
Abstract
Anaplastic thyroid carcinoma (ATC) is a highly aggressive and treatment-resistant form of thyroid cancer, characterized by poor prognosis, rapid metastasis, and resistance to conventional therapies. Current treatment options, including surgery, chemotherapy, and radiation, are often ineffective in controlling the disease, underscoring the urgent need for novel therapeutic approaches. Nanotechnology has emerged as a promising strategy to overcome these challenges, offering innovative solutions for targeted drug delivery and noninvasive therapeutic modalities. This review explores the latest advancements in nanotechnology-driven strategies for treating ATC, with a particular focus on noninvasive therapies such as sonodynamic therapy and nano-pulse stimulation, as well as the development of nanomaterial-based drug delivery systems. These systems, including RNA-based nanocarriers, radionuclide-labeled nanoparticles, and nanoclay-based delivery systems, provide enhanced specificity and efficacy, overcoming the limitations of traditional treatments. Additionally, dual-modality theranostic systems, which combine diagnostic imaging and therapeutic payloads, hold great promise in improving early detection and real-time treatment monitoring. Despite the promising preclinical results, challenges such as tumor heterogeneity, drug resistance, and biocompatibility of nanomaterials remain in the clinical use. This review provides a comprehensive overview of the potential of nanotechnology to revolutionize the treatment of ATC, offering new hope for patients with this highly aggressive malignancy.
Impact Statement
The innovative use of nanotechnology in the treatment of anaplastic thyroid carcinoma (ATC) represents a transformative shift in cancer therapy, offering targeted, noninvasive, and highly effective alternatives to traditional treatment methods. By leveraging cutting-edge nanomaterials for precise drug delivery and integrating them with noninvasive therapeutic strategies such as sonodynamic therapy and nano-pulse stimulation, this review highlights the potential for significantly improving patient outcomes in ATC. The development of dual-modality theranostic systems that combine diagnosis and treatment within a single platform offers unparalleled opportunities for real-time monitoring and personalized treatment, addressing the critical challenge of early metastasis and therapeutic resistance in ATC. These advancements not only pave the way for more effective treatment options for ATC but also contribute to the broader field of cancer nanomedicine, setting the stage for more targeted and individualized therapies across various malignancies.
Keywords
Introduction
Thyroid cancer, a type of malignancy originating in the thyroid gland, ranks as one of the most common endocrine cancers.1,2 Thyroid cancer encompasses a heterogeneous group of malignancies with varied clinical behavior. 3 It is categorized into several subtypes based on histopathological characteristics, including papillary thyroid carcinoma (PTC), follicular thyroid carcinoma (FTC), medullary thyroid carcinoma (MTC), and anaplastic thyroid carcinoma (ATC). 4 Among these subtypes, ATC is considered the most aggressive and lethal, representing a significant challenge for both diagnosis and treatment.5,6 This carcinoma is characterized by an extremely poor prognosis, primarily due to its rapid growth, early metastasis, and resistance to most conventional therapies.7,8 Unlike PTC and FTC, which generally have favorable outcomes and respond well to treatments like surgery and radioactive iodine, ATC patients experience a much more dismal clinical course. 9
One of the key factors contributing to the poor prognosis of ATC is its highly aggressive biological behavior. 10 ATC cells often exhibit extensive genetic mutations and aberrant molecular signaling pathways, which make them particularly resistant to standard treatments such as chemotherapy, radiation therapy, and even targeted therapies that may be effective for other types of thyroid cancers. 11 Moreover, ATC frequently metastasizes early, often spreading to distant organs such as the lungs, liver, and bones, complicating the management and treatment options for these patients. 12 Surgical resection, the most common treatment for solid tumors, is often ineffective in ATC due to the rapid invasiveness of the tumor, making complete excision challenging. 13 Another major clinical challenge is that ATC lacks specific molecular targets that can be effectively targeted with precision medicine, a hallmark of modern oncology. 14 ATC is characterized by an exceptionally aggressive clinical course, which is underpinned by complex molecular and genetic alterations. Among the most frequently observed mutations are BRAF V600E, TP53, and TERT promoter mutations, which collectively drive rapid proliferation, resistance to apoptosis, genomic instability, and poor responsiveness to conventional therapies. Dysregulation of key signaling pathways, including MAPK, PI3K/AKT, and p53-mediated networks, further contributes to tumor aggressiveness and therapy resistance. These molecular features not only define the malignant phenotype of ATC but also provide a rationale for developing targeted therapeutic strategies. 15 Targeted therapies have been developed for specific molecular subtypes, notably BRAF V600E-mutated ATC, for which combination treatment with dabrafenib (BRAF inhibitor) and trametinib (MEK inhibitor) has demonstrated improved response rates in clinical studies.
In the past decade, significant strides have been made in the development of advanced treatment strategies, particularly with the integration of nanotechnology into cancer therapy.16,17 Nanotechnology has revolutionized the potential to enhance drug delivery systems by offering solutions that improve the specificity and efficacy of drugs. 18 Nanomaterials, which are engineered at the nanoscale, possess unique properties such as high surface area, the ability to be functionalized with targeting ligands, and the capacity for controlled drug release.19,20 These attributes allow for more targeted delivery of therapeutic agents directly to tumor cells, potentially bypassing the limitations of traditional therapies and minimizing side effects.21,22 In particular, nanotechnology has shown great promise in overcoming some of the major obstacles in ATC treatment. 23 Traditional chemotherapies often suffer from nonspecific drug distribution, leading to systemic toxicity and damage to healthy tissues. Nanomaterial-based systems, however, can be designed to target specific receptors or antigens that are overexpressed on the surface of ATC cells, such as epidermal growth factor receptor (EGFR), allowing for more precise drug delivery. 24 Additionally, the use of nanomaterials in combination with other therapeutic modalities, such as radiation therapy and immunotherapy, has the potential to create synergistic effects that enhance the overall therapeutic efficacy. 25 While several recent reviews have explored nanomedicine applications in thyroid cancers broadly, ATC remains underrepresented due to its rarity, aggressive progression, and therapy resistance. By focusing on these cutting-edge nanotechnology-based strategies, this review aims to provide a comprehensive overview of the potential for improving treatment outcomes in ATC by noninvasive approaches and targeted drug delivery (Fig. 1). This review was conducted as a structured narrative review of nanotechnology-driven noninvasive and targeted therapeutic strategies for ATC. We prioritized original studies directly related to ATC, nanotechnology-based delivery systems, or noninvasive therapeutic approaches with clear translational relevance, with emphasis on study design, therapeutic mechanism, model system, and translational significance. Our goal is to highlight how these novel systems can overcome the limitations of traditional therapies, offering new hope for patients with this highly aggressive form of thyroid cancer (Table 1).
