
Abstract
In this study, we explored whether embryonic stem cell-derived mesenchymal stem cell (ES-MSC) cellular spheroids in combination with a closed chamber system could be used to create scaffold-free cartilage and endochondral graft tissues. ES-MSC cellular spheroids were cultured in chondrogenic medium for 3–4 days and seeded into a customizable Net Mold chamber system (NCS) and cultured in chondrogenic medium for an additional 18 days to fuse and form a single tissue construct. To assess potential for cartilage repair, cellular spheroids were matured in the NCS for only 7 days before implantation into ex vivo human cartilage defects. To engineer osteochondral tissues, cellular spheroids were initially cultured in chondrogenic medium for 14 days, seeded into one well of the NSC, and cultured together in osteogenic medium for 21 days. For the chondrogenic phase, cellular spheroids were initially cultured in chondrogenic medium for 14 days before seeding in an NCS chamber, adjacent to the osteogenic spheroids. The combined osteogenic and chondrogenic constructs were cultured in serum-free medium for an additional 3 weeks. Cellular spheroids cultured in the NCS developed into neocartilage tissues expressing cartilage-associated genes (COL2A1, ACAN, and COMP) and stained positive for cartilage matrix molecules (glycosaminoglycan and collagen type II). The cartilage-like constructs that were implanted into cartilage defects created in ex vivo osteoarthritic (OA) tissue resulted in repair tissue with an elastic modulus of 46 ± 6 kPa that was histologically integrated with the explant tissues. Spheroids cultured in osteogenic medium produced tissues that were positive for von Kossa stain and for osteopontin immunostaining. Pre-differentiation in chondrogenic and osteogenic medium before placing in the NCS resulted in fused cartilage and bone-like constructs with regional production of chondrogenic and mineralized matrix (Alizarin Red S, von Kossa, and osteopontin positive). Spheroids in stacked NCS chambers produced osteochondral neotissues up to 2 mm in thickness. Our results indicate the potential for cellular spheroids, from a clinically relevant ES-MSC source, to generate scaffold-free chondrogenic or osteochondrogenic graft tissues.
Impact Statement
This study demonstrates the possibility to use a clinically relevant embryonic stem cell-derived mesenchymal stem cell (ES-MSC) source to make cellular spheroids to fabricate scaffold-free cartilage and bone-like constructs, using a culture chamber system. Neocartilage tissues expressing cartilage-associated genes and matrix molecules, when implanted into ex vivo cartilage defects, integrated with existing tissue and showed promising repair potential. An osteochondral ossification differentiation approach generated scaffold-free osteochondral tissues with regional production of chondrogenic and mineralized matrix. Combining clinically relevant ES-MSC, cellular spheroids, specific culture environments within a chamber system offers a promising approach for cartilage and osteochondral repair.
Introduction
Tissue engineering of cartilage and bone typically involves three main components: the cells, a scaffold system, and the medium containing factors that sustain viability and promote neotissue formation. A wide variety of natural or synthetic scaffolds have been tested for cartilage, bone, and osteochondral engineering.1,2 While scaffolds can be useful for cell attachment, to provide differentiation cues, and for mechanical support, 3 there are several limitations. These include inadequate cellular seeding and distribution, poor integration of scaffold with host tissues, challenges with biodegradation of scaffolds, and issues with biocompatibility leading to cytotoxicity and inflammation.4,5 Scaffold-free approaches have been developed to circumvent these issues. The main challenges for generating scaffold-free approaches are obtaining high cell numbers and achieving mechanical properties for in vivo implantation.6,7
Generating scaffold-free engineered cartilage and bone-like tissues typically involves some form of high-density cell culture to emulate the cell-to-cell contact and communication observed during cell condensation and cartilage differentiation in the developing limb bud 8 (also termed “developmental engineering” 9 ). Examples include the formation of layered cellular sheets,10–12 high-density cell seeding onto permeable membranes13–17 or within a closed permeable chamber, and the use of cellular microspheroids as building blocks that are placed in close proximity to induce fusion and form cartilage18–23 and bone neotissues.24–32 Using cellular micro spheroids for bone-like tissue formation involves the induction of chondrogenesis and subsequent exposure to pro-osteogenic factors. This leads to cellular hypertrophy and the expression of osteogenic markers.33–35
Cellular microspheroids are self-assembled cellular aggregates of living microtissues with newly synthesized extracellular matrix (ECM) and have several advantages. Cellular microspheroids can be assembled into higher order structures. This approach of “bottom-up” tissue engineering leverages the inherent capacity of microspheroid building blocks to differentiate and fuse into larger tissue constructs. 36 Cells within microspheroids experience biological, biochemical, and biophysical conditions that more closely reflect those in developing native tissue.5,37–40 This combination of cells and ECM more closely mimics the physiological connections that enhance cell survival, direct differentiation,41–44 secrete growth factors, 45 and withstand mechanical loading.46,47 Clinical repair of cartilage lesions using autologous chondrocyte microspheroids led to better outcomes compared with microfracture.48–50 However, because of the limitations of sourcing autologous chondrocytes, mesenchymal and pluripotent stem cells have been proposed for generating scaffold-free cartilage and bone tissues.
We previously bioprinted cellular microspheroids on microneedles to fabricate neocartilage tissues from embryonic stem cell-derived mesenchymal stem cell (ES-MSC) using a robotic arm bioprinter coupled with computer vision. 21 The printed microspheroids fused rapidly to form neocartilage and successfully repaired tissue defects in ex vivo human osteoarthritic cartilage explants as well as osteochondral defects in vivo in rabbits. However, the robotic arm bioprinter was expensive and required microspheroids of precise size. To overcome these limitations, we investigated a simpler chamber system to produce scaffold-free cartilage and osteochondral tissues (Net Mold, Tissue by Net, Co. Kitamoto, Saitama, Japan). This system is less expensive and consists of thin stainless steel plates and thin wires to contain premade cellular spheroids within a defined space. We have used this system with a range of spheroid sizes and “fused” cartilage and bone neotissues into a single integrated construct.
Here, we show the potential to generate cartilage and bone tissues using a cell source that is compatible with clinical translation. We demonstrate the feasibility of producing scaffold-free neocartilage and osteochondral constructs by assembling cellular microspheroids in high density within an adjustable chamber system to promote spheroid fusion. We also show the potential for regeneration and repair of cartilage defects in ex vivo human osteoarthritic cartilage.
Methods
Cell source and cultivation
Human ES-MSCs were derived as previously described. 51 Briefly, xeno-free-derived ESC: HADC-100 ESC 52 was placed into suspension culture with serum-free medium to form small cell clusters and then subjected an ALK5 inhibitor (SB525334, 10 mM; Selleckchem, Houston, TX) for 5 days before plating onto fibronectin coated flasks in the presence of fibroblast growth factor basic (FGF) (20 ng/mL). The emergent cells displayed a stem cell-like surface marker profile (>85% positive for CD73, CD90, and CD105 and <2% positive for CD34 and CD45) and produced neocartilage with ECM composed of glycosaminoglycan (GAG) and collagen type II.
Net Mold chamber system
We utilized a cellular spheroid building block system (Net Mold, Tissue by Net, Co. Kitamoto, Saitama, Japan), which consists of a reusable cage of stainless steel. The Net Mold culture system (NCS) consists of thin stainless steel plates and thin wires with specific spacing that are stacked in alternate layers to create square or rectangular wells or subchambers of various sizes (see Fig. 1). A base plate/grid consists of multiple wires that are spaced closely together (∼0.1 mm) to confine the seeded cellular spheroids within a given chamber. The sizes of inner chambers can be varied (from 2 × 2 mm to 14 × 14 mm) with adjustable heights (from 1 to 3 mm, in 100 µm increments). A plate with closely spaced wires is placed on top to enclose the seeded cellular spheroids and promote fusion of the cellular spheroids into a larger tissue (Figs. 2 and 3).
