
Abstract
Aging is a gradual process leading to the decline of physiological functions across cells, organs, tissues, systems, and the surrounding microenvironment, particularly affecting the musculoskeletal system. Bone aging often presents with osteoporosis and impaired osteogenic niche, thereby increasing fracture risk and decreasing regenerative capacity. Therefore, bone aging and osteoporotic bone defects have become a significant challenge in clinical practice. Tissue-engineered scaffolds are of significant importance in managing osteoporotic bone defects by providing mechanical support, facilitating bone regeneration and repair. They can also serve as a vehicle for drugs or factors for osteoporosis management, thereby enabling localized targeted therapy. The local release of active pharmaceutical agents for the treatment of osteoporosis via biomaterials could serve to reduce the occurrence of systemic side effects, while improving the local aging metabolic microenvironment and immune microenvironment. This review presents a comprehensive discussion of the mechanisms and treatment methods of osteoporosis. The scaffolds used for osteoporotic bone defects are also reviewed. We conducted an in-depth analysis of the impact of diverse preparation techniques and modifications on the osteogenic properties of the scaffolds, and reviewed different materials of drug delivery scaffolds for the repair of osteoporotic bone defects. Finally, we put forward our scientific concept regarding the treatment of bone aging and osteoporotic bone defects. We hope to provide a theoretical basis and research ideas for further in-depth studies on treating osteoporosis and bone aging.
Impact Statement
This review systematically comprehends the pathogenesis and therapeutic strategies of bone aging and osteoporosis-related bone defects, emphasizing the central role of tissue-engineered scaffolds in local drug delivery and microenvironment regulation. High-performance scaffolds can markedly improve the osteogenic niche and stimulate bone repair. This study provides theoretical support for precision therapy in the context of bone aging and is expected to promote the development of this field toward smarter and personalized treatment.
Introduction
Aging is associated with a progressive decline in the physiological functioning of tissues, organs, and cells. This decline is associated with immune composition and signaling within the microenvironment, particularly affecting the musculoskeletal system, which could lead to osteoporosis and make a higher incidence of adverse outcomes in the elderly. 1 The incidence rate of osteoporosis is continuously rising with the aggravation of population aging.2,3 Especially when patients with osteoporosis have bone defects, it will greatly increase the difficulty of bone repair and bring a heavy burden to society and families. 4 The World Health Organization classifies osteoporosis as the second most prevalent chronic disease posing the greatest threat to human health after cardiovascular disorders. 5 However, inadequate disease awareness persists among patients, with a 32% prevalence rate yet only a 7% awareness rate in individuals over 65 years of age. 6 Over the past two decades, the incidence of fractures caused by population aging and osteoporosis has increased by 24%. 7 By 2035, the number of osteoporosis-related fractures and associated treatment costs is projected to double. 8 Bone tissue not only faces the challenge of defects but also inevitably undergoes the process of aging, and bone aging is closely related to bone defects. 9 With the increase in age, the microstructure and physiological functions of bone tissue gradually degenerate, and then osteoporosis occurs. 10 The current therapeutic armamentarium for osteoporosis encompasses medications, physical therapies, and surgical procedures. However, these methods still have certain limitations in treating osteoporotic fractures, such as drug side effects, slow fracture healing, and a high failure rate of internal fixation.11,12 Therefore, finding a safe and effective treatment method to promote bone healing in patients with osteoporosis is the focus of research in recent years.
Tissue-engineered scaffolds have emerged as a new treatment method and have been modified by various means to enhance their osteogenic ability.13,14 Scaffolds can provide mechanical support, promote bone regeneration and repair, and can also carry drugs or bioactive factors for treating osteoporosis to achieve local targeted therapy. 15 With ongoing advances in materials science and biotechnology, the performance and function of bone repair scaffolds have been continuously improved and perfected.16,17 Novel materials and technologies are used to fabricate scaffolds with complex structures, personalized shapes, and diverse functions to better adapt to the bone defects of patients with different degrees of osteoporosis, and to promote bone regeneration while regulating the local immune microenvironment of bone defects.18,19 Herein, we reviewed osteoporosis mechanisms and treatments, summarized scaffold strategies for osteoporotic bone defects, and analyzed current implant materials’ pros and cons, proposing new solutions to guide future material development for osteoporosis and bone aging.
Osteoporosis Mechanism and Treatment
Osteoporosis mechanism
Primary osteoporosis
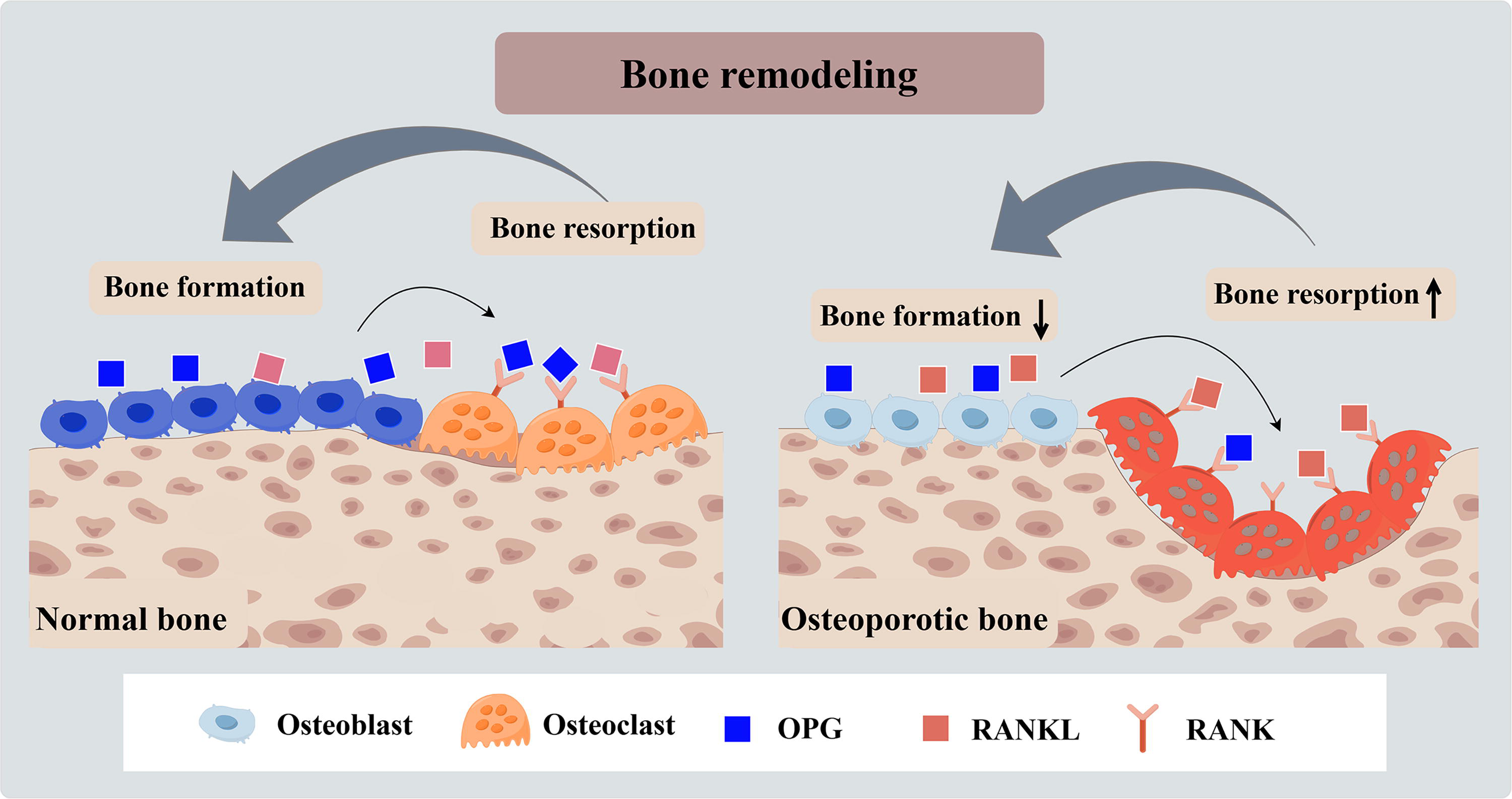
Osteoporosis is a pathological condition that affects bone metabolism, manifested as a long-term reduction in bone mass and an increased susceptibility to fractures. Primary osteoporosis encompasses postmenopausal osteoporosis (type I) and senile osteoporosis (type II). Among them, type I osteoporosis arises from the significant reduction in estrogen following menopause. 20 Type II, namely senile osteoporosis, is the outcome of the combined action of multiple factors.21–23 In normal bone matrix, osteoblast-released OPG (Osteoprotegerin) binds to RANK (Receptor Activator of Nuclear Factor-κB) of osteoclasts more than RANKL (Receptor Activatorof Nuclear Factor-κB Ligand).24,25 However, in the bone matrix of osteoporosis, the binding of RANKL to RANK is greater than that of OPG, leading to enhanced osteoclast activity and increased bone resorption (Fig. 1). 26
The mechanism of osteoporosis and the mechanism of bone remodeling.
