
Abstract
Injuries to the avascular region of the knee meniscus—the inner “white–white” zone—pose a significant therapeutic challenge due to its lack of vascular supply and limited intrinsic healing capacity. While conventional meniscal repair techniques often fail in this region, recent advances in regenerative medicine have turned to explant culture systems as a bridge between simple cell cultures and complex in vivo models. This review synthesizes the current literature on the role of explant cultures in understanding and advancing avascular meniscus repair. Explant cultures maintain native extracellular matrix structure and provide a controlled three-dimensional environment to study cellular responses to injury. Within these systems, a distinct subpopulation of cells termed migratory meniscus cells emerge from the tissue edge, exhibiting progenitor-like features, including clonogenicity, multipotency, and responsiveness to transforming growth factor-β signaling. These cells have demonstrated the capacity to infiltrate defect zones, remodel extracellular matrix, and synthesize reparative fibrocartilaginous tissue. Experimental manipulations within explant models, including fibrin scaffolds, enzymatic border conditioning, sequential growth factor delivery, mechanical loading, and electrical stimulation, have shown promise in enhancing integration strength and tissue quality. These studies underscore the importance of biochemical and biophysical cues in orchestrating effective repair in avascular regions. Current explant systems, however, are constrained by limited culture durations, the absence of vascular and immune components, and species-specific differences in matrix biology, thereby limiting their ultimate utility in translational research. Despite these limitations, explant models remain essential for dissecting the mechanistic basis of meniscal repair and for evaluating candidate therapies in a reproducible, hypothesis-driven manner. Looking ahead, next-generation platforms incorporating perfusion bioreactors, immune cocultures, and validated integration assays will be critical to better replicate in vivo physiology. Personalized strategies targeting patient-specific tear characteristics and cellular profiles, including autologous progenitor cell delivery and biomaterial-based signaling systems, hold potential for transforming the clinical management of avascular meniscus injuries. This review highlights the central role of explant cultures in shaping such innovations and guiding their translation into meaningful orthopedic therapies.
Impact Statement
This review summarizes the current state of meniscal explant culture models for avascular-zone repair and explains how they can serve as a practical, translational bridge between cell studies and in vivo models. This will help guide development of true meniscus-preserving therapies that will eventually lead to deliverable solutions that will revolutionize meniscus injury care.
Introduction
The menisci serve as critical biomechanical structures within the knee, distributing loads, aiding joint congruity, and contributing to proprioception and lubrication.1–3 Injuries to the menisci compromise these functions and, if not properly addressed, predispose the joint to progressive degenerative changes.4,5 Particular concern arises from injuries that affect the avascular region of the meniscus, known as the white-white zone. Healing in this region is hindered by the absence of vascular support, resulting in a lack of fibrin clot formation, inflammatory cell infiltration, and endogenous growth factor delivery.6–8 Tears confined to this zone exhibit a poor spontaneous repair response, making them a substantial clinical challenge.9,10 This inherent limitation has prompted interest in strategies that can simulate or substitute for vascular-mediated repair mechanisms. Among such strategies is the application of explant cultures, which offer controlled environments for studying meniscal biology, tissue responses to injury, and potential reparative interventions.11–14
Explant cultures maintain the native three-dimensional matrix of the meniscus, preserving both structural and cellular characteristics. They provide a bridge between isolated cell cultures and in vivo models.15,16 Explant systems have enabled the characterization of migratory meniscus cells, a cell population that emerges from meniscal tissue when cultured ex vivo.17–19 They have been described as a distinct population that emerges from meniscal tissue under explant culture conditions and exhibits several features associated with progenitor-like behavior. However, recent evidence suggests that these cells are better understood within the broader framework of functional heterogeneity among meniscal fibrochondrocytes rather than as a uniform progenitor population analogous to mesenchymal stromal cells derived from bone marrow or synovium.
Ma et al. 20 demonstrated in a recent study while comparing meniscus fibrochondrocytes isolated by collagenase digestion, cellular outgrowth, and digestion-after-outgrowth, that the modality of cell isolation significantly influences cellular phenotype and downstream functional behavior. Outgrowth-isolated cells, most closely resembling the migratory cells observed in explant culture systems, displayed a predominantly spindle-shaped morphology, increased proliferative capacity, enhanced migratory behavior, and elevated expression of contractile markers, including alpha-smooth muscle actin and transgelin. In contrast, digestion-after-outgrowth cells exhibited greater chondrogenic capacity and generated larger matrix-rich microtissues, while digestion-isolated cells demonstrated intermediate characteristics. These cells have attracted attention for their potential role in repair and regeneration due to their expression of progenitor markers and motile behavior.17,21,22
This literature review explores how explant culture systems, with particular focus on migratory meniscus cells, contribute to the understanding and advancement of avascular meniscus repair. The review spans meniscal biology, conventional treatment methods, experimental models, cellular mechanisms, and translational directions with their relevance to clinical applications.
Methods
A comprehensive search of scientific databases, including PubMed, Scopus, Web of Science, and Embase, was conducted to identify literature relevant to explant-based meniscal repair. The search strategy employed Boolean combinations of key terms, including “explant culture,” “meniscus,” “migratory meniscus cells,” “avascular meniscus repair,” “fibrochondrocytes,” “growth factors,” “scaffolds,” and “cyclic loading.” Only articles published in English before 2025 were considered. Studies were screened based on abstract content, followed by full-text review for relevance to explant culture methodology, cellular behavior, and tissue engineering applications. Reference lists of selected publications were reviewed to capture additional relevant works. Foundational articles were incorporated to provide historical context for recent developments. The final review included 104 peer-reviewed articles and was completed in July 2025.
