
Abstract
This systematic review and meta-analysis evaluated the efficacy of platelet-rich plasma (PRP)-loaded scaffolds for endometrial regeneration in preclinical in vivo models. Endometrial damage, manifesting as endometrial thinning or adhesion formation within the uterine cavity, is a major cause of infertility. While PRP is a promising regenerative therapy, its short half-life limits its effectiveness. The hypothesis was that combining PRP with a hydrogel-based scaffold would provide sustained growth factor release and improve regenerative outcomes compared with monotherapies. The review was conducted per PRISMA guidelines and registered in PROSPERO (CRD420251004274). A comprehensive search of PubMed, Scopus, Web of Science, and Cochrane databases was carried out through April 2025. Seven studies in rodent models met the inclusion criteria. The meta-analysis demonstrated that PRP/scaffold combinations significantly enhanced key outcomes over untreated controls, including endometrial thickness (standardized mean difference [SMD] = 2.85, p < 0.001), gland density (SMD = 4.11, p < 0.001), angiogenesis (SMD = 6.13, p < 0.001), fibrosis reduction (SMD = −5.21, p < 0.001), and embryo implantation rates (SMD = 4.04, p < 0.001). Injectable hydrogels were particularly effective. Compared with PRP alone, the PRP/hydrogels demonstrated improved performance across the majority of structural and functional parameters, though statistical significance varied, partly attributable to variability in scaffold materials and PRP preparation methods. These results suggest that PRP-loaded scaffolds represent a promising approach for improving both structural and functional endometrial regeneration. The therapeutic success is closely tied to the scaffold’s degradation kinetics and its ability to preserve PRP bioactivity. This evidence supports the further development of standardized, degradable PRP-scaffold systems for clinical translation in treating endometrial infertility.
Impact Statement
This systematic review and meta-analysis represents the first study to quantitatively assess the in vivo regenerative potential of platelet-rich plasma (PRP) incorporated into hydrogel scaffolds for endometrial injury. Across seven preclinical studies, scaffold-assisted delivery enhanced endometrial thickness, glandular density, angiogenesis, and implantation rates, while reducing fibrosis, compared with PRP alone or untreated controls. By prolonging the bioactivity of PRP-derived growth factors and providing structural support, these biomaterial-cell constructs address a key barrier to treating infertility caused by endometrial damage. The findings establish a translational framework for standardized scaffold-PRP systems in reproductive tissue engineering.
This is a visual representation of the abstract.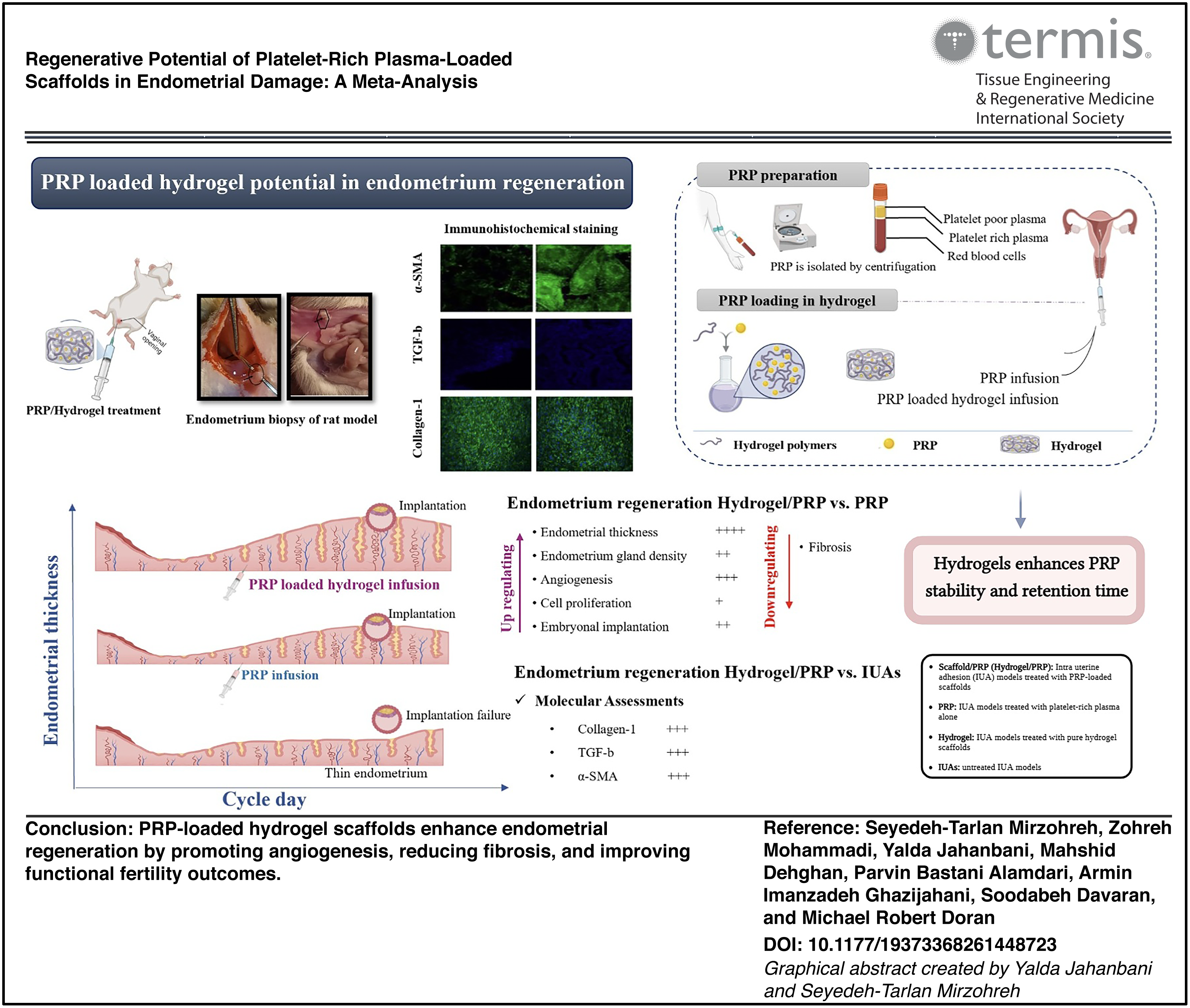
Keywords
Introduction
The uterine cavity represents a three-dimensional structure composed of endometrium, myometrium, and perimetrium arranged from the inner to the outer layers. 1 Endometrial receptivity, the ability to support embryo implantation, is crucial for IVF success,2,3 with two-thirds of unsuccessful cases associated with impaired receptivity due to thin endometrium (TE, <7 mm; 6.08% incidence) and intrauterine adhesions (IUAs), both of which increase with age.4–7 TE and IUA impair fertility by reducing endometrial thickness, delaying gland development, raising uterine artery resistance, and inhibiting vascular endothelial growth factor (VEGF)-mediated angiogenesis, leading to implantation failure and cycle cancellation. 8 TE treatments (estrogen, growth hormone, vasodilators) often have inconsistent efficacy because of side effects and limited patient adherence,9,10 while IUA management via hysteroscopic adhesiolysis carries recurrence rates of 20–62.5%, and adjunct therapies risk bleeding and infection.11,12
Recently, stem cells along with their derivatives have been explored for endometrial regeneration. Tissue remodeling involves increased release of angiogenic factors such as VEGF, bFGF, and TGF-β1,13–16 which stimulate endothelial cell migration, proliferation, differentiation, and tube formation, enhancing microvessel density and angiogenesis. 14 In addition, therapeutic agents may regulate endometrial inflammation through interactions involving inflammatory mediators, enzymes related to steroid metabolism, cellular receptors, and components of the innate immune system.