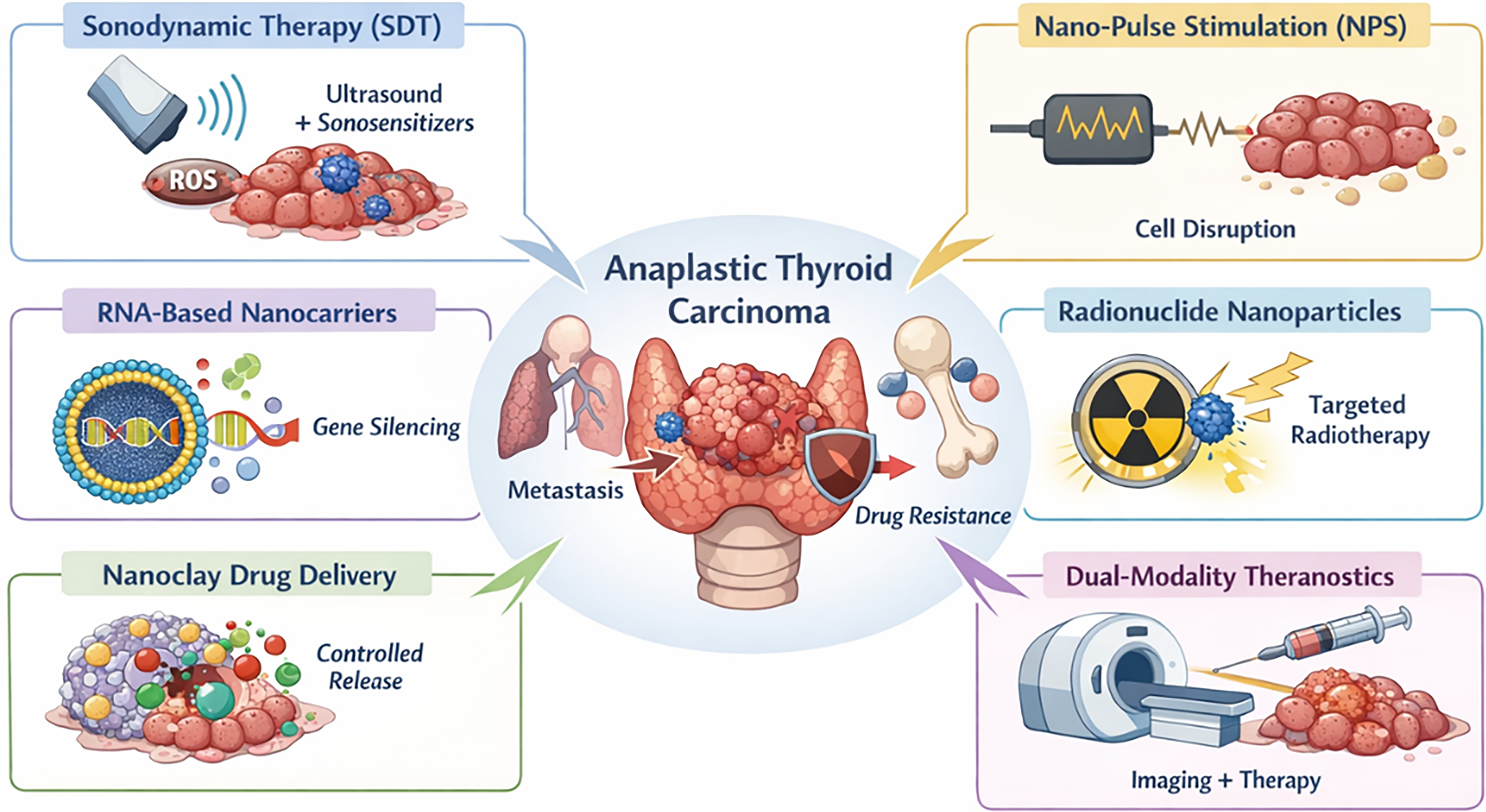
Nanotechnology-driven therapeutic strategies for anaplastic thyroid carcinoma: noninvasive approaches and targeted drug delivery.
Nanotechnology-Driven Therapeutic Strategies for Anaplastic Thyroid Carcinoma
ATC, anaplastic thyroid carcinoma; EGFR, epidermal growth factor receptor; hERG, human ether-à-go-go-related gene; NPs, nanoparticles; NPS, nano-pulse stimulation; ROS, reactive oxygen species; SDT, sonodynamic therapy; siRNA, small interfering RNA; shRNA, short hairpin RNA; VEGFR, vascular epidermal growth factor receptor.
Noninvasive Physics-Based Therapeutic Approaches: Sonodynamic Therapy and Nano-Pulse Stimulation
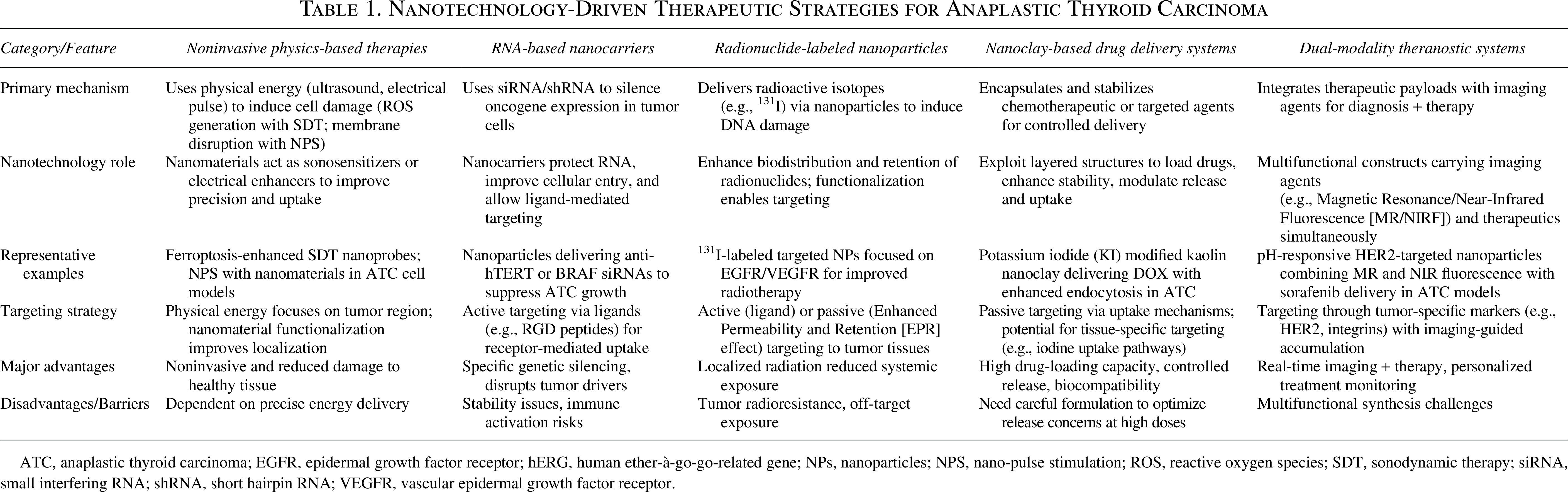
The rapid advancements in nanotechnology and biomedical engineering have led to the emergence of various noninvasive therapeutic modalities that utilize physical stimuli for cancer treatment. 26 Two such techniques, sonodynamic therapy (SDT) and nano-pulse stimulation (NPS), are gaining significant attention due to their unique mechanisms of action and promising preclinical and clinical results (Fig. 2). These therapies leverage the power of physical energy, such as ultrasound or electrical pulses, to activate therapeutic agents or induce direct cellular damage. 27 When combined with nanomaterials, these therapies can significantly enhance the precision and effectiveness of cancer treatments, including for difficult-to-treat cancers like ATC. 28 SDT is a relatively novel approach that combines ultrasound with sonosensitizing agents to selectively destroy tumor cells. 29 This therapy uses ultrasound waves to activate a sonosensitizer, a type of drug or molecule that becomes toxic only when exposed to ultrasound. 30 Upon exposure to ultrasound, sonosensitizers absorb acoustic energy and transition to an excited state. In this state, they interact with molecular oxygen to generate reactive oxygen species (ROS), which induce oxidative stress and damage tumor cells. 31 SDT has several advantages, including its noninvasive nature, precise targeting, and minimal side effects on surrounding healthy tissue, making it a promising option for ATC and other malignancies.
Noninvasive physics-based therapeutic approaches: Sonodynamic therapy and nano-pulse stimulation.
