
Abstract
Environmental stressors delay cutaneous wound healing and significantly impact patient survival rates. Traditional wound medications suffer from low delivery efficiency and susceptibility to degradation. Microneedle technology, characterized by its minimally invasive nature and high efficiency, significantly enhances transdermal drug delivery capabilities, while nanomaterials improve therapeutic efficacy through superior drug protection and controlled-release properties. The combination of these two technologies synergistically enables rapid wound repair and reduces the risk of complications. Current research predominantly focuses on single-component analyses (with only nine related studies indexed in Web of Science from 2014 to 2025), lacking systematic investigation into their synergistic mechanisms. This review innovatively establishes a classification system for microneedle–nanomaterial combinations, elucidating their fabrication processes, functional characteristics, and synergistic enhancement mechanisms, thereby providing a critical theoretical reference for the field of cutaneous repair.
Impact Statement
This study pioneers a systematic classification and mechanistic analysis of synergistic microneedle–nanomaterial systems for advanced wound healing and cutaneous repair. By elucidating fabrication strategies, functional enhancements, and therapeutic mechanisms, it bridges critical knowledge gaps in transdermal delivery and tissue regeneration. The framework enables precise engineering of combinatorial platforms to overcome barriers like drug degradation, biofilm resistance, and dysregulated inflammation. This work accelerates clinical translation of minimally invasive, multifunctional therapies, offering transformative solutions for chronic wounds, scarring, and infections. It establishes a foundational roadmap for next-generation dermatological innovation and personalized regenerative medicine.
Introduction
Skin is vulnerable to microbial colonization, dysregulated inflammation, and metabolic disturbances during the repair process, often impairing wound healing and increasing systemic complication risks. 1 In clinical practice, strategies for promoting skin tissue repair include surgical debridement, negative pressure therapy, and wound dressings, with pharmacotherapy being the mainstream approach.2–4 However, the complex wound environment often leads to drug inactivation before it reaches the target site. 5 Therefore, developing efficient and reliable drug delivery systems and loading strategies is of critical importance.
Microneedle (MN) technology provides a distinctively advantageous drug delivery platform for skin repair, capitalizing on its precise tissue targeting, high delivery efficiency, and minimally invasive nature. 6 Currently, various types of microneedles, such as solid and dissolving microneedles, have been employed in research for skin repair.7,8 Furthermore, previous studies have applied microneedles to cardiac, 9 vascular, 10 and ocular 11 tissue repair. Nanomaterials serve as advanced vectors with high drug-loading capacity, nanozyme activity, and spatiotemporal release modulation, making them ideal carriers for microneedle-based drug delivery systems. 12 In skin repair, both microneedles and nanomaterials can independently play critical roles. For instance, magnesium microneedles exhibit inherent antibacterial and anti-inflammatory efficacy, 13 while selenium nanoparticles (SeNPs) demonstrate remarkable antimicrobial, antiviral, and anti-inflammatory properties. 14 Integrating the two components enables full exploitation of their synergistic advantages. Consequently, numerous studies have explored this combined strategy for cutaneous repair applications. 15
This review begins by outlining the current challenges in cutaneous wound healing, subsequently delineates the foundational applications of microneedles and nanomaterials, respectively, and ultimately focuses on their combined therapeutic strategies, innovatively establishing a function-based classification framework.
Structure and Damage of Cutaneous Tissue
Effective wound management requires a thorough understanding of normal cutaneous architecture and pathological alterations. This section outlines essential anatomical and pathophysiological context.
Cutaneous structure
Human skin comprises three layers (Fig. 1): (1) Epidermis: Primary barrier regulating moisture loss and blocking external substances. (2) Dermis: Provides structural support and elasticity via collagen/elastin. (3) Subcutaneous tissue: Primarily adipose tissue for organ protection, energy storage, and thermoregulation.16,17
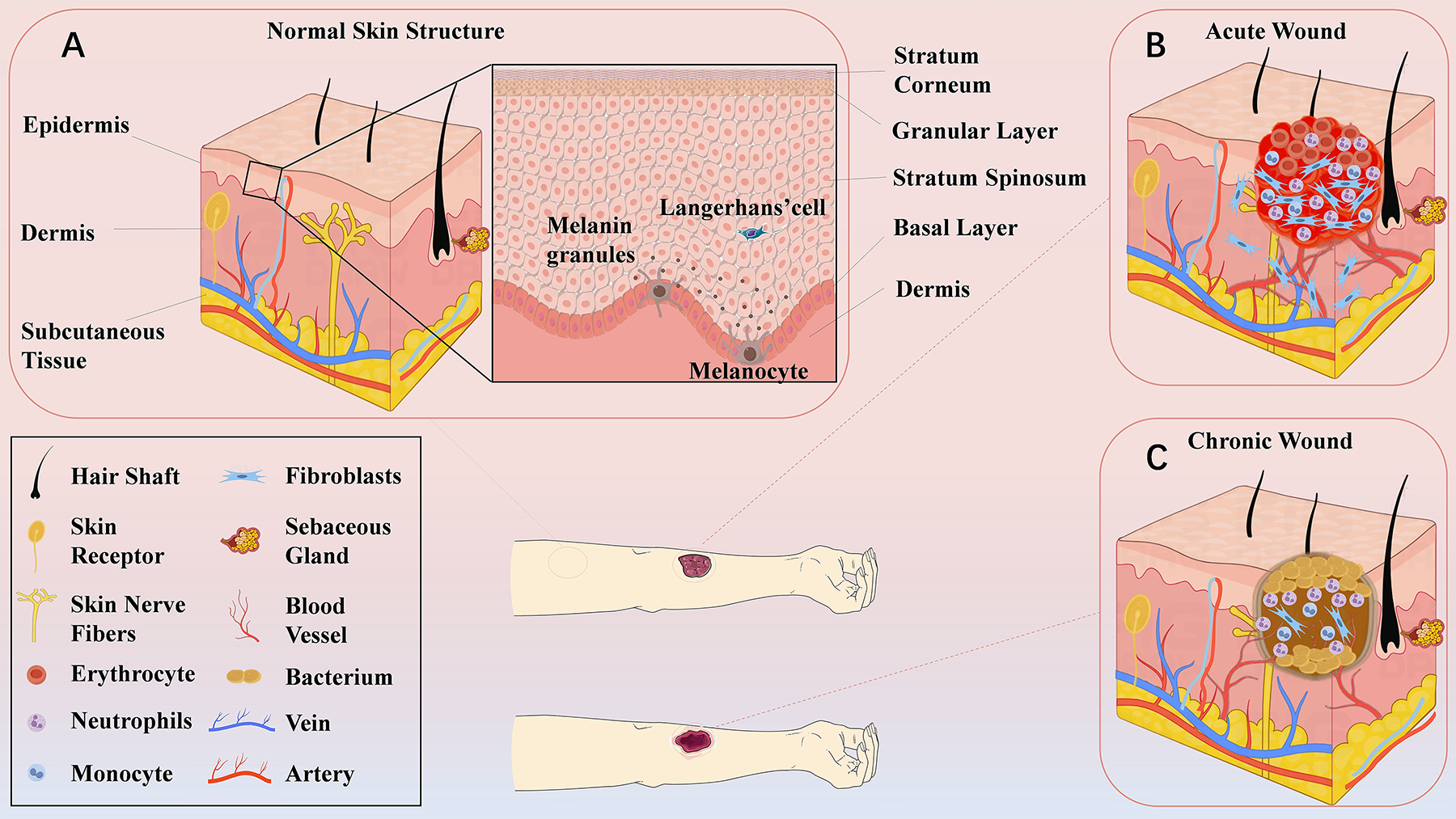
Normal cutaneous structure and damaged cutaneous structure.
Classification of cutaneous wounds
Cutaneous wounds are classified as acute or chronic (Fig. 1). 16 Acute wounds heal via the inherent repair capabilities, 18 while chronic wounds exhibit persistent dermal/epidermal disruption and impaired healing. Unlike trauma-induced acute wounds, chronic wounds primarily stem from (1) peripheral vascular disease, (2) metabolic disorders, and (3) immune dysfunction. Additional risk factors include obesity, aging, and smoking. 19 These contribute to common complications such as infection, metabolic dysregulation, and prolonged inflammation.
Functional Design and Fundamentals of Microneedles
Microneedles can effectively deliver therapeutic agents across the skin barrier. This section delves into the functional design and fundamental principles of microneedle systems, aiming to assist researchers in their rational design.
Functional design
Microneedles consist of a base for support and positioning and a needle for penetration and drug delivery. 6 Both the parameters and topological structure of the needle are the critical determinants of its functionality. The following sections will systematically elaborate on the specific effects of length, diameter, array density, and topological structure on microneedle performance.
Microneedle length
The structural thickness of human skin varies across different anatomical sites. This analysis primarily references the characteristic layered thickness of the inner forearm for discussion. To achieve effective drug delivery, microneedles must penetrate the epidermal layer (>0.1 mm) and reach the vascular-rich dermal layer (<2 mm).20,21 Consequently, microneedle lengths are predominantly designed within the 0.1–2 mm range. 22 The clinical implications associated with different microneedle lengths are summarized as follows: (1) 0.1–0.3 mm: enables epidermal penetration, enhancing the transdermal permeation efficiency of active ingredients 23 ; (2) 0.3–0.8 mm: accesses the papillary dermis, leveraging its high-density immune microenvironment (e.g., Langerhans cell clusters) to potentiate vaccine efficacy. For example, glioblastoma vaccines can utilize this mechanism to elicit specific CD8+ T cell responses 24 ; (3) 0.8–1.5 mm: reaches the reticular dermis, where the dense vascular and lymphatic networks facilitate enhanced delivery efficiency for macromolecular drugs such as insulin 25 ; and (4) 1.5–2.0 mm: while this depth contains high neural density that may induce pain, studies indicate its potential for modulating hair follicle activity in alopecia treatment. 26
Diameters and array density
Diameter balances penetration mechanics and neural sensitivity 21 : smaller diameters reduce the likelihood of stimulating nerve endings (decreasing pain) but risk structural bending; larger diameters improve stability and drug-loading capacity, but it requires greater insertion force and intensifies pain due to increased contact with neural tissue and amplified tissue trauma. 27 Array density impacts delivery: high density increases release rates and prevents occlusion via multichannel effects, but excessively high density can lead to the “nail bed effect,” where the skin is uniformly pushed down without being penetrated.27,28 Optimal design integrates both parameters: high-density/small-diameter arrays minimize discomfort in sensitive areas, while low-density/large-diameter configurations are suited for applications that demand the delivery of high-dose drugs or need to penetrate challenging, thicker cutaneous layers.
