
Abstract
Objectives:
The objectives of this research were to describe the interactions (formal and informal), in which macrocognitive functions occur and their location on a pediatric intensive care unit, to describe challenges and facilitators of macrocognition using space syntax constructs (openness, connectivity, and visibility), and to analyze the healthcare built environment (HCBE) using those constructs to explicate influences on macrocognition.
Background:
In high reliability, complex industries, macrocognition is an approach to develop new knowledge among interprofessional team members. Although macrocognitive functions have been analyzed in multiple healthcare settings, the effect of the HCBE on those functions has not been directly studied. The theoretical framework, “macrocognition in the healthcare built environment” (mHCBE) addresses this relationship.
Method:
A focused ethnographic study was conducted including observation and focus groups. Architectural drawing files used to create distance matrices and isovist field view analyses were compared to panoramic photographs and ethnographic data.
Results:
Neighborhoods comprised of corner configurations with maximized visibility enhanced team interactions as well as observation of patients, offering the greatest opportunity for informal situated macrocognitive interactions (SMIs).
Conclusions:
Results from this study support the intricate link between macrocognitive interactions and space syntax constructs within the HCBE. These findings help increase understanding of how use of the framework of Macrocognition in the HCBE can improve design and support adaptation of interprofessional team practices, maximizing macrocognitive interaction opportunities for patient, family, and team safety and quality.
The importance of improving the healthcare environment and interprofessional team work to reduce errors and improve safety has been established by the Institute of Medicine (Reid, Compton, Grossman, & Fanjiang, 2005). A systems approach has the potential to radically improve healthcare quality and safety. Such a view goes beyond individual caregiver knowledge, skills, and performance to include adaptive interprofessional team cognitive performance within the complex environment in which healthcare teams function.
The overarching goal of this research was to empirically investigate the influence of the healthcare built environment (HCBE) on macrocognition (m). The theoretical framework for this research advances a novel conceptual framework, “macrocognition in the HCBE” (mHCBE), which is comprised of the nursing metaparadigm (person, health, nurse, and environment; Fawcett, 1984; Nightingale, 1860), macrocognition theory (Patterson & Hoffman, 2012), and space syntax theory (Haq & Luo, 2012; Hillier, 2008).
Macrocognition, the “adaptation of cognition to complexity” (Patterson & Hoffman, 2012, p. 221), provides a broad cognitive approach to improving patient quality and safety. The theoretical framework of macrocognition comprises five interrelated functions: sensemaking, replanning, detecting problems, deciding, and coordinating (Patterson & Hoffman, 2012). Macrocognition has been studied in industrial environments (Patterson, Watts-Perotti, & Woods, 1999), as well as healthcare, but the influence of the built environment on macrocognition has not been evaluated.
A key framework influencing healthcare design is space syntax theory, which assumes that the configuration of a space is created to accommodate planned functions, while the functions are influenced and changed by the shape of the space (Hillier, 2014). The space syntax theory constructs utilized in this study are openness (lack of boundaries or partitions), connectivity (adjacencies to other spaces), and visibility (line of sight; Haq & Luo, 2012; Trzpuc & Martin, 2010).
This study examines the influence of the HCBE on macrocognition in a pediatric intensive care unit (PICU). The specific aims are, in a PICU in an academic medical center, to: describe interactions (formal and informal) in which macrocognitive functions occur and their location, describe challenges and facilitators of macrocognition within the physical environment using space syntax constructs, and analyze the HCBE using space syntax to explicate influences on macrocognition.
Background
In healthcare, macrocognitive functions have been analyzed. In two outpatient settings (cardiology and diabetes care), attention to macrocognitive functions offered a more structured approach to patient decision making and self-care, with some improvements in glucose regulation and adherence to medication planning (Dhukaram & Baber, 2015; Klein & Lippa, 2008). In the inpatient setting, macrocognition has been studied through formal team cognitive interactions, such as intensive care unit (ICU) rounds and handovers, which resulted in fewer medical errors and better judgment, improved communication, and better learning (Hill, 2010; Patel, Shine, & Almoosa, 2014; Patterson, 2008).
Several studies suggest that macrocognitive functions are influenced by work environment design. Designs that allow coworkers to see each other in the inpatient or emergency department settings (Fackler et al., 2009; Schubert, Denmark, Crandall, Grome, & Pappas, 2013) enhanced the relationships between novices and experienced team members, improving task prioritization and increasing overall patient care unit expertise (Patterson, Ebright, & Saleem, 2011).
Visibility between care teams in ICUs remains a critical factor for reducing mortality rates (Joseph & Rashid, 2007; Leaf, Homel, & Factor, 2010; Lu, Ossmann, Leaf, & Factor, 2014; Rashid, 2014) and improving collaboration (Apple, 2014; Ball & McElligot, 2003). Although researchers disagree on whether designing decentralized nurses’ stations (NSs) improves patient visibility, they concur that by distributing NSs, nursing interactions, and collaboration with other team members are reduced (Pati, Harvey, Redden, Summers, & Pati, 2015; Zborowsky, Bunker-Hellmich, Morelli, & O’Neill, 2010).
Theoretical Framework
mHCBE is a novel framework that encompasses the intersection of cognition and actions in time and space with the goal of improving patient care. The HCBE is defined as a physical space or group of spaces (campus) that incorporate clinical, architectural, and operational science as well as interprofessional teams (also referred to as team members) to provide adaptive, high-quality, culturally appropriate, and cost-efficient patient and family care. This framework has been influenced by the disciplines of nursing (environment of care), human factors engineering (macrocognition theory), and architecture (space syntax theory).
A key concept is “situated macrocognitive interaction (SMI),” which describes an interaction representative of the macrocognitive functions, situated in the built environment. It is influenced by definitions of formal and informal interactions: situated episodes or communications within work places and between colleagues (Wagner, 1994). A formal interaction is a routine or scheduled activity or meeting lasting more than a few minutes often with planned participants and agendas. Informal interactions are unplanned, spontaneous events often occurring due to proximity to another individual in a space or visual prompts (Kraut, Fish, Root, & Chalfonte, 1990).
