
Abstract
Hydrogels have emerged as promising delivery vehicles for periodontal ligament stem cells (PDLSCs) due to their biocompatibility and resemblance to the native extracellular matrix. The objective of this systematic review was to evaluate the efficacy of hydrogels as delivery vehicles for PDLSCs in animal models of bone regeneration. This systematic review is reported according to the (Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines and included only in vivo studies evaluating PDLSCs encapsulated in hydrogels for the regeneration of periodontal, alveolar, mandibular, calvarial, or orthodontic defects. Searches were conducted in PubMed, Scopus, Embase, and Web of Science until March 2025. The risk of bias was assessed using the Systematic Review Centre for Laboratory Animal Experimentation tool. Eleven studies were included. Hydrogels included gelatin methacrylate, alginate, chitosan-based matrices, collagen, and thermosensitive poly (lactic-co-glycolic acid)–polyethylene glycol–poly (lactic-co-glycolic acid), functionalized or not with growth factors, bioactive peptides, or nanoparticles. Quantitative microcomputed tomography (micro-CT) analyses assessed bone volume/total volume, bone mineral density, and trabecular thickness. Osteogenic induction typically involved the use of dexamethasone, β-glycerophosphate, and ascorbic acid. Histology confirmed new bone formation and, occasionally, vascularization. In periodontal defects, five studies showed enhanced bone fill and periodontal ligament-like tissue formation. Alveolar bone models reported improved mineralization and neovascularization in two studies. Mandibular defects, evaluated in large animals, exhibited trabecular bone formation. One calvarial and one orthodontic bone loss model reported increased bone density and accelerated deposition, respectively. Due to substantial methodological heterogeneity, a qualitative synthesis was performed. The risk of bias was generally high or unclear in the blinding and allocation domains. The main limitations of this review included heterogeneity across animal models, hydrogel formulations, and outcome measures. Hydrogel-encapsulated PDLSCs promote bone regeneration across diverse defect types, particularly when delivered via injectable and functionalized scaffolds in animal models.
Impact Statement
This systematic review highlights the translational potential of hydrogels as delivery systems for periodontal ligament stem cells in bone defect repair. By integrating data from multiple in vivo models, this study provides a comprehensive overview of hydrogel formulations, cell encapsulation strategies, and regenerative outcomes. The findings contribute to advancing the design of bioengineered scaffolds for future clinical applications in periodontal and craniofacial tissue engineering.
Keywords
Introduction
Bone loss associated with periodontal disease poses a significant clinical challenge in dentistry, with implications that extend beyond oral health and affect overall patient well-being. 1 Periodontitis is classically defined as a chronic and progressive inflammatory disease of the periodontium, driven by microbial dysbiosis and immune dysregulation and resulting from a dysregulated host immune response to a microbial biofilm.2,3 This results in the breakdown of the bone matrix and the formation of infrabony defects. 4 Such defects compromise the structural integrity of the periodontium and are a major cause of tooth loss in advanced stages of the disease. 5 These limitations stimulated the development of biologically based regenerative approaches, among which the use of periodontal ligament stem cells (PDLSCs) has emerged as a promising strategy for tissue restoration. 6
PDLSCs, first isolated and characterized by, 7 are a population of mesenchymal stem cells derived from the periodontal ligament. PDLSCs possess osteogenic differentiation potential and can produce a mineralized matrix under appropriate microenvironmental conditions. 8 In addition to their direct differentiation into osteoblast-like cells, these cells also exert important paracrine effects by secreting growth factors and cytokines that promote angiogenesis, modulate inflammation, and recruit endogenous progenitor cells, thereby supporting the overall regenerative process. 9 These cells can differentiate into osteoblasts, adipocytes, and chondrocytes 10 and are known to exhibit immunomodulatory and proangiogenic properties. 11 Through paracrine signaling, PDLSCs secrete cytokines and growth factors that contribute to immune modulation and neovascularization, critical steps in bone regeneration. 12 Their application in cell-based therapies has demonstrated potential in promoting bone regeneration in periodontal defects, improving both structural and functional tissue outcomes. 13 Recent preclinical studies have evaluated these cells in a variety of anatomical models, including mandibular, alveolar, calvarial, and periodontal defects.14,15
In addition, the choice of an appropriate biomaterial carrier becomes a critical determinant of therapeutic success. Scaffolds play a fundamental role in bone tissue engineering by providing a three-dimensional structure that supports cell adhesion, proliferation, and differentiation. In addition to serving as a physical framework for newly forming tissue, scaffolds help maintain the regenerative space and can modulate the local microenvironment by facilitating nutrient diffusion and the controlled presentation of bioactive signals.16,17 Traditional rigid or preformed scaffolds, including those based on polycaprolactone (PCL), polylactic acid, or poly(lactic-co-glycolic acid), may present limitations in periodontal applications due to their limited adaptability to irregular defect geometries and their mechanical mismatch with the soft–hard tissue interface of the periodontium. 18 In contrast, hydrogels offer distinct advantages as cell delivery systems, as they can be administered in an injectable or in situ–forming manner, allowing precise filling of complex periodontal and alveolar defects. 19 Moreover, their hydrated three-dimensional structure more closely resembles the native extracellular matrix of the periodontal ligament, providing a favorable microenvironment for cell retention, survival, and osteogenic differentiation. 12 Taken together, these characteristics suggest a rationale for focusing on hydrogel-based systems as carriers for PDLSCs in bone regenerative strategies. 11