Pathobiology and Contemporary Management
The meniscus is a semilunar fibrocartilaginous structure in the knee, with two distinct medial and lateral meniscal structures.2,23 The collagen network within the meniscus is oriented to resist hoop stresses, and the cellular composition varies according to location.24,25 The vascular anatomy reveals that only the peripheral 10–30% of the tissue receives direct vascularization, a feature established early in development and persisting into adulthood.2,3,24 The avascular nature of the inner one-third renders it susceptible to nonhealing tears, especially in the setting of degenerative changes or mechanical overload (Fig 1).

Meniscal zone anatomy and avascular zone tear patterns.
Meniscal fibrochondrocytes constitute the primary resident cell type. These cells exhibit mixed phenotypes, expressing both fibroblastic and chondrocytic markers.26–28 In the outer vascularized zone, cells tend to adopt a more fibroblastic phenotype, whereas the inner zone contains cells with chondrocytic characteristics. This regional differentiation may influence the ability of cells to engage in repair processes. Recent evidence supports the existence of meniscus progenitor cells, a subset of cells exhibiting clonogenicity and multipotency. These cells are of particular interest in the context of repair, as they may be harnessed or stimulated in response to injury or culture conditions.17,21,22,29
Healing in the avascular meniscus is limited by the absence of a vascular-mediated inflammatory cascade, fibrin clot formation, and sufficient cell density. Without these elements, tissue cannot bridge a defect or initiate the deposition of extracellular matrix.6–8 Any reparative process must rely on migration of cells from adjacent regions or on supplementation with exogenous cells or signaling molecules.17,30,31 Strategies aiming to enhance such migration or to introduce functional substitutes have gained attention, providing a rationale for evaluating experimental approaches that may overcome these limitations.6,13,30,31
The historical standard for managing avascular meniscal tears has often involved partial meniscectomy.2,23,32 While this procedure provides symptom relief, it involves removal of functional tissue and can accelerate joint degeneration. The altered load distribution contributes to cartilage breakdown, raising the long-term risk of osteoarthritis. 33 Consequently, there has been a shift toward preserving meniscal tissue when possible, even in cases of avascular tears.7,34
Surgical techniques for meniscal repair include inside-out, outside-in, and all-inside suturing procedures.35,36 These approaches are effective primarily in the vascularized periphery, where biological healing potential supports mechanical fixation. However, tears located entirely in the white-white zone exhibit poor healing even when sutured, prompting the development of augmentation techniques. 7
Efforts to improve healing in the avascular meniscus include trephination, rasping, and fibrin clot insertion.37,38 Trephination involves creating vascular access channels to allow blood and cellular components to reach the injury site. Rasping induces a local healing response by mechanically disrupting the tear edge. Fibrin clot implantation introduces an exogenous scaffold that may carry growth factors and facilitate cell migration.37,38 Although these interventions have demonstrated some success, the results are inconsistent and suggest the need for further biological enhancement.6,7,37 This has led to developments expanding into the realm of regenerative medicine, where cell-based therapies and scaffolds are being employed. Mesenchymal stem cell (MSC) injections have been investigated for their ability to populate meniscal defects and contribute to tissue repair.39–41 Similarly, biomaterial scaffolds, both acellular and cell-laden, have been developed to provide a structural and biochemical environment conducive to healing. These concepts align with the observation that introducing cells or creating an environment supportive of cellular recruitment can enhance repair, echoing principles explored in explant culture systems.12,13,39,42,43
Explant Culture Platforms for Avascular Meniscus Research
Explant cultures involve the maintenance of viable meniscal tissue segments under in vitro conditions.12,44,45 Unlike dissociated cell cultures, explants retain native extracellular matrix, allowing for the study of cell behavior within a physiologically relevant environment.12,46 This setup enables reproducible experimentation and direct observation of repair dynamics, including cell migration, matrix deposition, and tissue integration.
Whole-organ explants, commonly derived from animal sources, permit the study of global tissue metabolism and degradation over time.47,48 Slice or wedge models focus on the inner zone and are often employed to simulate avascular injuries. 49 These models allow for improved nutrient diffusion and targeted observation of reparative processes. Standardized defect creation enables comparison of treatment effects, facilitating analysis of repair progression under various experimental conditions.50,51
Explant culture conditions vary substantially across studies and represent a major source of experimental heterogeneity (Table 1). Differences occur across several aspects of experimental design, including media composition, serum concentration, culture duration, mechanical loading, scaffold environment, and cell isolation methods. Media formulation alone varies widely. Some investigators use defined or fibrochondrogenic media supplemented with growth factors to promote matrix synthesis and cellular differentiation, 59 whereas others rely on basal culture conditions or serum supplementation. Even subtle changes in nutrient composition can influence outcomes; for example, alterations in glucose concentration significantly affect proteoglycan production and collagen fiber formation in meniscal cultures. 60 Similarly, serum concentration strongly influences biomechanical properties, with 10% fetal bovine serum producing significantly greater increases in explant Young’s modulus than lower serum conditions. 44
A Selected Summary of Meniscus Explant Studies: Model, Culture Conditions, and Outcomes

This table summarizes representative studies employing meniscus explant models, including species and tissue source, explant or defect configuration, culture medium and biological supplements, experimental interventions, assessment timepoints, and principal outcomes. Together, these studies illustrate the methodological diversity of explant systems used to investigate meniscal repair, cellular migration, matrix synthesis, and integrative healing under controlled in vitro conditions.
BMP, bone morphogenetic protein; DMEM, Dulbecco’s Modified Eagle Medium; DMEM/F12, Dulbecco’s Modified Eagle Medium/Ham’s F-12 nutrient mixture; ECM, extracellular matrix; FBS, fetal bovine serum; FCS, fetal calf serum; FGF-2, fibroblast growth factor-2; GF, growth factor; IL-1β, interleukin-1 beta; ITS, insulin–transferrin–selenium supplement; MDM, meniscus-derived matrix; MSC, mesenchymal stromal cell; NR, not reported; OA, osteoarthritis; PG, proteoglycan; PRP, platelet-rich plasma; rAAV, recombinant adeno-associated virus; TGF-β, transforming growth factor beta; TKR, total knee replacement.
