
Abstract
Cobalt (Co) and chromium (Cr) are widely used in medical implants due to their strength and biocompatibility. However, implant wear and corrosion can lead to systemic release of these metals, raising concerns about cardiotoxic effects, especially with long-term exposure. This review summarizes current data on the potential cardiotoxicity of implant-derived Co and Cr, focusing on molecular mechanisms, inflammatory responses, and clinical observations. Case reports and clinical studies document considerable variability in serum Co and Cr concentrations postimplantation, influenced by implant type, material composition, and patient-specific factors. While extreme elevations are strongly associated with cardiomyopathy and fibrosis, moderate increases also correlate with subclinical changes such as ventricular dilatation and impaired strain. Nonetheless, many studies fail to find a direct relationship between ion levels and cardiac dysfunction, highlighting the complexity and interindividual variability of toxic responses and underlying pathomechanisms. Existing experimental data suggest that Co and Cr ions interfere with calcium and magnesium handling, impair mitochondrial respiration, and promote the generation of reactive oxygen species. Additionally, both metals can induce inflammatory responses, including cytokine release that results in DNA damage, apoptosis, and impaired cardiomyocyte physiology. Although Co and Cr implants offer substantial clinical benefits, emerging evidence indicates that they may contribute to cardiotoxicity in susceptible individuals. Current findings emphasize the importance of personalized monitoring, including serum ion concentration assessments and advanced imaging techniques. Given the absence of universally accepted toxicity thresholds, further mechanistic and longitudinal clinical studies are essential to define risk stratification strategies, establish safe exposure limits, and improve the cardiovascular safety of patients with metal implants.
Impact Statement
Cobalt and chromium ions or particles released from orthopedic implants can impair cardiac function by disrupting calcium homeostasis, inducing oxidative stress, and triggering systemic inflammation. These ions reach the heart via the bloodstream and may contribute to cardiomyocyte dysfunction, fibrosis, and heart failure. Existing clinical data indicate that patient-specific factors, implant type, and exposure duration strongly influence the severity of effects. Understanding these mechanisms is essential for recognizing cardiovascular risks associated with metal implants and for developing strategies to prevent subclinical and overt cardiotoxicity.
Introduction
Metals have revolutionized modern medicine as they provide life-improving solutions for a wide range of pathological conditions, from orthopedic joint replacements to cardiovascular stents and dental prostheses. The utilization of medical implants has been constantly increasing over the last decades due to an aging population, advances in surgical techniques, and the improvement of healthcare conditions. For example, the mean number of hip replacements across all OECD countries in 2018 was 191.5 per 100.000 individuals, which was a 21.7% incline compared to 2008. 1 Likewise, the incidence rate for knee arthroplasty has risen by more than 100% in Europe and the United States, with an estimated increase of 469% projected for 2060.2,3
Strategies of implant fixation
Joint implants usually consist of three main components, including the stem, head, and articular cup. Two different approaches exist for anchoring the implant in the bone: cemented and uncemented fixation, the latter commonly applied for total hip arthroplasty (THA). Implant design and surfaces differ depending on the fixation methods. Cemented implants typically possess smooth surfaces and a more straightforward structure. A two-component, acrylic-based bone cement (polymethylmethacrylate) is utilized for secure bonding of the implant. Conversely, cement-free implants exhibit modified surface structure and coating, such as hydroxyapatite, to promote bone ingrowth. The pressure generated by the implant (press-fit design) stimulates bone growth, thereby forming a natural connection between the implant and bone tissue (osseous integration).4,5
The aforementioned methods have different implications and are associated with advantages and disadvantages. Cement allows for implant stabilization in unstable bone architecture, for example, osteoporotic bone. However, it is evident that the cement may undergo degradation over time, possibly resulting in implant loosening and inflammatory reactions, exacerbated by cement particles. 5 Furthermore, the implantation process can lead to rare Bone Cement Implantation Syndrome, a phenomenon caused when cement components enter the bloodstream. This dangerous side effect can manifest itself in various clinical symptoms, which may be caused by induced vasodilatation.6,7
Cement-free implants are primarily indicated for young and active patients, as cement is more prone to mechanical stress, leading to faster degradation. In addition, cementless implants favor active bone growth. Nevertheless, cement-free femoral implants for THA have been demonstrated to exhibit a significantly higher incidence of intra- and postoperative periprosthetic femoral fractures than cemented stems. The risk of these periprosthetic femoral fractures was found to be dependent on implant materials and geometry, as demonstrated by a meta-study conducted by Carli et al. 8 Titanium and ceramic implants are typically used in a cementless setup. However, a meta-analysis published by Zhang et al. includes products with cobalt-chromium alloy coatings for both cemented and cementless applications. 9 Moreover, hybrid implants exist that combine both fixation methods, as they can be applied as cemented stems and cementless cups or reverse hybrid.4,10
The selection of a fixation system should primarily aim to improve the patient’s condition, while additional factors such as physiological age, bone quality, and comorbidities, along with activity level and cost, must also be taken into consideration. 10
Articulating surfaces for THA
Furthermore, joint implants are typically characterized by their materials utilized for the configuration of the bearing surfaces between the head and the cup: metal-on-metal (MoM), metal-on-polyethylene (MoP), ceramic-on-ceramic (CoC).