Despite these promising biological features, the clinical application of PDLSCs faces significant barriers, particularly related to their posttransplantation viability, retention, and functionality. 20 The local microenvironment plays a pivotal role in regulating these factors. In this regard, hydrogels have emerged as attractive delivery systems capable of mimicking the physicochemical and biological features of the extracellular matrix, thereby supporting cell survival, proliferation, and differentiation. 11 These hydrophilic, biocompatible polymers derived from either natural or synthetic sources can be tuned to create scaffolds that provide both mechanical support and controlled biochemical stimulation. 11 In general, injectable and implantable formats may be employed, utilizing hydrogels such as alginate, gelatin methacryloyl (GelMA), type I collagen, and others synthesized in the laboratory. 21
Encapsulation of PDLSCs within hydrogels may not only improve cell survival and localization but also enable the controlled release of regenerative signals such as growth factors and osteoinductive agents. 6 Functionalization strategies include the incorporation of bioactive molecules such as platelet-derived growth factor-BB (PDGF-BB), metformin, and bone morphogenetic protein-2 (BMP-2), as well as nanomaterials like gold nanoparticles, yttrium-doped graphene oxide quantum dots, and arginylglycylaspartic acid (RGD) peptides. Recent in vivo findings indicate that the synergistic combination of PDLSCs with engineered hydrogels may contribute to enhanced bone volume, mineralization, and trabecular organization in critical-sized defects, as reported. 1 Furthermore, functionalization strategies, including the incorporation of nanoparticles or osteogenic molecules, have demonstrated added benefits in enhancing the regenerative response. 22
Given this biological and translational potential, the present systematic review aims to summarize the available in vivo evidence on the use of hydrogels as delivery vehicles for PDLSCs in bone defect repair. In addition, this review focuses on evaluating the regenerative outcomes, characterizing hydrogel composition and delivery strategies, and identifying methodological trends and limitations. By integrating these findings, we aim to clarify the efficacy of PDLSC-laden hydrogels in promoting bone regeneration and to outline key directions for future translational research in periodontal regenerative medicine.
Methods
This systematic review was reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020 statement). 23 The protocol for this systematic review was registered on the Open Science Framework platform, and any modification in the original plan was reported as an amendment in the same platform [registration link: https://osf.io/s3hvp/?view_only=f81694c59ee54dd8a7b85e8bbe1517cf].
The research question was structured according to the PICOS framework:
The core research question was formulated as: “What is the effect of using hydrogels as delivery vehicles for PDLSCs, compared with cell-free hydrogel controls or untreated bone defects, in promoting bone regeneration in animal models with defects?”
Eligibility criteria
Original, peer-reviewed, full-text animal studies (any species, any publication year, searched on March 21, 2025) that tested hydrophilic biomaterial hydrogels such as GelMA, alginate, collagen, chitosan-oxidized chondroitin sulfate (CHI-OCS), or poly (lactic-co-glycolic acid)–polyethylene glycol–poly (lactic-co-glycolic acid) (PLGA-PEG-PLGA) loaded exclusively with PDLSCs to repair bone defects were included. Papers qualified only if they (i) were conducted in vivo, (ii) compared the PDLSC-hydrogel with an appropriate control (empty defect, cell-free hydrogel, or nonfunctionalized scaffold), and (iii) reported at least one quantitative bone-healing outcome (e.g., bone volume/total volume [BV/TV], BMD, trabecular thickness, histomorphometry).
Studies limited exclusively to in vitro or ex vivo experimental models, without in vivo validation in animal models, were excluded. Purely in vitro or ex vivo studies; biomaterials that were not hydrogels (sponges, membranes, and foams); investigations using mixed or non-PDLSC cell populations; experiments lacking a relevant control group; articles in languages other than English; conference abstracts, case reports, pilot or feasibility studies, reviews, and other nonpeer-reviewed formats were excluded. If any record whose full text remained unavailable after two documented contact attempts with the authors via the corresponding email and researchgate.com.
Information sources and databases
A comprehensive and systematic search was independently performed by two experienced reviewers (T.S.A. and E.T.C.) across four major biomedical databases and portals: PubMed, Scopus, Embase, and Web of Science. Reference lists of included articles and related systematic reviews were manually screened.
Search strategy
The search strategy was structured using a combination of Medical Subject Headings, controlled vocabulary, and relevant free-text terms grouped into three conceptual domains: hydrogel-related terms, stem cell-related terms, and periodontal-related terms. Representative terms (e.g., hydrogel, stem cells, periodontitis) within each block were linked with AND or OR to build the final queries. The full, database-specific strings are provided in Supplementary Table S1.