Method
Design
A focused ethnographic study was conducted within a PICU. Focused ethnography was used to understand one aspect of a culture in a short engagement (Cruz & Higginbottom, 2013; Fetterman, 2010; Hammersley & Atkinson, 2007). This study, congruent with Cruz and Higginbottom's emphasis, is about the problem of macrocognition and the HCBE in a PICU context and with a discrete interprofessional team community. The theoretical framework provided the orientation for the principle investigator’s observations and focus group participants (n = 15 and 21). These participants held a specific knowledge of care of the PICU patient. Approval was obtained from the institutional review board.
Sample
Maximum variation sampling (Creswell, 2007) was used. Members of the clinical, operational, and therapeutic ancillary groups were all included in the observations (Table 1). PICU teams were assigned geographically as depicted in Figure 1: blue team (patient rooms [PRs] 1–21); green team (PRs 22–41), and the red team (ad hoc rooms).
IPT Members and Stakeholder Groups.
Note. Focus group: Mean years in profession: 12.38 (range 0.9–46); mean years in PICU: 6.33 (range 0.9–31). PICU = pediatric intensive care unit; IPT = interprofessional team; IV = intravenous; NP = nurse practitioner.

Overall floor plan with patient care rounding configuration. Red team is “ad hoc.”
Setting
The setting was a 40-bed PICU at an academic medical center on the East coast. A pediatric critical care setting was particularly useful for this research because it includes the complexity and criticality in which emergent phenomenon occur on a healthcare unit. This 21,000 sf unit is nearly triple the size of the previous PICU unit (7,500 sf). Patients’ ages range from infant to young adults requiring medical and surgical intensive care.
Procedures
Prior to data collection, two investigators visited the unit to meet the leadership team, compare the unit to the floor plan, and finalize the study design. The floor-plan drawing file was obtained and converted to a file program (Figure 1).
Data Collection
Data collection included observation, focus groups, and collection of architectural data. The study was introduced to interprofessional team members by unit leadership prior to the preliminary visit, then via posters, e-mails, notices, and introductory meetings on the first day of data collection; access to the unit was facilitated by investigators who worked on the unit. Informed consent and voluntary participations were obtained.
Unit observation was conducted over an 11-day consecutive period between 7 a.m. and 5 p.m. The day shift allowed for maximization of interprofessional engagement. Observations took place outside PRs and in support spaces (SSs), including NSs, and circulation spaces (CSs; corridors) as consistent with healthcare architectural planning (Rashid, 2015). Participants were observed individually and within teams during formal and informal interactions. Individual observation (shadowing) of 15 representatives from interprofessional team member groups (Table 1) lasted from 30 min to 4 hr. Nursing station “observation rounds” were conducted to ascertain use and number of team members in the stations. Handwritten field notes were documented on observation and floor-plan worksheets.
Four focus groups with 21 total participants (range two to seven per group; see Table 1) were conducted on the last 2 days of data collection to minimize influence on behavior. The makeup and recruitment of the focus group was in keeping with factors described by Krueger (2014), which highlight the importance of inviting participants in keeping with the purpose of the study (Krueger, 2014, p. 82). A semistructured interview guide was used. During the focus group, each participant annotated a blank floor plan with the location of their interactions with team members and areas that depicted openness, connectivity, and visibility.
Architectural drawing files were collected, and panoramic photographs from NSs were taken to gauge visibility (privacy protected by obscuring monitors/faces and removing patient identifiers). PICU specific artifacts (rounding scripts and informational family welcome packets) were obtained to inform understanding of the unit culture.
Data Analysis
Path distances (in feet) generated a distance matrix between rooms on the unit. These were used to develop isovist views, with a 360° field of vision from NSs into PRs. These were compared to panoramic photos to assess visibility between patients and interprofessional team members.
Focus group audio recordings were transcribed verbatim. NVivo 11 Pro software and Microsoft Excel were used in analysis and coding of focus group and field observation findings. Directed content analysis as described by Hsieh and Shannon (2005) was utilized, as this approach uses predefined categories, which allowed focus on the concepts of formal and informal SMIs and space syntax constructs. The research also remained open to emergent themes.
Saturation was met during analysis of observation notes, focus groups, and artifacts. Iterative analysis was performed in stages. Initially, all observation and focus group responses were organized on a spreadsheet according to types of SMIs and space syntax constructs. In the second stage, each room on the floor plan was added to code data by location, which helped to determine where the SMIs and space syntax constructs occurred. In the third stage, cognitive analysis was performed to compare preexisting codes and emergent themes. The results of this multistage process were then compared to the data from distance matrices, isovist analyses of the floor plan (see Tables 2 and 3), and panoramic photographs. Reflection at each stage allowed for emergence of additional findings.
Distance Matrix Analysis Reported in Feet.