Environmental conditions further modulate experimental outcomes. Mechanical loading protocols, inflammatory stimulation with cytokines such as IL-1β, and scaffold composition can all alter gene expression, cellular migration, and integrative repair responses.52,61,62 Consequently, these methodological differences influence extracellular matrix deposition and tissue integration strength. As highlighted in reviews of explant models, the lack of standardized culture protocols complicates comparisons across studies and likely contributes to the heterogeneous outcomes reported in the literature. 48
Explant coculture systems introduce external cell populations, such as synovial fibroblasts or bone marrow-derived cells, to assess their interactions with meniscal tissue (Fig 2). These setups provide insight into paracrine signaling and the potential for cross-tissue migration.11,48,59,63–65 While explants offer valuable control over variables and enable hypothesis-driven research, limitations include the absence of systemic factors such as immune cell infiltration and the inability to replicate long-term vascularized healing.11,12,48,66 Cellular behavior may also shift during prolonged culture, leading to phenotypic changes that may not reflect in vivo states.27,28,67
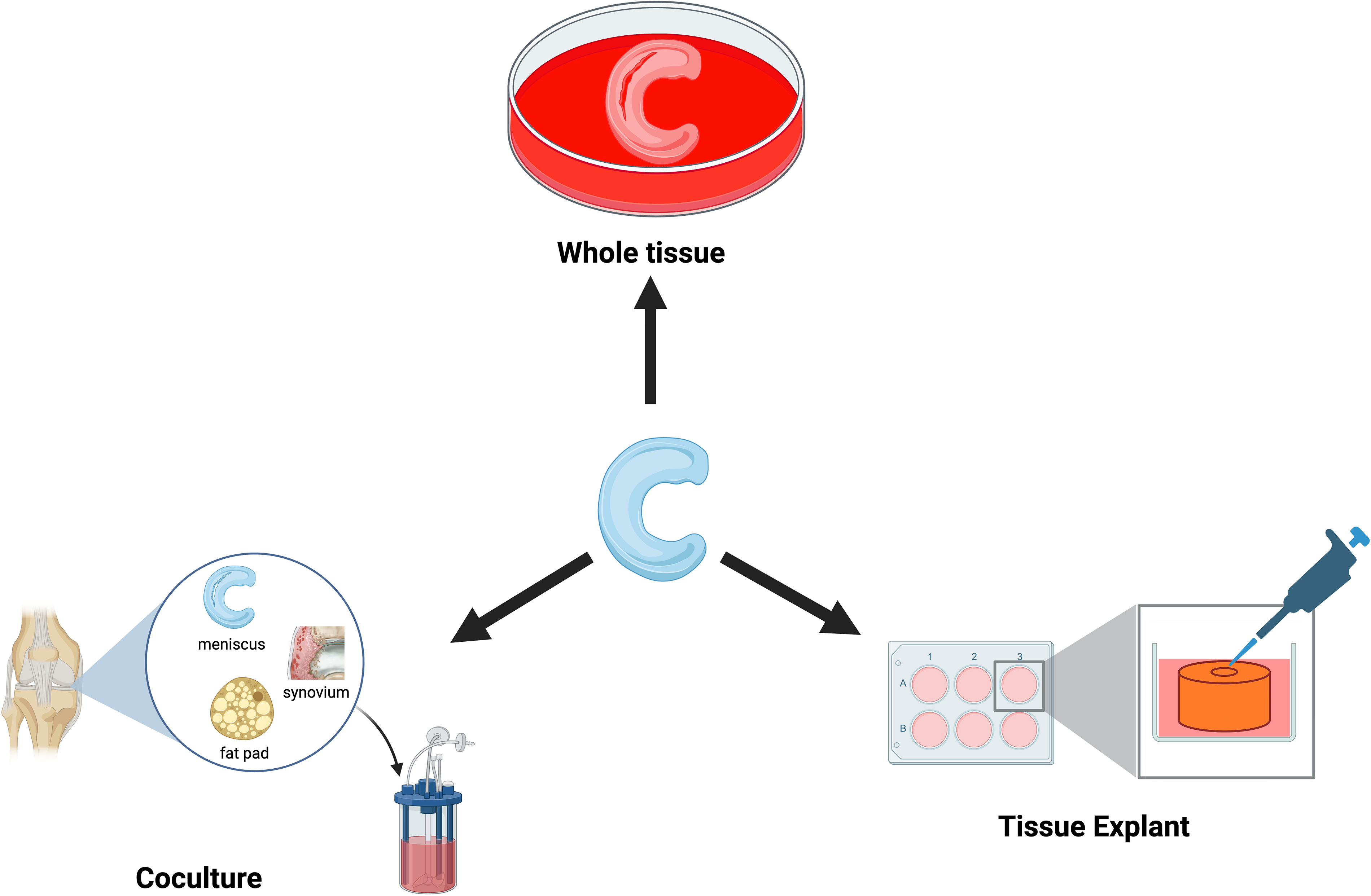
Explant culture platforms for avascular meniscus injury repair.
Cartilage explants have been widely studied in the past. Knowledge gained from these studies can be insightful in conducting meniscal explant studies. These studies collectively show that cartilage and meniscus share several therapeutic responses, including responsiveness to biological stimulation such as platelet-rich plasma (PRP) and related regenerative therapies. 54 Both tissues also contain progenitor-like cell populations that participate in repair processes. 17 However, key biological differences exist between these tissues. Distinct cellular phenotypes differentiate meniscal cells from articular chondrocytes, 67 while extracellular matrix composition differs markedly between fibrocartilaginous meniscus and hyaline cartilage. 1 Healing potential is also influenced by vascular supply within the meniscus. 68 In addition, the meniscus performs unique biomechanical functions within the joint 12 and exhibits marked regional cellular heterogeneity. 67 Therefore, cartilage explant findings can inform general regenerative strategies but require tissue-specific optimization for avascular meniscal repair (Table 2).