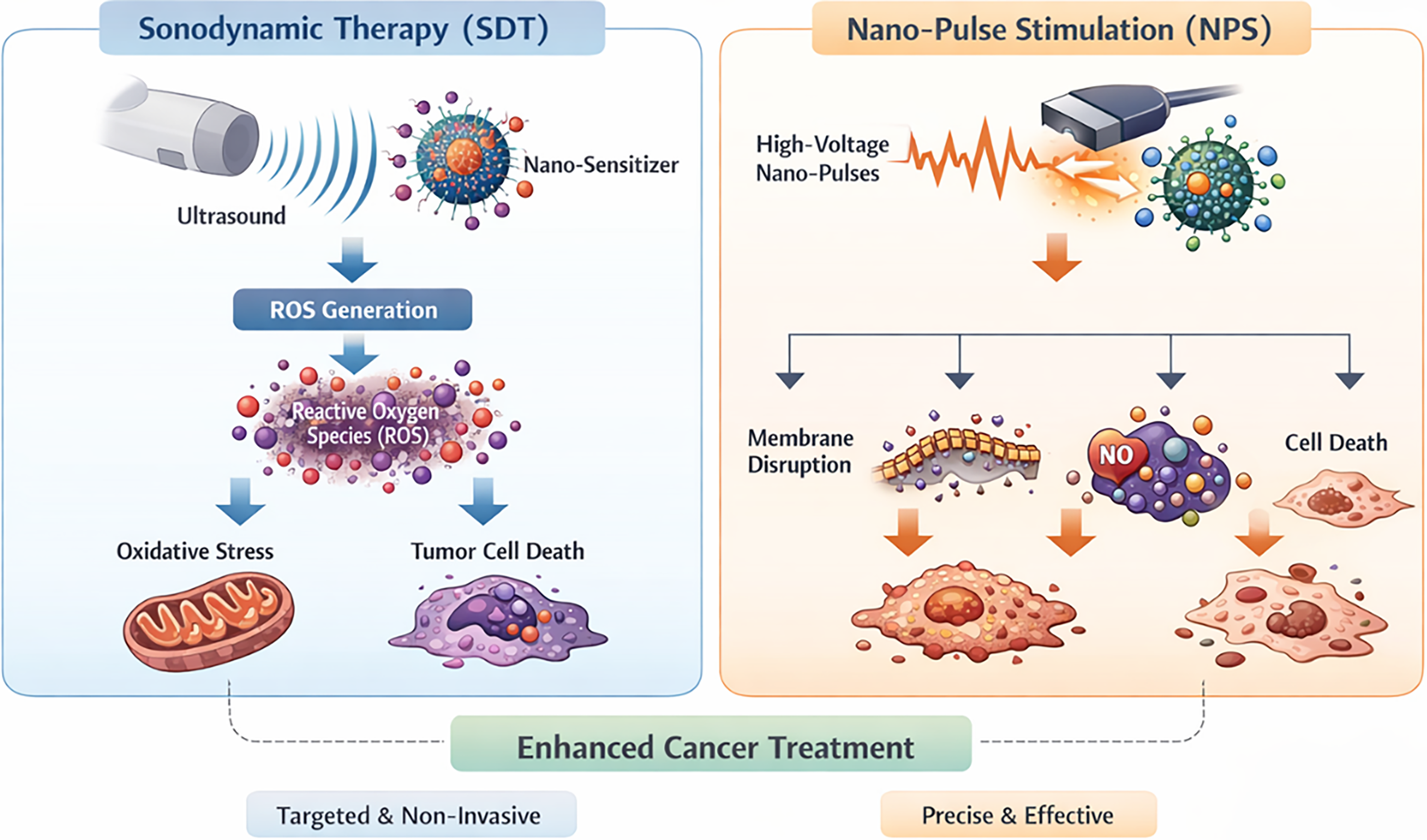
One of the emerging combinations in SDT for treating ATC is the synergy between ferroptosis and SDT. 32 Ferroptosis is an iron-dependent, nonapoptotic form of cell death characterized by the accumulation of lipid peroxides. 33 Recent studies have shown that inducing ferroptosis in cancer cells can be an effective method for combating tumor growth. 34 However, the challenge lies in the insufficient accumulation and poor penetration of ferroptosis inducers in deep tumor tissues, which significantly limits their therapeutic effects. To overcome this limitation, a cascade-penetrating metal–polyphenol ultrasonic molecular probe called Fe3+Cur-PFP@IR780-LIP (FCIPL) was developed (Fig. 3). 35 The FCIPL nanoparticles (NPs) enhance ferroptosis induction when combined with SDT. Microbubbles were coadministered to facilitate acoustic droplet vaporization (ADV) and ultrasound-targeted microbubble destruction (UTMD). In the cascade-penetrating FCIPL SDT-ferroptosis system, SDT was driven by low-frequency ultrasound (∼0.5–3 MHz) at intensities below ∼3 W/cm2, facilitating ADV and UTMD cavitation effects that enhance deep NP penetration and tumor uptake, as described in comparable SDT systems.
The cascade-penetrating metal–polyphenol ultrasound molecular probe FCIPL.
NPS is another advanced noninvasive therapy that utilizes ultrashort electrical pulses to selectively target tumor cells. 36 NPS has been shown to disrupt cell membranes, inducing apoptosis, necrosis, and electroporation. 37 When combined with nanomaterials, NPS can enhance the delivery of therapeutic agents or enhance cell membrane permeability, facilitating drug uptake. 38 These nanosecond pulses transiently permeabilize the plasma membrane and intracellular organelle membranes, inducing nanoporation. This disruption alters ionic gradients and triggers intracellular signaling cascades, including calcium influx and activation of apoptotic pathways. Recent studies have demonstrated the in vitro antitumor effects of NPS on human ATC cells. One such study treated the 8305C ATC cell line with NPS and assessed its effects using Cell Counting Kit-8 (CCK-8) assays, clonogenic assays, and apoptosis assays. 39 The study found that NPS significantly (p < 0.05) inhibited ATC cell proliferation. In vitro NPS treatment of 8305C ATC cells applied electric pulses at a field strength of ∼30 kV/cm with ∼60 pulses, resulting in a reduction in survival rate to ∼42% at 24 h and significant apoptosis alongside increased inducible nitric oxide synthase (iNOS) activity. The effect was field strength dependent, with higher pulse amplitudes producing greater apoptosis. This indicates that NPS can effectively halt the growth of ATC cells by inducing programmed cell death, even at lower power densities. Further analysis revealed a critical increase in nitric oxide synthase (NOS) activity in cells treated with NPS. Nitric oxide (NO) is a potent signaling molecule that regulates various physiological processes, including cell proliferation and apoptosis. The study showed that NPS treatment led to the activation of iNOS, a key enzyme involved in NO production. This iNOS-dependent mechanism is crucial for the antitumor effect of NPS, as the increase in NO levels induces oxidative stress within the tumor cells, contributing to their destruction.
RNA-Based Nanocarriers for Gene Silencing
Gene therapy, particularly RNA interference (RNAi) technology, has emerged as a promising approach in the treatment of various cancers, including ATC. 40 RNAi involves the introduction of small RNA molecules, such as small interfering RNA (siRNA) or microRNA (miRNA), that specifically silence the expression of target genes. 41 This strategy offers a novel and highly specific mechanism for addressing the molecular drivers of cancer progression. 42 Unlike traditional therapies, which primarily focus on inhibiting protein function, RNA-based therapies directly modulate gene expression, enabling a more precise approach to cancer treatment. 43 One of the key advantages of RNA-based therapies is their ability to target specific genetic alterations driving cancer. In ATC, numerous mutations in critical oncogenes, such as EGFR, p53, and BRAF, provide ideal targets for RNA intervention. By silencing these mutant or overexpressed genes, RNA therapies can disrupt critical signaling pathways involved in tumor cell proliferation, survival, and metastasis, leading to significant therapeutic benefits. However, RNA molecules are inherently unstable and cannot easily cross cellular membranes, posing a challenge for their effective delivery to tumor cells. This is where the integration of nanotechnology plays a pivotal role, enhancing both the stability and delivery efficiency of RNA-based therapies.