Due to their increased stability and less volumetric wear, MoM implants are commonly used for THA. 11 In particular, the use of large femoral heads in MoM implants decreased the risk of dislocation. 12 On the contrary, Graves and colleagues outlined a positive correlation between the size of the femoral head and higher failure rates of MoM implants, based on National Joint Registry data from Australia, England, Wales, and New Zealand. This registry data showed that MoM implants with large femoral heads were associated with a revision rate more than doubling that of smaller heads. 13 The reasons for revision surgery of MoM implants with large femoral heads included loosening and infection of the implant, as well as metal-related pathology. 14
While MoP implants appeared to be a promising alternative in the beginning, it became evident that the abrasion of the polyethylene resulted in implant failure and required revision surgery due to aseptic loosening. 15 In contrast, CoC implants have been associated with reduced wear and are particularly selected for younger patients. Nevertheless, the elevated risk of dislocation and fracture, as well as cost considerations, have limited the widespread utilization of CoC implants. 16
An innovative advancement in joint implants was the development of bimodular stems that contain an additional modular junction at the neck-stem interface, enabling enhanced flexibility and a patient-specific design. Despite these advantages, bimodular systems have been reported to result in higher failure rates due to corrosion and fretting at the neck-stem junctions, leading to implant loosening.17–19 Therefore, careful consideration of patient-specific factors—including body weight, activity level, and hip offset—is essential when determining their use.20,21
A common issue among all implant types described herein is the mechanical stress, which can lead to processes of abrasion and corrosion of the implant materials. The most significant risk area is the head-neck junction of the implant. Corrosion at this site is also referred to as trunnion corrosion and has emerged as a major source of metal ion release.22,23 Besides MoM designs, trunnion corrosion has also been observed in MoP 24 and CoC implants. 25 Furthermore, particularly implants with large femoral heads that increase torsional stresses at the junction 26 and bimodular systems with an additional articulation reveal a more pronounced risk for trunnion corrosion. 21 Clinically, trunnionosis has been linked to elevated systemic metal ion concentrations, adverse local tissue reactions, implant loosening, and premature revision surgery. 22
Titanium alloys
Most commonly used implant materials consist of titanium alloys made up of titanium (Ti) as well as smaller amounts of aluminum (Al) and vanadium (V), and are in particular favored for their excellent mechanical strength, corrosion resistance, and biocompatibility. 27 However, implant failure can result in the release of Ti, Al, and V ions into surrounding tissues or the bloodstream. Few clinical cases showed negative effects of Ti wear debris resulting in adverse local tissue reactions, including pseudotumors, rather than systemic complications.28–30 Furthermore, Patients receiving TiAlV implants demonstrated elevated vanadium levels in blood and urine, compared to the unexposed cohort. 31 Experimental in vitro data and in vivo studies confirmed the potential of V to induce significant cytotoxic effects on osteoblasts, kidney cells, and neural tissue.32,33 In particular, pentavalent V acts as a pro-oxidant, enhancing oxidative stress that leads to cytotoxic events. 34 Although direct clinical evidence for V-induced cardiotoxicity remains elusive, these mechanistic studies suggest potential pathways through which V could adversely affect cardiac cells. A recent preclinical study by Wang and colleagues revealed that V intoxication impaired cardiac tissue architecture, including loss of striation in muscle fibers, myocyte inflammation, and necrosis of cardiomyocytes. 35
The release of Al ions has also been shown to exert its toxic effects predominantly by local reactions. Mizuno and colleagues found delayed cell proliferation and impaired bone formation in mesenchymal cells due to increased Al ions. 36 However, these cytotoxic effects are biphasic, depending on the ion concentration released from the implant. It has been found that low concentrations can even stimulate cell proliferation of osteoblasts. Compared to other metal ions, Al has been shown to be less cytotoxic than cobalt (Co), chromium (Cr), and V. 37 Regarding systemic effects, Al toxicity was associated with neurotoxicity rather than cardiotoxicity. Furthermore, the phenomenon of Al intoxication is closely linked to gastrointestinal absorption of Al ions rather than with increased systemic ion levels derived from orthopedic implants.38,39
Cobalt and chrom alloys
Other alloys that are commonly used for MoM implants include Co and Cr, which are favored for their durability, strength, and biocompatibility. 40 The widespread use of these metal implants has significantly improved patient outcomes, enabling mobility restoration, pain relief, and enhanced quality of life for many individuals. However, despite their indisputable clinical benefits, the long-term presence of metal implants in the human body has raised concerns about their potential toxic effects. Corrosion, particularly trunnion corrosion, wear, and other degradation processes, result in the release of metal ions and particles. 41 While Co and Cr are generally well-tolerated in their solid form, their ionic and particulate forms can elicit adverse biological responses. The release of metal ions from implants can result in their entry into the systemic circulation, leading to their distribution to distant organs, including the heart, liver, or kidneys. 42 Among these, cardiotoxicity has emerged as a critical concern, as accumulating evidence suggests that Co and Cr ions can affect cardiac function, induce oxidative stress, and promote inflammatory responses. 41
These cardiotoxic effects of metal implants are thought to arise from multiple mechanisms. Co ions, for example, have been shown to interfere with calcium (Ca) handling in cardiomyocytes, leading to impaired contractility and arrhythmias. 43 Additionally, Co and Cr ions can induce oxidative stress by generating reactive oxygen species (ROS), which can damage cellular components, including the DNA machinery.44,45 Experimental studies clearly demonstrate the toxic effects of metals on the cellular level, and a number of clinical case reports have shown a correlation between increased serum levels of metal ions and considerable cardiotoxic effects. Here, we provide an overview of the existing preclinical and clinical data on implant-induced cardiac toxicity and discuss potential safety concerns of Co and Cr, released from metal implants.