Study selection process
After duplicate removal in EndNote X9 (Clarivate Analytics, USA), all records were subjected to blinded independent screening in Rayyan (Rayyan Systems Inc., Qatar Computing Research Institute, Qatar) by two reviewers. An initial calibration exercise using the first 20 full-text articles was conducted to ensure alignment on eligibility criteria. Disagreements were resolved by a third reviewer (W.L.O.R.).
Data extraction
Data extraction was independently performed by two reviewers using a standardized Excel spreadsheet. Extracted variables included study details, characteristics of PDLSCs, hydrogel properties, in vitro and in vivo methodologies, comparative groups, and main outcomes. Authors were contacted to clarify unclear or missing data when necessary. Extracted data were compiled in comparative tables for synthesis and interpretation.
Risk of bias assessment
The methodological quality of the included studies was assessed using SYRCLE’s Risk of Bias tool, which was adapted from the Cochrane guidelines for use in animal research. 24 This evaluation considered key domains, including random sequence generation, baseline characteristics, allocation concealment, random housing, blinding of caregivers and investigators, random outcome assessment, blinding of outcome assessors, completeness of outcome data, and selective outcome reporting.
Two reviewers independently judged each domain, with disagreements resolved through discussion until consensus was reached. To facilitate interpretation of the risk of bias judgments, a traffic-light summary figure was generated for all included studies. The risk of bias visualization was produced using the RobVis tool 25 for graphical reporting in systematic reviews.
Data synthesis and statistical analysis
Due to significant methodological heterogeneity, a meta-analysis was not performed. Instead, a narrative synthesis was conducted, tabulating quantitative outcomes and summarizing qualitative findings from histological analyses. The synthesis also identified methodological patterns, strengths, and weaknesses while highlighting the need for standardized reporting to support future meta-analytic efforts.
Results
Study selection
The systematic search identified a total of 938 records across four databases: PubMed (n = 288), Scopus (n = 240), Embase (n = 217), and Web of Science (n = 193). After removal of 424 duplicates, 514 unique records were screened by title and abstract. Of these, 497 were excluded for not meeting the eligibility criteria. The remaining 17 full-text articles were assessed for eligibility, and none were classified as irretrievable. Six studies were excluded from full‐text review: two were in vitro investigations, and four did not employ PDLSC delivery via hydrogels. As a result, 11 studies met all inclusion criteria and were included in the qualitative synthesis (Fig. 1).
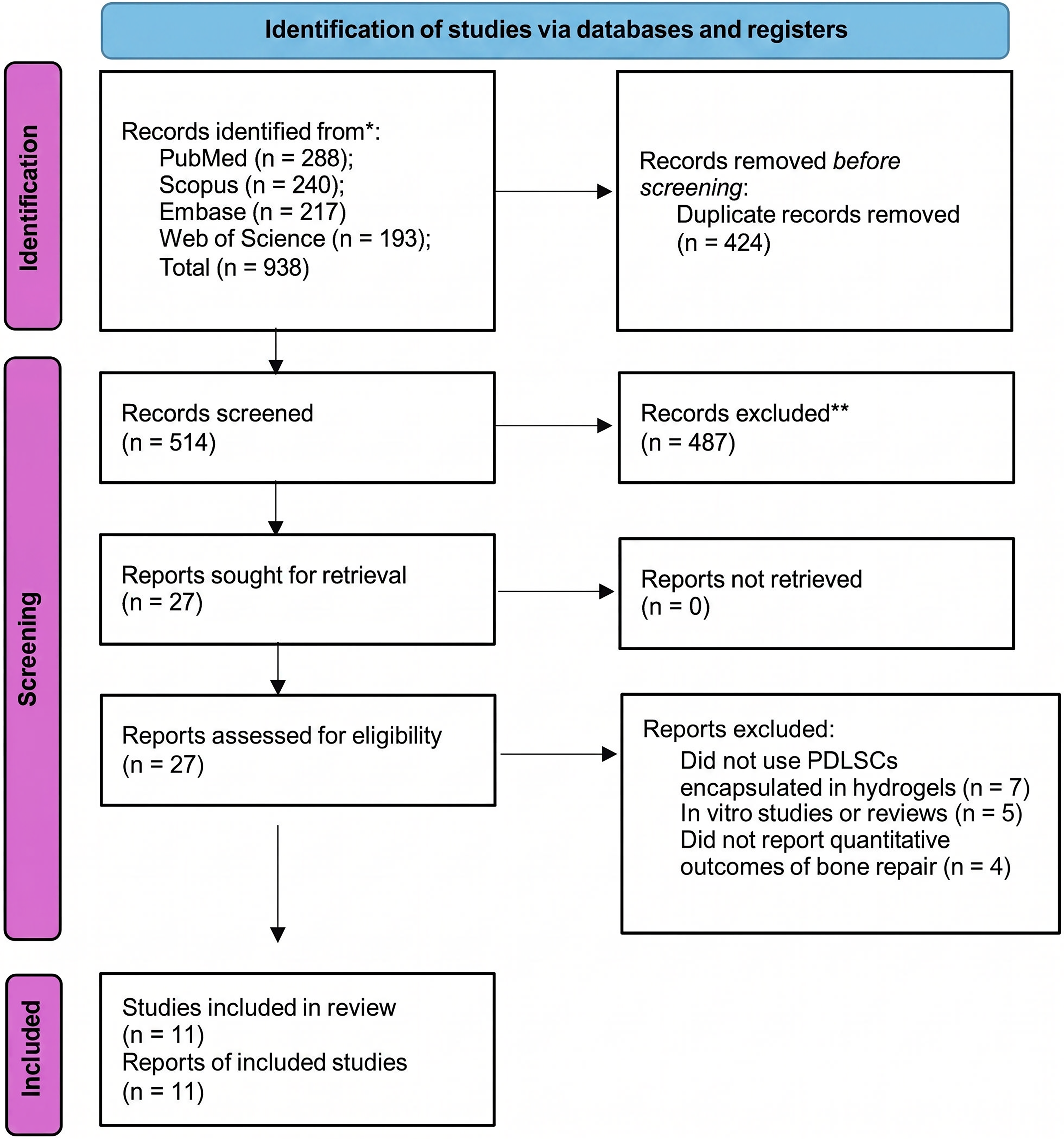
PRISMA flow diagram illustrating the study identification, screening, eligibility assessment, and inclusion process. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Characteristics of included studies
