
Abstract
Myocardial infarction (MI), a prevalent critical cardiovascular disease (CVD), poses a severe threat to patients’ lives. Despite the availability of pharmacological, interventional, and surgical treatments in clinical practice, these conventional therapies encounter the bottleneck of difficulty in repairing and reconstructing damaged myocardial tissue. Additionally, novel cardiac repair approaches based on stem cell and cardiomyocyte injections are restricted by the harsh microenvironment of infarcted areas. However, biomaterial hydrogels emerge as promising candidates for MI treatment due to their strong mechanical properties, good biocompatibility, high water absorption capacity, and excellent anti-inflammatory and antioxidant properties. These features enable them to enhance the microenvironment, promote myocardial regeneration, and restore myocardial function. This article delves into the therapeutic effects of sodium alginate (SA) and its composite hydrogel materials in repairing and regenerating myocardial injuries caused by MI. Furthermore, it offers insights into the future research directions of SA and its composite hydrogel materials. It also explores their potential applications in the field of CVDs.
Impact Statement
This review article highlights the significance and potential impact of sodium alginate (SA)-based hydrogels in myocardial infarction (MI) treatment. It effectively communicates the importance of the research, the gap in the current treatments for MI, and how the reviewed SA hydrogels offer a promising solution with their unique properties. It also clearly states the intended contribution to the field and the potential benefits for researchers and clinicians.
Introduction
Myocardial infarction (MI), a common critical cardiovascular disease (CVD), occurs when blood flow to the coronary arteries is significantly reduced or interrupted, causing myocardial cell ischemic necrosis due to ischemia. Globally, it is the leading cause of death, accounting for 42% of CVD-related fatalities, posing a severe threat to patient safety.1,2 Traditional treatments like drug therapy, interventional procedures, and surgery can alleviate MI symptoms, though they struggle to repair the damaged myocardial tissue due to its limited regenerative potential.3,4 Cardiac repair therapy using stem cell or cardiomyocyte injections is promising but faces low cell survival and retention in the harsh infarcted microenvironment.5,6 Thus, cardiac tissue engineering (CTE) techniques, particularly biomaterial hydrogels, have gained attention for repairing and regenerating infarcted hearts. Hydrogels, known for their high water absorption, anti-inflammatory and antioxidant properties, robust mechanical properties, and biocompatibility,7–9 can modulate the infarcted microenvironment, attenuate ventricular remodeling, and induce myocardial regeneration and function restoration.10,11
Currently, hydrogels for MI therapy are classified into six types based on their therapeutic mechanisms: Reactive oxygen species (ROS)-scavenging, conductive, matrix metalloproteinases (MMP)-responsive, immune-modulating, angiogenesis-promoting, and three-dimensional (3D)-printed hydrogels.12–14
They can also be categorized as natural polymer-based (e.g., sodium alginate [SA], cellulose, chitosan, hyaluronic acid, collagen) and artificial polymer-based (e.g., polyacrylic acid, polyacrylamide, poly(vinyl alcohol)) hydrogels.15,16 Among natural polymer-based hydrogels, SA is a promising scaffold material for tissue engineering. SA, a polysaccharide polymer composed of β-
To ensure a stable interfacing between SA hydrogels and beating myocardium, hydrogels matching cardiac tissue biomechanics (e.g., tensile strength, self-healing) and functional properties have been engineered using sol–gel transitions.24,25 This stabilizes the infarct zone via strategies such as bioadhesive moieties (e.g., dopamine), in situ photochemical/enzymatic crosslinking, micro/nanostructuring, and bioactive mediators.26,27 Covalent or strong noncovalent interactions with intrinsic tissue components (e.g., collagen, laminin, and transglutaminase) prevent displacement and enable long-term therapeutic integration. 7 Owing to its superior biocompatibility and injectability, SA hydrogel has been extensively studied for MI repair and functional recovery. SA hydrogel can enhance cardiac function by increasing the thickness of infarct scar, promoting angiogenesis, and inhibiting apoptosis and myocardial fibrosis.28,29 The therapeutic relationship between the physicochemical characteristics of SA-based hydrogels and MI pathology is summarized in Table 1. As an excellent delivery vehicle, injectable SA-based hydrogels can be loaded with therapeutic cargo (e.g., growth factors, extracellular vesicles [EVs], nanomaterials, or stem cells) to restore cardiac function (Fig. 1). This review aims to provide a comprehensive analysis of the mechanisms and therapeutic efficacy of SA-based hydrogels in MI treatment while highlighting future research directions and potential applications in cardiovascular and other diseases.
The Therapeutic Relationship Between the Physicochemical Characteristics of Sodium Alginate-Based Hydrogels and the Pathological Features of Myocardial Infarction Diseases
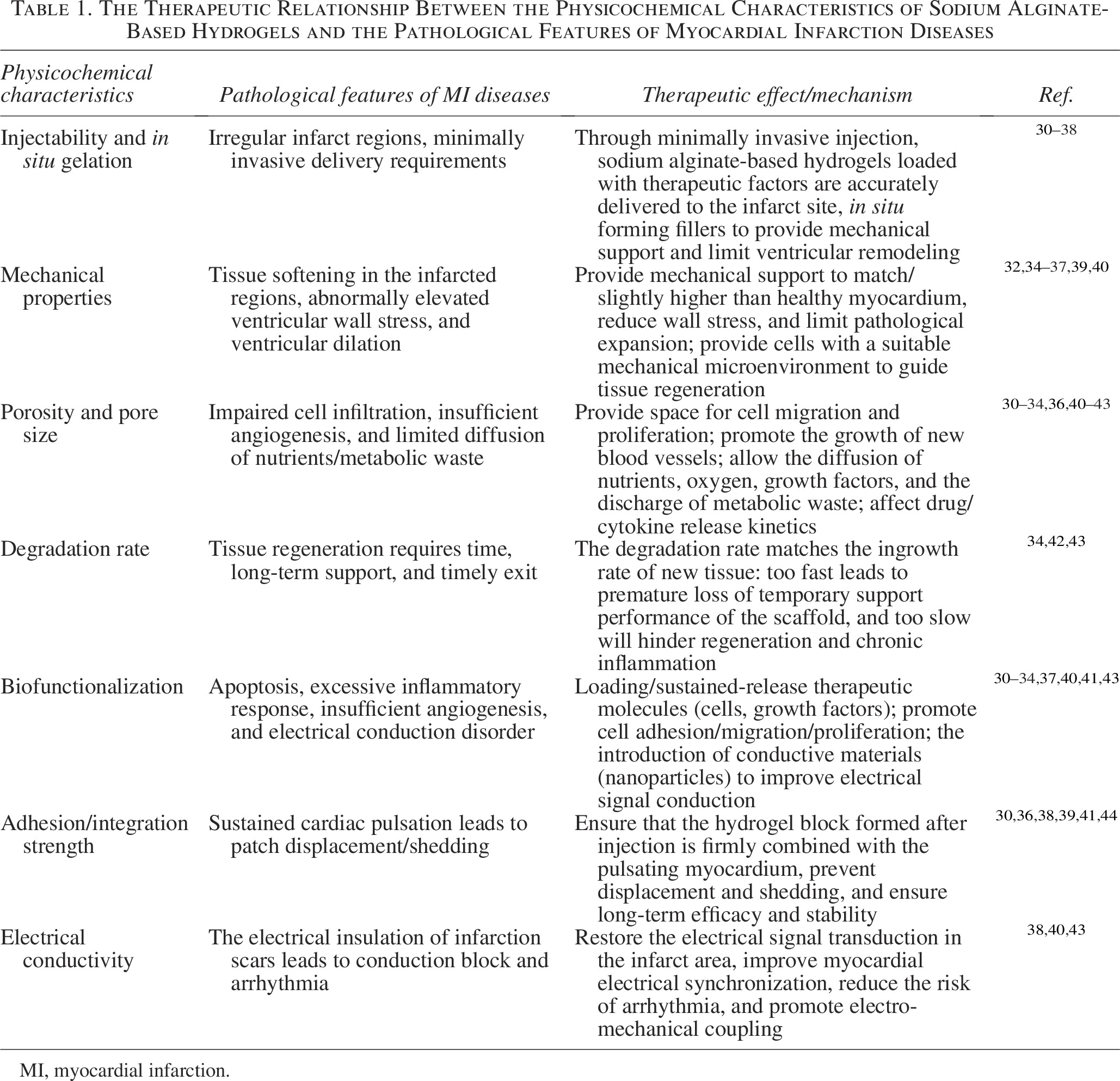
MI, myocardial infarction.