Autologous platelet-rich plasma (PRP), which is rich in growth factors, has shown potential for endometrial regeneration. Studies have reported increases in endometrial thickness, pregnancy rates, and reductions in fibrosis following intrauterine administration.17,18 Bovine research showed PRP upregulates ER/proliferation genes, 19 while rat models confirmed enhanced endometrial repair. 20 In clinical trials, PRP helped 50% of patients with TE achieve pregnancy. 21 However, its short half-life 22 may be addressed through the use of sustained-release biomaterials such as hydrogels.23,24
Pathological alterations resulting from injury or aging can impair the natural capacity for tissue regeneration.25,26 Tissue engineering addresses this by creating biological substitutes designed to restore or improve damaged tissues. Beyond bioactive factors, the timing and spatial distribution of their delivery are critical for replicating physiological healing processes. 25 Scaffolds, especially hydrogels, provide structural support and controlled release, promoting cellular integration and tissue regeneration.27,28 Their efficacy increases when combined with cytokines or stem cells. 29 Both natural (e.g., collagen, alginate) and synthetic (e.g., polycaprolactone) polymers are useful, with hybrid systems offering optimal performance.30–32 Notably, PRP-loaded hydrogels improved reproductive outcomes more effectively than PRP alone in rats.33,34
This systematic review evaluates the effects of PRP-loaded scaffolds on endometrial regeneration, analyzing their effects on key parameters and signaling pathways to assess their therapeutic potential for IUAs and TE.
Materials and Methods
The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines were followed in this study. 35 The PRISMA checklist is provided as a supplement (Supplementary Data S1). The protocol of the current meta-analysis was registered in PROSPERO (Registration ID: CRD420251004274). We used the PICOs framework to design this study.
Search strategy
A systematic literature review was conducted in April 2025 across four electronic databases: PubMed, Scopus, Web of Science, and the Cochrane Library. The investigation was guided by the following research question: “In in vivo models of endometrial damage, do PRP-loaded scaffolds improve regenerative outcomes compared to control interventions?”
The search approach utilized a comprehensive set of keywords and medical subject headings related to three core concepts: (1) scaffold and biomaterial, (2) PRP and growth factors, and (3) endometrial and uterine terms. Only studies published in English were included. To ensure literature saturation, the reference lists of all relevant identified articles and associated systematic reviews were manually examined by two independent reviewers. The full search strategies for all databases are provided in Supplementary Data S2.
Eligibility criteria
Due to the absence of clinical studies meeting the inclusion criteria following a comprehensive database search, this systematic review focuses on the efficacy of PRP-loaded scaffolds in animal models.
The inclusion criteria were defined as follows: Eligible studies were preclinical in vivo investigations that (a) utilized animal models of induced endometrial damage, (b) assessed PRP-loaded scaffolds with defined composition and preparation methods, (c) reported quantitative histological, molecular, or functional regenerative outcomes, and (d) included an appropriate control group. Exclusion criteria: Studies were excluded if they were (a) in vitro, clinical, or nonprimary research; (b) utilized scaffolds without PRP or with undefined methodologies; (c) lacked an appropriate control group or had methodological limitations; or (d) were duplicates or provided insufficient outcome data.
Study selection
Two reviewers independently screened each title and abstract, and if the articles fulfilled the inclusion criteria, the full text was reviewed. The third reviewer (Z.M.) then evaluated the eligibility of the selected articles by reviewing their full texts. Any discrepancies were resolved through discussion with a fourth reviewer (P.B.A.). The study selection process was summarized using the PRISMA flow diagram.
Data extraction
Data extraction was performed independently by two reviewers (S.-T.M., Y.J.). For each study, we recorded study design, animal model characteristics (species, strain, age, weight), intervention details (PRP type/concentration, scaffold material, delivery method, treatment duration, follow-up), and outcomes. Histological endpoints included endometrial thickness, gland density, and fibrosis reduction; molecular outcomes involved growth factors, gene/protein expression, and signaling pathways. Functional outcomes, including embryo implantation and live birth rates, were prioritized for clinical relevance.
Risk of bias assessment
SYRCLE’s risk of bias tool was used to assess methodological quality in animal randomized trials. It evaluates seven domains, including selection, performance, detection, attrition, reporting, and other biases. No studies were excluded based on bias assessment.
Statistical analysis
The detailed statistical analysis methods are provided in Supplementary Data S5.