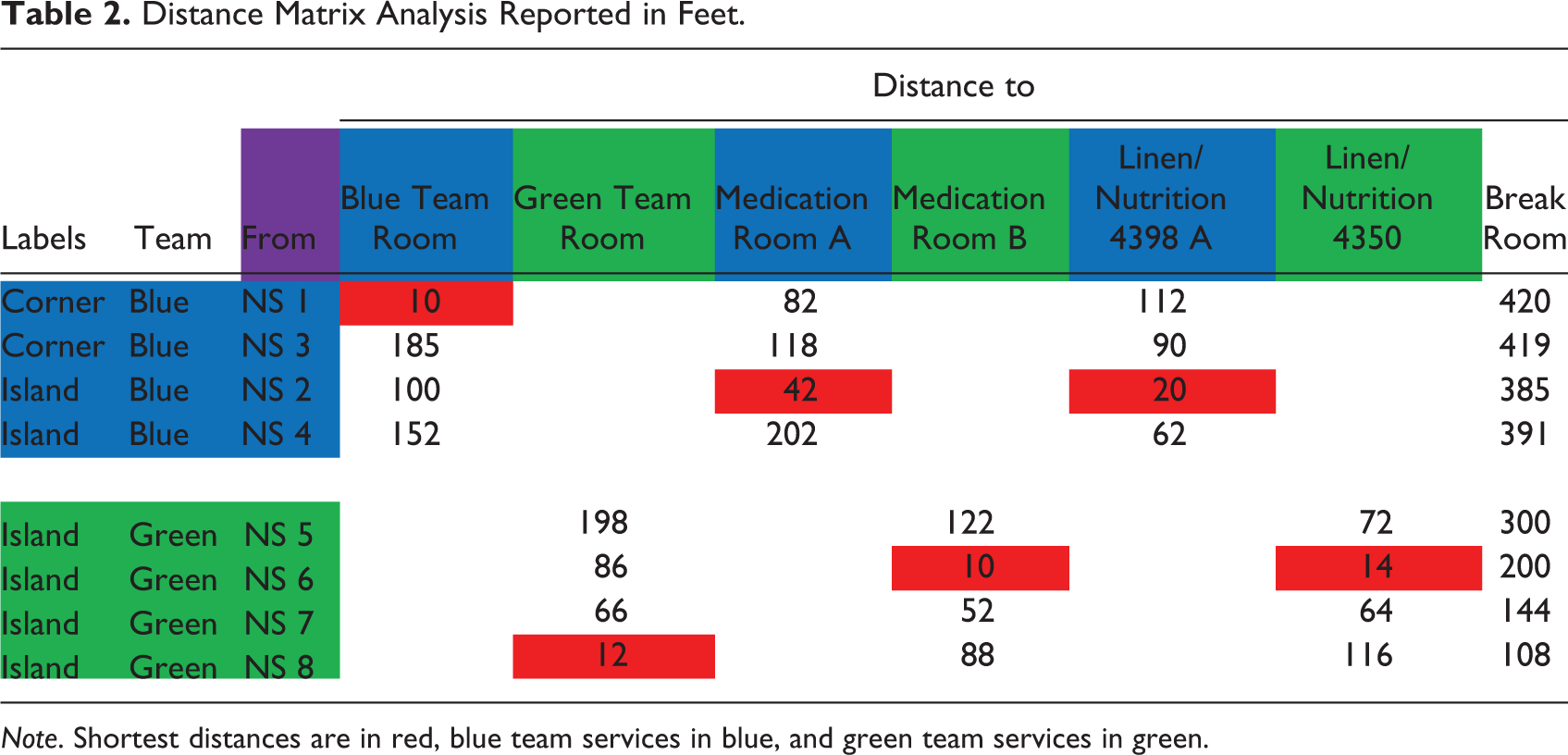
Note. Shortest distances are in red, blue team services in blue, and green team services in green.
Isovist Analysis.
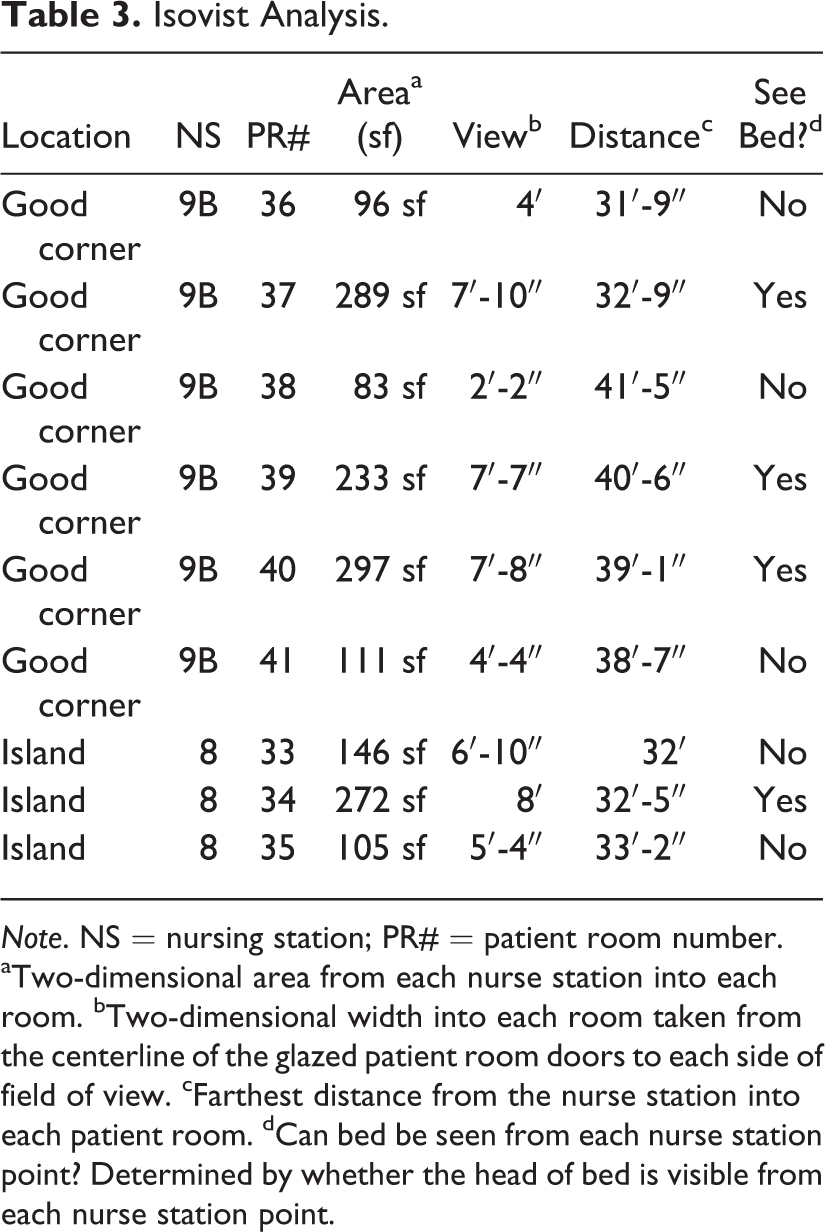
Note. NS = nursing station; PR# = patient room number.
aTwo-dimensional area from each nurse station into each room. bTwo-dimensional width into each room taken from the centerline of the glazed patient room doors to each side of field of view. cFarthest distance from the nurse station into each patient room. dCan bed be seen from each nurse station point? Determined by whether the head of bed is visible from each nurse station point.