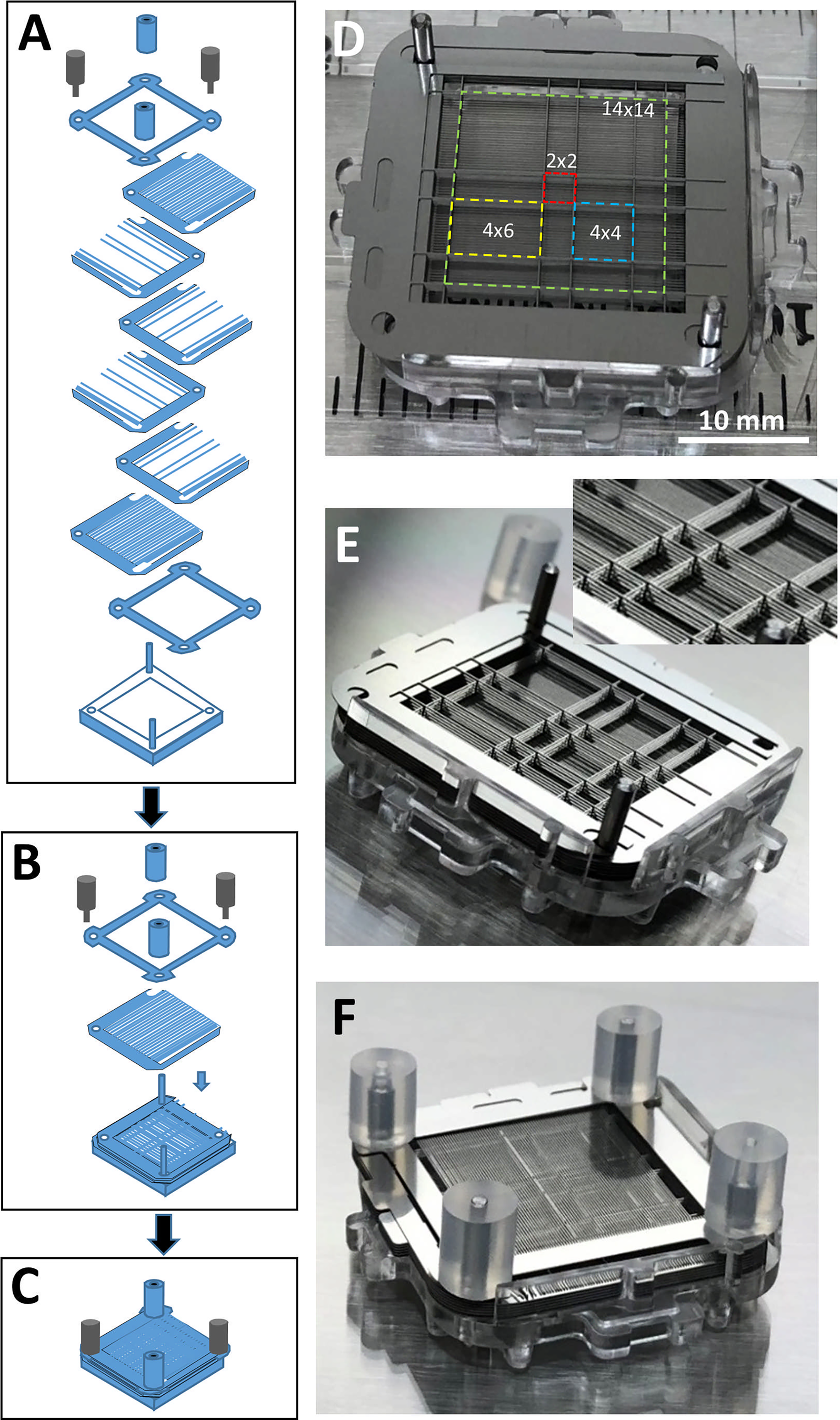
Overview of the NCS.
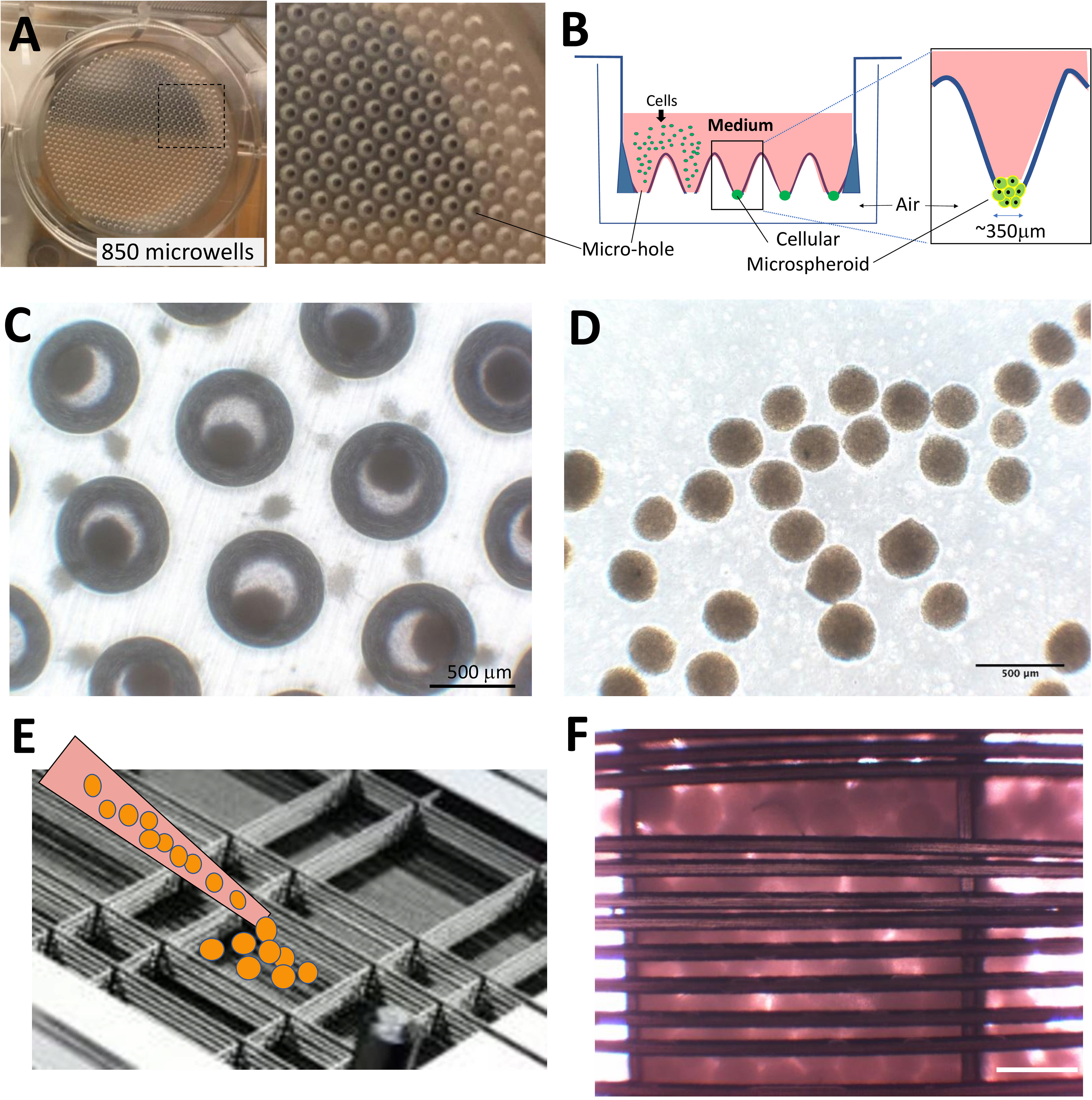
Production of ES-MSC microspheroids and seeding into NCS for neotissue formation.
Cellular spheroid production
Three methods were used to produce cellular spheroids: (1) hanging drop cultures, (2) ultra-low adhesion plates, and (3) pellet cultures using micro centrifuge tubes.
