
Abstract
Chronic tympanic membrane (TM) perforation remains difficult to resolve without surgery because of poor intrinsic healing capacity and limitations of passive, nonsurgical materials. Although patch-based approaches are common, most merely provide passive coverage and lack intrinsic therapeutic capability to drive tissue regeneration. We developed and clinically evaluated an extracellular matrix (ECM)-mimetic, drug-free nanopattern guidance (NG) patch for TM repair, marking a paradigm shift from passive coverage to active, biophysically driven regeneration. The NG patch is a biocompatible, implantable scaffold with aligned nanotopography that recapitulates native ECM architecture, coupled with a hydrocolloid adhesive layer to ensure secure placement. In a prospective study of 18 patients, the NG patch achieved a 61% overall healing rate with 50% complete closure and no serious adverse events. In rat models, a single application induced complete healing within 2 weeks. Mechanistic in vitro assays demonstrated that the nanopatterned surface enhances fibroblast adhesion, alignment, and directional migration, supporting organized tissue closure. Collectively, the NG patch offers a minimally invasive approach that activates TM repair through physical cues without exogenous drugs. This first clinical evaluation of an ECM-mimetic nanotopographical scaffold introduces a strategy to redefine the standard of care for chronic TM perforation and related defects.
Impact Statement
We report the first clinical evaluation of a drug-free, extracellular matrix-mimetic nanotopographical scaffold for chronic tympanic membrane perforation, shifting treatment from passive patching to active, biophysically guided regeneration. The nanopattern guidance (NG) patch combines aligned poly(lactic-co-glycolic acid) (PLGA) nanotopography with a hydrocolloid adhesive layer to promote fibroblast alignment/migration and maintain stable tympanic membrane contact. In a prospective study, it achieved a 61% overall healing rate (50% complete closure) without serious adverse events, with rapid and complete healing in animal models. This platform establishes a minimally invasive, clinically translatable strategy for otologic membrane repair.
Keywords
Introduction
Chronic tympanic membrane (TM) perforation is a common otorhinolaryngologic condition that can lead to severe hearing impairment.1–4 It is defined by persistent failure of TM regeneration, leading to discomfort and auditory complications.5,6 Because the TM is easily damaged, perforation often triggers recurrent inflammation and infection that further limits repair.7,8 Consequently, spontaneous healing and biomaterial-based patch repair frequently fail, making tympanoplasty the standard option.9,10 However, autologous graft tympanoplasty requires an incision and can cause bleeding, infection, scarring, discomfort, higher costs, and prolonged recovery. 11 Nonsurgical materials (paper patches, synthetic polymers, and hydrogels) are often ineffective in chronic cases due to limited regenerative potency and poor TM retention. 12 Thus, a high-performance, minimally invasive regenerative platform enabling nonsurgical TM healing is urgently needed.
Scaffold-based tissue engineering has emerged as a viable therapeutic strategy for TM repair by providing a provisional structural framework and modulating cell-material interactions essential for tissue closure.5,13 However, TM regeneration is governed by stringent anatomical and biomechanical constraints that differ substantially from those of conventional cutaneous or mucosal wound healing.14,15 The TM is an ultrathin, curved, trilaminar, and mechanically active membrane that must restore both barrier integrity and sound-conducting vibration. 16 Accordingly, an optimal TM scaffold should ensure sustained retention at the moist perforation margin, conform to the native membrane curvature, preserve membrane mobility, and establish a permissive microenvironment for coordinated cell migration, proliferation, and extracellular matrix remodeling.13,17 Although scaffold systems incorporating growth factors, proteins, or drug-releasing components have demonstrated regenerative potential, their clinical translation remains limited by rapid molecular degradation, short residence time within the middle-ear microenvironment, and insufficient control over local release kinetics.18,19 These approaches may also induce off-target inflammatory or fibrotic responses and increase regulatory complexity, further restricting their practical application.20,21 Furthermore, various delivery scaffolds, including hydrogels, sponges, and nanoparticle-based formulations, may suffer from inadequate adhesion to the fragile and curvilinear TM surface, uncontrolled swelling or degradation, and mechanical mismatch with the native membrane, potentially leading to premature detachment or compromised vibratory function.22,23 These limitations indicate that effective TM repair requires not only biochemical stimulation but also rational scaffold engineering that integrates structural stability, interfacial adhesion, mechanical compliance, and bioinstructive regulation of cellular behavior.13,24 Therefore, the development of a drug-free scaffold capable of directing endogenous repair through physical microenvironmental cues may provide a clinically practical and translationally relevant approach for nonsurgical TM regeneration.
Given limitations of current treatments, recent work has focused on biocompatible scaffolds incorporating nanoscale surface topographies.14,25 Such nanostructured scaffolds can promote directional cell migration and alignment, which are critical for effective regeneration.26,27 For example, silk fibroin and acellular collagen-based scaffolds have supported TM repair in preclinical models.28,29 Electrospun nanofibrous scaffolds are another promising class, as they emulate TM ultrastructure and enhance cell adhesion, proliferation, and alignment. Notably, nanofibrous patches have been reported to support cell growth, confer indirect antimicrobial effects, and upregulate healing-related mRNA expression. These effects were further evaluated in vitro using human dermal keratinocytes and human umbilical vein endothelial cells as representative TM-relevant models.2,30–32 Collectively, these studies highlight the potential of nanoengineered platforms to recapitulate the TM microenvironment and enable functional repair. Accordingly, combining biocompatible materials with nanoscale engineering is emerging as a promising nonsurgical strategy for chronic TM perforation. Future studies should validate clinical translatability and further optimize scaffold structure and function for therapeutic outcomes.
In this study, we developed a biocompatible PLGA-based nanopattern guidance (NG) patch with aligned 800-nm grooves/ridges that mimic native TM extracellular cues and conducted the first prospective clinical evaluation for chronic TM perforations. The NG patch promoted regeneration in a preclinical chronic perforation rat model. To optimize performance, four patch versions were engineered by tuning thickness, flexibility, and bioadhesion, and the best-performing variant was selected for clinical application in patients to validate therapeutic efficacy.