RNA-based nanocarriers are designed to encapsulate RNA molecules, such as siRNA or short hairpin RNA, within NPs, which protect the RNA from degradation and facilitate its efficient delivery into tumor cells. These nanocarriers are often functionalized with ligands or antibodies that specifically bind to overexpressed receptors on cancer cells, enabling precise and targeted delivery to tumor sites. NP size and zeta potential were usually determined by dynamic light scattering. 44 In the case of ATC, common targets include EGFR, which is frequently overexpressed on the surface of ATC cells, as well as other tumor-associated antigens. 45 Once the nanocarriers enter the tumor cells, the RNA molecules are released in response to specific stimuli, such as changes in pH, enzyme activity, or temperature, which are common characteristics of the tumor microenvironment (TME). 46 Upon release, the RNA molecules interact with the RNA-induced silencing complex, leading to the degradation of target messenger RNA and silencing the expression of oncogenes responsible for tumor progression. A theranostic near-infrared polymeric NP system demonstrated systemic delivery of siRNA targeting the BRAF oncogene, resulting in effective gene knockdown and suppression of tumor growth and metastasis in orthotopic ATC models. 47
To improve the delivery efficiency of RNA molecules in ATC, dendritic nanocarriers, such as polyamidoamine-polyethylene glycol-cyclic RGD (PAMAM-PEG-cRGD) NPs, have been developed. 48 These nanocarriers can encapsulate siRNA molecules targeting specific genes, such as hERG (human ether-à-go-go-related gene), which plays a crucial role in cancer cell proliferation and metastasis. The overexpression of hERG has been associated with aggressive cancer types, including ATC, making it a critical target for RNA-based therapies. The PAMAM-PEG-cRGD nanocarriers are designed with cyclic RGD peptides that specifically target integrins, which are commonly overexpressed in tumor cells. This enhances the specificity and efficiency of the nanocarriers, allowing them to selectively deliver siRNA to ATC cells. Besides, Chen et al. 49 developed nanosystems, platelet-derived growth factor receptor (PDGFR-β) targeted-polypeptide-modified poly (β-amino ester) (pBAE) (T-pBAE)/siB7-H3 NPs, targeting PDGFR-β+ cancer-associated fibroblasts (CAFs) and featuring B7-H3 knockdown. T-pBAE/siB7-H3 NPs were efficiently internalized by CAFs, achieving targeted knockdown of B7-H3 expression. Silencing B7-H3 significantly suppressed the expression of cell division cycle 27 and other cell cycle-related genes, thereby inhibiting CAFs’ proliferation. This study demonstrates that PDGFR-β polypeptide-modified pBAE could successfully deliver B7-H3 siRNA to CAFs. After knockdown of B7-H3 within CAFs, ATC proliferation, invasion, and migration were inhibited.
In addition to gene silencing, RNA-based nanocarriers can also be integrated with detection systems to enable in situ tracing and highly sensitive biomarker analysis, particularly in the context of thyroid cancer. A novel example of this integration is the use of spatial confinement nano-assembly in DNA detection. Traditional molecular assays that rely on DNA assembly often face challenges with random collisions between freely diffusing probes, leading to inefficiencies in the assembly process and background leakage that reduces the specificity of the assay. To overcome these issues, a new approach known as the extended linear confined zipper hybridization chain reaction (ZHCR) was developed, in which the DNA assembly relies on two extended linear confined probes (Fig. 4). 50 The ZHCR system is particularly effective in providing precise in situ target information by enabling stable DNA assembly within live cells. This system was employed to analyze two thyroid cancer-specific miRNAs, allowing for in situ tracing and serum content detection of these biomarkers.
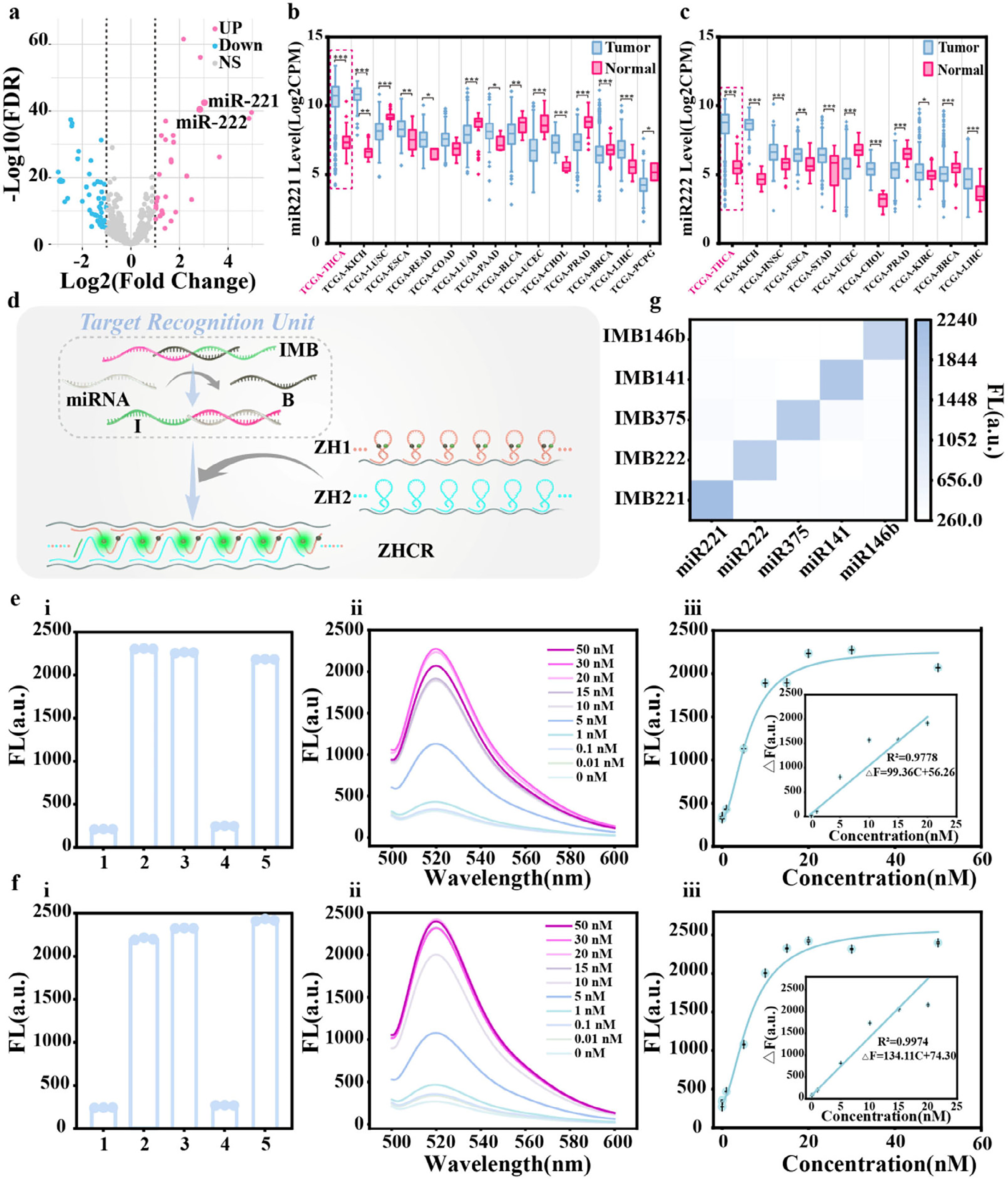
ZHCR response to microRNAs (miRNAs).