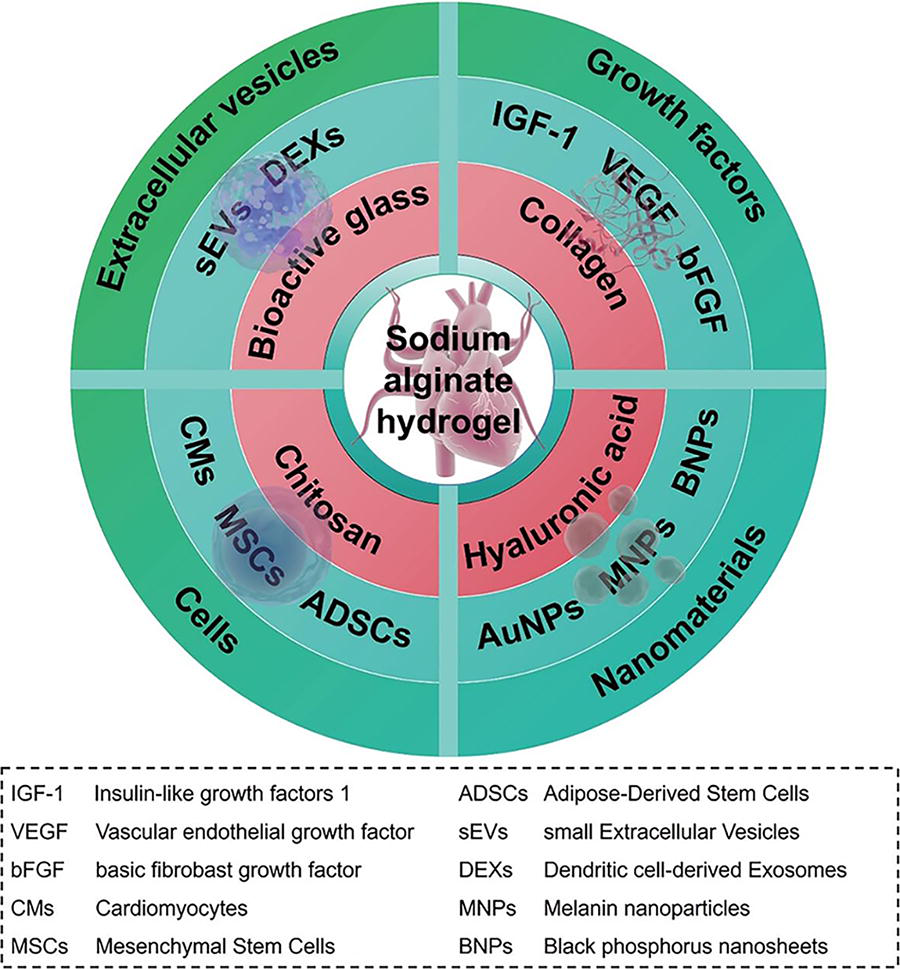
Schematic representation of sodium alginate and composite hydrogel-mediated delivery of bioactive substances for myocardial infarction therapy.
SA hydrogel
As a nonimmunogenic, water-soluble linear polymer, SA is widely employed in biomedical applications, including drug delivery and wound healing, due to its biodegradability, injectability, and favorable safety profile.45,46 Its excellent physicochemical and mechanical properties enable mechanical support to reduce cardiomyocyte apoptosis while promoting vascular regeneration and immune regulation, thereby establishing a reparative microenvironment for myocardial tissue. SA hydrogels can further be loaded with bioactive factors, 47 EVs, 48 nanomaterials, 49 and stem cells 50 to restore cardiac function. In summary, SA hydrogel serves as a safe and versatile therapeutic biomaterial with efficient drug-loading/release capabilities, while its injectability enhances patient comfort and treatment adherence. 7
Loading of bioactive factors
MI is characterized by massive cardiomyocyte death, inflammation, and fibrotic scar formation, influencing cardiac function. Myocardial fibrosis, a common pathophysiological feature, involves excessive extracellular matrix (ECM) protein deposition, distorting myocardial structure and causing arrhythmias and dysfunction.51,52 Various growth factors and cytokines, such as tumor necrosis factor-α (TNF-α), interleukin (IL-1), transforming growth factor-β (TGF-β), stromal cell-derived factor-1 (SDF-1), vascular endothelial growth factor (VEGF), and platelet-derived growth factor (PDGF), are secreted via paracrine mechanisms, playing a role in myocardial fibrosis activation and cardiac function improvement.30,53,54 Introducing appropriate bioactive factors is a promising MI treatment strategy. SA hydrogel, with good biocompatibility and ECM-like mechanical properties, serves as an excellent carrier for loading and releasing bioactive factors.
Insulin-like growth factor 1 (IGF-1), a key cytoprotective factor, enhances cardiac function by reducing postinfarction inflammation, increasing cardiomyocyte survival, and inhibiting apoptosis.31,55 However, its clinical use is limited by its short half-life and low myocardial uptake efficiency. Feng et al. developed an injectable SA hydrogel incorporating IGF-1-loaded silk fibroin (SF) microspheres prepared via coaxial needle technology (Fig. 2a). 56 The hydrogel with 1.5% SA showed optimal proliferation-promoting and antihypoxia effects on H9C2 cardiomyocytes (CMs). Compared with the Gel/IGF-1 group, SF microspheres enabled sustained IGF-1 release for up to 28 days. Echocardiography revealed the Gel + SF/IGF-1 group had the highest left ventricular ejection fraction (LVEF) and cardiac function improvement. Hematoxylin and eosin and Masson trichrome staining indicated thicker walls and reduced fibrosis. Additionally, this group showed the lowest inflammatory factor expression (IL-6 and TNF-α), leading to smaller infarct sizes and significant cardiac function improvement 28 days postprocedure.