Materials and Methods
Fabrication of the NG patches
A UV-curable polyurethane acrylate (PUA; MINS-311RM, Minuta Technology Co., Ltd.) precursor containing a photoinitiator was dispensed onto a silicon master mold bearing 800-nm linear grooves/ridges fabricated by photolithography and reactive ion etching. After covering with a polyethylene terephthalate (PET) film to promote capillary filling, the mold was UV-cured (λ = 352 nm, 40 W, 60 s) to obtain a nanopattern PUA replica, followed by overnight UV exposure to consume residual acrylate groups. A PLGA solution (15% w/v in chloroform) was cast onto the nanopatterned PUA replica and covered with a flat polydimethylsiloxane (PDMS) block to form a nanopattern film. After solvent evaporation and brief heat treatment, the PUA mold was peeled off to yield a PLGA scaffold with 800-nm ridges and grooves. To optimize TM adhesion, four patch variants were evaluated as follows: (1) a 30-μm nanopattern patch (Version 1), (2) a 15-μm patch with improved conformability (Version 2), (3) Version 2 supplemented with topical fibrin glue after placement (Version 3), and (4) a hybrid design comprising the 15-μm nanopattern patch reinforced with a hydrocolloid adhesive ring (Version 4). All variants were assessed in clinical trials for adhesion stability and therapeutic performance in TM regeneration.
Characterization of the scaffolds
All samples were characterized by field-emission scanning electron microscopy (FE-SEM; ZEISS Gemini SEM 500, ZEISS, Germany) at 15 kV after Pt coating (working distance, ∼8.8 mm).
Mechanical properties of the scaffolds
Mechanical properties were evaluated using an MCT-1150 system (A&D, Japan). Tensile stress-strain tests were conducted on patch specimens (12 × 20 mm) at a cross-head speed of 100 mm/min, with loading applied parallel to the nanotopographic alignment (cross-head positioned 10 mm from the specimen center). Adhesion stress tests were performed separately at 1.5 mm/s, and the peak detachment load and corresponding displacement were recorded.
In vivo animal study of TM regeneration
In vivo efficacy was assessed in 20 male Sprague–Dawley rats (8 weeks; 40 ears) with bilateral TM perforations under Institutional Animal Care and Use Ccommittee (IACUC) approval. Standardized anterior-quadrant defects (∼40–50% TM area) were created, and ears were randomized to NG patch or paper patch control (n = 20 ears/group) without additional fixation. Healing was monitored for 14 days by serial otomicroscopy and graded as complete, partial (>50% reduction) or none (≤50% reduction), with complete closure defined as therapeutic success.
Clinical study
The NG patch was clinically evaluated in patients with chronic otitis media–associated pars tensa TM perforations under IRB approval (Cheonan Hospital, Soonchunhyang University College of Medicine; IRB No. 2021-06-043) and in accordance with the Declaration of Helsinki. Patients with small (<25%) to moderately sized (<60%) chronic perforations without active infection were enrolled, excluding cases with cholesteatoma, ossicular pathology, otorrhea, granulation tissue, severe vertigo, profound sensorineural hearing loss, facial nerve palsy, temporal bone fracture, or suspected ossicular disruption. Patients presented with chronic TM perforations of varying sizes and clinical histories, representing a clinically heterogeneous population commonly encountered in outpatient otologic practice. Baseline assessments included otomicroscopy and pure-tone audiometry (PTA; mean air-conduction thresholds at 0.5, 1, 2, and 4 kHz). Under local anesthesia in an outpatient setting, a single experienced otologic surgeon refreshed the perforation margin, placed a 5–7-mm nanopatch using microsurgical instruments, and secured it with a thin medical adhesive layer. Patients received 3 days of oral antibiotics and standard precautions, with follow-up at weeks 1, 4, and 8 and then weekly up to 12 weeks or until closure. Outcomes were categorized as complete closure within 12 weeks without persistent otorrhea or reintervention (success), >50% reduction in perforation size (partial healing), or ≤50% reduction/no change (no healing), and PTA was repeated at 3 months to evaluate hearing outcomes.
In vitro studies: Immunocytochemical staining
NIH3T3 fibroblasts cultured on nanopattern PLGA patches for 24 h were fixed, permeabilized, and blocked, then stained for vinculin and F-actin (phalloidin) with 4′,6-diamidino-2-phenylindole (DAPI) nuclear counterstaining. Images were acquired using a Zeiss LSM 980 confocal microscope (Airyscan 2).
In vitro studies: Scanning electron microscopy
NIH3T3 cell-seeded scaffolds were fixed in PBS containing 2% paraformaldehyde and 2% glutaraldehyde for 4 h, washed, and postfixed with 1% osmium tetroxide for 1.5 h. After additional PBS washes, samples were dehydrated through a graded ethanol series (30–100%), Pt-sputter coated (∼5 nm), and imaged using a ZEISS Gemini SEM 500 FE-SEM.
In vitro studies: Cell migration assay
NIH3T3 cell migration on flat surfaces and NG patches was assessed using a PDMS barrier (1-mm diameter) to create a cell-free zone. NIH3T3 cells (1 × 106 cells/scaffold) were seeded and cultured for 24 h, after which the barrier was removed to initiate migration. Migration into the gap was imaged at 0, 12, 24, and 48 h using an optical microscope, and the covered area was quantified using ImageJ.
Statistical analysis
All quantitative data are presented as mean ± standard deviation (SD) unless otherwise indicated. Comparisons between two groups were performed using unpaired Student’s t-tests, whereas comparisons among three or more groups were analyzed using one-way analysis of variance. Nonparametric data were analyzed using the Kruskal–Wallis test. Categorical healing outcomes were analyzed using the chi-square test or Fisher’s exact test, as appropriate. Healing rates are reported as proportions with 95% confidence intervals (CIs), calculated using the Wilson score method. Statistical significance was defined as p < 0.05. Statistical analyses were performed using SPSS software (IBM Corp., Armonk, United States of America). Since the clinical component of this study was designed as an exploratory prospective pilot study to evaluate the feasibility, safety, and preliminary therapeutic efficacy of the NG patch, a formal a priori power calculation was not performed. Instead, the observed effect sizes and CIs were used to inform the statistical interpretation and to provide a basis for designing future adequately powered multicenter clinical trials.