Trustworthiness
Trustworthiness is comprised of four criteria: credibility, transferability, dependability, and confirmability (Lincoln & Guba, 1985). Credibility criterion was established through saturation, peer debriefing, and triangulation of data from multiple sources of observation, focus groups, and architectural floor-plan data. Transferability was achieved through thick description of SMIs as evidenced by robust quoted texts. Confirmability was achieved by an audit trail for all collected data. For example, daily research notes, reflexive journaling, verbatim audio recordings, and other investigator communications were dated in field notes. Finally, dependability was achieved and assured through the audit trail document reviewed with the investigative team for consistency. Reflexive journaling occurred within each of these criteria and throughout the research.
Results
Findings are based on analyses of data collected from observations, focus groups, and architectural evaluation. To maintain confidentiality, quotations by study participants are identified by interprofessional stakeholder groups: clinical, operational, or therapeutic.
Formal and Informal SMIs
Situated Macrocognitive Interactions (SMIs): Formal.
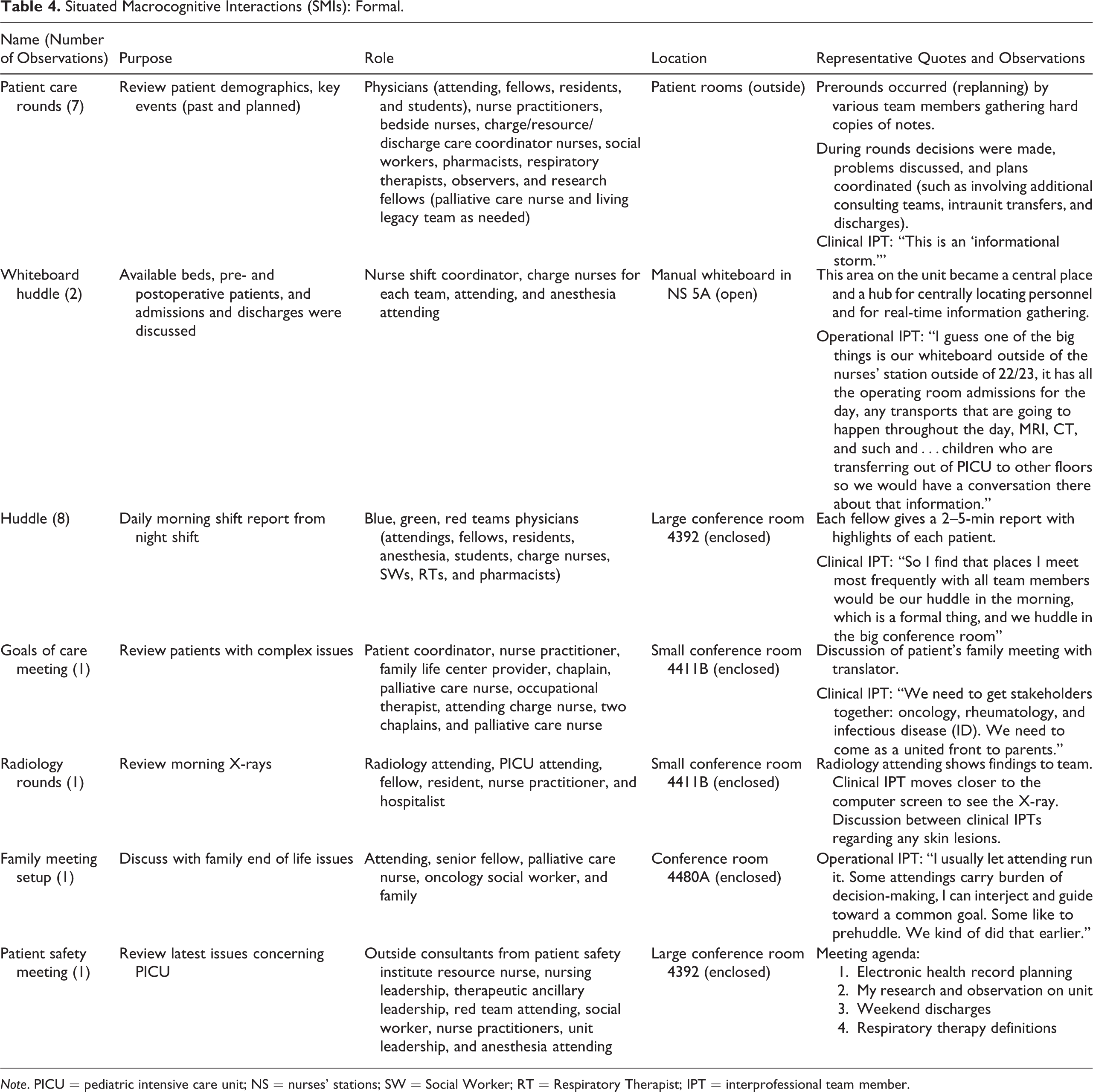
Note. PICU = pediatric intensive care unit; NS = nurses’ stations; SW = Social Worker; RT = Respiratory Therapist; IPT = interprofessional team member.
Prerounding. I come up with a game plan, then examine with nurse and on computer, look at labs. I have an ear listening…. The resident, NP, and medical students are trainees working and learning. One, resident presents; two, fellow critiques game plan. Then go through and, three, attending critiques, asking the question, “What do we think we should do?”