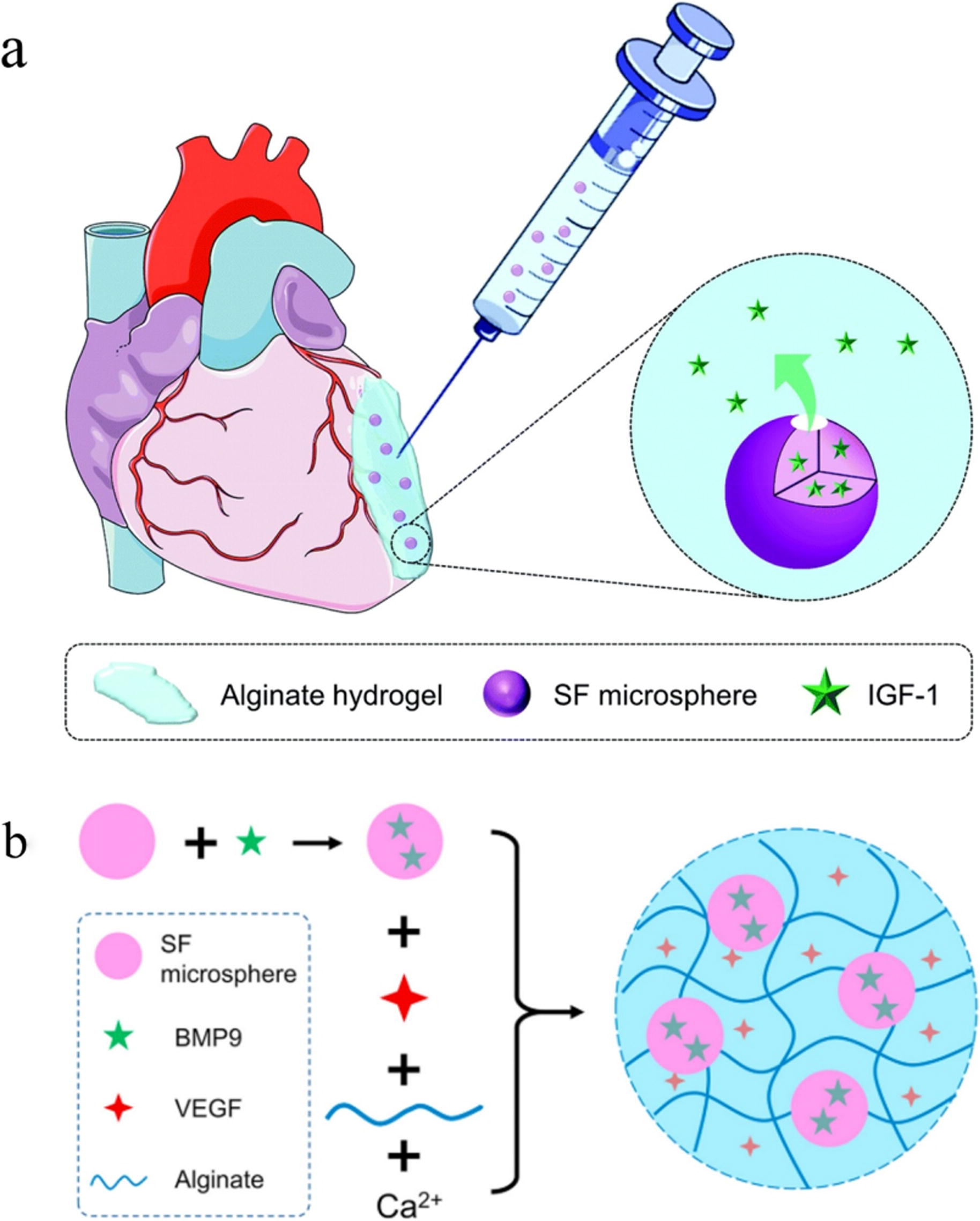
VEGF promotes endothelial cell proliferation and migration in the infarcted area, accelerating neointimal formation and early infarcted microenvironment improvement. 58 Bone morphogenetic protein 9 (BMP9), an endogenous myocardial fibrosis inhibitor, protects cardiac function long-term by suppressing TGF-β1 activity. 59 However, uncontrolled VEGF and BMP9 release limits their application. Wu et al. developed an injectable SA hydrogel loaded with VEGF and BMP9-containing SF microspheres for controlled release (Fig. 2b). 57 In vitro experiments showed VEGF achieved rapid initial release, while BMP9 released slowly and continuously. ELISA and immunohistochemical staining (α-SMA and CD31) indicated VEGF-containing groups (Gel + V and Gel + B/SF + V) had the highest vessel density, highlighting VEGF’s angiogenesis promotion. The Gel + B/SF + V group demonstrated the best antifibrotic effect in a mouse MI model with smaller infarct areas. In conclusion, SA hydrogels mediate bioactive factor release to promote early angiogenesis and long-term fibrosis suppression post-MI, demonstrating clinical potential. Future work should optimize controlled release kinetics for enhanced therapeutic efficacy.
Loading of EVs
Containing soluble proteins, mitochondrial DNA, mRNA, and noncoding RNAs, EVs play a pivotal role in reducing cardiomyocyte death, promoting vascular regeneration, and repairing myocardial tissue damage.41,60 EVs can be divided into exosomes (30–150 nm), microvesicles (150–1000 nm), and apoptotic bodies (>1000 nm), with exosomes showing therapeutic potential due to low immunogenicity. 61 EVs mainly mediate intercellular communication by modulating the downstream signaling pathway.62,63 However, high intracardiac pressure impedes their retention, limiting therapeutic duration. Therefore, SA hydrogel, with its 3D network structure, water absorption, and biocompatibility, has been used as a carrier for EVs.
Stem cell-derived small EVs (sEVs) show antiapoptotic, proangiogenic, and immunomodulatory properties. 64 Lv et al. proposed loading sEVs from bone marrow mesenchymal stromal cells (MSCs) in SA hydrogel (sEVs-Gel) for MI therapy. 39 In vitro fluorescence imaging showed sEVs-Gel enhanced sEVs retention in the heart, reducing cardiomyocyte apoptosis and CD68+ macrophage numbers. CD31 and α-SMA staining showed higher vessel density in the sEVs-Gel group. Also, echocardiography and Masson trichrome staining revealed better cardiac function and neovascularization in the sEVs-Gel group (Fig. 2a). Thus, sEVs loaded in SA hydrogel prolonged their retention time and promoted angiogenesis, decreased cardiomyocyte apoptosis, inhibited myocardial fibrosis, enhanced scar thickness, and improved cardiac function.