Results
Design and fabrication of the NG patches
Figure 1A and B schematically summarize the clinical limitations of conventional TM repair materials and the design of the NG patch (15-µm thickness with uniaxially aligned 800-nm grooves/ridges). Conventional options, including paper patches, absorbable materials, and autologous fascia, have limitations related to retention, durability, or regenerative performance. To address these limitations, a PLGA-based nanopattern guidance (NG) patch was fabricated. In contrast with the nonpatterned surface of flat patches (Fig. 1C), the NG patch surface (Fig. 1D) exhibited a highly aligned topography composed of 800 nm-sized grooves and ridges. The fabricated scaffolds were freestanding and flexible (Fig. 1E), which allows them to conform to complex and irregular surfaces of biological tissues or organs. This structural adaptability makes them well-suited for use as transplantable biomaterials. Furthermore, the fabricated NG patch exhibited superior mechanical properties and adhesion capabilities. In tensile tests, with mechanical load applied along the direction of the nanopatterns (Fig. 1F and G), the NG patch exhibited greater tensile strength (17.32 MPa) than the flat patch (9.26 MPa). In addition, surface analysis revealed that the NG patch possesses increased nanoscale surface roughness and hydrophilicity, which likely enhances adhesion through van der Waals–like interfacial interactions. Accordingly, in adhesion tests, the NG patch demonstrated higher adhesion force (16.21 kPa) than the flat patch (13.84 kPa; Fig. 1H). Overall, the NG patch exhibited higher tensile strength and adhesion force than the flat scaffold.
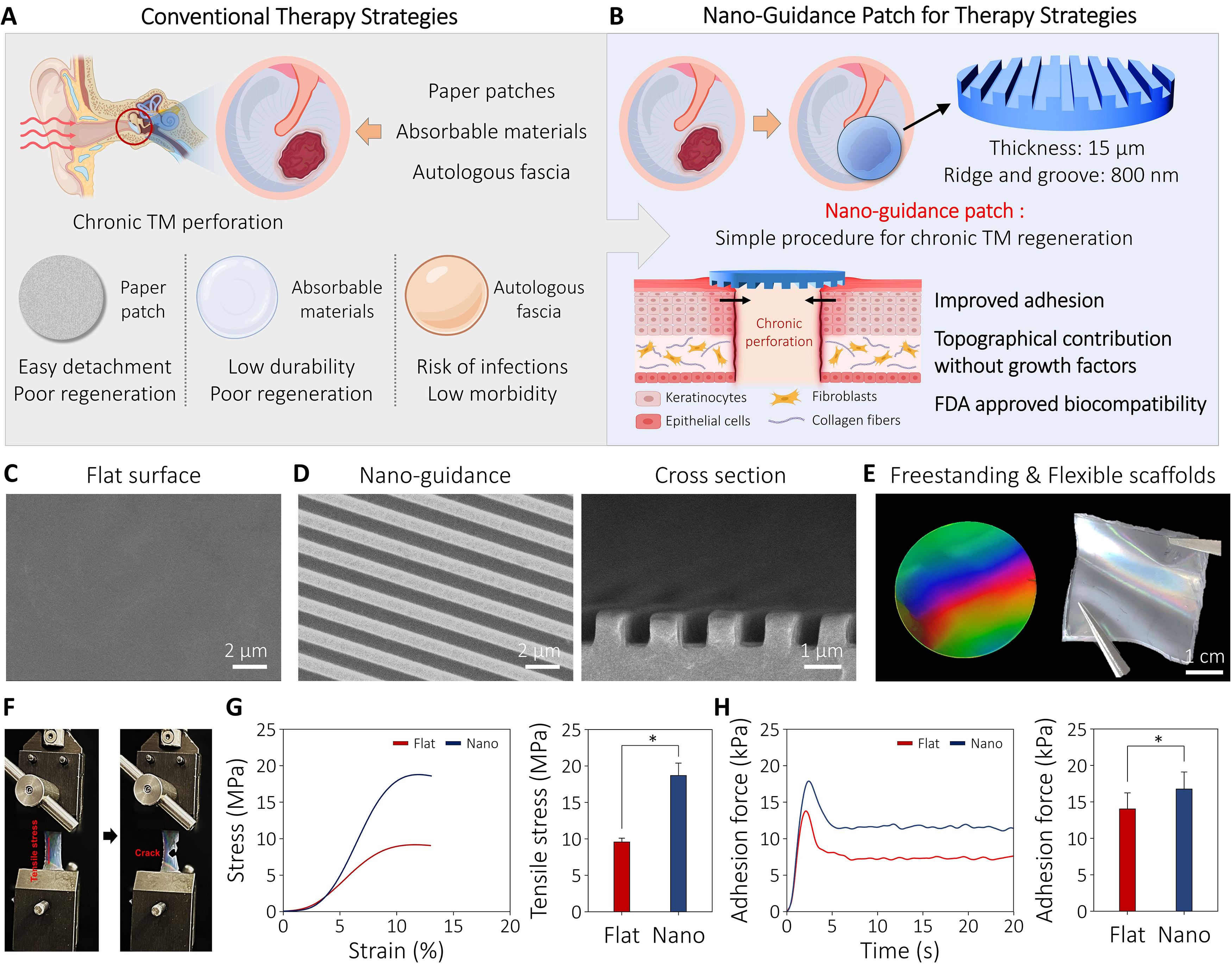
Design, fabrication, and characterization of nanopattern guidance (NG) patches for chronic tympanic membrane (TM) perforation.
In vivo animal study on TM regeneration
Figure 2A provides a schematic representation of the study design for in vivo animal trials. TM perforations were surgically induced in 20 male SD rats, resulting in a total of 40 ears. The ears were randomly assigned to the NG patch or paper patch control group, with 20 ears per group. Healing outcomes (Fig. 2B and C) were evaluated as described in Section 2.7 and categorized as complete, partial, or no healing. In the NG group, 14 ears (70%) exhibited complete healing within week 1, and the remaining 6 ears achieved complete healing by week 2, resulting in a complete healing rate of 100% (20/20 ears; 95% CI: 83.9–100.0%). In contrast, the paper patch control group showed a significantly lower healing outcome, with 3 cases of complete healing in week 1 and 13 additional cases at week 2; a total of 4 ears remained partially healed even after 2 weeks, resulting in a complete healing rate of 80% (16/20 ears; 95% CI: 58.4–91.9%). Healing outcomes differed significantly between groups (χ2 = 13.6966; p = 0.00106).
