
Abstract
The reconstruction of critical-sized bone defects remains a challenging clinical problem. At present, the implantation of autogenous and allogeneic grafts is the main clinical treatment strategy but faces some drawbacks, such as inadequate source, donor site-related complications, and immune rejection, driving researchers to develop artificial bone substitutes based on distinct materials and fabrication technologies. Among the bone substitutes, bioceramic-based substitutes exhibit a remarkable biocompatibility, which can also be designed to degrade concomitantly with the formation of new bone. In addition, three-dimensional (3D) printing technologies are frequently used for fabricating personalized 3D bioceramic scaffolds, which can achieve accurate imitation of native bone structures. Especially, bioprinting can produce organoids by integrating cells into scaffolds, which achieves the simultaneous imitation of organ structure and biological function. This review summarizes recent progresses of bioceramic-based materials, including hydroxyapatite, tricalcium phosphate, bioactive glass, calcium silicate, alumina, and zirconia. In addition, the application of 3D printing technologies and bioprinting is also elaborated in this text, offering important reference for future research of 3D-printed bioceramics.
Impact Statement
At present, there are abundant studies on 3D-printed bioceramics. However, bioceramic scaffolds are rarely applied to clinical practice. This review summarizes the bioceramic materials (hydroxyapatite, tricalcium phosphate, bioactive glass, calcium silicate, alumina, and zirconia) and 3D printing technologies (digital light processing, stereolithography, fused deposition modeling, direct ink writing, selective laser sintering, and inkjet printing), especially elaborating the application of bioprinting technology in bone regeneration, with the aim of providing direction for future research and clinical translation of products.
Introduction
With the increasing incidence of traffic accidents, bone tumors, etc., the critical-sized bone defects have become a challenging clinical problem, seriously affecting the life quality of patients and increasing social burden.1–3 The treatment strategies for critical-sized bone defects include autogenous and allogeneic bone transplantation. 4 Among them, autogenous bones have excellent biocompatibility and no risk of disease metastasis, but their application is limited due to inadequate source and donor site-related complications. Allogeneic bones are relatively easy to obtain, but faced with the problems of immune rejection, infection, and ethics. 5 Therefore, developing suitable artificial bones to replace autogenous and allogeneic bones is urgent.
Artificial bones mainly include metals, polymers, and bioceramics. 6 Due to excellent ductility, strength, and fracture toughness, most implants are made of metal materials. 7 However, metal materials have a higher elastic modulus than native bones, which may lead to insufficient callus formation and delayed fracture healing. 8 In addition, although polymers such as polyether ether ketone (PEEK) have similar elastic modulus with the native bone, as well as possess the ability of X-ray penetration and anti-infection, the expensive costs of processing and poor biological activity impede the clinical application of PEEK.9,10
Bioceramics include hydroxyapatite (HA), tricalcium phosphate (TCP), biphasic calcium phosphate (BCP), bioactive glass (BG), calcium silicate (Ca-Si), alumina (Al2O3), and zirconia (ZrO2). Based on the response level of tissues, bioceramics are further divided into bioinert (Al2O3, ZrO2) and bioactive (HA, TCP, BCP, BG, Ca-Si).
11
Among them, bioactive ceramics have attracted great interest from researchers due to good biocompatibility.12–15
By releasing bioactive ions such as Ca2+,
Comparison of Characteristics of Different Bioceramic Materials
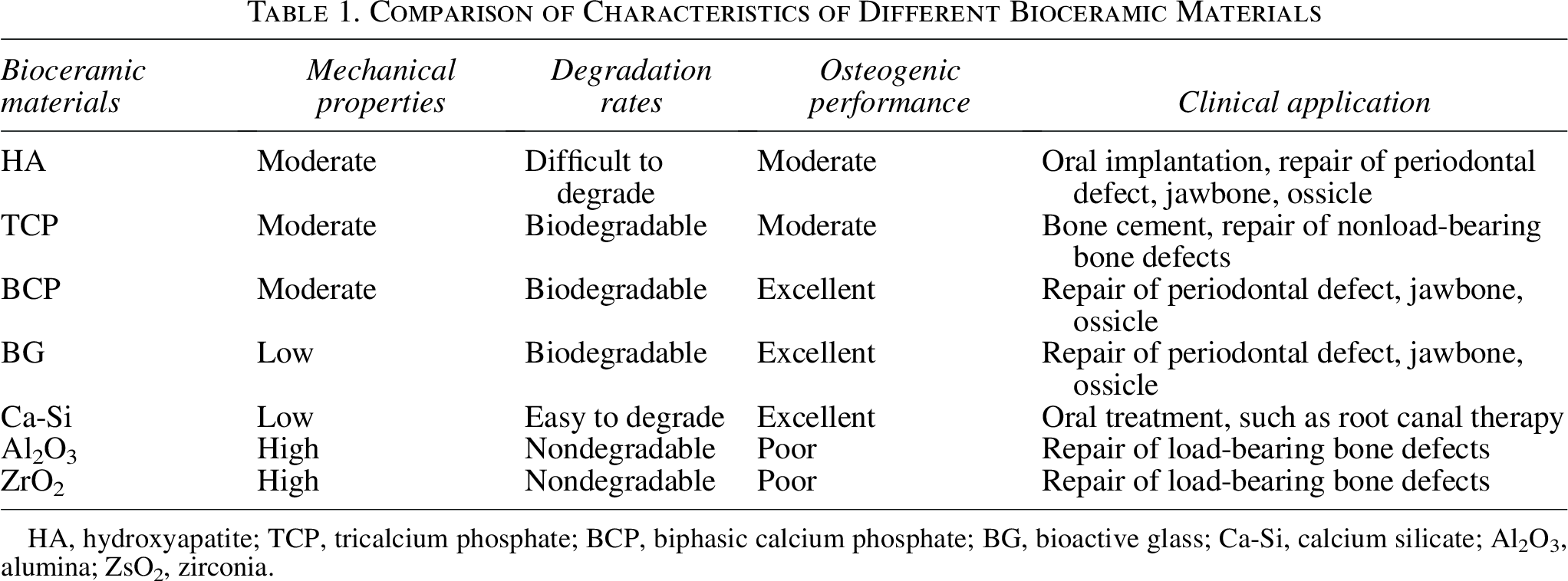
HA, hydroxyapatite; TCP, tricalcium phosphate; BCP, biphasic calcium phosphate; BG, bioactive glass; Ca-Si, calcium silicate; Al2O3, alumina; ZsO2, zirconia.
Conventional ceramic fabrication methods include slip casting, gel casting, etc. Slip casting manufactures green bodies by pouring slurry into a gypsum mold, which can achieve batch production of complex and large-sized products. 19 Gel casting produces green bodies through adding the organic monomer, initiator, and cast into ceramic slurry with high solid content (volume fraction ≥50%) and low viscosity (<1Pa·s). After heating or cooling, the organic monomer in the slurry can be in situ polymerized into a three-dimensional (3D) network structure, and the green body is shaped. Finally, the green body is demolded, dried, degreased (required for gel casting), and sintered to obtain ceramic products. 20 Among them, ceramic sintering is a physicochemical process in which ceramics become dense and hard through material transfer at high temperature. After sintering, ceramics can achieve higher strength by removing pores within them. 21 Nevertheless, sintering may also lead to cracks and pores of ceramics. In summary, the conventional ceramic fabrication methods have difficulties in forming complex structures. Slip casting requires a long time to dry, and the viscosity of the slurry is too high, which may lead to insufficient filling of the mold. In addition, gel casting can produce a green body with uniform composition, high strength, fewer sintering defects, and realize net-size molding of complex parts. However, gel casting cannot fabricate individualized ceramics.
3D printing, also known as additive manufacturing (AM) technologies, fabricates solid parts by accumulating materials layer by layer, the process is regulated by a computer-aided design model. 22 Compared with the conventional fabrication methods, 3D-printed bioceramic scaffolds have some special advantages, such as enhanced bioactivity, a faster degradation rate, and individualized fabrication (Table 2). 3D printing technologies mainly contain digital light processing (DLP), stereolithography (SLA), fused deposition modeling (FDM), direct ink writing (DIW), selective laser sintering (SLS), inkjet printing (IJP), and so forth. 23 In addition, bioprinting, as a kind of new printing technology, can more comprehensively mimic human organs by incorporating cells and bioactive molecules into 3D structures. 24 To conclude, 3D printing can precisely regulate the pore shape and size of bioceramics, providing a favorable microenvironment for osteogenesis. However, bioceramic products are not perfect currently, considering the brittleness and ordinary osteogenic effect. Therefore, it is necessary to summarize the recent research on 3D-printed bioceramics, aiming to provide direction for overcoming the defects of bioceramics.