Secondary osteoporosis
Secondary osteoporosis is due to atypical bone remodeling caused by a variety of diseases. 27 It is characterized by an increased bone turnover rate and decreased osteogenic activity, ultimately leading to bone loss and microstructural degeneration. Figure 2 showed the process of bone remodeling in normal and osteoporotic conditions. Patients with hyperthyroidism, Cushing’s syndrome, and diabetes have varying degrees of osteoporosis.28,29 Glucocorticoids, antiepileptic drugs, etc., interfere with bone metabolism through different pathways, resulting in bone mass loss.30,31
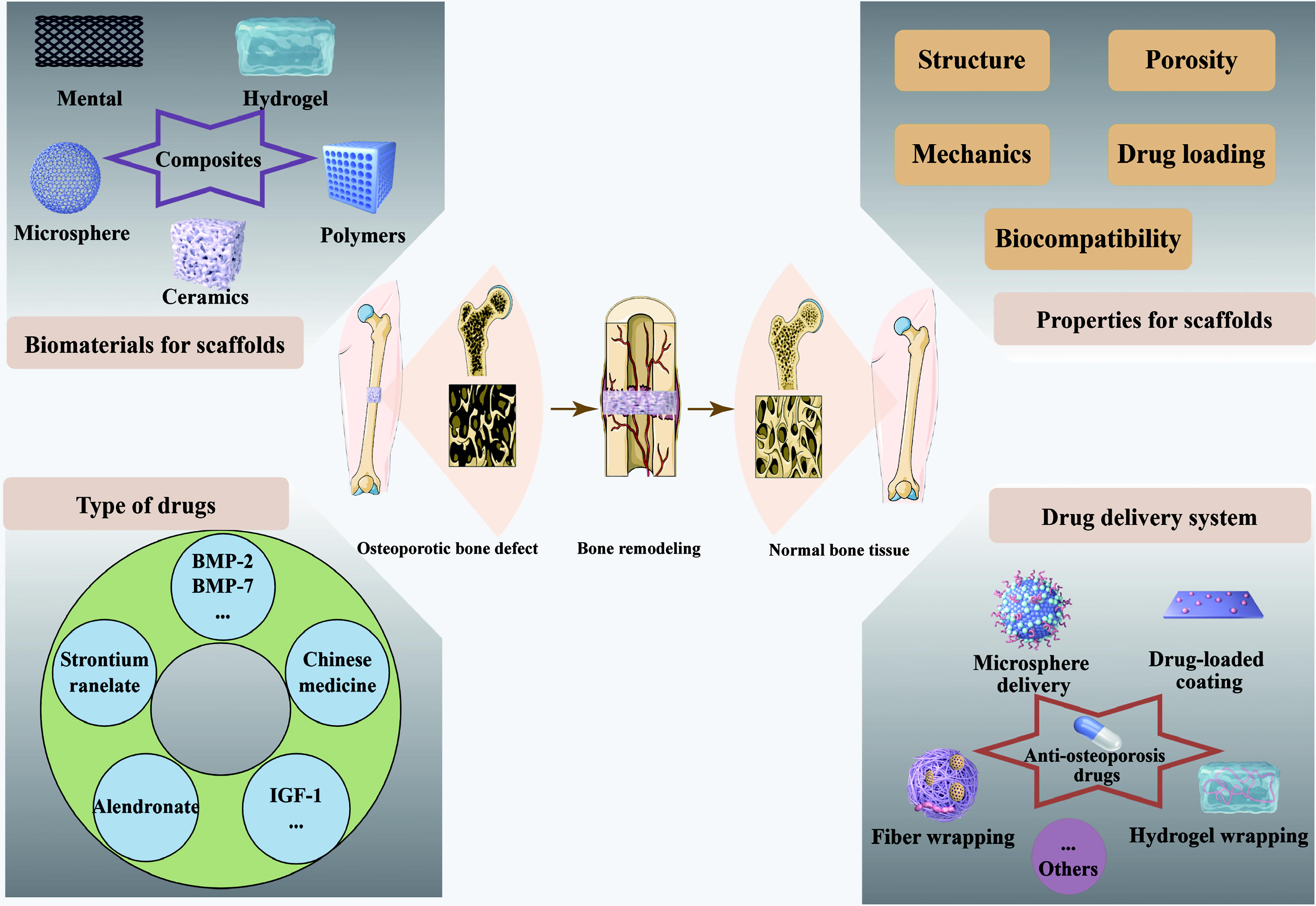
Schematic diagram of bone defect repair by bioactive scaffolds of various materials and preparation methods.
Drug treatment for osteoporosis
The therapeutic drugs are mainly classified into two categories: antiresorptive drugs and anabolic drugs, which play different roles in the treatment of osteoporosis. 32
Antibone resorption drugs
Antiresorptive drugs aim to reduce bone resorption, thereby maintaining or increasing bone mass. Raloxifene is a selective estrogen receptor modulator. By regulating estrogen receptor activity, it shows estrogen-like effects in some tissues, inhibits osteoclast activity, and reduces bone resorption. 33 Bisphosphonates are commonly used antiosteoporosis drugs in clinical practice. They can tightly bind to the bone surface and inhibit the function of osteoclasts, significantly reducing bone turnover and bone loss. Salmon calcitonin can reduce bone resorption by inhibiting the activity and number of osteoclasts. 34 Furthermore, it has been shown to possess analgesic properties, which supports its use as an adjunctive therapy for the management of osteoporosis-related bone pain. By binding soluble and membrane-bound RANKL, denosumab precludes RANK activation on osteoclast-lineage cells, thereby reducing osteoclast formation, functional activity, and longevity, with consequent suppression of bone resorption. 35
Anabolic drugs for bone
Anabolic drugs mainly serve to promote bone formation and increase bone mass. Parathyroid hormone (PTH) and its analogue teriparatide can directly stimulate the activity and proliferation of osteoblasts, facilitating bone formation and increasing bone density.36,37 Abaloparatide is a synthetic PTH-related protein analog that selectively activates the Gsα/cAMP signaling pathway downstream of the PTH1 receptor to promote bone formation while avoiding excessive bone resorption. 38 Bone morphogenetic proteins have the ability to induce osteoblast differentiation and promote the formation of new bone. Strontium ranelate (Sr) has a dual-action mechanism. It can not only promote the proliferation and differentiation of osteoblasts and increase bone formation but also inhibit osteoclast activity and reduce bone resorption.39,40 Also, Romosozumab is a monoclonal antibody that targets osteosclerotic proteins. It promotes therapeutic effects and new bone formation via Wnt/β-catenin activation, and concomitantly reduces RANKL expression, thereby suppressing osteoclast-driven bone loss. 41
Drug delivery systems
For better efficacy and safety, the drug must be delivered to the target bone tissue in an appropriate amount, and the blood drug concentration does not cause systemic toxicity. 42 The effectiveness of the drug can be improved by using various drug delivery systems. Among them, the scaffolds enable the appropriate drug activity to play a role at a specific site while repairing bone defects. 43 In addition to the performance of a simple bioactive scaffold, the conditions that an ideal drug delivery scaffold needs to meet should also include the uniform distribution of the drug on the surface and inside the scaffold, and the appropriate binding force between the drug and the scaffold, thereby enabling targeted, rate-controlled drug release.