Comparison of Cartilage and Meniscus Explant Culture Systems
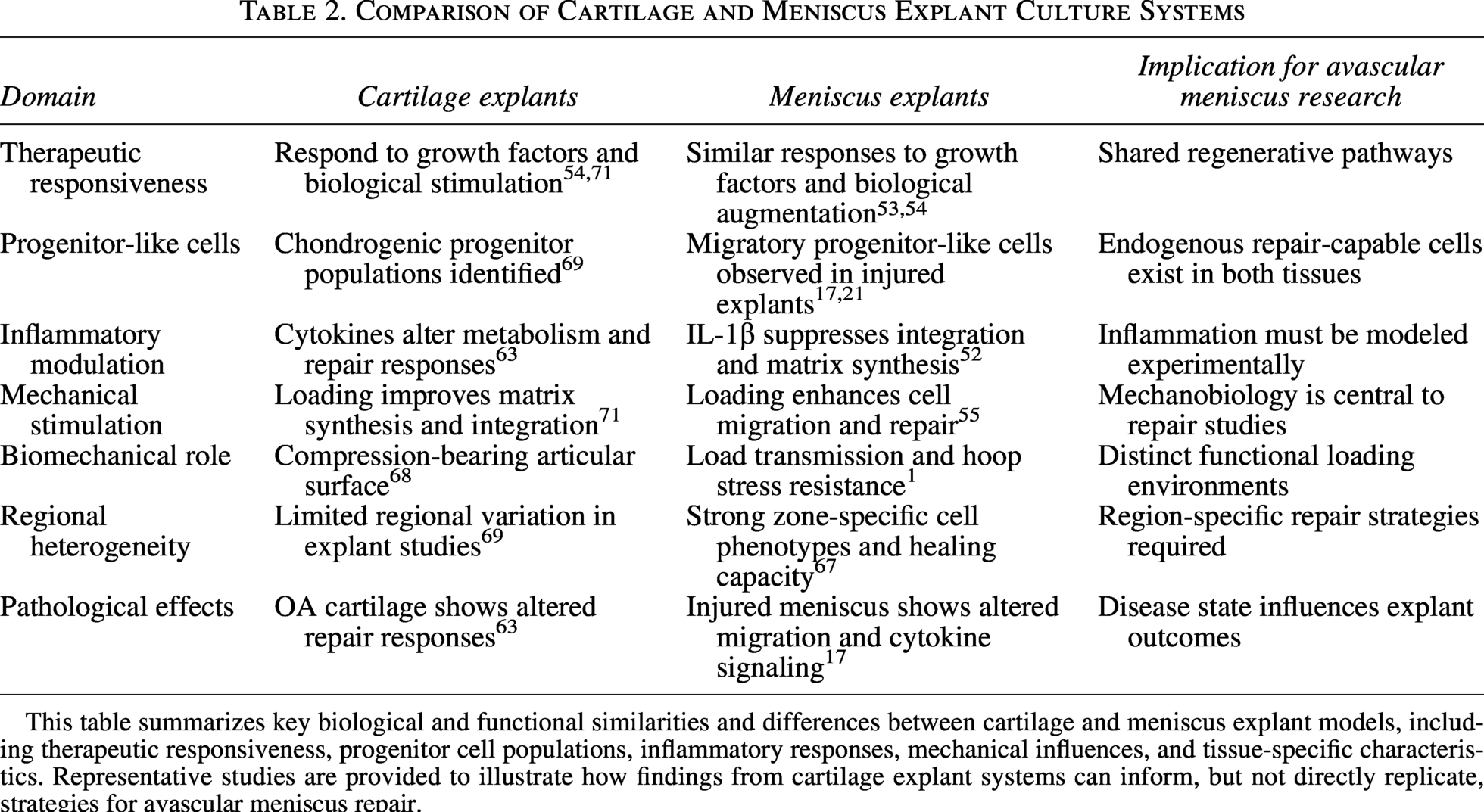
This table summarizes key biological and functional similarities and differences between cartilage and meniscus explant models, including therapeutic responsiveness, progenitor cell populations, inflammatory responses, mechanical influences, and tissue-specific characteristics. Representative studies are provided to illustrate how findings from cartilage explant systems can inform, but not directly replicate, strategies for avascular meniscus repair.
Reparative Cell Dynamics and Experimental Intervention in Explant Models
One notable feature of explant cultures is the observation of cell outgrowth from tissue margins.17,51 These cells, often referred to as migratory meniscus cells, exhibit increased motility and display markers associated with reparative function.17,18,21,22 They have been shown to express alpha-smooth muscle actin, indicating a contractile phenotype, and to exhibit in vitro functions suggestive of myofibroblastic behavior.62,70,72
Studies comparing outgrowth cells with enzymatically isolated cells have reported differences in migratory capacity, with outgrowth cells displaying enhanced motility in scratch assays. These cells often show progenitor-like characteristics, including clonogenic potential and expression of stem cell markers. 73 Their behavior implies that the meniscus harbors a resident population capable of contributing to wound healing.20,22,74
Tissue origin appears to influence the extent of cellular outgrowth. 67 Menisci obtained from osteoarthritic or injured joints exhibit a greater propensity for cell migration in explant culture compared with those from healthy donors.17,47,75 This observation suggests that tissue injury or matrix breakdown may activate latent cellular programs or alter the extracellular matrix in ways that facilitate cell egress. For example, human meniscus explants with structural damage demonstrated spontaneous cell outgrowth from lesion borders, whereas intact samples did not.17,47,56,76
Although human meniscal explants provide the most clinically relevant experimental platform, many samples used in research are obtained from patients undergoing total knee arthroplasty for osteoarthritis.21,56 These tissues frequently exhibit degenerative changes and altered cellular behavior that may influence experimental findings.