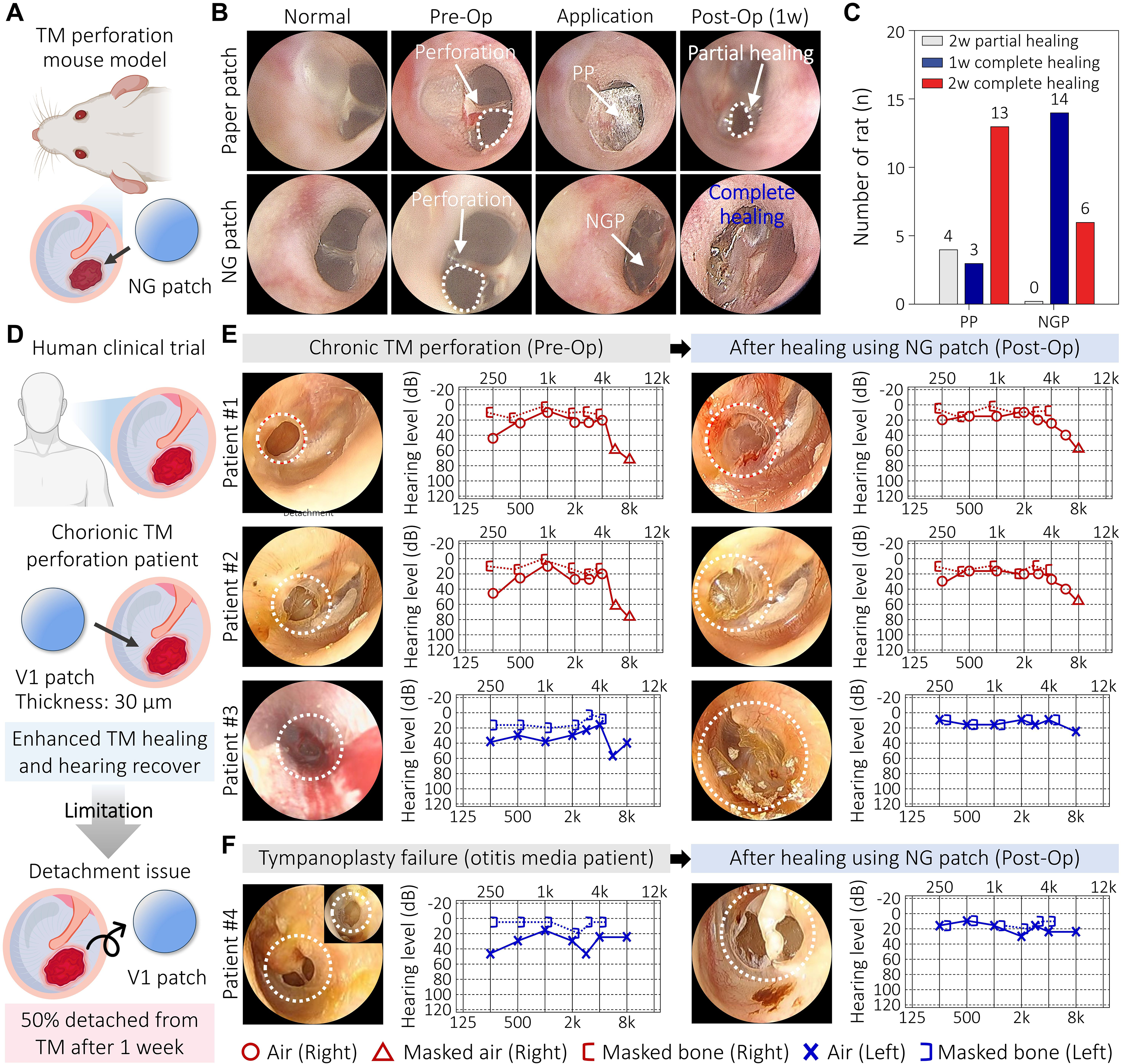
In vivo study and clinical study of Version 1 NG patches.
Clinical study on chronic TM perforation
A preliminary clinical study was conducted using Version 1 of the NG patch (30-μm thickness) to evaluate its therapeutic potential in patients with chronic TM perforations (Fig. 2D). Four female patients aged 32–59 years with chronic TM perforation and conductive hearing loss were enrolled. Following application of the NG patch, complete TM closure and hearing improvement were observed in three of the four patients (Fig. 2E and F). Notably, one patient with a previous failed tympanoplasty achieved complete TM closure and hearing restoration after treatment with the NG patch (Fig. 2F).
A total of 27 clinical procedures were subsequently performed using Version 1 of the NG patch, including the 4 initial cases. During the healing period, premature patch detachment was frequently observed. In cases where the patch remained attached, reductions in perforation size and TM regeneration were observed. However, most patches detached within 1 week of application.
For Version 2 of the NG patch (15-μm thickness), 47 clinical procedures were conducted (Fig. 3A). Compared with Version 1, the thinner patch demonstrated improved adhesion. In cases where the patch remained attached, regeneration of more than 50% of the perforated area was observed (Fig. 3B). However, premature detachment still occurred in a considerable number of cases (Fig. 3C).
