
Abstract
Erythropoietin (EPO) is a glycoprotein hormone stimulating erythropoiesis. Over the last two decades, EPO has additionally gained attention as a therapeutic compound in plastic and reconstructive surgery. This is mainly due to its pleiotropic action profile, which promotes angiogenesis, suppresses apoptosis, and modulates inflammation, resulting in enhanced tissue regeneration. Accordingly, many studies have demonstrated the efficacy of EPO and its derivatives in the management of wound healing, flap surgery, peripheral nerve regeneration, fat grafting, and bone repair. However, for the broad clinical implementation of EPO as a therapeutic in these fields, several critical steps are yet to be taken. These include the development of standardized and safe treatment protocols and their evaluation in randomized multicenter clinical trials for the establishment of personalized, targeted therapies adapted to the specific needs of surgical patients. If this succeeds, EPO treatment may markedly improve the outcome of many different therapeutic approaches in regenerative medicine and reconstructive surgery.
Impact Statement
This review represents an overview of erythropoietin (EPO) applications in different fields of plastic and reconstructive surgery. By synthesizing current evidence across these fields, the study highlights the potential of EPO to serve as a versatile therapeutic agent capable of enhancing tissue regeneration and functional recovery, supported by modern tissue engineering approaches, such as scaffolds for controlled and sustained EPO delivery. Accordingly, this review may help to establish and improve EPO-based therapeutic protocols. If this succeeds, EPO may enhance surgical outcomes, reduce complications, and minimize patient discomfort.
Introduction
Erythropoietin (EPO) is a glycoprotein hormone, which is mainly produced by the kidneys in response to anemia and stimulates the proliferation and differentiation of erythroid precursor cells. 1 It exerts its effects in a dose-dependent manner by binding to its receptor (EPOR). 2 In addition to its erythropoietic activity, EPO has demonstrated promising tissue-protective properties. 1 In fact, in 1998 Sakanaka et al. 3 reported the neuroprotective effect of EPO against cerebral ischemia, which stimulated further investigations under ischemic conditions in heart, 4 retina, 5 lung, 6 liver,7,8 intestine, 9 and kidney. 10 In these organs, EPO exerted significant antiapoptotic, antioxidative, anti-inflammatory, and antifibrotic effects that persisted for several days. 1 These effects appear to be mainly mediated through an EPOR isoform (EPOR/β-common receptor (βcR), also known as EPOR/CD131 or tissue-protective receptor (TPR)), including βcR, which has a lower affinity for the hormone than the homodimer receptor alone.11,12 Both EPOR and EPOR/βcR are expressed in a variety of cell types across multiple tissues and systems (Table 1).13–35
Overview of Different Cell Types and Tissues Expressing the Erythropoietin Homodimer (Erythropoietin Receptor) and/or Heterodimer (Erythropoietin Receptor/β-Common Receptor) Receptor Across Multiple Tissues and Systems Relevant to Different Applications in the Field of Plastic and Reconstructive Surgery
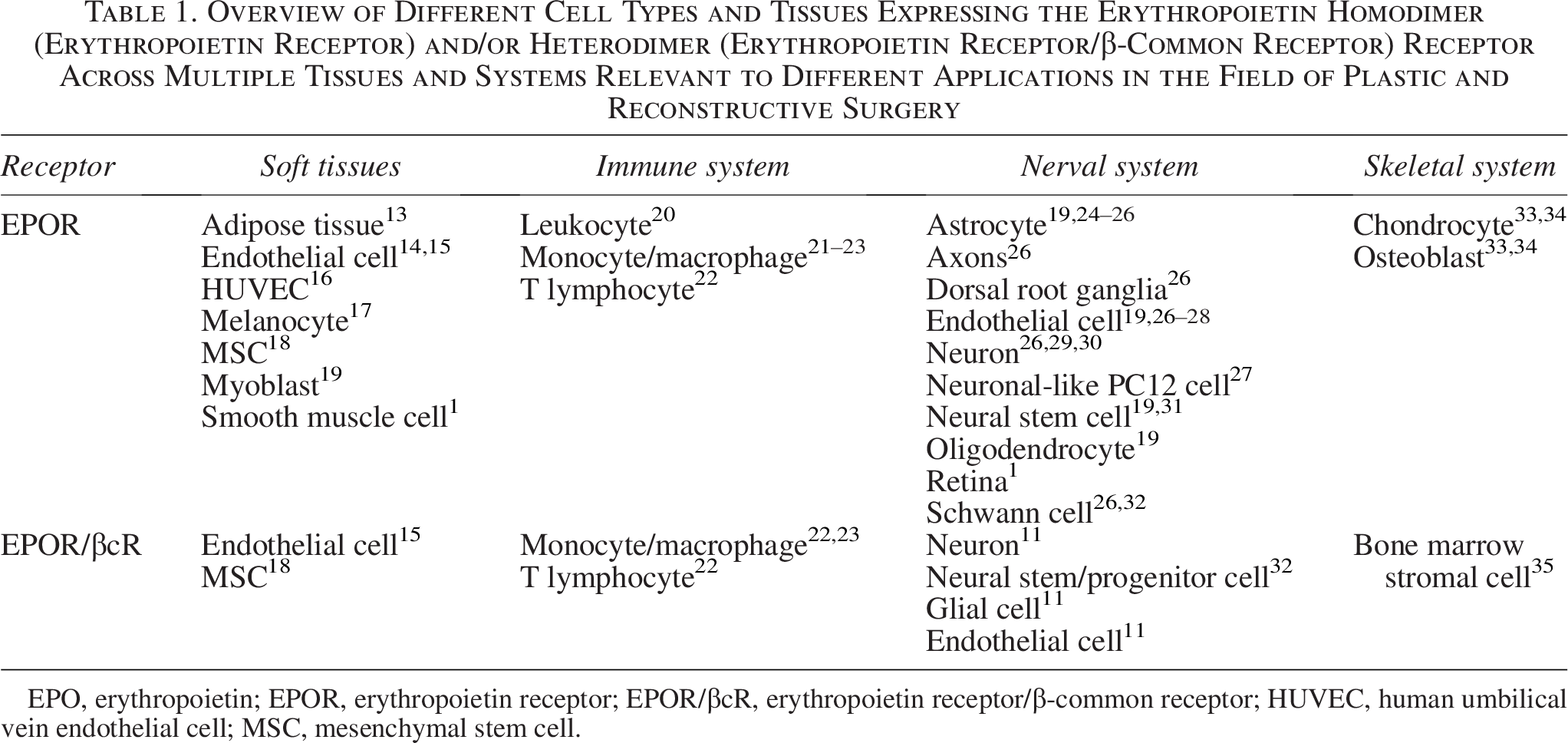
EPO, erythropoietin; EPOR, erythropoietin receptor; EPOR/βcR, erythropoietin receptor/β-common receptor; HUVEC, human umbilical vein endothelial cell; MSC, mesenchymal stem cell.
The detection of both EPO and its receptors outside the hematopoietic system has prompted interest in discovering additional beneficial functions of this hormone, particularly within the field of regenerative medicine. Numerous studies investigated the capacity of EPO to promote cutaneous wound healing, protect from ischemia–reperfusion injury of flaps, and induce peripheral nerve regeneration, as previously summarized by Günter et al. 36 more than 10 years ago. A more recent review selectively reported on the effects of EPO on wound healing. 37 However, during the last years substantial progress has been made in these fields with novel applications emerging, such as bone repair and autologous fat grafting.34,38 Therefore, the present review represents an up-to-date overview of these EPO applications in plastic and reconstructive surgery. Moreover, it specifically addresses novel tissue engineering aspects. These include scaffolds for controlled and sustained EPO delivery as well as the combination of EPO treatment with prevascularization strategies. Finally, it critically discusses major challenges in the translation of preclinical findings to clinical practice. Detailed protocols for all included studies are summarized in Tables 2–6.