Results
Study selection
This systematic review assessed the effectiveness of PRP-enriched hydrogel scaffolds in promoting endometrial regeneration in IUA models compared with PRP or scaffolds alone. The search identified 155 studies in PubMed, 412 in Scopus, 307 in WOS, and 5 in Cochrane. After removing 113 duplicates using Rayyan, 766 abstracts were screened. A total of 589 unrelated articles, 154 conference presentations, reviews, or unavailable full texts, and 16 that did not meet criteria were excluded. As shown in Figure 1, a total of seven studies were ultimately included in this systematic review. Six in vivo studies were published in 202433,34,36–39 and one study in 2022. 40
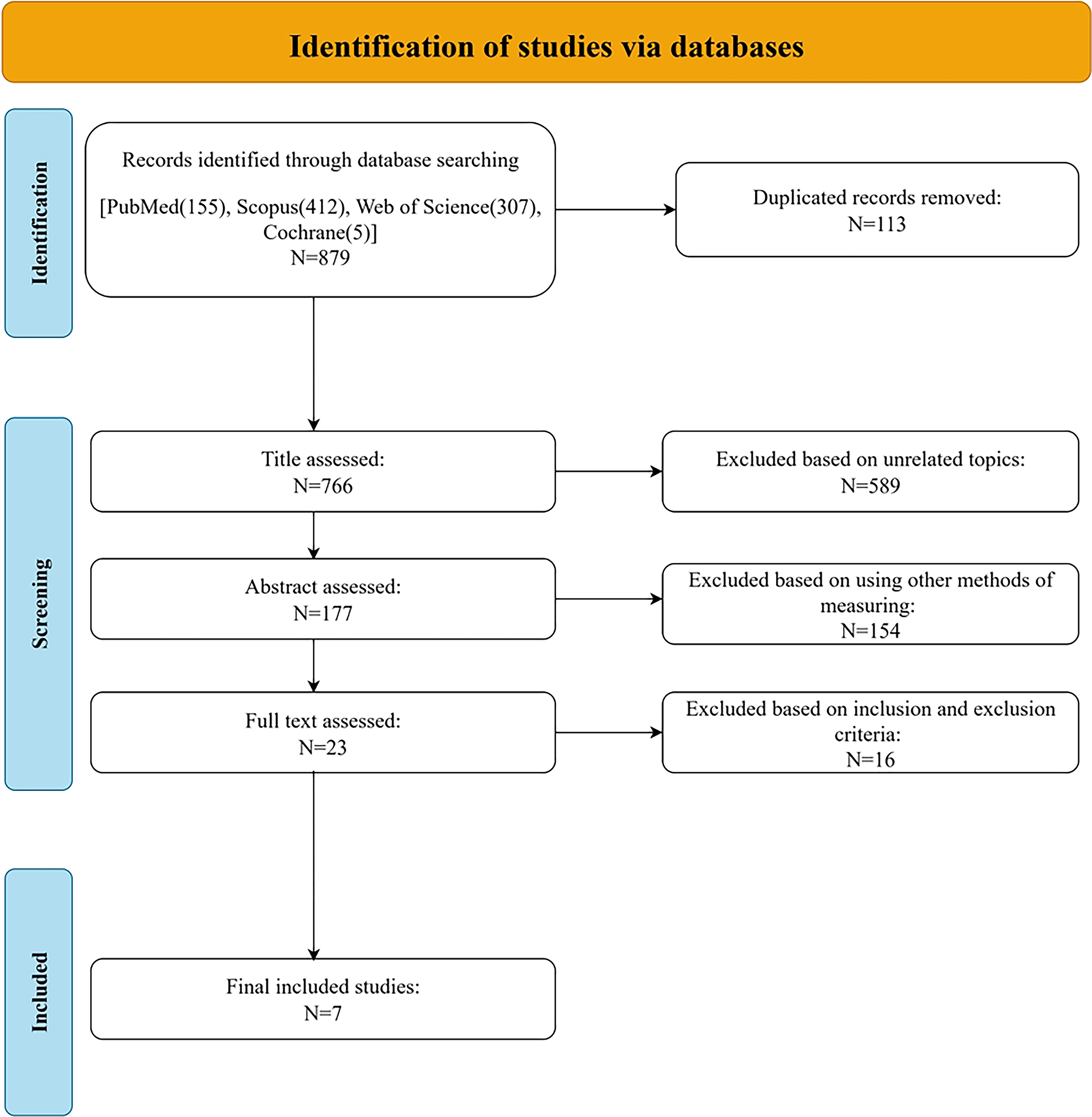
Flow diagram of the study selection process. The chart illustrates the identification, screening, eligibility, and inclusion of studies in the systematic review. A total of 879 records were identified through database searching (PubMed: 155, Scopus: 412, Web of Science: 307, Cochrane: 5). After 113 duplicates were removed, 766 titles were screened. Following the exclusion of 589 records for unrelated topics, 177 abstracts were assessed. A further 154 records were excluded for using other methods of measuring. The remaining 23 full-text articles were assessed for eligibility, of which 16 were excluded based on predefined inclusion and exclusion criteria, resulting in 7 studies being included in the final review.
Characteristics of included studies
Animal models
Five studies used Sprague-Dawley (SD) rats,33,34,36,38,39 one used C57BL/6 mice, 40 and one used SPF-grade ICR mice. 37 The number of animals per group consisted of 5 rats,38,39 6 rats, 34 10 rats, 36 10 C57BL/6 mice, 40 14 rats, 33 and 15 ICR mice 37 per group. Animals were aged 8 or 12 weeks.38,39 For IUA modeling, most studies injected 95% ethanol into clamped uterine horns, followed by PBS washing.33,36,37,40 Others induced endometrial damage via mechanical scraping or disruption using forceps following uterine incision.34,38,39 Some included optional lipopolysaccharide (LPS; 10 mg/L) to enhance inflammation. 34
Endometrial regeneration
PRP/hydrogel scaffolds consistently improved endometrial regeneration in rodent models, demonstrating significant enhancements in endometrial thickness,33,34,36–40 glandular density,33,34,36,38–40 and angiogenesis33,34,36,40 while reducing fibrosis33,34,36,38–40 relative to IUA controls.
The comparative efficacy of PRP/hydrogel versus PRP alone was scaffold-dependent. PRP/semiconducting polymer nanoparticles (SPN) 36 and PRP/GEL 33 demonstrated superior outcomes across multiple parameters, while PRP/DN GEL 34 and endometrial extracellular matrix (EndoECM)/PRP 40 provided only limited additional benefit. PRP/gelatin methacrylate (GelMA) matched triple PRP perfusion efficacy. 37 Treatments using scaffold alone produced variable outcomes, and PRP monotherapy exhibited variable efficacy, though several studies lacked direct comparisons for these interventions.38–40
Endometrial functional outcomes
PRP/hydrogel enhanced embryo implantation rates33,36–38 and live birth rates33,37 in animal IUA/TE models. However, some studies39,40 found no benefit over untreated IUAs. Poly(ethylene glycol) diacrylate–sodium alginate–
The comparative efficacy of PRP/hydrogel versus PRP alone was scaffold-dependent. PRP/SPN 36 and PRP/GelMA 37 showed better performance than PRP alone, with GelMA/PRP matching triple PRP efficacy. In contrast, PRP/GEL showed no significant improvement.33,38,40 When compared with hydrogel alone, PRP/hydrogel was superior in some studies33,37,38 but not others,36,39 highlighting variability based on scaffold type, PRP delivery, and experimental design. Further refinement is required to achieve consistent therapeutic outcomes.
Underlying mechanisms
Fibrosis Reduction
PRP/DN GEL 34 reduced fibrosis through suppression of COL1A1, WNT4, and the TGF-β1-SMAD2/3 pathway. GEL/PRP 33 decreased collagen-I, α-SMA, and TGF-β versus PRP/hydrogel/IUAs. PRP/SPN, 36 PSL/PRP, 39 and PMLA60/PRP 38 reduced collagen-I and TGF-β expression via SMAD pathway inhibition. EndoECM/PRP 40 showed weaker antifibrotic effects than PRP alone.
Angiogenesis
PRP/DN gel 34 increased CD31+ vessels versus PRP/IUAs. PRP/SPN 36 and PSL/PRP 39 boosted PECAM+ (platelet endothelial cell adhesion molecule) vascularization. GEL/PRP 33 upregulated VEGFA/PDGFA in HUVECs. GelMA/PRP 37 demonstrated angiogenic effects comparable with triple PRP through sustained VEGF/PDGF release.