The rounding teams, composed of 4–20 individuals, met for 30–180 min, and occupied from 6 to 180 sf. The unit layout influenced configurations in which the number of staff and their equipment flexibly conformed to the shape of the existing space. The rounding configurations were square, rectangular, and semicircular depending on layout, location, and adjacencies to PR being visited (Figures 1 and 2). These configurations sometimes obstructed corridors for other staff and patient’s family members, appearing to impede hearing and engagement, as exemplified by interprofessional team members moving in closer to the speaker and asking for communications to be repeated.
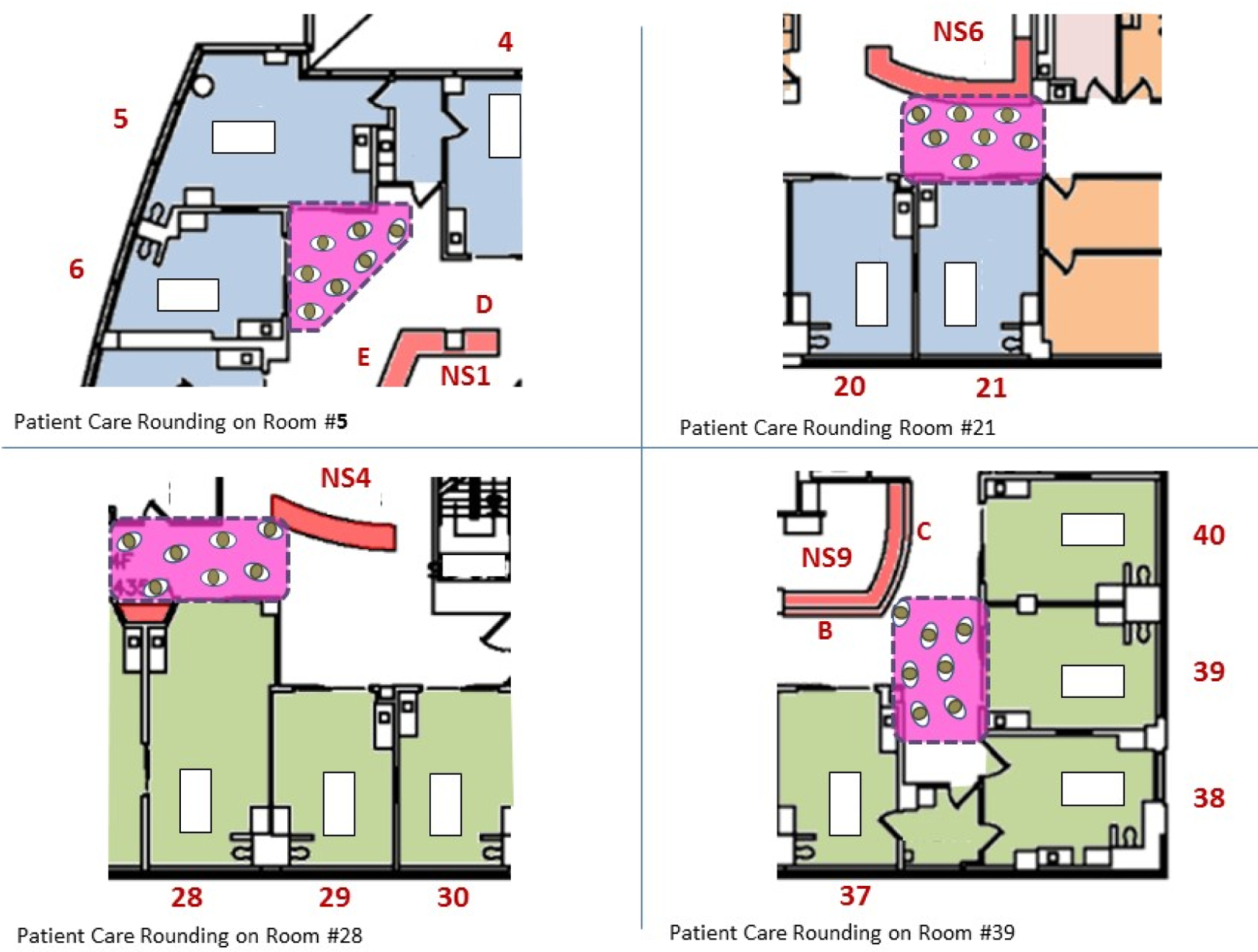
Rounding configurations.
Informal SMIs were triggered by visual cueing (bumping into), auditory cueing (overhearing), and spontaneous searches (Table 5). The category of spontaneous searches was a finding that emerged from the data analysis.
Situated Macrocognitive Interactions (SMIs): Informal.