Hanging drop cultures
Each hanging drop plate insert has 850 microholes with an approximate diameter of 350 µm (see Fig. 2). Cells suspended in medium settle by gravity and accumulate at the base of each microhole suspended by surface tension. Each well of a 6-well hanging drop plate insert (Kuraray Elplasia “MPc350” Kuraray Co. Ltd. Tokyo, Japan) contained 4 × 106 single cells in 4 mL of serum-free chondrogenic medium. The serum-free chondrogenic medium was made with Dulbecco’s modified eagle medium (DMEM) (Mediatech Inc., Manassas, VA), 1× supplemented with Insulin - Transferrin - Selenium (ITS); Sigma-Aldrich, St. Louis, MO, 100 nM dexamethasone (Sigma), 1.25 mg/mL human serum albumin (Bayer, Leverkusen, Germany), 100 µM ascorbic acid 2-phospahate (Sigma), 1% penicillin/streptomycin/gentamicin (PSG, Gibco, Carlsbad, CA), and supplemented with 10 ng/mL transforming growth factor beta 3 (TGFβ3, PeproTech, Rocky Hill, NJ). After 4–6 days in culture, the insert was removed and placed into another 6-well plate that was prefilled with 1–2 mL of phosphate buffered saline (PBS) to release the microspheroids. Microspheroids were then collected by pipette (P1000) and transferred to the NCS as detailed later.
Ultra-low adhesion cultures
Ultra-low cluster and ultra-low attachment 96-well plates with round-bottom wells (Sigma-Aldrich, St. Louis, MO) were seeded with 10,000 cells per well and suspended in 100 µL of serum-free chondrogenic medium. The cellular microspheroids were cultured for a minimum of 3 days before being pooled into a single microcentrifuge tube and seeding via pipette into the NCS.
Pellet cultures
High-density pellets of human ES-MSC cells ranging from 0.2 × 106 to 0.5 × 106 were created by centrifuging cells in 0.5 mL of chondrogenic medium at 900 rpm (∼770 g) for 5 min in sterile 1.5 mL centrifuge tubes. The pellets were stable enough to be transferred into the NCS after 3–4 days.
Seeding of chamber system with cellular spheroids for creation of cartilage neotissue
Cellular spheroids (microspheroids or pellets) were seeded into defined wells of the chamber system (see Figs. 1 and 2). The NCS was submerged into 7–8 mL of chondrogenic medium in one well of a 6-well plate and placed on an orbital shaker at 150 rpm (Ohaus Parsippany, NJ) in a carbon dioxide incubator at 37°C. Medium was changed every 3–4 days. After the appropriate duration of culture in chondrogenic medium, the fused tissue was removed after disassembling the NCS (Fig. 3A). Tissue samples were processed for mechanical testing (N = 3), preserved for RNA extraction (N = 4) or histology (N = 3), or for ex vivo implantation (N = 3).
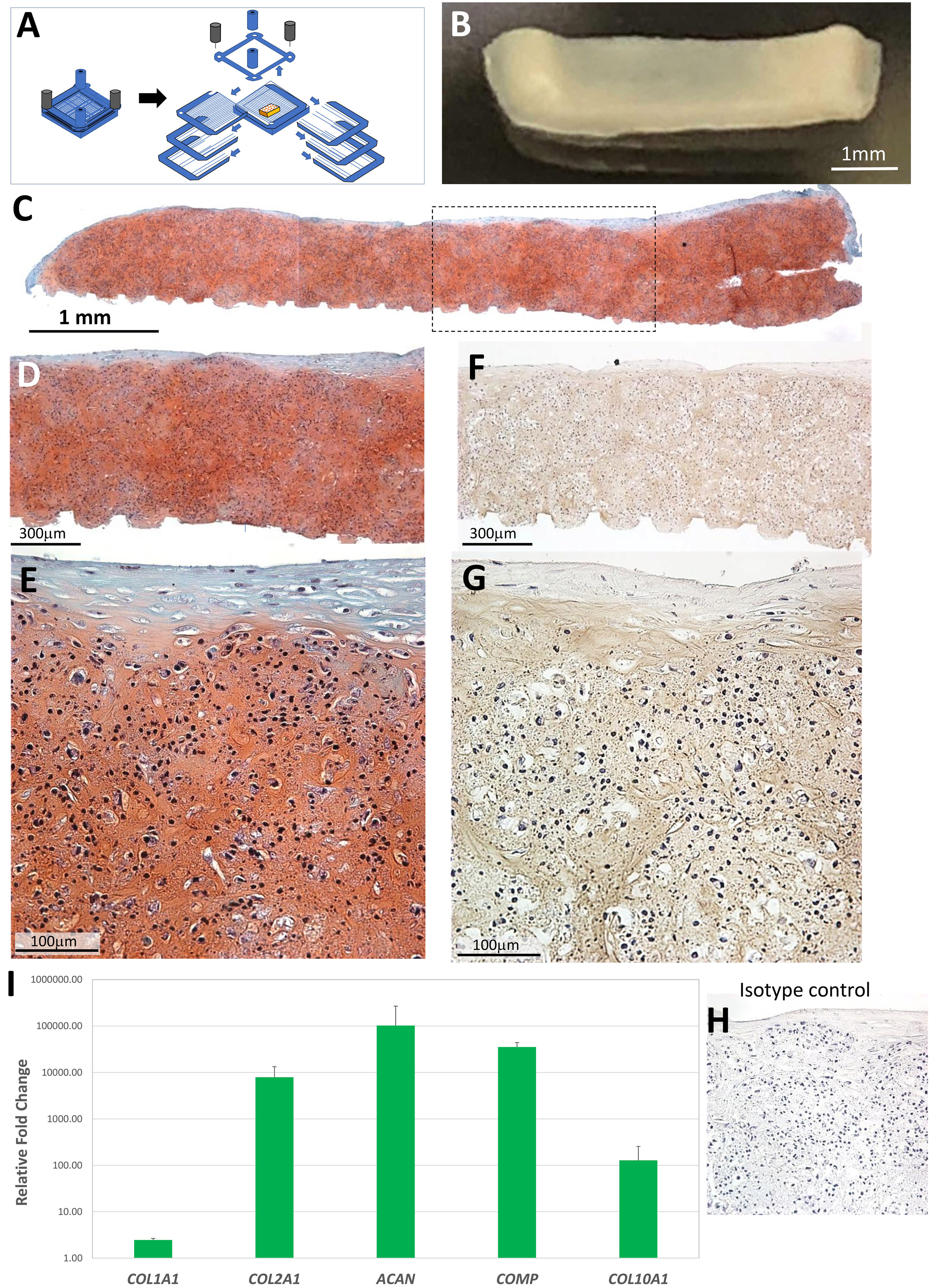
Neocartilage tissue formation using ES-MSC cellular microspheroids seeded into the NCS and cultured in chondrogenic medium over 3 weeks.
Human ex vivo chondral defect model
Osteochondral tissues were acquired from patients undergoing total knee arthroplasty (approved by Scripps Institutional Review Board). Cartilage was removed from the subchondral bone using a scalpel, and sterile dermal punches were used to harvest 6 mm cartilage disks. The tissue explants were cultured in medium consisting of DMEM (Mediatech Inc., Manassas, VA) supplemented with 10% calf serum (Omega Scientific Inc., Tarzana, CA) and 1% PSG (Life Technologies, Carlsbad, CA). A flame-sterilized stainless steel burr was used to make irregular chondral defects, approximately 4 mm2 in area and up to 1 mm deep. Fused microspheroid constructs cultured for 7 days within the NCS were cut to size and implanted into chondral defects. The implanted tissues were cultured in chondrogenic medium for 3 weeks (N = 3).
Mineralized tissue formation
To differentiate the cellular spheroids to a neo-bone-like tissue, an endochondral ossification differentiation approach was adopted.53,54 Microspheroids or micropellets of ES-MSC were cultured in the serum-free chondrogenic medium for 7–14 days and then switched to osteogenic medium (osteoblast differentiation medium, Cell Applications, San Diego, CA) for an additional 14–21 days (N = 4).
Decalcified osteochondral defect model
Osteochondral tissues from donor patients were fixed for 7 days (Z-Fix) and decalcified in TBD-2 (Formic acid; Shandon. ThermoFisher Scientific Inc.) for 10–12 days. Tissues were then washed extensively with sterile PBS for 2–3 weeks.