Mechanism of action
The toxicity of Cr and Co for cells, tissues, and organisms is undisputed and has been demonstrated by in vitro and in vivo experiments, observational studies, and case reports. However, the exact mechanism by which implants based on Cr and Co exert their toxic effects is hardly known. In particular, the adverse effects on heart tissue are still difficult to determine, as this involves a complex interplay of local and systemic processes, the distribution and transport of metals within the human body, and finally cardiomyocyte toxicity. In this regard, researchers have proposed various explanations for the severe pathological impact of Co and Cr on the cardiovascular system (Fig 1).
Cobalt
Co is an ubiquitous trace metal and an important cofactor in human physiology as it represents the metallic component of vitamin B12. However, substantial exposure to Co ions, for example, by implant failure, can result in toxic effects on various organs.
Co ions are thought to interfere with Ca handling in cardiomyocytes due to their divalent cation properties.43,46 In this context, Co was demonstrated to bind to sarcolemmal proteins and use the Ca-transporting machinery to enter cardiac cell types.47,48 Once entering the cells, Co might be able to affect Ca-dependent enzymes, like Ca2+/calmodulin-dependent protein kinase II, which plays a pivotal role in proper cardiac function.49,50
Additionally, Co can promote the generation of ROS molecules by inhibiting the activity of respiratory enzymes in cardiac mitochondria.51,52 Mitochondrial dysfunction and a defective energy metabolism directly influence cardiomyocyte behavior, resulting in impaired cardiac structure and function. 53 Moreover, increased oxidative stress triggers apoptosis and contributes to the development of fibrosis, that is, excessive deposition of extracellular matrix in the cardiac muscle, as observed in patients suffering from Co-induced cardiomyopathy.54,55
Besides Ca, Co can also compete with magnesium, another divalent cation that is required for the proper functioning of the cardiac contraction machinery. Under physiological conditions, magnesium, together with ATP, binds to myosin, which enables force generation. 56 As the ATPase activity depends on the cation species bound to myosin, it might be tempting to speculate that Co ions are capable of altering ATP hydrolysis, thus affecting the contraction of sarcomeres in cardiac cells. 56
Chromium
Cr is considered a nutrient that is involved in carbohydrate, lipid, and protein metabolism, although recent research does not support Cr as being an essential element for human physiology. 57 Cr exists in different oxidation states, with Cr3+ and Cr6+ being the most common ones. Compared to Cr3+, hexavalent Cr is highly toxic, inducing carcinogenic, teratogenic, and mutagenic effects.58,59 Cr3+, the most stable form, shares similarities in size and charge to ferric iron, thus, it can bind to transferrin, which supports transport in the bloodstream and cellular uptake. 60 In addition, cellular entry of Cr ions can occur via passive diffusion or phagocytosis. 61 After crossing the cell membrane, Cr undergoes a series of chemical reactions, resulting in the production of ROS species that in turn provoke cell toxic effects. ROS molecules directly or indirectly modulate myofilament functions and alter the activity of ion channels, like sarcoplasmic/endoplasmic reticulum Ca2+-ATPase (SERCA) and ryanodine receptor (RyR), in cardiomyocytes. 62 Increased cellular ROS levels have been further attributed to inflammatory events, fibrosis, and cardiac hypertrophy.62–64 Moreover, Cr can directly interact with chromatin and histones, altering the epigenetic profile and the pattern of gene expression.59,65
Both Co and Cr can initiate their toxic effects in two different ways, either as ions or as solid particles of various sizes. Larger particles accumulate in the tissue and commonly reside at the implant site, which is also described as metallosis. Here, particles can be uptaken by macrophages and trigger an inflammatory response. 66 While larger particles mainly induce local toxicity, smaller metal nanoparticles with less than 100 nm in diameter may pass the endothelial barrier, entering the bloodstream and reaching organs and tissues distant from the implant. An in vitro study by Taterra and coworkers revealed a cytotoxic effect of Co and Cr particles on platelet function, reflected by cell aggregation, swelling, and lysis. 67 Similar to the ion form, Co and Cr nanoparticles are able to cause DNA damage, inflammation, and oxidative stress. 68 Experimental in vitro data show that exposure to Co oxide nanoparticles results in intracellular ROS accumulation in ventricular rat cardiomyocytes, accompanied by impaired calcium handling and electromechanical properties. 69
Systemic inflammation caused by implant wear and cardiotoxic effects
Inflammatory processes are a central component of implant-associated toxicity. Wear particles released from metal implants can provoke both local and systemic inflammatory responses, with the systemic response being particularly relevant to cardiotoxicity. The release of proinflammatory cytokines in response to these particles contributes to widespread inflammation and has been associated with increased cardiovascular morbidity and mortality.70,71 Understanding the immunological mechanisms triggered by implant wear debris—both at the implant site and systemically—is essential for improving implant safety and identifying early indicators of adverse systemic effects.