Cell Proliferation and Stromal Repair
PRP/SPN 36 and PSL/PRP 39 increased Ki-67+/PCNA+ stromal cells; PRP/SPN also elevated LGR5+ stem cells. GEL/PRP 33 promoted TOP2A/MKI67+ proliferation while downregulating COL1A1/WNT4 expression. PMLA60/PRP 38 and PSL/PRP 39 enhanced cell viability through sustained release of growth factors.
Growth Factor and Pathway Analysis
PRP/DN gel 34 showed sustained VEGF/PDGF release while suppressing TNF-α, NF-κB, and JAK-STAT signaling pathways and reducing M2 macrophages and neutrophils. GelMA/PRP 37 retained growth factors for 30 days, aligning degradation with repair timelines. PRP/SPN 36 promoted anti-inflammatory M2 polarization (↑IL-10/VEGF; ↓TNF-α/IL-1β). EndoECM/PRP 40 released PDGF-BB/EGF linearly but failed to reverse fibrosis. Gel/PRP 33 inhibited TGF-β1-SMAD2/3 in HESCs, reducing SMA/collagen-I.
These advanced delivery platforms not only promoted cellular proliferation and migration but also enhanced immunomodulatory effects by decreasing proinflammatory cytokine expression and promoting an anti-inflammatory environment. Table 1 summarizes the main characteristics of the included studies.

ARG-1, arginase-1; CD31, cluster of differentiation 31; COL1A1, collagen type I alpha 1 chain; EGF, epidermal growth factor; EndoECM, endometrial extracellular matrix; GelMA, gelatin methacrylate; HA, hyaluronic acid; HESCs, human endometrial stromal cells; hESCs, human endometrial stromal cells; HGF, hepatocyte growth factor; IL-10, interleukin-10; IL-1β, interleukin-1 beta; IUAs, intrauterine adhesions; JAK-STAT, Janus kinase–signal transducer and activator of transcription; Ki-67, marker of cell proliferation; LGR5, leucine-rich repeat-containing G-protein-coupled receptor 5; LPS, lipopolysaccharide; MQs, macrophages; NF-κB, nuclear factor kappa B; PCNA, proliferating cell nuclear antigen; PDGF, platelet-derived growth factor; PECAM, platelet endothelial cell adhesion molecule; PMLA60,
Risk of bias assessment
Figure 2 presents a summary of the RoB assessment across seven included animal studies using the SYRCLE Risk of Bias tool. Across the studies, the most frequent sources of concern were related to performance bias, particularly in random housing (D4) and blinding of caregivers/investigators (D5). A high risk of bias was identified in fewer than 15% of evaluations, primarily confined to D4 and D5. Unclear risk was more common, especially in D3–D5, affecting up to 50% of the studies in those domains. A detailed assessment along with the rationale for each bias is provided in Supplementary Data S5.
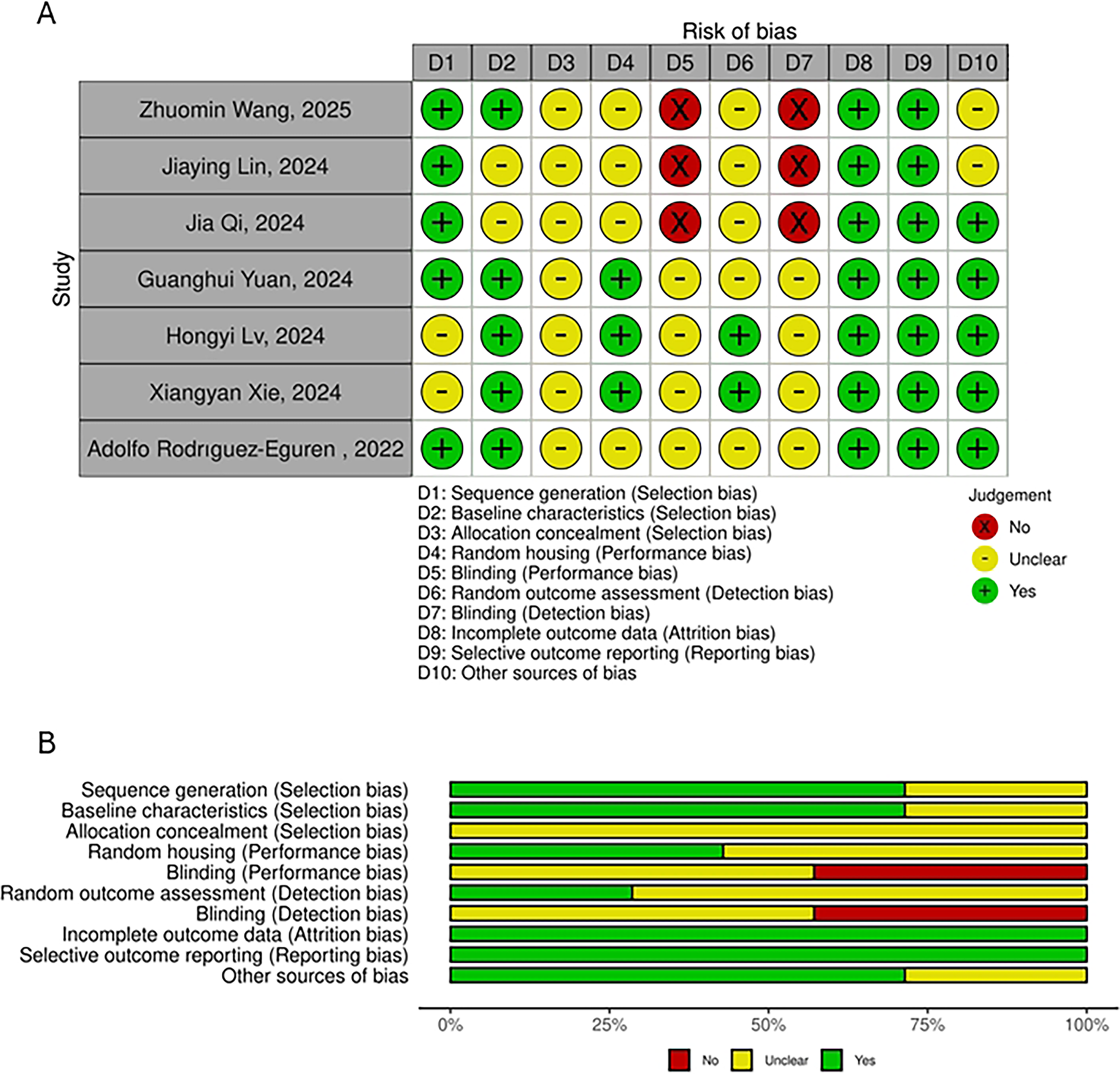
Risk of bias assessment of the included studies.