Exosomes, the smallest EV subtype, have important roles in tissue repair, immunomodulation, and disease treatment due to their low immunogenicity and excellent biocompatibility.65–67 Dendritic cell-derived exosomes (DEXs) improve myocardial function by activating CD4+ T cells but have a short in vivo half-life. 68 Zhang et al. constructed a DEXs-Gel delivery system by combining DEXs with SA hydrogel to prolong DEXs’ retention time. 69 Near-infrared fluorescence imaging showed DEXs-Gel achieved controlled release for 10–12 days. Echocardiography at 14 days postoperatively showed a significant increase in LVEF (69.76% ± 4.16%) and LVFS (34.97% ± 3.04%) in the DEXs-Gel group (Fig. 2b). Immunofluorescence staining showed DEXs reduced proinflammatory M1 macrophage (iNOS+) infiltration and increased anti-inflammatory M2 macrophage (CD206+) and Treg cell infiltration (Foxp3+). In summary, DEXs-Gel effectively improved postinfarction inflammation, cardiomyocyte apoptosis, and neovascularization by prolonging DEXs’ retention time. This study also revealed the potential mechanism of SA hydrogel delivering DEXs to activate Treg cells and regulate macrophage polarization to improve cardiac function.
Loading of nanoparticles
The hypoxic microenvironment in early MI features elevated ROS levels, substantially limiting cardiac repair/regeneration strategies.70,71 This oxidative stress causes irreversible damage to CMs and vascular cells while activating signaling pathways that induce excessive inflammatory factor secretion via M1 macrophages, triggering severe inflammatory responses.3,32 Nanomaterials, including metallic nanoparticles, carbon-based structures, and natural nanoparticles, offer tunable, biocompatible platforms exhibiting quantum size effects and high specific surface areas. These properties enable their application as drug delivery carriers that enhance therapeutic stability and facilitate targeted biodistribution.72,73 Particularly, nanoparticles (NPs) demonstrate significant therapeutic potential through anti-inflammatory/antioxidant effects, promotion of neovascularization, and immune modulation. Therefore, integrating SA hydrogel with multifunctional NPs represents a synergistic strategy for MI therapy.
To address the irreversible damage to CMs and vascular cells caused by elevated ROS in hypoxic microenvironments, new strategies are needed to scavenge ROS, reduce oxidative stress in CMs, and promote macrophage polarization to an anti-inflammatory M2 phenotype, which is crucial for postinfarction repair.33,71 Zhou et al. used melanin nanoparticles (MNPs) from squid ink and alginate (Alg) from seaweed to form a novel injectable hydrogel (MNPs/Alg) via Ca2+ crosslinking, exploring its effects on ROS scavenging and macrophage M2 polarization (Fig. 3a). 74 The MNPs/Alg hydrogel significantly improved CMs survival in vitro, increasing survival rates by about 30% even in 200 μM H2O2-induced oxidative stress. In a rat MI model, the hydrogel increased cardiac LVEF by approximately 20% and reduced infarct size from 54.3% to 20.7%. It also promoted gap junction formation, angiogenesis between CMs, and increased left ventricular (LV) wall thickness, thus improving cardiac remodeling and function. The hydrogel was also found to promote macrophage M2 polarization and attenuate inflammation by modulating the PI3k/Akt1/mTOR signaling pathway. However, the specific signaling pathways and mechanisms by which MNPs regulate macrophage polarization require further exploration. Additionally, future studies should investigate combining the MNPs/Alg hydrogel with other therapies, like stem cell or gene therapy, to enhance cardiac repair.
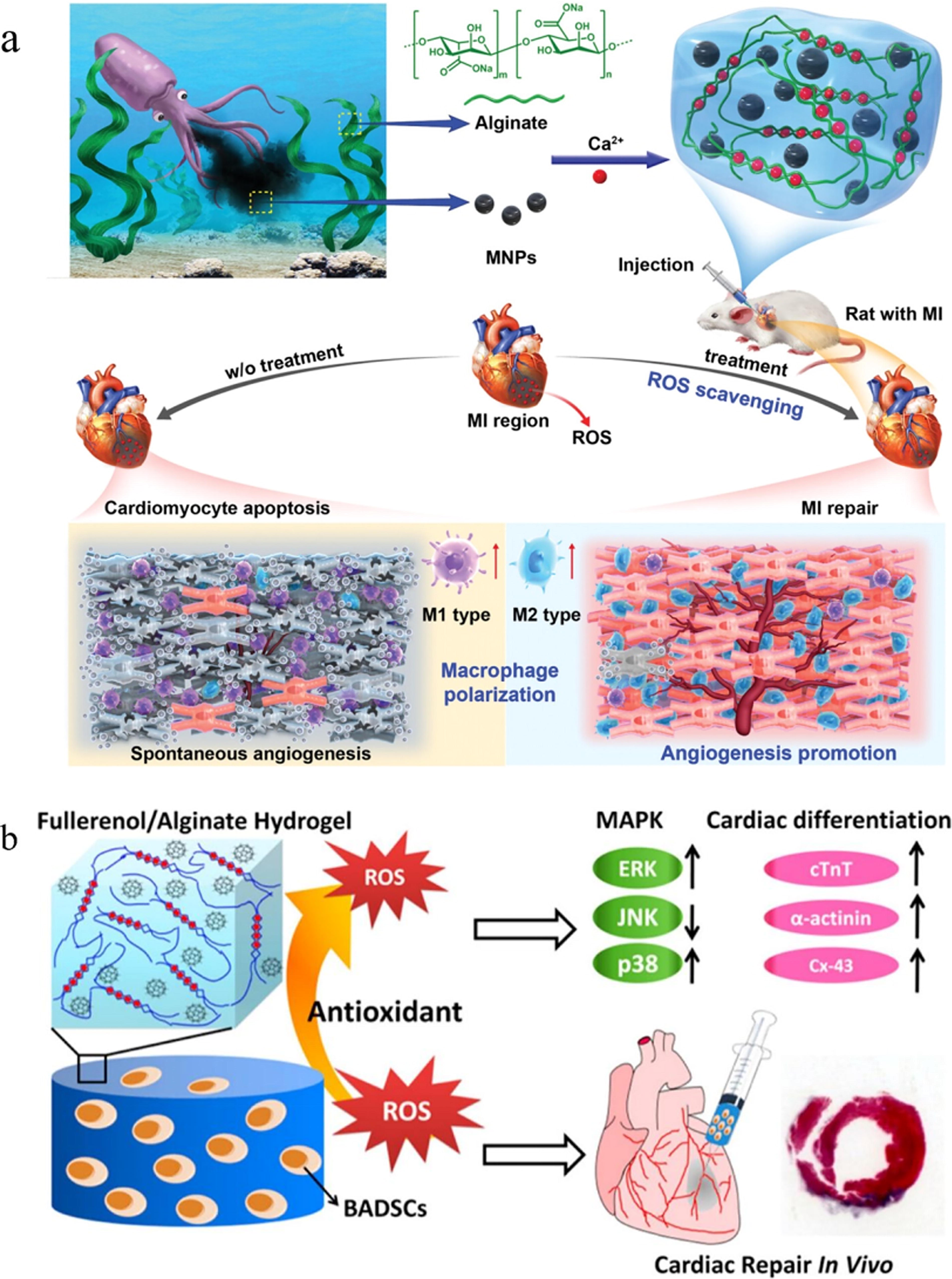
Carbon-based nanoparticles also show good antioxidant properties for scavenging ROS in the infarcted microenvironment. 76 Unlike other carbon materials, fullerenol, as a fullerene derivative, has excellent water solubility, antioxidant properties, and low cytotoxicity. It can adsorb ROS to electron-deficient sites on its surface, alleviating oxidative stress in CMs.77,78 Hao et al. prepared an injectable cell delivery vehicle with antioxidant activity by loading fullerenol nanoparticles into SA hydrogel (Fig. 3b). 75 The fullerenol/SA hydrogel demonstrated good injectability and mechanical strength and effectively scavenged superoxide anions (O2−) and hydroxyl radicals (·OH). In vitro, it significantly improved the survival and differentiation of brown adipose-derived stem cells (BADSCs) under oxidative stress, with a survival rate of 43.6% versus 1.6% in the control group, and 27.2% of BADSCs still survived four weeks postprocedure. Furthermore, the fullerenol/SA hydrogel group showed significant cardiac function improvement, with LVEF and LVFS higher than other groups (LVEF: 48.3% vs. 32.6%, LVFS: 32.5% vs. 20.1%). In summary, recent studies present a novel antioxidant SA hydrogel with excellent biocompatibility. By modulating the infarcted microenvironment, enhancing stem cell survival, and promoting cardiomyocyte differentiation, this system offers a promising approach for injectable cell delivery in MI treatment.