Osteoarthritic tissue may demonstrate increased cellular migration and matrix remodeling responses compared with healthy tissue,17,47 and donor pathology may introduce substantial variability in tissue quality and biological behavior. 19 These factors should therefore be considered when interpreting results from human explant studies (Table 3).
Key Biological and Methodological Variables Influencing Outcomes in Meniscus Explant Studies
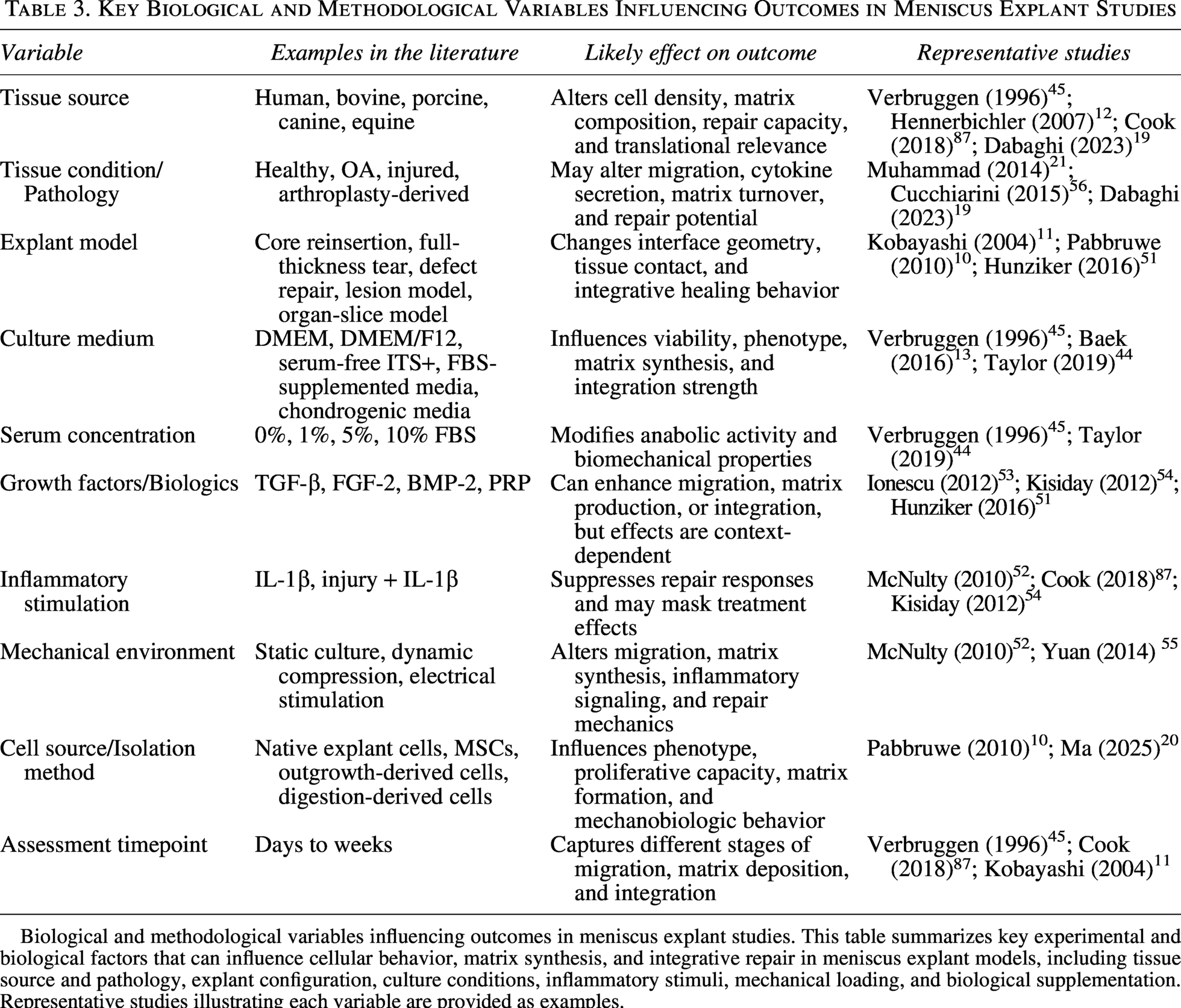
Biological and methodological variables influencing outcomes in meniscus explant studies. This table summarizes key experimental and biological factors that can influence cellular behavior, matrix synthesis, and integrative repair in meniscus explant models, including tissue source and pathology, explant configuration, culture conditions, inflammatory stimuli, mechanical loading, and biological supplementation. Representative studies illustrating each variable are provided as examples.
A 2014 study by Muhammad and colleagues identified a migratory progenitor cell population in human menisci. 21 These cells demonstrated proliferative capacity and responded to transforming growth factor beta signaling. Their discovery supports the hypothesis that endogenous progenitor cells may be mobilized under injury conditions and potentially harnessed for therapeutic purposes.
In animal models, similar cell populations have been identified within meniscal defects. One study in a canine model observed alpha-SMA-positive cells within experimentally created meniscal lesions. 77 These cells participated in matrix deposition and contributed to a seamless repair tissue that integrated with the native meniscus. Such findings reinforce the concept that resident meniscus cells can respond to injury with proliferative and migratory behavior under the appropriate stimuli.
The initial step in repairing an avascular meniscus defect is cellular infiltration into the lesion.46,78,79 Explant models have facilitated the visualization of this process. Incisions in the inner zone result in observable cell migration from adjacent tissue. The presence of chemotactic factors can enhance this migration.78,80 In one study, the application of connective tissue growth factor in a fibrin matrix significantly increased synovial MSC migration into meniscal explants, demonstrating the influence of biochemical gradients on cellular behavior. 48
Matrix remodeling plays a complementary role in facilitating migration. Enzymatic treatment of the defect border with collagenase has been shown to degrade the extracellular matrix, reducing barriers to cell movement and promoting integration. 81 Such manipulation underscores the role of matrix architecture in regulating cellular access to injury sites.
