years.
Based on t-tests (for continuous measures) and proportion tests (for categorical measures), women with a cervical or breast cancer diagnosis are less likely to be married or living with a partner, have lower income, higher education, be older in age, and not as likely to be working compared to the overall sample of the data. There was no statistically significant difference between the two cancer diagnoses across race, health status, education, and whether they cohabit with a partner or not. However, women with a previous breast cancer diagnosis were more likely than women with cervical cancer to have a higher family income (1.9 versus 1.6, p < .05), own a home (.73 versus .55, p < .001), be older currently (67.74 versus 51.14, p < .001), be older at diagnosis (55.28 versus 33.00, p < .001), not be working (.32 versus .53, p < .001), live longer at their residence (3.75 versus 3.05, p < .001), have higher perceptions of social cohesion (3.24 versus 2.88, p < .001), and have lower psychological distress (1.53 versus 1.84, p < .001). In addition, the pattern of women with breast cancer being older can lead to an understanding that they are less likely to be working due to retirement. Prior to running the OLS regressions, we additionally explored the correlations among all variables in the analyses. Almost all variables are significantly correlated with each other. We assessed multicollinearity with the variance inflation factor and found that none of the variables are highly correlated enough to cause problems in the analyses.
Relationship between Cancer Diagnosis and Psychological Distress
When controlling for demographic characteristics such as income, age, age at onset, race, living with a partner/marital status, health status, education, and work status, the effect of a cancer diagnosis on psychological distress is not statistically significant as seen in Table 2. Looking further at Model 1, the coefficients of income, age, and health status are statistically significant indicating that an increase in each is associated with a decrease in distress.
In the second column in Table 2, we present the unstandardized regression coefficients for Model 2, which controls for neighborhood social cohesion, length of time at residence, and housing tenure status. After controlling for these three variables, the coefficient for cancer decreased and is statistically nonsignificant. Within this model, neighborhood social cohesion, income, age, and health status are statistically significant. A similar trend can be seen for income, age, and health status as shown in Model 1. More notably, as individuals perceive their neighborhoods to be more cohesive, their distress decreases significantly. Although the R2 changed minimally from Models 1 to 2 (.234 to .257), this change was significant, meaning that adding the neighborhood variables significantly add to the explained variance, F (3, 675) = 4.18, p < .01.
Model 3 shows the unstandardized regression coefficients for the independent variables, the controls, and the interaction term for cancer and neighborhood social cohesion. Based on the significance of the interaction term, the relationship between cancer diagnosis and psychological distress varies based on the degree of neighborhood social cohesion. For women with cervical cancer, each one-unit increase in neighborhood social cohesion is correlated with a .191 unit decrease in psychological distress (b = −.059 to .132, p < .05). Compared to women with breast cancer, women with cervical cancer report .483 units increase in psychological distress when all other variables are kept constant. This finding suggests that neighborhood social support moderates the relationship between cancer diagnosis and distress. In highly cohesive neighborhoods, women with cervical cancer experience an associated psychological benefit while women with breast cancer do not. Similar to Models 1 and 2, the variables income, age, and health status are statistically significant. After performing an F-test to compare models, we find that the R2 change from Models 2 to 3 is significant after adding the interaction term, F (1, 674) = 3.90, p < .05. A visual representation of the interaction is shown in Figure 1. This figure illustrates that women with cervical cancer show an association of decreased psychological distress with higher neighborhood social cohesion. In contrast, psychological distress for breast cancer does not depend on different levels of neighborhood social cohesion.