Overview of Studies About Erythropoietin Effects in Wound Management, as Included in the Present Review

↑, increased; ↓, reduced; d, day; ARA290, nonerythropoietic EPO-derived peptide; EGF, epidermal growth factor; FN, fibronectin; h, hour; i.p., intraperitoneal; i.v., intravenous; min, minute; n.s., not specified; s.c., subcutaneous; w, week.
Overview of Studies About Erythropoietin Effects in Bone Repair, as Included in the Present Review
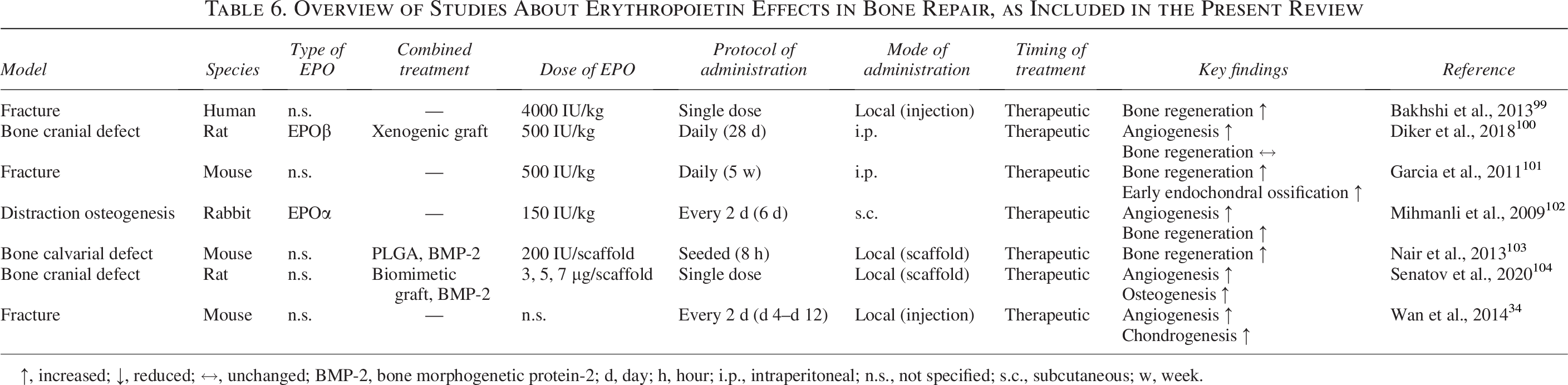
↑, increased; ↓, reduced; ↔, unchanged; BMP-2, bone morphogenetic protein-2; d, day; h, hour; i.p., intraperitoneal; n.s., not specified; s.c., subcutaneous; w, week.
Methods
A literature search was conducted using PubMed and Google Scholar with the following algorithm: erythropoietin AND wound healing OR peripheral nerve regeneration OR flap surgery OR fat grafting OR bone repair OR erythropoietin receptor OR plastic surgery. Both animal and human studies published in English up to March 2025 were considered. Original articles were included, whereas reviews, conference abstracts without complete data, and case reports were excluded. Duplicates were removed before screening. Ultimately, 129 original articles met the inclusion criteria. No formal risk-of-bias assessment was performed, although methodological limitations were considered. In this review, “EPO” refers broadly to erythropoietin and its recombinant forms, such as EPOα and EPOβ, whereas “EPO derivatives” refers to nonerythropoietic EPO forms, such as ARA290.
Wound management
Delayed wound healing represents a major clinical challenge, as it is frequently associated with increased patient morbidity. 105 Moreover, therapeutic approaches for managing chronic wounds are often insufficient. 106 EPO has shown promising therapeutic potential to improve wound healing.37,107 It inhibits inflammation by decreasing cytokine levels and suppresses apoptosis by upregulating antiapoptotic B cell lymphoma-extra large (Bcl-XL) and downregulating proapoptotic Bcl-2-associated X protein (Bax) (Fig. 1). 45 Moreover, EPO promotes blood vessel formation by upregulating vascular endothelial growth factor (VEGF), endothelial nitric oxide synthase, and inducible nitric oxide synthase (iNOS) and by enhancing the mobilization of endothelial progenitor cells (Fig. 1).21,40,108 In addition, EPO accelerates epithelialization and extracellular matrix organization through the upregulation of transforming growth factor and α-smooth muscle actin, supporting myofibroblast differentiation as well as fibronectin and collagen formation (Fig. 1).40,109 Owing to these pleiotropic effects, EPO has been investigated for the treatment of different acute and chronic tissue lesions.
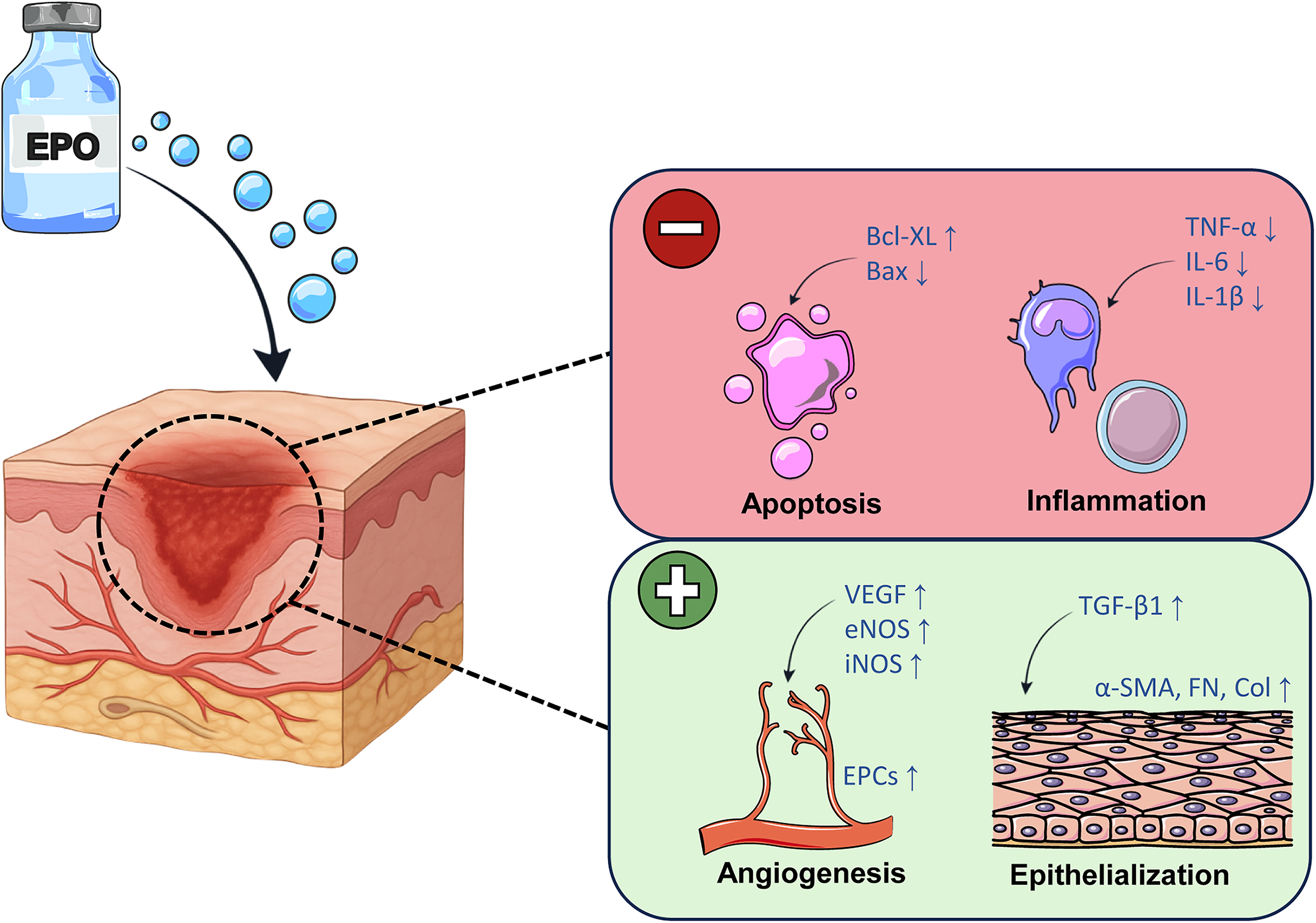
Erythropoietin (EPO) effects on wounds. EPO inhibits inflammation by decreasing tumor necrosis factor (TNF)-α, interleukin (IL)-6, and IL-1β levels. Moreover, it suppresses apoptosis by upregulating B cell lymphoma-extra large (Bcl-XL) and downregulating Bcl-2-associated X protein (Bax). In contrast, EPO promotes blood vessel formation by upregulating vascular endothelial growth factor (VEGF), endothelial nitric oxide synthase (eNOS), and inducible nitric oxide synthase (iNOS) and by enhancing the mobilization of endothelial progenitor cells (EPCs). In addition, EPO accelerates epithelialization and extracellular matrix organization through the upregulation of transforming growth factor (TGF)-β1 and α-smooth muscle actin (SMA), supporting myofibroblast differentiation as well as fibronectin (FN) and collagen (Col) formation. Taken together, this figure demonstrates that EPO exerts pleiotropic beneficial effects on different mechanisms in wound healing.