Following migration, cells must engage in matrix synthesis to form a reparative tissue.10,30,46 Early repair is typically characterized by fibrous matrix deposition, predominantly collagen type I. Over time, with appropriate stimuli, this tissue may undergo remodeling toward a more fibrocartilaginous phenotype, incorporating collagen type II and proteoglycans.28,60,72,82 One explant study demonstrated that sequential application of connective tissue growth factor (CTGF) followed by TGF-β3 promoted this transition, resulting in repair tissue that resembled native inner meniscus. 83
Mechanical loading exerts additional effects on repair dynamics. Dynamic compression has been shown to counteract catabolic cytokine activity and improve integration strength in meniscal explants.52,61 Electrical stimulation represents another modality with potential benefit. A 2014 study reported that pulsed electrical fields enhanced meniscus cell migration and improved integration strength, attributed in part to upregulation of the adenosine A2B receptor. 55 These findings suggest that bioelectrical cues can modulate cellular behavior and contribute to improved healing.
Biochemical agents such as platelet-derived growth factor and PRP have also been applied to explant systems.7,53,78 These biological factors stimulate cellular proliferation, migration, and matrix synthesis. Their application has led to increased cell infiltration and improved repair quality, underscoring their potential as therapeutic adjuncts. Human explant studies confirm the responsiveness of meniscus cells to such factors, albeit with differences in magnitude and timing compared with animal models.7,53,54
Historical Perspective of Explant Culture Systems
Foundational studies have laid the groundwork for current investigations. Early research in the 1990s demonstrated the potential for meniscal tissue to undergo integrative repair.8,38,45,79 In canine models, defects created within the meniscus healed with tissue that was histologically and biomechanically similar to the native structure.77,84,85 Alpha-SMA-positive cells were implicated in this process, indicating a contractile repair phenotype that contributed to seamless bridging of the defect. Simultaneous investigations into fibrin clot implantation showed that the introduction of a biologically active scaffold could enable healing in avascular meniscal regions.8,38,84
Subsequent developments in the early 2000s introduced quantitative assays for assessing integration in explant models. 49 Techniques such as push-out and tensile strength testing (Fig 3) allowed for measurement of repair strength following various interventions.12,49 These approaches revealed that enzymatic pretreatment of defect margins improved bonding between meniscal segments by facilitating matrix remodeling. Growth factors such as TGF-β and fibronectin further augmented repair strength, providing mechanistic insight into the requirements for effective integration.56,70,76,85
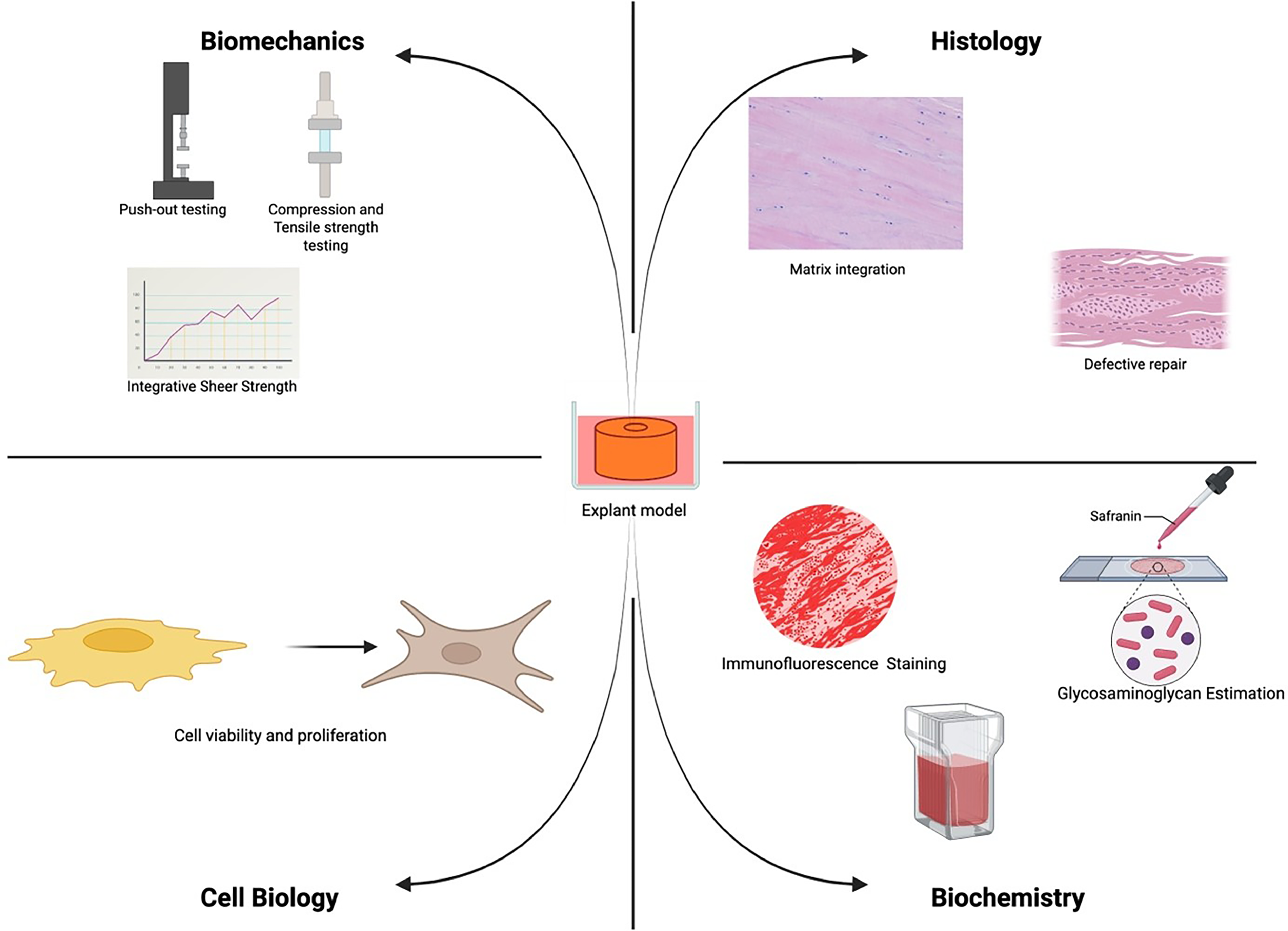
Integrative repair outcome assessment in explant studies.