Quality assessment of outcomes
Within the GRADE framework, high-certainty evidence was assigned to endometrial thickness (PRP/scaffold vs. IUAs; scaffold/PRP vs. PRP; hydrogel vs. IUAs), endometrial gland density (PRP/scaffold vs. IUAs; hydrogel vs. IUAs), and embryonal implantation (PRP/scaffold vs. IUAs). Conversely, moderate-certainty evidence was identified for angiogenesis, fibrosis (PRP/scaffold vs. IUAs), cell proliferation (PRP/scaffold vs. IUAs; hydrogel vs. IUAs), embryonal implantation (hydrogel vs. IUAs; hydrogel vs. PRP), and molecular markers, including collagen-1, TGF-β, and α-SMA. Low-certainty evidence was observed for hydrogel versus PRP in endometrial thickness and angiogenesis, as well as scaffold/PRP versus PRP in gland density, fibrosis, and implantation, whereas very low certainty was assigned to scaffold/PRP versus PRP for fibrosis and cell proliferation. Outcomes categorized as moderate, low, or very low certainty were mainly attributed to a limited number of studies, substantial heterogeneity, and potential risk of bias. Detailed results are presented in Table 2.
GRADE Assessment of Outcomes

The study by Jia Qi (2024) 33 was deemed to be at high risk of bias for this particular outcome due to its disparate effect size and CI range compared with other studies. A sensitivity analysis by excluding this study did not change the direction or statistical significance of the summary estimate.
Level of heterogeneity is moderate to high.
Level of heterogeneity is low to moderate.
The study by Guanghui Yuan (2024) 37 was deemed to be at high risk of bias for this particular outcome due to its disparate effect size and CI range compared with other studies. A sensitivity analysis by excluding this study changed the statistical significance of the summary estimate.
The study by Jiaying Lin (2024) 36 was deemed to be at high risk of bias for this particular outcome due to its disparate effect size and CI range compared with other studies. A sensitivity analysis by excluding this study did not change the direction or statistical significance of the summary estimate.
Number of studies is low.
Confidence interval of the summary estimate included 0.
The study by Jia Qi (2024) 33 was deemed to be at high risk of bias for this particular outcome due to its disparate effect size and CI range compared with other studies. A sensitivity analysis by excluding this study changed the statistical significance of the summary estimate.
The study by Zhuomin Wang (2024) 8 was deemed to be at high risk of bias for this particular outcome due to its disparate effect size and CI range compared with other studies. A sensitivity analysis by excluding this study did not change the direction or statistical significance of the summary estimate.
The number of studies is very low.
The study by Zhuomin Wang (2024) 8 was deemed to be at high risk of bias for this particular outcome due to its disparate effect size and CI range compared with other studies. A sensitivity analysis by excluding this study changed the statistical significance of the summary estimate.
SMD, standardized mean difference; CI, confidence interval.
Results of synthesis
In this meta-analysis, four comparison groups were defined: (1) scaffold/PRP (hydrogel/PRP): IUA animal models treated with scaffolds incorporating PRP, (2) PRP: IUA models treated with PRP alone, (3) hydrogel: IUA models treated with pure hydrogel scaffolds without PRP, and (4) IUAs: untreated IUA models serving as negative controls.
The results of the overall meta-analysis are provided in Table 3, and the corresponding subgroup analyses are reported in Table 4.
Result of Synthesis

Bold values indicate statistical significance.
The comparison involves rats/mice with IUA that received treatment with a scaffold and PRP, versus those with IUA that did not receive any treatment.
The studies by Qi et al. (2024) and Yuan et al. (2024) were deemed to be at high risk of bias for this particular outcome due to their disparate effect size and CI range compared with other studies. A sensitivity analysis was conducted by excluding these studies to assess their impact on the overall findings.
The comparison involves rats/mice with IUA that received treatment with a scaffold and PRP, versus those with IUA that received treatment with PRP alone.
The study by Yuan et al. (2024) was deemed to be at high risk of bias for this particular outcome due to its disparate effect size and CI range compared with other studies. A sensitivity analysis was conducted by excluding this study to assess its impact on the overall findings.
The studies by Lin et al. (2024) and Qi et al. (2024) were deemed to be at high risk of bias for this particular outcome due to their disparate effect size and CI range compared with other studies. A sensitivity analysis was conducted by excluding these studies to assess their impact on the overall findings.
The study by Qi et al. (2024) was deemed to be at high risk of bias for this particular outcome due to its disparate effect size and CI range compared with other studies. A sensitivity analysis was conducted by excluding this study to assess its impact on the overall findings.
The studies by Wang (2024) and Qi et al. (2024) were deemed to be at high risk of bias for this particular outcome due to their disparate effect size and CI range compared with other studies. A sensitivity analysis was conducted by excluding these studies to assess their impact on the overall findings.
The study by Lin et al. (2024) was deemed to be at high risk of bias for this particular outcome due to its disparate effect size and CI range compared with other studies. A sensitivity analysis was conducted by excluding this study to assess its impact on the overall findings.
The study by Wang et al. (2024) was deemed to be at high risk of bias for this particular outcome due to its disparate effect size and CI range compared with other studies. A sensitivity analysis was conducted by excluding this study to assess its impact on the overall findings.
The studies by Lin et al. (2024) and Rodrigues et al. (2022) were deemed to be at high risk of bias for this particular outcome due to their disparate effect size and CI range compared with other studies. A sensitivity analysis was conducted by excluding these studies to assess their impact on the overall findings.
The study by Hongyi et al. (2024) was deemed to be at high risk of bias for this particular outcome due to its disparate effect size and CI range compared with other studies. A sensitivity analysis was conducted by excluding this study to assess its impact on the overall findings.
Subgroup Analysis

Bold values indicate statistical significance.
The comparison involves rats/mice with IUA that received treatment with a scaffold and PRP, versus those with IUA that did not receive any treatment.
The studies by Qi et al. (2024) and Yuan et al. (2024) were deemed to be at high risk of bias for this particular outcome due to their disparate effect size and CI range compared with other studies. A sensitivity analysis was conducted by excluding these studies to assess their impact on the overall findings.
The studies by Lin et al. (2024) and Qi et al. (2024) were deemed to be at high risk of bias for this particular outcome due to their disparate effect size and CI range compared with other studies. A sensitivity analysis was conducted by excluding these studies to assess their impact on the overall findings.
The study by Qi et al. (2024) was deemed to be at high risk of bias for this particular outcome due to its disparate effect size and CI range compared with other studies. A sensitivity analysis was conducted by excluding this study to assess its impact on the overall findings.
The studies by Wang (2024) and Qi et al. (2024) were deemed to be at high risk of bias for this particular outcome due to their disparate effect size and CI range compared with other studies. A sensitivity analysis was conducted by excluding these studies to assess their impact on the overall findings.