Radionuclide-Labeled NPs for Targeted Therapy
Radionuclide therapy is a form of targeted radiation treatment that utilizes radioactive isotopes to selectively deliver radiation to tumor cells. 51 This approach has become a promising avenue in cancer treatment due to its ability to target specific cancer cells while minimizing the exposure of surrounding healthy tissue. 52 In particular, radionuclide-labeled NPs have gained significant attention for their potential in delivering both therapeutic agents and radioactive isotopes directly to tumor sites, enhancing the effectiveness of radiation therapy. 53 In the context of thyroid cancer, particularly ATC, radionuclide therapy has long been a treatment modality, with iodine-131 (I-131) being the most widely used isotope. 54 However, ATC’s resistance to radioiodine therapy due to a lack of functional sodium–iodine symporter (NIS) expression and the rapid mutation of key oncogenes complicates the use of traditional radioiodine therapy. The advent of radionuclide-labeled NPs, which can be engineered to target specific molecular markers or tumor-associated antigens, has overcome this challenge by providing a more targeted and effective delivery mechanism for radiation. 55 NPs are highly promising carriers for radionuclides, as they can be engineered to specifically target tumor cells, delivering radiation directly to the tumor site. 56 Radionuclide-labeled NPs offer dual capabilities for imaging and therapy, serving as theranostic agents in aggressive thyroid cancers such as ATC. These multifunctional NPs can be labeled with radioisotopes for targeted radiotherapy while simultaneously providing imaging signals through Single-Photon Emission Computed Tomography (SPECT), Positron Emission Tomography (PET), or optical modalities. The theranostic approach allows real-time monitoring of NP biodistribution, tumor accumulation, and retention, enabling optimization of dosing and scheduling. Compared with conventional radioiodine therapy, theranostic NPs enhance specificity, reduce off-target toxicity, and provide quantitative readouts of treatment efficacy, which is particularly valuable given ATC’s heterogeneity, rapid growth, and early metastatic spread. Integrating imaging with therapy in a single platform thus facilitates personalized treatment strategies and supports mechanistic evaluation of NP-mediated targeting in preclinical and potentially clinical settings. 57 These NPs can be functionalized with ligands that bind to overexpressed receptors on the surface of ATC cells, such as the EGFR, which is frequently upregulated in ATC. 58 This specific targeting capability significantly improves the accumulation of the radionuclide at the tumor site, while minimizing radiation exposure to healthy tissues, thereby reducing systemic toxicity. 59 However, EGFR expression is heterogeneous across ATC tumors, and reliance on a single receptor limits broad applicability. This highlights the need for multitarget or personalized targeting strategies that account for receptor heterogeneity when designing therapeutic platforms for ATC.
One notable example of this approach is the use of Anlotinib-nBSA-131I NPs (Fig. 5). 60 Anlotinib is a multitargeted kinase inhibitor that targets the vascular endothelial growth factor receptor, fibroblast growth factor receptor, PDGFR, and c-KIT, all of which are involved in the angiogenesis and growth of ATC cells. By encapsulating Anlotinib in an NP composed of bovine serum albumin (BSA) and labeling it with iodine-131, researchers have created a system that not only targets ATC cells but also delivers targeted radiation to the tumor site. The Anlotinib-nBSA-131I system demonstrated targeted uptake in EGFR-overexpressing ATC cell lines, with cellular radioiodine accumulation increasing. In vitro studies demonstrated that the NPs significantly increased the cellular uptake of iodine-131 in ATC cell lines, such as 8305C and C643, compared to free iodine-131. The C643 cell line, which has a high expression of EGFR, exhibited the highest cellular uptake of the Anlotinib-nBSA-131I NPs, which indicates that the NPs were effectively targeting EGFR overexpression in ATC cells. The mechanism of action of radionuclide-labeled NPs is based on the targeted delivery of radioactive isotopes, which emit ionizing radiation capable of inducing cellular damage. The radiation can cause DNA breaks, leading to apoptosis or cell cycle arrest in tumor cells. The specific targeting of EGFR and other molecular markers in ATC cells enhances the delivery of radiation directly to the tumor, which maximizes the therapeutic effect while minimizing off-target effects.
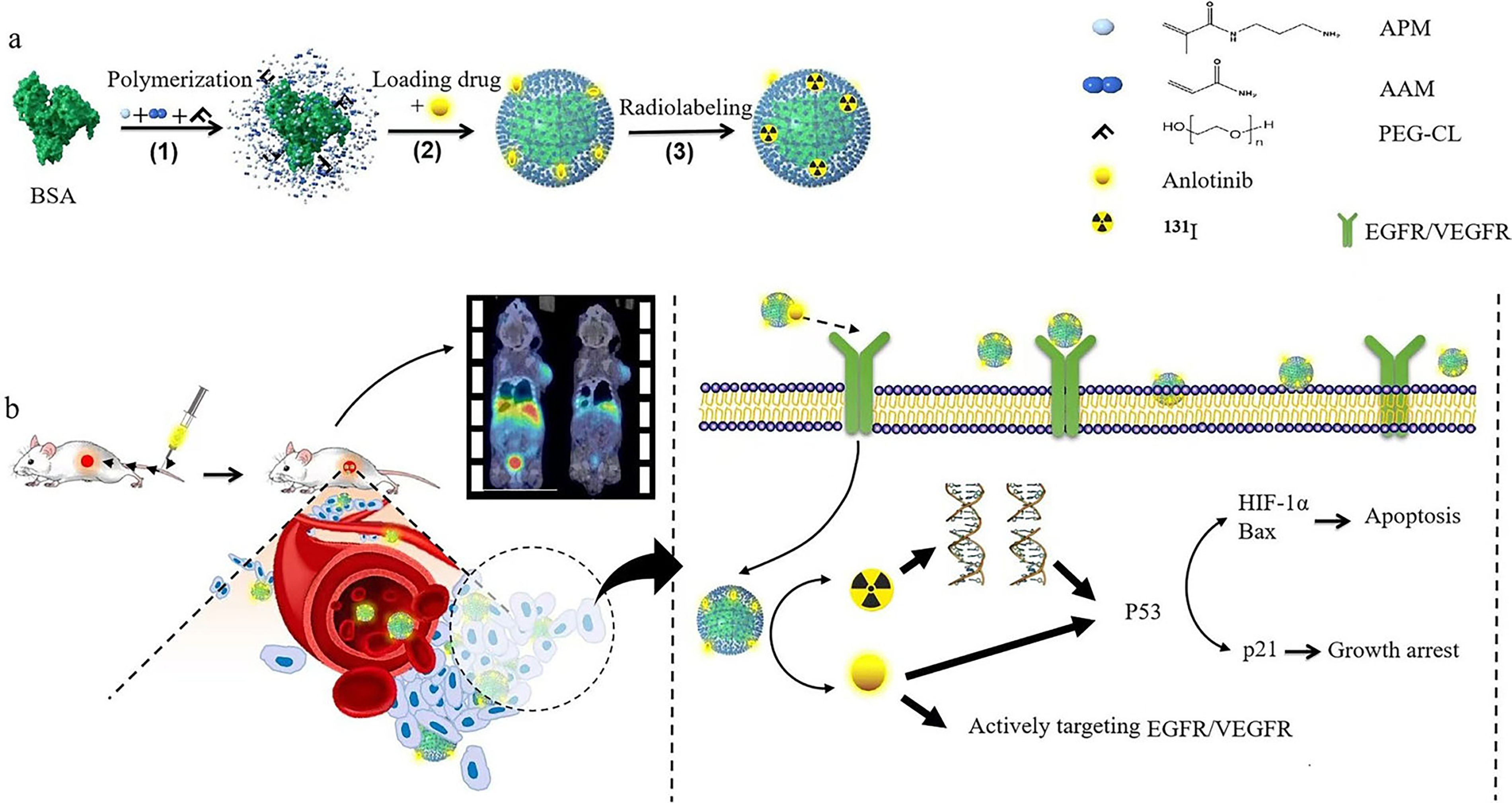
Radiolabeled 131I-anlotinib-nBSA nanoparticles.
Nanomaterials-Based Systems for Enhanced Drug Delivery
Nanotechnology provides diverse platforms for delivering therapeutic agents to ATC cells with enhanced specificity and efficacy. These systems can be categorized into four major classes: liposomes, which are phospholipid vesicles capable of encapsulating hydrophilic and hydrophobic drugs and can be functionalized with targeting ligands to enhance uptake while reducing systemic toxicity; polymeric NPs, composed of biodegradable polymers such as Poly(lactic-co-glycolic acid) (PLGA) or PEGylated dendrimers, which allow controlled drug release, protection from enzymatic degradation, and delivery of RNAi molecules to silence oncogenes like EGFR or hERG. Inorganic NPs, including metal and metal oxide-based NPs such as gold, iron oxide, and silica, which offer stability, tunable optical and magnetic properties, and theranostic capabilities for imaging and targeted therapy. Importantly, nanoclays, layered silicates with large surface area, and modifiable surfaces that can encapsulate chemotherapeutics, radionuclides, or RNA molecules, providing controlled release and tumor-targeting potential, with potassium iodide (KI)-modified nanoclays exploiting iodide uptake in thyroid tissue when combined with strategies that restore or enhance NIS function. Categorizing these platforms highlights their versatility, clarifies the rationale for selecting specific systems for ATC therapy, and emphasizes the unique advantages and limitations of each approach in preclinical and potential clinical applications.