Scaffolds for Osteoporotic Bone Defect Repair
Performance regulation of bioactive scaffolds
Material optimization for bone repair scaffolds
To address the clinical challenge of repairing bone defects, extensive research has been conducted on fabricated scaffolds based on metals, ceramics, bioactive glasses, natural/synthetic polymers, and composite systems. 15 Metals has strong mechanical stability; however, there are certain deficiencies in their application, such as nondegradability, whereas an inert surface limits tissue bonding and remodeling at the interface. Bioactive glasses have strong biocompatibility. However, they have high brittleness and are prone to fracture in the early stage of implantation. Polymer materials are usually biodegradable and can be prepared through a variety of processes. However, their degradation rate is usually uncontrollable, and the degradation products will also have an adverse impact on the microenvironment. Table 1 showed a comparative analysis of different biomaterials used for osteoporotic bone defects. Sufficient cells are required to properly fill the scaffold and produce a long-lasting bone extracellular matrix. Degradation behavior is largely controlled by scaffold composition and pore morphology. The degradation rate should be synchronized with the in vivo progression of new-tissue development after implantation. 44
Comparative Analysis of Biomaterial Scaffolds for Osteoporotic Bone Defects
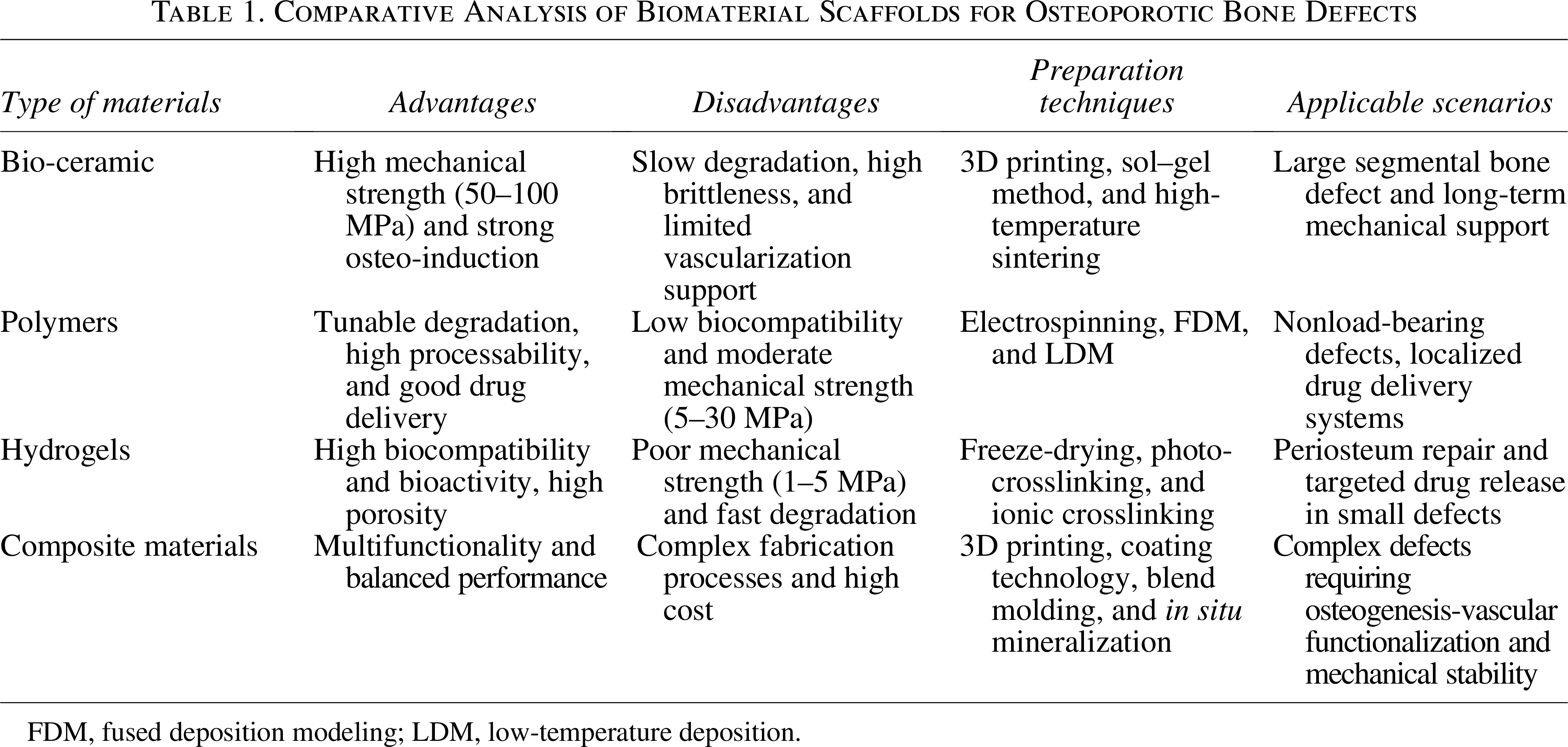
FDM, fused deposition modeling; LDM, low-temperature deposition.
Enhancement of bone repair scaffold structures
The characteristics of scaffolds’ structure are a direct regulator in shaping the interactions between the scaffold and immune cells. With precision additive manufacturing, structures can be engineered to regulate bone-aging processes and immune activity. Ordered designs increase immune-cell adhesion and motility and modulate macrophage phenotypes to refine the immune response.45,46 Optimizing the scaffolds’ pore diameter and overall porosity can also modulate immune responses. In particular, pore-scale architecture governs macrophage infiltration, adhesion, and phenotypic polarization, thereby influencing the tissue repair and immunoregulation. 47 The study fabricated pore sizes of 209.9 ± 77.1 μm (P200), 385.5 ± 28.6 μm (P400), and 582.1 ± 27.2 μm (P600). Among these, the P600 architecture significantly enhanced M2 polarization, vascularization, and new bone formation.
Enhancement of osteogenic activity of bone repair scaffolds
Incorporating bioactive factors has emerged as a prominent strategy for age-related bone repair and osteo-immunomodulation. Such constructs can attenuate excessive inflammatory signaling and bias macrophage polarization toward proresolving, reparative phenotypes, thereby fostering a regeneration-permissive microenvironment. In parallel, deliberate control of immune-cell spatial organization within the construct can further augment immunoregulatory efficacy.48,49 Some modified methods are used to promote osteogenic differentiation of the scaffold for osteoporotic bone defects.50,51 Among them, the calcium phosphate scaffold has shown the ability to enhance osteogenic potential and bone integration due to its surface charge, and chemical and morphological characteristics. In addition, many methods using osteogenic-inducing scaffolds and grafts have been studied, aiming to improve the regenerative outcomes by driving osteogenic differentiation.52,53 The study demonstrated that gelatin scaffolds incorporating 7.5% (m/v) ceramic compound showed an elevated Young’s modulus and afforded prolonged bone morphogenetic protein-2 (BMP-2) release kinetics with a comparatively lower growth factor dosage (600 ng/scaffold).
Drug delivery system
Bio-ceramic materials
Bio-ceramic materials can be used for porous scaffold implantation in bone defects and bone-filling powder to boost bone regeneration. Bio-ceramics are classified into absorbable ceramics like calcium phosphate and calcium sulfate, as well as inert bioactive glasses such as zirconia. Typical applications of bio-ceramic scaffolds for osteoporotic bone defect repair are shown in Table 2. Due to the strong biocompatibility, bioactivity, osteo-conduction, and osteo-induction capabilities of calcium phosphate, along with its nontoxicity and low immunogenicity, calcium-phosphate bio-ceramics are frequently fabricated as coatings for bone fillers and prostheses. 54
Bio-Ceramic Scaffolds for Osteoporotic Bone Defect Repair
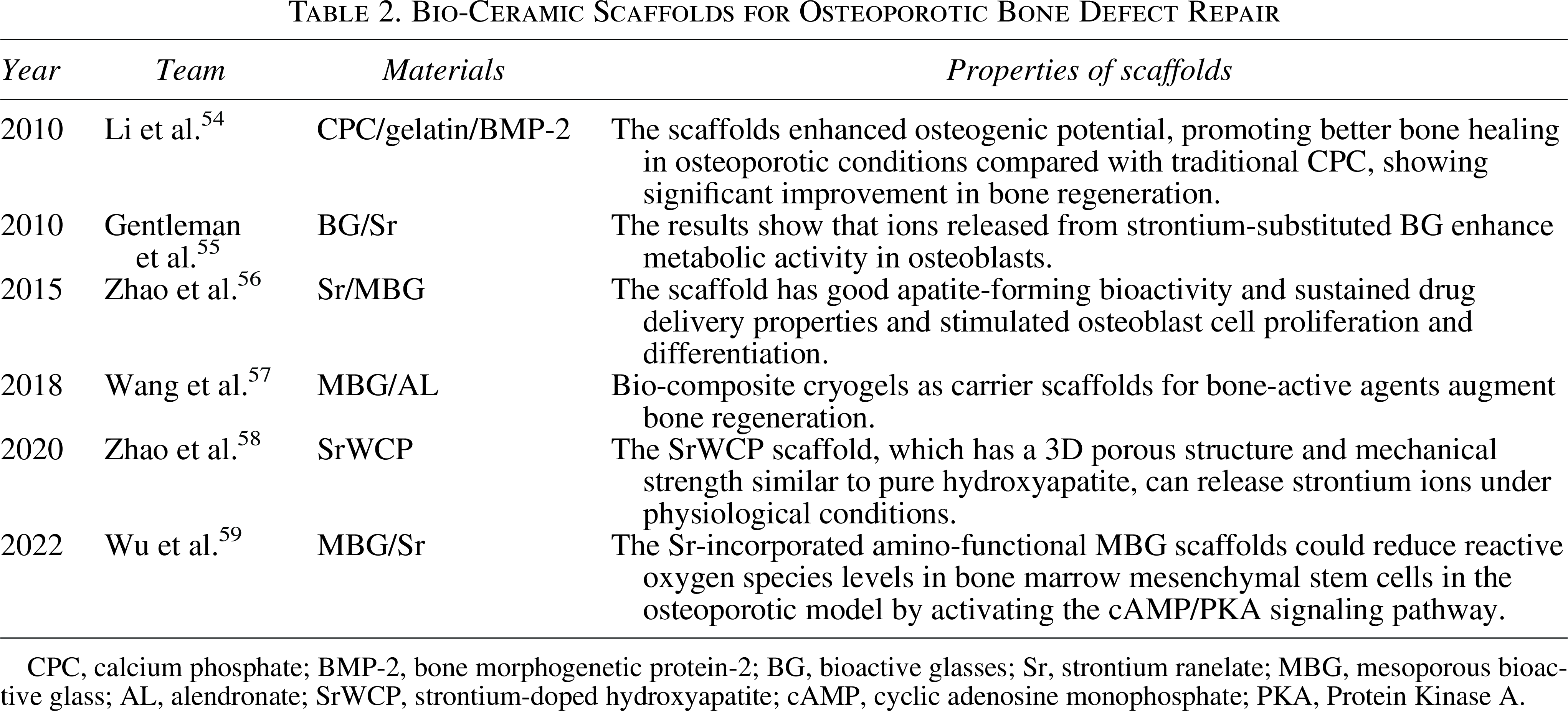
CPC, calcium phosphate; BMP-2, bone morphogenetic protein-2; BG, bioactive glasses; Sr, strontium ranelate; MBG, mesoporous bioactive glass; AL, alendronate; SrWCP, strontium-doped hydroxyapatite; cAMP, cyclic adenosine monophosphate; PKA, Protein Kinase A.