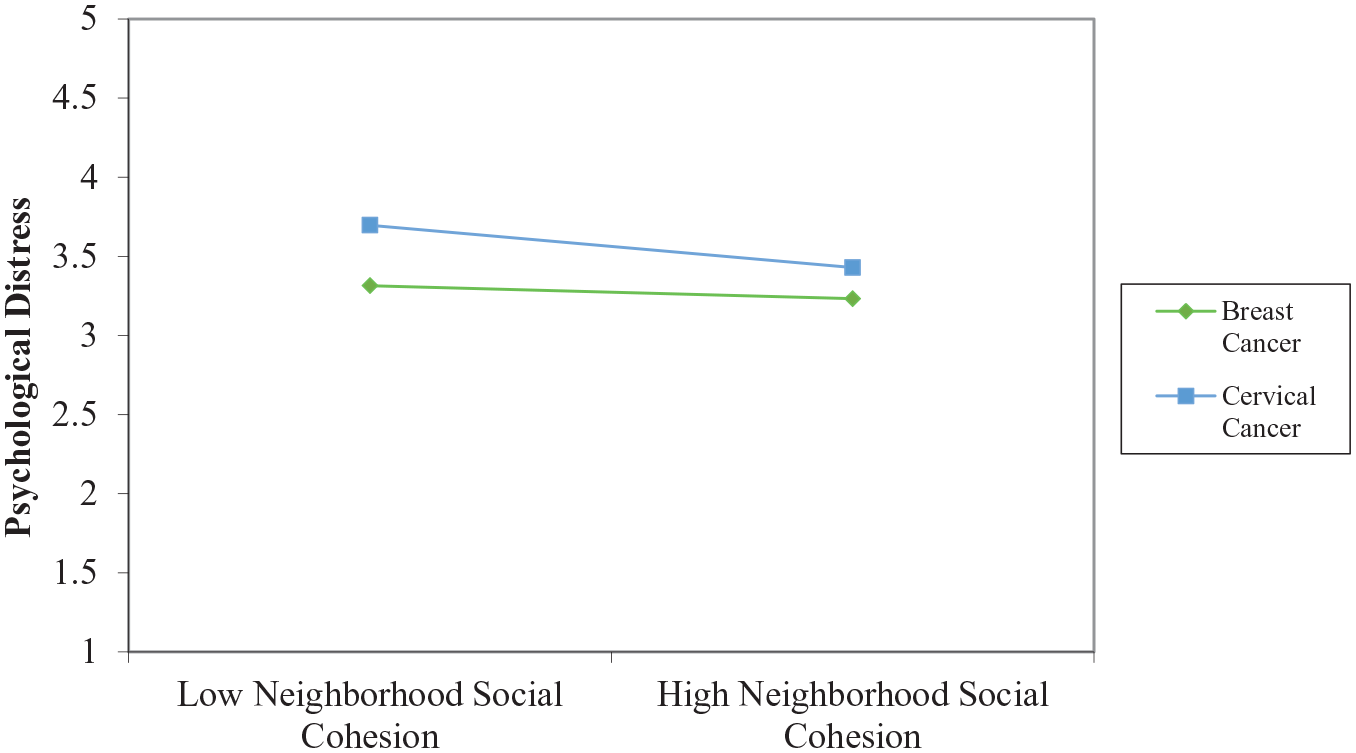
Psychological distress: interaction between cancer diagnosis and perceptions of neighborhood social cohesion.
Discussion
We use data from the 2013 NHIS to examine (a) if there is an association between cancer diagnosis and psychological distress and (b) the degree to which this association is moderated by neighborhood social cohesion. Adjusting for the sociodemographic factors, our results do not reveal any statistically significant difference in levels of distress between women with breast and cervical cancer. However, a statistically significant difference in distress reported between those with breast and cervical cancer does emerge when we add neighborhood-level variables, including neighborhood cohesion, housing tenure, and time lived in the neighborhood.
In order to understand the association between cancer and distress, we focused our analyses on two cancer diagnoses that affect millions of women worldwide: breast and cervical cancers. Prior research has brought to light that there are significant demographic differences between these two cancers, particularly age of onset of disease and race and ethnicity (Newmann and Garner 2005). When controlling for these characteristics, along with other characteristics that could potentially influence distress (e.g., income and education), our findings reveal that there is no statistically significant difference between the two cancer types and psychological distress. This is surprising but could be explained by the fact that cancer, in general, is distressing—regardless of the type of cancer (Bell 2014). There are coping mechanisms that may alleviate the effect of a stressor on mental health (Thoits 2011); however, these coping mechanisms, such as social support, themselves may be unequally distributed (Thoits 2010), thus creating disparities for groups of individuals.
The most important purpose of this study was to assess the extent to which the relationship between cancer and psychological distress is conditioned by perceptions of neighborhood social cohesion. And, as expected, we do find the link between cancer and depressive symptoms to be moderated by one’s perception of trust and connectedness among neighbors. Perceiving more connectedness with those living in close proximity is associated with a decrease in mental distress among those living with cancer. Important to highlight, however, is the differential impact of the perceived neighborhood social cohesion on the distress levels between women with breast versus cervical cancer. Specifically, when perceiving their neighborhood as unsupportive, women with cervical cancer have significantly higher levels of psychological distress than women with breast cancer. This suggests that when women with cervical cancer perceive lower levels of neighborhood cohesion, they typically exhibit greater levels of distress. Put otherwise, when perceiving their neighborhoods as more cohesive, women with cervical cancer express lower levels of psychological distress.