Histology and immunohistochemistry
Tissues were fixed in Z-Fix (ANATECH, Battle Creek, MI), dehydrated, embedded in paraffin, and sectioned (4–6 µm thick). Safranin O/Fast Green stain was used to detect GAGs. For collagen type I and type II detection, sections were pretreated with pepsin (Digest-All 3; Thermo Fisher Scientific) for 9 min at 37°C in a humid chamber before incubation at 4°C for 12–16 h with either a collagen type I antibody (Ab 34710; Abcam, Cambridge, MA) at 1 mg/mL or a collagen type II antibody (II-II6B3; Hybridoma Bank, University of Iowa) at 2 µg/mL. Rabbit anti-osteopontin (ab8448, Abcam, Cambridge, UK) at 5 mg/mL was used to detect osteopontin without any demasking procedure, and sections incubated at 4°C for 12–16 h. For color development, the ImmPRESS AP-red kit was used for collagen type I, whereas both collagen type II and osteopontin, the ImmPRESS DAB kit, were used (Vector Laboratories, Burlingame, CA). Isotype controls were used to assess nonspecific staining of all immuno-stained targets. Calcium deposits were detected by the von Kossa or the Alizarin Red S stain. Sections for von Kossa stain were incubated for 20 min in a 1% silver nitrate solution in a clear glass Coplin jar that was placed into sunlight. The sections were placed into 5% sodium thiosulfate for 5 min and counterstained with Nuclear Fast Red for 5 min. Sections for Alizarin Red S stain were exposed to a 2% solution (pH 4.1–4.3) for 1–2 min and then dehydrated in acetone.
Quantitative polymerase chain reaction
The RNeasy kit (Qiagen Valencia, CA) was used to extract total RNA. Complementary DNA (cDNA) was made using total RNA as a template according to the manufacturer’s protocols (High Capacity cDNA Reverse Transcription Kit; Applied Biosystems, Foster City, CA). Gene expression of COL1A1, COL2A1, COMP, ACAN, RUNX2, and COL10A1 was measured using prevalidated TaqMan® gene expression reagents (Applied Biosystems) using the Lightcycler 96 (Roche, real-time polymerase chain reaction [PCR] device). The expression levels were normalized to GAPDH using the method as previously reported, 55 and the relative change in gene expression of the neocartilage constructs (N = 4) was compared with the expression levels of ES-MSC in monolayer culture.
Mechanical testing
Indentation testing was performed on constructs (N = 3) either immediately after removal from the NCS or after implanting in ex vivo tissue (N = 3), as described previously.21,56,57 Briefly, an electromagnetic actuator system (SMAC, Carlsbad, CA, USA) was used to first apply a 0.02 N tare load. The peak force generated was then measured after a ramp compression to 150 μm at 50 μm/s. Indentation stiffness was calculated as peak force divided by the indentation depth. The elastic modulus was computed assuming a Poisson’s ratio of 0.5. 56
Statistical analysis
The online BootstRatio application was used to determine significant changes in gene expression between undifferentiated cells in monolayer culture and the neotissues. P values <0.05 were considered significant (http://regstattools.net/br). 58
Experiment
Specific culture conditions required to produce neocartilage and osteochondral tissues
An overview of the culture conditions and times involved in microspheroid formation, the creation of chondral-tissue only, calcified cartilage, and osteochondral tissues is outlined in Figure 4.
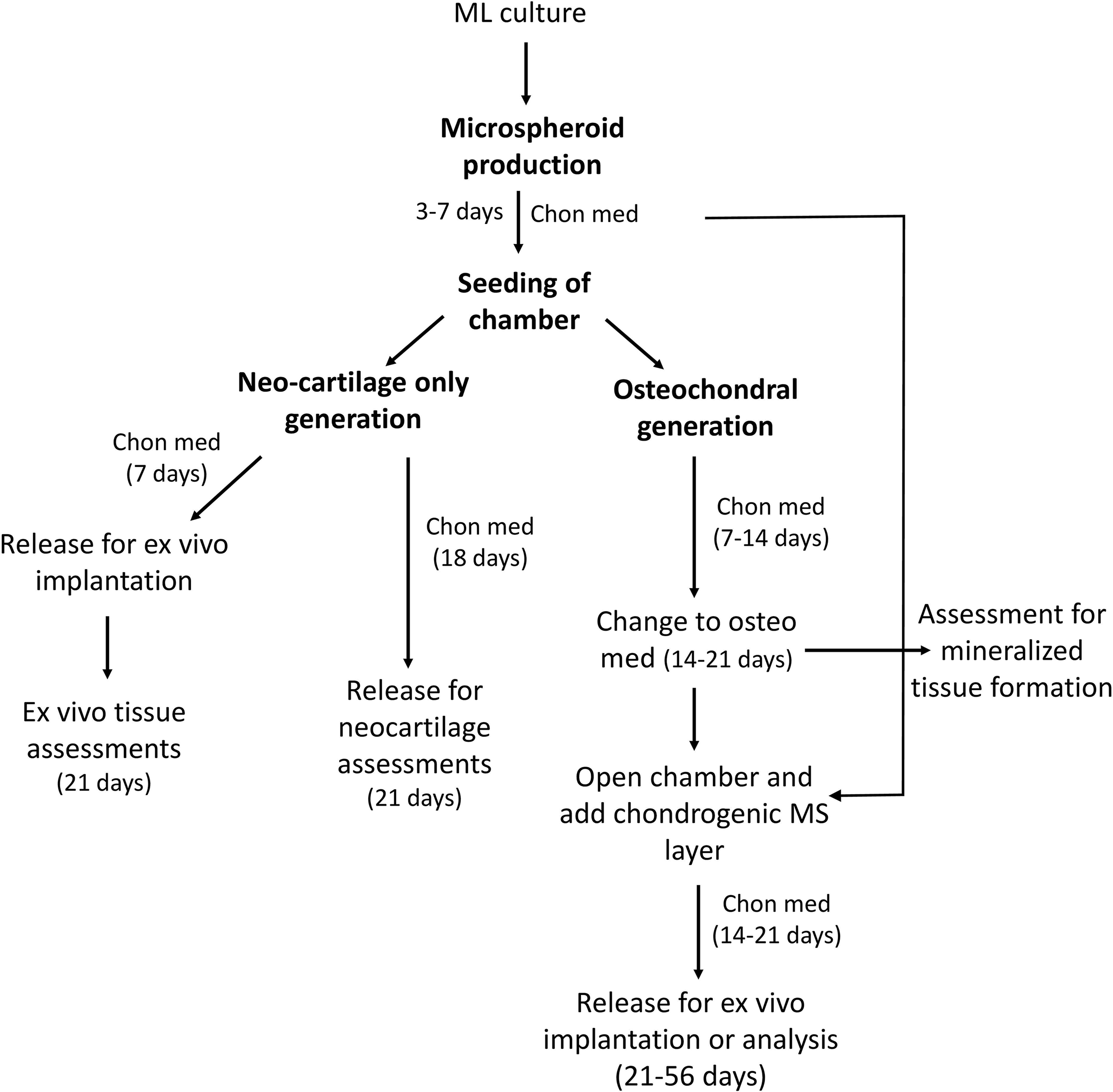
Overview of scaffold-free cartilage and osteochondral tissue fabrication. Key steps including cultures times, medium used, and assessments made are outlined for each type of tissue produced. Chon med, chondrogenic medium; osteo med, osteogenic medium.
ES-MSC microspheroids fuse to produce neocartilage tissues
Hanging drop culture wells seeded with 4 × 106 ES-MSC (approximately 4,700 cells per micro well) generated cellular spheroids averaging 270 ± 18 µm in diameter after 4 days (Fig. 2). The cellular spheroids were transferred into the NCS for 3 weeks of culture in chondrogenic medium. The resulting neotissue stained positive for Safranin O (Fig. 3C–3E) and collagen type II (Fig. 3F, G). Gene expression of COL2A1, ACAN, and COMP increased and COL1A1 expression was low, relative to undifferentiated ES-MSC in monolayer (Fig. 3I; N = 3). COL10A1 expression was detected; however, no mineralized matrix was observed in these constructs with Alizarin Red S or von Kossa stain, which is consistent with our previous study. 51
Ex vivo chondral defect repair with neocartilage
A neocartilage construct (1 mm wide, 4 mm long, and 1 mm high) using ES-MSC spheroids in the NCS was matured for 7 days and cut into four pieces of approximately 2 × 1 mm each. Three of the neocartilage pieces were implanted into surgically created chondral defects made in human osteoarthritic tissue explants. After 3 weeks of culture in chondrogenic medium, the implanted neotissue produced Safranin O and collagen type II positive tissues, with an elastic modulus of 46.3 ± 5.9 KPa, that appeared well integrated with the explant tissue (Fig. 5A). We also noted extensive cell migration into the defects and robust neotissue formation (Fig. 5B).