Nanoclay-based drug delivery systems have gained significant attention in recent years due to their unique properties, including biocompatibility, biodegradability, and ease of functionalization. 61 Nanoclays are naturally occurring or synthetic layered materials that can be engineered to deliver drugs more effectively to specific sites, such as cancerous tumors. 62 These materials can encapsulate various therapeutic agents, such as chemotherapeutic drugs, nucleic acids, and proteins, and can be tailored to provide controlled and sustained drug release. Their surface properties allow for the incorporation of targeting ligands, which further enhances their ability to selectively deliver drugs to tumor cells, while minimizing systemic toxicity. In the context of ATC, nanoclay systems hold great promise for improving treatment outcomes. ATC is a highly aggressive cancer with limited effective treatment options, which often leads to poor prognosis and high mortality rates. Nanoclay-based drug delivery systems are particularly well-suited for addressing the challenges posed by ATC, as they can encapsulate a wide range of therapeutic agents and be functionalized to target specific tumor-associated biomarkers, such as EGFR and VEGF. Additionally, the ability to incorporate chemotherapy agents, RNA molecules, or radionuclides into nanoclay systems offers a versatile approach to treating ATC through combination therapies.
Nanoclay-based drug delivery systems work by exploiting the natural properties of clays to facilitate the encapsulation and controlled release of therapeutic agents. 63 The interlayer spaces between the layers of nanoclays provide a compartment for the loading of drugs, allowing for a more efficient drug release profile. This controlled release can be triggered by specific stimuli in the TME, such as changes in pH, temperature, or enzymatic activity. The nanoclays’ layered structure also enables the codelivery of multiple therapeutic agents, which can work synergistically to enhance therapeutic efficacy. One of the most significant advantages of nanoclay-based systems is their biodegradability. After delivering their payload to the target tumor site, the nanoclays degrade over time, reducing the risk of long-term toxicity and accumulation in the body. Moreover, their negative surface charge allows for easy functionalization with targeting ligands, such as antibodies, peptides, or small molecules, which can specifically recognize and bind to overexpressed receptors on tumor cells. In the case of ATC, EGFR and VEGF are common targets, as they are frequently upregulated in ATC cells and are associated with tumor growth, metastasis, and angiogenesis.
A particularly promising example of a nanoclay-based drug delivery system for ATC involves the modification of nanoclays with KI (Fig. 6). 64 KI-modified nanoclay systems enhance iodide-mediated targeting in differentiated thyroid tissue. However, ATC cells typically lack a functional NIS, limiting direct applicability in this context. These systems may be combined with redifferentiation strategies to restore NIS expression, enabling effective iodide uptake and targeted drug delivery. Therefore, while promising for differentiated thyroid cancer, KI-modified targeting in ATC should be interpreted as a potential strategy contingent upon restoration of NIS function. By introducing KI into the nanoclay, the nanoclay–iodine complex becomes highly concentrated in thyroid tissue, ensuring targeted drug delivery to the tumor site while minimizing the exposure of surrounding healthy tissues. The KI-modified nanoclay system not only improves the dispersibility of the drug-loaded NPs but also enhances endocytosis and autophagy in ATC cells. This mechanism ensures that the chemotherapeutic agent is delivered directly to the tumor site, where it can be taken up by the cells and exert its cytotoxic effects.
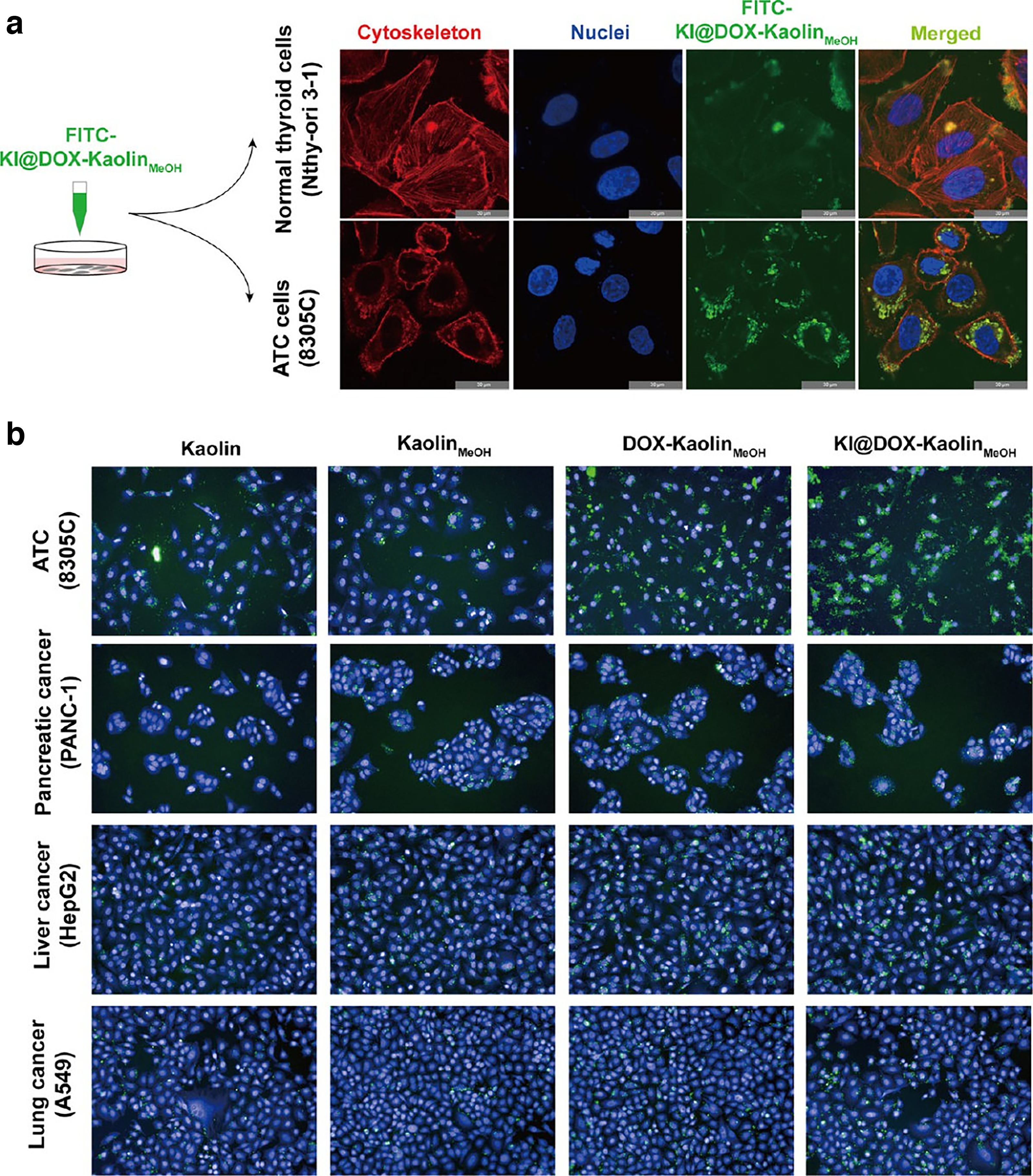
Cellular uptake of nanoclay-based systems for enhanced drug delivery.