The included studies were published between 2014 and 2024 and were predominantly conducted in China. The experimental parameters, including country of origin, animal model, anatomical site, defect size, hydrogel application method, follow-up time, and control groups, are summarized in Table 1, which highlights the substantial variability across studies with respect to animal species, defect location, and follow-up duration, underscoring the heterogeneity of the experimental designs included in this review. One study originated from Portugal, and others involved collaborations with institutions in Belgium and the United States. The most frequently used animal model was the rat (n = 8), followed by mini pigs (n = 2) and mice (n = 1). All studies induced critical-sized bone defects in various anatomical regions, including alveolar, mandibular, calvaria, and periodontal areas. Notably, small-animal (rodent) and large-animal (mini-pig) models were evaluated separately to preserve biological and physiological relevance across species. Hydrogel concentrations generally ranged from 5% to 15%, and PDLSC doses varied from 1 × 106 to 3 × 106 cells per defect site. Defect dimensions varied considerably depending on the anatomical area and the animal model used, ranging from small fenestration-type defects (3 × 2 × 1 mm) to large volumetric defects in mini pigs (1.0 × 1.2 × 0.6 cm). Follow-up periods ranged from 4 to 12 weeks, with 8 weeks being the most frequently adopted timepoint.
General Characteristics of Included Studies

AuNP, gold nanoparticle; CHI-GEL, chitosan–gelatin; CPC, calcium phosphate cement; GelMA, gelatin methacryloyl; nHA, nanohydroxyapatite; PDGF-BB, platelet-derived growth factor-BB; PDLSC, periodontal ligament stem cell; Y-GOQD, yttrium-doped graphene oxide quantum dot.
Regarding biomaterial applications, most studies employed injectable hydrogels for defect filling, while others utilized prefabricated or 3D-printed scaffolds surgically implanted into the defect site. Table 2 highlights a preference for injectable systems in anatomically complex defects, reflecting their adaptability to irregular geometries. All experiments included at least one appropriate negative control group, such as cell-free hydrogels, nonfunctionalized scaffolds, or empty defects. Stem cells were predominantly derived from human periodontal ligament tissues obtained from extracted third molars or premolars, except for one study that used rat-derived PDLSCs. 29 All studies used stem cells at passages 3 to 6 and performed phenotypic characterization using flow cytometry, either alone or in combination with immunofluorescence, to confirm the mesenchymal identity of PDLSCs. Commonly reported markers included (CD90+), CD105+, CD146+, and STRO-1+, while the absence of hematopoietic markers such as CD34– and CD45– was consistently verified. This consistency in cell characterization, summarized in Table 3, supports the comparability of biological inputs across studies despite differences in experimental models.
PDLSC Origin, Cultivation, and Characterization

AA, ascorbic acid or sodium ascorbate; BMP-2, bone morphogenetic protein-2; CD, cluster of differentiation; Dexa, dexamethasone; DMEM, Dulbecco’s modified Eagle medium; FBS, fetal bovine serum; HG, high glucose; IF, immunofluorescence; LG, low glucose; P3, P4, and so on; PDL, periodontal ligament; PDLSC, periodontal ligament stem cell; pen-strep, penicillin–streptomycin; α-MEM, alpha minimum essential medium; β-GP, beta-glycerophosphate; cell passage number.
Hydrogel Properties and Experimental Parameters

3D, three-dimensional; AuNP, gold nanoparticle; CG, chitosan–gelatin; CHI-GEL, chitosan–gelatin; CHI-OCS, chitosan–oxidized chondroitin sulfate; CPC, calcium phosphate cement; GelMA, gelatin methacryloyl; nHA, nanohydroxyapatite; PDGF-BB, platelet-derived growth factor-BB; PDLSC, periodontal ligament stem cell; PLGA–PEG–PLGA, poly (lactic-co-glycolic acid)–polyethylene glycol–poly (lactic-co-glycolic acid); RGD, arginine–glycine–aspartic acid peptide; Y-GOQD, yttrium-doped graphene oxide quantum dot.