Sr-substituted nanohybrid scaffolds composited of HA and chitosan significantly elevated alkaline phosphatase (ALP) activity, promoted mineralization of the extracellular matrix, and enhanced osteo-inductivity. 60 The Sr-substituted calcium phosphate scaffold exhibited better performance in promoting bone healing than the HA scaffold alone through the corelease of strontium and calcium ions. 55 Zhao et al. successfully fabricated Sr-doped HA bio-ceramic scaffolds by the hydrothermal method (Fig. 3B). 58 At 8 and 12 weeks, serum Sr concentrations in animals receiving the Sr-incorporated bio-ceramic scaffolds were undetectable and comparable with the normal. In contrast, the Sr-Ran group exhibited serum Sr concentrations 22- and 8-fold higher than normal levels at these respective time points. Under physiological conditions, the resulting structure presents a three-dimensional porous morphology, has appropriate mechanical strength, and can slowly release Sr ions. 63
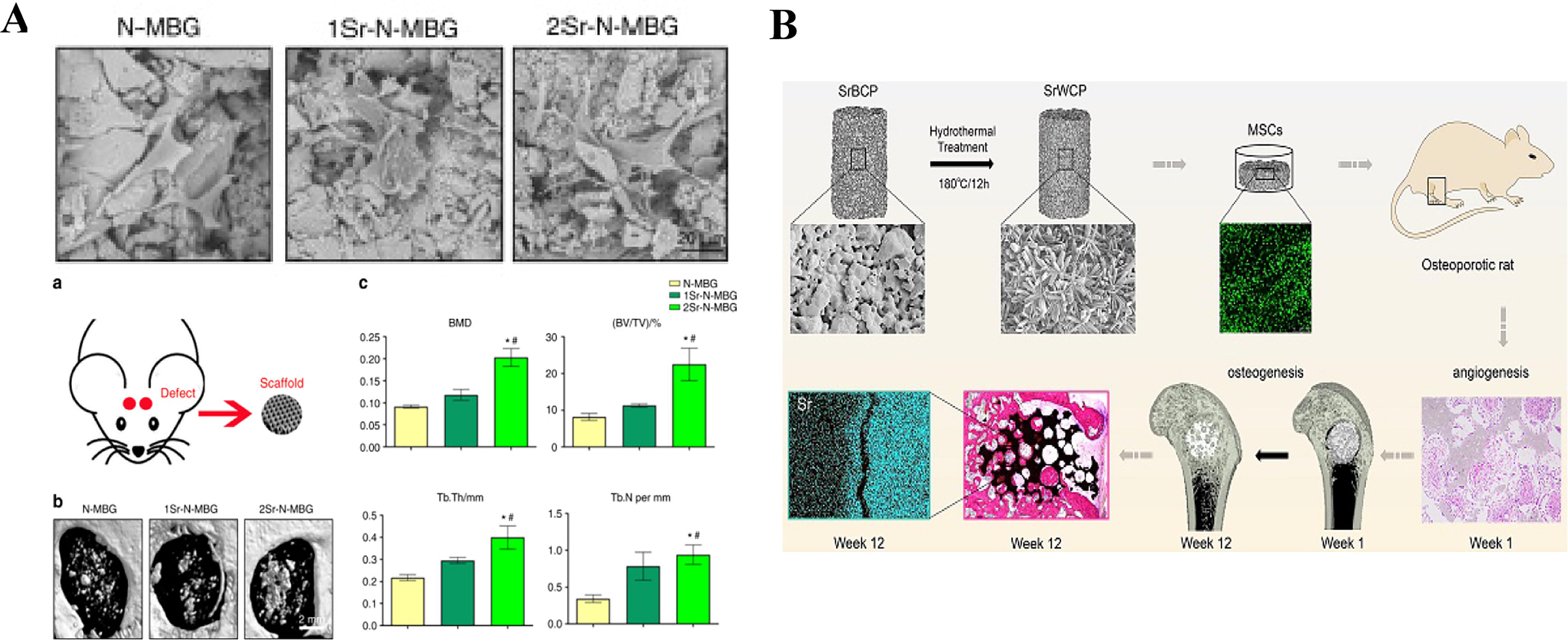
Mesoporous bioactive glass has a remarkable ability for fabricating strategies and therapeutic delivery. Its orderly mesoporous arrangement, appropriate pore size distribution, and high specific surface area confer superior loading and delivery of drugs, genes, and growth factors. Sr-doped mesoporous bioactive glass scaffolds demonstrated a strong osteogenic ability, which could assist in microvascularization in bone defect areas (Fig. 3A). 59 The osteogenic differentiation was enhanced by the optimization of the structure and the drug delivery system.56,57 Terzopoulou et al. successfully prepared Sr-substituted mesoporous bioglass (SiO2–SrO–P2O5) and loaded the antiosteoporosis drug ibandronate. 62
Polymer materials
Scaffolds fabricated from polymer materials possess good research value and application prospects in bone formation and drug delivery for the well biodegradability and processability. Nevertheless, polymer materials are generally poorly hydrophilic and require modification or compounding with other materials to enhance their biocompatibility. Typical applications of bio-ceramic scaffolds for osteoporotic bone defect repair are shown in Table 3.
Polymer Scaffolds for Osteoporotic Bone Defect Repair
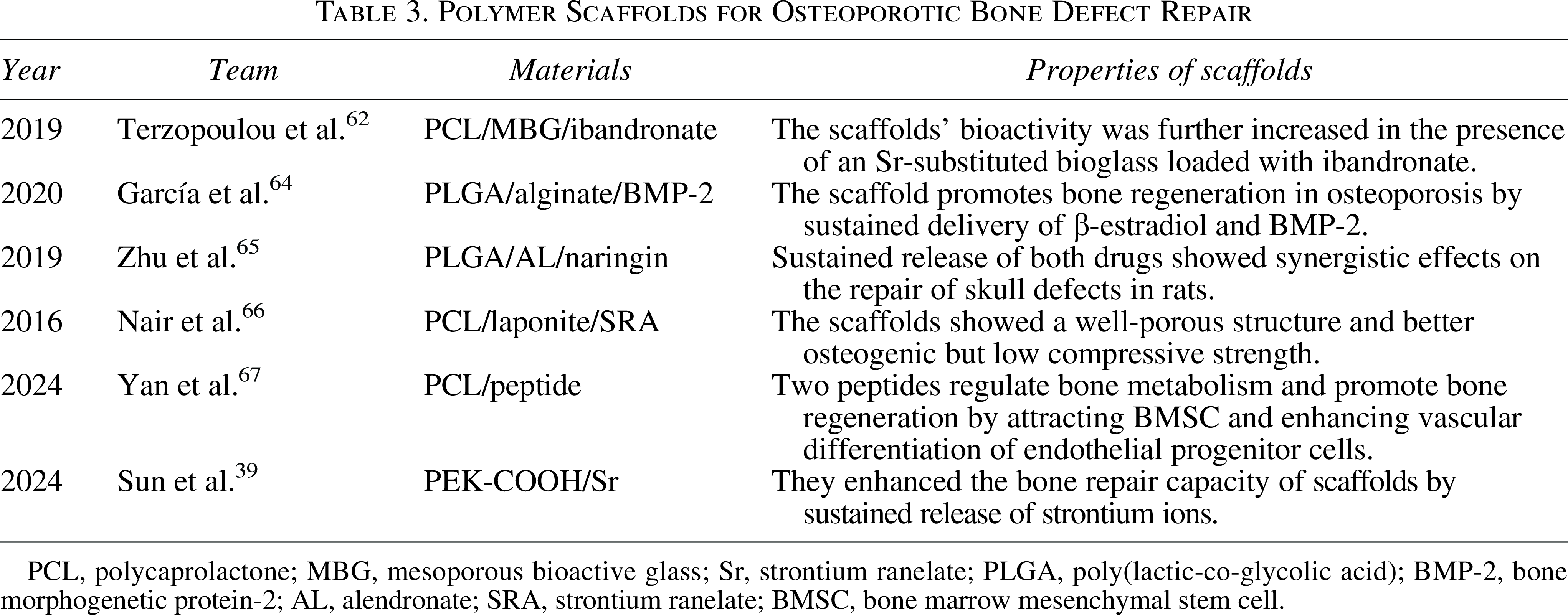
PCL, polycaprolactone; MBG, mesoporous bioactive glass; Sr, strontium ranelate; PLGA, poly(lactic-co-glycolic acid); BMP-2, bone morphogenetic protein-2; AL, alendronate; SRA, strontium ranelate; BMSC, bone marrow mesenchymal stem cell.