Dual-Modality System Integrating Diagnostic and Therapeutic Functions
The integration of diagnostic and therapeutic functions in a single platform, often referred to as theranostics, represents a transformative approach in cancer treatment. This dual-modality system combines both diagnostic imaging and therapeutic interventions, allowing for real-time monitoring of the tumor while simultaneously delivering targeted treatment. 65 The ability to monitor treatment progress and adapt accordingly enhances the efficacy of cancer therapies and allows for personalized treatment regimens. This innovative approach is particularly promising for the treatment of ATC, an aggressive cancer that requires precise targeting and effective therapeutic strategies due to its poor prognosis and resistance to conventional treatments. Incorporating nanotechnology into theranostic systems has led to the development of multifunctional NPs capable of integrating both diagnostic imaging and therapeutic payloads. These NPs can be engineered to carry various diagnostic agents and therapeutic molecules in a single system. This dual-modality approach provides a comprehensive solution for both early diagnosis and targeted therapy, improving the efficacy and precision of cancer treatment. A recent study developed a pH-responsive, HER2-targeted nanoparticle system for the diagnosis and treatment of ATC (Fig. 7). 66 The system, which encapsulates sorafenib and indocyanine green within manganese dioxide-based NPs, offers both magnetic resonance and near-infrared fluorescence imaging capabilities. This dual-modality system enables the precise localization of the NPs at tumor sites, enhancing drug delivery and improving therapeutic outcomes. In vivo studies in ATC xenograft models demonstrated that theranostic NPs accumulated preferentially in tumors, and no overt toxicity was observed in major organs.
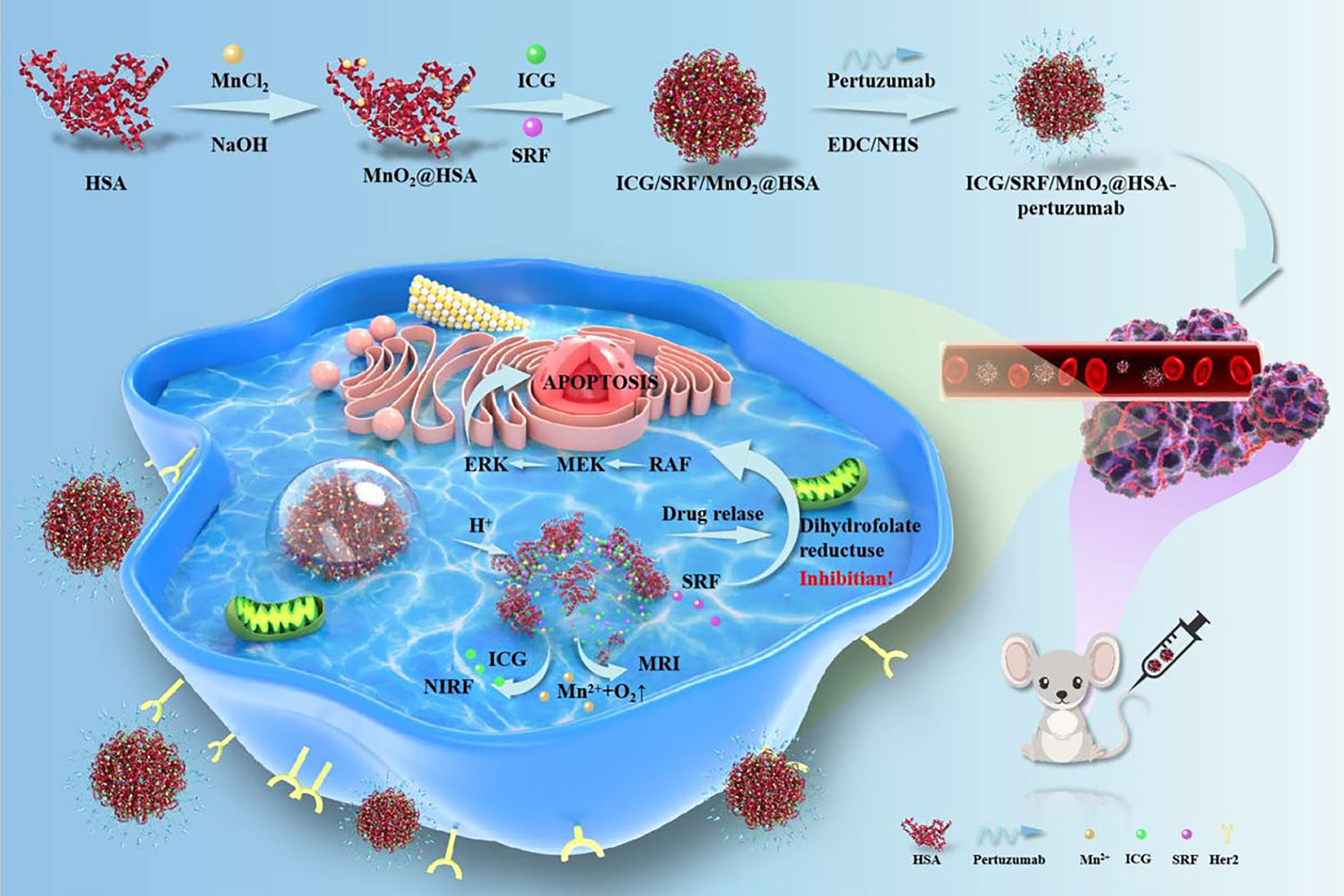
Dual-modality system integrating diagnostic and therapeutic functions. Adapted from Jia et al. 66
Challenges and Future Perspectives
While nanotechnology-driven therapeutic strategies, as summarized in Table 2, show immense promise in the treatment of ATC, several challenges remain in their clinical translation. The complexity of ATC, coupled with the limitations of current treatment modalities, underscores the need for continuous innovation. One of the primary concerns with nanomaterial-based drug delivery systems is their biocompatibility and potential toxicity. 67 NPs must be designed to avoid causing adverse effects when they accumulate in the body, particularly in critical organs such as the liver, spleen, and kidneys. Toxicity can vary depending on the size, shape, and surface charge of NPs. For example, positively charged NPs may cause membrane disruption in healthy cells, leading to cytotoxicity. Furthermore, the long-term effects of NPs within the body, such as their accumulation and clearance, need thorough investigation. To address these concerns, surface modification techniques, such as PEGylation (attachment of polyethylene glycol), have been developed to enhance biocompatibility, stability, and circulation time in the bloodstream. However, optimizing these properties while maintaining effective drug delivery remains a challenge. Future studies should be designed to capture endpoints that reflect ATC’s aggressive clinical features, beyond short-term primary tumor regression. These include metastatic burden, tumor recurrence, and survival outcomes in orthotopic or xenograft models. Resistance reversal should be evaluated systematically by benchmarking nanomaterial-based therapies against standard chemotherapies in cell lines and animal models that exhibit drug efflux or harbor mutations common in ATC. Stimuli-responsive delivery systems should be tested for their ability to overcome efflux- or mutation-driven resistance, and mechanistic readouts should be quantified. Toxicity and clearance studies should include detailed pharmacokinetics, biodistribution, systemic toxicity assessment, and long-term nanoparticle accumulation monitoring to inform translational feasibility. Future advancements will focus on the biodegradability and safe clearance of NPs from the body after drug delivery, minimizing the risk of chronic toxicity.