Bioglass/SA hydrogel
Composed of SiO2, Na2O, P2O5, and CaO, bioactive glass (BG) is a multifunctional inorganic material with good biocompatibility and biodegradability, with its applications in proangiogenesis, immunomodulation, and regenerating muscle, cartilage, and gastrointestinal tissues increasing.79–81 In addition, BG ions can downregulate proinflammatory cytokines (e.g., IL-6, TNF-α) and upregulate anti-inflammatory ones (e.g., TGF-β, VEGF) in LPS-stimulated macrophages.34,82 The SA network serves as a physical barrier, delaying BG dissolution to enable sustained, tunable release of therapeutic ions. Concurrently, Ca2+ released from BG maintains the alginate’s cross-linked structure. This self-sustaining synergy establishes the SA-BG composite hydrogel as a promising strategy for continuous myocardial repair.
Cardiac blood flow reestablishment is vital for postinfarction regeneration, since increased local blood flow improves cardiac function. 83 VEGF and bFGF, key angiogenic proteins, drive endothelial and smooth muscle cell proliferation, migration, and angiogenesis.42,84 Qi et al. developed an injectable BG-SA composite hydrogel by mixing BG and SA to promote angiogenesis and improve cardiac function (Fig. 4a). 85 In vitro, 20 μg/mL BG-SA showed good biocompatibility with H9C2 cells. It increased vascular density to 65.52 ± 1.46/mm2 compared with 36.26 ± 3.45/mm2 (saline), 38.10 ± 3.87/mm2 (SA), and 39.80 ± 3.43/mm2 (BG-S groups) by upregulating VEGF and bFGF. Echocardiography confirmed that BG-SA improved cardiac function by reducing infarct area and maintaining wall thickness. This study first proposes BG-SA hydrogel as a minimally invasive, in situ treatment for MI, though future research should focus on improving its biodegradability and tissue permeability.
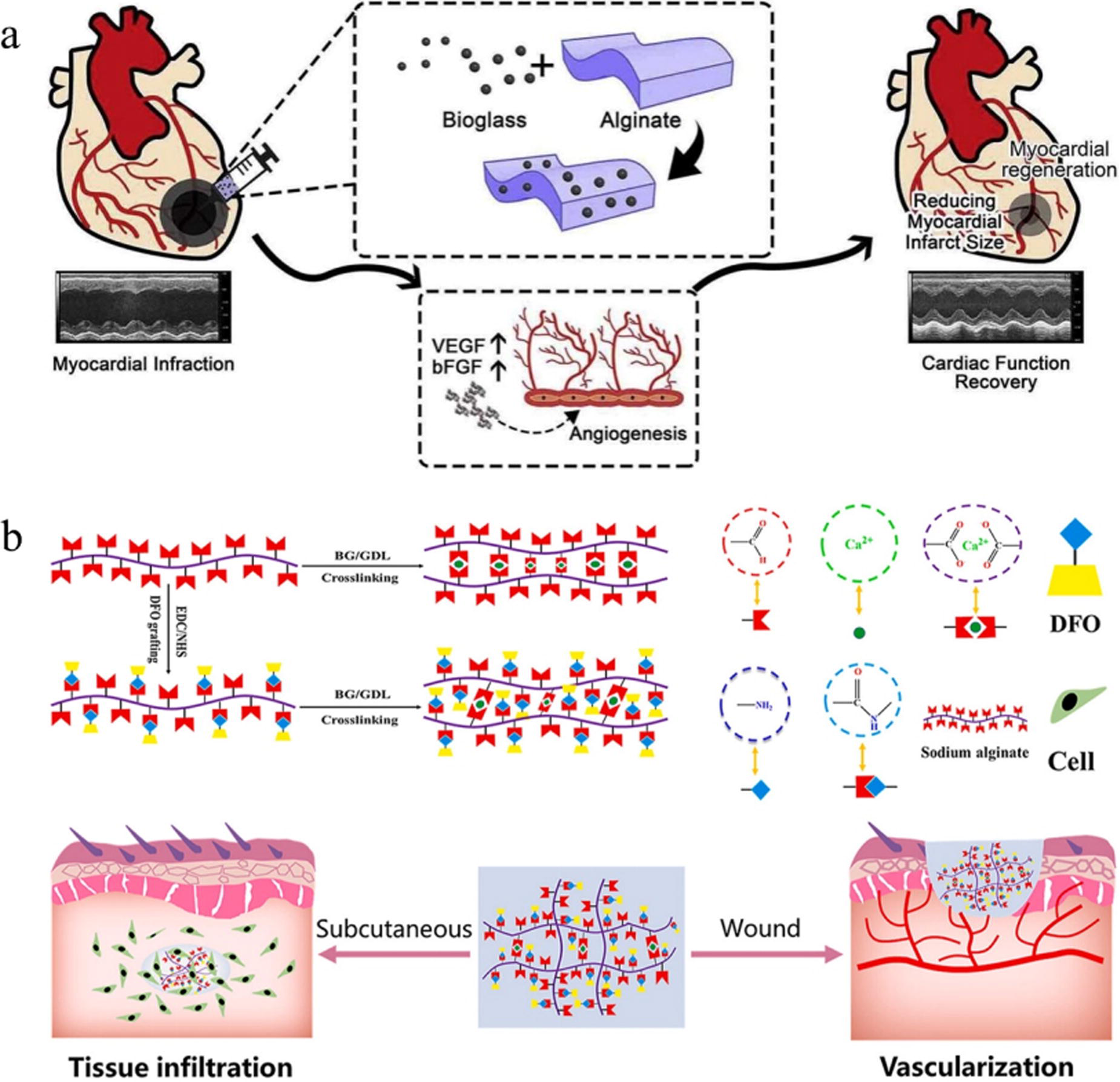
Schematic representation of the preparation and therapeutic effect of BG/SA hydrogel in in vivo cardiac repair
Traditional hydrogels limit the penetration of cells and new tissues due to the limitation of nanopore size, which hinders tissue regeneration. To overcome this, studies aim to develop hydrogels with macroporous structures or controlled degradation.87,88 Zhang et al. prepared a novel G-DFO-SA/BG hydrogel by grafting deferoxamine (DFO) onto SA to modulate degradation properties (Fig. 4b). 86 In vitro, G-DFO-SA/BG showed faster mass loss and structural disintegration than SA/BG. In vivo, it degraded faster, with complete degradation by day 14, compared with SA/BG’s significant degradation starting on day 14. G-DFO-SA/BG also accelerated wound healing, reaching a 99% healing rate on day 14 versus 96% for SA/BG. This study developed a G-DFO-SA/BG hydrogel with rapid degradation and good tissue permeability, whose degradation can be regulated by DFO grafting, showing potential for promoting angiogenesis in myocardial repair. This study developed G-DFO-SA/BG, a novel hydrogel featuring rapid degradation and enhanced tissue permeability. The hydrogel demonstrated significant tissue repair/regeneration capabilities, highlighting its therapeutic potential for promoting angiogenesis in MI repair, warranting further validation.