The topological structure of needles
Current microneedle tip configurations predominantly include conical and beveled geometries. To optimize penetration capability and tissue adhesion, researchers have developed specialized tip architectures.
Penetration optimization: Serrated tips, inspired by mosquito proboscis, reduce insertion force via vibrational motion during application, improving penetration with less discomfort. 29
Adhesion enhancement: Strategies focus on increasing microneedle–tissue friction to prevent shedding: (1) Swellable structures: hydrogels rapidly absorb interstitial fluid (e.g., CH-Arg/PVA hydrogel exhibiting 800 ± 50% swelling in phosphate-buffered saline 30 ), expanding intradermally to enhance mechanical anchorage. 31 (2) Bioinspired structures: designs mimicking natural systems (e.g., shark tooth barbs, 32 porcupine quill, 33 goosegrass microhooks 34 ) mechanically interlock with tissue via barbs to prevent displacement. 35 (3) Hybrid adhesion: combining vacuum-assisted suction and chemical bonding yields superior adhesion. For instance, a mussel-octopus bionic system integrates a polydopamine (PDA) hydrogel base (catechol-mediated chemical adhesion) with octopus-sucker-inspired conical tips featuring concave cavities for vacuum sealing. This provides robust adhesion in both dry and moist conditions (Fig. 2). 36 Needle topology is fundamental to penetration, drug delivery, and fluid extraction efficacy. Fabrication advances enable precise tailoring of these geometries for specific applications.21,27
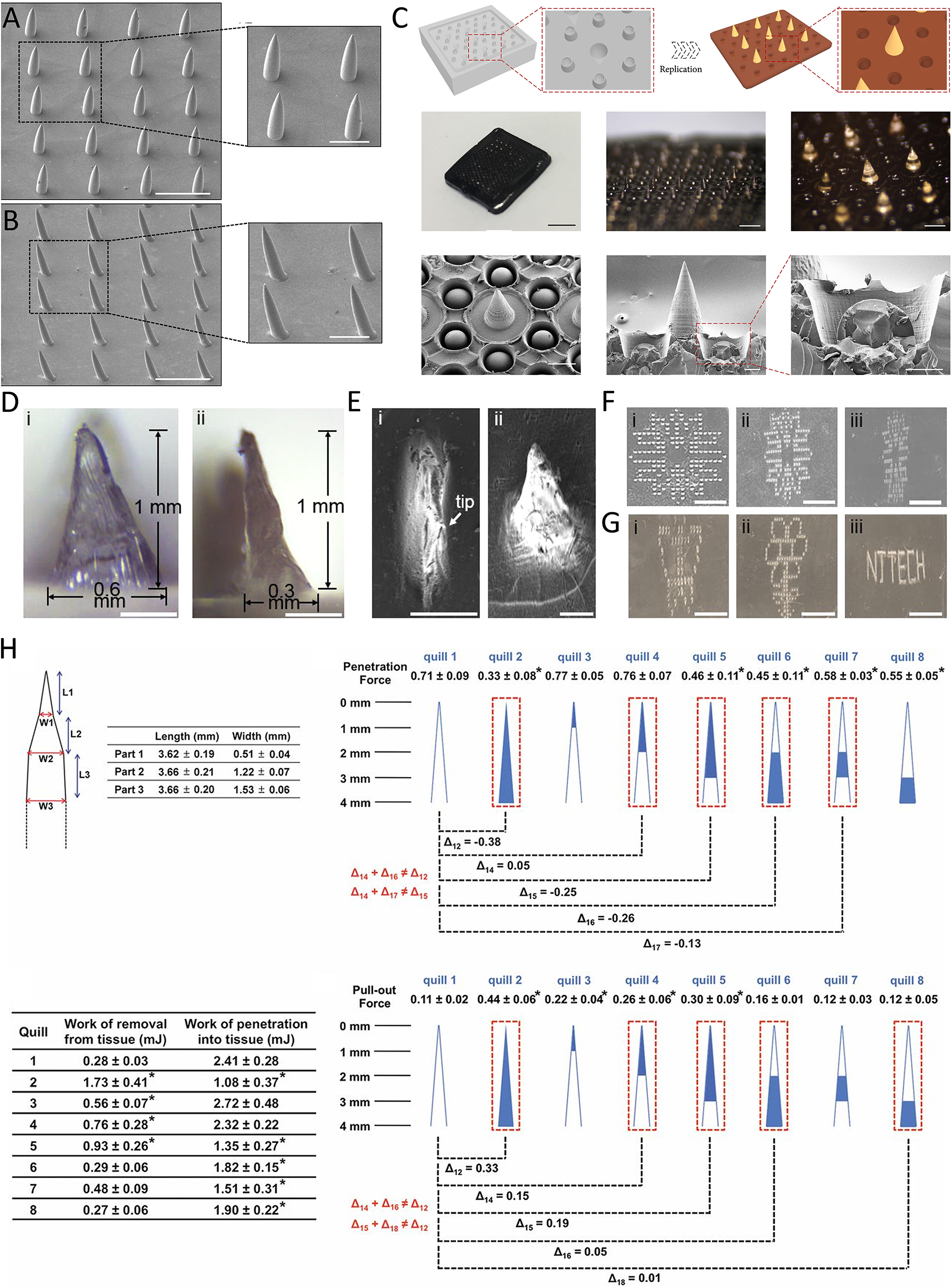
Biomimetic structure schematic diagram.32–34,36
In addition, needle physical structure, needle body angle, thickness, coating thickness, and the design of the base substrate all significantly impact performance.
Microneedle classification
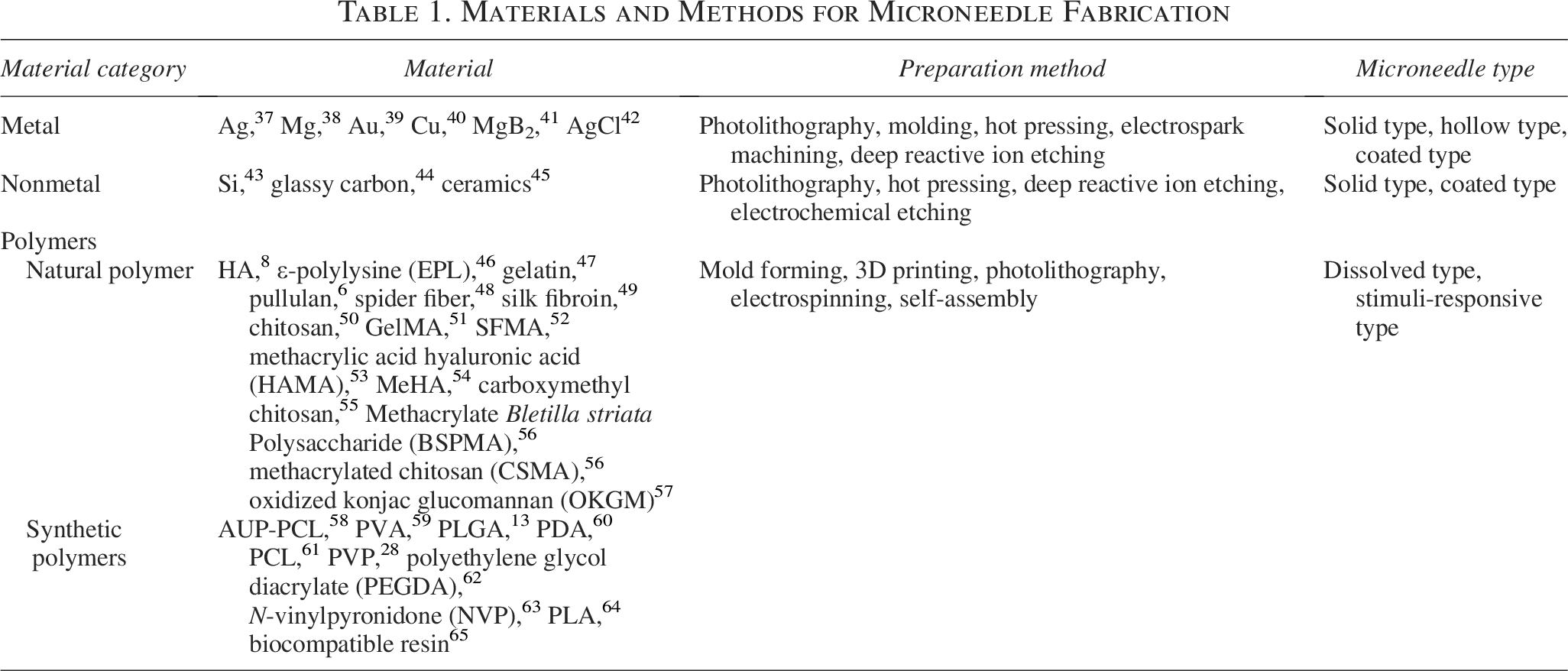
Building upon the design principles discussed earlier, we present a functional classification of microneedles that highlights the mechanism by which they exert their effect (Table 1 and Fig. 3).