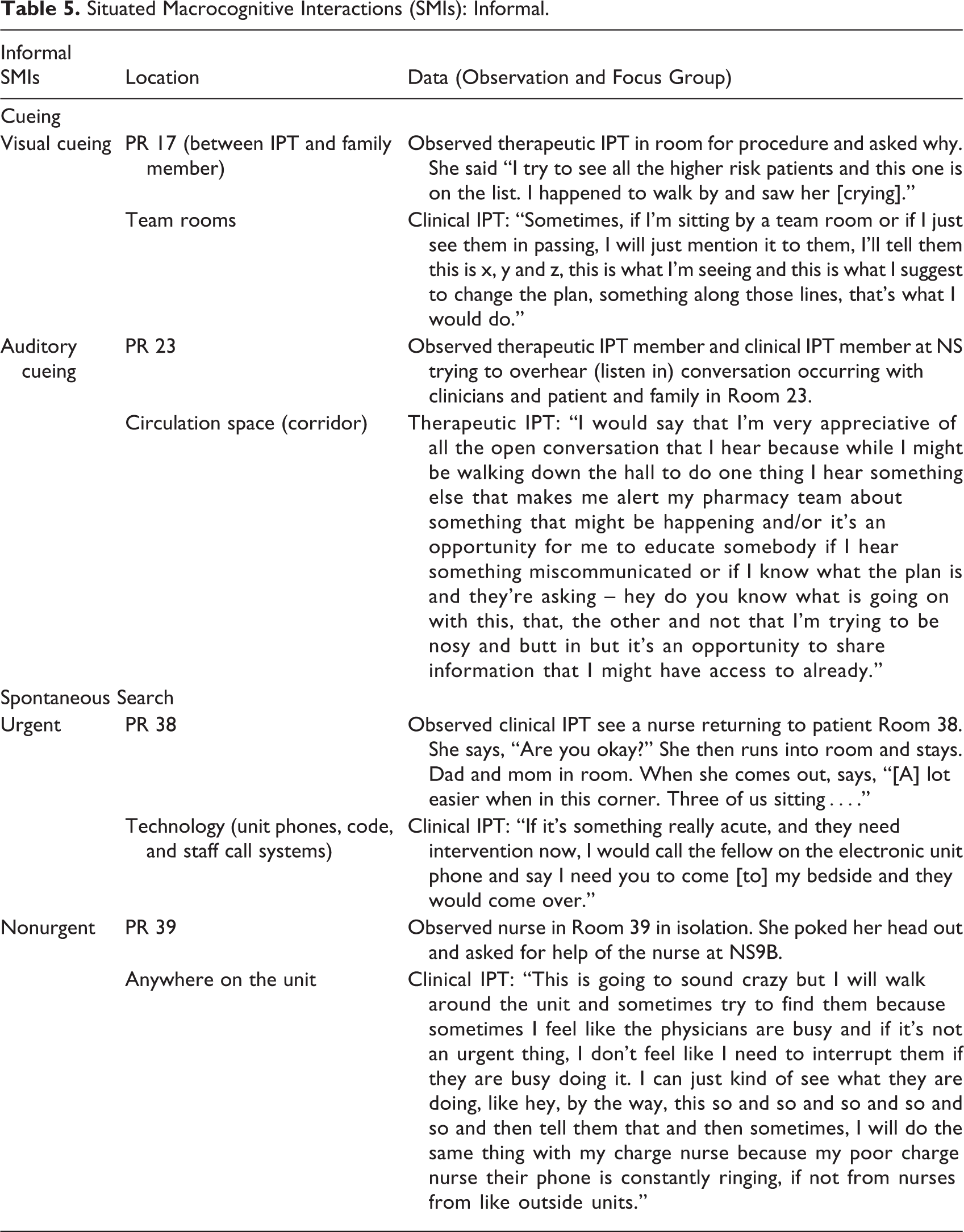
SMIs prompted by a visual cue (Table 5) were observed (n = 27) and described by focus group participants (n = 50). These SMIs were observed more often at a PR doorway when an interprofessional team member stood waiting for another team member to walk by, than in the corridor where they bumped into each other, or the NSs. Macrocognitive activities observed during visual cueing episodes focused on the exchange of information regarding a patient. For example, one interaction resulted in the updating of a care plan, when two clinical teams ran into each other as one exited a PR. In another example, the attending physician ran into an interprofessional colleague, and they discussed their patients’ symptoms and planning activities.
SMIs prompted by auditory cueing interactions (Table 5) were observed less often (n = 3) and described during the focus group responses (n = 18). These interactions occurred in corridors and in the NSs nearest to the team rooms. Nurses were observed to push their desk chairs closer to the open doorway of the team rooms to better hear the conversations occurring, so that they could join in when they thought appropriate. Other informal SMIs prompted by auditory cueing occurred in the NSs. At times, one conversation between interprofessional team members would occur while others, not initially included, would listen in and contribute new information or use the dialogue to inform their care plan.
SMIs prompted by spontaneous searches also emerged from observation of team members (Table 5). Nonurgent searches often occurred when one team member needed advice or assistance from another interprofessional team on something. Participants also described searching for interprofessional team members in the corridors when they needed to discuss a patient condition. This action was referred to by some interprofessional team members as “poking head in or out” (n = 21) as observed or explained by focus group participants. Urgent searches (n = 4) for team members were observed during a code blue or critical event by witnessing others actively running to or assisting a team member or by utilizing electronic notification systems. Both urgent and nonurgent searches were observed in the corridors and within NSs.
Challenges and Facilitators of Macrocognition Using Space Syntax Constructs
Observation and focus group data were used in analysis to interpret the relationship of three space syntax constructs to macrocognition and how space challenged or facilitated team interactions (Table 6).
Space Syntax Constructs Within Informal Situated Macrocognitive Interactions.