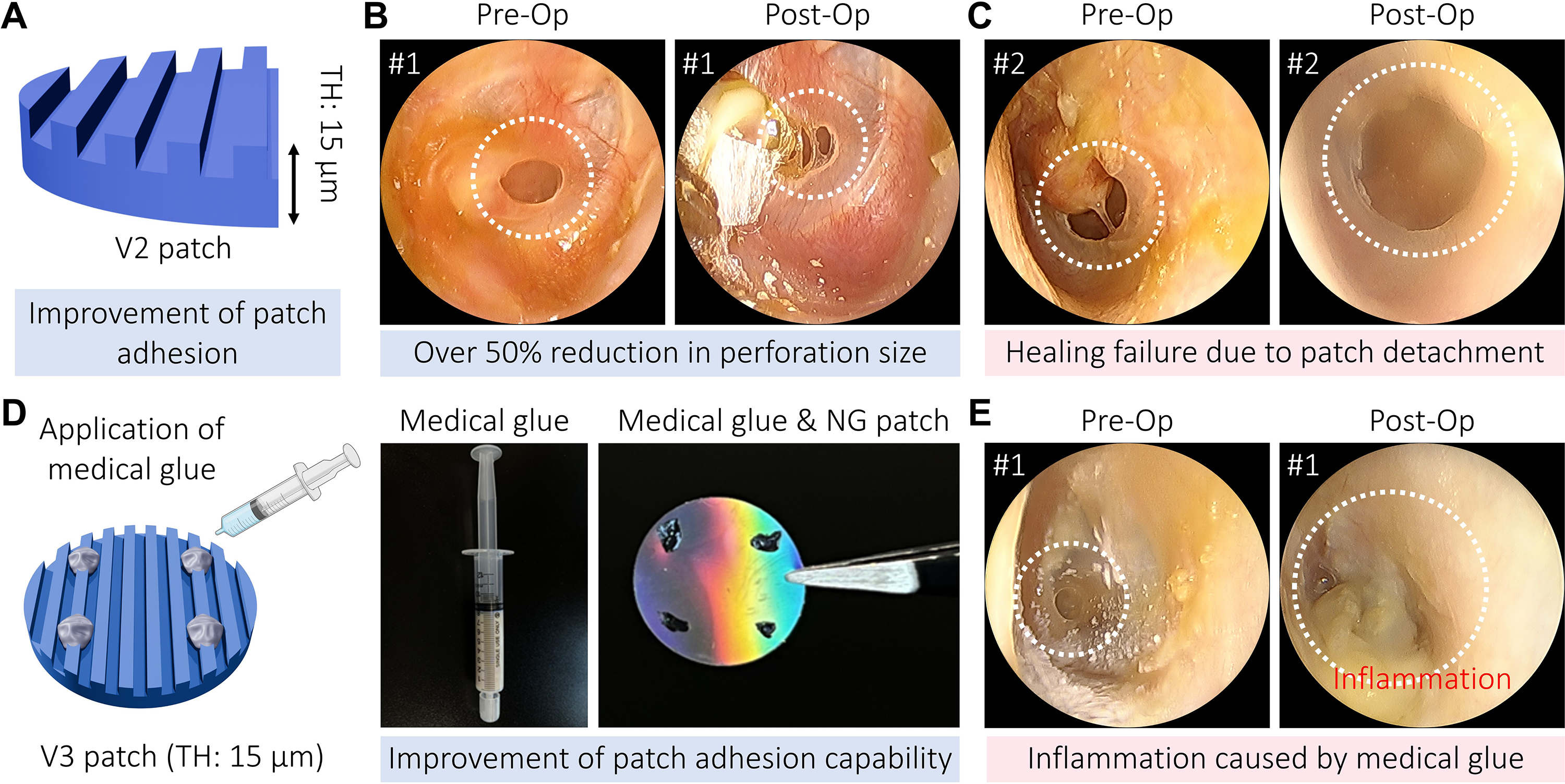
Clinical study of Version 2 and 3 NG patches.
For Version 3, the patch thickness was maintained at 15 μm, and medical fibrin glue was incorporated to improve adhesion to the TM (Fig. 3D and E). Five clinical procedures were performed using this design. Improved patch retention was observed, and successful TM regeneration occurred in cases with stable attachment. However, inflammatory reactions were observed following application of the fibrin glue-assisted Version 3 patch, limiting its clinical applicability (Fig. 3E). Previous reports have described inflammatory and foreign-body responses associated with fibrin sealants, suggesting that fibrin glue may have contributed to the observed reaction. 33 These outcomes highlighted the need for the development of safer NG patches that could provide strong adhesion without reliance on fibrin glue.
To improve patch retention on the TM, a Version 4 NG patch was developed by integrating a hydrocolloid layer, a biocompatible material widely used in wound care and skin tissue regeneration (Fig. 4A). In contrast to the earlier iterations, Version 1 (30 μm; prone to early detachment), Version 2 (15 μm; improved adhesion but limited durability), and Version 3 (15 μm with fibrin glue; improved adhesion but associated with inflammatory reactions), the Version 4 patch showed improved adhesion without requiring external adhesives (Fig. 4A). The hydrocolloid layer facilitated reliable contact with the perforated membrane and provided mechanical support during regeneration (Fig. 4D). A total of 18 clinical procedures were performed using the Version 4 NG patch in patients with chronic TM perforations. Overall healing (defined as complete closure or >50% reduction in perforation size) was observed in 11 of 18 patients, corresponding to an overall healing rate of 61.1% (95% CI: 38.6–79.7%), while complete TM closure was achieved in 9 of 18 patients, corresponding to a complete healing rate of 50.0% (95% CI: 29.0–71.0%; Fig. 4B–D). Follow-up visits were scheduled at weeks 1, 4, and 8, and then weekly for up to 12 weeks or until complete TM closure was achieved. In patients where the patch remained attached throughout the healing period, TM regeneration and reduction in perforation size were observed. Minor complications occurred in two patients (mild otalgia and transient otorrhea), both of which resolved with short-term medication without surgical intervention. No patch-related inflammatory reactions were observed.