Sorg et al. 51 investigated the effects of EPO on acute full-thickness skin wounds in mice by comparing three dosing regimens of intraperitoneally administered EPO: repetitive low-dose EPO (400 IU/kg, daily for 12 days), repetitive high-dose EPO (5000 IU/kg, daily for 12 days), and single high-dose EPO (5000 IU/kg). Their results showed that a single high-dose EPO injection accelerates wound epithelialization, reduces wound cellularity, and promotes maturation of newly formed microvessels. In contrast, repetitive high-dose EPO injections impaired wound healing, as evidenced by delayed epithelialization, increased wound cellularity, and immature microvascular networks. In addition, repetitive high-dose EPO injections led to excessive erythrocyte mass and rheological impairment, which may have further deteriorated vessel and tissue maturation. 51
Particularly in patients with metabolic disorders, such as diabetes, wound healing is highly compromised. This is due to a persistent inflammatory and apoptotic state, oxidative stress, and an impaired neovascularization of the wound bed.42,110,111 In a murine model of diabetes, Galeano et al. 42 found that subcutaneous (s.c.) administration of low-dose EPO (400 IU/kg) for 12 days increases angiogenesis in ischemic wounds. This was associated with a higher VEGF gene expression on day 3. Similarly, Elsherbiny et al. 41 demonstrated that repeated intraperitoneal (i.p.) EPO injections (1000 IU/kg) over 11 days improve the microvessel density of incisional wounds in mice with hypercholesterolemia.
Based on these encouraging outcomes, the chronic nature of ulcers has prompted the search for more patient-friendly application routes. Hong and Park 49 developed a topical spray combining EPO with epidermal growth factor, which accelerated wound healing in diabetic rats compared with control sprays containing only one of these factors. Hamed et al. 45 tested an EPO-loaded cream that was applied to a fibronectin matrix in a murine model of diabetic ulcers. Interestingly, this topical formulation significantly improved the wound closure rate in a dose-dependent manner. Given the fact that cells in diabetic wounds are more susceptible to apoptosis, they also assessed the expression of the antiapoptotic protein Bcl-XL, which was upregulated following treatment. 45
EPO has also been investigated as a therapy for burn wounds, which are typically characterized by three concentric “zones” of coagulation, stasis, and hyperemia (Fig. 2). The central coagulation zone is irreversibly damaged, whereas tissue in the outer hyperemic zone usually recovers without any sequelae. The area of interest is therefore the intermediate zone of stasis, where tissue damage primarily results from compromised blood perfusion and an intense inflammatory response. 112 If left untreated, this critically perfused tissue will be recruited into the central zone by means of “secondary burn wound progression”. 113 Consequently, restoring adequate blood flow and tempering inflammation in the zone of stasis are essential for preventing secondary extension of the burn. 39
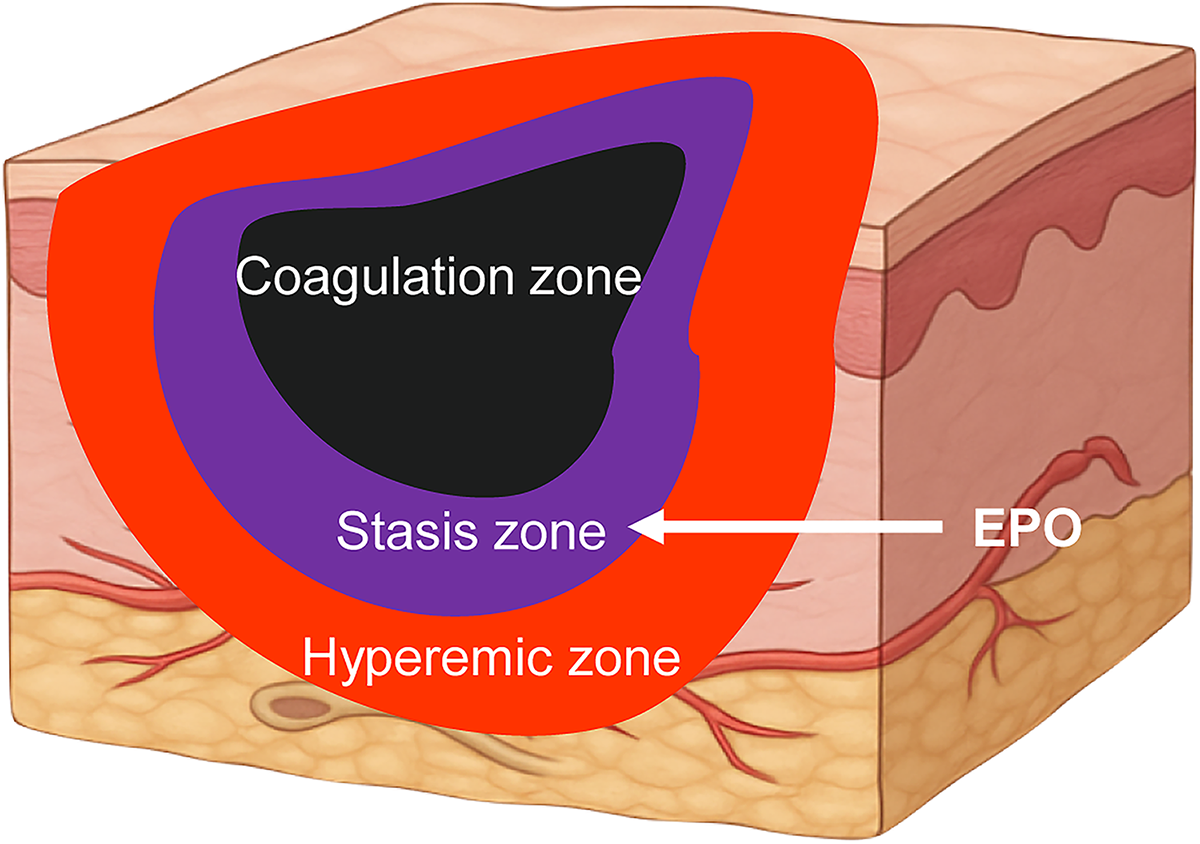
Typical concentric zones of burn injury. The central coagulation zone (black) is irreversibly damaged. This zone is surrounded by the intermediate stasis zone (purple), which can recover under beneficial conditions. The outer hyperemic zone (red) typically recovers without any sequelae. This figure demonstrates that erythropoietin (EPO) treatment particularly helps to preserve the zone of stasis by supporting perfusion and reducing secondary tissue loss, thereby preventing burn progression.
Since the temporal dynamics of secondary wound progression remain poorly defined, 114 several EPO treatment regimens have been tested. Of interest, systemic low-dose EPO (500 IU/kg) administration 45 min after burn injury in rats preserved the intermediate dermis from progressive damage, whereas a 6-h delay of this treatment was ineffective.52,53 In line with these results, s.c. or topical gel applications of EPO immediately after burn injury significantly enhanced angiogenesis and epithelial regeneration.22,43,46,50 These findings underscore the importance of early therapeutic EPO application to preserve tissue perfusion and viability in burn injuries.