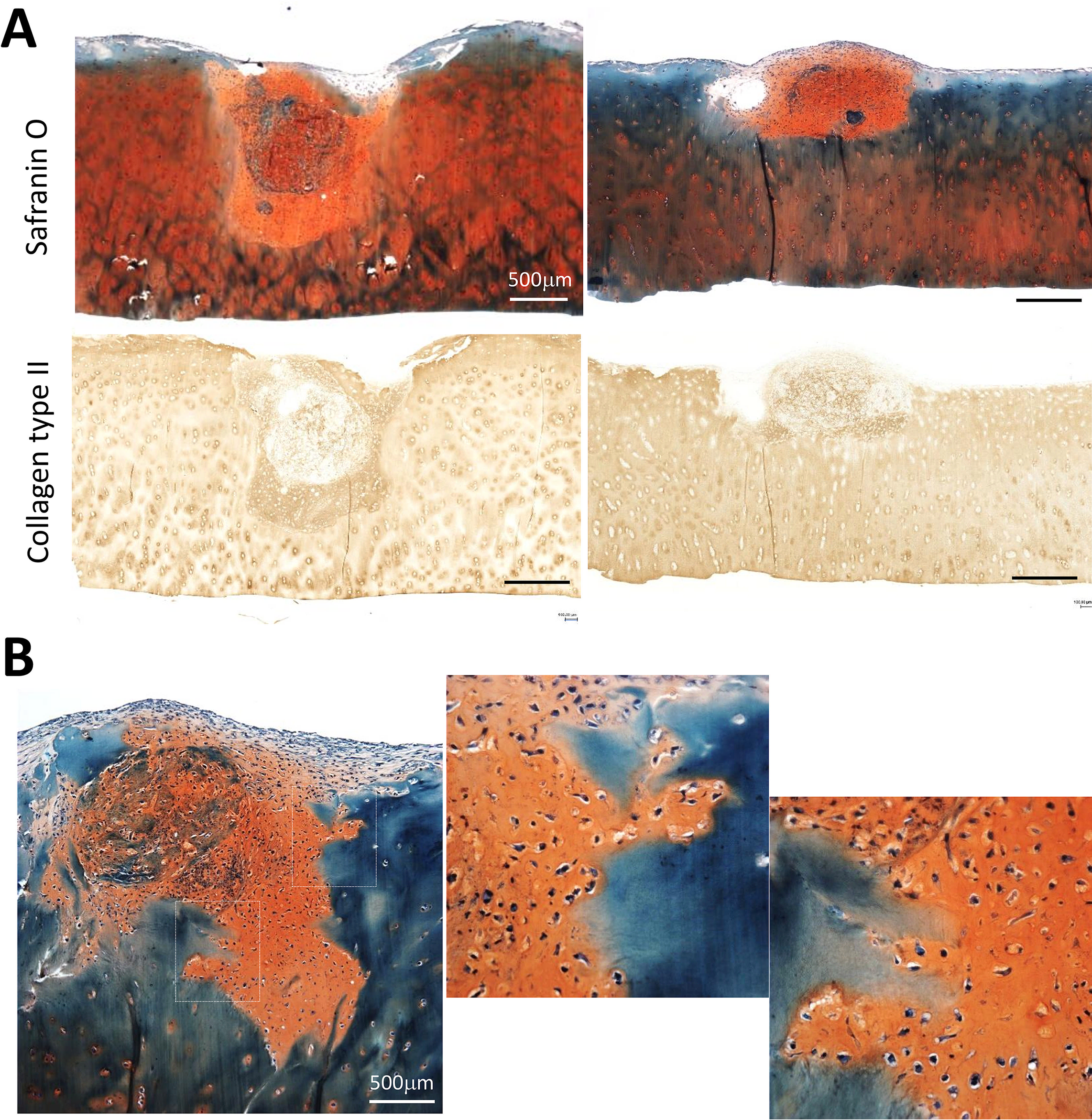
Implanted neocartilage tissue formed in the NCS over 7 days and implanted into OA human cartilage ex vivo defects for 3 weeks.
Chondrogenic priming before osteogenic treatment of microspheroids produces mineralized neo-bone tissues
The process of endochondral ossification in vivo involves the formation of a transient cartilage tissue that progresses to a terminally differentiated hypertrophic phenotype, followed by deposition of a mineralized matrix.53,54 Replicating the stages of endochondral ossification, in vitro has produced bone-like mineralized tissues.9,33,59,60 We adopted a modified approach, using a shorter chondrogenic exposure of 14 days before switching to a pro-osteogenic medium for an additional 21 days. This approach generated Safranin O and collagen type II positive cartilaginous tissues (Fig. 6A, B), with evidence of mineralization by positive von Kossa staining (Fig. 6C) and osteogenic differentiation by positive immunostaining for osteopontin (Fig. 6D). The mineralization was predominately localized in the regions between the fused pellets.
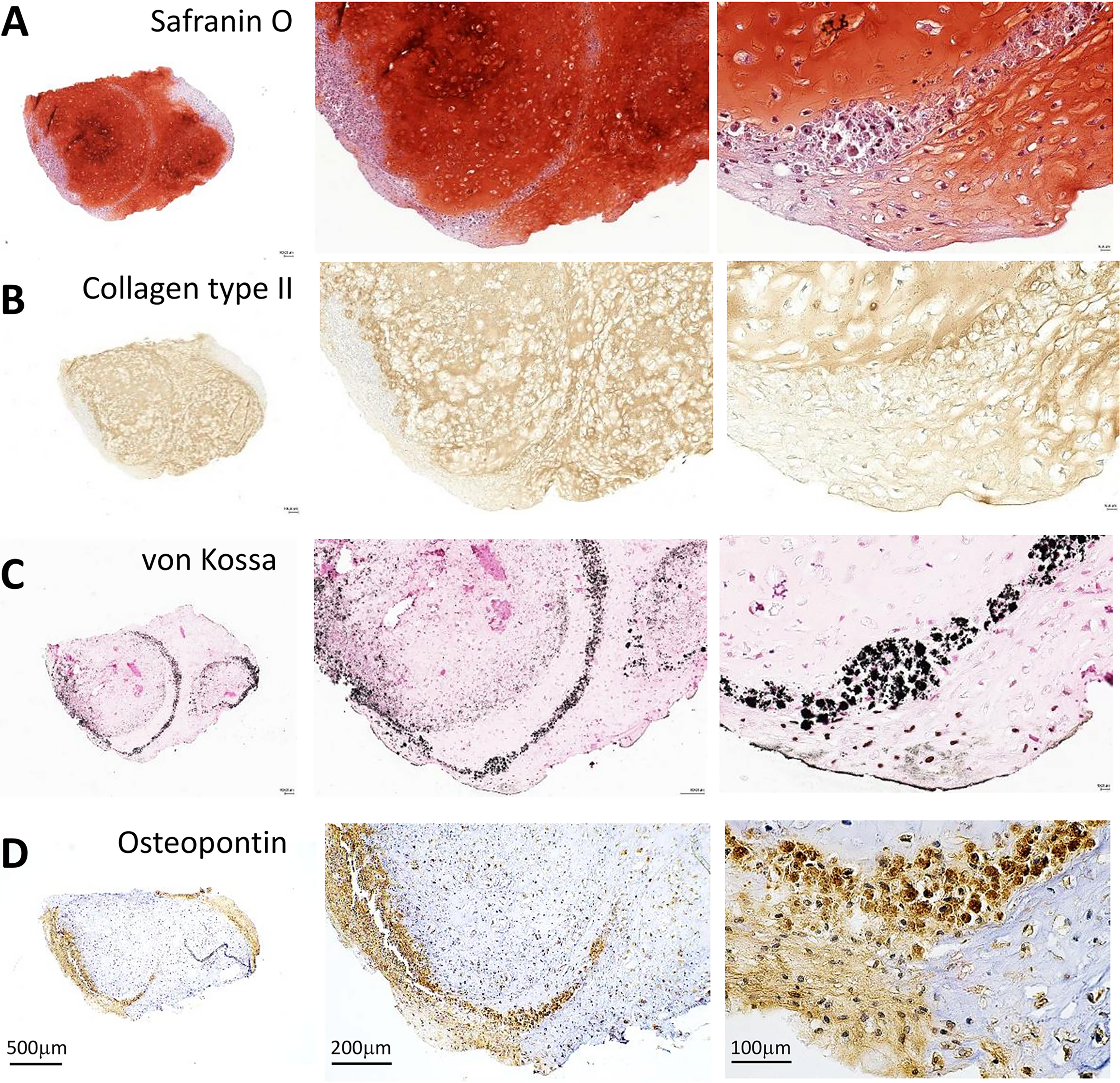
Mineralization of cartilage tissues. ES-MSC was cultured in chondrogenic medium for 2 weeks and then switched to a pro-osteogenic medium for 3 additional weeks. While it is still predominantly cartilage like with
Formation of integrated biphasic cartilage and bone constructs
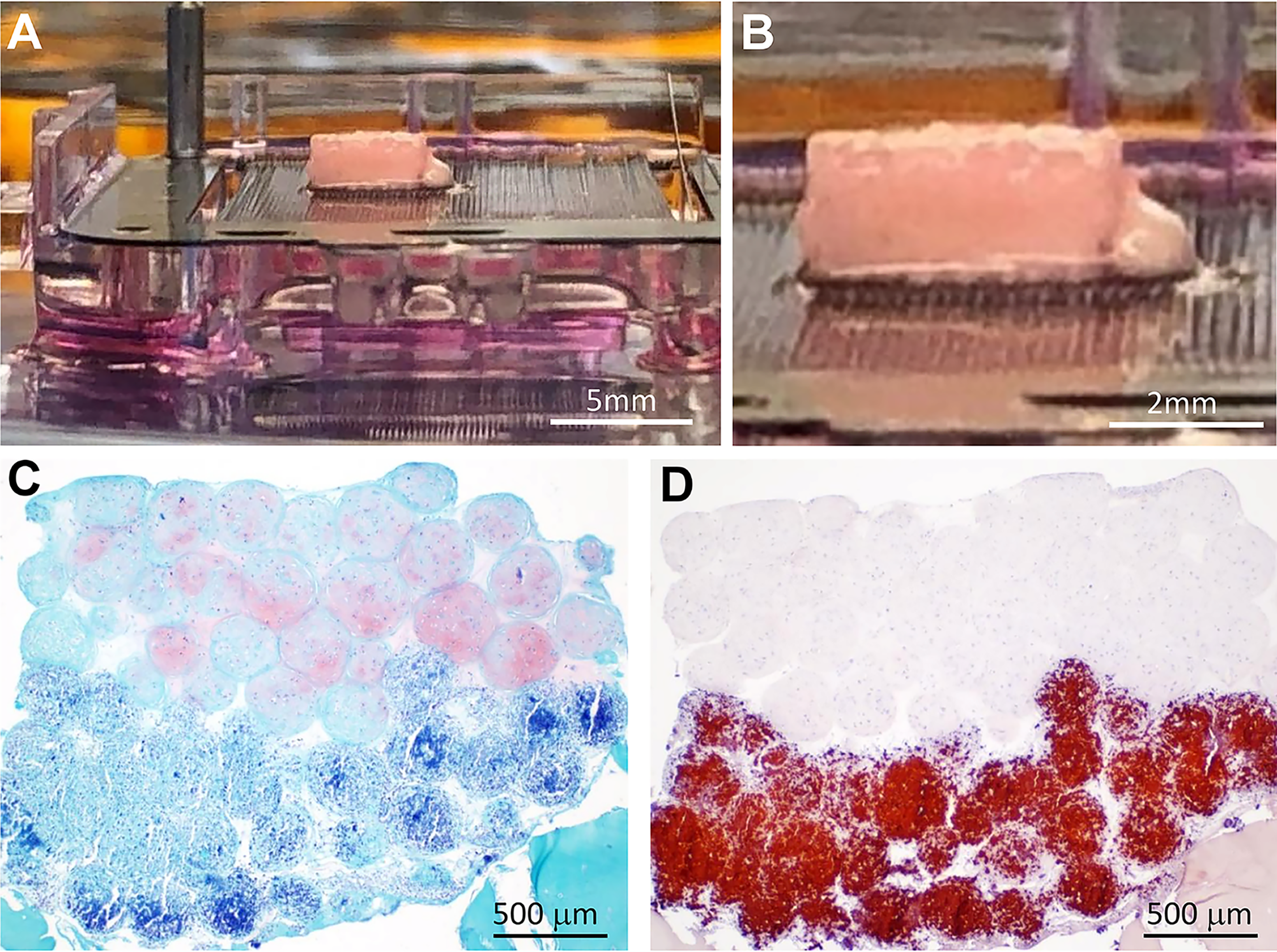
We then sought to produce osteochondral tissues by seeding prechondrogenic and preosteogenic cellular microspheroids in adjacent chambers of the NCS. To scale up tissue production, we made cellular spheroids using high-density pellet culture (0.2 × 106–0.5 × 106 cells per pellet). These pelleted spheroids were precultured in chondrogenic medium for 7 days in single tubes before being added to one well of the chamber system and cultured for another 