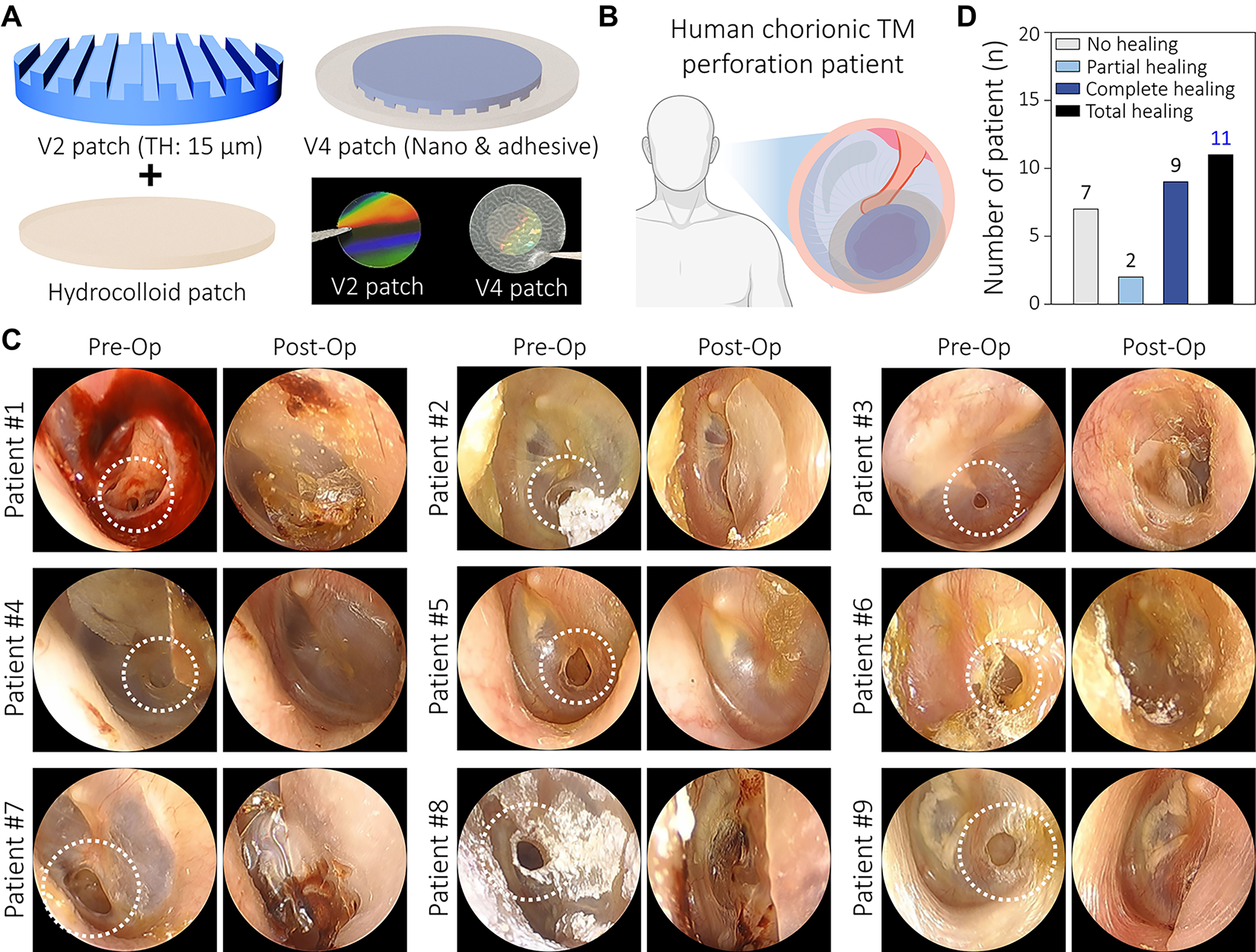
Clinical study of Version 4 NG patches.
Overall, progressive modifications from Version 1 to Version 4 were associated with improvements in patch retention and clinical performance, culminating in a hydrocolloid-integrated design that demonstrated favorable healing outcomes and biocompatibility.
Effect of the NG patch on cellular behavior in vitro
In vitro studies were performed using NIH3T3 fibroblasts. Cell adhesion was assessed 6 h after seeding, and a greater number of attached cells was observed on the NG patch than on the flat-surfaced control (Fig. 5A). Proliferation assays performed on days 3 and 5 showed higher cell proliferation on the NG patch compared with the flat patch and levels comparable to those observed on standard tissue culture polystyrene (TCPS). In addition, fibroblasts cultured on the NG patch exhibited an aligned morphology, whereas cells cultured on TCPS and flat patches displayed a more randomly oriented morphology (Fig. 5B and D).
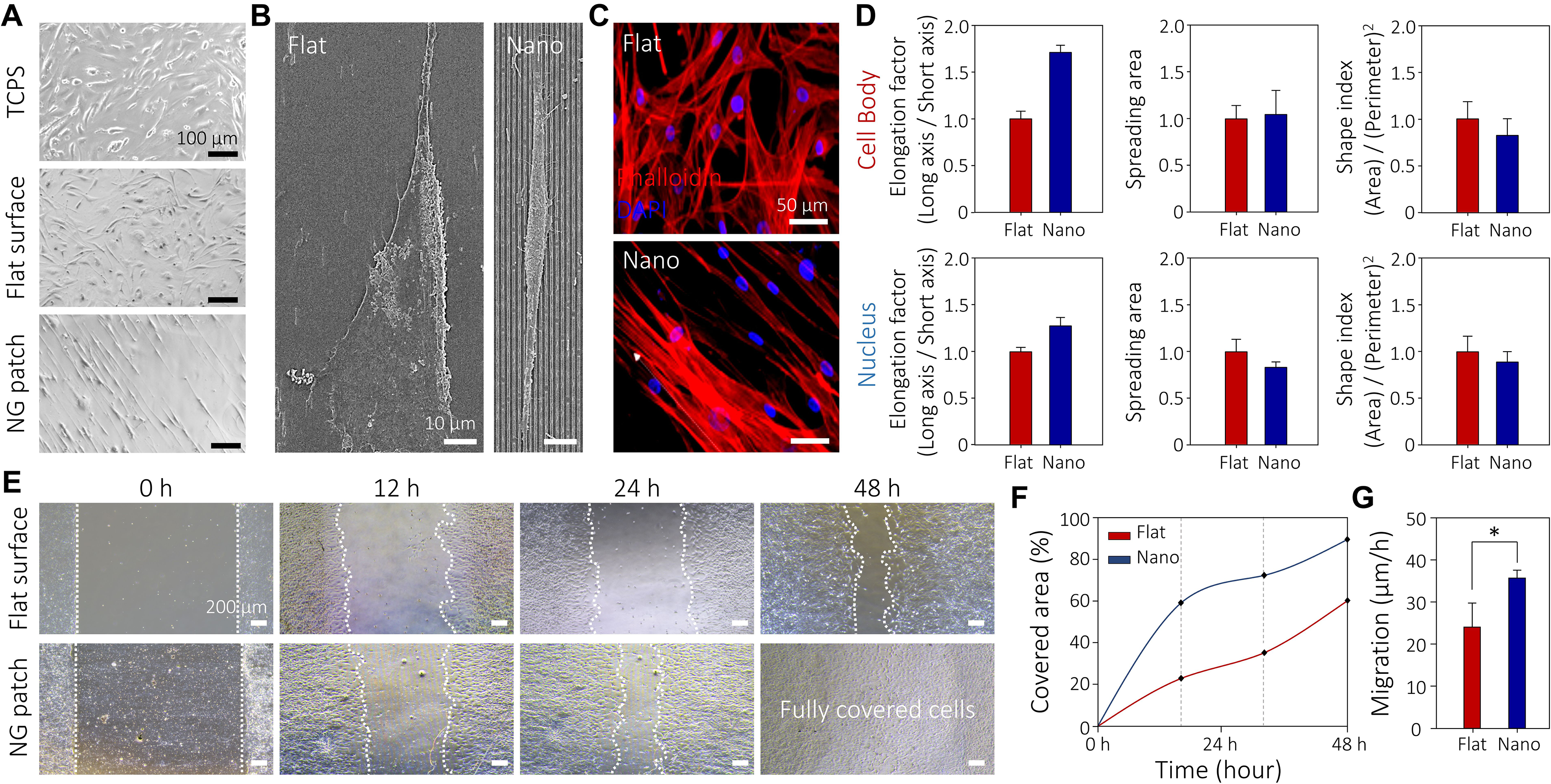
Effect of the NG patches on cellular behavior.