Chitosan/SA hydrogel
Chitosan (CS), a deacetylated derivative of chitin, is a linear polysaccharide with abundant amine (-NH2) and hydroxyl (-OH) groups that forms hydrogels with good biocompatibility and mechanical properties.35,89 CS hydrogels can activate the PI3K/Akt signaling pathway and upregulate the expression of VEGF to promote myocardial regeneration and neovascularization while inhibiting oxidative stress and inflammation.90,91 Nevertheless, polysaccharide hydrogels formed via Schiff base reaction between CS and SA show promise in drug delivery, wound healing, and myocardial tissue engineering due to their excellent mechanical properties, biocompatibility, and biodegradability.36,92
Postinfarction LV remodeling is usually caused by inflammation and MMP upregulation. Deng et al. developed a temperature-responsive injectable CS/SA hydrogel to prevent LV remodeling and improve cardiac function. 93 In rats injected with the hydrogel, cardiac function improved significantly, with reduced infarct dilatation, fibrosis, and increased scar tissue thickness (0.6 mm) compared with CS (0.33 mm) and SA (0.48 mm) groups. The hydrogel also promoted angiogenesis (vessel density 60% ± 3.2/mm2) and reduced CMs apoptosis (25% ± 1.2%) compared with SA (39% ± 1.4%) and CS (48 ± 2.1%) groups. At 4 weeks posttreatment, LVEF in the CS/SA group was 40.53% ± 4.65%, higher than CS (34.42% ± 3.88%) and PBS (24.84% ± 2.64%) groups. This demonstrates the hydrogel’s potential in reducing LV remodeling and lowering heart failure risk.
Additionally, the ECM is composed of collagen, elastin, and proteoglycans, is crucial for cardiac support, structure, function, and tissue regeneration. After decellularization, ECM-based biomaterials offer low immunogenicity and good biocompatibility.94,95 Tamimi et al. created high-porosity (>96%) hydrogel scaffolds by mixing decellularized bovine myocardial ECM with CS and SA. 96 The 75:25 ECM/CS/SA ratio (E75/P25) showed superior mechanical properties (tensile strength >200 kPa vs. pure ECM’s 49.6 kPa) and cell proliferation. It also promoted human bone marrow mesenchymal stem cells (hMSCs) proliferation and cardiomyocyte differentiation, with immunofluorescence showing higher cardiac troponin-T (cTnT) expression (55.5% ± 7.38%) than pure ECM (24% ± 7.17%). This ternary scaffold material shows great potential for CTE due to its biocompatibility, mechanical properties, and pore structure, which facilitate cardiac cell regeneration/repair. This ECM-SA-based ternary scaffold exhibits biocompatibility, suitable mechanical properties, and pore structure conducive to myocardial regeneration, demonstrating promise for CTE.
Hyaluronic acid/SA hydrogel
Hyaluronic acid (HA) is a naturally occurring linear polysaccharide that is widely found in human connective tissue and is biocompatible, biodegradable, and moisturizing. 97 HA received attention in the treatment of inflammatory diseases and tissue regeneration applications as a key ingredient in the modulation of inflammatory responses. 37 The HA/SA composite hydrogel, combining HA and SA, provides an excellent microenvironment for CMs and improves cell survival in infarcted areas, thereby alleviating postinfarction ventricular remodeling and restoring cardiac function.98,99 This hydrogel’s 3D network can load slow-release growth factors, nanomaterials, and stem cells to enhance therapeutic effects in infarcted regions.
Platelet-rich fibrin (PRF) is a second-generation platelet concentrate that is widely used for angiogenesis and tissue repair because of its safety profile and ability to release growth factors.43,100 Qian et al. created a novel injectable composite hydrogel by freeze-drying PRF to obtain lyophilized platelet-rich fibrin (Ly-PRF) and combining it with ALG-HA. 101 In vitro, the alginate (ALG) hydrogel with 20% HA showed the best mechanical properties. Ly-PRF released growth factors like PDGF-AA more effectively and sustainably (21 days) in the ALG-HA hydrogel than the platelet-rich plasma (PRP) group, with a total release of 10638.55 ± 1577.43 pg/mL compared with 7940.06 ± 910.28 pg/mL in the PRP group. In vivo, rats injected with ALG-HA (Ly-PRF) hydrogel showed a significant increase in LVEF (43.51 ± 2.48%) after 4 weeks, compared with the MI group (24.86 ± 2.82%) and ALG-HA group (34.30 ± 2.46%). This study proposes a new, effective, and safe MI treatment strategy by combining Ly-PRF with ALG-HA hydrogel, achieving sustained growth factor release and promoting neovascularization and myocardial repair (Fig. 5a). It also reveals Ly-PRF’s potential in regulating inflammatory responses and myocardial fibrosis, providing a theoretical basis for future clinical applications.