Materials and Methods for Microneedle Fabrication
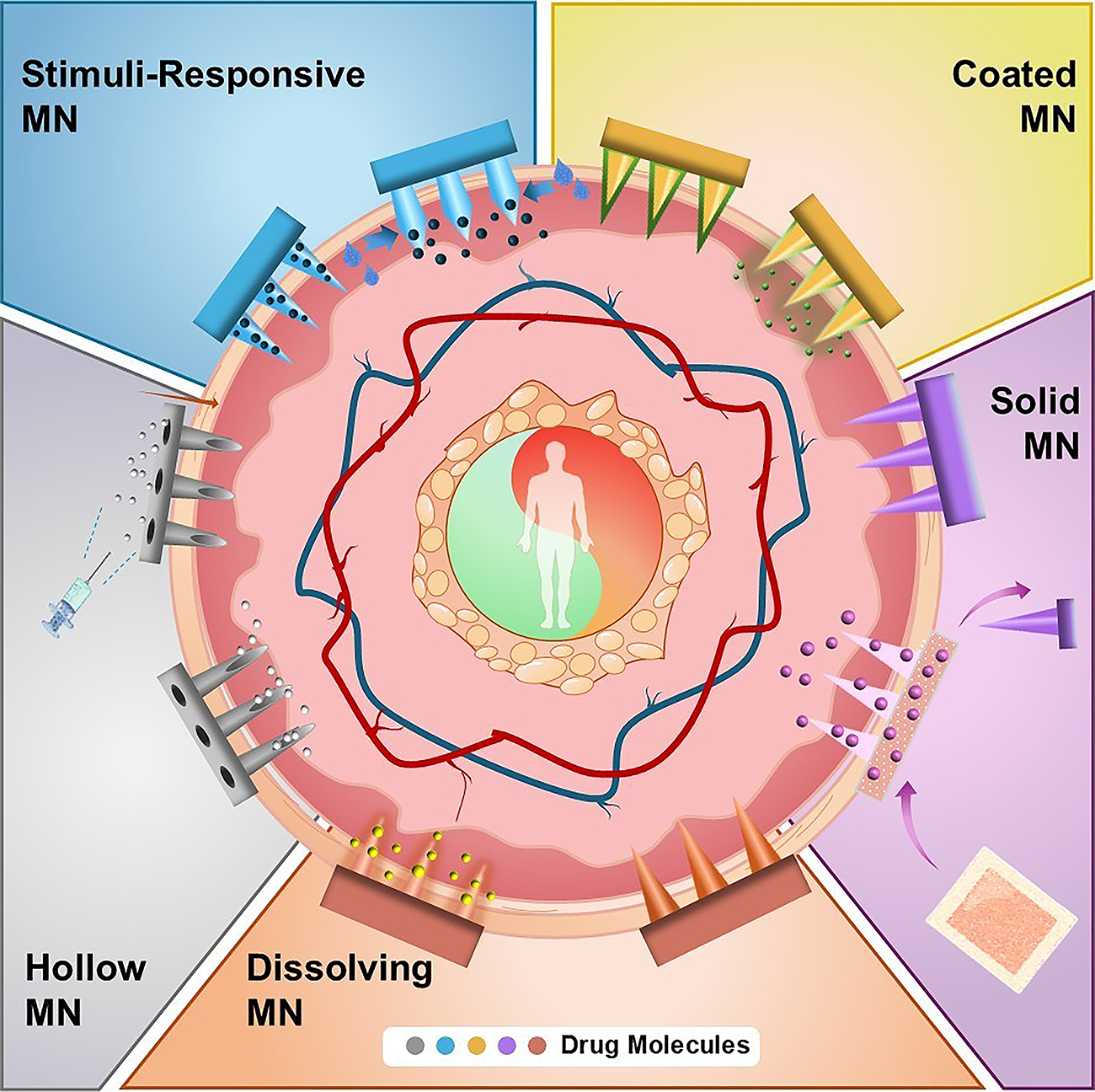
Classification of microneedles and their mechanisms of action.
Solid microneedles
Solid microneedles, fabricated from metals, silicon, or polymers, lack intrinsic drug-carrying capacity or delivery channels. Their mechanism of action involves creating microchannels through skin/biofilm/granulation tissue penetration, followed by passive drug diffusion via transdermal patch application.66,67 Metallic microneedles provide superior mechanical strength for deep tissue access, while degradation products (e.g., magnesium microneedles release Mg2+ and H2 during biodegradation, thereby regulating keratinocytes and exerting anti-inflammatory effects) enable synergistic therapy.38,40 These devices exhibit biocompatibility, supporting clinical safety and reusability.37,68 However, limitations include noble metal costs impeding mass production, 7 therapeutic dependence on secondary patches restricting standalone use, and risks of retained microtips triggering foreign body reactions that impair healing. 69
Coated microneedles
Coated microneedles feature a shaft surface coated with drug molecules, enabling barrier penetration for targeted drug delivery. This design increases local drug concentration, improving therapeutic efficacy, bioavailability, and controlled release. 70 Coated microneedle fabrication uses methods such as dip-coating and casting. 71 They are also suitable for in vivo sampling, as demonstrated by an alginate-peptide nucleic acid hybrid hydrogel coating that selectively captures specific miRNA through base complementation for detection. 72 Metallic-coated microneedles maintain structural integrity due to material stability, allowing repeated drug delivery.37,68 Silicon-based systems combine nanowire arrays with silver-catalyzed etching techniques to increase drug-loading capacity while maintaining puncture resistance. 43 Key limitation: restricted drug-loading capacity impedes high-dose applications, necessitating improved coating technologies for enhanced delivery efficiency and biomedical utility.
Dissolving microneedles
Dissolving microneedles are made of biodegradable materials. After insertion into the skin, they dissolve gradually, releasing encapsulated therapeutic agents. 59 This characteristic makes them an ideal platform for encapsulating nanocarriers, thereby enabling the precise delivery of nanotherapeutic agents to deep wound regions for targeted treatment. These microneedles require biocompatible materials to avoid toxicity from dissolved substances.8,52,59,73 Besides drug delivery, their degradation products can promote tissue regeneration by stimulating cell migration, angiogenesis, and collagen synthesis. 74 For example, hyaluronic acid (HA)-based systems modulate macrophage polarization (M1-to-M2 switching) to suppress inflammation while promoting CD44 receptor-mediated endothelial migration for vascularization, enhancing HA-assisted wound healing. 8 After dissolving, they restore tissue integrity and prevent additional damage from extraction.
Hollow microneedles
Hollow microneedles contain internal channels that allow drug injection under external pressure from a pump or syringe. They can be made of metals, silicon, or polymers. Hollow microneedles can deliver multiple drugs without repeated insertions, 75 with controllable drug release parameters including type, dose, and flow rate. These microneedles can incorporate internal electrodes to detect body substance concentrations. 37 Using silicon’s semiconducting properties, researchers have integrated microelectro-mechanical system 43 and biosensing modules 76 in microneedle lumens to detect interstitial fluid biomarkers for minimally invasive diagnostics. However, the internal channels may become blocked by cutaneous tissue, hindering drug injection. 27
Stimuli-responsive microneedles
Stimuli-responsive microneedles consist of hydrophilic hydrogels that absorb water and expand upon insertion into the body, interacting with surrounding tissues and anchoring the microneedles through the mechanism of the previously mentioned swellable structures. 31 The hydrogel absorption removes excess exudates from wounds. 77 By responding to pH and temperature changes, they control drug release and improve targeting. 52 Stimuli-responsive microneedles have greater drug-loading capacity than other types while delivering various therapeutic agents like growth factors, cells, and DNA. They are also easy to fabricate and cause little wound irritation, 78 making them promising for drug delivery and wound management.
This taxonomic system provides a framework for clinical compatibility screening of microneedle systems. However, current classification standards have three main limitations: (1) existing classification methods (by material composition, structure, and drug release mechanisms) lack a unified framework; (2) new microneedle technologies challenge traditional classification approaches; and (3) most importantly, there is no classification system guided by clinical translation principles.
Nanomaterial Classifications and Functions
Nanomaterials as drug carriers have been widely studied in cutaneous repair due to their drug-loading capacity and controlled-release properties. However, nanomaterials must be delivered to the deep wound regions to fully exert their therapeutic efficacy. Microneedle technology effectively addresses this delivery challenge, enabling a combination that yields significant synergistic enhancement. Recent studies have integrated nanomaterials with microneedle technology to synergistically enhance cutaneous repair efficacy. This section systematically classifies these microneedle-combined nanomaterials into organic and inorganic categories based on their chemical composition and elaborates on their mechanisms of action in promoting the cutaneous regeneration process.
Inorganic nanomaterials
Metal and metal oxide nanomaterials
Drug loading strategies for metal/metal oxide nanomaterials primarily encompass the following: covalent conjugation (e.g., Au–S bonds in gold nanoparticles 79 ) ensures payload stability but risks conformational changes; physical adsorption (e.g., polyethylenimine-modified silver carriers 80 ) offers simplicity with limited efficiency; mesoporous encapsulation (e.g., Fe3O4@SiO2 81 ) enhances drug capacity but requires burst release control.
These nanomaterials exert bactericidal effects via membrane disruption, enzyme inhibition, and reactive oxygen species (ROS) generation. 82 For example, silver nanoparticles release Ag+ ions that bind with sulfhydryl (–SH) groups in bacterial membranes, disrupting the electron transport chain and inhibiting nicotinamide adenine dinucleotide hydride dehydrogenase activity. The tannic acid-synthesized silver nanoparticles inhibit methicillin-resistant staphylococcus aureus (MRSA) and other resistant strains, 83 and silk fibroin microspheres (SFM)-AgNPs composite shows broad-spectrum antibacterial activity. 84 The Au-Cu2MoS4 (Au-Cu2MoS4 的缩写 [CMS]) nanoplatforms combine enzymatic glucose oxidase/catalase activity with photothermal effects.40,85
In tissue regeneration, copper nanomaterials activate MEK1/PDK1/PI3K proliferation pathways while promoting angiogenesis via NF-κB/HIF-1α regulation. 86 For anti-inflammatory applications, MnO2 nanoparticles convert excess ROS to oxygen via catalase/superoxide dismutase-mimetic (CAT/SOD) activity. 77 MgO nanoparticles release Mg2+ to induce M2 macrophage polarization, enhancing tissue repair and vascular formation to mitigate inflammation. 87
Metal-organic frameworks
Metal-organic frameworks (MOFs) are crystalline porous materials formed by metal ion-organic ligand self-assembly. For cutaneous repair drug delivery, MOFs must meet specific structural requirements: pore sizes 1.5–2 times larger than therapeutic molecules, 88 active group functionalization (e.g., amino/carboxyl) enhancing drug adsorption, 89 topological design improving hydrothermal stability and mechanical strength, 90 and stimuli-responsive (e.g., pH/light) properties enabling controlled release. 91 Common dermal MOFs include zinc-based ZIF-8 (Zn2+/2-methylimidazole), 51 iron-based MIL-101 (Fe³+/1,4-benzenedicarboxylic acid), 59 zirconium PCN-224 (Zr6+/5,10,15,20-tetrakis(4-carboxyphenyl)porphyrin), 92 magnesium Mg-MOF-74 (Mg2+/2,5-dihydroxyterephthalic acid), 93 and hybrid Zn-MOF-hydrogel systems. 94
These materials exert antimicrobial effects through metal nodes (Cu2+/Ag+/Zn2+) and ligands (imidazole/porphyrins), disrupting biofilms via charge-modulated hydrophobicity,51,95 with ZIF-8 exemplifying multimechanism action via membrane damage, glutathione (GSH) depletion, ROS induction, and anti-inflammatory cytokine upregulation.54,96 MOFs also exhibit anti-inflammatory, proangiogenic, and tissue-regenerative properties. The gallic acid/Cu-based MOF (CuGA-MOF) system releases Cu2+ to prolong therapeutic time while reducing cytotoxicity. Cu2+ drives neovascularization via HIF-1α/vascular endothelial growth factor (VEGF) signaling. 97
Silicon nanomaterials
Silicon nanomaterials provide high drug-loading capacity, surface modifiability, and biocompatibility. Mesoporous silica nanoparticles (MSNs) incorporating betamethasone dipropionate offer a new psoriasis treatment strategy. MSNs regulate drug adsorption/release and provide targeting, enhancing local drug efficiency. 57 Intracellular degradation of MSNs releases Si2+ ions that activate HIF-1α/VEGF signaling to drive angiogenesis via endothelial progenitor cell recruitment. 98 Thiol-functionalized MSNs modulate NF-κB-mediated inflammation through surface sulfhydryl groups.99,100 For diabetic wounds, silicon nanoparticles coloaded with glucose oxidase and metformin reduce local glucose while generating antibacterial ROS, promoting wound healing. 101
Organic nanomaterials
Polymer nanomaterials
Polymer nanomaterials provide biocompatibility, diverse fabrication methods, and controlled drug delivery. Some exhibit biological activity: chitosan nanomaterials use cationic surfaces to enhance cell migration through electrostatic membrane interactions 102 and show broad-spectrum antibacterial activity. 103 PDA nanomaterials reduce inflammation by scavenging radicals and inhibiting NF-κB signaling and NLRP3 inflammasome assembly. 104 These materials encapsulate antibacterial agents for microneedle delivery into biofilms, releasing agents upon nanoparticle dissolution.