Studies Based on Nanotechnology for Treating Anaplastic Thyroid Carcinoma
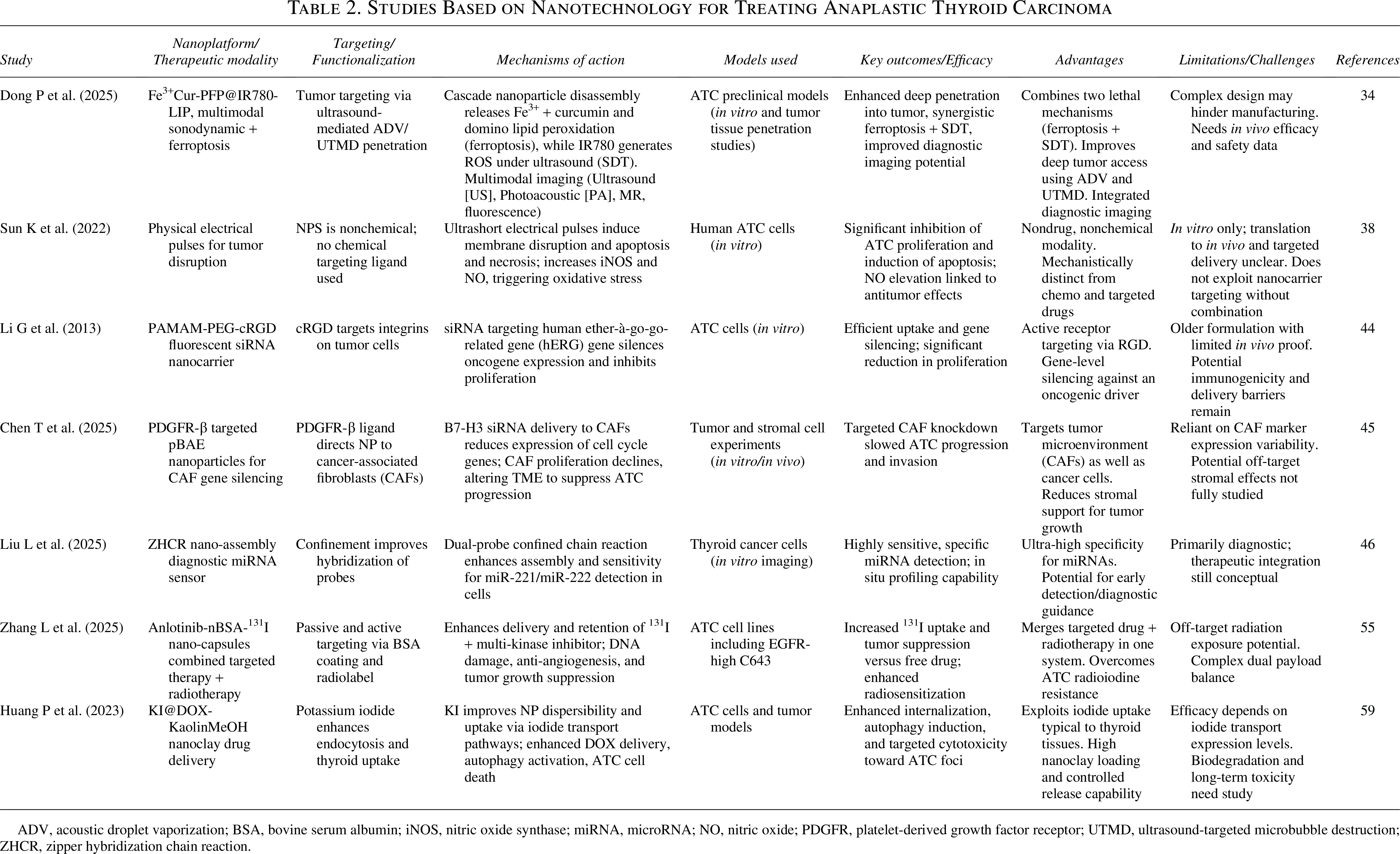
ADV, acoustic droplet vaporization; BSA, bovine serum albumin; iNOS, nitric oxide synthase; miRNA, microRNA; NO, nitric oxide; PDGFR, platelet-derived growth factor receptor; UTMD, ultrasound-targeted microbubble destruction; ZHCR, zipper hybridization chain reaction.
Tumor heterogeneity is a significant barrier to the success of targeted nanotherapies. 68 ATC is a highly heterogeneous cancer, with variations in gene expression, mutation profiles, and TME within different regions of the same tumor. The TME of ATC presents multiple barriers to effective therapy. Hypoxia is a hallmark of ATC tumors due to rapid proliferation and inadequate vascularization, which can reduce the generation of ROS in therapies such as SDT and limit the efficacy of oxygen-dependent treatments. Immune suppression is another critical factor, with abundant tumor-associated macrophages and regulatory T cells contributing to a protumorigenic milieu that can blunt the effects of immunomodulatory nanomedicines or combination therapies. Additionally, stromal barriers, including dense extracellular matrix and cancer-associated fibroblasts, impede nanoparticle penetration and homogeneous distribution within the tumor, leading to spatial heterogeneity in drug delivery. Strategies to overcome these challenges include surface-functionalized NPs for enhanced tissue penetration, stimuli-responsive release systems to increase local payload delivery, and combinatorial approaches that modulate the TME, such as codelivery of immunomodulators or matrix-degrading agents.
As a result, tumor cells may have different susceptibilities to therapeutic agents, including those delivered via NPs. Overexpression of specific receptors, such as EGFR or VEGF, in some tumor cells may not be uniform across all tumor regions, leading to targeting inefficiencies. To overcome this issue, multivalent targeting strategies using NPs functionalized with multiple ligands have been proposed. These strategies aim to target several tumor-specific markers, improving tumor targeting and therapeutic efficacy. Moreover, personalized treatment approaches, guided by genetic profiling and real-time imaging of the tumor, can lead to the development of customized nanocarriers designed to address the unique molecular characteristics of each patient’s tumor. This approach can enhance the precision and effectiveness of therapy while minimizing side effects.
Drug resistance remains a major hurdle in treating ATC. 69 ATC cells often exhibit resistance to chemotherapy and radiation due to the upregulation of drug efflux pumps (such as P-glycoprotein) and mutations in key oncogenes. Nanomaterial-based systems offer a promising solution by delivering drugs in a controlled manner that bypasses the typical resistance mechanisms. For example, NPs can encapsulate drugs and protect them from being pumped out of the cells by efflux pumps. In addition, stimuli-responsive NPs that release drugs in response to tumor-specific stimuli such as low pH and high enzyme activity can improve drug efficacy and overcome resistance. The combination of chemotherapies with RNA-based therapies, such as siRNA or CRISPR–Cas9 systems, can further target and silence resistance-associated genes, making tumor cells more sensitive to conventional treatments. This multimodal approach can enhance the therapeutic outcomes by targeting multiple pathways involved in resistance. Finally, clinical trials will play an essential role in evaluating the safety and efficacy of nanomaterial-based therapies in ATC patients. With the continued development of nanotechnology, the precision and efficacy of cancer treatments can be significantly improved, offering hope for better survival rates and quality of life for ATC patients.
Conclusions
ATC is a rare and highly aggressive form of thyroid cancer, characterized by its poor prognosis, early metastasis, and resistance to conventional treatment modalities. Despite significant advances in the understanding of ATC and its molecular mechanisms, the lack of effective therapies has left patients with limited treatment options and low survival rates. However, nanotechnology-based drug delivery systems have emerged as a promising strategy to address the challenges in treating ATC, offering targeted, precise, and personalized treatment approaches. This review has highlighted the significant progress made in the development of nanomaterial-enhanced therapies for ATC, focusing on several cutting-edge approaches that combine diagnosis and treatment in a single system. Noninvasive physics-based therapies such as SDT and NPS have demonstrated potential in overcoming the limitations of traditional treatments. The use of NPs to carry chemotherapeutic agents, RNA molecules, sonosensitizers, or radioactive isotopes has shown great promise in targeting ATC cells while minimizing off-target effects and systemic toxicity. Dual-modality theranostics, such as NPs integrated with diagnostic imaging agents and therapeutic payloads, provide a comprehensive solution for the early detection and real-time monitoring of tumors, as well as precise drug delivery. Despite the promising preclinical findings, several challenges remain. Translating nanotechnology-based therapies for ATC to the clinic requires addressing regulatory requirements, including safety, pharmacokinetics, immunogenicity, and reproducible nanoparticle characterization, as well as challenges in manufacturing scalability. Clinical trials will play an essential role in evaluating the efficacy and safety of nanomaterial-based therapies for ATC, with the ultimate goal of improving survival rates and quality of life.
Authors’ Contributions
L.M. and X.P.: Methodology, software, and writing—original draft preparation. Y.L.: Data curation. T.H.: Visualization. G.Y. and Y.W.: Validation. W.C.: Conceptualization, supervision, and writing—review and editing.
Footnotes
Disclosure Statement
The authors report no conflicts of interest in this work.
Funding Information
No funding was received for this article.