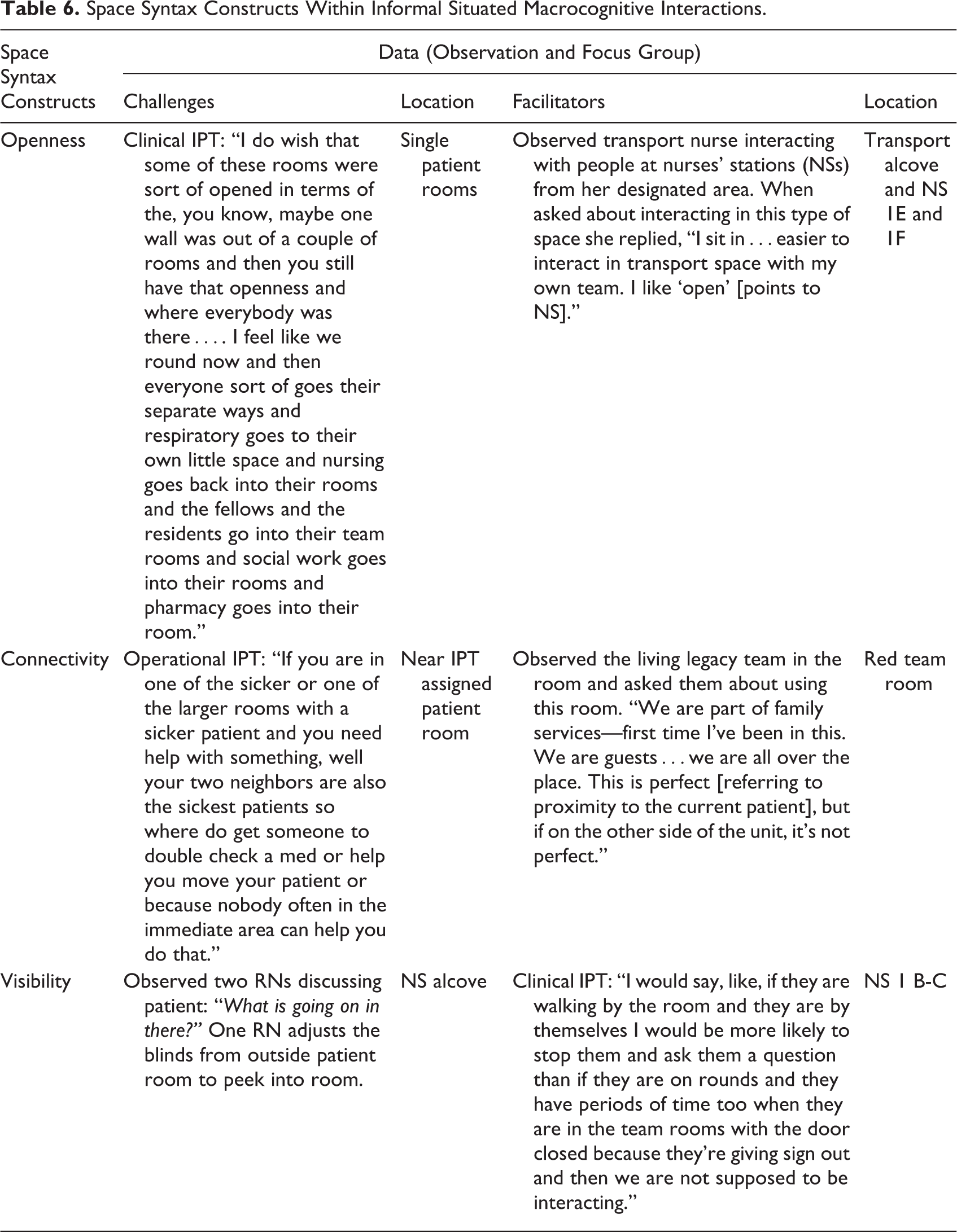
Openness
Openness (lack of boundaries or partitions) supporting connections with other interprofessional team members helped facilitate macrocognition. Openness was observed and described by focus group participants as occurring primarily in corridors, then in front of teams’ rooms, and finally NSs. As a therapeutic interprofessional team member said, I like to use…green and blue [team] rooms…the providers sit…typically…when everybody is done rounding so during the morning, I will find most of my communication happens in the hallways, outside patients’ rooms. You guys normally shut the door…for the family to have their own space because everything is so open here that to have your own space is valuable…so shutting the door allows them to have that space.
Connectivity
Connectivity (adjacency to other spaces) was observed in spaces between interprofessional team members and between the interprofessional team members and their patients. A bedside nurse shared:
Connectivity with other team members was a challenge when interprofessional team members did not have a designated space on the unit, or they shared a space with members of their same professional team. Further, the PICU layout of single PRs appeared to impact nurse to patient ratios and sometimes intraunit transfers.
Some rooms had a column or a gap between them or a door or corner that made it hard to go between these two rooms or contributed to their assignment bridging two NSs. The location appeared to influence whether a nurse was assigned one or two patients.
Visibility
The layout of the unit influenced visibility (line of sight) of interprofessional team members and patients. Team members used “corners and islands” to describe the best nursing assignments by marking up a floor plan and providing a walking tour to these areas. They further classified corners as “great, lovely, or good.” Some NSs were classified by interprofessional team members as islands. When discussing with one clinical team member the comparison between an island NS on this PICU to previous employment in another PICU facility, she replied, I didn’t get stuck on these islands. Had alcove, so always had someone. I feel all alone. If anything happened…” She noted that when she needs help, she “yell[s] out loud to nurses in neighborhood, [and] wait[s] for someone to pass by.

Panoramic and isovist views from nurses’ stations (NS) 8 (island) and NS 9 B, C (good corner).
In one nursing station with an island configuration (NS 8), the room that has a view of patient’s bed has the larger area of vision (272 sf). Of note is that the distances between the NS and the door of the PR are nearly equal (the width of the corridor). The difference between the corner and the island configuration is the visual field between this station and other NSs, which does not correlate with the distance. In NS 9, other NSs (9B and 9C) are visible, but in NS 8, no other NSs are visible.
On a smaller scale, challenges to visibility were observed when the doors to PRs were closed and the window shades drawn. Bedside nurses could not see people going by and other interprofessional team members could not see into the room. Interprofessional team members were observed poking their head in or out of the PRs looking for help, which was described to be done at the risk of micromanaging. A therapeutic interprofessional team member was observed to poke her head out of a room and say to the nurse, “I heard that. Sorry I’m nosy.”
When challenges to visibility occur, interprofessional team members actively searched for other interprofessional team members. As described by a therapeutic interprofessional team, “If I have a question, say about transport, and I’m not busy, I will walk over and see if someone is in the transport alcove [behind NS 1E on Figure 1] and just ask them.”
When describing the smaller size of the old unit, many interprofessional team members’ referred to ‘eyes on the patient’: “There were lots of people to watch that child…so that they didn’t wake up and maybe pull out their ET tube.”
Influence of the HCBE Space Syntax Constructs on Macrocognition
As noted, the intersecting relationship between macrocognition and the space syntax constructs was evident throughout the study and can be summarized in an overarching theme called the “neighborhood.” This theme emerged through deeper analysis and interpretation of the data, particularly the way that team members described the spatial functioning of the unit. Within this larger theme of neighborhood, three subthemes emerged: “corners and islands,” “neighbors and buddies,” and “eyes on the patient.”