Exosomes
Exosomes are cell-derived nanovesicles with biocompatibility, targeting precision, and modifiability. 105 In wound repair, the core function of exosomes is to regulate inflammatory pathways and drive vascular regeneration. Platelet-derived exosomes (PLT-Exos) reduce inflammation via NF-κB inhibition and macrophage polarization, while promoting angiogenesis through VEGF/fibroblast growth factor activation. 106 Mesenchymal stem cell exosomes activate fibroblasts, endothelial cells, and macrophages to drive vascular remodeling and immune balance. 107 Human mesenchymal stem cell exosomes polarize macrophages to M2 by suppressing NF-κB and upregulate VEGF/HIF-1α to enhance regeneration.108,109 Rejuvenated fibroblast exosomes (Y-EXO) improve aged cutaneous repair by accelerating healing, increasing collagen, and reducing IL-17A. 110 During wound repair processes, M2 macrophage exosomes promote angiogenesis via Wnt/β-catenin signaling in granulation tissue, optimizing the regenerative microenvironment. 111
Liposomes
Liposomes are phospholipid vesicles that encapsulate DNA, proteins, and small molecules for controlled drug delivery. 60 Functionalized liposomes loaded with NACHT, Leucine-Rich repeat, and pyrin Domains-Containing Protein 3 (NLRP3) inhibitor MCC950 reduce inflammation by polarizing macrophages from M1 to M2 and enhancing fibroblast–endothelial communication, improving tissue regeneration. 112 A macrophage-derived liposome system delivers purpurolide C (PC), which inhibits NF-κB phosphorylation to regulate macrophage function. This system enhances PC bioavailability and accelerates diabetic wound healing through polarization reprogramming. 113
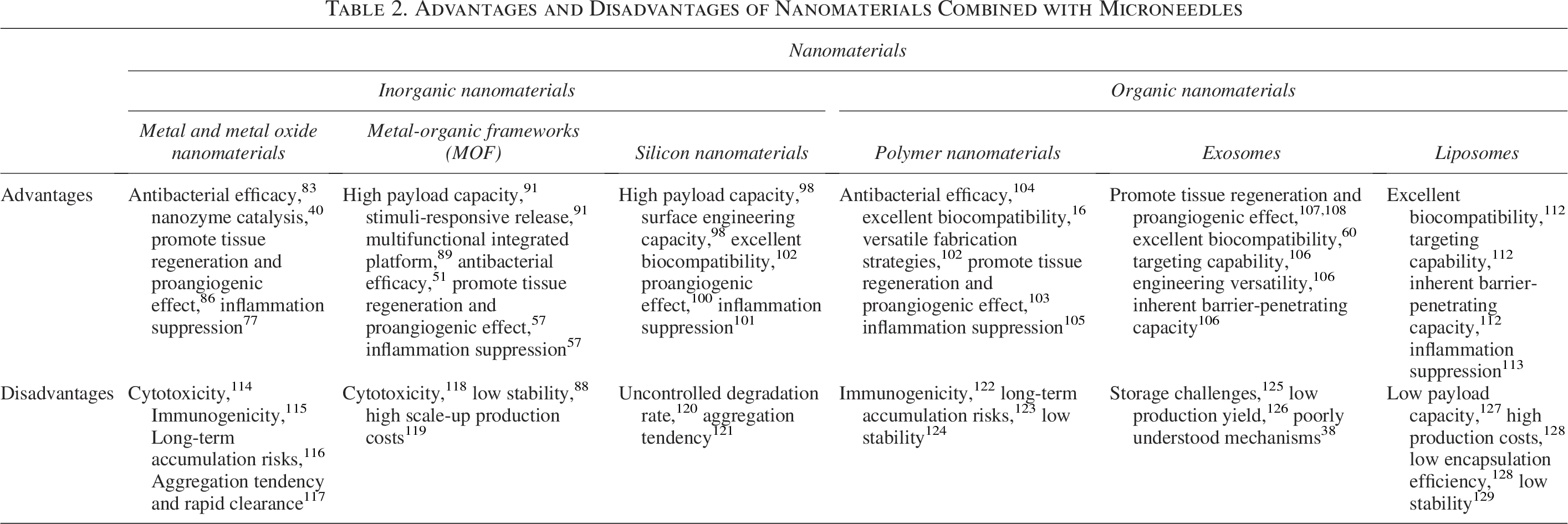
Through a systematic review of the aforementioned content, it can be observed that inorganic nanomaterials confer antibacterial and enzyme-mimetic catalytic functions through their physicochemical properties, enhancing wound therapy efficacy. Organic nanomaterials provide biocompatibility and targeting capabilities for precision treatment. Integration with microneedle platforms enables precise regulation of wound healing processes. However, clinical application faces challenges: inorganic nanomaterials need long-term biosafety evaluation, while organic nanomaterials face immunogenicity risks and stability issues. To provide a clearer overview of current research progress, Table 2 systematically summarizes the performance characteristics and limitations of commonly used nanomaterials in microneedle technology.
Advantages and Disadvantages of Nanomaterials Combined with Microneedles
Synergistic Mechanisms of Microneedle–Nanomaterial Systems for Cutaneous Repair
Building upon the methodically investigated and elucidated individual therapeutic mechanisms of microneedles and nanomaterials in wound management, this chapter centers on the microneedle–nanomaterial composite system. It summarizes three ubiquitous pathological barriers: (1) pathological scar formation, (2) bacterial colonization, and (3) localized excessive inflammatory responses.
Promoting normal wound healing and alleviating scar formation
During wound repair, moderate scarring is normal. However, dysregulated repair can cause hypertrophic scars (HS), driven by fibroblast hyperproliferation and excessive extracellular matrix accumulation. 130 HS impairs healing and causes aesthetic and psychological impacts. HS treatment requires suppressing cell overgrowth while addressing drug delivery challenges through thickened cutaneous barriers. 131
Inhibition of fibroblast proliferation
Suppressing aberrant fibroblast proliferation is key to reducing pathological thickness in HS. Studies show that miR-141-3p inhibits HS fibroblast proliferation but is downregulated in pathological microenvironments. To overcome this, researchers developed a microneedle exosome delivery system that precisely transports miR-141-3p-overexpressing exosomes (miR-141-3p-OE-Exos), inhibiting fibroblast proliferation in HS models (Fig. 4A). Histological analysis demonstrated a significant reduction in scar thickness and restoration of organized fibroblast architecture in the experimental group compared with controls (Fig. 4A), confirming that microneedle-delivered exosomes effectively inhibit HS formation. 8
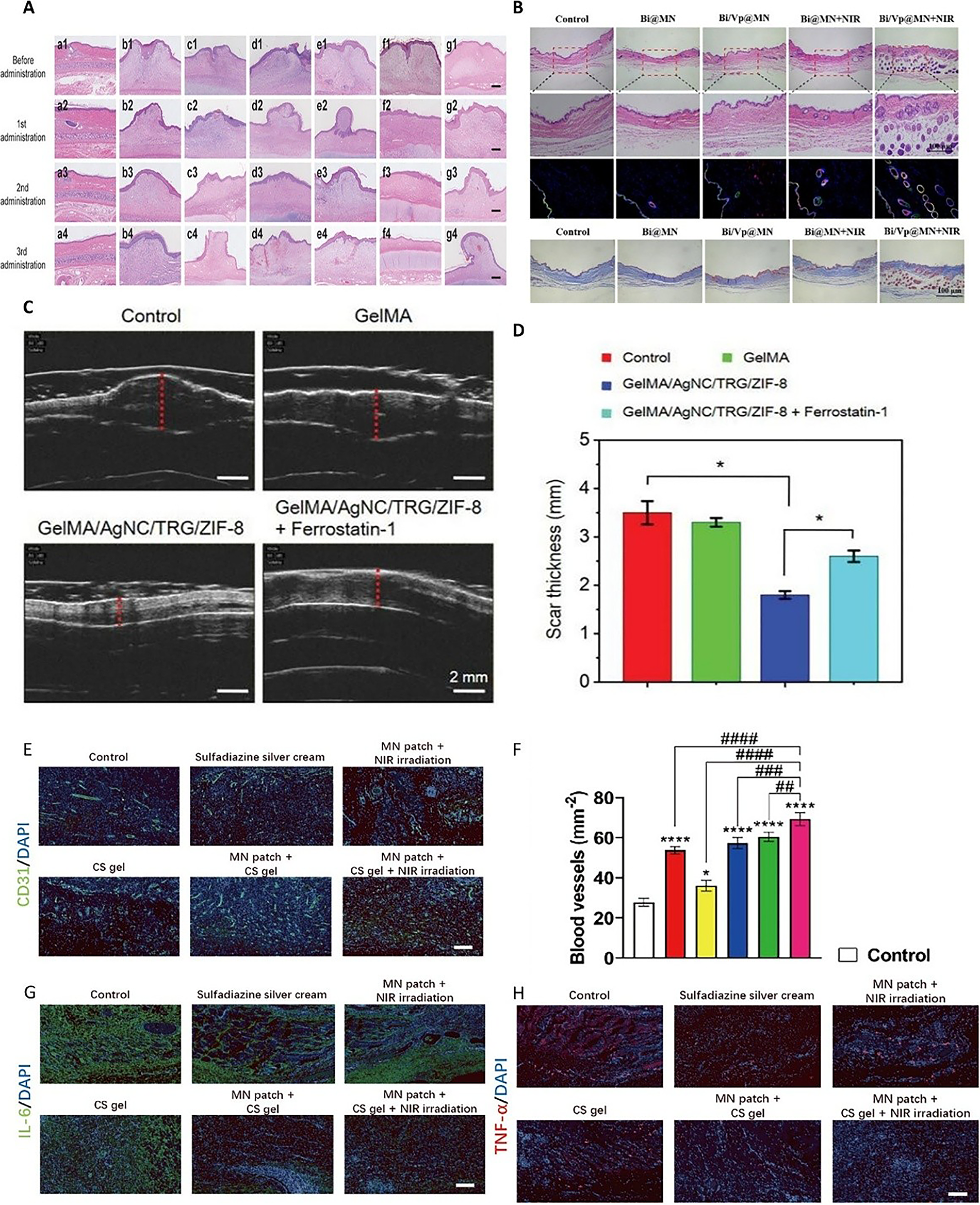
Building on synergistic therapeutic principles, a bismuth nanosheet-verteporfin (Vp) composite microneedle penetrates scar tissue/biofilms for dual-action therapy. Bismuth exerts broad-spectrum antibacterial effects, while Vp inhibits the yes-associated protein (YAP) pathway to block fibroblast hyperproliferation. Longitudinal monitoring confirmed complete prevention of pathological scarring within 90 days, with tissue progressively normalizing to native morphology (Fig. 4B). 52