Attention turned toward intrinsic cell populations in the 2010s. Investigators isolated meniscus-derived cells exhibiting progenitor-like behavior, capable of multilineage differentiation and proliferation. Muhammad et al. identified a population of migratory progenitor cells in human explants, responsive to TGF-β signaling and capable of participating in matrix synthesis. This finding emphasized the reparative capacity of native meniscus cells and encouraged exploration of strategies to mobilize or expand these populations. 21
Parallel advances in explant modeling refined the experimental platform. MSCs, including synovial-derived MSCs, have been investigated in both explant models and in vivo animal models for their potential to enhance meniscus repair, particularly within the avascular region where intrinsic healing is limited. 41
Control groups are essential for interpreting results. Untreated defects generally fail to heal in explant culture, reflecting the in vivo limitations of the avascular meniscus.11,12,49 Positive controls, such as TGF-β treatment, establish benchmarks for maximal expected response. However, disparities in factor concentrations, exposure durations, and tissue sources complicate cross-study comparisons.49,86 The absence of standardized protocols remains a barrier to reproducibility and collective data synthesis.
Limitations of Explant Culture Models
Limitations inherent to explant models must be acknowledged. Nutrient diffusion is restricted in the absence of vascular perfusion, leading to cell death in the core of larger samples over time.44,45,48 Most studies are limited to durations of 4–8 weeks, beyond which tissue viability declines. The immune response, a critical component of in vivo healing, is absent unless simulated by cytokine supplementation.58,87,88 Differences between animal and human tissue further complicate the extrapolation of results. Juvenile bovine or porcine menisci exhibit greater cellularity and matrix plasticity compared with adult human specimens, potentially leading to overestimation of treatment efficacy. 89
Methodological biases may influence the interpretation of progenitor cell studies. Publication bias favors positive results, and outgrowth assays preferentially analyze motile subpopulations that may not represent the broader meniscal cell population.69,74 Variability in characterization techniques, including immunostaining and gene expression analysis, can produce inconsistent definitions of progenitor status. 17 These factors necessitate critical appraisal of experimental design and cautious generalization of findings.
Animal models complement explant studies by incorporating physiological variables. In vivo models in rabbits, pigs, and dogs have been employed to test surgical techniques, cellular therapies, and biomaterial scaffolds. These systems permit longitudinal assessment of tissue integration and joint health. However, anatomical and vascular differences limit direct translation. For example, vascular penetration into the meniscus may differ among species, affecting the baseline healing capacity.90–94 Nonetheless, animal explant models have provided valuable platforms for mechanistic and proof-of-concept studies.
Human tissue explants, derived from surgical discards or cadaveric sources, offer direct insight into the regenerative potential of clinically relevant specimens. 48 Studies have demonstrated that damaged human menisci can yield migratory cells with reparative capacity.17,21,69 Such findings support the potential for autologous cell-based therapies and underscore the importance of evaluating treatments in human-derived systems.40,41,78 Variability in donor age, health status, and tissue quality presents challenges but also reflects real-world conditions. 95
A comparative analysis between animal and human data reveals both alignment and divergence. Certain factors, such as PRP, show efficacy in explant culture but produce inconsistent results in clinical application. Discrepancies may result from differences in delivery method, local retention, or patient-specific variables. 96 Conversely, success in animal models has informed clinical trials of meniscal implants, biologics, and cell therapies, indicating the translational potential of well-designed preclinical research.90,91,93
Future Directions
Future directions in avascular meniscus repair emphasize the integration of biomaterials, cell biology, and mechanical stimulation.68,97 Scaffold systems designed to sequentially release chemotactic and chondrogenic factors seek to replicate successful treatment regimens observed in explant studies. Hydrogels and nanofibers are being developed to enhance cell retention and control degradation kinetics.97–99 Bioadhesive formulations capable of bridging meniscal defects while delivering bioactive cues represent a promising therapeutic modality. 8