14 days in chondrogenic medium (21 days). Other spheroids chosen for osteogenic differentiation were cultured in chondrogenic medium for 7–10 days followed by 14 days in osteogenic medium. The NCS chamber containing the preseeded chondrogenic pellets was opened, and the osteo-induced spheroids were seeded in the well adjacent to the chondrogenic spheroids (Fig. 7A). The chamber was placed into serum-free chondrogenic medium without TGFβ or any osteogenic factors, for an additional 14 days. Following the combined culture, a fused construct was formed (Fig. 7B) and was trimmed to be implanted into a decalcified osteochondral explant tissue and cultured in chondrogenic medium for an additional 3 weeks (Fig. 7C and Supplementary Fig. S1). The osteochondral tissue was stained for Safranin O (Fig. 7D) and immunostained for collagens type I (Supplementary Fig. S2) and type II (Fig. 7E) for cartilage-tissue assessment. For detection of hypertrophy and mineralization, sections were processed for von Kossa staining (Fig. 7F and Supplementary Fig. S1) and immunostained for osteopontin (Fig. 7G). The implanted construct was aligned with the cartilage and bone interface and shows the deposition of mineral deposits (von Kossa) in the lower bone region. Closer analysis shows the upper cartilage-like region with well-developed ECM rich in sulfated GAGs (Safranin O; Fig. 7D) and positive for type II collagen (Fig. 7E) without mineral deposition and without hypertrophy (Fig. 7E upper inset). The lower osteogenic region shows morphological evidence of a hypertrophic phenotype (7E lower inset) and mineral deposition with von Kossa (Fig. 7F) and the presence of osteopontin (Fig. 7G), which represents an advanced stage of chondrocyte hypertrophy or an indication of differentiation to an osteoblastic phenotype.61,62 Alizarin Red S also stained the same regions as von Kossa and osteopontin (Supplementary Fig. S2).