Cell morphology was quantitatively evaluated using elongation factor (EF; major axis/minor axis), cell area, and shape index (SI; 4π × area/perimeter2; Fig. 5D). The cell body and nuclear EFs were significantly higher in the NG patch group than in the flat patch group, with greater changes observed in the cell body than in the nucleus. No significant differences were observed in cell area between groups. The SI values indicated reduced cell spreading in cells cultured on the NG patch. These results demonstrated distinct differences in cellular morphology and organization between the NG patch and flat patch groups.
Cell migration assays were performed using a PDMS barrier model (Fig. 5E). The cell-free area created by barrier removal was completely covered within 48 h on the NG patch, whereas only 59.54% closure was observed on the flat patch at the same time point (Fig. 5F). Quantitative analysis showed that migration speed was higher on the NG patch (34.24 μm/h) than on the flat patch (24.14 μm/h; Fig. 5G). Overall, fibroblasts cultured on the NG patch exhibited increased adhesion, enhanced proliferation, aligned morphology, and faster migration compared with those cultured on flat patches.
Discussion
TM patches are widely used in outpatient otologic care because they are simple to apply and generally biocompatible.34,35 However, conventional materials (e.g., paper patches, gelatin sponges, hyaluronic acid sheets, and silicone membranes) primarily function as passive barriers that provide temporary coverage and moisture control rather than actively promoting tissue regeneration. 35 Their limited adhesion and positional stability on the moist, mobile TM often result in variable closure rates and recurrence in chronic perforations. 24 To address these limitations, we developed and clinically evaluated a first-in-human, ECM-mimetic, drug-free regenerative nanoscaffold designed to promote TM repair through biophysical guidance rather than passive coverage.
In a prospective clinical study, a single application of the NG patch achieved an overall healing rate of 61%, including approximately 50% complete closure, without serious adverse events. In parallel, in vivo testing in a rat model demonstrated complete healing within 2 weeks, whereas residual perforations remained in the paper patch control group at the same time point. These findings support the ability of the NG patch to accelerate TM regeneration compared with conventional patching approaches. Given the limited spontaneous healing capacity of chronic TM perforations and the frequent need for surgical intervention, these findings support the potential of the NG patch as a minimally invasive regenerative alternative. Importantly, the hydrocolloid adhesive layer enabled stable and anatomically conformal placement on the TM, overcoming a major limitation of conventional patch materials and facilitating sustained contact throughout the regenerative process.
Mechanistically, the regenerative effects of the NG patch appear to arise from the combination of ECM-mimetic nanotopographical guidance and prolonged physical contact with the perforated membrane. The aligned nanopatterns promoted fibroblast adhesion, elongation, alignment, and directional migration in vitro, resulting in accelerated closure of cell-free regions. 36 These cellular responses are consistent with contact-guidance phenomena, whereby cells sense and respond to nanoscale surface features through cytoskeletal reorganization and focal adhesion formation. 13 By providing structural cues that resemble the aligned architecture of the native TM extracellular matrix, the NG patch directs cellular organization and migration toward the perforation site. In addition, the hydrocolloid backing improves retention of the scaffold on the moist TM surface, maintaining intimate contact between the regenerative scaffold and host tissue throughout the healing process. Together, these effects support endogenous tissue regeneration through a materials-driven mechanism without the use of exogenous growth factors or drugs.
From a translational perspective, the NG patch combines a drug-free design with modular components consisting of a nanopattern scaffold and hydrocolloid adhesive layer, while remaining compatible with standard outpatient procedures and requiring no specialized equipment. 23 These characteristics facilitate manufacturing, clinical deployment, and broader adoption. Furthermore, comparison of the four NG patch versions highlights the importance of balancing conformability, adhesion, and biocompatibility for successful TM regeneration. Version 1, composed of a thicker PLGA scaffold, exhibited limited retention due to insufficient conformability to the TM surface. Version 2 improved flexibility through thickness reduction but remained susceptible to detachment. Version 3 further enhanced adhesion through the incorporation of fibrin glue; however, inflammatory reactions limited its clinical applicability. In contrast, the hydrocolloid-backed Version 4 provided stable retention, improved biocompatibility, and the most favorable regenerative outcomes among all designs.37,38 These findings demonstrate how iterative engineering refinements progressively addressed key translational barriers and ultimately led to a clinically feasible regenerative patch. Collectively, this work represents the first clinical evaluation of an ECM-mimetic nanotopographical scaffold for TM regeneration and demonstrates a shift from passive wound coverage toward active, materials-guided tissue repair.