Ferroptosis
Ferroptosis plays a pivotal role in the treatment of HS. Pathological analysis reveals iron metabolism dysregulation in HS myofibroblasts, which activates the ferroptosis process. To promote this therapeutic mechanism, Dr. Bin Zhao’s team constructed an AgNC/TRG/ZIF-8 composite by coloading silver nanoclusters (AgNC) and trigonelline (TRG) into ZIF-8 frameworks, delivered via microneedles. This system promotes myofibroblast ferroptosis: ZIF-8/AgNC reduced GSH by 50% versus controls, while TRG suppressed GPX4 activity and NRF2 pathway—key ferroptosis regulators. α-smooth muscle actin (α-SMA) and collagen I/III were downregulated in HS tissues. Microneedle delivery reduced HS thickness from 3.5 ± 0.3 mm to 1.8 ± 0.1 mm after 3 weeks (Fig. 4C, D). 51
Remodeling the pathological microenvironment of HS
Remodeling the pathological microenvironment of HS is a crucial strategy for reducing abnormal scar formation. Studies have demonstrated that the precise delivery of 5-fluorouracil (5-Fu) via a microneedle system, when encapsulated in sodium carboxymethyl cellulose nanoparticles, plays a significant role. As a pyrimidine analogue with antimetabolic activity, 5-Fu effectively inhibits fibroblast proliferation and suppresses abnormal angiogenesis by regulating the Bcl-2-associated death promoter, insulin-like growth factor 1 receptor (IGF1R) pathway, remodeling the pathological microenvironment of HS, and promoting normal wound healing. 132 Microneedle-delivered nanomaterials increase neovascular density to 57.2 ± 2.3/mm2, reduce IL-6/TNF-α to 29.84 ± 2.46% of controls, alleviate microcirculatory dysfunction, and create a prohealing immune microenvironment (Fig. 4E–H). 101
Anti-inflammatory and regenerative strategies
Anti-inflammatory and regenerative strategies play a pivotal role in the artificial intervention of wound healing processes. Among these, antimicrobial action, as a key component of anti-inflammatory measures, will be elaborately discussed in Antibacterial strategy.
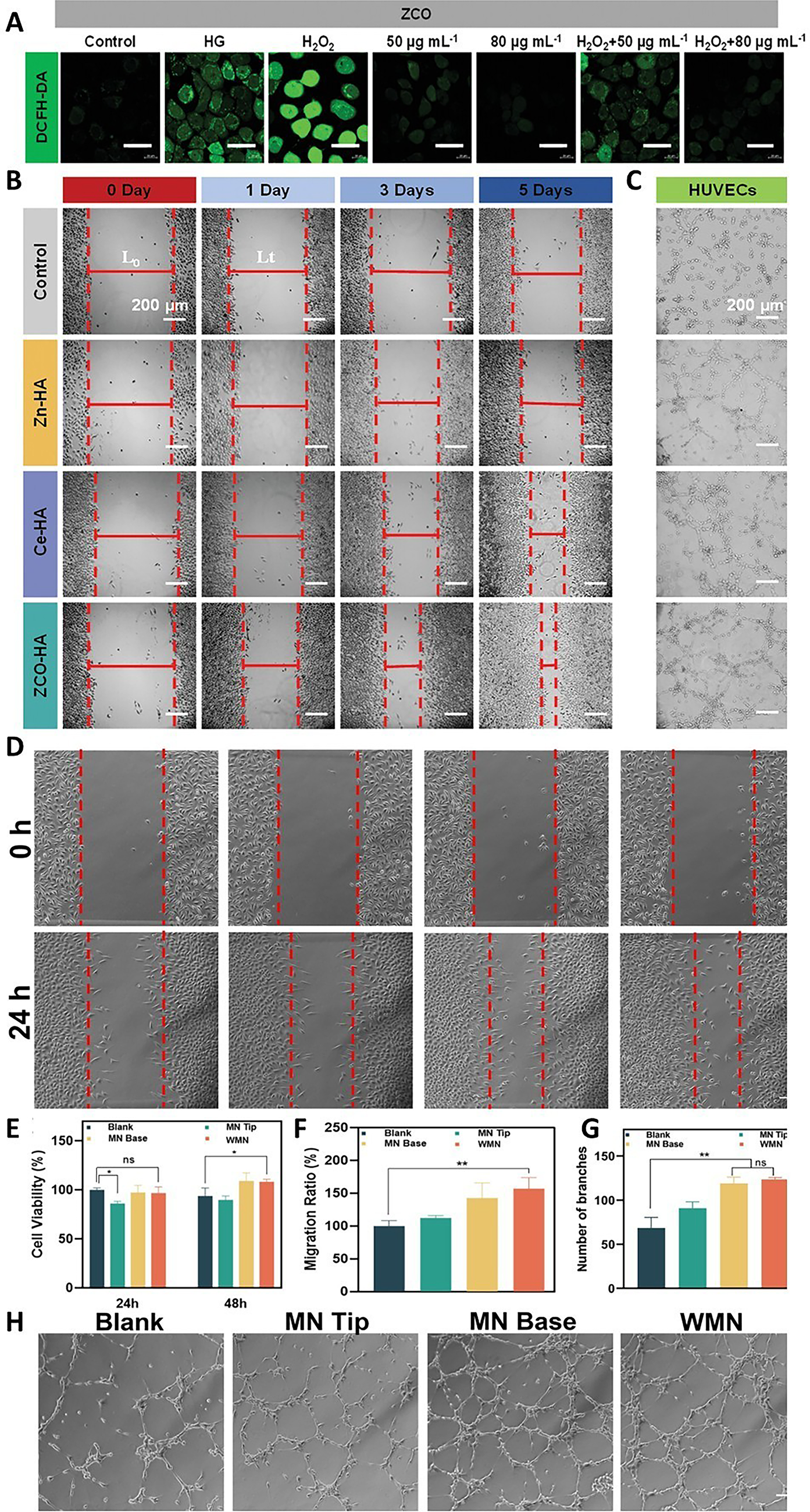
Metal nanomaterials show anti-inflammatory/regenerative dual functions. Dr. Juan Yang’s zinc-cerium oxide (ZCO) nano-system releases Zn2+/Ce³+/Ce4+ via microneedles. Against MRSA, the minimum inhibitory concentration (MIC) is 80 μg/mL and the minimum bactericidal concentration (MBC) is 140 μg/mL, with 24 h complete inhibition. ZCO nanozymes with SOD/CAT activity reduce oxidative stress by scavenging ROS (Fig. 5A). Microneedle-controlled release prevents Zn2+ burst toxicity during cell proliferation and angiogenesis (Fig. 5B, C). 82 Shengbo Li’s glucose oxidase (Gox)/HA-functionalized PDA-iron oxide nanoparticles combine chemodynamic therapy (CDT). After microneedle delivery, they decompose in acidic/GSH-rich microenvironments, releasing GOx, Fe, and PDA. GOx converts glucose to gluconic acid + H2O2, fueling Fe-mediated CDT to enhance antibacterial and healing effects. 101 Vascular regeneration advances include Li Yang’s deferoxamine nanoplatform promoting angiogenesis. 133 QHREDGS peptide with microneedles increases cell migration by 147.7%, improving vascular parameters (1.8× branch points, 86% longer tubules vs. baseline) (Fig. 5D–H). 59 Mechanistically, M2 macrophages drive vascularization via VEGF paracrine signaling. 134
Antibacterial strategy
Bacterial infection significantly disrupts the physiological process of cutaneous repair, exacerbates local inflammatory responses at the wound site, and thereby delays the healing process. Moreover, bacterial infection poses a risk of triggering systemic infections such as sepsis and septicemia, which constitute a severe threat to the patient’s life safety. Particularly for diabetic wounds, the combined effects of disrupted glucose metabolism, vascular structure destruction, and impaired immune function at the wound site make them more susceptible to bacterial invasion and infection. 140 Therefore, the development and implementation of effective antibacterial strategies are of paramount importance for promoting optimal wound healing and ensuring the life safety of patients. Nanomaterials can load antibacterial active substances such as antibiotics141,142 antibacterial peptides143,144 and plant extracts 145 , achieve targeted delivery of these active substances to the wound site, and then exert efficient local antibacterial effects. The related technical schemes described subsequently mostly adopt the strategy of combination with other antibacterial technologies to synergistically enhance the antibacterial efficacy.