Comparison of Three-Dimensional-Printed and Conventionally Fabricated Bioceramics
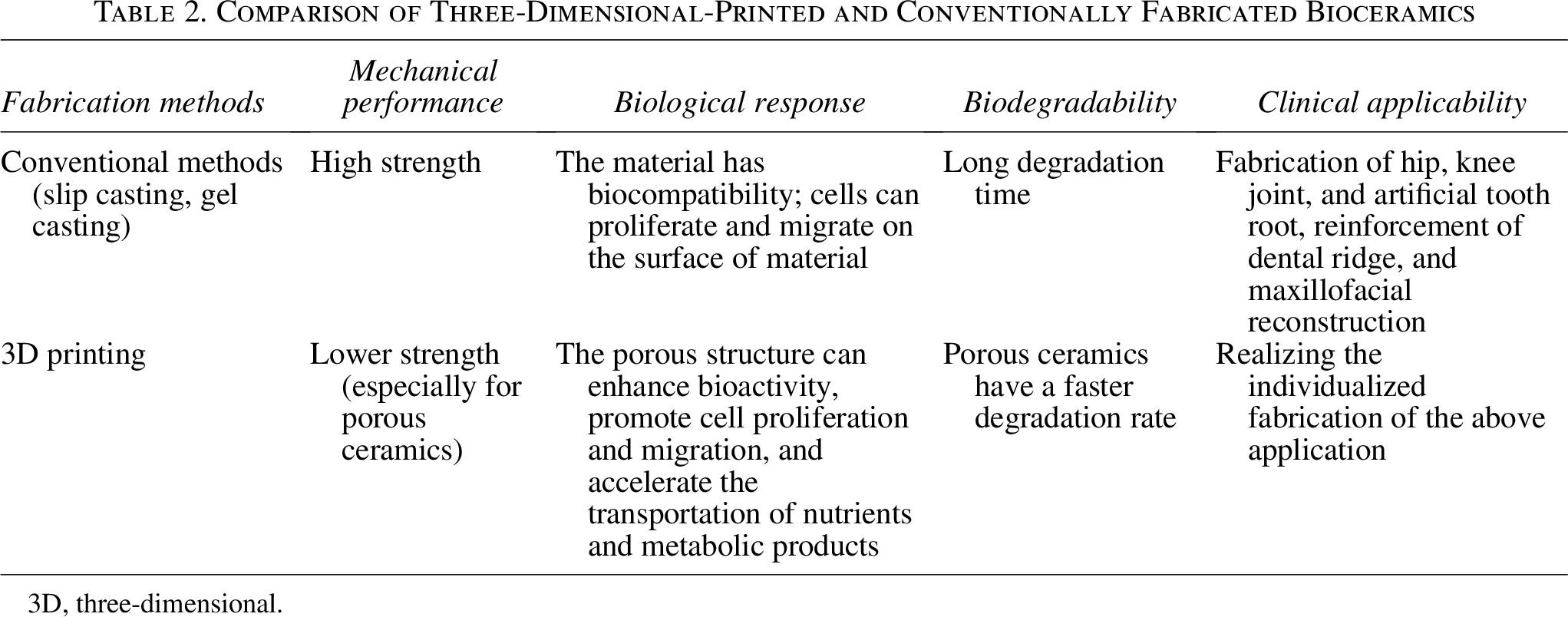
3D, three-dimensional.
Bioceramic Materials for Repairing Bone Defect
Hydroxyapatite
CaP is the most commonly used bioceramic material in craniomaxillofacial bone reconstruction. It has excellent biocompatibility, osteoinductivity, and osteoconductivity properties.25,26 According to the Ca/P atomic ratio, CaP can be further classified into HA (Ca:p = 1.67) and TCP (Ca:p = 1.5).
HA (Ca5(PO4)3(OH)) has excellent osseointegration and osteoconductivity properties.27,28 Table 3 lists some cases of HA bioceramics applied in the field of bone regeneration. It is evident that HA bioceramics exhibit excellent performance in repairing bone defects and enhancing the mechanical strength of the scaffold. It is attributed to the following aspects. First of all, HA can release bioactive Ca2+and
Application and Remarks on Hydroxyapatite in Bone Regeneration
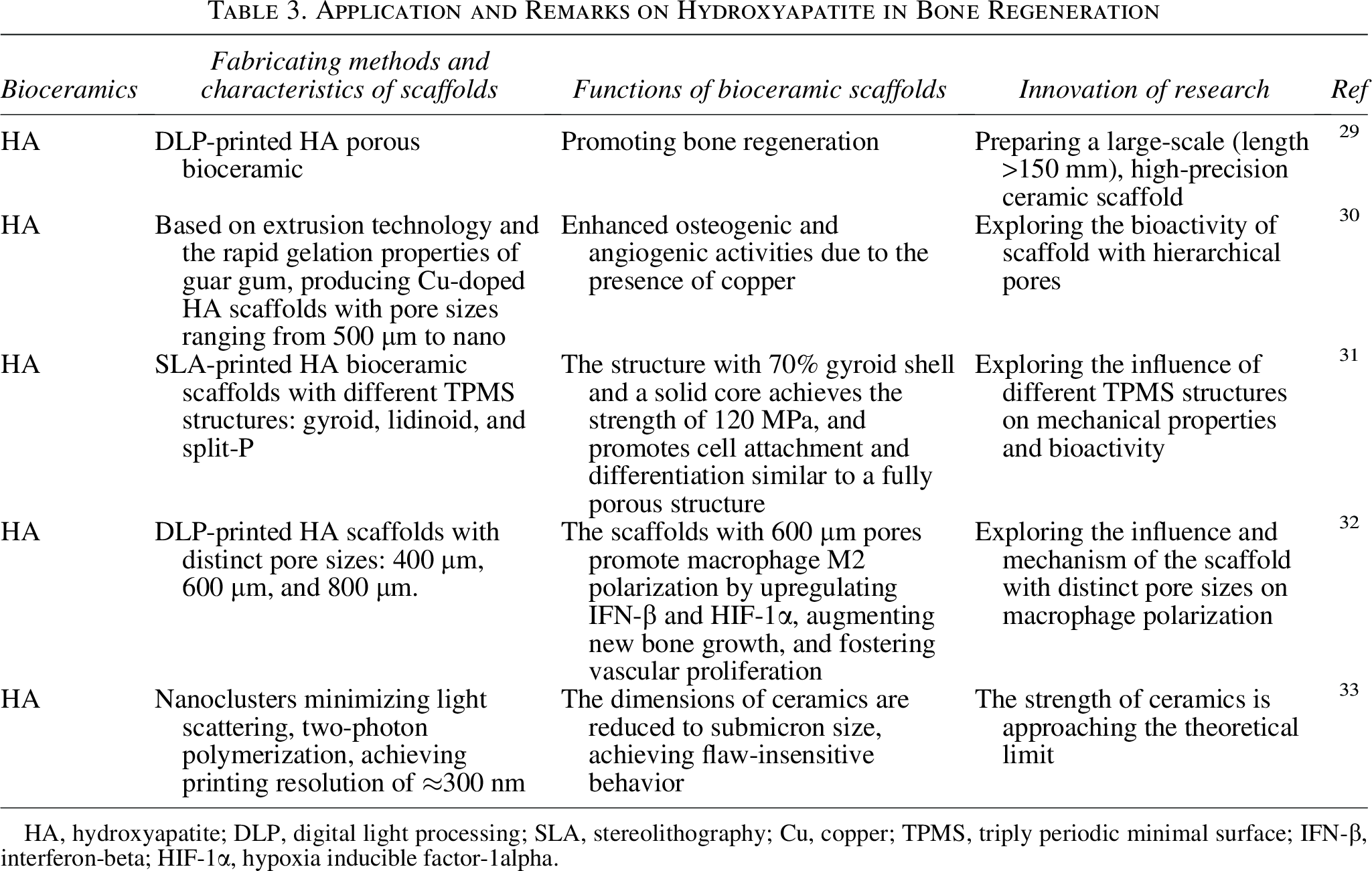
HA, hydroxyapatite; DLP, digital light processing; SLA, stereolithography; Cu, copper; TPMS, triply periodic minimal surface; IFN-β, interferon-beta; HIF-1α, hypoxia inducible factor-1alpha.
Although HA bioceramic scaffolds have been extensively studied in the field of bone regeneration, HA is more suitable to be used as a bone filler, such as cement and granules or coated on the surface of metallic prostheses, in consideration of the brittleness and poor degradation ability of HA.
34
In addition, the strength of porous ceramics is poor, and Ca2+and
Tricalcium phosphate
TCP [Ca3(PO4)2] includes two forms: α- and β-TCP. α-TCP is easily soluble in aqueous systems and is often used as bone cement. 35 While β-TCP has excellent bioactivity, which can be prepared through solid-state reaction or thermal conversion. 36 In addition, β-TCP has good degradation performance and is stable under room temperature, which is frequently used for preparing bone scaffolds. 37
Table 4 summarizes some application examples of TCP in bone regeneration. It can be seen that TCP bioceramics play an important role in repairing bone defects. It is attributed to the following reasons. On the one hand, by adjusting porosity, pore size, and surface morphology, the optimized scaffold structure enhances the osteogenic effect of TCP ceramics. On the other hand, by affecting Ca/P molar ratio of the ceramic, sintering atmosphere can suppress the process of osteoclastic resorption.
Application and Remarks on Tricalcium Phosphate in Bone Regeneration
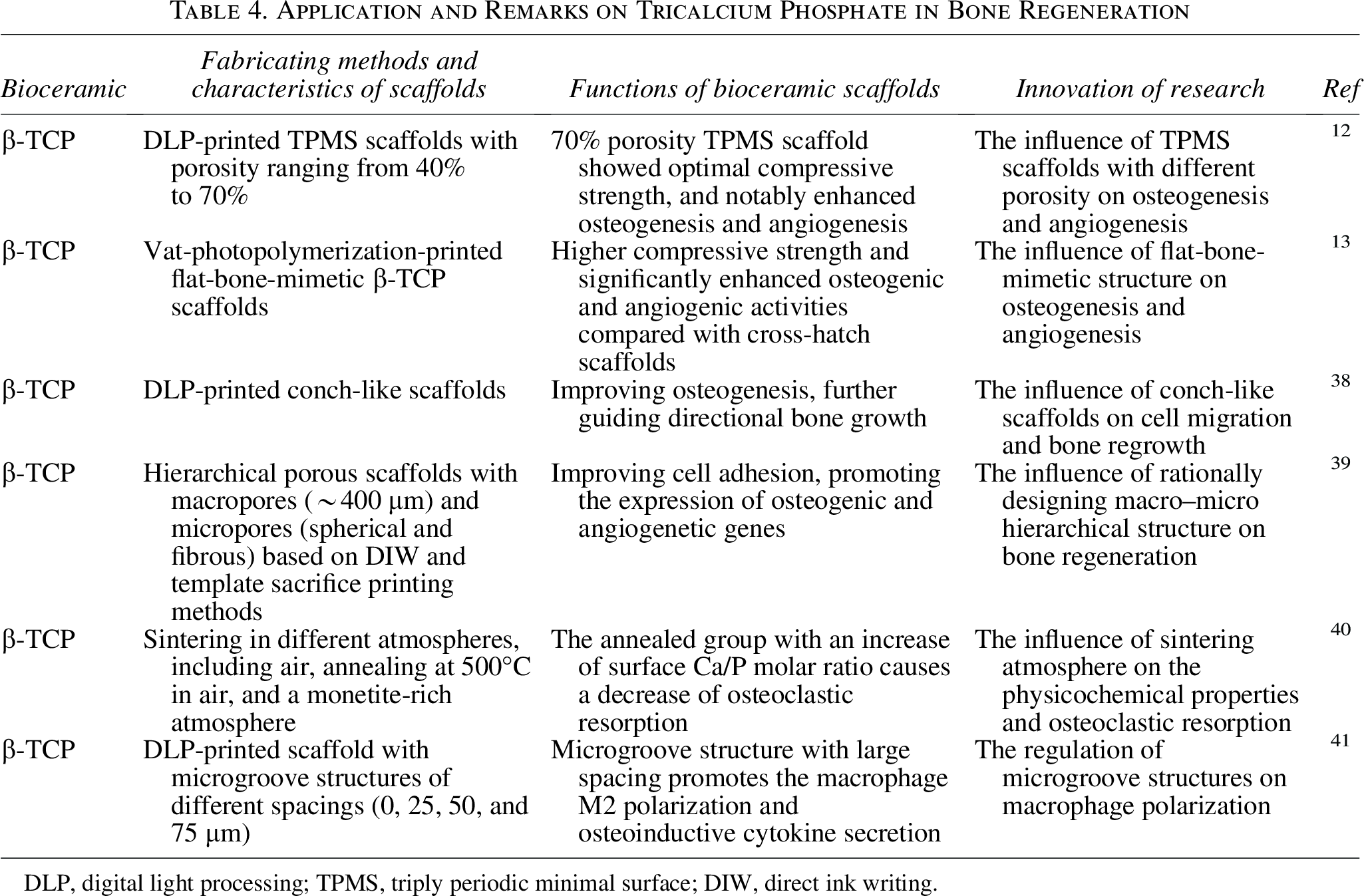
DLP, digital light processing; TPMS, triply periodic minimal surface; DIW, direct ink writing.