Besides its proangiogenic properties, EPO also promotes neuroprotection by modulating the expression of Bcl-2, Bax, and cleaved caspase-3. 54 Accordingly, systemic administration of high-dose EPO (3000 IU/kg) attenuated motor neuron loss and muscle atrophy in a murine model of full-thickness burn injury.54,55 However, this high-dose treatment led to a marked rise in hematocrit, which impaired microvascular flow and, thus, perfusion of the zone of stasis.54,55 To overcome this problem, Bohr et al. 39 used ARA290, a nonerythropoietic EPO-derived peptide that selectively targets the EPOR/βcR complex while not binding to EPOR, to treat burn wounds. Of interest, the treated group exhibited less microvascular thrombosis compared with untreated controls, thereby preventing secondary burn wound progression.
In summary, various administration routes and doses of EPO have been proposed to improve key processes in wound healing (Table 2). These processes are summarized in Figure 1, which illustrates the coordinated anti-inflammatory and proangiogenic effects of EPO in wound repair. However, EPO treatment protocols vary widely across preclinical models, making it difficult to extrapolate standardized dosing regimens for clinical use. This problem is even reinforced by the fact that low and high EPO doses can markedly differ in their outcomes and side effects. Prolonged high-dose EPO treatment has been shown to increase the risk of adverse events. 115 In contrast, subtherapeutic EPO doses may be ineffective in promoting tissue repair. To overcome this problem, topical applications of low-dose EPO may represent a good solution, because they are safe, effective, and simple to administer in the clinical setting.
Flap surgery
Tissue transfer using surgical flaps is a widely performed procedure in reconstructive surgery. However, ischemia compromises flap survival in 20–33% of cases, particularly in their distant and extended areas. 66 To limit this complication, different “conditioning” strategies have been developed. “Preconditioning” entails the controlled exposure of tissue to specific supraphysiological stimuli before flap elevation to activate intrinsic protective and regenerative mechanisms. 116 Conversely, “postconditioning” refers to therapeutic interventions following flap elevation with the primary aim of preserving capillary flap perfusion.
Over the years, various stressors for tissue conditioning, including cold, heat, growth factors, hypoxia, and local shock waves, have been investigated to promote vascularization and protect flap tissue from ischemia.117,118 Among these, EPO has been administered before (preconditioning), before and after (overlapping treatment), and after (postconditioning) flap elevation in different animal models (Table 3).
Overview of Studies About Erythropoietin Effects in Flap Surgery, as Included in the Present Review
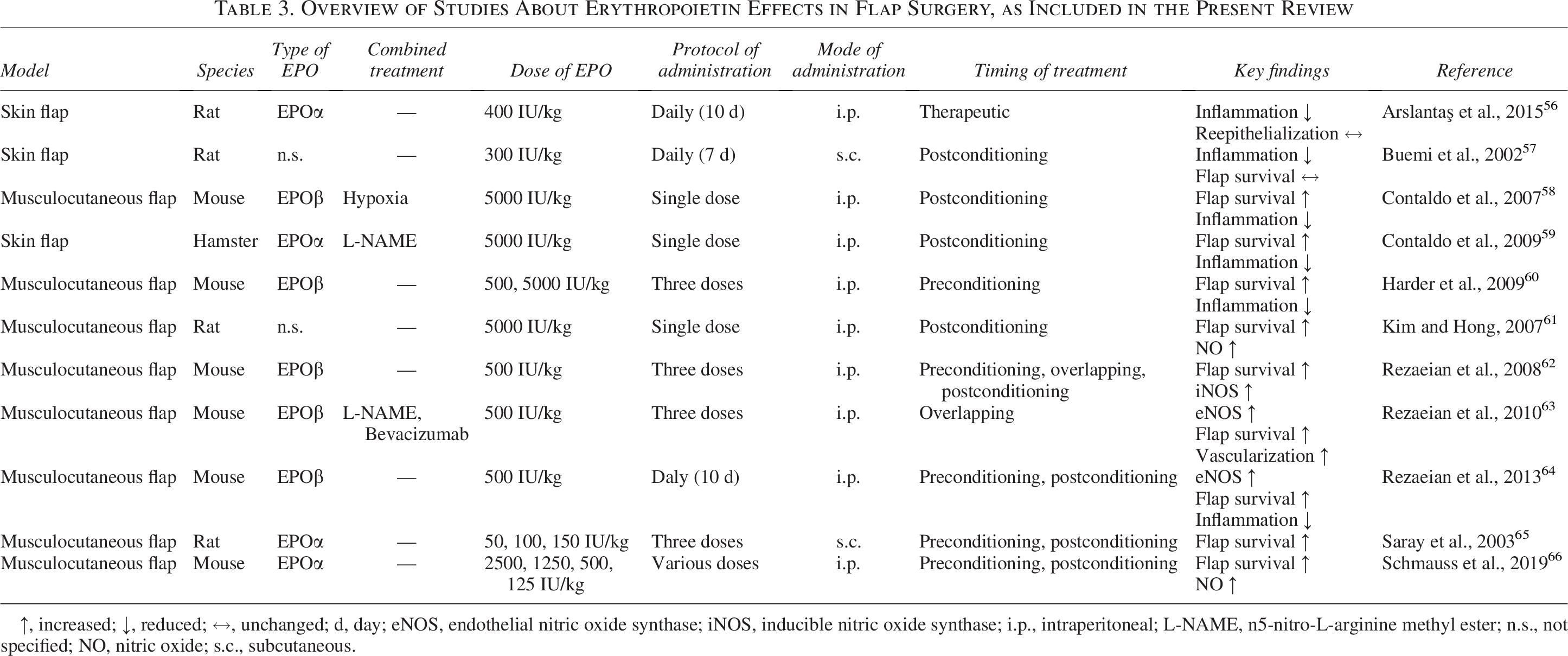
↑, increased; ↓, reduced; ↔, unchanged; d, day; eNOS, endothelial nitric oxide synthase; iNOS, inducible nitric oxide synthase; i.p., intraperitoneal; L-NAME, n5-nitro-L-arginine methyl ester; n.s., not specified; NO, nitric oxide; s.c., subcutaneous.