Poly(lactic-co-glycolic acid) (PLGA) material, noted for excellent biocompatibility, is extensively employed in bone scaffolds, with controllable degradability and mechanical properties, supporting effective bone regeneration and repair, making it ideal for bone repair applications. PLGA scaffolds coated with gelatin and PLGA-alginate hydrogel membrane incorporated with BMP-2 were fabricated to enhance mechanical strength and hydrophilicity, as well as the synergistic effect in bone repair.64,65 Compared with injectable hydrogels, gelatin sponges demonstrated 30% higher porosity, more than double the water absorption capacity, and a 30% increase in bone regeneration efficacy.
Polycaprolactone (PCL) is another widely used polymer for fabricating scaffolds. As the scaffold degrades, Laponite and Sr are released from PCL scaffolds in a timely sequence and play a dual role in osteoporotic bone regeneration, inducing osteogenic differentiation. 66 Yun et al. utilized electrospinning to construct a PCL nanofiber scaffold containing Aln, which can increase ALP activity and calcium deposition and promote osteogenic genes. 61 Then, the capacity of scaffolds to promote the regeneration of new bone was studied in a rat calvarial defect model. Yan et al. fabricated 3D-printed PCL scaffolds modified with EPLQLKM and SVVYGLR peptides based on the theory of “vascularization-bone metabolism,” which led to the up-regulation of osteoblast-related genes (Fig. 4A). 67 Moreover, functional microvascular regeneration and new bone tissue formation were achieved in femoral-condyle defects in osteoporotic Sprague-Dawley rats.
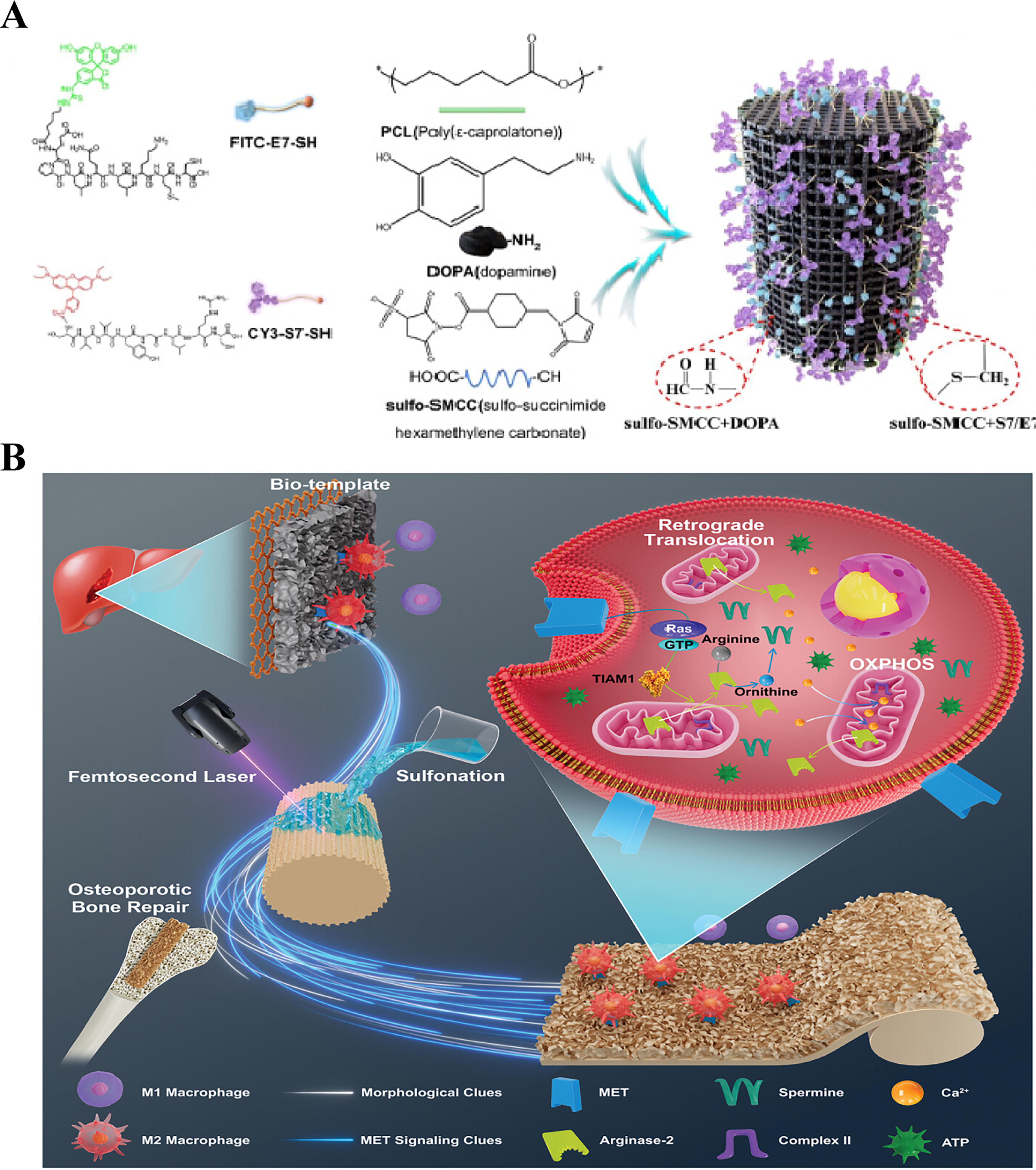
Polyetherketone material is applied in bone tissue engineering scaffolds due to its outstanding mechanical strength, biocompatibility, and stability, providing durable support for bone regeneration and making it well-suited for load-bearing bone repair applications. Gu et al. fabricated a bionic morphology on polyetherketone ketone scaffolds by femtosecond-laser patterning with post-sulfonation (Fig. 4B). 70 The morphology replicated Methionine signaling in macrophages, leading to positive immunomodulation and optimized osteogenesis. This study was inspired by the rapid regeneration of the liver and provides a novel bionic scaffold that can mimic regenerative signals, offering new possibilities for the repair of osteoporotic bone defects. In previous studies, our collaborative team synthesized an amorphous polyaryletherketone with carboxyl groups (PAEK-COOH). 18 They used low-temperature 3D printing technology to prepare scaffolds, in which the scaffolds featured hierarchically controlled porosity and induced in vivo osteogenesis. Under identical porosity conditions, PEK scaffolds fabricated via low-temperature printing exhibited superior mechanical properties (6.15 ± 0.45 MPa) compared with conventional PLGA or hydrogel scaffolds. Subsequently, our team loaded a strontium-doped biomimetic mineralized coating on the surface of the low-temperature printed PEK-COOH scaffold, with the objective of enhancing the osteogenic ability of the scaffold through the slow release of strontium ions. 39
The local delivery of BMSCs has also become a research strategy for healing osteoporotic fractures, and scaffolds loaded with osteoinductive BMSCs significantly induce the in vivo osteogenesis.71,72 Nevertheless, BMSCs encapsulated in PLGA/type I collagen microspheres promoted greater trabecular bone regeneration in ovariectomized rats than BMSCs alone. 71
Hydrogels
A wide array of hydrogels have been engineered for bone tissue applications, including natural matrices and synthetic counterparts. They have abundant chemical groups on their surfaces and are commonly utilized as materials for bone scaffolds and the development of delivery systems. 73 Typical uses of hydrogel scaffolds for bone repair are shown in Table 4.