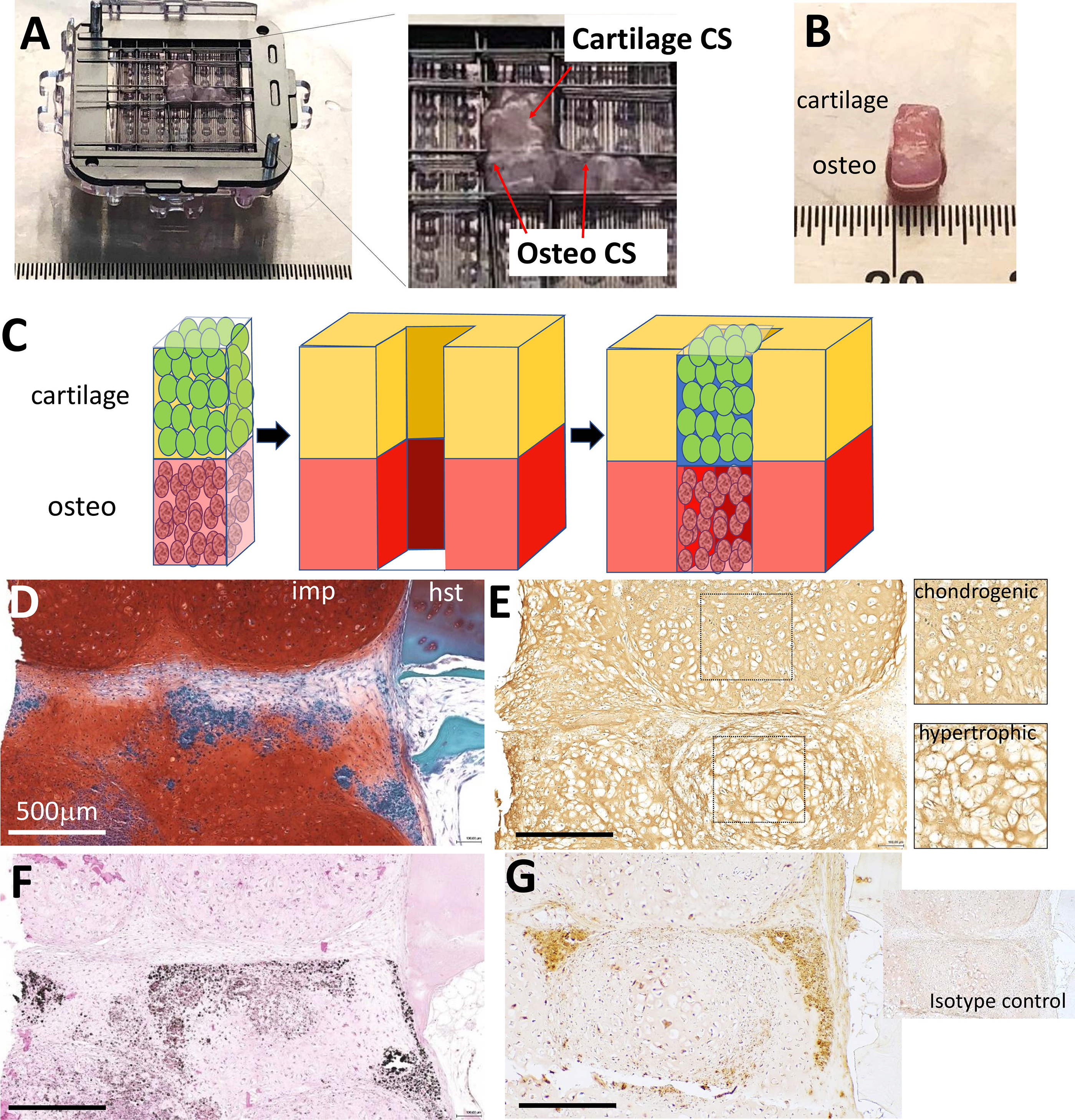
Creation of biphasic osteochondral implant in the NCS and implantation into an ex vivo osteochondral defect.
Microspheroid stacking strategy to produce thicker and more mature osteochondral constructs
Assembling constructs in adjacent wells side-by-side demonstrated proof of concept of producing 1 mm thick biphasic constructs. To fabricate thicker constructs, we stacked spheroids vertically in the NCS chambers (Fig. 8). Larger microspheroids were assembled in ultra-low adherent round bottom 96 well plates as described previously 21 by seeding 10,000 ES-MSC per well. By day 5, the average size of microspheroids was 467.2 ± 14.8 µm. For the bottom layer of the osteochondral construct, we seeded 7-day old chondrogenic precultured microspheroids into a 1 mm high chamber well and cultured these microspheroids for 14 days in osteogenic medium in the chamber (Fig. 8A). A second batch of ES-MSC microspheroids were precultured in chondrogenic medium for 14 days. These chondrogenic microspheroids were seeded on top of the osteogenic microspheroids in a second layer of chamber scaffolding constructed on top of the lower chamber and cultured together in chondrogenic medium with TGFβ3 (10 ng/mL) for an additional 14 days (Fig. 8A–C). The elastic modulus of these constructs (N = 2) averaged 48 KPa. Histology shows a clear demarcation of Safranin O positive layer of microspheroids above a Safranin O negative osteo/bone region (Fig. 8G).
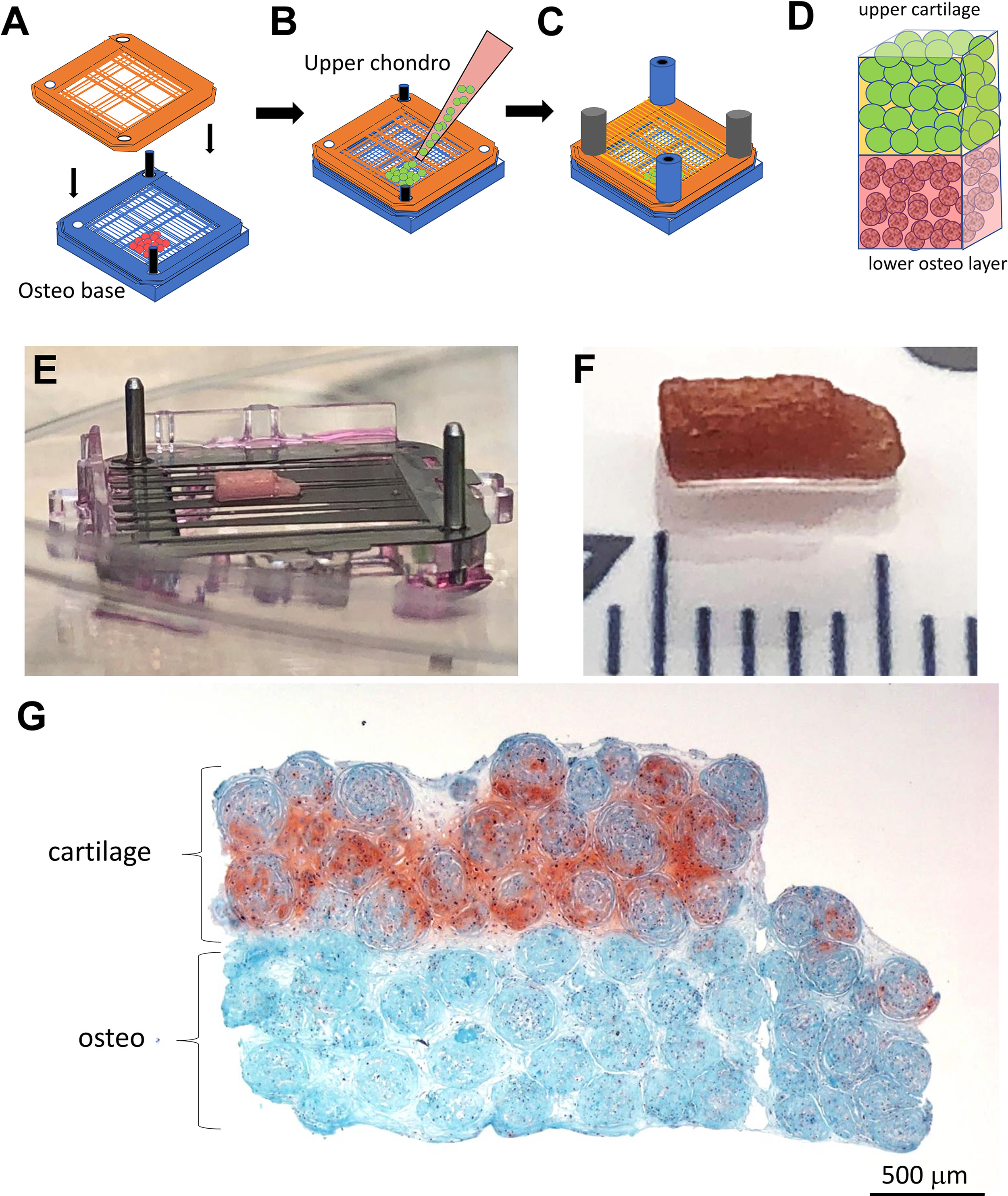
Formation of thicker osteochondral tissue by stacking two NCSs.