Rezaeian et al. 62 compared all three conditioning timings by i.p. administration of three equal low doses of EPO (500 IU/kg) in mice for each experimental setting. They demonstrated that EPO preconditioning enhances arteriolar dilatation and attenuates the ischemia-induced decrease of functional capillary density within the flap tissue. These effects were most probably induced by nitric oxide (NO). Indeed, they proved a significantly higher iNOS expression in the preconditioned and overlapping treatment group. 62 Accordingly, the administration of EPO and N5-nitro-L-arginine methyl ester (L-NAME) hydrochloride, a selective iNOS inhibitor, completely abolished NO-induced effects of EPO. 63 Consequently, both preconditioning and overlapping treatment with EPO markedly reduced flap necrosis. In contrast, postconditioning alone did not improve microvascular perfusion or tissue viability.62,63 In a subsequent study, the same group evaluated a 10-day EPO regimen (500 IU/kg, i.p.) in mice, again comparing pre- and postconditioning. Only in the preconditioned group, they observed reduced skin necrosis. This was predominantly caused by capillary maintenance and reperfusion as well as improved tissue regeneration. However, by day 10, elevated hematocrit levels were observed in both groups that may have impaired microcirculatory rheology and tissue perfusion. 64 Similarly, Arslantaş et al. 56 reported that daily administration of low-dose EPO (400 IU/kg) for 10 days following flap elevation in rats failed to improve flap survival, while inducing a progressive increase in hematocrit levels over time. Another study compared low doses of EPO (50, 100, and 150 IU/kg) in a short-term postconditioning period of 1 week or a long-term preconditioning period of 3 weeks. 65 However, improved flap survival was only found in the short-term postconditioning group. This was explained by the fact that long-term EPO treatment may have impaired flap survival due to a rise in hematocrit and the resultant blood hyperviscosity, thus increasing microvascular thrombus formation. 65
The preconditioning strategy was explicitly investigated by Harder et al., 60 who examined the effects of daily EPO administration for 3 consecutive days before flap elevation in mice at both low (500 IU/kg) and high (5000 IU/kg) i.p. doses. Interestingly, a significant reduction in flap necrosis was observed in the low-dose group compared with the high-dose group. Furthermore, animals treated with the high-dose regimen exhibited elevated hematocrit levels that proved to be counterproductive for blood rheology and eventually maintenance of capillary perfusion. 60
Buemi et al. 57 demonstrated that EPO postconditioning significantly enhances revascularization of randomly perfused ischemic flaps in rats. This was particularly achieved by low-dose EPO (300 IU/kg) administered once daily for 7 days after flap elevation, primarily through attenuation of oxidative and inflammatory stress as well as an increase in capillary density. 57 Contaldo et al. 58 showed that the administration of a single high dose of EPO (5000 IU/kg) after flap elevation in mice significantly protects flap tissue from ischemia by preserving nutritive perfusion, reducing inflammation, and inducing angiogenesis. In a subsequent study, the authors reported that postconditioning treatment with a single high dose of EPO (5000 IU/kg) induces an overexpression of iNOS and NO, thus promoting tissue perfusion and oxygenation by increasing the diameter, flow, and density of microvessels. The administration of L-NAME completely abolished these NO-related effects of EPO. 59 However, the anti-inflammatory and antiapoptotic properties of EPO remained unaffected by L-NAME coadministration. This suggests that these effects are NO independent. Similarly, Kim and Hong 61 administered a single high dose of EPO (5000 IU/kg) after flap elevation. They found that NO expression was significantly higher already 24 h after flap elevation, resulting in an improved flap vascularization and survival 10 days after surgery. 61
Schmauss et al. 66 demonstrated that pre- and postconditioning with low doses of EPO protects critically perfused musculocutaneous flap tissue. They tested different EPO application regimens, including high-dose EPO (2500 IU/kg) followed by declining doses (1250–125 IU/kg) or repeated low doses (125 IU/kg). Only the latter regimen was associated with a significant reduction of necrosis. Moreover, high-dose EPO provoked higher hematocrit levels at day 10 after surgery. 66
Overall, there is a broad consensus that the tissue-protective effects of EPO are largely mediated through the overexpression of endothelial-derived NO synthases.58,59,61–66 Furthermore, it is important to note that the angiogenic response induced by EPO typically emerges 5 days after flap elevation, as new vessels must first develop before becoming functional. This indicates that neovascularization does not really contribute to immediate tissue survival, but rather tissue regeneration. 117
Taken together, these preclinical studies partly report contradictory results regarding the timing of EPO treatment and its effects on flap survival. In fact, the efficacy of preconditioning versus postconditioning protocols has been assessed differently across studies. However, there is clear consensus that short-term EPO treatment should be preferred to preserve tissue viability and reduce flap necrosis. Moreover, most studies indicate that low-dose or single high-dose EPO administration results in better outcomes while also minimizing the risk of adverse events.
Peripheral nerve regeneration
Peripheral nerve injury (PNI) occurs when motor or sensory nerves are damaged, leading to functional deficits and pain. 119 To bridge larger nerve defects and restore functional continuity, a variety of surgical techniques, including neurorrhaphy, tubulization, and autologous nerve grafting, are currently used. Despite progress in microsurgical procedures, full functional recovery remains elusive in many cases, underscoring the need for adjunct pharmacological therapies. 120 Among emerging candidates, EPO has gained particular attention due to its cytoprotective effects on neurons and glial cells in the central nervous system following ischemic injury. 121
Different animal models, such as chronic constriction injury (CCI), nerve crush injury (NCI), and nerve transection injury (NTI), have been used to test the effects of EPO after PNI. Yin et al. 87 demonstrated that systemic high-dose EPO (5000 IU/kg) administration following nerve tubulization after NCI in rats significantly increases the number of myelinated axons and, thus, improves functional recovery. Similarly, systemic administration of three subsequent high doses of EPO (5000 IU/kg) significantly improved functional recovery after NCI in mice. 71 Other studies focused on muscle recovery after PNI, showing the benefits of EPO in the attenuation of muscle atrophy and strength loss in rats.78,79,82 More recently, novel EPO delivery strategies have also been explored. Zhang et al. 91 tested a chitosan-based nerve conduit seeded with EPO showing a significant acceleration in nerve regeneration in a rat NCI model. The same authors demonstrated that codelivery of EPO and nerve growth factor via a poly-lactic-coglycolic acid (PLGA) scaffold used as a nerve conduit enhances nerve regeneration even further. 93
Several preclinical studies investigated EPO as a stand-alone therapy following CCI, NCI, and NTI (Table 4).69,70,74,85 Across these studies, EPO showed antiapoptotic, anti-inflammatory, and proangiogenic effects, thereby enhancing nerve functional recovery and alleviating neuropathic pain. Notably, no significant differences were observed between local and i.p. administration of a single high dose of EPO 83 nor among different s.c. doses of EPO (1000, 2680, and 5000 IU/kg) administered daily for 18 days. 68
Overview of Studies About Erythropoietin Effects in Peripheral Nerve Regeneration, as Included in the Present Review
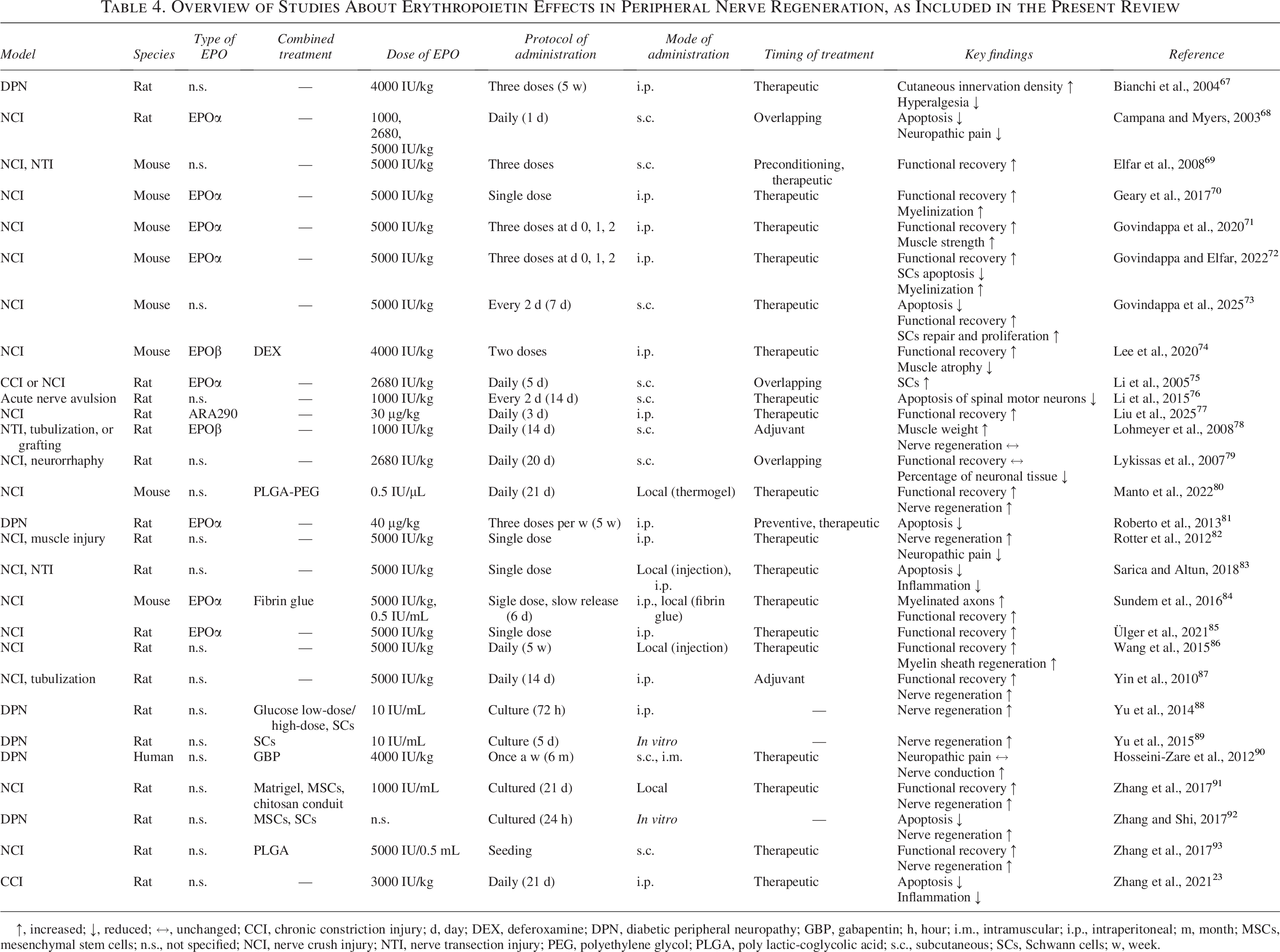
↑, increased; ↓, reduced; ↔, unchanged; CCI, chronic constriction injury; d, day; DEX, deferoxamine; DPN, diabetic peripheral neuropathy; GBP, gabapentin; h, hour; i.m., intramuscular; i.p., intraperitoneal; m, month; MSCs, mesenchymal stem cells; n.s., not specified; NCI, nerve crush injury; NTI, nerve transection injury; PEG, polyethylene glycol; PLGA, poly lactic-coglycolic acid; s.c., subcutaneous; SCs, Schwann cells; w, week.