Hydrogel Scaffolds for Osteoporotic Bone Defect Repair
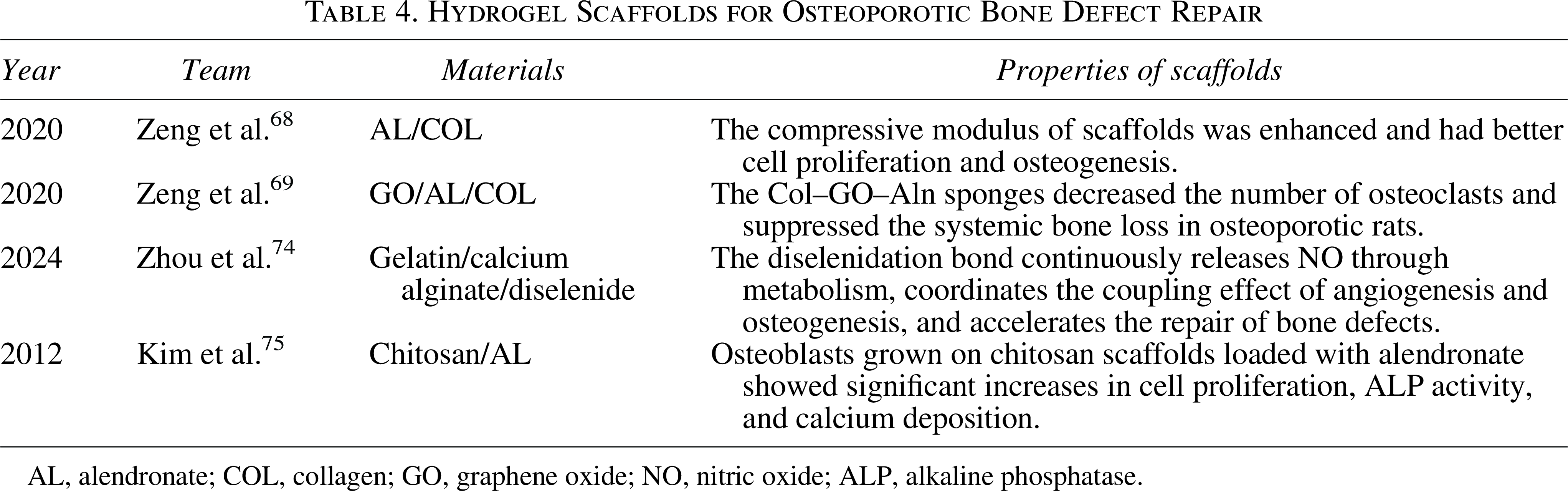
AL, alendronate; COL, collagen; GO, graphene oxide; NO, nitric oxide; ALP, alkaline phosphatase.
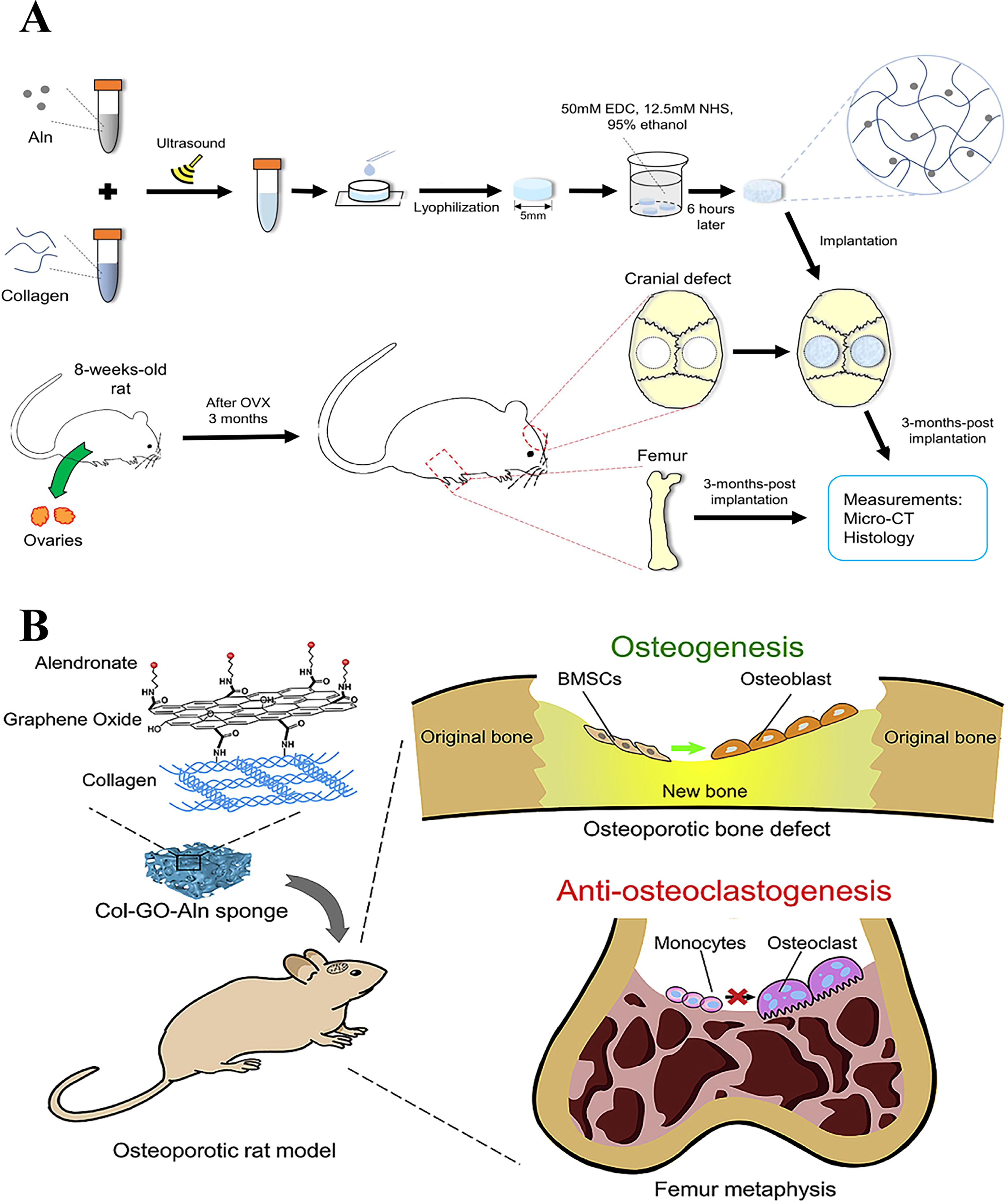
The composite tissue engineering scaffolds loaded with Aln in hydrogel are a common methodology for bone repair. Zeng et al. prepared a collagen–Aln composite engineered scaffold with the sustainable release of Aln (Fig. 5A). 68 It can sustainably release Aln to increase the osteogenic differentiation level of BMSCs. Therefore, this collagen scaffold capable of the continuous delivery of Aln can be used as an effective alternative bone repair material for 5 mm cranial defects in ovariectomized rats. Subsequently, their team prepared a graphene-oxide-modified hydrogel scaffold loaded with Aln, which could inhibit systemic bone loss (Fig. 5B). 69 The results indicated that defect sites filled with gelatin sponges containing 0.05% GO yielded nearly three times the new bone volume observed in the control group. The dual-network scaffold with diselenide bonds enables sustained nitric oxide (NO) release through endogenous nitrosothiols metabolism, activating the NO–cGMP (cyclicguanosine monophosphate) pathway to accelerate bone defect repair. 74
Chitosan is frequently applied in bone tissue engineering scaffolds due to its natural biocompatibility, ease of degradation, and capacity to enhance cellular attachment and proliferation, offering a conducive environment for effective bone healing and tissue regeneration. Kim et al. utilized low-temperature freeze-drying technology to prepare chitosan scaffolds loaded with Aln, which enhanced the function of osteoblasts while inhibiting the function of osteoclasts. 75 The Aln-loaded scaffolds achieved dual antiosteoporosis functions.
Composite materials
All kinds of materials have their own unique advantages and limitations. Composite scaffolds can give full play to the advantages of multiple materials and overcome the inherent drawbacks of single materials. By organically integrating the multiple properties, composite scaffolds show better performance and bring new ideas for the preparation of osteoporotic bone defect repair scaffolds. Typical applications of composite material scaffolds for osteoporotic bone defect repair are shown in Table 5.