To examine longer-term culture, a 28-day-old osteochondral construct (Fig. 9A, B) was implanted into another ex vivo osteochondral explant and cultured for 4 more weeks. The longer-term cultured construct displayed an upper chondrogenic profile (Safranin O positive) without signs of hypertrophy or mineralization (Fig. 9C). However, substantial mineralization in the lower osteo region was observed with alizarin red staining (Fig. 9D).
Longer-term cultured osteochondral construct with enhanced mineralization.
Discussion
We had previously reported on bioprinting cellular microspheroids for in vivo repair of cartilage defects in rabbit femoral condyles. 21 In this study, we show the proof of concept with a clinically relevant source of ES-MSC using a more efficient process (NCS) to fabricate scaffold-free chondral and biphasic osteochondral neotissues. Ex vivo implantation of neotissues showed an evidence of integration with host tissue.
The cellular microspheroid approach has been studied for cartilage tissue engineering using several cell types including chondrocytes, bone marrow-derived MSCs (BM-MSCs), adipose-derived MSC, and human EC-MSC. These cells have been assembled as microspheroids using a variety of methods 63 including pellet culture, 64 prefabricated microchambers of agarose, and various microfluidic devices; 65 hanging drop culture,66,67 random positioning machines, 68 spinner suspension cultures,69,70 and low adherent plates.21,22 Human chondrocyte microspheroids have been used for cartilage repair in phase III trials with better outcomes compared with microfracture.48–50 However, autologous chondrocytes are a less optimal cell source for larger lesions, especially osteochondral lesions, which require substantially more cells. Hence, alternative cell sources with greater proliferative potential, such as stem cells, are more attractive.
The size of microspheroids in these previous studies typically ranged between 100 and 600 µm in diameter. These microspheroids have been assembled on needle arrays21,71,72 or within custom molds22,23,73 to promote fusion into tissue constructs. The “Kenzan” approach uses computer vision to select microspheroids of specific size (500–600 µm) and a robotic arm for precise positioning on a needle array.21,72 The NCS used here does not require such strict restrictions on microspheroid size. Micromass cultures of 10 × 103 cells per unit resulted in better cartilage tissue formation with reduced hypertrophy when compared with larger pellets containing between 2.5 × 105 and 5 ×105 cells, 64 presumably due to a combination of improved cell to cell interactions, improved nutrient exchange, and reduced core necrosis.
Griffith et al. 74 cultured pellets of 0.3 × 106 MSC (derived from HUES7 ES cells) under hypoxic conditions for 4 weeks to produce scaffold-free tissues which integrated with human cartilage explants under coculture. Our neotissues only required 7 days in the NCS and integrated well into ex vivo human osteoarthritic tissue implants. Several studies have explored the utility of using microspheroid-based tissue regeneration using BM-MSC, adipose-derived stem cells, or synovial-derived MSC in combination with cylindrical Teflon molds or the Kenzan microneedle approach to create tissue grafts for implantation and repair of in vivo osteochondral defects in lapine, porcine, and equine models.22,23,72,73,75 We and others have used pluripotent stem cells to engineer cartilage.21,76
Collectively, these studies consistently demonstrated the ability of these constructs to promote cartilage regeneration, with varying degrees of success in repairing the articular cartilage. However, common limitations across these studies included fibrocartilage formation, issues with graft–host integration, and inadequate subchondral bone regeneration, even after extended periods (up to 12 months).
Despite the potential of MSC microspheroids for cartilage repair, these studies have also highlighted the need for improved strategies to enhance subchondral bone regeneration. Most clinically, symptomatic articular lesions involve subchondral bone. The cartilage thickness in animal models, especially in rats and rabbits, is only 0.1–0.3 mm,77,78 requiring deeper osteochondral defects to assess outcomes of grafting. Others have commonly fabricated osteochondral tissues by engineering cartilage on top of osteogenic scaffolds.79–83 We produced scaffold-free osteochondral tissues to potentially address these limitations and to accelerate repair of osteochondral defects.
To form mineralized bone-like tissue in vitro, investigators have emulated the two natural osteogenic differentiation processes, namely intramembranous or endochondral bone formation. 84 Intramembranous bone formation involves direct differentiation of progenitor cells to osteoblasts that deposit mineralized matrix. 85 MSC microspheroids when cultured in osteogenic medium for 3–4 weeks result in an increased expression of osteogenic genes.29–32 Endochondral ossification involves an initial phase of chondrogenic differentiation, which then progresses to chondrocyte hypertrophy and the production of mineralized matrix and, in vivo, the infiltration of blood vessels.53,54 Investigators have used this approach in vitro by initially forming a cartilage template for 1–4 weeks before providing pro-osteogenic conditions to induce mineralization.53,54 Because the subchondral bone in the knee is formed via the endochondral ossification process, we explored this process to produce calcified cartilaginous tissue using a scaffold-free microspheroid building block approach.
After finding evidence of chondrogenic and osteogenic tissues in microspheroid building blocks, we decided to combine these tissues to form osteochondral tissue integrated into one construct. Breathwaite et al. 20 printed microspheroids of BM-MSC using the Kenzan needle array system and cultured in chondrogenic only, osteogenic only, or mixed chondro-osteogenic conditions. However, no condition was shown to be able to maintain a stable cartilage-like phenotype when combined with osteogenic graft tissues. In our study, we show the potential to produce osteochondral tissues with distinct chondral and osteogenic compartments fused into a single construct. We accomplished this fusion by preconditioning microspheroids for cartilage or mineralized tissues before combining the spheroids in a single culture system to promote fusion and continued neotissue formation. While chondrocytes differentiated from BM-MSC tend to become hypertrophic, chondrocytes differentiated from our ES-MSC cell line did not.
The scaffold-free microspheroid approach has several weaknesses. The high cell density requires large cell numbers, which can be an issue for autologous cell sources. We therefore elected to use a clinically relevant pluripotent cell source capable of generating cell banks of adequate size. Allogeneic cells have potential for inducing immune response. We have implanted these cells in vivo in rabbit knees without evidence of immune response. 21 To address potential for scaling up, we are exploring spinner suspension cultures to generate larger volumes of microspheroids. In vivo implantation over longer durations is needed to document persistence of cellular and tissue phenotypes and enhancement of subchondral repair and remodeling.
This study demonstrates that ES-MSC-derived spheroids, when combined with a customizable NCS, can generate scaffold-free cartilage and osteochondral tissues with region-specific matrix deposition. The neocartilage constructs expressed chondrogenic markers and exhibited mechanical properties suitable for implantation and integration into ex vivo cartilage defects. By predifferentiating spheroids in chondrogenic or osteogenic media, we achieved fused osteochondral tissues with distinct mineralized and cartilaginous regions. These results highlight the potential of ES-MSCs as a clinically translatable cell source for scaffold-free engineering. Future work should focus on scaling constructs for in vivo implantation and evaluating long-term functional outcomes in animal models.
Authors’ Contributions
S.P.G. and D.D.D. were responsible for the overall experimental design. S.P.G. and D.D.D. wrote the article in close collaboration with the other authors. N.E.G. maintained and cultured the cells, 3D cultures, ex vivo studies, and coordinated histological studies. E.W.D. performed the mechanical testing. S.P.G. coordinated and performed quantitative PCR characterizations. All authors discussed the results and reviewed and approved the final version of the article.
Footnotes
Acknowledgments
The authors are grateful for technical assistance by April Damon and Jessica Edwards for gene expression, histology, and immunostaining. They are thankful for the copy editing by Emily Martin. They appreciate the support of the Shaffer Family Foundation and Donald and Darlene Shiley.
Funding Information
This work was funded in part by CIRM (PC1-08128), the Shaffer Family Foundation, and Donald and Darlene Shiley.
Disclosure Statement
No competing financial interests exist.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.