To elucidate the mechanisms underlying the neuroprotective effects of EPO, Li et al. 75 investigated EPO therapy in both in vivo CCI and NCI models and in an in vitro hypoxia model. In these models, EPO upregulated the expression of its receptor on Schwann cells (SCs) and thereby suppressed their apoptotic cell death. These findings were confirmed by subsequent studies.88,89,122 A deeper investigation revealed that EPO attenuates and delays the activation of the JNK/c-Jun/caspase apoptotic pathway, a key driver of SC apoptosis following PNI. 76 EPO also promotes nerve regeneration by upregulating genes involved in myelin synthesis, as demonstrated in murine models of NCI. 123 In addition, EPO fosters a proregenerative microenvironment by inducing macrophage polarization toward the M2 phenotype, which enhances the clearance of axonal and myelin debris.72,73
Diabetic peripheral neuropathy (DPN) is a common complication of diabetes mellitus, affecting approximately 50% of patients. 124 Bianchi et al. 67 evaluated the effects of systemic EPO administration in diabetic rats. They found an increased cutaneous innervation density when applying both preventive and therapeutic regimens. In addition, Roberto et al. 81 observed a significant increase in intraepidermal nerve fiber density following systemic EPO treatment in diabetic rats.
Several studies demonstrated that mesenchymal stem cells (MSCs) promote nerve repair in DPN through differentiation into SC-like phenotypes.125,126 Zhang and Shi 92 hypothesized that there may be a synergistic effect between MSCs and EPO. By transducing MSCs with the EPO gene via lentiviral vectors and coculturing them with SCs isolated from the sciatic nerves of diabetic rats they demonstrated a significant reduction in SC apoptosis.
Wang et al. 86 investigated the role of insulin-like growth factor (IGF)-1, which is involved in myelination and axonal regrowth. They demonstrated that EPO treatment in a rat NCI model significantly enhances IGF-1 expression, thereby promoting remyelination and improving functional outcomes. Similarly, the combined administration of EPO and dexamethasone exerted a synergistic effect in a mouse model of NCI, attenuating nerve degeneration, accelerating functional recovery, and reducing neurogenic muscle atrophy (Fig. 3). 74 This combination treatment may allow minimization of the negative anti-inflammatory effects associated with the use of dexamethasone while enhancing its myeloprotective effects. 74
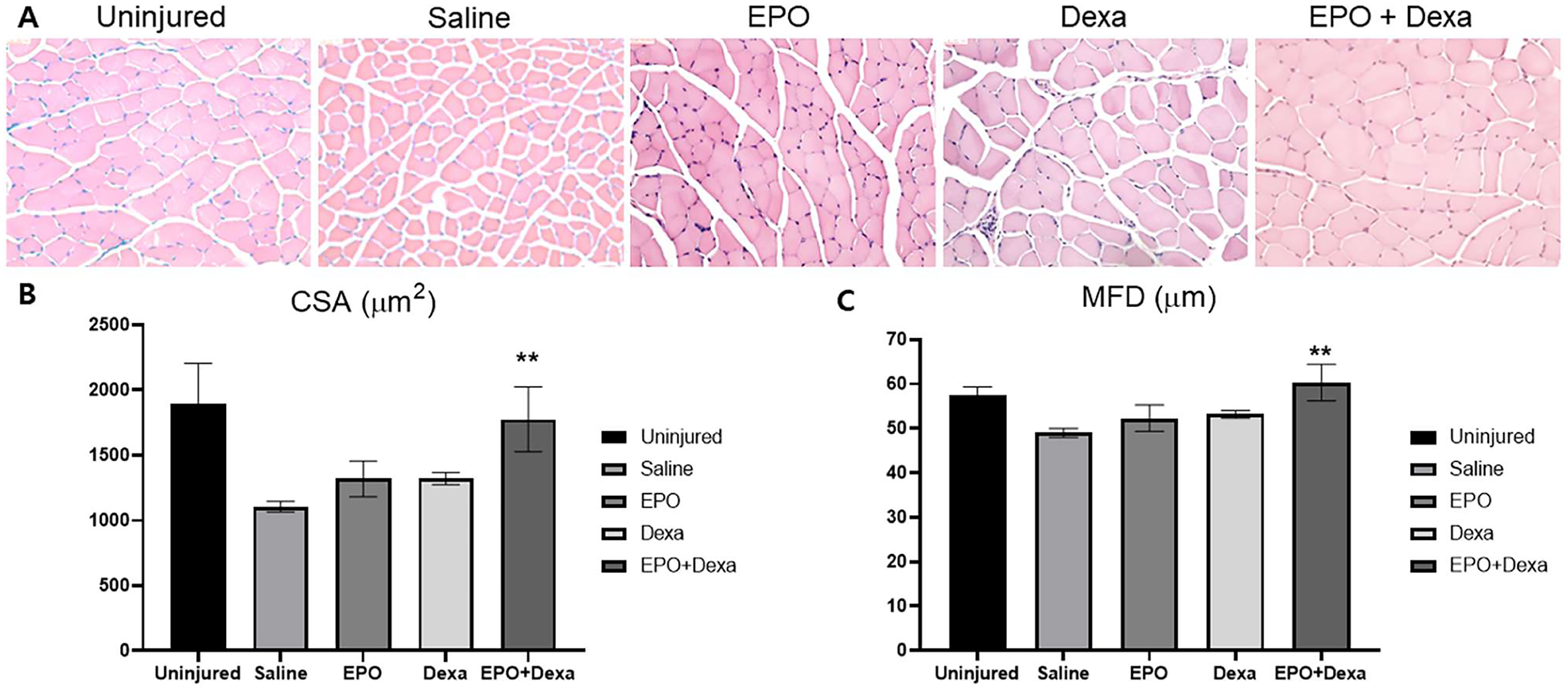
Morphometric assessments of muscles in a mouse model of acute PNI according to Lee et al.