Abrasion particles are recognized by innate immune cells, including macrophages, neutrophil granulocytes, and dendritic cells. 72 These particles are identified as danger signals (DAMPs = damage-associated molecular patterns), which are detected via pattern recognition receptors (PRRs), including toll-like receptors (TLRs). 73 The uptake and recognition of these particles lead to activation of the NLR family pyrin domain containing 3 (NLRP3) inflammasome, an intracellular sensor protein complex in macrophages that mediates the maturation and secretion of interleukin (IL)-1β. 74 In addition to IL-1β, other proinflammatory mediators such as tumor necrosis factor (TNF)-α, IL-6, IL-8, IL-18, interferon (IFN)-γ, monocyte chemoattractant protein 1 (MCP-1), and macrophage inflammatory proteins (MIP)-1α are released,42,75,76 which not only act locally but can enter the systemic circulation, reach distant organs—including the heart—and contribute to chronic low-grade inflammation.77,78 Furthermore, prostaglandin-like mediators (e.g., PGE2), ROS, and nitric oxide (NO) are produced, which amplify the local inflammatory response and induce vascular changes. 75 These mediators can exert their effects on distant tissues by affecting endothelial cells, fibroblasts, and cardiomyocytes, thereby altering cardiac function and structure.41,77,79 Among the many cytokines implicated in this systemic response, TNF-α, IL-1β, and IL-6 are the most frequently studied in the context of cardiovascular impact and are discussed in the following paragraphs.
TNF-α is a proinflammatory cytokine that is produced by various cells in the human body, including cardiomyocytes.80,81 TNF-α exerts its effects via two different receptors: TNFR1, which is typically associated with detrimental responses, and TNFR2, which is involved in tissue protection and repair. 82 High levels of TNF-α can impair heart function by reducing cardiomyocyte contractility and lowering the heart rate.83–85 Further, it promotes inflammation, cell damage, and remodeling processes within the cardiac tissue.86–88 Elevated TNF-α levels are particularly prominent in patients with advanced heart failure and are correlated with worse cardiac performance and poor prognosis. In contrast, low TNF-α levels may have protective effects, for example, in adapting to oxygen deficiency.89,90 Despite the importance of balanced TNF-α levels in heart disease, clinical trials with TNF-α inhibitors failed to show a clear benefit and, in some cases, even led to adverse side effects.91,92 Nevertheless, TNF-α remains an important marker for the risk and progression of heart failure.
IL-1β is a central mediator of systemic inflammation and was shown to be highly elevated in the myocardium following ischemic injury.93–95 Through its receptor IL-1R1, IL-1β provokes downstream signaling via myeloid differentiation primary response 88 (MyD88) and interleukin-1 receptor-associated kinase (IRAK), leading to the activation of nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB) and mitogen-activated protein kinase (MAPK) pathways. 74 This cascade promotes the expression of additional inflammatory genes, including IL-6, TNF-α, and cyclooxygenase-2 (COX-2), as well as p38 and c-Jun N-terminal kinases (JNK), that in turn facilitate apoptosis, inflammatory responses, and tissue remodeling.96–98 In cardiomyocytes, IL-1β directly contributes to cardiac dysfunction, fibrosis, and loss of contractility.99,100
IL-6 is a pleiotropic cytokine that—similar to TNF-α—plays a dual role in cardiac physiology. While transient IL-6 signaling is associated with protective effects, chronically elevated IL-6 levels increase the risk of heart failure, myocardial infarction, and dilated cardiomyopathy.101,102 IL-6 signaling is mediated via two distinct mechanisms: classical signaling via the membrane-bound IL-6 receptor (IL-6R) and transsignaling via the soluble IL-6 receptor (sIL-6R), leading to activation of the signal transduction cascade involving glycoprotein 130 (gp130), janus kinase (JAK) and signal transducer and activator of transcription 3 (STAT3). 103 Activated STAT3 translocates into the nucleus where it regulates a wide range of genes associated with inflammation, cell survival, and tissue remodeling.104,105 The acute activation of STAT3 is primarily protective, for example, through antiapoptotic effects, however, chronic stimulation promotes pathological hypertrophy, myocardial fibrosis, and maladaptive remodeling. 106 In addition, IL-6 activates the PI3K/AKT and MAPK/ERK1/2 pathways, further contributing to structural alterations in the heart tissue. 107
In summary, implant wear particles can elicit a systemic inflammatory response through the activation of innate immune cells. Key proinflammatory cytokines such as TNF-α, IL-1β, and IL-6 serve as central mediators linking local immune activation to distant cardiac dysfunction. Additional mediators—including IL-8, IL-18, IFN-γ, MCP-1, and MIP-1α—further amplify the systemic inflammatory milieu and may contribute to myocardial remodeling and impaired cardiac performance. Targeting these inflammatory pathways represents a promising therapeutic strategy to mitigate implant-related cardiotoxicity. However, the clinical relevance of these mechanisms remains incompletely understood. Further translational and clinical research is essential to validate these findings, identify susceptible patient populations, and guide the development of personalized prevention and treatment approaches. Moreover, it is important to understand how and in which quantities Co and Cr are transported from the implant site to the heart to unfold their toxic potential. Here, the serum concentrations in patients undergone implant surgery are a crucial parameter to assess potential toxic effects.
Clinical manifestations of metal implant-induced cardiac toxicity
Variability of metal ions in serum
A number of prospective and retrospective studies have been conducted aiming to evaluate a correlation or causal relationship between metal implants and impaired cardiac structure and function. However, available datasets are not consistent and demonstrate a variable picture of implant-based cardiotoxicity.