Photodynamic therapy
Photodynamic therapy (PDT) generates antibacterial ROS via photosensitizer activation at specific wavelengths. 53 A Dimethyloxalylglycine (DMOG) @PCN-224 MOF coloaded with meropenem (MEM) in HA microneedles releases nanoparticles upon delivery. Under 650 nm laser, nanoparticles convert O2 to 1O2/OH, synergizing with MEM to achieve equivalent sterilization at lower antibiotic doses than monotherapy (Fig. 6A–C). Furthermore, DMOG activates HIF-1α to stimulate neovascularization, combining with PDT for 96.4 ± 0.7% wound closure by day 11 (Fig. 6D). 92 For sustained antimicrobial effects, Cu2+-doped Zn2GeO4 long-afterglow nano catalysts (ZGC), preactivated by laser, continuously produce ROS via cascade reactions (Fig. 6C). Experimental results demonstrated a significant reduction in MRSA viability under prolonged illumination (Fig. 6E–I). 136
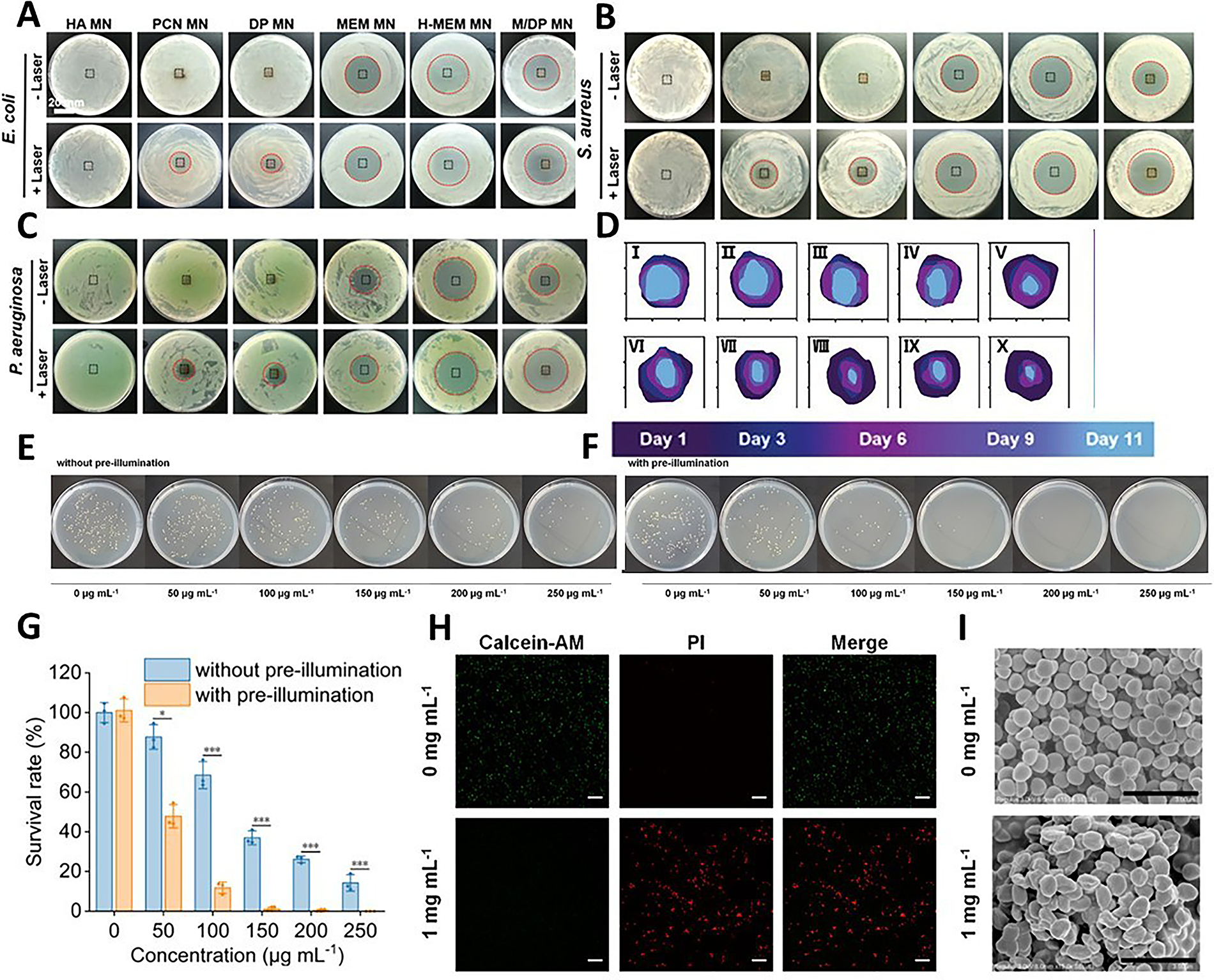
Representative photographic images of inhibition zones against
Photothermal therapy
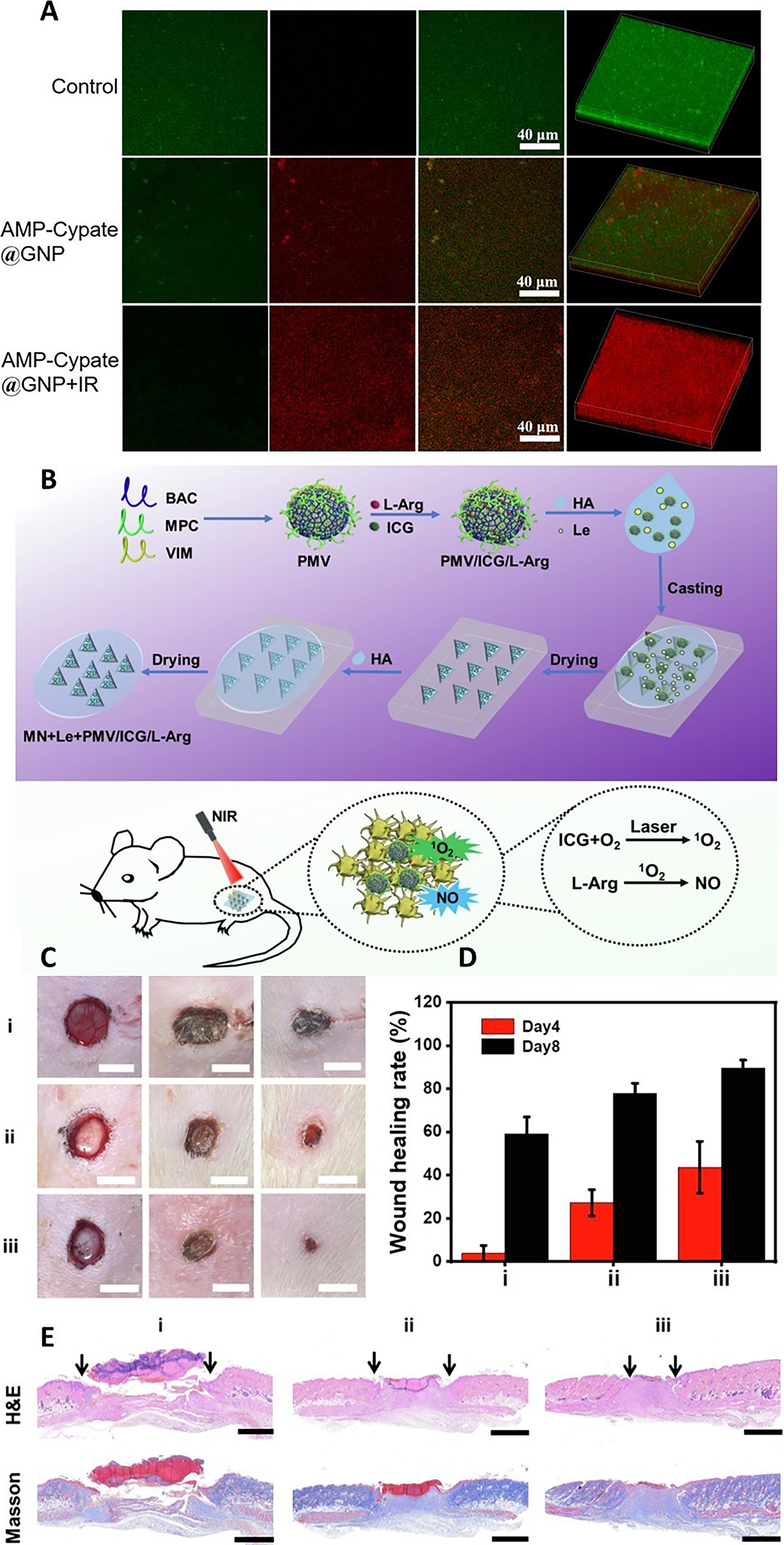
Photothermal therapy (PTT) uses photosensitizers to convert specific-wavelength light into heat, eliminating bacteria through hyperthermia while avoiding antibiotic resistance. 52 MnO2 NPs and PDA materials show photothermal antibacterial effects under near-infrared radiation (NIR) light.77,101 Lei Xiaoling’s team encapsulated antimicrobial peptide (AMP)-Cypate in gelatin nanoparticles (GNPs) for microneedle delivery, combining peptide activity with photothermal effects. At 6 μg/mL, this system achieves >90% killing of Staphylococcus aureus, with MIC90 reduced from 6 to ∼4 μg/mL under NIR (Fig. 7A). 135 Furthermore, PTT-generated heat can propel nanoparticles, as demonstrated by a microneedle-delivered nanomotor system (PMV nanogel/indocyanine green (ICG)/L-Arg). NIR-activated ICG provides direct antibacterial effects and drives nanomotor penetration; concurrently, heat-triggered NO release from L-Arg inhibits bacterial proliferation by disrupting DNA repair. Animal studies confirmed a 90% wound healing rate after 7 days with NIR treatment, supported by histological evidence of reduced granulation tissue gaps (Fig. 7B–E). 139
Ultrasonic response
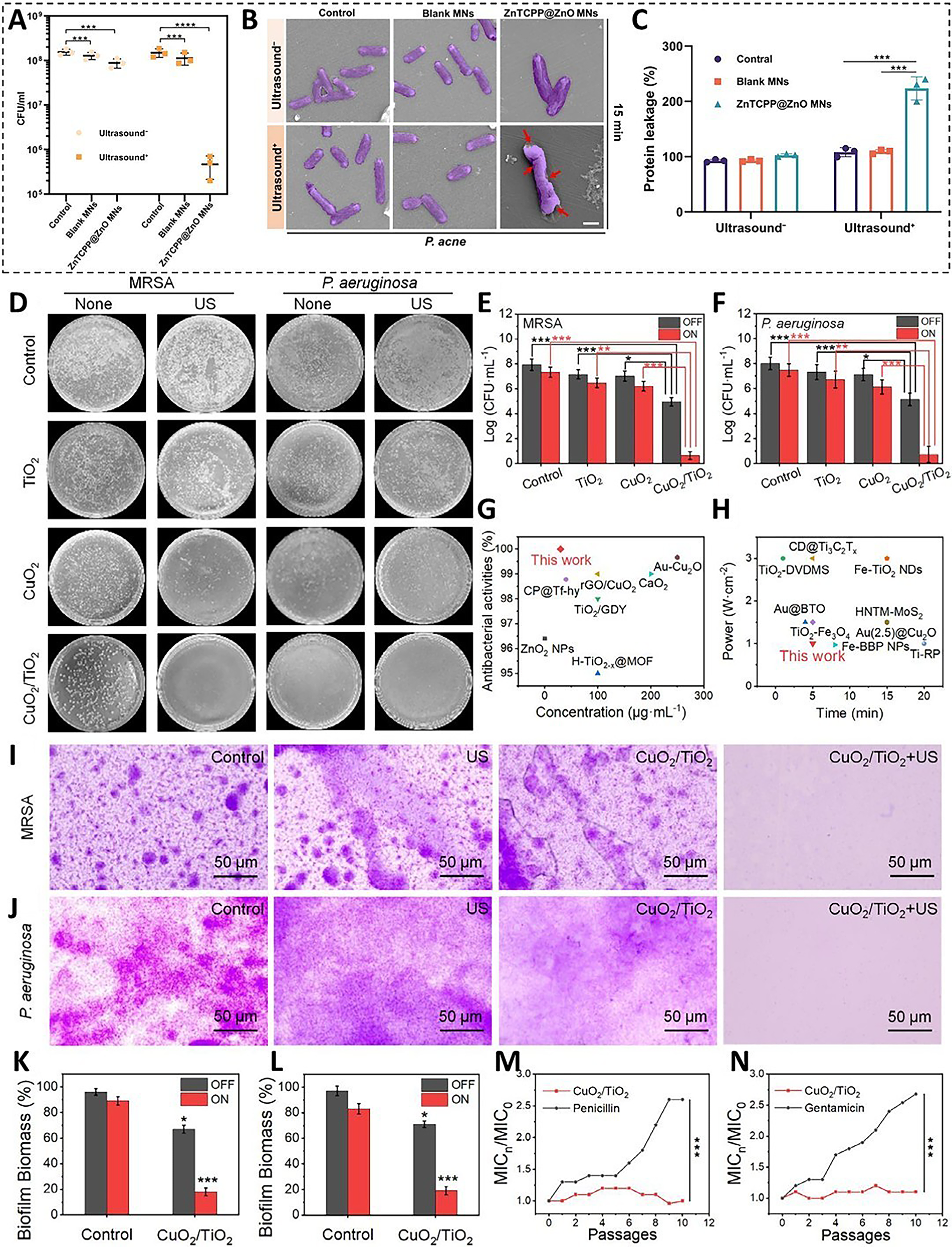