Bioinert ceramics
Al2O3, as one kind of bioinert ceramic, is biocompatible and resistant to chemical corrosion, as well as possessing high Young’s modulus and hardness. Al2O3 is often used for fabricating cortical bone. 42 While ZrO2 has excellent toughness and is often used for constructing artificial load-bearing bone. 43 Based on ZrO2 ceramics, Jiang et al. prepared triply periodic minimal surface (TPMS) structures, which promote bone regeneration by regulating osteogenic immunity and angiogenesis. 44
Due to high mechanical strength and long-term stability, bioinert ceramics have a special advantage in repairing bone defects of load-bearing areas. However, poor bioactivity and mismatched elastic modulus limit their application in complex stress environments. 45 Some measures can be taken to overcome the above shortcomings, including surface modification (coated with HA), composite design (ceramic/native polymer), and 3D structure design.
Bioceramic composite materials
HA composite materials
The preparation of conventional ceramic composite materials requires degreasing and sintering steps, leaving only inorganic components. However, many implants currently contain not only inorganic components but also various organic components, which play an important part in bone regeneration. For example, the organic components in bioceramic composites are frequently used for improving osteogenesis and angiogenesis, enhancing the flexibility and plasticity of materials. 46 Therefore, some composite materials are no longer subjected to high-temperature treatment in the end.
Table 5 illustrates some application examples of HA composite materials in bone regeneration. It is evident that HA composite materials offer stronger bone healing potential and superior mechanical properties. For the synthetic polymers/HA composite materials, synthetic polymers such as polycaprolactone (PCL) and polylactic acid (PLA) have strong hydrophobicity. However, HA possesses high surface energy, which can partially offset the hydrophobicity of the synthesized polymer. Therefore, the composite materials of synthetic polymers and HA exhibit excellent function of cell attraction and adhesion. Besides, the incorporation of synthetic polymers with high elastic modulus may offset the brittleness of bioceramics, improving the mechanical properties of composite materials. Furthermore, most synthetic polymers release acidic products during degradation, which can neutralize the alkalinous ions from bioceramics. Finally, synthetic polymers possess excellent processability, so the mixed slurry composed of synthetic polymers and bioceramics has the potential to be produced into various complex structures compared with pure bioceramic slurry.
Application and Remarks on Hydroxyapatite Composite Materials in Bone Regeneration
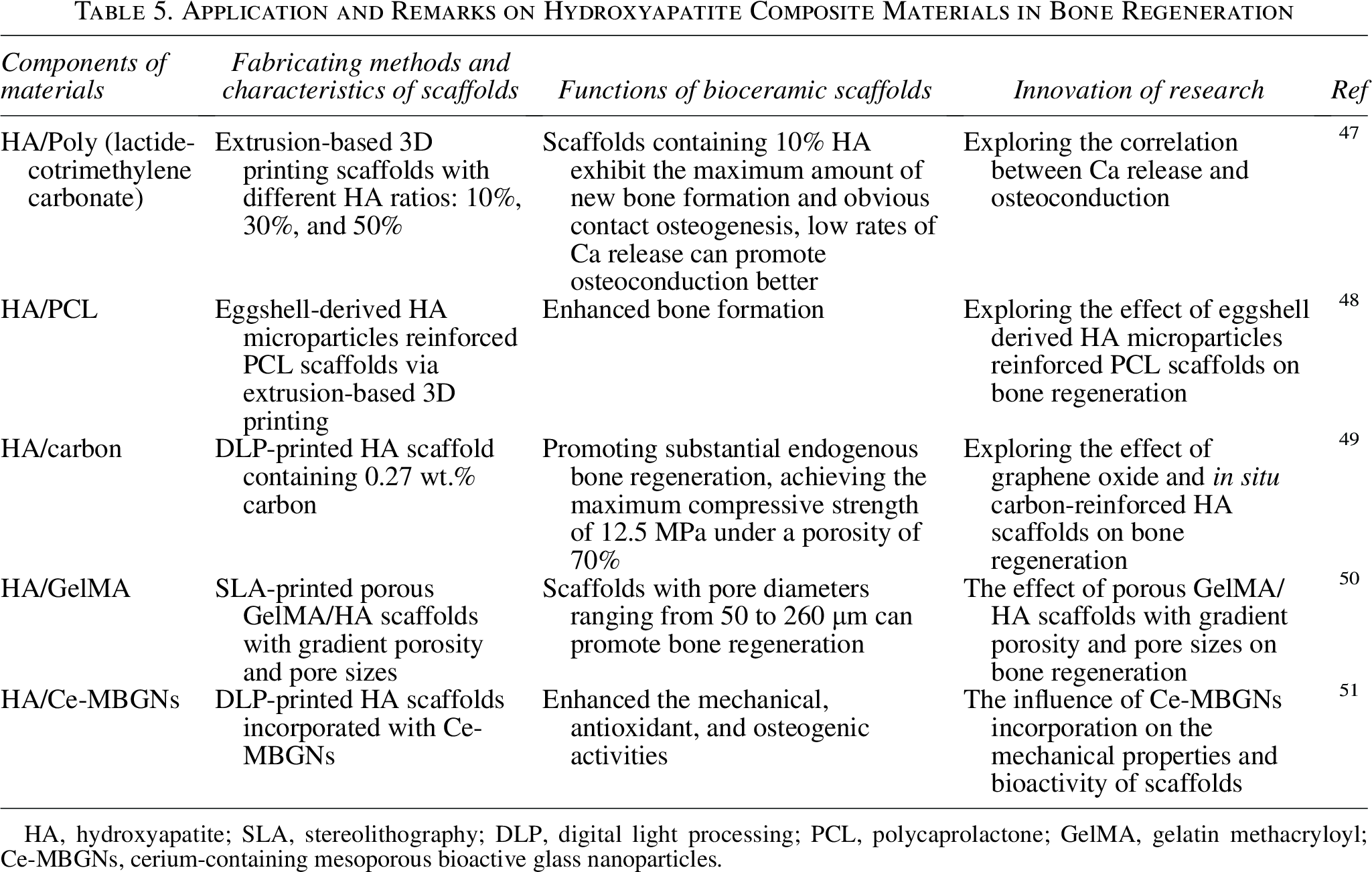
HA, hydroxyapatite; SLA, stereolithography; DLP, digital light processing; PCL, polycaprolactone; GelMA, gelatin methacryloyl; Ce-MBGNs, cerium-containing mesoporous bioactive glass nanoparticles.
TCP composite materials
Table 6 summarizes some application examples of TCP composite materials. It can be seen that the incorporation of osteogenic components can enhance bone regeneration. Osteogenic components, such as differentiation-inducing factors, trace nutrient elements, osteogenic drugs, and bone marrow mesenchymal stem cells (BMSCs), are frequently introduced into materials or modified on the surface of materials to exert the key function of promoting osteogenesis. Nevertheless, there is a potential risk that excessive osteogenic components may lead to side effects, such as heterotopic ossification. Therefore, it is necessary to blend osteogenic components into ceramic slurry or use the chemical networks of hydrogels to wrap them, which can avoid the burst release of osteogenic components, as well as create an environment conducive to the survival of MSCs.