The present study represents an initial prospective clinical evaluation of the NG patch and, therefore, has several limitations. The clinical cohort was relatively small, and the study did not include a randomized or controlled comparator group, limiting statistical power and direct comparison with existing treatment approaches. In addition, the enrolled patients represented a heterogeneous population with respect to perforation size and clinical history, which may have contributed to variability in treatment outcomes. Follow-up was limited to 12 weeks, precluding assessment of membrane durability, recurrence, and sustained hearing outcomes beyond the early healing period. Additional patients are currently being recruited, and ongoing clinical studies are underway to enable extended follow-up assessments, including evaluation of membrane integrity, recurrence rates, and hearing restoration. Furthermore, because the clinical component of this study was exploratory and involved a relatively small cohort, it was not statistically powered to establish definitive clinical efficacy. Therefore, the reported CIs should be interpreted as preliminary estimates of therapeutic performance, and future multicenter studies with predefined power calculations will be required to validate the clinical efficacy of the NG patch.
Reported outcomes of conventional nonsurgical patch-based treatments for chronic TM perforations vary substantially depending on perforation characteristics and patch design. For example, paper patch myringoplasty alone has been reported to achieve closure rates of approximately 21.6% at 8 weeks in chronic perforations, whereas adjunctive treatment with autologous serum increased closure rates to 54.5%. 39 More advanced regenerative approaches, such as Retympa™ (Nobelpharma Co., Ltd., Tokyo, Japan), which combines a gelatin scaffold with basic fibroblast growth factor (bFGF) and fibrin glue, have demonstrated closure rates of approximately 68.8% after treatment.40–43 However, gelatin scaffolds provide limited mechanical support and undergo relatively rapid degradation, whereas bFGF is regulated as a pharmaceutical agent in many jurisdictions, potentially increasing regulatory complexity and delaying clinical translation. Moreover, fibrin glue has been reported to induce inflammatory and foreign-body reactions in certain clinical settings, which may have contributed to the inflammatory response observed in the fibrin glue-assisted Version 3 patch. 33 In the present study, the NG patch achieved an overall healing rate of 61% following a single application. Although direct comparisons should be interpreted cautiously because of differences in patient populations, perforation characteristics, and study designs, these findings suggest that the NG patch provides regenerative outcomes within the range reported for currently available nonsurgical regenerative approaches while avoiding the use of exogenous growth factors or biologically active agents.
In addition, exogenous growth factors may pose risks of hyperplasia or aberrant tissue responses when dosing control is challenging. Clinical studies of Retympa have reported complications in 14.8% of patients, including epithelial pearl formation, TM retraction, otitis media with effusion, persistent otorrhea, transient vertigo, and drug-induced rashes. 41 Although these events were not classified as serious adverse events, they underscore important safety considerations associated with growth factor-based therapies. In contrast, the NG patch achieved comparable regenerative outcomes through topographical and material-based design alone, without exogenous biological agents, supporting its potential as a safer, broadly applicable, and globally translatable platform for TM regeneration.
To further support clinical translation, the NG patch design is inherently compatible with scalable manufacturing approaches. The nanopattern PLGA scaffold can be produced using established nanoimprint or replica molding techniques, enabling high-fidelity and batch-to-batch reproducible fabrication of aligned nanoscale grooves over large areas. Similarly, the hydrocolloid adhesive layer is derived from commercially available medical-grade materials that are already manufactured at an industrial scale, facilitating regulatory familiarity and consistent quality control. Importantly, the decoupled modular architecture of the NG patch allows independent optimization and standardized production of each component prior to final assembly, reducing variability between batches. Together, these features support robust manufacturing reproducibility and scalability, which are essential prerequisites for clinical adoption and potential commercialization of nanostructured regenerative devices.
Conclusions
In this study, we developed and clinically evaluated an NG patch for nonsurgical regeneration of chronic TM perforations. The optimized design integrates a 15-µm PLGA film bearing uniaxially aligned 800-nm grooves/ridges with a hydrocolloid adhesive layer, providing mechanical robustness, conformal TM adhesion, and sustained retention that supported consistent regeneration in preclinical and clinical studies. In the prospective clinical cohort, the patch achieved a 61% overall healing rate (∼50% complete closure) without serious complications, supporting the NG patch as a safe, effective, and minimally invasive therapeutic platform and underscoring the translational potential of engineering-driven regenerative strategies.
Authors’ Contributions
Conceptualization, writing—original draft preparation, and writing—review and editing: J.K., S.J.C., and W.K. Methodology: W.K., S.W.B., S.C., S.J.C., and J.K. Investigation: W.K., S.W.B., S.C., H.W.Y., D.K., S.L., S.J.C., and J.K. Visualization: W.K., S.W.B., S.C., H.W.Y., D.K., S.L., H.S., C.P., S.J.C., and J.K. Funding acquisition, project administration, and supervision: S.J.C. and J.K. All authors have read and agreed to the published version of the article.
Footnotes
Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korean government (RS-2024–00337706, RS-2025–02216206, RS-2020-NR049568, and RS-2022-NR067329). This work was supported by Korea Institute of Planning and Evaluation for Technology in Food, Agriculture and Forestry (IPET) through Companion Animal Intractable Disease Overcoming R&D Project, funded by Ministry of Agriculture, Food and Rural Affairs (MAFRA) (RS-2026-25519399). This work was supported by the Korea Institute of Planning and Evaluation for Technology in Food, Agriculture and Forestry through the Agriculture and Food Convergence Technologies Program for Research Manpower Development funded by the Ministry of Agriculture, Food and Rural Affairs (Project No. RS-2024–00397026). This research was supported by the Commercialization Promotion Agency for R&D Outcomes (COMPA) funded by the Ministry of Science and ICT (MSIT) (RS-2025-25430866). This work was partly supported by the [Technological Innovation R&D Program (SCALEUP TIPS, Tech Investor Program for Scaleup)] (RS-2023-00304358) funded by the Ministry of SMEs and Startups (MSS, Korea).