In contrast, women with breast cancer reported lower levels of psychological distress regardless of their perceived level of neighborhood cohesion. That is, neither higher or nor lower perceptions of neighborhood connectedness conditioned the depressive symptomology among women with breast cancer. Even when reporting perceptions of lower neighborhood cohesion, women with breast cancer showed lower levels of psychological distress than women with cervical cancer. This finding suggests that the support within a community does not benefit women with breast cancer to the same extent that it does women with cervical cancer. Consistent with previous literature, this might be due to the fact that women with breast cancer primarily rely on informal support from family and friends (Bell 2014; Dunkel-Schetter 1984; Else-Quest and Jackson 2014), likely because they feel more at ease reaching out for support. It is possible that due to high awareness of this cancer (Bell 2014), women with breast cancer may perceive their neighborhoods to be close-knit, but the support from family and friends is what is most consequential for mental health.
Limitations and Future Directions
Although our study has several strengths, it is not without limitations. First, the NHIS data precluded the detailed measurement of cancer as an experience and a stressor. A complete understanding of this stressor would include a whole host of questions that map for us the trajectory of this health condition as opposed to the mere diagnosis of it. While our study finds neighborhood cohesion to condition the association between cancer and distress, whether or not this association remains despite the stage of cancer remains to be determined. We do not know because NHIS does not contain such data, which sources of support matter most at what stage of the cancer experience. Do the varying levels of support matter differentially based on the stage of cancer? Is any particular source of support more or less consequential as the disease progresses? It is possible that supportive neighbors matter in the early stage or during remission whereas immediate social networks (i.e., partner, adult child, and a sibling) become more consequential during the end stage of this health condition. Stage of cancer also reflects the progression of the illness, which may shape both systems of support and mental health. For example, on one hand, a prolonged exposure to an illness may alter the interactional nature of social relationships and result in greater mental distress. On the other hand, individuals who live with a chronic condition may find effective ways of coping with stressors associated with that condition compared to their counterparts who experience it as a more sudden or short-lived illness transition. As such, future studies that are able to consider the stage of cancer within a longitudinal framework would be in a stronger position to discern the extent to which the evolution of cancer shapes both, the perceptions of support and mental health repercussions of this illness.
Second, in addition to a more thorough measurement of cancer, future studies would benefit from a more exhaustive profile of respondents’ neighborhood. So, while our study is focused on neighborhood social cohesion and we do control for duration in a neighborhood and home ownership status (rent vs. own), we are unable to assess neighborhood structural advantages (availability of parks, health stores, and formal support groups), spatial dimensions of neighborhoods (e.g., distance between immediate neighborhood and cancer clinic, place of employment, and grocery store) and neighborhood SES. Future studies would be in a much better position to make stronger inferences on the linkage between cancer, neighborhood contexts, and mental distress if they were to include these additional assets of a neighborhood.
Third, the NHIS is an annual, cross-sectional survey, which lacks a longitudinal component that would be critical to understanding the on-going relationship between cancer, neighborhood contexts, and psychological distress. Longitudinal data would lend us a glimpse into both the short and long-term impact of neighborhood cohesion on cancer and psychological health. Last, while NHIS contains reliable and valid measurement of the key variables in this study, such as psychological distress and perceptions of neighborhood social cohesion (Kessler et al. 2003; Sampson et al. 1997), the use of self-reported measurements may mean that responses are biased. For instance, because of the stigma attached to cervical cancer (Else-Quest and Jackson 2014; Newmann and Garner 2005), it may be that women with cervical cancer are underreporting their diagnosis which is likely to cause an underestimation in the relationship among these variables.
Notwithstanding the limitations, the findings from this study highlight the importance of looking beyond one’s family and relatives when examining the mental health implications of cancer. Cancer is a disease that affects not just an individual but their family, which means that families as a whole have to grapple with this physically and emotionally debilitating condition (Woźniak and Izycki 2014). In a situation where both individuals with cancer and their significant others experience distress, the perception of having supportive, trusting relationships with persons outside of one’s immediate social circle may be even more helpful than otherwise expected. Stress researchers argue that the tenaciousness of the stressor–distress relationship is contingent upon individuals’ ability to make use of all of the resources available to them (Pearlin et al. 1981). We argue that neighborhood social cohesion is one such resource.