The study by Lin et al. (2024) was deemed to be at high risk of bias for this particular outcome due to its disparate effect size and CI range compared with other studies. A sensitivity analysis was conducted by excluding this study to assess its impact on the overall findings.
The study by Yuan et al. (2024) was deemed to be at high risk of bias for this particular outcome due to its disparate effect size and CI range compared with other studies. A sensitivity analysis was conducted by excluding this study to assess its impact on the overall findings.
Endometrial thickness
The combination of PRP/scaffold significantly enhanced endometrial thickness compared with untreated IUAs (standardized mean difference [SMD] = 2.85, 95% confidence interval [CI] = [1.59, 4.12], p < 0.001, I2 = 76%). Injectable hydrogels significantly enhanced endometrial thickness versus untreated models (SMD = 3.09, p < 0.001), though with considerable heterogeneity (I2 = 78%). PRP/scaffold showed a marginal advantage over PRP alone for endometrial thickness (SMD = 1.44, p = 0.01), though with substantial heterogeneity (I2 = 80%). Sensitivity analysis excluding Qi et al. 33 and Yuan et al. 37 significantly reduced heterogeneity.
PRP/scaffold showed a marginal advantage over PRP alone (SMD = 1.44, p = 0.01), though with substantial heterogeneity (I2 = 80%). Sensitivity analysis excluding Qi et al. 33 and Yuan et al. 37 eliminated heterogeneity but rendered the effect nonsignificant (SMD = 0.529, p = 0.05). Subgroup analyses revealed significant benefits for injectable hydrogels (SMD = 1.75, p = 0.005), both treatment durations (short-term: SMD = 1.04, p = 0.038; long-term: SMD = 1.64, p < 0.001), and in rats (SMD = 1.93, p = 0.03) but not mice (SMD = 1.03, p = 0.205).
Hydrogel scaffolds alone showed a marginal disadvantage versus PRP alone (SMD = −2.07, p = 0.014) that became nonsignificant after sensitivity analysis (SMD = −0.57, p = 0.069). However, hydrogels significantly improved thickness versus untreated IUAs (SMD = 1.12, p = 0.001), particularly in short-term treatments (SMD = 2.05, p < 0.001; I2 = 0%) versus long-term (SMD = 0.67, p = 0.009; I2 = 8%).
Endometrial gland density
PRP/Scaffold significantly improved glandular density versus untreated IUAs (SMD = 4.11, p < 0.001), though with high heterogeneity (I2 = 83%). Excluding Qi et al. 33 and Lin et al. 36 eliminated heterogeneity while maintaining significance (SMD = 2.31, p < 0.001). Subgroup analyses confirmed benefits for injectable hydrogels in rat models (SMD = 5.21, p < 0.001), and across both short-term (SMD = 5.23, p = 0.016) and long-term treatments (SMD = 3.84, p = 0.01).
Injectable hydrogels specifically showed significant improvement versus PRP alone (SMD = 3.28, p = 0.027), particularly in short-term interventions (SMD = 1.56, p = 0.004) but not long-term (SMD = 2.79, p = 0.236). Injectable hydrogels alone were inferior to PRP alone for gland density (SMD = −2.66, p = 0.03), a finding that remained significant after sensitivity analysis (SMD = −0.93, p = 0.016). However, hydrogels alone still significantly improved gland density versus untreated IUAs (SMD = 1.94, p = 0.002), a robust effect confirmed by sensitivity analysis (SMD = 1.31, p < 0.001).
Fibrosis
PRP/scaffold significantly reduced fibrosis versus untreated IUAs (SMD = −5.21, p < 0.001), with injectable hydrogels showing the strongest effect (SMD = −5.81, p = 0.001). Benefits were consistent across treatment durations (short-term: SMD = −8.56; long-term: SMD = −4.19; both p < 0.001). Sensitivity analyses excluding Wang et al. 34 and Qi et al. 33 eliminated heterogeneity while maintaining significance.
Compared with PRP alone, PRP/scaffold showed a nonsignificant trend toward greater fibrosis reduction (SMD = −1.14, p = 0.153). Injectable hydrogels alone were inferior to PRP alone (SMD = 13.96, p = 0.04) but still reduced fibrosis versus untreated IUAs (SMD = −2.25, p = 0.021), with both findings confirmed by sensitivity analyses.
Angiogenesis
PRP/scaffold significantly enhanced angiogenesis versus untreated IUAs (SMD = 6.13, p < 0.001), with benefits maintained after sensitivity analysis (SMD = 3.95, p < 0.001). Significant improvements were observed across both treatment durations and scaffold types. PRP/scaffold also outperformed PRP alone (SMD = 1.99, p = 0.002), particularly with injectable hydrogels (SMD = 2.46, p = 0.001) across all treatment durations. Injectable hydrogels alone improved angiogenesis versus IUAs (SMD = 3.72, p = 0.003) but were inferior to PRP alone (SMD = −4.10, p = 0.009), a finding strengthened by sensitivity analysis.
Cell proliferation
PRP/scaffold significantly enhanced cell proliferation versus untreated IUAs (SMD = 3.91, p < 0.001), particularly for Ki-67+ markers (SMD = 3.26, p < 0.001) and in long-term interventions. However, PRP/scaffold did not significantly outperform PRP monotherapy (SMD = 3.43, p = 0.315). Injectable hydrogels alone significantly improved cell proliferation versus IUAs (SMD = 2.35, p < 0.001).
Embryo implantation
PRP/scaffold significantly improved implantation rates versus untreated IUAs (SMD = 4.04, p = 0.002), with sensitivity analyses confirming robustness (SMD = 5.74, p < 0.001). Injectable hydrogels showed particularly strong effects (SMD = 4.91, p < 0.001).
While PRP/scaffold overall did not significantly outperform PRP alone (SMD = 0.96, p = 0.108), injectable hydrogels specifically demonstrated superior efficacy versus PRP monotherapy (SMD = 1.42, p = 0.010). Injectable hydrogels alone provided modest improvement versus IUAs (SMD = 0.55, p = 0.009) but were inferior to PRP alone (SMD = −2.76, p = 0.008).
Fibrosis biomarkers (collagen-1, α-SMA, and TGF-β)
Hydrogel/PRP combinations significantly reduced collagen-1 expression compared with untreated IUAs (SMD = −3.71, p = 0.001; I2 = 67%), with heterogeneity eliminated after excluding Lv et al. 38 (SMD = −4.05, p < 0.001; I2 = 0%). Hydrogels alone also reduced collagen-1 (SMD = −1.57, p < 0.001; I2 = 0%). Similarly, both PRP/hydrogel combinations and hydrogels alone significantly lowered α-SMA (SMD = −2.67 and −1.07, respectively; both p < 0.001; I2 = 0%) and TGF-β expression (SMD = −3.71 and −1.57, respectively; both p ≤ 0.001; I2 = 0%).