Application and Remarks on Tricalcium Phosphate Composite Materials in Bone Regeneration
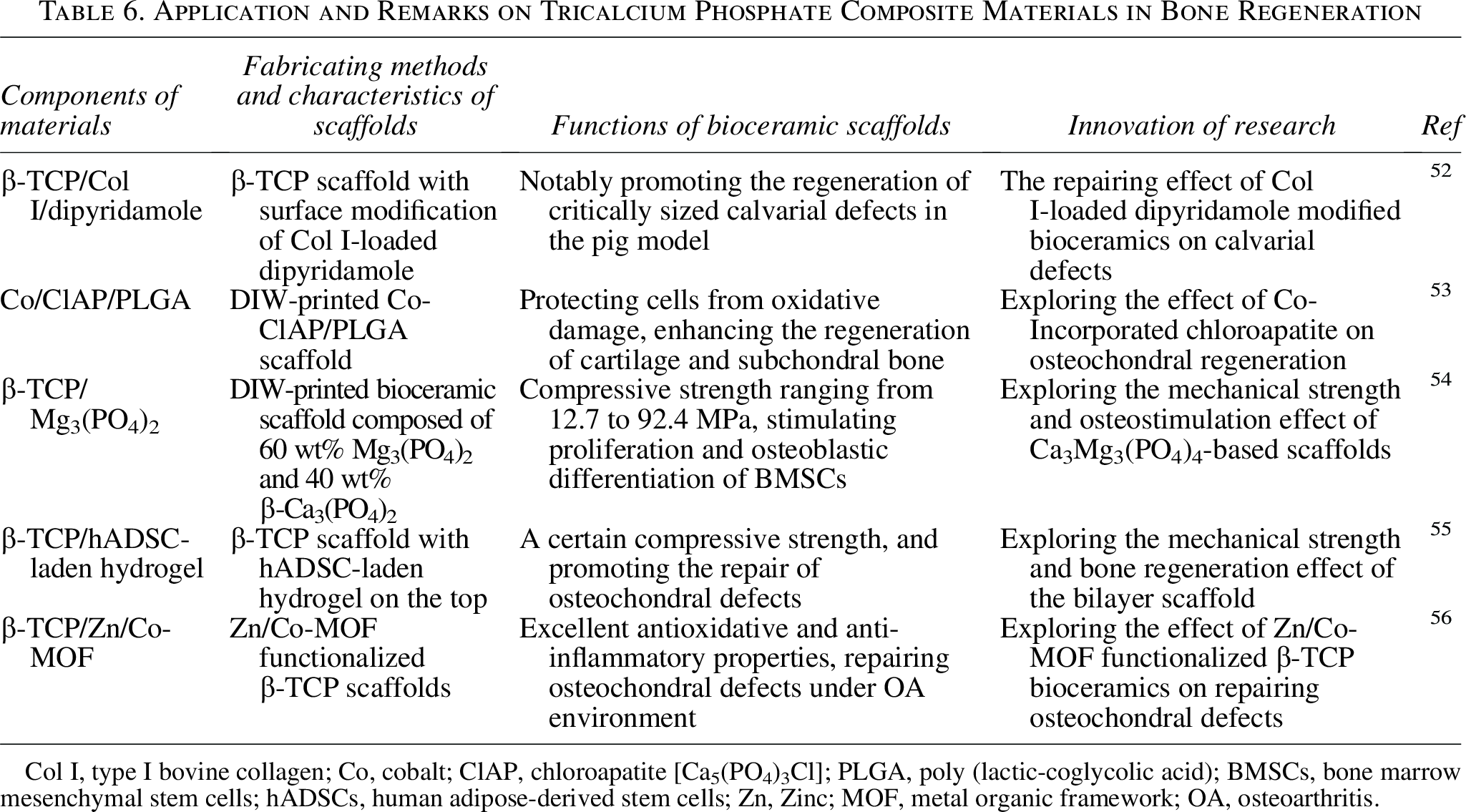
Col I, type I bovine collagen; Co, cobalt; ClAP, chloroapatite [Ca5(PO4)3Cl]; PLGA, poly (lactic-coglycolic acid); BMSCs, bone marrow mesenchymal stem cells; hADSCs, human adipose-derived stem cells; Zn, Zinc; MOF, metal organic framework; OA, osteoarthritis.
BCP composite materials
Compared with HA, β-TCP has the advantage of easy degradation, which is an ideal characteristic for implant materials. However, rapid degradation may lead to a decrease in mechanical properties, even implant failure. BCP composite materials, composed of HA and β-TCP in a different ratio, have the advantages of slow degradation and excellent bioactivity. 57 BCP has been widely explored in the field of bone regeneration. Table 7 illustrates some application examples of BCP bioceramic. It is evident that BCP composite materials have good mechanical properties and osteogenic activity, making them a great potential for future transformation research.
Application and Remarks on Biphasic Calcium Phosphate and Mesoporous Bioactive Glass Composite Materials in Bone Regeneration
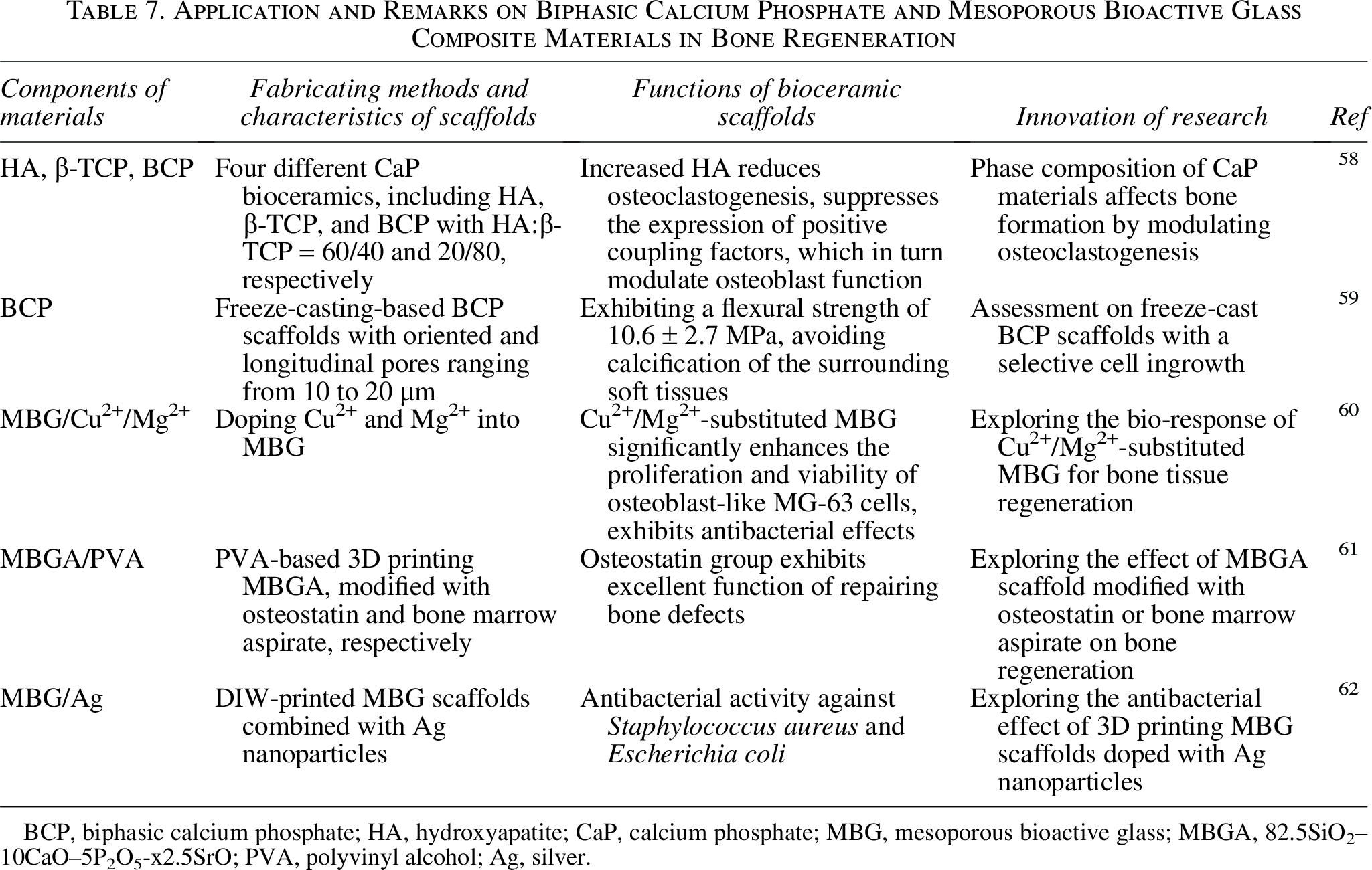
BCP, biphasic calcium phosphate; HA, hydroxyapatite; CaP, calcium phosphate; MBG, mesoporous bioactive glass; MBGA, 82.5SiO2–10CaO–5P2O5-x2.5SrO; PVA, polyvinyl alcohol; Ag, silver.
BG composite materials
BG [45S5 Bioglass, 45SiO2–24.5Na2O–24.5CaO–6P2O5 (wt%)], including phosphate-, silicate-, and borate-based glasses, is produced by sol–gel or traditional melting–quenching techniques.63,64 With the dissolution of Ca2+, P5+, Na+, and Si4+, the surface of BG will form HA, which can help BG bond to tissues tightly.65,66
Mesoporous bioactive glass (MBG), as one type of BG, has a well-organized mesoporous texture, and the pore sizes of MBG range from 2 to 50 nm. 67 MBG has a large surface area and pore volume, which facilitate the formation and attachment of HA layer and ensure the excellent bioactivity of MBG. 68 Currently, many researchers use MBG to deliver drugs, inorganic ions, and organic compounds to the injured sites, further promoting bone regeneration and resisting bacteria. 69 Table 7 summarizes some application examples of MBG composite materials. It can be seen that MBG is frequently doped with some metal ions such as Cu2+, Mg2+, and Ag+ to promote osteogenesis, as well as to exert antibacterial effects.
Ca-Si composite materials
Ca-Si can significantly promote the repair of bone defects in nonload-bearing areas, and is frequently used as sealers in stomatology, which shows bioactivity by releasing Ca2+ and Si4+. Ca2+ is crucial for regulating metabolic processes of bone regeneration, 70 while Si4+ can promote cell adhesion and angiogenesis in the early stage of calcification.71,72 Based on the constituent and property, Ca-Si is divided into monocalcium silicate (CaSiO3), dicalcium silicate (Ca2SiO4), and tricalcium silicate (Ca3Si2O7). 73
Ca-Si is often mixed with other components to improve material properties. Table 8 illustrates some application examples of Ca-Si composite materials. It is evident that the composition of Ca-Si with organic polymers (silk fiber/gelatin), metal element Mg2+, or inorganic polymers [PCL, polyvinyl alcohol (PVA)] significantly improves material properties. It can be attributed to the following reasons. First, combining Ca-Si with organic polymers such as silk fibroin/gelatin can further reduce immune rejection responses, making Ca-Si ceramics more suitable for tissue repair. Besides, organic polymers generally possess good flexibility and plasticity, which can be used for improving the mechanical properties of Ca-Si ceramics. What is more, most of the native organic polymers have antimicrobial properties, which makes Ca-Si composite materials suitable for an infection environment. Finally, the high degradation rate of Ca-Si may lead to high pH values around the grafts. Acidic products from synthetic polymers can neutralize alkaline ions, further regulating pH values to a normal level.