Figure 2 presents the overall distribution of hydrogel types, PDLSC passage ranges, animal models, and applications across the included in vivo studies. It illustrates the predominance of GelMA-based injectable hydrogels and rat models, providing a visual overview of prevailing experimental trends in the field. GelMA was the most frequently used hydrogel formulation, with most delivery systems applied via injectable scaffolds. Most studies used PDLSCs at early passages (P3–P5) and employed rat models to evaluate bone regeneration in mandibular, alveolar, calvarial, periodontal, or orthodontic defects. Common outcomes included increased bone volume, mineralization, structural organization, and neovascularization, highlighting the regenerative potential of hydrogel-based PDLSC delivery platforms. These aspects are comprehensively presented in Table 3.

Distribution of animal models, defect types, and hydrogel formulations used across the included in vivo studies. Created in BioRender. Da Rosa, W.L.O. https://BioRender.com/upt7eo5
Risk of bias
Overall, the risk of bias across studies was considered moderate. Most studies showed a low risk in the domains related to completeness of outcome data and baseline comparability between groups. However, many domains remained rated as “unclear,” particularly with respect to allocation concealment, blinding of caregivers, and random housing, due to insufficient methodological details provided in the manuscripts. Three studies reported the use of randomization procedures,13,19,32 and another three described blinding of outcome assessors.13,22,28 Detailed domain-specific judgments for each study are presented in Figure 3 and Table 5.

Summary of the risk of bias assessment for the included studies based on SYRCLE’s tool for preclinical animal research. SYRCLE, Systematic Review Centre for Laboratory Animal Experimentation.
SYRCLE Risk of Bias Assessment for Included Studies

AC, allocation concealment; BC, baseline characteristics; BOA, blinding of outcome assessors; high, high risk of bias; IOD, incomplete outcome data; judgment levels: low, low risk of bias; PC, blinding of caregivers; RH, random housing; ROA, random outcome assessment; RS, random sequence generation; SRR, selective outcome reporting; unclear, unclear risk of bias.
Summary of quantitative and qualitative outcomes of in vivo bone regeneration
Collectively, the results showed that hydrogels as delivery vehicles for PDLSCs promoted repair or regeneration across multiple bone defect types compared with respective control groups. Despite these promising outcomes, heterogeneity in experimental design, hydrogel formulation, and outcome measures limits comparability and precludes meta-analysis. Importantly, data from small-animal models (rats and mice) and large-animal models (mini pigs) were not pooled in a single quantitative analysis due to marked physiological and anatomical differences that could confound interpretation. Across the five anatomical categories analyzed, several convergent trends emerged regarding the efficacy of PDLSC-loaded hydrogels for bone regeneration. Quantitative analyses were predominantly based on micro-CT, assessing BV/TV, trabecular thickness, trabecular number, and BMD. Histomorphometry was also employed in selected models. Given this heterogeneity, a qualitative narrative synthesis was deemed the most appropriate approach, allowing results to be interpreted within the biological context of each animal model and defect type. A detailed synthesis of these quantitative and qualitative outcomes, including evaluation methods, osteogenic markers, and neovascularization findings, is provided in Table 4.
In Vivo and Histological Outcomes with Marker Expression for Each Application

BV/TV, bone volume/total volume; BMD, bone mineral density; Tb.Th, trabecular thickness; Tb.N, trabecular number; HE, hematoxylin and eosin; IHC, immunohistochemistry; CT, computed tomography; COL1, collagen type I; RUNX2, runt-related transcription factor 2; OCN, osteocalcin; ALP, alkaline phosphatase; DMP1, dentin matrix protein 1; CD31, cluster of differentiation 31, endothelial marker; OPG, osteoprotegerin; LC3B, microtubule-associated protein 1 light chain 3 beta; PDGF-BB, platelet-derived growth factor-BB; PDL, periodontal ligament.
Mandibular defects
Mandibular defects were primarily induced in rats and mini-pig models through surgical bone excisions in the posterior mandible or edentulous ridges. These models allowed assessment of large and load-bearing bone defects. One study 19 reported that the use of PDLSCs embedded in a graphene oxide-modified GelMA hydrogel enhanced bone volume and mineral density, in addition to improving the orientation of newly formed collagen fibers. In another experiment 30 using rat mandibles, the application of a 10% GelMA hydrogel scaffold led to a denser and more mineralized bone matrix, with improved trabecular organization. Another study 6 in a mini-pig model demonstrated that a composite scaffold of chitosan-gelatin with nano-hydroxyapatite (CG/nHA), loaded with PDLSCs, supported extensive trabecular bone formation and the presence of embedded osteocytes, indicating advanced stages of bone maturation.