Using the French national health insurance database, 255,350 individuals with metal and nonmetal hip implants were compared in regard to the appearance of dilated cardiomyopathy and heart failure. 108 Following statistical analysis of different subgroups, metallic head implants were found to slightly increase the risk for both cardiovascular diseases. In another retrospective cohort study with 4,019 patients, Gillam et al. revealed that a certain type of large prosthesis (Articular Surface Replacement XL Acetabular System) led to a higher rate of hospitalization for heart failure in men. 109 On the contrary, no association between MoM hip prostheses and increased incidence of cardiac failure could be discovered in an analysis of more than half a million patients with MoM arthroplasties up to seven years postsurgery. 110 Noteworthy, these studies only performed statistical evaluation of existing datasets, thereby, did not consider patient-specific serum levels of metal ions and the severity of cardiovascular adverse events.
The clinical monitoring of patients undergone implant surgery has revealed a huge variability of serum concentrations of metal ions. In a recently published systematic meta-analysis, Miglironi et al. investigated the concentration of Co and Cr in serum of patients that have been subjected to THA. 111 While control groups demonstrated metal ion levels of ∼0.3 µg/L, the mean serum concentration of Co and Cr in patients undergone arthroplasty ranged between 0.5–3.5 µg/L and 0.6–2.6 µg/L, respectively. The detected differences in metal concentrations are correlated with the utilized implant material configuration, where MoM implants (CoCr–CoCr) demonstrated the highest serum levels. In accordance with these findings, a comparative study of ceramic and MoM hip arthroplasty showed mean concentrations of Cr and Co, 10.45 and 9.26 μg/L, respectively, in MoM patients. 112 In another prospective study, patients receiving CoCr alloy-based megaprosthesis were monitored before and after implantation. Serum levels of Cr and Co increased 11-fold and 64-fold after surgery, with a varying range between 2.93–27.12 µg/L (Cr) and 5.12–9.98 µg/L (Co). 113
This systemic release of metal ions, following implant surgery, can lead to their accumulation within cardiac tissue, capable of inducing cardiomyopathy or heart failure. Postmortem analysis of patients who had undergone hip arthroplasty with CoCr implants (primary or revision) demonstrated 69% increased Co concentrations in myocardial tissue, when compared to non-arthroplasty control groups (range between 0.006 to 6.299 μg/g). In contrast, no significant differences in mean concentrations were detected for Cr. 114 Moreover, the authors compared functional and pathological cardiac parameters and revealed a higher frequency for lowered ejection fraction, higher heart weight and size, as well as for increased intestinal fibrosis in the arthroplasty group, suggesting an association between implant exposure and cardiac diseases. These results are supported by Bellourd and colleagues, who found significantly higher Co levels in the heart tissue of autopsied arthroplasty implant patients. 115 However, since the measurement of metal ions in these studies was performed postmortem, the time-dependent change of Co or Cr levels was not considered.
In this regard, large longitudinal data sets at various intervals provide valuable insights into possible variations in metal concentrations over the long term. Results from a controlled clinical trial showed elevated Co and Cr serum levels in nine patients for up to 10 years after receiving a CoCr alloy hip implant. 116 While the concentrations of Co decreased over time, serum levels of Cr increased throughout the follow-up period, reaching a 3.9-fold maximum after 10 years, when compared to the baseline concentration. Another study of 71 patients who underwent MoM THA showed the highest median ion concentrations for both Co and Cr during the 3- to 4-year postoperative interval, followed by a general decline over the next 5 years. 117 Interestingly, a small group of the cohort (n = 9) showed a secondary Co and Cr peak at 6 to 7 years postsurgery, which was even more pronounced than the detected maximum concentration during the first interval, indicating a patient-specific effect of ion release. These patient-dependent variances were also observed by Bitar et al., who monitored Co and Cr levels over a period of 11 years in patients who underwent large-head THA. The mean ion levels of 14 patients demonstrated a gradual increase in Co levels over the entire follow-up period. 118 A progressive elevation of Co and Cr ions in serum was also reported in a 15-year follow-up study of patients receiving MoM hip implants. Particularly, Co levels were found to increase by 40-fold in comparison to the perioperative conditions. 119 Wan and coauthors identified fluctuations of both Co and Cr levels (two- to threefold) in patients with MoM hip resurfacing arthroplasty during a follow-up of more than 10 years. After an initial peak at 24–36 months postoperatively, there was a second and third rise in serum concentrations between 84 and 120 months after surgery. 120 In addition to hip implants, time-dependent fluctuations of ion levels have also been shown for MoM cervical disc implants. Here, the serum concentrations of Cr constantly increased within a 3-year period, subsequently reaching a plateau phase that persisted until the end of the 7-year follow-up interval. 121
These data highlight the strong patient-dependent variations of metal serum levels during follow-up intervals. The amount of ion release is determined by the type of implant, utilized material, and implant size, as well as individual patient-specific physiology and pathology, which makes it difficult to define a proper threshold of toxic metal concentration.