Composite Material Scaffolds for Osteoporotic Bone Defect Repair
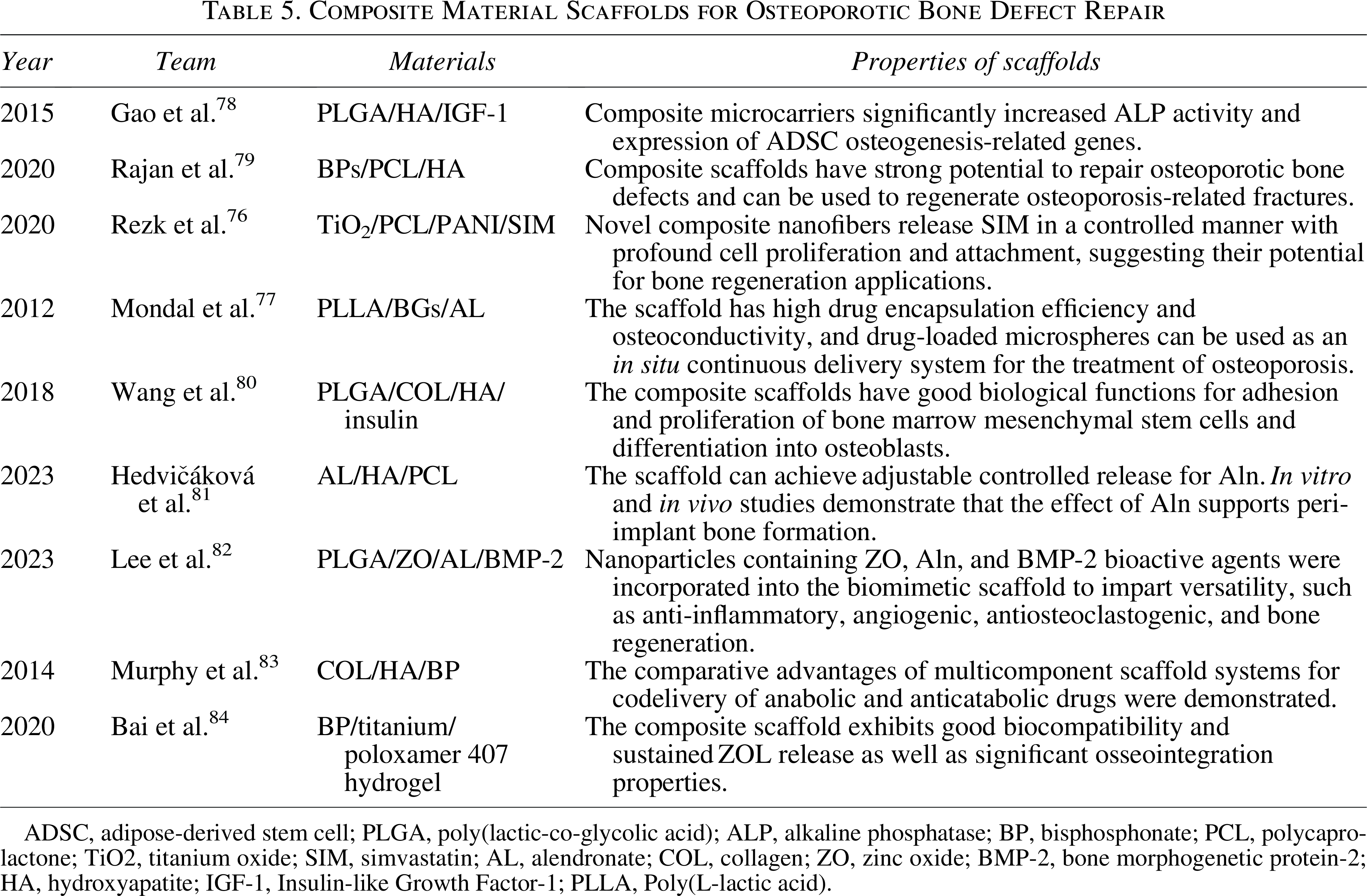
ADSC, adipose-derived stem cell; PLGA, poly(lactic-co-glycolic acid); ALP, alkaline phosphatase; BP, bisphosphonate; PCL, polycaprolactone; TiO2, titanium oxide; SIM, simvastatin; AL, alendronate; COL, collagen; ZO, zinc oxide; BMP-2, bone morphogenetic protein-2; HA, hydroxyapatite; IGF-1, Insulin-like Growth Factor-1; PLLA, Poly(L-lactic acid).
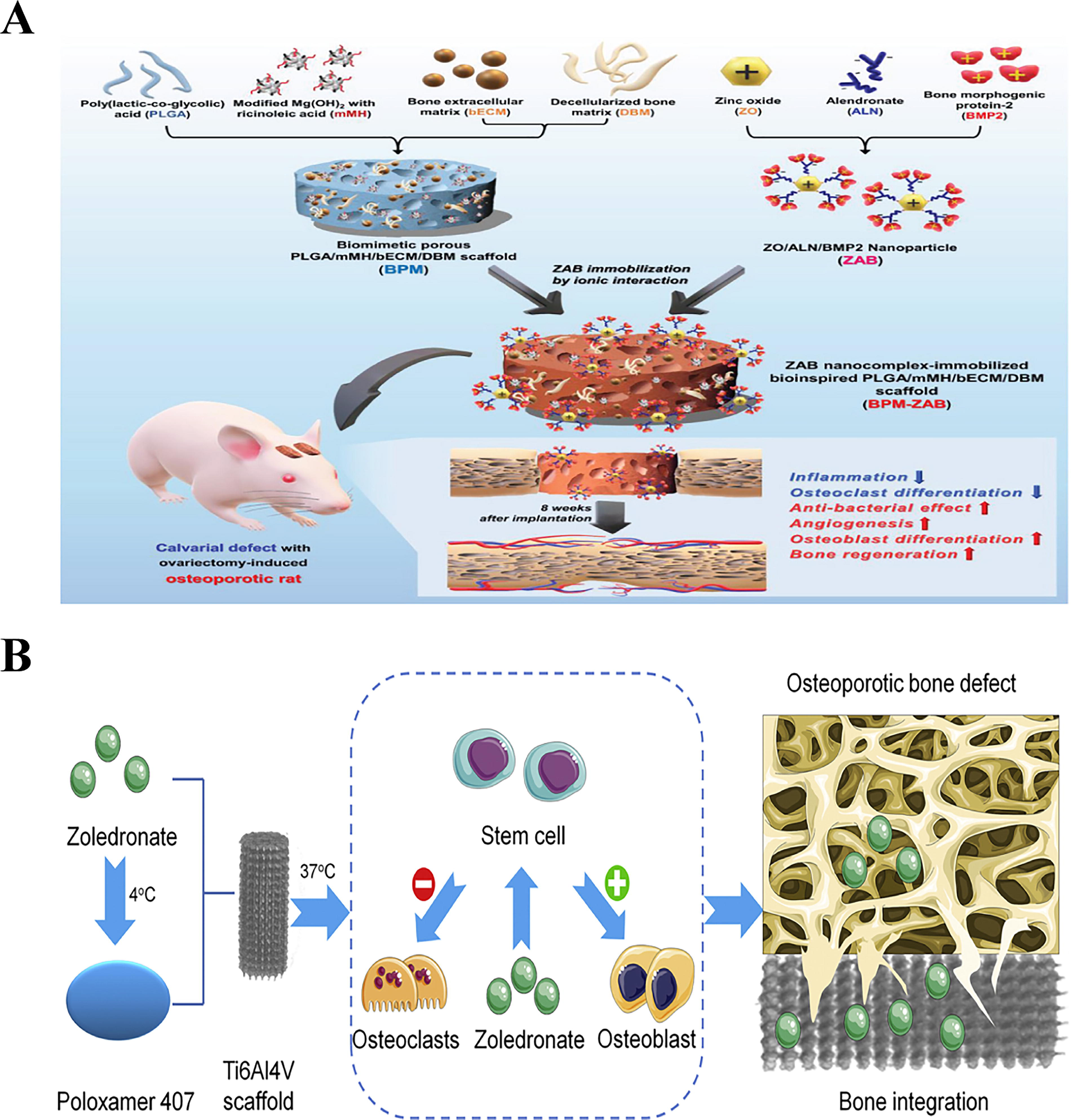
The combination of organic and inorganic materials in bone tissue engineering scaffolds leverages the biocompatibility of organics with the mechanical strength of inorganics, creating structures that support robust bone regeneration and improved integration with native tissue.78,79 The combination of drug-loaded microspheres has been demonstrated to enhance therapeutic effects by supporting bone regeneration while facilitating sustained drug release, which in turn promotes healing and reduces infection risk. PCL scaffold composited with polyaniline-coated titanium oxide nanoparticles with simvastatin exhibited excellent osteoconductivity, vascular, and osteoinductive properties in osteoporotic bone defects. 76 Drug-loaded nanomicrospheres were loaded on functional composite scaffolds for the repair of bone defects.77,80 Hedvičáková V et al. prepared composite scaffolds containing HA and PCL as a drug delivery system for Aln by utilizing electrostatic spinning technology. 81 Lee et al. composited nanoparticles containing biologically active substances, including zinc oxide (ZO), Aln, and BMP-2, into the PLGA scaffold mixed with extracellular matrix (Fig. 6A). 82 This was in order to enhance the scaffold’s functions of anti-inflammation, proangiogenesis, and osteoclast inhibition. As a result, the scaffolds maintained a constant NO release rate (≈600 ppm ≈6.07 nmol/L), while demonstrating 1.5-fold higher ALP staining intensity and approximately 10-fold elevated expression of osteogenesis-related RNAs compared with controls. The scaffold successfully regulated the homeostasis at the bone defect of the osteoporosis rat model, and the new bone formation was better than that of the control group. The collagen serves to promote the binding of BMP-2, while the bisphosphonates have strong binding to HA. 83 Bai et al. constructed a porous titanium/poloxamer 407 hydrogel scaffold and loaded it with the bisphosphonate drug zoledronate using 3D printing, with the objective of promoting osseointegration in a rabbit osteoporosis model (Fig. 6B). 84
Immune microenvironment regulation
Bone regeneration is a multistage and tightly regulated biological process that progresses through four distinct but overlapping phases: the initial inflammatory response, the formation of a fibrocartilaginous callus, the transition to a bony callus, and eventual bone remodeling. 86 Immune cells play a pivotal role in modulating bone repair, primarily through their involvement in both acute and chronic inflammatory responses. Polymorphonuclear neutrophils are among the earliest immune cells recruited to sites of injury. The subsequent immune response is largely shaped by two major macrophage phenotypes: the classically activated, proinflammatory M1 type and the alternatively activated, anti-inflammatory M2 type. M1 macrophages dominate the initial phase of bone healing, releasing proinflammatory cytokines that facilitate the clearance of necrotic tissue and the degradation of damaged bone matrix. In contrast, M2 macrophages emerge during later stages, characterized by their secretion of IL-10 and TGF-β, key anti-inflammatory mediators that enhance reparative and regenerative processes. 87
All implanted biomaterials are often identified by the host immune system as exogenous materials, which can trigger varying degrees of immune responses. Recent advances in designing immunomodulatory biomaterials to direct immune cell behavior establish the pivotal role of immune responses in determining therapeutic outcomes of scaffold-based interventions for enhanced biomaterial-tissue integration.88,89 Therefore, the capacity of scaffolds to modulate the local immune microenvironment is a key determinant in facilitating successful bone repair and regeneration. The structural design of scaffolds plays a pivotal role in directing interactions with immune cells. Specifically, scaffolds with well-organized architectures could facilitate immune-cell adhesion and migration while modulating the inflammatory response, particularly through the regulation of macrophage polarization.45,46,85 Furthermore, scaffold properties such as porosity and surface hydrophilicity are crucial determinants of the local immune milieu.47,90–92 Variations in pore size have been shown to markedly influence immune cell behavior, especially the functional state of macrophages.