Application and Remarks on Calcium Silicate Composite Materials in Bone Regeneration
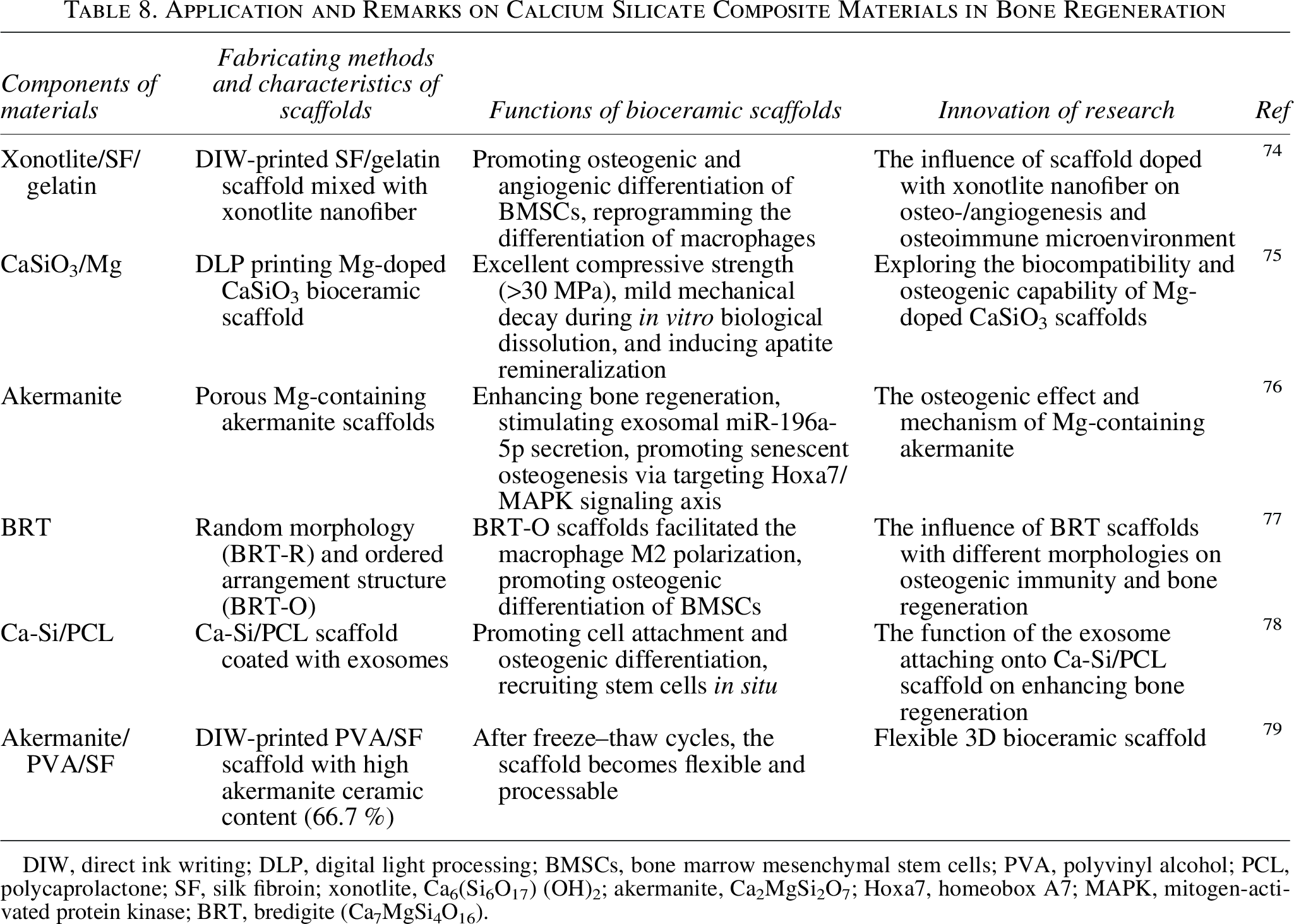
DIW, direct ink writing; DLP, digital light processing; BMSCs, bone marrow mesenchymal stem cells; PVA, polyvinyl alcohol; PCL, polycaprolactone; SF, silk fibroin; xonotlite, Ca6(Si6O17) (OH)2; akermanite, Ca2MgSi2O7; Hoxa7, homeobox A7; MAPK, mitogen-activated protein kinase; BRT, bredigite (Ca7MgSi4O16).
3D Printing Technologies for Bioceramic Scaffolds
3D printing technologies for bioceramic scaffolds include DLP, SLA, DIW, FDM, SLS, and IJP (Fig. 1). 80 Except for the above traditional printing technologies, bioprinting can produce 3D organ structures such as blood vessels and bones, preliminarily by integrating cells, cytokines, etc. into composite scaffolds, 81 which achieves the simultaneous imitation of organ structure and biological function. The characteristics of different 3D printing technologies are summarized in Table 9.
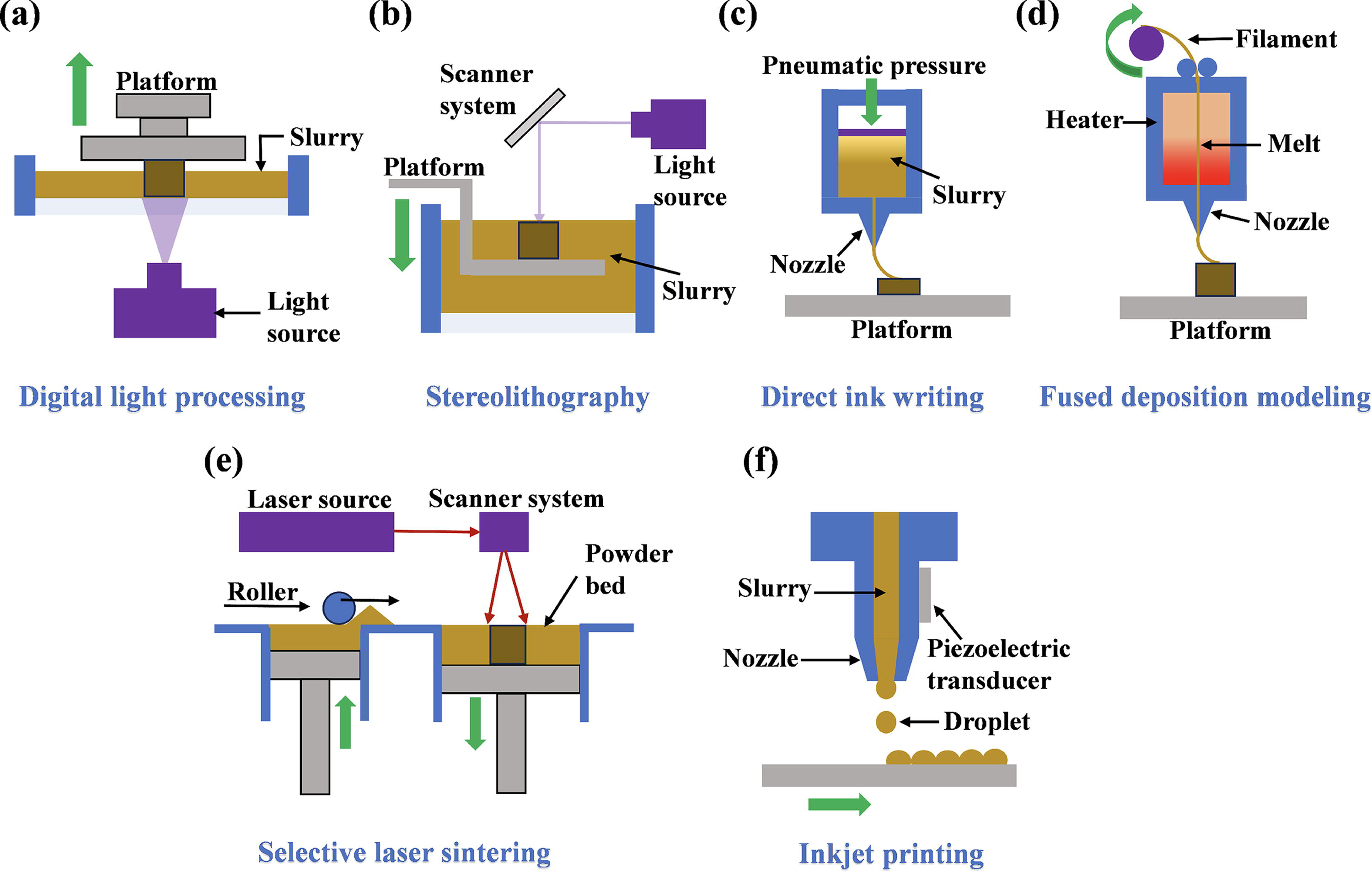
Schematic of three-dimensional (3D) printing bioceramic technology.
The Comparison of Different Three-Dimensional Printing Technologies
DLP, digital light processing; SLA, stereolithography; FDM, fused deposition modeling; DIW, direct ink writing; SLS, selective laser sintering; IJP, inkjet printing; BCP, biphasic calcium phosphate; HA, hydroxyapatite; CaP, calcium phosphate; MBG, mesoporous bioactive glass; TCP, tricalcium phosphate; CaP, calcium phosphate; Ca-Si, calcium silicate; ZrO2 zirconia.
Digital light processing
DLP printing, as one type of vat photopolymerization technology, uses a high-resolution digital light projector as a light source to sequentially project each layer onto the surface of the slurry, achieving solidification of the slurry. As the platform moves, each solidified layer can combine with the previous layer, producing a 3D structure in the form of “layer-body.” 82
Based on DLP printing, Wang et al. prepared CaP ceramic scaffolds with distinct macroporous structures, including simple cube, octet-truss, and inverse face-centered cube. Among them, the structure of inverse face-centered cube shows the largest porosity and compressive strength, as well as the strongest osteoinductivity (Fig. 2). 83 Wu et al. fabricated the BCP scaffold with a hexagonal close-packed spherical pore structure, which promotes the expression of osteogenic genes and proteins in MC3T3-E1 cells, and effectively repairs the femoral condyle defects of rabbits. 84 In addition, TPMS is a kind of structure that has curved pore architectures and fully interconnected pore networks. It has been reported that DLP-printed TPMS structures, such as gyroid and diamond, can notably induce osteogenic differentiation of BMSCs. 14 What is more, the research of Li et al. also demonstrates that TPMS structure has a significant impact on the synthesis of new blood vessels. 85 In summary, the fine structure of scaffolds will determine the properties of bioceramics. By designing and accurately printing the external shape and internal structure, DLP can obtain bioceramic scaffolds with excellent strength and osteogenic activity.