Metal ion concentrations inducing cardiotoxic effects
Severe cardiotoxic effects are commonly associated with very high serum concentrations of Co and Cr, as shown by multiple case reports. For example, a systematic review analyzed 23 case reports of Corelated cardiomyopathy in patients with hip arthroplasty implants. Individuals with Coinduced myocardial hypertrophy and interstitial fibrosis, confirmed by histopathological analysis, demonstrated the highest blood concentrations, ranging from 122 to 251 µg/L. 122 Nevertheless, adverse changes of Co-specific systemic toxicity, such as increased vacuolization, mitochondrial dismorphologies, and elevated concentration of lipofuscin, have been detected even in patients with lower Co levels (112–1556 µg/L). Another prospective clinical trial, comprising 110 patients receiving total hip or knee arthroplasty with metal implants, evaluated the association between total joint implant surgery and cardiac function. 123 While imaging data from echocardiography revealed no correlations between Cr concentrations (1.1–21.4 µg/L) and assessed cardiac parameters, increased Co levels (1.1–24.6 µg/L) were associated with left and right ventricular dilatation but did not impair the ejection fraction. Similarly, a former single-center blinded cross-sectional study with 90 patients failed to show a correlation between elevated Cr (1.71–69.0 µg/L) and Co ion levels (7.54–118 µg/L) and cardiac performance, following metal implant surgery. 124 These results are supported by a study from Darrith and colleagues, who compared MoM patients receiving total hip joint replacement and a non-MoM group. 125 Despite significantly increased Co and Cr concentrations in MoM individuals (Co: 11.12 ± 31.52 µg/L; Cr: 5.0 ± 9.76 µg/L), the ejection fraction remained unaffected. However, contractility analysis demonstrated a lower global longitudinal strain (GLS) in patients with MoM implants, though still falling within the normal range. Differences between contractility measurement and determined ejection fraction were also observed in a recently published small cohort study with 16 individuals. The authors detected a significantly reduced cardiac contractility in the MoM implant group (mean Co level: 29 µg/L), while other echocardiographic parameters, including ejection fraction, showed no differences from control patients. 126 As strain analysis is a more sensitive and reproducible method than the detection of left ventricular ejection fraction, determination of the GLS might be more suitable as a predictor for implant metal-based cardiac toxicity.