74
Taken together, preclinical studies suggest that EPO reduces neuropathic pain and promotes functional recovery after PNI. To enable local EPO delivery, innovative strategies have been developed, such as the implantation of EPO-loaded nerve conduits and scaffolds or the injection of thermosensitive hydrogels and fibrin glue containing EPO.80,84 In addition, the combined administration of EPO and ARA290 has been proposed as a safe and effective approach for promoting peripheral nerve repair and regeneration. In fact, Liu et al. 77 reported that ARA290 retains the neuroprotective effects of EPO while minimizing its erythropoiesis-associated side effects, effectively reducing neuropathic pain and inflammation.
Fat grafting
Autologous fat grafting offers a minimally invasive approach for restoring soft tissue volume following trauma and oncological surgery. 127 However, a key limitation of this intervention is the delayed revascularization of grafted fat, which begins ∼7 days after transplantation.128,129 During the initial “avascular window”, the grafted adipose tissue is particularly susceptible to ischemic injury and apoptosis, bearing the risk of tissue resorption. 130
In a pioneering study, Hamed et al. 94 transplanted human fat tissue s.c. into immunodeficient nude mice and administered EPO every 3 days for 18 days. This treatment resulted in a significantly reduced rate of fat resorption, which was accompanied by an increased microvessel density and expression of angiogenic growth factors within the grafts. In addition, EPO administration led to a downregulation of inflammatory and apoptotic markers. 94 These in vivo findings were supported by in vitro experiments demonstrating the proangiogenic and anti-inflammatory effects of EPO as key mechanisms in preventing fat resorption.38,96 Moreover, Olaru et al. 95 showed that combining EPO with insulin significantly increases the volume of fat grafts 1 and 2 months after their transplantation into rats. Hence, this study underscored the potential of combination therapies for the improvement of fat graft vascularization and eventually survival.
More recently, increasing attention has been directed toward the use of autologous fat derivatives for the prevascularization of dermal skin substitutes, which are widely used to treat chronic wounds and large skin defects.131,132 Particularly adipose tissue-derived microvascular fragments (MVFs) have been shown to effectively accelerate the vascularization and integration of dermal skin substitutes. 98 Karschnia et al. 98 pretreated isolated MVFs with EPO for 24 h under culture conditions, which resulted in the upregulation of angiogenic growth factor expression, enhanced endothelial cell proliferation, and reduced apoptotic cell death of perivascular cells (Fig. 4). The pretreated MVFs were then seeded onto collagen-glycosaminoglycan matrices, which were implanted into mouse dorsal skinfold chambers. In comparison with MVFs not exposed to EPO, the pretreated MVFs promoted the early vascularization of the implants. 98 In a subsequent study using the same model, Später et al. 97 demonstrated that daily i.p. administration of EPO over 5 days also improves the vascularization and integration of MVF-seeded matrices.
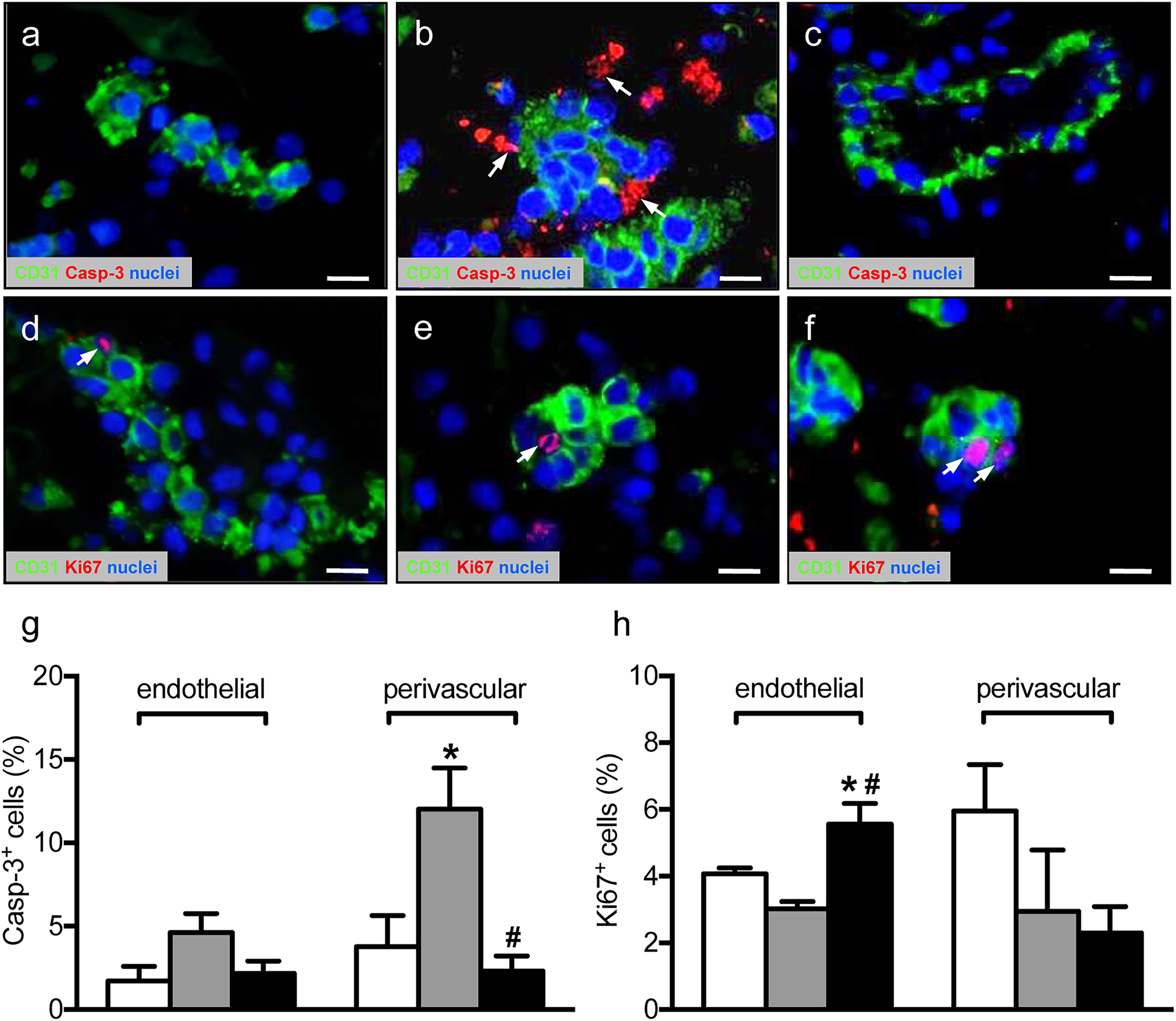
Viability and proliferation of isolated MVFs exposed to EPO for 24 h according to Karschnia et al.