Overall, robust increases in BV/TV, BMD, and trabecular organization were found in mandibular defects, particularly in large animal models. Histological findings confirmed the presence of organized collagen and mature osteoid, while mineralization was frequently enhanced by the use of 10% GelMA scaffolds or composite matrices incorporating nano-hydroxyapatite. 30
Alveolar defects
Alveolar defects were surgically created in the socket or ridge area of rats. In models simulating extraction sites or alveolar dehiscence, the use of PDLSCs encapsulated in injectable collagen hydrogels functionalized with BMP-2 showed significant new bone formation and signs of vascular invasion. 26 In another experiment, 22 a collagen-based matrix incorporating gold nanoparticles and seeded with PDLSCs promoted mineralization and tissue ingrowth, as evidenced by organized lamellar bone and neovascularization formation within the scaffold region.
Alveolar bone defects, often mimicking postextraction sites, demonstrated substantial mineralized tissue formation and neovascularization, especially when injectable hydrogel systems were used. 26 Functionalization with agents such as BMP-2 gold nanoparticles contributed to increased trabecular number and improved matrix architecture. 22 Quantitative micro-CT measurements supported these observations, and immunohistochemical staining consistently identified osteogenic markers such as RUNX2, COL1, ALP, and OCN. 26
Periodontal defects
Periodontal defects were predominantly three-wall or fenestration-type defects created in the buccal aspect of the molar regions in rats. In these models, PDLSCs were delivered via diverse hydrogel matrices such as alginate-chitosan, thermosensitive PLGA-PEG-PLGA, and GelMA. Across studies, the application of hydrogel-encapsulated PDLSCs consistently led to greater bone fill and improved periodontal ligament-like tissue regeneration, often accompanied by increased vascularization and cementum deposition. 29 In some models, functionalization of the hydrogel with PDGF-BB or RGD peptides resulted in superior integration of newly formed tissue and enhanced alveolar bone architecture compared with controls. 13 Osteogenic induction using dexamethasone and β-glycerophosphate was commonly employed prior to transplantation, enhancing cellular differentiation and matrix deposition.
The most consistent improvements in periodontal defect models involved increased trabecular thickness and bone fill, accompanied by signs of periodontal ligament-like tissue regeneration. 29 Histological sections frequently revealed organized fiber insertion and the presence of cementum-like structures. 29 Composite hydrogels containing metformin, PDGF-BB, or RGD peptides showed superior outcomes in terms of osteoid formation, vascular ingrowth, and scaffold integration with native tissues. 28
Calvaria defects
A calvarial defect model was included.28,31,32 Standardized 5 mm circular defects were created in the rat parietal bone. PDLSCs encapsulated in a thermosensitive hydrogel were applied, resulting in increased bone volume and trabecular connectivity. Micro-CT analysis revealed a substantial rise in BMD 32 and histological evaluation demonstrated mature bone bridging across the defect with seamless integration into host tissue. 28
Overall, this model exhibited enhanced bone density and volume. Continuous trabecular bridges were visible on micro-CT, and a mature, mineralized matrix was evident histologically within eight weeks, supporting the efficacy of thermosensitive hydrogels in guiding calvarial bone regeneration.28,31,32
Orthodontic bone loss
Orthodontic bone loss was assessed in rats undergoing first-molar movement. 22 After removing the orthodontic force, PDLSCs delivered in gold nanoparticle-functionalized collagen hydrogels maintained BMD and trabecular structure. Micro-CT confirmed preserved trabecular number and bone volume, and histology showed continuous bone bridging, aligned collagen fibers, and ligament-like tissue formation at treated sites. These findings demonstrate the effectiveness of gold nanoparticle-enhanced hydrogels for localized PDLSC delivery under orthodontic stress. 22
Discussion
All studies reported favorable outcomes in bone regeneration using hydrogels as delivery vehicles for PDLSCs. These results support the evidence for the regenerative potential of PDLSCs, which is attributed to their multilineage differentiation capacity, immunomodulatory functions, and proangiogenic properties, features that make them promising candidates for advanced tissue engineering approaches beyond traditional periodontal repair. 28 However, considerable methodological heterogeneity was observed among the studies, particularly regarding hydrogel composition, stem cell source, animal models, anatomical implantation sites, and follow-up durations. While periodontitis represents the classical indication for PDLSC-based therapy, given its hallmark of connective tissue and alveolar bone destruction, 29 this systematic review reported encouraging outcomes for PDLSC‐based treatments across a broader spectrum of bone defect models, including calvarial, mandibular, alveolar, and orthodontic defects.
Beyond the descriptive synthesis of the included studies, some consistent patterns emerged that help explain the observed regenerative outcomes. One relevant aspect is the ability of hydrogels to create a biomimetic microenvironment that favors the survival and function of PDLSCs after implantation. 8 Unlike traditional scaffold systems, hydrogels closely resemble the hydrated structure of the extracellular matrix, which facilitates nutrient diffusion, cell migration, and paracrine signaling. 21 This microenvironment may enhance the biological activity of PDLSCs, allowing them to exert both direct osteogenic differentiation and indirect regenerative effects through the secretion of bioactive factors. 12
From a translational perspective, the characteristics of the bone defect appear to be an important factor guiding scaffold selection. Injectable hydrogel systems offer practical advantages in defects with complex geometries, such as periodontal and irregular alveolar defects, as they can conform to the morphology of the defect and allow minimally invasive delivery of PDLSCs. 33 In contrast, preformed or 3D-printed scaffolds may provide superior mechanical stability and structural support in larger or load-bearing defects, in which space maintenance and mechanical integrity are critical for tissue regeneration. 20 Therefore, scaffold selection in PDLSC-based regenerative strategies should consider both the anatomical configuration of the defect and its mechanical requirements, suggesting that injectable hydrogels and structurally reinforced scaffolds represent complementary approaches rather than competing technologies.