Beyond structural attributes, the incorporation of bioactive factors into scaffolds also plays a crucial role in the regulation of immune responses during bone regeneration. The controlled release of specific ions and biologically active molecules from the scaffold has been shown to modulate the local immune microenvironment, particularly by directing macrophage polarization toward a regenerative phenotype.93–95 This immunomodulatory effect not only attenuates excessive inflammation but also facilitates osteogenesis and overall tissue integration.
Discussion
Research challenges
However, implantable scaffolds for osteoporosis face challenges in optimizing biocompatibility, degradability, and mechanical properties. First, current scaffold architectures exhibit limited integration with the senescent bone microenvironment. Most existing designs primarily target conventional bone defects, largely overlooking the multiscale structural and functional degenerative characteristics of aged bone tissue. Moreover, prevailing immunomodulatory strategies are predominantly reliant on passive modulation via material surface properties or loaded factors, which often fail to achieve spatiotemporally precise control over macrophage polarization and immune cell recruitment. Furthermore, the long-term implications of scaffold–immune system interactions on bone homeostasis remain incompletely elucidated, and the understanding of senescence mechanisms within scaffold–cell crosstalk is still inadequate. In addition, persistent challenges exist in the loading and controlled release of bioactive molecules, particularly concerning limitations in release kinetics regulation, bioactivity preservation, and targeting precision, such as initial burst release or excessively rapid carrier degradation. Spatiotemporal regulation of immune responses by biomaterial scaffolds remains a continuing challenge. Consequently, developing multifunctional biomaterials capable of simultaneously promoting osteogenesis, modulating immune responses, and preventing infection has become imperative. 89
Future opportunities
Improving scaffold integration with bone and enhancing targeted drug delivery remain key goals. This requires a deeper understanding of osteoporosis and the development of simpler, cost-effective, and scalable scaffold technologies. Although 3D printing enables personalized design, high costs and low output hinder its clinical use. Thus, affordable synthetic alternatives are needed. Future clinical applications of bioactive scaffolds may focus on two key areas. First, the materials are intended for individuals afflicted with pathological bone defects, with the objective of accelerating bone healing and forestalling subsequent fractures by providing mechanical support to the scaffolds and facilitating local drug delivery. Second, these materials could be used preventively in high-risk individuals, delivered via minimally invasive injection to enhance bone density and regulate metabolism. Accelerating clinical translation requires robust research frameworks, including optimized large animal models, advanced evaluation tools like single-cell sequencing, and long-term bone density monitoring to boost acceptance of preventive interventions.
Multiscale alterations and optimization of structures
Traditional scaffolds provide mechanical support but fail to adapt to aging bone, leading to stress shielding and poor integration. Aging alters bone structure at multiple levels, reducing regeneration capacity. Emerging strategies focus on functionally adaptive scaffolds that mimic bone’s dynamic hierarchy. 3D printing allows precise control of scaffold architecture, and smart materials could adjust to mechanical needs over time. Machine learning might enable personalized design by predicting individual bone aging patterns.
Active molecules for bone repair scaffolds
Recent studies have identified a number of naturally occurring substances with potential benefits for the management of osteoporosis. These include minerals found in deep-sea water, such as calcium, potassium, selenium, and magnesium, which have been shown to promote the proliferation of osteoblasts and the expression of osteogenesis-related genes.96,97 Phytoestrogens from deep-sea and terrestrial plants—such as epimedium, flaxseed lignans, soy isoflavones, and others—have shown potential in promoting bone formation and managing osteoporosis. Traditional Chinese herbs like Herba epimedii, Fructus ligustri lucidi, and Fructus psoraleae also exhibit bone-regenerative effects, which were demonstrated to be effective in the treatment of osteoporosis in animal models. 98 These bioactive compounds can be incorporated into advanced bone scaffolds and released in a controlled manner to achieve targeted prevention and treatment of osteoporosis.
Multimodal intelligent responsive scaffolds
Future development of bone repair scaffolds should focus on multimodal coordinated regulation of mechanical support, osteogenesis, angiogenesis, and microenvironmental remodeling in senescent bone. This may be achieved through multifunctional growth factor loading or biomimetic structural design to enhance bone regeneration efficiency. Furthermore, scaffolds should integrate intelligent responsiveness to microenvironmental cues such as pH, enzymes, and inflammatory factors, thereby constructing smart biomaterials capable of on-demand release, adaptive mechanical modulation, and dynamic immunomodulation.
Regulation of senescent osteogenic microenvironment and cells
Furthermore, it seems that the research on osteoporosis mainly concentrates on the macro-level aspects such as hormone regulation and bone density, while the treatment at the cellular level has received relatively less attention. This is especially significant considering the increasingly aging population nowadays, as osteoporosis may occur due to the aging of osteoblasts. Cellular senescence is a pivotal mechanism in the pathological process of osteoporosis. 99 Senescent osteoblasts and BMSCs exhibit a loss of proliferative and differentiative capacity, contributing to exacerbated local inflammation through the secretion of senescence-associated secretory phenotypes. 100 Antiaging therapies that target senescent cells have been shown to significantly improve the bone microenvironment, reduce bone marrow fat deposition, and increase bone density. 101 Based on this rationale, our team proposed loading quercetin onto biomimetic mineralized bone repair scaffolds. This strategy aimed to modulate the immune and metabolic microenvironment by scavenging reactive oxygen species and regulating macrophage polarization, providing a new strategy to regulate the osteogenesis–vascularization coupling. Significantly, it requires careful assessment of immune and inflammatory risks, as surface properties and acidic degradation byproducts may provoke adverse responses. Future strategies should focus on bioactive molecule modifications to guide macrophage polarization and on pH/enzyme-responsive materials to balance scaffold degradation with tissue regeneration.
Gene editing and epigenetic modulation can restore stem cell activity, promoting osteogenesis and angiogenesis, but their long-term safety and interaction with scaffolds need further study. Gene reprogramming enables targeted changes in cell expression, reverting cells to a pluripotent, stem-like state.102,103 In contrast, partial reprogramming techniques modify the gene expression of cells to a limited extent, rejuvenating them without changing their fundamental fate. 104 To treat and prevent osteoporosis in the elderly, researchers should explore rejuvenating senescent osteoblasts using tissue engineering and gene reprogramming. Our team proposed a novel scaffold composed of bio-ceramics and polymers, combined with lipid-encapsulated microspheres carrying reprogramming factors. These are integrated into bioactive hydrogels that release antiaging and immunomodulatory agents in a targeted manner, promoting bone repair and regulating osteoporosis.
Conclusion
Bone aging and osteoporotic bone defects pose a significant challenge. In this review, we comprehensively discuss the mechanisms and treatments of osteoporosis and describe scaffolds used for osteoporotic bone defects by category. The contribution of different preparation methods and modifications to the osteogenic properties of scaffolds is discussed. Then, we review different materials of drug delivery scaffolds for the repair of osteoporotic bone defects. In conclusion, despite advances in scaffold development for bone aging and osteoporotic defects, critical limitations persist: inadequate structural integration with the senescent microenvironment, constrained immunomodulatory capacity, and insufficient mechanistic understanding of senescence in scaffold-cell interplay. Future efforts should prioritize the development of multimodal, intelligent, and patient-specific scaffold systems. By integrating therapeutic agents with microenvironmental modulation mechanisms, such platforms can deliver safer, more efficient, and precision-targeted therapeutic solutions for geriatric bone defect regeneration.
Authors’ Contributions
T.S.:Data curation, writing—original draft. Q.L.: Conceptualization, data curation. H.C.: Data curation, software. W.Z.: Investigation, visualization. N.H.: Writing—review and editing, project administration. Y.K.: Writing—review and editing, supervision.
Footnotes
Acknowledgments
The authors would like to thank all the participants in the studies.
Author Disclosure Statement
All the authors declare that they have no conflict of interest.
Funding Information
This study was supported by National Key R&D Program of China, MOST (2023YFC2509900), Basic Science Center Program of National Natural Science Foundation of China (No. T2288102).