Case reports published over the last 10 years (Table 1) further underline the systemic and cardiotoxic effects caused by elevated cobalt and chromium levels following failure of metal-based hip implants. In most cases, implant failure was attributed to increased wear of metal components, possibly due to residual particles from previous ceramic implants. In addition, fractures or dislocations of the primary implant triggered excessive metal wear, thus leading to local metallosis in the periprosthetic tissue and increasing metal ion concentrations in blood and serum. Most patients demonstrated a markedly reduced LVEF, while some patients were even diagnosed with heart failure and cobalt-induced cardiomyopathy. Notably, the onset of cardiac symptoms varied widely, ranging from 10 months and 10 years postimplantation. This variability in both symptom onset and metal ion concentrations suggests a patient-specific mechanism of Co/Cr-induced toxicity. Chelation therapy was carried out in nearly all cases as the primary therapeutic strategy to counteract elevated systemic metal ion levels. Chelating agents such as N-acetyl-cysteine or ethylenediaminetetraacetic acid were applied to bind metal ions, thereby promoting the elimination through renal excretion. While chelation therapy has been shown to reduce systemic ion concentrations in all documented reports, this therapy remains symptomatic as long as the metal implant continues to act as a persistent source of exposure. Therefore, revisions to nonmetal alternatives such as ceramic-on-polyethylene (CoP) or CoC are widely recommended.127,128
Reported Cases of CoCr-Induced Cardiotoxicity Following Failed Hip Implants
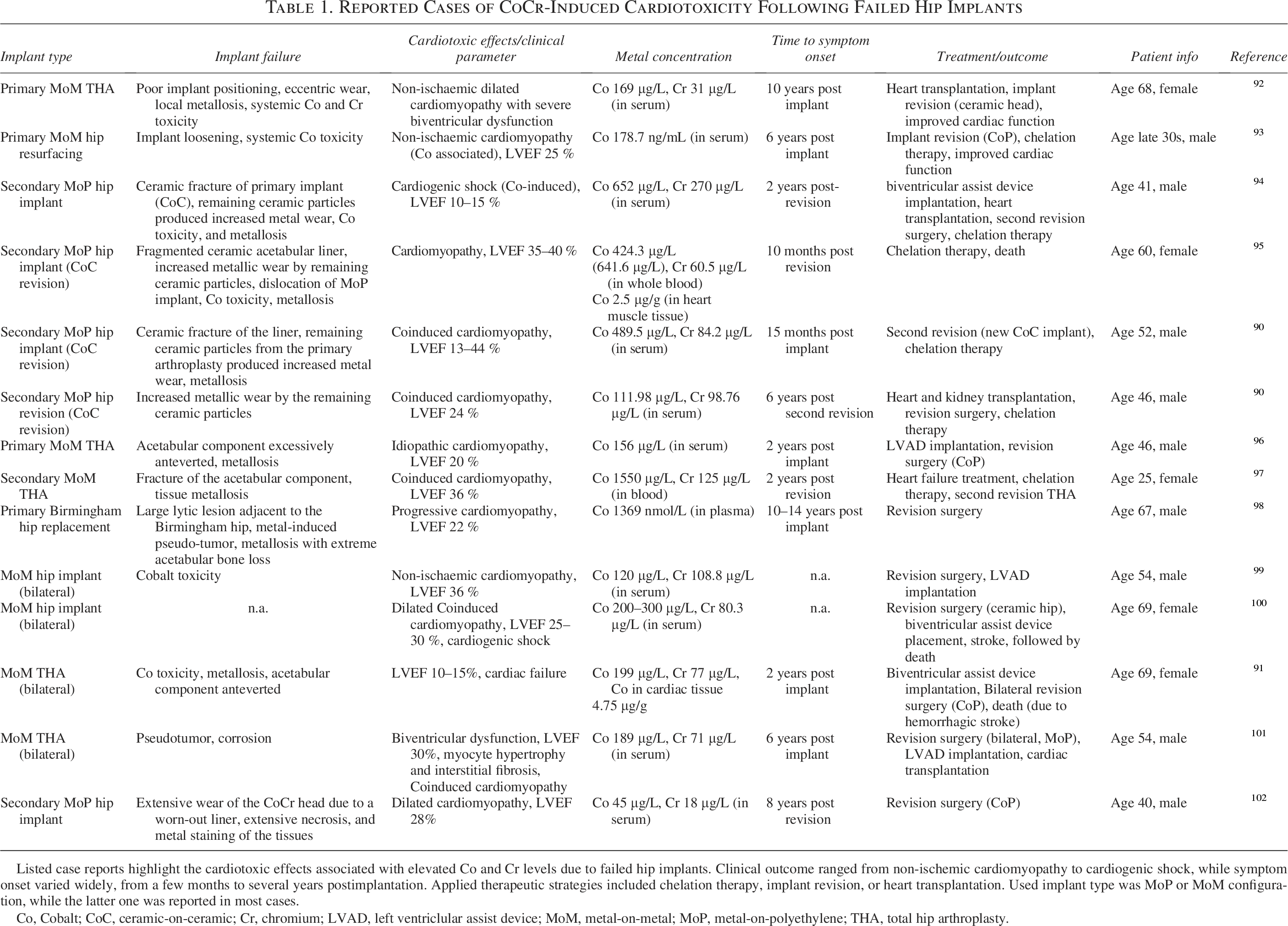
Listed case reports highlight the cardiotoxic effects associated with elevated Co and Cr levels due to failed hip implants. Clinical outcome ranged from non-ischemic cardiomyopathy to cardiogenic shock, while symptom onset varied widely, from a few months to several years postimplantation. Applied therapeutic strategies included chelation therapy, implant revision, or heart transplantation. Used implant type was MoP or MoM configuration, while the latter one was reported in most cases.
Co, Cobalt; CoC, ceramic-on-ceramic; Cr, chromium; LVAD, left ventriclular assist device; MoM, metal-on-metal; MoP, metal-on-polyethylene; THA, total hip arthroplasty.
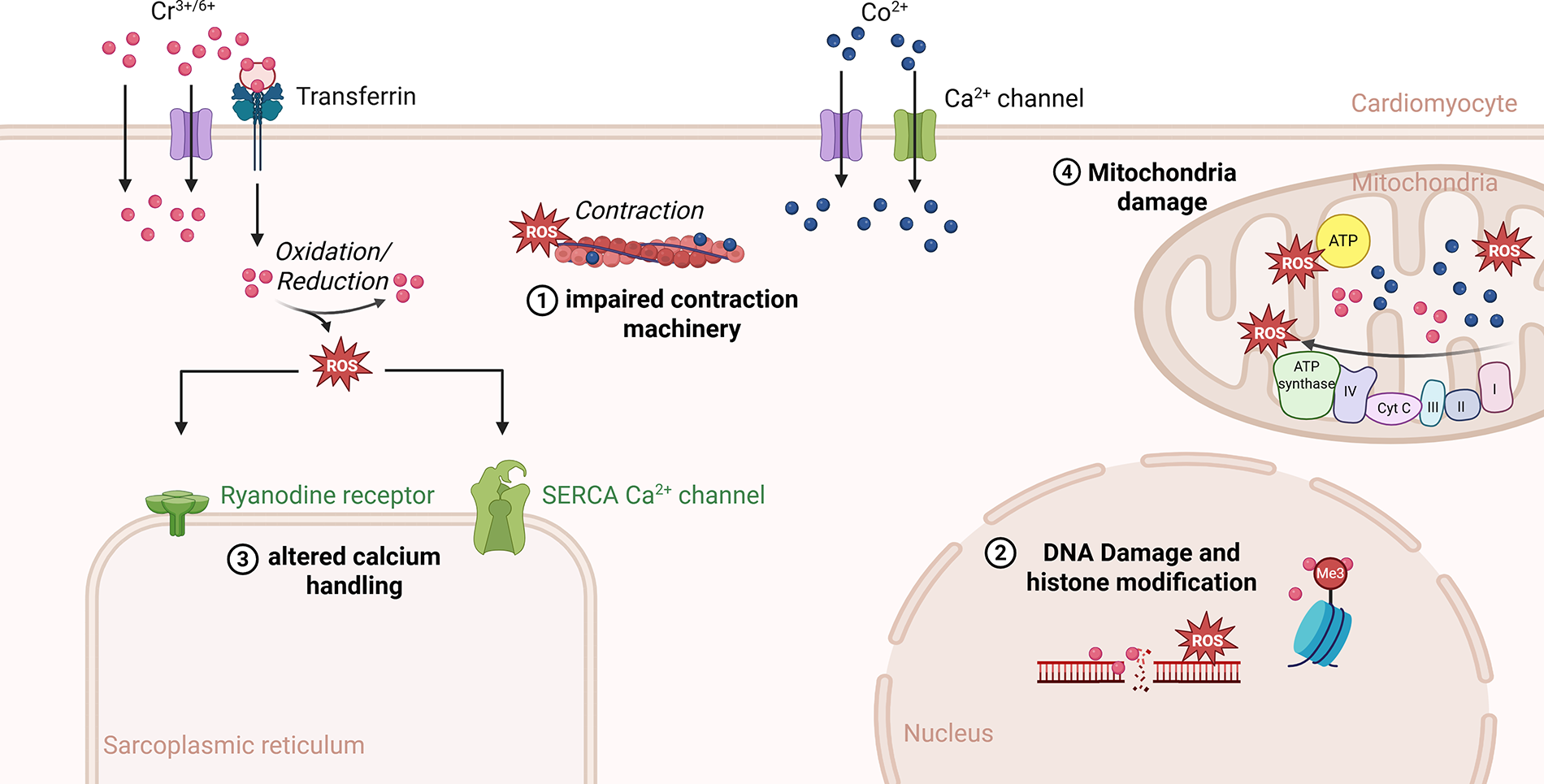
Potential cell toxic mechanisms of Cobalt (Co) and chromium (Cr) in cardiomyocytes. The cellular uptake of metal ions is suggested to be mediated by different ion channels, for example, Ca2+ channels, passive diffusion, or phagocytosis. For Cr, transferrin has also been shown to be involved in cellular uptake. After crossing the cell membrane, metal ions can directly interact with the contraction machinery (1) and chromatin, provoking DNA damage and histone modifications (2). Moreover, Co and Cr promote the production of cytotoxic reactive oxygen species (ROS) molecules that, in turn, lead to altered calcium handling (3) and DNA single or double-strand breaks. In mitochondria, metal ions can inhibit the activity of respiratory enzymes, which contribute to elevated ROS levels and lowered ATP production (4).