Ultrasound-responsive materials absorb, reflect, scatter, and propagate sound waves. Ultrasound penetrates skin and connective tissues beyond 5 cm depth. Based on this, Xiang Yiming’s team developed zinc tetracarboxyphenyl porphyrin (ZnTCPP) @ZnO MOF/ZnO composites delivered by microneedles. Under ultrasound, this system generates ROS for sterilization while enhancing catalytic efficiency and reducing energy consumption. Against Propionibacterium acnes, ultrasound-activated treatment achieved 99.73% antibacterial efficacy (Fig. 8A–C). 95 TiO2 is a classical sonosensitizer, producing ultrasound-triggered ROS with high stability and biocompatibility. 137 Recent CuO2/TiO2 heterostructures—combining ultrasmall CuO2 nanoclusters and oxygen-deficient OV-TiO2 nanosheets—enable synergistic CDT/sonodynamic therapy. This eradicated 82% of MRSA and 81% of Pseudomonas aeruginosa biofilms, with >7-log reduction (>99.99% inhibition) in bacterial colonies (Fig. 8D–N). 138
Enzymes
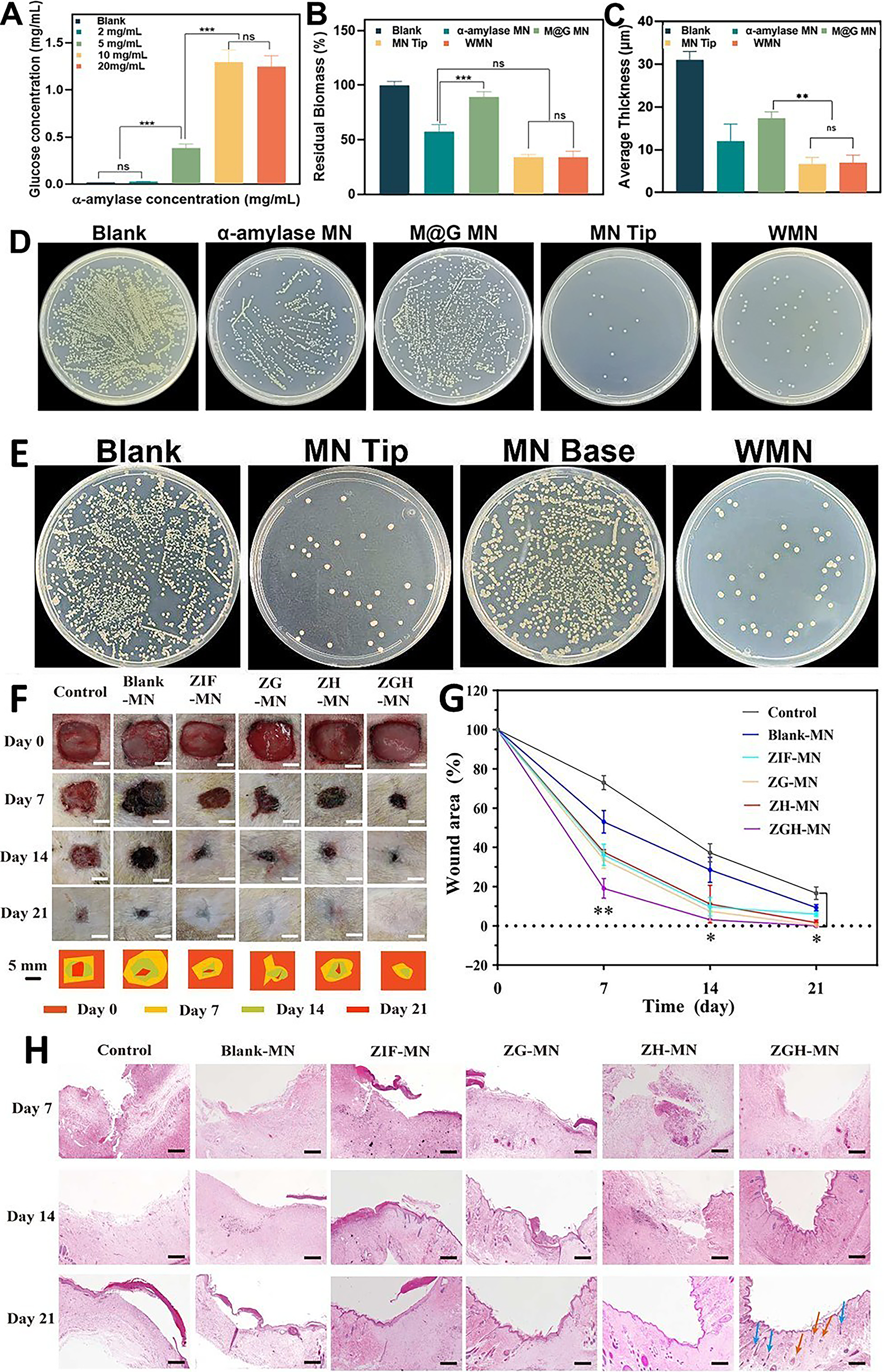
Hypoglycemic therapy corrects dysregulated glucose metabolism in diabetic wounds, improving immune function and enhancing autologous immune cell antibacterial capacity. Enzymes such as GOx effectively lower blood glucose. Loading GOx into MOFs protects it from degradation before reaching wounds, increasing utilization efficiency.54,59 Traditional agents (e.g., metformin and insulin) delivered via microneedles also achieve glycemic control. 141 The enzyme cascade strategy enhances antibacterial efficacy. Researchers constructed a microneedle system coloading α-amylase and GOx into MIL-101: α-amylase degrades bacterial EPS to disrupt biofilms while generating glucose; GOx utilizes wound glucose (including EPS products) to produce H2O2; MIL-101 catalyzes H2O2 conversion into ROS for sterilization. This achieves 90% antibacterial efficiency (Fig. 9A). 59 Further work developed a biofuel cell–microneedle system coencapsulating GOx/horseradish peroxidase in ZIF-8, controlling glucose through metabolism while generating anti-inflammatory microcurrents. It achieves complete wound healing by day 21, outperforming controls (Fig. 9B). 54
The microneedle–nanomaterial system addresses three core wound management challenges: (1) precise fibroblast modulation enabling restorative healing with minimal scarring, (2) inflammatory response regulation, and (3) multidimensional antimicrobial protection. These capabilities establish it as a versatile platform for comprehensive wound healing. However, clinical translation faces three obstacles: first, most studies rely on standardized animal models (e.g., murine full-thickness defects) that poorly replicate human chronic wound complexity; second, synergistic therapeutic interactions are poorly understood with inadequate combinatorial toxicity assessment; and third, unified efficacy evaluation standards are lacking.