98
In summary, current evidence highlights the potential of EPO as an effective compound to enhance vascularization, integration, and long-term survival of autologous fat grafts and tissue-engineered constructs (Table 5). Notably, combining EPO with other angiogenic agents (e.g., insulin) or emerging prevascularization strategies (e.g., MVF-seeding of implants) seems to be a promising approach. 133
Overview of Studies About Erythropoietin Effects in Fat Grafting, as Included in the Present Review
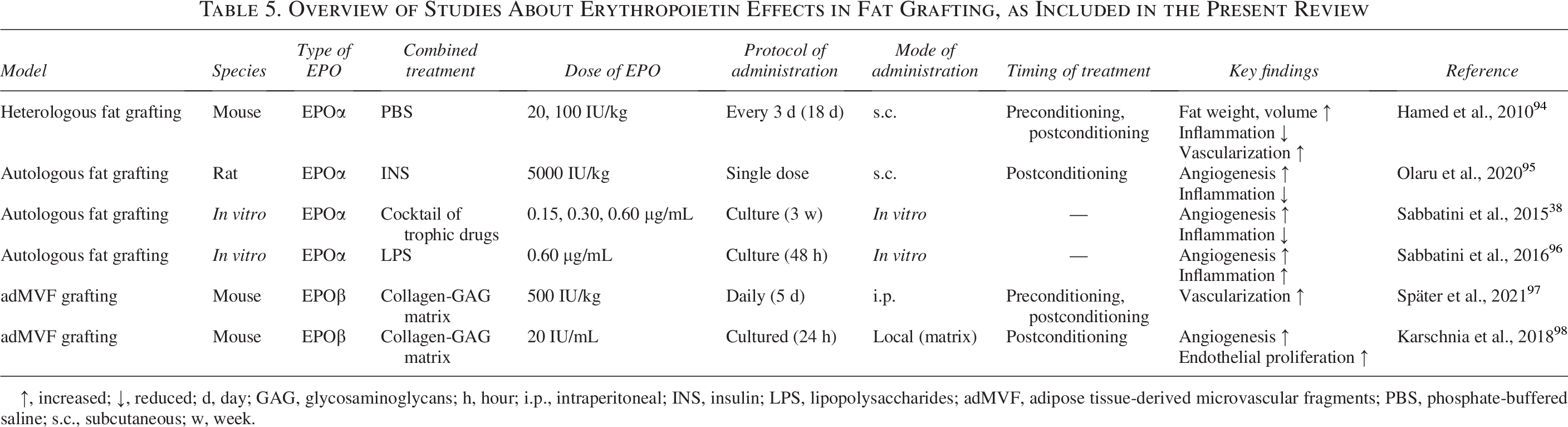
↑, increased; ↓, reduced; d, day; GAG, glycosaminoglycans; h, hour; i.p., intraperitoneal; INS, insulin; LPS, lipopolysaccharides; adMVF, adipose tissue-derived microvascular fragments; PBS, phosphate-buffered saline; s.c., subcutaneous; w, week.
Bone repair
Bone healing typically starts with an inflammatory phase, which is followed by soft callus formation through endochondral ossification. Of interest, the EPOR/βcR complex is expressed in hypertrophic chondrocytes and bone marrow stromal cells that are crucially involved in this endochondral repair process. 33 Accordingly, several studies reported that the application of EPO can improve bone regeneration (Table 6). However, daily systemic treatment with low-dose EPO (500 IU/kg) has also been associated with significantly elevated hematocrit levels after 2 and 5 weeks. 101
To mitigate systemic side effects, local EPO delivery has emerged as a promising alternative, offering targeted efficacy while avoiding hematological complications.34,99,102–104 For instance, Wan et al. 34 reported that EPO application at the fracture site in mice enhances cartilaginous callus formation and bone regeneration.
Current strategies for managing large bone defects involve the implantation of biological or synthetic scaffolds with osteoconductive and osteoinductive properties. 134 However, the use of these materials often faces significant problems, such as their insufficient vascularization and integration at the defect site. To address this, Diker et al. 100 performed systemic EPO treatment after implantation of biological bone substitutes into rat parietal bone defects, which promoted angiogenesis and graft integration. Alternatively, EPO may be also directly loaded onto scaffolds. For instance, Nair et al. 103 reported that PLGA scaffolds loaded with EPO, either alone or in combination with bone morphogenetic protein (BMP)-2, markedly improve the healing of murine calvarial bone defects compared with control scaffolds only loaded with BMP-2. More recently, a novel scaffold composed of ultra-high molecular weight polyethylene and hydroxyapatite has been developed. This scaffold binds and gradually releases EPO, which promotes blood vessel formation and osteogenesis in vitro as well as in murine cranial defects. 104
These findings suggest that EPO improves bone repair via different mechanisms. In fact, beyond its high proangiogenic activity, EPO also appears to directly stimulate endochondral ossification. Nonetheless, the balance between therapeutic benefit and systemic risks remains a key concern.
Current clinical evidence: limitations and gaps
Despite the encouraging evidence of beneficial EPO effects in preclinical studies, there are yet only a few clinical trials assessing the therapeutic potential of EPO in regenerative medicine. The first clinical trial on EPO in DPN was conducted in 2012. 90 In this study, patients with DPN and mild-to-moderate chronic kidney disease received weekly s.c. injections of EPO in addition to gabapentin for 6 months. Although gabapentin is widely used off-label for managing diabetic neuropathic pain, 135 neither gabapentin alone nor in combination with EPO improved the symptoms of DPN. In 2013, Bakhshi et al. 99 reported on a clinical trial including 60 patients that were treated with a single local EPO dose (4000 IU/kg) 2 weeks after fracture fixation. This treatment significantly reduced the time to fracture union by an average of 2.1 weeks. More recently, Hamed et al.47,48 published the results of a multicenter, single-blind, randomized, controlled trial to assess the safety and efficacy of a carbopol-based hydrogel containing EPO and fibronectin matrix for the local treatment of diabetic foot ulcers. They found that this topical formulation facilitates the local distribution of EPO, leading to a faster wound closure rate in treated patients without treatment-related side effects. Likewise, Günter et al. 44 reported a faster onset of reepithelialization in burn-injured patients following s.c. low-dose EPO administration every other day for 21 days.
EPO bears the major advantage that it is already clinically approved for the treatment of anemia. However, its use in plastic and reconstructive surgery requires additional regulatory approval. For this purpose, standardized and safe treatment protocols must be established, particularly considering patient-specific risk profiles. In fact, high-dose or prolonged systemic EPO administration has been shown to elevate hematocrit levels, thereby increasing blood viscosity and predisposing to hypertension and thrombosis. These risks are especially critical in plastic surgery where microcirculatory integrity is of paramount importance for treatment success. For instance, even subtle increases in thrombotic tendency may compromise flap survival in free flap transfer after oncologic resection. Similarly, patients with diabetic vasculopathy, who already exhibit endothelial dysfunction and higher thromboembolic susceptibility, may require adapted EPO treatment protocols. Moreover, perioperative hypercoagulability, common in major reconstructive procedures, further complicates systemic EPO administration and highlights the need for rigorous hematological monitoring and individualized dosing strategies.
To overcome these challenges, several avenues warrant further exploration. Nonerythropoietic EPO derivatives, such as ARA290, which selectively target the EPOR/βcR TPR complex while avoiding erythropoietic side effects, represent a promising alternative. Likewise, localized delivery systems, including EPO-loaded scaffolds enabling controlled and sustained release, may enhance site-specific tissue regeneration while minimizing systemic complications. Hence, these approaches should be particularly tested in randomized multicenter clinical trials for the establishment of personalized, targeted therapies adapted to the specific needs of patients in plastic and reconstructive surgery.
Conclusions
Many studies demonstrate the efficacy of EPO across a broad spectrum of indications in the field of plastic and reconstructive surgery (Tables 2–6). However, these studies are highly heterogeneous in terms of study design, including different dosages, routes, and periods of EPO administration. This high methodological heterogeneity currently prevents proposing standardized clinical protocols. Moreover, it may explain that the study results are partly contradictory in terms of outcomes and adverse effects (Table 7). Nonetheless, EPO-based strategies hold significant promise for the treatment of patients with various tissue defects. In fact, EPO bears the major advantage that it exhibits a pleiotropic action profile. It promotes angiogenesis, suppresses apoptosis, modulates inflammation, and enhances tissue growth, which may ideally promote many regenerative processes.
Summary of the Reported Outcomes and Adverse Effects of Erythropoietin Treatment Across the Different Applications in Plastic and Reconstructive Surgery Included in This Review, Considering Both the Administered Dose (Low: 20–2500 IU/Kg; High: 2500–5000 IU/Kg) and the Duration of Treatment

The threshold between short-term and long-term EPO administration is set at 7 days.
NA, not assessed; -, not existing.
Authors’ Contributions
V.P.: Conceptualization, data curation, formal analysis, investigation, methodology, project administration, validation, visualization, writing—original draft preparation, and writing—review and editing. F.B.: Conceptualization and writing—review and editing. E.L.: Writing—review and editing. A.W.: Writing—review and editing. Y.H.: Writing—review and editing. M.W.L.: Conceptualization, funding acquisition, project administration, resources, supervision, validation, visualization, writing—original draft preparation, and writing—review and editing.
Footnotes
Acknowledgments
Funding Information
There was no specific funding of this review.
Disclosure Statement
The authors have no conflicts of interest to declare.