When hydrogel-based systems were compared with other scaffold types in the included studies, hydrogels generally demonstrated favorable regenerative outcomes, particularly in terms of cell viability and integration with host tissues. 11 Their highly hydrated structure may support efficient cell encapsulation and facilitate the diffusion of nutrients and signaling molecules, which are critical for maintaining PDLSC functionality. 21 However, some scaffold systems, such as polycaprolactone, may provide superior mechanical properties and structural stability, which may be advantageous in larger or mechanically demanding defects. 34 These findings suggest that although hydrogels are highly effective as cell delivery platforms, their performance may depend on the specific mechanical and anatomical requirements of the defect. 35
Hydrogels and PDLSCs used
Hydrogels varied substantially in their composition, bioactivity, and delivery formats. Nonetheless, all studies consistently indicated that hydrogel-based systems carrying PDLSCs improved bone regeneration relative to control conditions. 28 GelMA was the most frequently employed scaffold, supporting significant increases in bone volume, mineral density, and trabecular organization. 19 Thermosensitive PLGA-PEG-PLGA hydrogels, especially when functionalized with PDGF-BB, appeared to facilitate both osteogenesis and neovascularization. 26
Additional strategies included alginate-based hydrogels combined with calcium phosphate cement and metformin, leading to substantial enhancements in bone formation and vascularization. 28 CHI-OCS scaffolds, particularly with aligned fiber orientation, promoted tissue organization, trabecular alignment, and increased bone density. 29 Composite constructs integrating type I collagen and gold nanoparticles yielded superior morphometric and molecular outcomes, while scaffolds modified with immunoregulatory agents exhibited anti-inflammatory and osteoinductive potential. 22
The regenerative efficacy of these systems was also influenced by scaffold architecture (e.g., injectable, prefabricated, or 3D-printed), polymer concentration (ranging from 5% to 15%), and the applied dose of PDLSCs (typically 1 × 106 to 3 × 106 cells per site). 19 Functionalization with bioactive agents such as metformin, PDGF-BB, RGD, or gold nanoparticles appeared critical in enhancing biological performance. 26 Overall, these findings suggest that the synergistic combination of PDLSCs and bioengineered hydrogels supports consistent and superior bone regeneration across various preclinical models.
All included studies verified the mesenchymal origin of PDLSCs using flow cytometry, identifying expression of canonical markers such as CD90, CD105, CD146, and STRO-1, while confirming the absence of hematopoietic markers like CD34 and CD45. 29 One study 29 utilized rat-derived PDLSCs, while the others used human cells. Cells were typically expanded up to passages 3–5 and cultured in alpha-Minimum Essential Medium or Dulbecco’s modified Eagle medium media enriched with fetal bovine serum and osteoinductive factors. 26 The passage number, cell density (1 × 106 to 3 × 106), and culture medium varied, yet all models showed osteogenic differentiation and integration in vivo, emphasizing the translational reproducibility of PDLSC protocols.
Efficacy of hydrogels as delivery vehicles for PDLSCs across bone defect models
In periodontal defects, PDLSCs delivered via implanted aligned‐porous CHI-OCS scaffolds promoted alveolar bone fill and the formation of cementum-like and ligament-like tissues, 29 while prefabricated 3D-printed GelMA scaffolds matched defect geometry and improved trabecular organization and mechanical stability, 13 and injectable thermosensitive PLGA-PEG-PLGA hydrogels functionalized with PDGF-BB gelled in situ to facilitate cell retention and neovascular invasion. 26
In mandibular and alveolar defects, especially in large animal models, PDLSCs encapsulated in injectable GelMA hydrogels (5% w/v) achieved uniform cell distribution with significant increases in bone volume fraction and trabecular connectivity 19 and 10% GelMA further enhanced matrix mineralization; 30 similarly, alginate hydrogels combined with calcium phosphate cement and metformin provided sustained osteoinductive release and markedly improved bone formation, 28 whereas implanted CG/nHA composite scaffolds supported robust osteocyte incorporation in minipigs. 6
In calvarial defects, injectable RGD-modified alginate microspheres encapsulating PDLSCs enabled in situ gelation and significant gains in bone volume fraction and trabecular connectivity, 31 implanted CHI-GEL/nHA composite scaffolds provided aligned porosity for continuous trabecular networks by 6 weeks, 32 and injectable calcium phosphate cement scaffolds with PDLSCs and metformin achieved the highest new bone area and neovascular density. 28
In orthodontic bone loss models, PDLSCs delivered via injectable type I collagen hydrogels functionalized with gold nanoparticles preserved BMD and trabecular architecture under mechanical loading. 22 Together, these data suggest that preformed scaffolds deliver mechanical stability potentially suitable for load-bearing and large defects, whereas injectable systems offer minimally invasive delivery and conformability to irregular geometries; selecting the appropriate hydrogel thus requires balancing handling ease, gelation kinetics, mechanical support, and controlled release of bioactive cues for each clinical application.