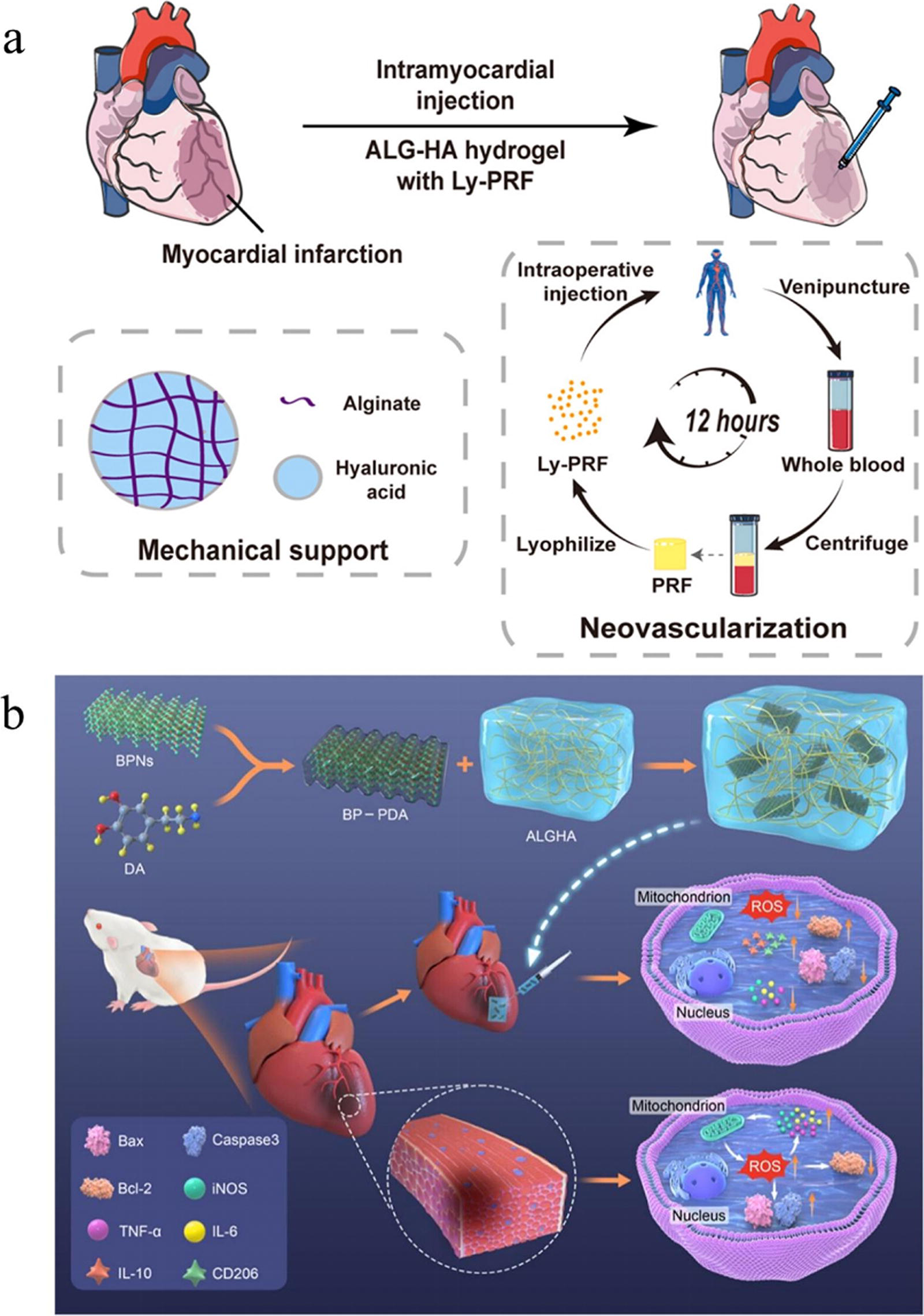
Black phosphine nanosheets (BPNs) are novel two-dimensional nanomaterials with excellent stability and biocompatibility that control oxidative stress and inflammation by scavenging free radicals.103,104 Guo et al. prepared an ALG-HA-BP-PDA hydrogel by loading polydopamine-modified BPNs into ALG-HA to inhibit the oxidative stress-inflammatory chain in MI (Fig. 5b). 102 The hydrogel showed good biocompatibility and electrical conductivity (about 0.085 S/m) without negatively affecting H9C2 CMs’ survival and function. It significantly reduced ROS levels, with 2,2-diphenyl-1-picrylhydrazyl radical and -OH scavenging rates of 81% and 89.6%, respectively. Compared with the MI group, ALG-HA-BP-PDA-treated rats showed a smaller infarct area (reduced by about 40%) and higher LVEF values (increased from 24.86% to 43.51%). The hydrogel reduced TNF-α and iNOS expression mainly by inhibiting the NF-κB signaling pathway and increasing M2-type macrophages, alleviating the inflammatory response. Although HA alone cannot form robust hydrogels via ionic crosslinking, its combination with SA creates a supportive primary network where HA undergoes physical entanglement and mild covalent crosslinking. The resulting ALG-HA-BP-PDA hydrogel demonstrated therapeutic efficacy by effectively scavenging ROS, suppressing inflammation and CMs apoptosis, significantly inhibiting LV remodeling, and improving cardiac function.
Gelatin/SA hydrogel
Gelatin hydrogel (GH), a biodegradable and water-soluble polymer derived from hydrolyzed collagen, exhibits excellent biocompatibility, promotes cell adhesion/proliferation, and maintains high cell retention/viability. It serves as an effective delivery platform for transplanted cells such as CMs, 105 MSCs, 106 and ADSCs. 107 It can provide mechanical support to the heart after infarction and promote infarct healing through anti-inflammatory, antioxidant stress, and angiogenesis-promoting properties. 86 Further studies have shown that GH hydrogels can be used to transport stem cells, organs, and nanoparticles.5,108 Moreover, combining Gel with SA forms a thermally stable gel network at physiological temperatures, resolving gelatin’s inherent melting and structural collapse issues. This synergy grants the GH/SA composite hydrogel significant advantages for myocardial repair applications.
Mitochondria regulate cell function, scavenge ROS to rescue macrophages, promote the expression of anti-inflammatory and tissue repair factors, and promote the proliferation and activation of myofibroblasts in the infarcted area.38,109 Hassanpour et al. assessed MSC-derived mitochondria encapsulated in PPy-rich Alg/Gel conductive hydrogel’s therapeutic effect in a rat MI model. 110 The Alg/Gel + PPy hydrogel (87.67% ± 0.57% porosity) was more porous than the Alg + PPy group (83.33% ± 1.52%), preserving mitochondrial integrity. Compared with the MI group, the mitochondria-loaded Alg/Gel + PPy hydrogel group showed increased LV wall thickness and more vWF+ capillaries and α-SMA+ small arteries, indicating proangiogenic and antifibrotic effects. This implies the hydrogel promotes CMs survival/recovery and improves the infarcted area’s microenvironment via neovascularization. Future studies should explore how mitochondria function in CMs and develop advanced delivery platforms for better tissue repair.
In MI, the death of CMs and the deposition of collagen fiber can interfere with the transmission of electrical signals in the myocardium, leading to cardiac dysfunction and arrhythmias. To address this, hydrogels must support the growth of CMs and be electrically conductive.111,112 Pournemati et al. developed a novel hydrogel with good electrical conductivity and biocompatibility by incorporating gold nanoparticles (AuNPs) into Alg/Gel hydrogel. 44 The Alg/Gel + AuNPs composite hydrogel had a porous network structure and electrical conductivity of 2.04 × 10−4 S/cm, much higher than Alg/Gel hydrogel’s 2.38 × 10−8 S/cm. Methylthiazolyldiphenyl-tetrazolium bromide experiments showed it had no significant toxicity to embryonic mouse CMs and improved cTnT and Cx43 expression. Moreover, Alg/Gel + AuNPs hydrogel encapsulating mECCs significantly increased cell survival in the infarcted area and improved cardiac function while reducing infarcted and fibrotic areas 30 days postoperation. This study presents an injectable hydrogel based on SA and gelatin, enhanced with AuNPs for improved conductivity and biocompatibility, for postinfarction mECCs transplantation and myocardial repair, demonstrating the potential of nanoparticle-loaded composite hydrogels for myocardial repair. These findings demonstrate the significant potential of nanoparticle-loaded GH/SA hydrogels in cardiac regeneration. Future work should establish multifunctional delivery platforms with expanded tissue repair capabilities and broader disease applicability.