Cell-based therapies aim to leverage the differentiation potential of MSCs or the reparative capacity of endogenous meniscal cells. Isolation and expansion of migratory progenitor populations could facilitate autologous implantation or in situ activation. Gene therapy and small-molecule delivery are being explored to stimulate regenerative pathways directly within the joint. 100
These approaches seek to enhance repair without extensive surgical intervention, aligning with minimally invasive treatment paradigms.6,7
Mechanobiological inputs are gaining traction as modulators of repair.71,101 Bioreactor systems simulate loading conditions to precondition constructs prior to implantation. Postoperative rehabilitation protocols incorporating controlled loading may enhance integration (Fig 4). Electrical stimulation devices need to be investigated for their ability to modulate cellular activity and promote tissue bonding, informed by findings from explant studies. 102
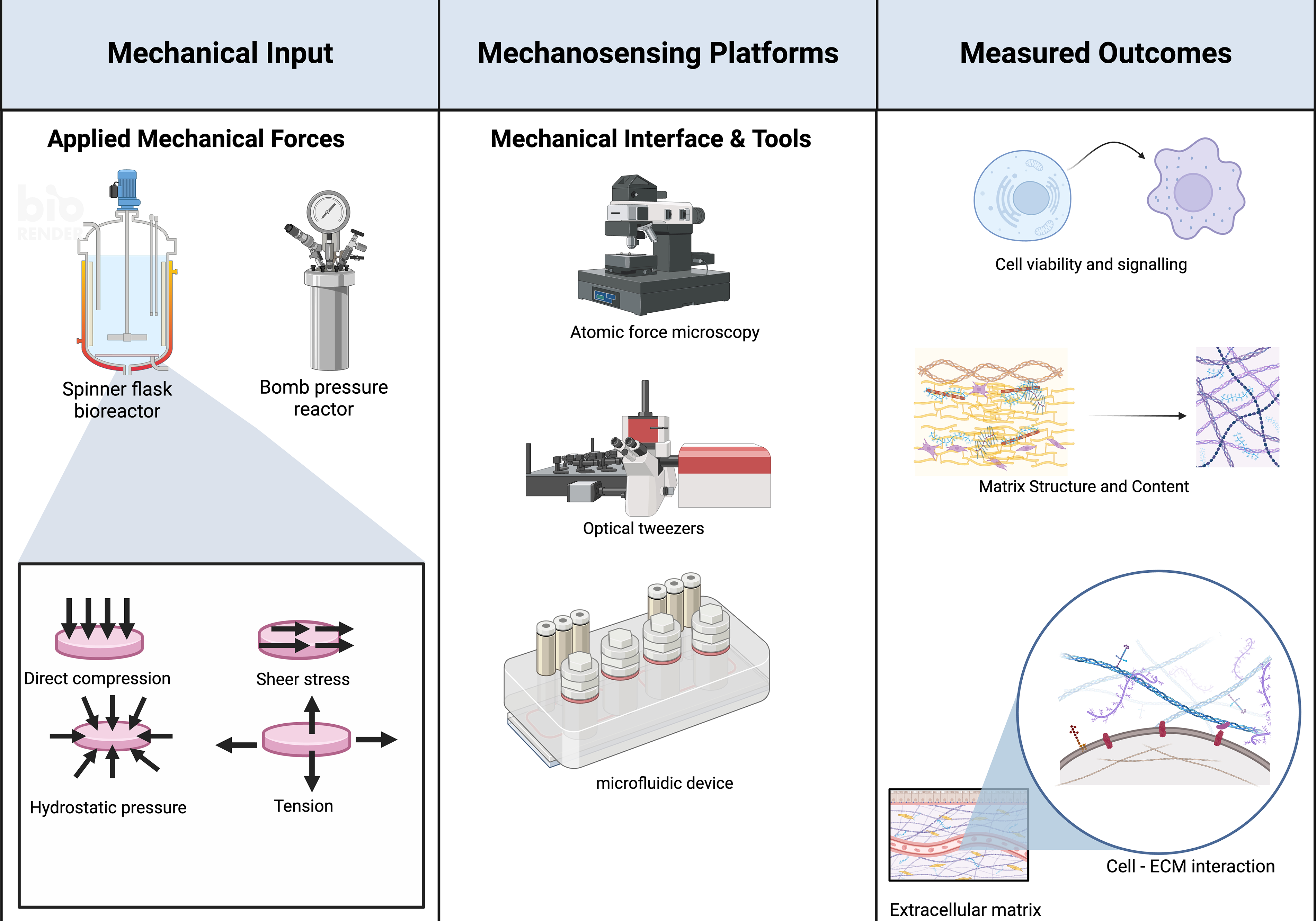
Mechanobiology in explant cultures.
Translation to clinical practice requires rigorous safety and efficacy evaluation. 103 Effective dosing, delivery vehicles, and long-term durability of repair must be established. Minimally invasive techniques for administering cells or factors are being developed, including the injection of gels or microspheres. 104 Longitudinal studies assessing joint preservation and functional outcomes will be essential to determine the value of these emerging therapies.
Key questions remain regarding the identity and regulation of reparative meniscus cells.17,21,22,74 Determining the molecular signature and lineage potential of migratory meniscus populations may guide therapeutic targeting. Improving in vitro models to incorporate vascular and immune components could enhance predictive validity. The integration of explant research with clinical and systems biology approaches will support the development of therapies that address the unique challenges of avascular meniscal repair.
Conclusion
Explant culture systems provide a controlled setting for studying avascular meniscal injury while preserving native matrix architecture. Within these models, investigators create defined inner-zone defects and measure integrative repair with mechanical testing and histology. The same platforms allow direct observation of endogenous migratory meniscal cells at the interface, as well as evaluation of the biochemical cue sequence that recruits cells and supports fibrocartilaginous matrix formation. Biomaterial carriers, including injectable hydrogels, bioadhesives, and microspheres, have been examined for their ability to retain cells and factors at the defect. Mechanobiologic inputs have also been tested, with physiologic loading used to influence catabolic activity and interface bonding.
Findings across these studies indicate that strategies, which lower matrix barriers at defect margins, apply appropriate growth factor programs, and use delivery formats that support retention can improve integration in the avascular zone. Loading protocols tailored to physiologic ranges further enhance bonding and matrix quality. Barriers to translational research exist because current explant platforms have diffusion limitations and lack vascular or immune inputs, while protocol variability and species- or age-related differences complicate direct translation. Future work should emphasize perfused, immune-competent human tissue systems, validated and comparable integration assays, durability testing under multiaxial loading, and stratification by patient or tear characteristics. Such refinements can align preclinical outcomes with clinical endpoints and support phased trials that will finally give a meaningful real-world solution to the problem of avascular meniscus injuries.
Authors’ Contributions
O.E.: Conceptualization, methodology, formal analysis, investigation, writing—original draft, writing—review and editing. A.B.A.: Conceptualization, writing—review and editing, supervision.
Footnotes
Acknowledgments
The authors acknowledge the staff in the Geoffrey & Robyn Sperber Health Sciences Library, University of Alberta for helping to design the search strategy.
Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
This work was supported by the Wu Tsai Human Performance Alliance Agility Project Award to A.B.A.