Threshold for Co and Cr
From a clinical point of view, it would be useful to define a proper threshold of metal ion concentrations. However, the patient-dependent variety of metal ion concentrations, their clinical relevance, and the lack of knowledge of underlying pathomechanisms make it difficult to determine an appropriate threshold for risk stratification. Hence, there is currently no international consensus on which metal ion concentrations in serum or blood are considered to be safe. Nevertheless, regulatory authorities have published follow-up recommendations for patients who received metal implants. The British Medicines and Healthcare products Regulatory Agency advises a closer follow-up, associated with cross-sectional imaging, when metal serum concentrations exceed 7 µg/L. 129 An opinion statement, published by the European Medicines Agency in 2014, suggested metal ion concentrations between 2 and 7 µg/L as a threshold for additional investigations. 130 A similar threshold range was declared by different US orthopedic associations, who determined three different risk categories: low risk <3 µg/L), moderate risk (3–10 µg/L), and high risk (>10 µg/L). 131 Based on these threshold values, a validation study was performed, involving 803 MoM hip arthroplasty patients. In terms of recognizing adverse events caused by metal debris, the authors found that lower, implant-specific thresholds of metal ion concentrations were more suitable for the detection of adverse events, compared to fixed thresholds. 132 Noteworthy, it is generally accepted that serum metal concentrations alone are insufficient for the predictive risk assessment of implant failure, and that additional clinical criteria need to be evaluated for adequate patient monitoring.
Limitations
While this review aims to provide a comprehensive synthesis of current knowledge regarding cobalt- and chromium-related cardiotoxicity arising from metal implants, several limitations should be acknowledged. In this regard, the included studies exhibit substantial heterogeneity in terms of design, patient populations, implant types, diagnostic methods, and follow-up durations, limiting comparability and the ability to derive generalized conclusions. Furthermore, this review only reflects the evidence available up to the time of article preparation and does not include unpublished or recently released data. Lastly, there is no universally accepted definition of cardiotoxicity, and studies vary in how they assess cardiac dysfunction. The absence of standardized toxicity thresholds complicates the interpretation of metal ion levels, and a clear dose-response relationship remains elusive.
Conclusion
Co and Cr metal implants have brought significant advances in medical treatment, but their long-term safety, particularly with regard to cardiotoxicity, remains a pressing concern. Wet lab studies consistently show that Co and Cr ions can induce oxidative stress, disrupt calcium and magnesium homeostasis, impair mitochondrial function, and trigger profibrotic signaling in cardiomyocytes — mechanisms that are directly linked to cardiac dysfunction. These molecular findings are supported by case reports of severe Coinduced cardiomyopathy and myocardial fibrosis, which are usually associated with highly elevated systemic Co levels.
However, clinical data show that Co and Cr ion concentrations and cardiac outcomes vary widely in different patient populations. While some studies report detectable cardiac changes such as ventricular dilatation or reduced contractility even at moderate serum levels, others do not show any distinct correlations. This discrepancy implies that cardiotoxic effects may not solely depend on the absolute metal concentrations, but also on the individual susceptibility of the patients, the implant design, and the duration of exposure. The employment of sensitive diagnostic tools and detailed stress analysis offers promising possibilities for the early detection of subclinical cardiac impairment, which may precede overt dysfunction.
Given the lack of generally defined safe limits and the complexity of the underlying pathomechanisms, the cardiotoxicity associated with metal implants requires further research. Future investigations should focus on linking mechanistic findings with longitudinal clinical studies to better characterize risk, refine surveillance protocols, and ultimately protect the cardiovascular health of patients with metal implants.
Authors’ Contributions
The conceptualization of the article was done by H.L., M.H., and S.K. Writing of the initial draft, including the preparation of figures and tables, was carried out by M.H. and H.L. with support from S.K. and A.S. Reviewing and editing of the article and acquisition of funding were carried out by R.D.