Publication bias
Because fewer than eight studies were included per analysis, formal publication bias assessment was not feasible. Funnel plots were visually inspected for outcomes with at least four studies (Supplementary Data S4), while fewer studies precluded assessment. Publication bias cannot be excluded. Details of PRP and scaffold preparations are provided in Supplementary Data S5.
Discussion
This systematic review and meta-analysis assessed the therapeutic potential of PRP combined with scaffold systems in rodent models of IUA and TE. These strategies enhanced endometrial thickness, gland density, angiogenesis, and functional outcomes such as implantation and live birth, while reducing fibrosis. Variability in efficacy was largely due to variations in PRP preparation, scaffold composition, and study design. This discussion integrates the main findings, situates them within existing literature, and highlights priorities for future research and translation.
Scaffold design: Engineering the microenvironment for regeneration
Natural and seminatural polymer scaffolds, like hyaluronic acid (HA) and GelMA, outperformed synthetic ones, improving endometrial thickness (SMD = 3.09) and reducing fibrosis (SMD = −6.22).33,34 RHC-HA hydrogels boosted stromal cell adhesion and angiogenesis, 41 while GelMA microspheres extended PRP bioactivity, contributing to fertility restoration. 37 However, rapid degradation (e.g., alginate) limited long-term efficacy, requiring IUD support for HA hydrogels. 42 Decellularized scaffolds (porcine EndoECM,43,44 amniotic ECM 45 ) retained tissue-specific proteins but demonstrated reduced antifibrotic effectiveness due to mismatched degradation profiles, highlighting the need for hybrid designs.
Synthetic/hybrid scaffolds helped address limitations in bioactivity. PEGDA with
Crosslinking approaches played a critical role; boronate bonds enabled self-healing, 33 UV-crosslinked GelMA sustained VEGF release, 37 and supramolecular chemistry reduced fibrosis. 50 Enzymatic crosslinking (e.g., thrombin/fibrinogen 34 ) often caused brittleness. Biofunctionalization strategies (heparin, 40 apoptotic bodies 50 ) improved immunomodulatory effects (↑IL-10, ↓TNF-α). Challenges included PRP heterogeneity and scaffold degradation variability (I2 = 54–97%).33,37 Future studies should focus on standardizing protocols 51 and advancing hybrid systems (e.g., 4D-printed scaffolds52,53) for clinical translation.
PRP preparation protocols: A critical determinant of efficacy
Hydrogel fabrication and PRP integration
Studies employed a range of approaches, each with strengths and limitations. Sodium alginate double-network hydrogels 34 and GelMA microspheres 37 enabled sustained growth factor release and cell adhesion, while decellularized porcine endometrial ECM 40 demonstrated reduced efficacy due to degradation or growth factor retention limitations. PRP-based regeneration success depends on scaffold biocompatibility, mechanical adaptability, and controlled-release properties.
Anticoagulant impact on PRP
EDTA (Wang et al. 34 ) inhibits coagulation yet disrupts platelet activation, 54 leading to increased platelet recovery but premature activation (↑CD62p/PAC-1) and reduced sustained growth factor release, 55 whereas sodium citrate (Yuan et al. 37 ) preserves platelet morphology and enables controlled GF release, enhancing angiogenesis (VEGF: 628.73 vs. EDTA’s 265.44 pg/mL). 56 Despite similar PDGF-BB levels,55,57 sodium citrate-PRP improves outcomes (e.g., hair regeneration, reduced inflammation 58 ), while EDTA delays healing.56,58 Unspecified anticoagulants33,36,38,39 introduce variability.
PRP source variability
Human antecubital vein, 34 umbilical cord (hUC-PRP),36,40 and rat cardiac puncture blood33,38,39 exhibit differences in growth factor (GF) profiles. hUC-PRP, rich in PDGF, VEGF, and IGF-1,45,59,60 demonstrates superior performance in neural repair. Rat PRP works preclinically33,38,39 but needs validation. Younger sources (e.g., cord blood) have higher FGF-2 and clusterin,60,61 which are associated with enhanced immunomodulatory effects.60,62
Endometrial regeneration: Bridging structural and functional recovery
Endometrial regeneration requires restoration of both histological structure and functional receptivity. PRP and hydrogel therapies consistently improved thickness, gland density, and angiogenesis compared with untreated IUAs.33,34,36–38,40 PRP and scaffold combinations significantly increased endometrial thickness (SMD ≈ 2.8), with PRP and injectable hydrogels showing the greatest effect (SMD ≈ 3.1). For instance, Wang et al. 34 reported DN gel restored thickness to 536 μm versus 330 μm in IUAs, and Qi et al. 33 achieved near-normal levels (449.3 μm versus 440.9 μm in sham rats). However, anatomical differences between rodents and humans remain a key limitation. Regenerated thickness in rodents matches their physiological range but only a limited proportion of the human endometrium, which typically ranges between 2 and 16 mm. 63 This scale gap reflects greater regenerative demands in humans, including tissue volume, vascularization, and structural forces. Thus, while rodent models are valuable for proof of concept, validation in large animal models such as pigs or nonhuman primates is needed to assess clinical potential.
Meta-analysis indicated that PRP/scaffold therapies significantly increased glandular density compared with untreated IUAs (SMD ≈ 4.1), though substantial heterogeneity (I2 = 75%) suggested variability across scaffold types. When excluding studies by Lin et al. 36 and Qi et al. 33 (reducing the effect size to SMD ≈ 2.3), heterogeneity was eliminated (I2 = 0%). For example, DN gel 34 increased glands by 2.8-fold versus IUAs (17.8 vs. 6.0 glands/section), and PRP-SPN 36 restored gland numbers to 7.7 versus 1.3 in IUAs.
PRP/hydrogel reduced fibrosis more effectively than PRP monotherapy (SMD ≈ −3.5). Mechanistically, DN gel 34 and HAMA-PBA-PVA 33 inhibited TGF-β1-SMAD2/3 signaling, lowering collagen-I expression by 60–70%, and PSL/PRP 39 reduced fibrotic area to 8.04% versus 28.88% in IUAs. PRP/hydrogel enhanced angiogenesis compared with untreated IUAs (SMD ≈ 5), with injectable hydrogels showing sustained benefits. Experimental validation indicated that DN gel 34 doubled CD31+ vessels versus PRP alone (37.6 vs. 29.8 vessels/section), and GelMA/PRP 37 increased VEGFA/PDGFA expression in endothelial cells, correlating with meta-analytical subgroup findings (rat models: SMD ≈ 2.8).