Conclusions
SA-based hydrogels exhibit a unique combination of mechanical robustness, exceptional biocompatibility, high hydration capacity, and inherent anti-inflammatory and antioxidant properties, which collectively enhance the therapeutic efficacy for MI. These advanced materials have demonstrated remarkable potential in improving cardiac function by increasing scar thickness, promoting angiogenesis, modulating oxidative stress and immune responses, and inhibiting apoptosis and myocardial fibrosis (Table 2). The injectable nature of SA hydrogels further enables minimally invasive delivery and precise targeting of the infarcted region, providing significant advantages in clinical applications.
Sodium Alginate and Its Composite Hydrogel in the Treatment of Myocardial Infarction
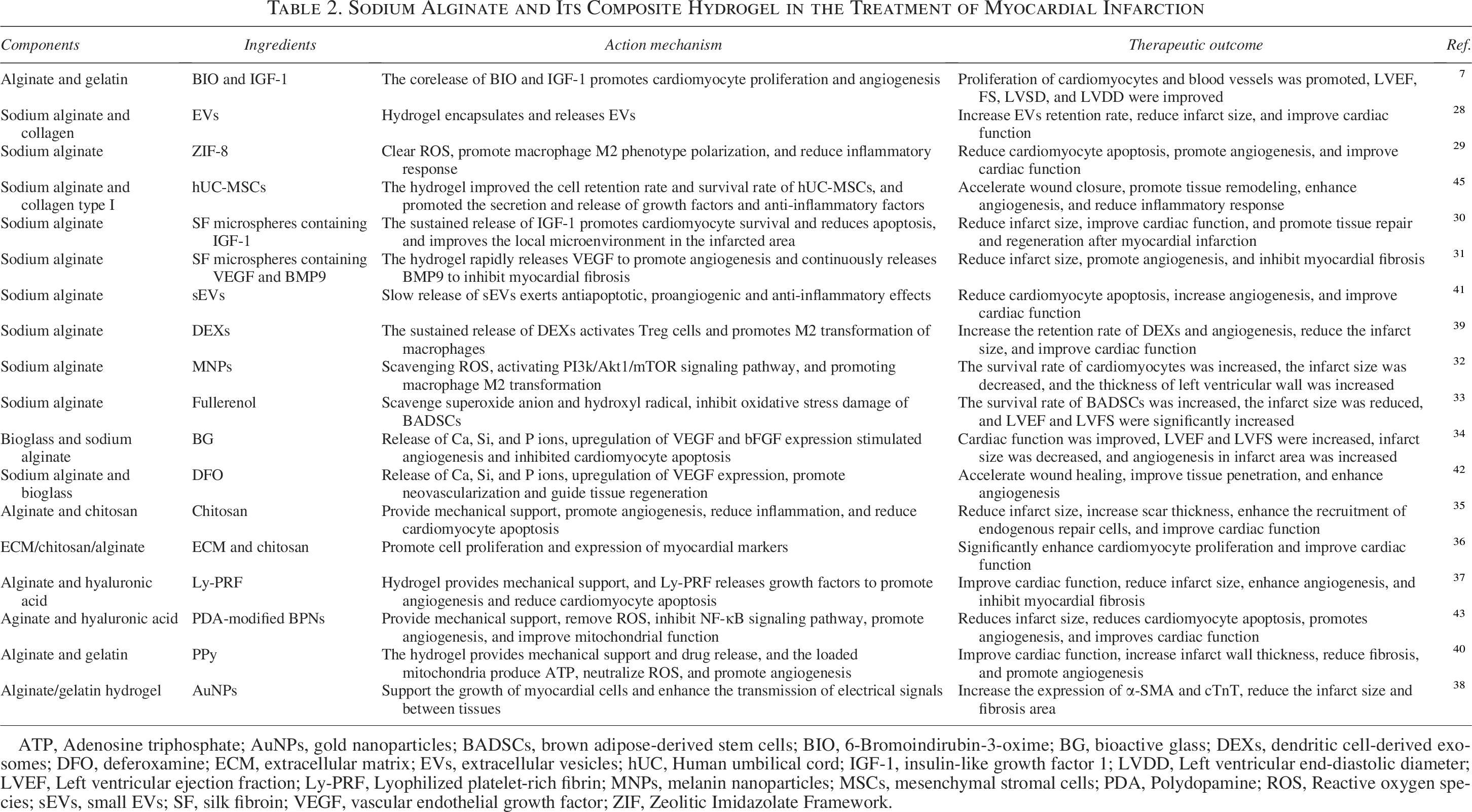
ATP, Adenosine triphosphate; AuNPs, gold nanoparticles; BADSCs, brown adipose-derived stem cells; BIO, 6-Bromoindirubin-3-oxime; BG, bioactive glass; DEXs, dendritic cell-derived exosomes; DFO, deferoxamine; ECM, extracellular matrix; EVs, extracellular vesicles; hUC, Human umbilical cord; IGF-1, insulin-like growth factor 1; LVDD, Left ventricular end-diastolic diameter; LVEF, Left ventricular ejection fraction; Ly-PRF, Lyophilized platelet-rich fibrin; MNPs, melanin nanoparticles; MSCs, mesenchymal stromal cells; PDA, Polydopamine; ROS, Reactive oxygen species; sEVs, small EVs; SF, silk fibroin; VEGF, vascular endothelial growth factor; ZIF, Zeolitic Imidazolate Framework.
The field of cardiac repair and regeneration is continuously evolving, and SA hydrogels have emerged as a promising solution to address the limitations of conventional therapies. However, several challenges remain to be addressed to fully harness their potential. These include the need for more precise control over the mechanical strength and degradation kinetics of the hydrogels to match the dynamic environment of the myocardium. Additionally, the development of multifunctional delivery platforms capable of spatiotemporal control and sustained release of multiple bioactive substances is critical to achieve coordinated improvements in mechanical properties, electrical conductivity, angiogenesis, and immunomodulation.
Future research should focus on optimizing material compositions and structure–property relationships to enhance the robustness, tunable degradation profiles, and biocompatibility of these hydrogels. Furthermore, rigorous clinical efficacy validation, mechanistic elucidation, and the establishment of standardized protocols are essential to ensure the safe and effective translation of these therapies into clinical practice. Addressing these challenges will not only accelerate the adoption of SA hydrogels as viable clinical therapeutics for MI but also pave the way for broader applications in cardiovascular and other regenerative medicine fields.
Authors’ Contributions
Z.C.: Conceptualization; writing, reviewing, and editing—original draft; and visualization. X.L. and E.Z.: Conceptualization, writing, reviewing, and supervision. J.L. and C.Z.: Writing, reviewing, and editing—original draft.
Footnotes
Author Disclosure Statement
The authors declare no competing interests.
Funding Information
This work was supported by Tianjin Municipal Science and Technology Commission Grant, No. 24ZXRKSY00010; and Program for Innovative Research Team in Peking Union Medical College, CAMS Initiative for Innovative Medicine, Nos. 2022-I2M-1-023, 2023-I2M-2-008, and 2021-I2M-1-065.