Findings from our study add to the emerging body of research that demonstrates how residing in cohesive neighborhoods may strengthen an individual’s ability to cope with adverse life circumstances (Cramm et al. 2013; Dawson et al. 2019). Conversely, living in communities that lack trust and solidarity can add to the stress residents already may be experiencing in their everyday lives (Elliott et al. 2014). Given that cancer as a stressor is consistently predictive of distress (Lashbrook et al. 2018), which often then predicts worse mental health outcomes (Brown and de Graaf 2013; Hodgkinson et al. 2007; Waldrop et al. 2011), identifying stress-alleviating factors for cancer patients and survivors remains a matter of crucial public health interest.
This study also underscores the importance of looking separately at breast and cervical cancers as opposed to the more traditional approach of grouping cervical, endometrial, vulvar, and/or ovarian cancers under the single umbrella of gynecological cancers. In general, factors causing cancer range from genetic mutations to a myriad of risky behaviors (Else-Quest and Jackson 2014). While breast cancer may emerge from old age, inherited genetic mutations (e.g., BRCA1 and BRCA2 genes), or risk factors unique to each individual, 99% of cases of cervical cancer are caused by the human papillomavirus (HPV), a sexually transmitted infection (STI) (Albini et al. 2015; American Cancer Society 2017; Dyer 2010). Consequently, cervical cancer carries the stigma of having a disease that is self-induced and avertable (Dyer 2010; Else-Quest and Jackson 2014).
While breast cancer still is stigmatizing, national movements, including Breast Cancer Awareness month and the “Wear Pink” campaign and the personal stories of several high-profile public figures, including actors, sports celebrities, and politicians have raised awareness and reduced the stigma attached to breast cancer (Gulyn and Youssef 2010; Sharf 2001). Increased awareness and visibility, in turn, have proliferated the amount of funding for breast cancer research and availability of advocacy and social support for breast cancer patients (Bell 2014; Else-Quest and Jackson 2014).
Stigmatization of cervical cancer, which stems from contracting a “preventable” cancer whose onset many people attribute to risky sexual behavior, such as unprotected sex and multiple sex partners (Dyer 2010; Kahn et al. 2007; Perrin et al. 2006; Shepherd and Gerend 2014) still remains strong. In fact, the guilt and shame felt by cervical cancer patients has soared since the introduction of vaccines for HPV in 2006 (Dyer 2010). The promotional strategy of HPV vaccinations emphasizes pre-emptive action to eliminate the potential for developing cervical cancer (Dyer 2010). This strategy has shifted the experience of cervical cancer patients from one of internal guilt and shame to one of enacted stigma (Blake et al. 2015).
Perceptions of stigma, which are tied to public discourse related to an illness, may force some to conceal their type of cancer. In their study on cervical cancer, Dyer (2010) found that some women may lie about their cancer type to protect themselves from the stigma of their diagnosis. Stigmatized cancers may also force some to reduce social interactions and activities (Drapeau, Marchand, and Beaulieu-Prevost 2012), limiting the resources and emotional support they may otherwise have had access to within their communities (Dyer 2010). While our data do not offer us the opportunity to control for perceptions of stigma, future studies should consider the extent to which it conditions the associations between cancer type, neighborhood-level support systems, and psychological distress.
Conclusion
Findings from our study contribute to a growing body of research suggesting the powerful mental health impact of where we live and the connections we form with those living in close proximity to us. They make us question the otherwise commonplace assumption that cancer is uniformly distressing to all. Instead, psychological repercussions of even the most dreadful of conditions, such as cancer are conditioned by social resources, such as ties within one’s neighborhood. This study adds to the conversation related to the relevance of social networks and social capital on health. This conversation is especially important as family structures continue to evolve (Seltzer 2019), increasing number of individuals choose to remain childless (Blackstone 2014), and friends, neighbors, and co-workers gain prominence in terms of a social network (Smith and Christakis 2008). More research, however, is needed not only to replicate our findings with more robust longitudinal data but also to determine some of the logical arguments—nevertheless speculations—we are proposing in our work. Understanding the grip of our surroundings on chronic and often fatal health conditions, such as cancer carries important implications for informing public policy and community level interventions.
Footnotes
Acknowledgements
The authors would like to thank Dr. Richard Adams, Dr. Kristen Marcussen, and Dr. Janette Dill who have read earlier versions of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.