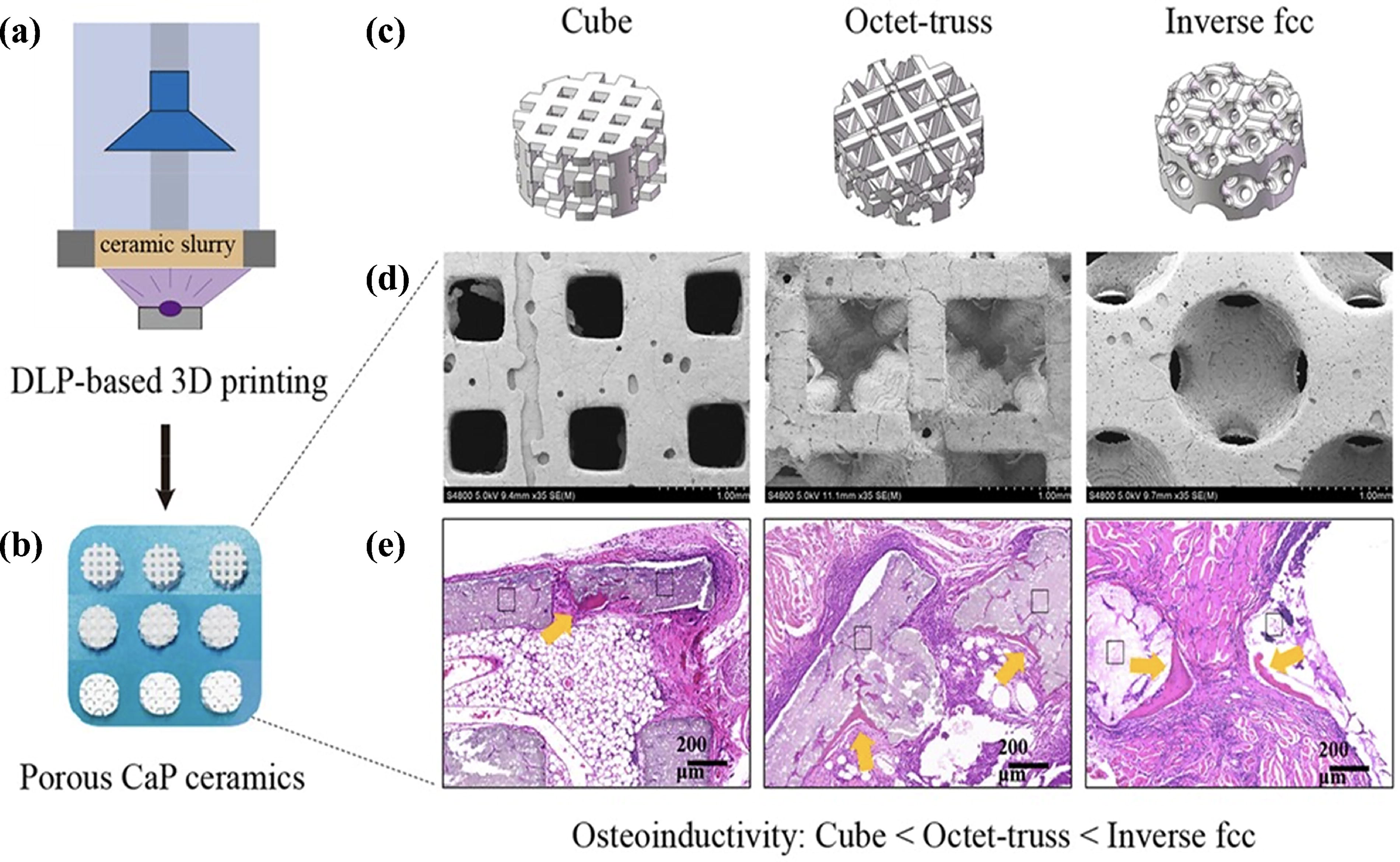
Digital light processing (DLP)-printed calcium phosphate (CaP) bioceramic scaffolds.
DLP technology has the advantages of high precision and short printing time.86,87 The high solid content of slurry is beneficial for maintaining material density, reducing shrinkage rate, and enhancing mechanical strength of bioceramics. Nevertheless, excessive solid content will lead to the slurry too viscous, even the failure of printing. Therefore, it is necessary to explore a suitable solid content that not only ensures excellent spreading ability, but also increases the density and compressive strength of the scaffolds.
Stereolithography
SLA, as another type of vat photopolymerization technology, uses point scanning of UV light and photopolymerization reaction to solidify slurry. Monomers in the slurry are UV-active and are converted into polymer chains under UV light. 88 To fabricate bioceramic scaffolds, bioceramic powder needs to be added into the slurry first. Once the photopolymerization reaction occurs, the organic phase will uniformly wrap bioceramic particles in an organic network, and the green bodies of bioceramic scaffolds are established. Furthermore, green bodies need to be sintered under high temperature (>1000°C) to remove organic additives, and improve the density and strength of materials. 89
The implications of different channel shapes, sizes, and curvatures of scaffolds on bone regeneration are still unclear. A recent study fabricated scaffolds with various shapes (circular vs. rectangular), channel sizes (0.3 to 1.5 mm), and curvatures (concave vs. convex). Among them, channel with a round 0.9 mm diameter notably enhances bone formation, while channel shapes exhibit no significant effect on bone regeneration. Moreover, a concave surface is beneficial for bone tissue growth. 15 Another study shows that the pore diameters ranging from 50 to 260 μm are beneficial for bone regeneration. 50 In conclusion, there is no standard for what size of pores can best promote osteogenesis currently. However, most research is inclined that the optimal size ranges from 100 to 1000 μm.
To overcome complications, such as inflammation and ectopic calcification brought by the migration of carbonate apatite granules, Hayashi et al. developed SLA-printed carbonate apatite chains (Fig. 3), which can conform to the defect shape and promote bone regeneration without complications. 90
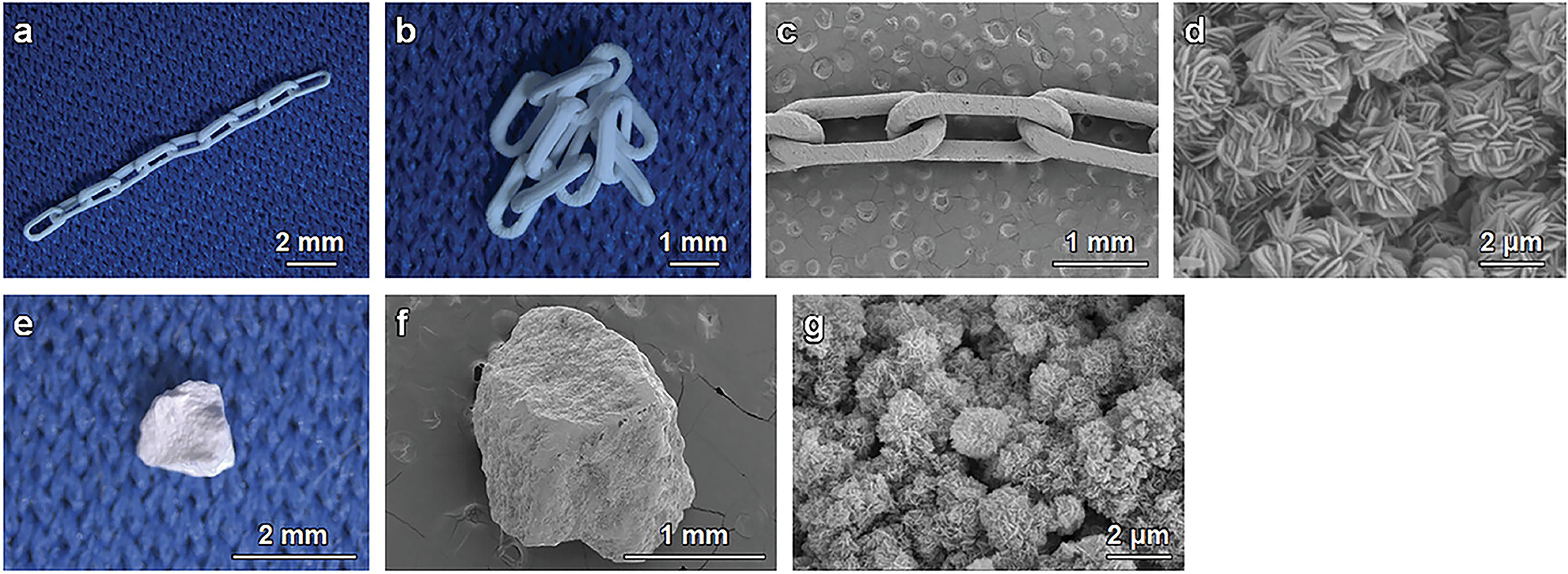
Shapes and structures of granule and stereolithography (SLA)-printed carbonate apatite chain.
SLA technology has the advantages of rapid prototyping and high-precision printing. 91 Nevertheless, the photoinitiators, unreacted monomers, etc. may lead to cytotoxicity and affect the synthesis of bone matrix. Therefore, further processing procedures are needed to remove the above toxic substances, such as soaked in deionized water and sintering.
Fused deposition modeling
FDM, as one type of material extrusion technology, uses a nozzle to extrude molten filament onto platform. After that, 3D structures are produced by stacking materials layer by layer. 92 FDM technology allows for rapid preparation of scaffolds with complex geometries, and has been used for printing multiple-component materials, such as metals, ceramics, and polymers. 93
FDM printing technology heavily relies on material filaments. To fabricate ceramic scaffolds based on FDM, the first step is to synthesize filaments containing ceramic components. Recently, FDM-printed scaffolds derived from calcium-deficient HA/PVA filaments, 94 and PLA/HA filaments 95 have exhibited excellent biocompatibility and osteogenic activity. In addition, there is also a study attempting to combine FDM with DLP technology to produce ceramic scaffolds with special structures, which undoubtedly extends the application scope of FDM ceramic printing. 96
To conclude, the advantages of FDM mainly reflect in low cost, simple operation, and the ability to produce complex structures. 97 However, FDM printing relies on the preparation of filaments, and the composition of filaments determines the composition and function of printed scaffolds. Therefore, it is necessary to develop bioceramic filaments with excellent properties.