Bibliometric Analysis of Keywords and Prediction of Hot Spots
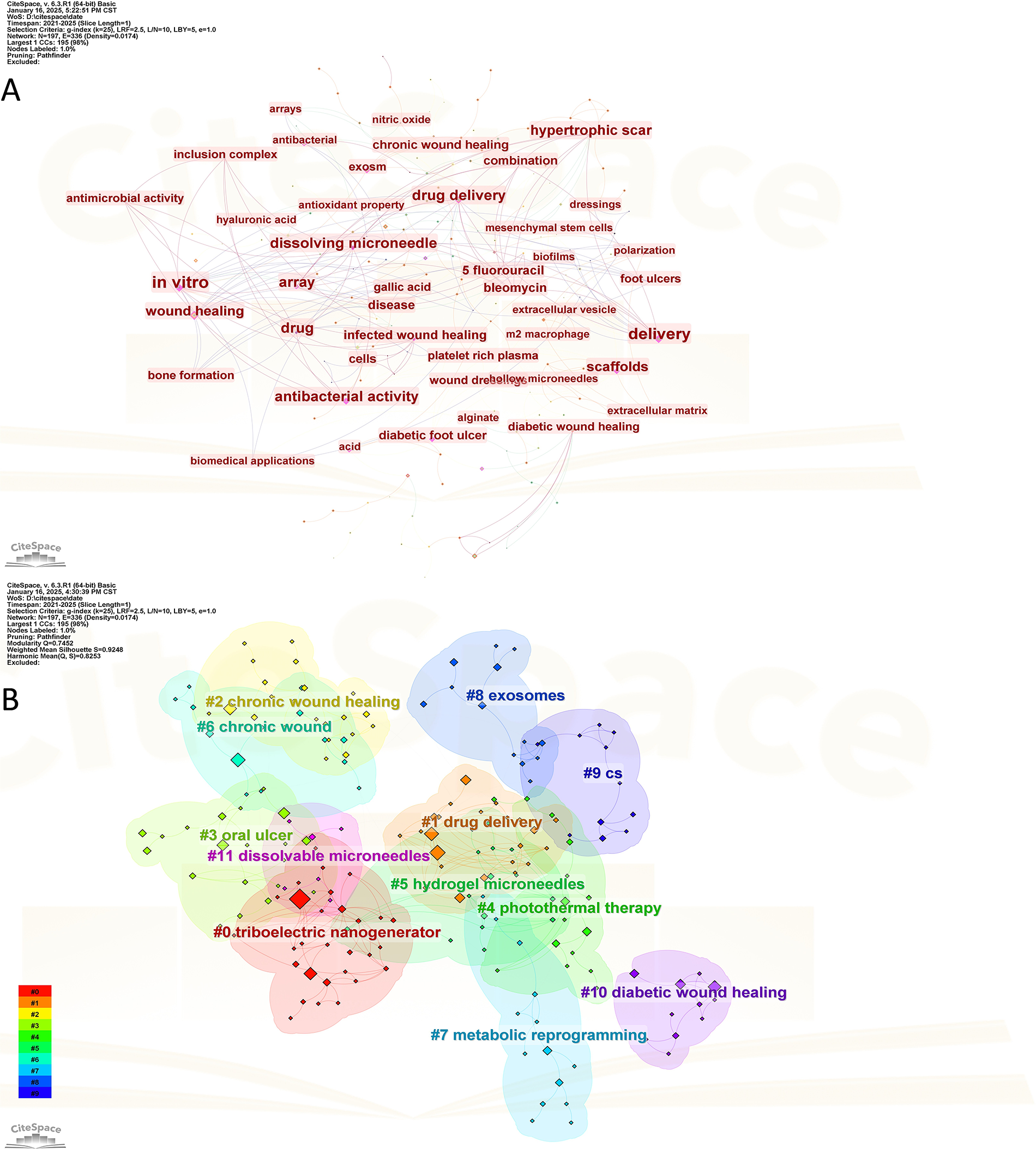
To evaluate the research value and potential of the microneedle–nanomaterial combination strategy, we first conducted an analysis of the trends in the relevant field. Systematic examination of the Web of Science literature on microneedles and wound healing identified current hotspots. Keywords appearing >5 times were visualized (Fig. 10A). Cluster analysis identified key themes including, chronic wound healing, drug delivery, photothermal therapy, exosomes, and dissolvable microneedles, as primary research focuses (Fig. 10B). Chronic wound healing emerged as the primary focus, with nanomaterials such as nanomotors and exosomes playing significant roles.
Keyword map of the paper.
These findings indicate substantial interest in microneedle-mediated nanomaterial delivery for wound healing. However, comprehensive reviews systematically discussing this combination remain scarce. Therefore, exploring this integration is timely and valuable.
Summary and Future Perspectives
Effective cutaneous repair is vital, and artificial intervention is required when natural healing is impaired. Since their introduction in the early 20th century, microneedles have been proven to effectively enhance tissue repair. However, their functionality as standalone drug carriers is limited. To address this limitation, researchers have focused on developing more advanced delivery systems. As indicated by the bibliometric analysis above, combining microneedles with nanomaterials has emerged as a current research hotspot. It has been demonstrated that nanomaterials can serve as highly efficient drug delivery platforms, which synergize with microneedle technology to significantly improve therapeutic outcomes. (Table 3)
Nanomaterial-Encapsulated Drugs and Their Treatment for Cutaneous Injuries
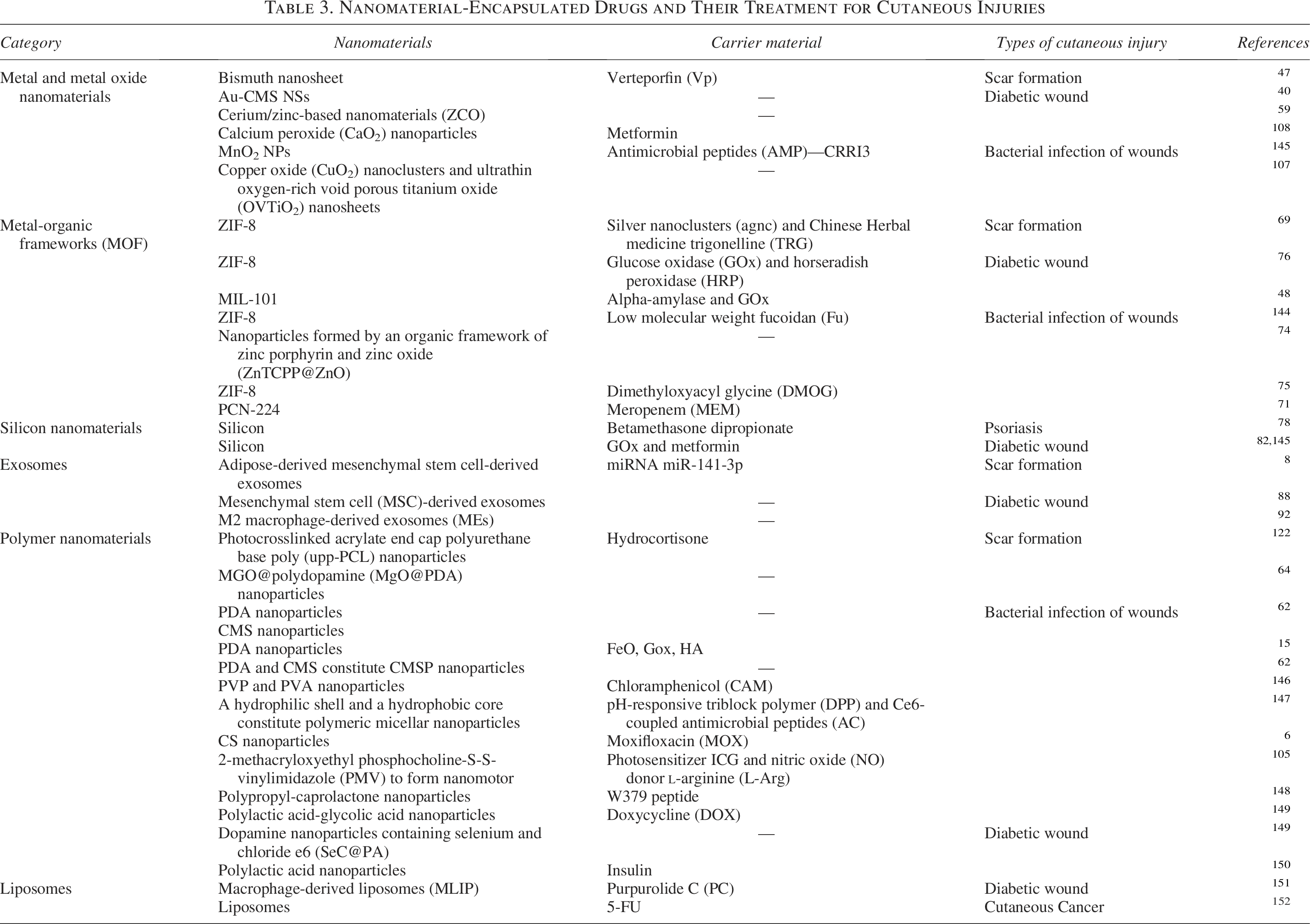
To address complex wound environments, microneedles can be tailored through parameters (length, diameter, tip design, array specifications), materials (metals, nonmetals, hydrogels), fabrication techniques (photolithography, 3D printing, molding), and delivery systems (solid, coated, dissolving, hollow, hydrogel microneedles). Nanomaterials serve as drug carriers—including metal/metal oxides, MOFs, exosomes, and polymers—enabling controlled release and functioning in wound healing stages such as antimicrobial action, nanozyme catalysis, and anti-inflammatory regulation. Integrating nanomaterials with microneedles effectively treats pathological scars, infected wounds, and diabetic wounds, aiding clinicians in wound management by shortening healing time and reducing patient burden.
For improved wound management and reduced burdens from repeated testing, closed-loop microneedle systems represent a key future direction. As Section “Synergistic Mechanisms of Microneedle-Nanomaterial Systems for Cutaneous Repair” details, metal/silicon-based conductive microneedle systems show potential here. For diabetic wounds, they integrate miniature sensors for real-time glucose monitoring, enabling algorithm-regulated drug release.61,140 Multilayered delivery systems (see the section “Nanomaterial Classifications and Functions”), exemplified by core/shell designs, optimize outcomes through differential release: in burns, the shell layer first releases naringenin (Nar) to scavenge ROS and downregulate IL-6 (Phase 1 anti-inflammation), followed by core-released exosomes promoting angiogenesis (Phase 2 healing). This programmed strategy enhances drug efficiency. 142 With nanomaterial advances and clinical translation, their integration offers synergistic potential. Given high drug-loading, antimicrobial/anti-inflammatory properties, and clinical precedents, nanomaterials are becoming preferred substrates for microneedle systems, providing material selection guidance for related research. However, clinical translation faces challenges: (1) limited scalability due to wound-specific customization needs, (2) lack of standardized development methodologies, and (3) barriers to universal solutions from histopathological complexity and patient variability.
Authors’ Contributions
G.W.: Investigation, writing—original draft, and writing—review and editing. Y.Y.: Investigation, visualization, and writing—original draft. J.L.: Investigation and writing—original draft. M.Q.: Visualization. R.W.: Data curation. Z.M.: Data curation. D.Z.: Conceptualization and supervision. J.W.: Formal analysis and supervision. L.Z.: Supervision.
Footnotes
Author Disclosure Statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this article.
Funding Information
This work was financially supported by Natural Science Basis Research Plan in Shaanxi Province of China (No. 2023-JC-QN-0824), Shaanxi Fundamental Science Research Project for Chemistry & Biology (No. 23JHQ064), Natural Science Foundation of Shaanxi Provincial Department of Education (Program No. 23JK0688), and National Project Program of The National College Student Innovation and Entrepreneurship Training (No. 202410697032).