Meta-analyses demonstrated scaffold-dependent variability in embryo implantation outcomes (PRP/hydrogel vs. IUAs: SMD ≈ 5.8). Key experimental findings indicated that HAMA-PBA-PVA 33 restored live birth rates to 87.5% versus 25% in IUAs, GelMA/PRP 37 matched triple PRP efficacy (8.38 vs. 12.50 embryos), and EndoECM/PRP 40 failed functionally (33% pregnancy rate vs. 66.67% for PRP alone), aligning with meta-analytical nonsignificance. Functional success depended on scaffold-mediated growth factor retention and hormonal synchrony. For instance, GelMA/PRP 37 caused sustained VEGF/PDGF release over 30 days matched to endometrial repair timelines, achieving implantation rates equivalent to triple PRP perfusion (8.3 vs. 12.5 embryos in sham mice). PSL/PRP 39 restored uterine morphology but showed no significant embryo count improvement over IUAs (1.13 vs. 1.38 embryos), emphasizing that structural repair alone is insufficient for functional recovery. PRP alone 40 achieved 66.67% pregnancy rates in mice, while EndoECM/PRP underperformed (33%), illustrating scaffold-dependent therapeutic windows.
However, scaffold design and degradation kinetics critically influenced functional fertility outcomes. Wang et al. 34 demonstrated that PRP-loaded double-network hydrogels reduced fibrosis by normalizing collagen III/I ratios. This aligns with Qi et al., 33 where HAMA-PBA-PVA hydrogels degraded within 4–5 days, synchronized with the murine estrous cycle, enabling sustained VEGF release and improving embryo implantation rates by 2.3-fold. Conversely, slow-degrading scaffolds like EndoECM 40 obstructed embryo attachment despite structural restoration, underscoring the need for temporally aligned degradation.
PRP monotherapy improved thickness (SMD ≈ 1.12) but underperformed versus PRP/hydrogel in gland density (SMD ≈ 1.65), endometrial thickness (SMD ≈ 1.7), and angiogenesis (SMD ≈ 2.5). It lacked sustained efficacy due to rapid growth factor clearance.34,37 For example, PRP alone 34 reduced fibrosis (40% vs. 60% in IUAs) but failed to restore gland density (13 vs. 26 in controls).
Hydrogels alone showed marginal structural benefits but inferior functional outcomes (embryo implantation). For example, PMLA60 hydrogel 38 improved endometrial thickness (329.0 → 449.3 μm) but required PRP to enhance fertility (live births: 6 vs. 1.1 in IUAs), highlighting PRP’s bioactivity as indispensable. In another study, PRP/hydrogel combinations outperformed both injectable hydrogels (HAMA-PBA-PVA 33 and GelMA 37 ), achieving endometrial thickness comparable with healthy controls (449 μm vs. 440 μm in sham rats 33 ) and reducing fibrosis (collagen deposition: 8% vs. 28.8% in IUAs 38 ). EndoECM/PRP 40 increased gland density (34.2 vs. 14.7 glands/mm2 in saline-treated IUAs) but failed to enhance pregnancy rates (33% vs. 66.67% for PRP alone), likely due to mechanical obstruction caused by delayed degradation.
Key regenerative mechanisms included antifibrotic signaling, angiogenesis, and cellular proliferation. Meta-analytical fibrosis reduction (SMD ≈ −5.21) was associated with inhibition of TGF-β1-SMAD2/3 signaling in 5/7 studies.33,34,36,38–40 PRP/hydrogels downregulated collagen-I (40% vs. 60% in IUAs 34 ) and α-SMA (70% vs. 86% in saline 39 ). Lin et al. 36 linked PRP-SPN efficacy to M2 macrophage polarization (↑IL-10, VEGF; ↓TNF-α, IL-1β), aligning with meta-analytical angiogenesis improvements (SMD ≈ 6.13). Regarding angiogenesis mechanisms, PRP/DN gel 34 doubled CD31+ vessel density versus PRP alone (37.6 vs. 29.83 vessels/section), while PRP@GelMA 37 upregulated VEGFA/PDGFA expression in endothelial cells. Considering cellular proliferation, PRP-SPN 36 enhanced Ki-67+ stromal cells (27% vs. 11.3% in saline) and LGR5+ stem cells, critical for niche reconstitution.
Heterogeneity in meta-analyses (e.g., I2 = 76% for thickness) was primarily driven by variability in scaffold design. Fast-degrading hydrogels (4–5 days), including HAMA-PBA-PVA 33 and DN gel, 34 matched estrous cycles, enhancing fertility, while slow-degrading scaffolds, such as EndoECM 40 and PEGDA, 39 caused physical obstruction despite structural repair.
This meta-analysis is limited by the small number of included studies, all of which were conducted in small animal models. In addition, the risk of bias was systematically assessed for all included studies. Nevertheless, the small evidence base limits the precision of effect estimates and precludes a reliable assessment of publication bias. Consequently, extrapolation of the findings to the human endometrial repair should be undertaken with caution. The results primarily reflect preclinical regenerative potential. Further well-designed large animal studies and human trials are required to establish translational relevance. Importantly, none of the included studies systematically compared PRP formulations with different cellular compositions (e.g., leukocyte-rich vs. leukocyte-poor PRP), preventing definitive conclusions regarding which PRP profile confers optimal regenerative benefit.
Conclusion
This systematic review and meta-analysis indicates that PRP in combination with hydrogel scaffolds significantly enhances endometrial regeneration in preclinical IUA and TE models. Injectable hydrogels, such as HAMA-PBA-PVA and DN gel, achieved the greatest structural restoration, improving thickness, gland density, and angiogenesis while reducing fibrosis. Functional outcomes were influenced by scaffold degradation behavior and PRP bioactivity. Fast-degrading hydrogels synchronized with estrous cycles restored fertility, whereas slow-degrading systems such as EndoECM impaired implantation despite structural repair. PRP alone produced transient effects due to rapid growth factor clearance, and hydrogels alone lacked PRP bioactivity. Heterogeneity was mainly attributable to variability in PRP preparation and scaffold composition. Notably, the impact of PRP cellular composition and specific growth factor profiles on endometrial healing remains unclear. Standardized reporting of PRP characteristics in future studies is required to clarify which components drive therapeutic efficacy.
Data Availability
The datasets used or analyzed during the present study are available from the corresponding author on reasonable request.
Authors’ Contributions
S.-T.M.: Review conceptualization, protocol registration, independent reviewer, GRADE (certainty of evidence) assessment, data collection, software and analysis, data interpretation, and writing—reviewing and editing. Z.M.: Independent reviewer, data collection, risk of bias assessment, software and analysis, GRADE (certainty of evidence) assessment, and writing. Y.J.: Independent reviewer, data interpretation and reviewing and editing the final article. M.D.: Independent reviewer, reviewing and editing the final article and revise the article after peer-review. P.B.A.: Independent reviewer, data validation and interpretation and reviewing and editing the final article. A.I.G.: Independent reviewer, data extraction, data curation, data validation, and writing—reviewing and editing the final article. S.D.: Independent reviewer, supervision, validation, and reviewing and editing the final article. M.R.D.: Independent reviewer, reviewing and editing the final article.
Footnotes
Acknowledgments
The authors have no acknowledgments to declare.
Disclosure Statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.