Direct ink writing
DIW, as another kind of material extrusion technology, extrudes precursor ink according to the designed paths, constructing 3D structures in the form of “line-lay-body.” The precursor ink, with the character of shear thinning, needs to have a certain storage modulus (G’’) and loss modulus (G’) to achieve excellent rheological properties. 98
Inspired by spicules of the marine sponge Euplectella aspergillum, Yang et al. prepared flexible bioceramic scaffolds based on DIW, which can be compressed, folded, rolled, twisted, and cut adaptably without the occurrence of fracture. 99 By polymer dissolving in acetone (15% w/v), another research prepared PLA/β-TCP scaffolds, which exhibit shape memory effect and can be applied for some special bone repair environments. 100 In addition, it has been reported that silk fibroin/gelatin mixed with xonotlite (Ca6(Si6O17) (OH)2) nanofiber can be printed into scaffold via DIW (Fig. 4), and the scaffold exhibits excellent bioactivity and mechanical properties. 74 Channels in scaffolds facilitate the transport of nutrient and metabolites, DIW printing can produce hollow-strut scaffolds with diverse cross-sectional channels by extruding slurry from customized nozzles. 101 In summary, compared with photopolymerization that requires chemical reactions, DIW produces 3D structures through extrusion, which has stronger compatibility with various types of materials. Therefore, DIW-printed structures are more complex and have better properties.
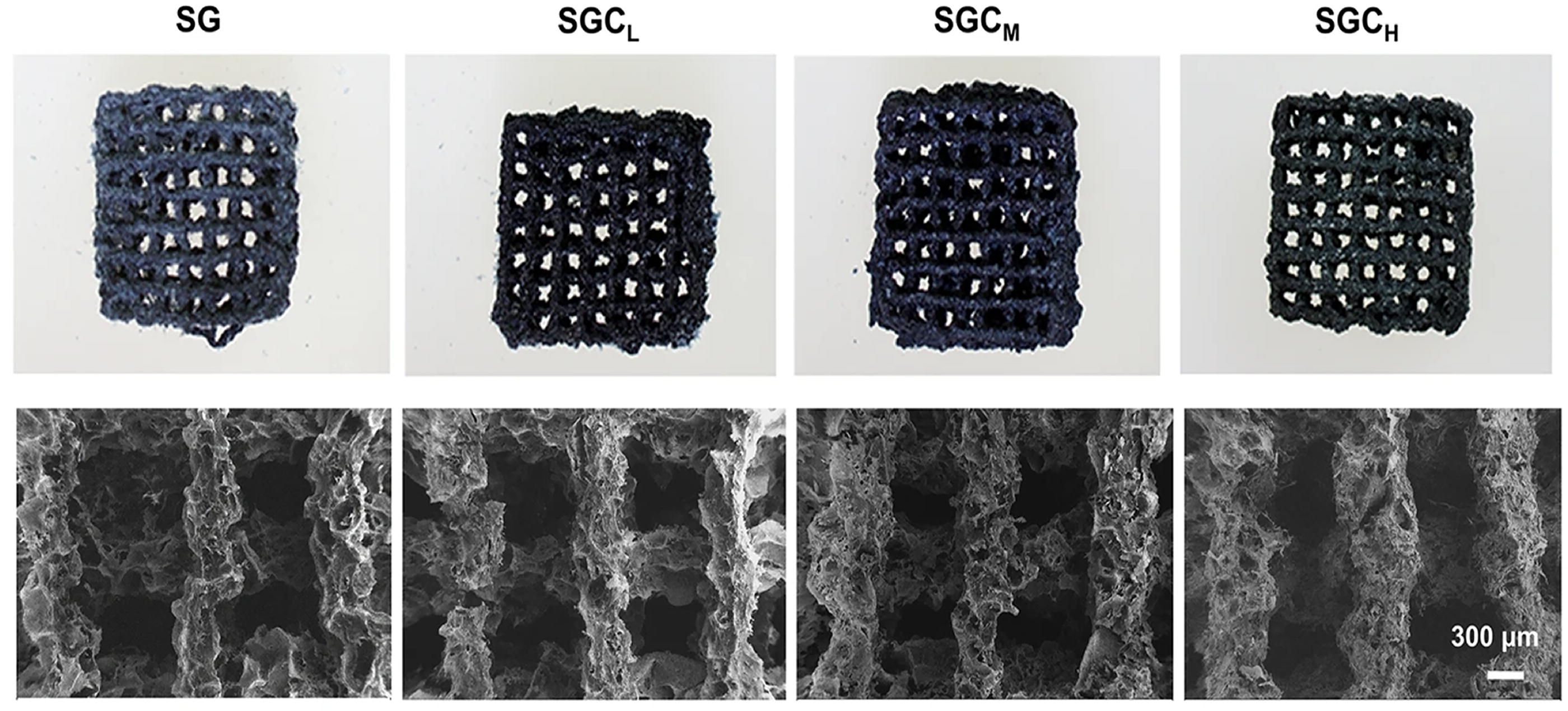
Images of macrography and SEM for four direct ink writing (DIW)-printed scaffolds with different proportions of xonotlite nanofiber. Reproduced with permission. 74 Copyright 2024, The Author(s).
Recently, it has been reported that DIW is used to print bioceramic scaffolds in the hydrogel, which utilizes fewer support structures while saving postprocessing time. In addition, scaffolds printed in the sanitizer bath can significantly promote cell growth and osteogenesis.102,103 Undoubtedly, DIW floating printing provides a new idea for the construction of complex and oblique structures.
DIW has the advantages of high-speed printing and a low requirement for precursor ink components. 104 By introducing binder into precursor ink, bioceramic slurry with high powder content and viscoelasticity can maintain an excellent shape after extrusion. However, DIW-printed bioceramic scaffolds still require solidification and sintering to ensure the scaffolds have a certain mechanical strength.
Selective laser sintering
SLS, as a kind of powder bed fusion technology, uses powder to fabricate 3D structures layer by layer, which is ideal for raw materials with low melting points, such as polymers. 105 With the uninterned powder supporting each layer, SLS printing does not need supporting materials or separate feeders when preparing complex structures, which significantly reduces the usage of raw materials and saves postprocessing time. 106
Ceramics are often combined with synthetic polymers for SLS printing. For example, Feng et al. prepared the composite powder including polydopamine, nano-HA, and PCL, and the printed scaffold derived from the composite powder exhibits excellent tensile and compressive strength, as well as accelerating the formation of apatite layers and promoting adhesion, proliferation, and differentiation of cells. 107 In addition, PVA has a high melting point and crystallinity, which cannot be used for SLS printing. The research by Li et al. indicated that destroying the strong hydrogen bonds of PVA can endow PVA/HA powder with SLS printing property. 108 In conclusion, due to the high melting point of bioceramic powder, the research on SLS bioceramic printing is very limited, and bioceramic powder is commonly mixed with polymer materials as an additive in SLS printing.
Inkjet printing
IJP, as a kind of material jetting technology, sprays ink onto the surface of paper or plastic, manufacturing 3D-printed structures in the form of “points-lines-layers.” IJP includes two modes, continuous mode and drop on demand (DOD) mode. DOD mode adopts piezoelectric effect to control ink extrusion, which has the advantages of accurate droplet controlling and positioning. Based on IJP, Mostofizadeh et al. developed the photocurable and biodegradable phosphoramide-based hydrogel scaffolds added with nano-HA. After the degradation of the hydrogel, phosphates can be produced and exert the effect of promoting osteogenesis. 109
Currently, the application of IJP in bioceramic printing is also limited, and there are some issues that need attention. First, the rheological properties of bioceramic ink are key factors for evaluating whether the ink can be used for high-precision printing. Excessive or insufficient viscosity may lead to the failure of printing. 110 Second, the ink needs to maintain an appropriate pH value to prevent the corrosion of the spray system. Third, the mechanical strength of the printed structure is poor. Last, compared with other printing technologies such as DIW and SLA, IJP has a lower printing accuracy. 111
Bioprinting
Bioprinting can fabricate complex structures containing biomaterials, cells, and bioactive molecules, which has attracted the interest of researchers recently. 112 When tissues are damaged due to trauma, chemical, or radiation exposure, bioprinting has the potential to fabricate personalized organoids and solve the problem of donor tissue shortage. 3D bioprinting strategies include the forms of inkjet, laser, and extrusion. Among them, extrusion-based bioprinting is widely used, considering that extrusion printing technologies are suitable for multimaterial printing. 113
Based on decellularized extracellular matrix, HA, and human adipose stem cells, Kim et al. used DIW technology to fabricate engineered tendon-to-bone tissue with biologically graded interface. 114 In addition, there is also a study developing a biomimetic scaffold, which includes Mo-containing silicate bioceramic power and tendon/bone-related cells (Fig. 5). The biomimetic scaffold can induce tenogenic and osteogenic differentiation, while enhancing the regeneration of tendon-to-bone interfaces in animal experiments. 115
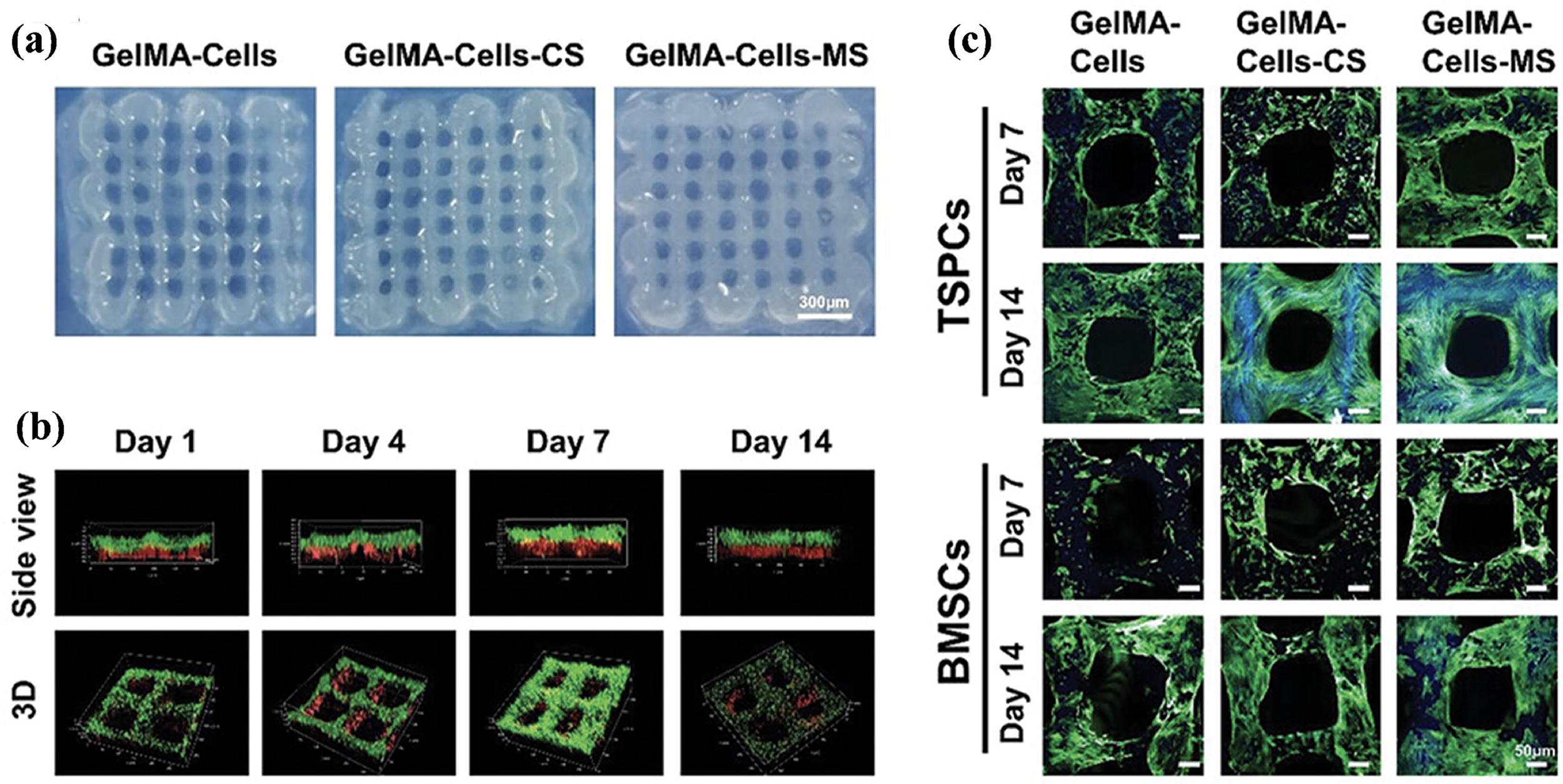
Characterization of bioprinted scaffolds containing both tendon stem/progenitor cell (TSPCs) and bone marrow mesenchymal stem cells (BMSCs).