A significant translational gap remains regarding the synchronization of hydrogel degradation with host bone turnover. While large animal models (e.g., minipigs) are structurally more predictive of human outcomes than rodent models, porcine bone metabolism and healing rates are considerably faster than those of humans. 36 Consequently, a hydrogel optimized to match the rapid regeneration of porcine bone may degrade too quickly when applied in humans, potentially leading to mechanical instability before adequate bone tissue is formed. 37 Future clinical translation must explicitly address how hydrogel degradation kinetics align with human bone turnover rates.
Methodological heterogeneity, limitations, and risk of bias
The included studies displayed pronounced methodological heterogeneity. Defect dimensions ranged from 3 × 2 × 1 mm to 10 × 12 × 6 mm, and models targeted distinct anatomical sites, mandibular, calvarial, or alveolar bone. Hydrogels were prepared at concentrations between 5% and 15% (w/v), while PDLSC doses varied from 1 × 106 to 3 × 106 cells per site. Moreover, investigators employed different animal species, from rodents and mice to minipigs, introducing additional biological variability. Collectively, these divergences limit direct comparison of outcomes and preclude a robust quantitative synthesis.
Risk-of-bias assessment revealed pervasive shortcomings: allocation concealment, random housing, and blinded outcome assessment were often inadequately reported and thus rated as “unclear,” and no study achieved a low-risk verdict across all SYRCLE (Systematic Review Center for Laboratory Animal Experimentation) domains. Furthermore, limitations of the included studies often comprised small sample sizes, which may reduce statistical power, and a lack of randomization details. These deficits weaken reproducibility and temper confidence in pooled conclusions. In addition, this review process itself is subject to limitations, such as the potential for language bias due to the exclusion of non-English literature.
Future investigations should adopt harmonized protocols for hydrogel formulation, cell validation, defect modeling, and outcome measurement, while also reporting randomization and blinding transparently. Although variability remains substantial, all studies indicated that PDLSC-laden hydrogels elicited superior bone regeneration relative to controls. Functionalization with growth factors, nanoparticles, or fiber alignment further enhanced performance, and next-generation “smart” hydrogels capable of stimulus-responsive release of bioactive cues may define the forthcoming frontier in periodontal and craniofacial tissue engineering. Despite their advantages, hydrogel-based systems also present some limitations in vivo. Their relatively low mechanical strength and limited ability to maintain space may restrict their use in large or load-bearing defects, and their degradation behavior may influence host responses depending on the material composition. 29 These factors highlight the importance of careful hydrogel design when developing regenerative strategies.
In general, the findings of this review suggest that hydrogels offer potential as vehicles for PDLSCs in oral and craniofacial regenerative applications, but substantial heterogeneity in scaffold formulations, cell dosages, and implantation protocols, as well as the limited number of methodologically comparable studies and high risk of bias, precludes definitive conclusions regarding efficacy. Moreover, long-term outcomes, immunological responses, and the mechanical stability of regenerated tissues were rarely assessed. To facilitate clinical translation, future investigations should adopt unified guidelines for hydrogel preparation, stem-cell encapsulation, and outcome evaluation; report in detail scaffold mechanical properties, degradation kinetics, and in vivo integration; and include direct comparisons between PDLSCs and other mesenchymal stem-cell sources (e.g., bone marrow or adipose-derived) to clarify the specific advantages of periodontal ligament-derived cells in tissue-engineering contexts.
Conclusions
This systematic review indicates that hydrogels can function as delivery vehicles for PDLSCs, potentially enhancing bone regeneration across various defect models. Mandibular and alveolar defects showed improved trabecular structure, mineral density, and neovascularization. Periodontal models presented not only bone fill but also regeneration of ligament-like tissues, indicating functional integration. Calvarial defects benefited from enhanced matrix formation and osteogenic activity, while orthodontic bone loss models exhibited preservation of bone mass and activation of reparative pathways. Although variability in hydrogel composition, cell doses, animal models, and outcome measures was noted, all included studies reported superior results in PDLSC-loaded groups. These findings highlight the translational promise of hydrogel-based systems, while emphasizing the need for standardized protocols, long-term validation, and functional outcomes to advance clinical application in periodontal and craniofacial regenerative therapies.
Authors’ Contributions
T.S.d.A. conceptualized and designed the study, performed data analysis, and drafted the article. E.T.C. and T.M.M. contributed to data extraction, methodology validation, and article editing. W.L.O.R. provided supervision, critical review, and final approval of the article. All authors contributed to data interpretation, approved the final version, and agree to be accountable for all aspects of the work.
Footnotes
Disclosure Statement
The authors declare that there are no conflicts of interest regarding the publication of this article.
Funding Information
This study was financed in part by the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq), grant number 406004/2024-2.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.