To enhance the mechanical strength of cell-laden hydrogel, Machour et al. used a novel thermosensitive ink to coprint with cell-laden hydrogel, and the thermosensitive ink can be sintered to form a porous, stiff scaffold at 37°C, which enhances the strength of hydrogel scaffold. 116 In addition, it has been reported that with the addition of PCL and nHA, a biomimetic scaffold composed of alginate, nHA-collagen, and human dental pulp stem/stromal cells can obtain excellent mechanical strength. 117 To conclude, synthetic polymer can improve the mechanical properties of bioprinted scaffold.
The regeneration of blood vessels and nerves is crucial for bone regeneration. Qin et al. constructed a prevascularization scaffold based on bioprinting technology, which is composed of Li-Mg-Si bioceramics, gelatin methacryloyl (GelMA), and human umbilical vein endothelial cell. The results indicated that the new scaffold has durable angiogenic capability, whether in in vitro or in vivo experiments. What is more, by releasing bioactive ions, the scaffold can promote osteogenic differentiation of MSCs and neurogenic differentiation of neurons. 118
In addition, it has been reported that the collagen/HA scaffold derived from whipped bioink has high porosity and cell-laden ability. In vitro experiments showed that the porous scaffold significantly enhances the osteogenic and angiogenic activity of cells. 119 Wollastonite, mainly containing CaSiO3, has the properties of osteoconductivity and mechanical resistance, a promising bone repair material. 120 Kotlarz et al. prepared apatite–wollastonite bioceramic scaffolds based on binder jet printing technology. After that, they delivered cell-laden hydrogel on the surface of the scaffold. The results showed that with the deposition of hydrogel, cells can penetrate the porous structure and achieve in situ seeding. 121 To conclude, bioprinting can premix bioactive components such as cells into a slurry, which ensures the biological activity of implants, as well as achieving personalized fabrication. Compared with pure material printing, bioprinting can save time for cell migration into the implant, further achieving vascularization and osseointegration of the implant in a shorter time.
Bioprinting is becoming an ideal option for fabricating biomimetic scaffolds. However, bioinks need to simultaneously satisfy printability, cell biocompatibility, and adequate mechanical strength, which existing materials struggle to fully meet. 122 In addition, the high costs of research and development limit its widespread application currently. Finally, bioprinted organoids may not fully replicate the function of native organs and the existing risks of abnormal cell proliferation.
Clinical Application of Bioceramics in Bone Regeneration
With the advancement of 3D printing technology, 3D-printed bioceramics are gradually entering orthopedics and oral and maxillofacial surgery. For example, a 3D-printed cage composed of PCL and β-TCP in a mass ratio of 1:1 has excellent biodegradability and mechanical strength. Liu et al. used the novel cage to conduct a prospective clinical trial in 22 patients undergoing lumbar interbody fusion. The 12-month follow-up showed that the application of biodegradable PCL/β-TCP cages yields satisfactory results, and the JOABPEQ and visual analogue scale scores are notably improved. 123 To reveal the safety and efficacy of 3D-printed PCL/HA scaffolds in cranioplasty surgeries, Babaei et al. selected three clinical cases to carry out a phase 1 clinical trial. The result indicated that the sterilized PCL/HA composite is safe for patients, having the potential to be a substitute for autologous bone in craniomaxillofacial surgery. 124 In addition, Ca-Si-based bioceramics are frequently applied for endodontic treatment. For example, Wang et al. fabricated a novel material composed of CaO, SiO2, P2O5, and MgO, which can guide bone regeneration and maintain bone volume stability for half a year postgrafting. 125
Although the application of bioceramic materials in orthopedics and oral and maxillofacial surgery is extensive, there still exist some problems. First, the complexity of operation and potential iatrogenic neurovascular injuries. Second, some complications correlated with degradability, such as implant breakage, damage from degraded debris entering the joint cavity, without the growth of new bone in the residual cavity after implant degradation. Third, inflammatory reactions. Finally, further follow-up is required to reveal long-term therapeutic effects.
Conclusion
3D printing is a promising method to fabricate personalized scaffolds for critical-sized bone defects, which can realize the reconstruction of complex anatomical shapes. At present, researchers are searching for the optimum fabrication parameters for bioceramic scaffolds, including porous structures, porous sizes, and sintering temperature. Meanwhile, by surface functional modification and other ingredients adding, bioceramic-based scaffolds can obtain better performance in mechanical properties, degradability, osteoinduction, and osteoconduction, as well as antitumor, antibacterial, etc.
This review elucidates various bioceramic materials and their applications in bone reconstruction. What is more, 3D printing technologies can prepare personalized bioceramic implants with promising mechanical and biological properties. Although significant advancements have been made in the field of bone repair, some issues still need to be solved.
Mechanical properties: It is difficult for current technologies to produce high-strength, tough, and scalable bioceramic scaffolds. By high-temperature sintering, the strength of bioceramics can be improved. However, porous bioceramic scaffolds have native disadvantages of insufficient toughness and scalability, which cause bioceramic scaffolds to not adapt to complex mechanical environments. In the next research, by mimicking the composition and structures of natural materials such as bone and mussels, modifying sintered ceramics through physical impregnation, or borrowing the dislocations strategy,
126
composite bioceramics may gain excellent toughness and scalability. Vascularization challenges: Vascularization of grafts is a critical premise for successful integration and function. After the implantation of pure ceramic scaffolds, it takes plenty of time to achieve vascularization, which impedes the process of bone integration. Bioprinting technology has the potential to fabricate prevascularized bioceramic scaffolds in vitro, which provides a new strategy for accelerating bone regeneration. Multiple functions: In some clinical cases, bone reconstruction and disease treatment need to be carried out simultaneously. For example, killing residual tumor cells is as important as promoting the regeneration of new bone, blood vessels, and nerves.
127
Thus, specific drug-laden bioceramic scaffolds are worth further exploration. Translational barriers: Regulatory approval and requirements for preclinical and clinical validation limit the clinical translation of new products. To solve the above problems, a standardized and simplified protocol for clinical translation of new products needs to be formulated. Meanwhile, strengthening the cooperation between researchers, doctors, regulatory bodies, and companies is crucial. In addition, with the advancement of machine learning and artificial intelligence, the design and function of grafts can be predicted, which will accelerate the clinical translation of new products.
128
Fine printing: The native bone has a highly complex and ordered microstructure. However, the existing bioceramic scaffolds are rarely able to mimic the fine structures. By attempting a different ratio of slurry composition, regulating sintering temperature, integrating electrospinning or laser engraving with 3D printing technologies, etc., fine structures may be achieved in the future.
Authors’ Contributions
Y.Z.: Writing—original draft. D.L.: Writing—review and editing. L.R.: Conceptualization. X.W.: Conceptualization. D.M.: Conceptualization and writing—review and editing.
Footnotes
Funding Information
The authors greatly appreciate the financial support from the Natural Science Foundation of Gansu Province, China (no. 23JRRA543; no. 24JRRA1124), the Clinical Research on Precise Treatment of Maxillofacial Trauma (no. 2021yxky004), the National Key Research and Development Program of China (2022YFB4600101), the National Natural Science Foundation of China (52175201 and 52205228), and the Research Program of Science and Technology Department of Gansu Province (22JR5RA093 and 22JR5RA107).
Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.