Thematic analysis: The neighborhood
The term neighborhood first appeared when the notice for “neighborhood huddle” was sent through the electronic phone system. Further clarification of the term was explained by the team members as “little areas” or “places to get answers.” An operational team member described neighborhood as originally used to help with the transition from a prior PICU, where all PRs and services were visible and staff interacted informally, to one that was linear and separated by individual PRs, and nearly 3 times the size. The idea was to create groups of adjacent spaces to make a neighborhood.
Corners and islands
The interprofessional team members used the term “corner” as a way of pointing to an actual place on the floor plan or showing these areas within the physical layout. They categorized (and annotated on a blank floor plan) these corners as “great” (NS 9); “good, lovely, and big” (NS 1B-D); or simply as “a smaller scaled corner” (NS 3A, B, C; Figure 1). As described by an operational interprofessional team member: I think a lot of the straighter ways where…kind of in between nurses’ stations and not necessarily around a team room, because the corners, since there’s enough patients on both sides at one nurses’ station, they tend to have more people, the corners are pretty good.
Other examples of island neighborhoods include NS 2, 4, 7, and 8. Although NS 8 is adjacent to a team room, it is considered an island when no other nurse buddies are available, such as if an assignment pairing of PR 31 and 32 occurs with rooms facing both NS 7 and 8. Nurses describe walking to other neighborhoods from these island locations not only for help but simply to see others.
Neighbors and buddies
The PICU HCBE appeared to facilitate the formation of clinically and socially supportive relationships, which the nurse study participants referred to as neighbors or “buddies.” Buddies are nurses with near or adjacent patient assignments, who are visible to each other, and on the same team. These buddies were identified as team mates for neighborhood patient care. To facilitate this relationship, they created a “neighborhood report” or “mini-huddle” following formal changeover report to understand their adjacent team member’s assignment. This huddle was performed to provide coverage and to increase the safety of their collective patient care activities by understanding their neighborhood’s events. As explained by a clinical interprofessional team member in a focus group, “sometimes, they’re just there for an extra pair of hands like when you get an admission, your buddy, your nurse next to you, always comes and helps you settle the kid.”
Eyes on the patients
The theme of “eyes on the patient” emerged from analysis of observations and focus group data. A clinical interprofessional team member described the difficulty of having eyes on the patient due to island configurations: “Very, very unideal such as we have a couple of rooms that are sort of on an island or in between NSs, where it is hard to have eyes on the patient because it looks out onto a hallway.”
Summary of Key Findings
Well-designed neighborhoods of the PICU are those in which all three of the space syntax constructs (openness, connectivity, and visibility) are present, facilitating both formal and informal SMIs. If the neighborhood limits or inhibits macrocognitive processing or lacks the space syntax components, it is considered an island.
Discussion
Neighborhoods are a place that includes the key functions of a group of residents. The importance of having “streets” or corridors that allow for interprofessional team member interactions and visibility is reminiscent of Jacobs’s (1961) view of neighborhoods: A city street…as the streets of successful city neighborhoods always do, must have…: a clear demarcation between public and private space; eyes upon the street, eyes belonging to those we might call the natural proprietors of the street. The building on a street…must be oriented to the street. They cannot turn their backs or blank sides on and leave it blind. (p. 35)
In this PICU, visibility (line of sight) is a major factor for design. The findings suggest that visibility is determined more by field of vision than distance. Findings are consistent with studies linking visibility with patient safety and quality care outcomes (Apple, 2014; Ball & McElligot, 2003). Findings also support the analysis of reduced team collaboration by Zborowsky et al.(2010) and add to the literature with isovist (field view) analysis demonstrating decreased field of vision between NSs. The only two alcove-style NSs in the hallway outside of PRs 25/26 and 27/27 (highlighted in red on Figure 1) help to mitigate the island configurations with increased visibility to these rooms and were a well-populated interprofessional team member location for sharing information.
These findings highlight the interrelated nature of the space syntax constructs and that modification of openness, while sometimes desirable for privacy, has an impact on visibility. Additionally, participants’ responses suggest visibility may enhance clinical and operational interprofessional team member development.
Macrocognitive Adaptation to Challenges
Interprofessional team members sometimes adapted or repurposed the space to meet their needs. When openness created a limitation, the interprofessional team member sought out any enclosed space, even an empty PR or medication room for privacy.
Implications for Practice
The implications for practice, based on this research, are centered on creating neighborhoods comprised of PRs, SSs, CSs, and teams. This supports improving the process of patient rounding to one that is neighborhood-based instead of geographically based. Long-term changes which support creating neighborhood’ configurations include reconfiguring NSs to team stations improving visibility within and between stations as well as standardizing PR sizes.
Recommendations for Healthcare Design and SMIs
The findings of this study suggest that macrocognition is enhanced by certain features of the HCBE that facilitate successful neighborhoods, particularly the dimensions of a “good corner” depicted in observation, participant responses, and isovist views. These features include NSs with visibility within and between other NSs or nurse alcoves and short and straight corridors without columns or walls blocking views (or design layout to increase number of corners and maximize views). Recommendations based on this study include designing and testing new or reconfigured HCBE spaces that maximize these features. Additionally, cost-effective adaptations of interprofessional team practice may also be developed for existing designs. For example, to reduce the number of persons in the corridor during patient care rounding, virtual interactions could be implemented from team rooms. Other uses of islands could be explored, such as multidisciplinary seating/monitoring to facilitate SMIs.
Architectural and computer simulation modeling methods and analyses could be used together to find the right balance between space syntax constructs, clinical care, and interprofessional team member SMIs (Cai & Zimring, 2012; O’Hara, 2014; Shaikh, 2015). The intersection of these fields is in its early stages; however, this could be a beneficial topic for interprofessional practice and education. Future studies could explore the SMIs in other settings as well as provide quantification of the situated SMI occurrences and examine the link between SMIs and patient outcomes.
Limitations and Strengths
The study was performed in one pediatric ICU over a period of 11 days (on day shift) which limits the generalizability of the findings to other shifts or ICUs. However, the use of thick description, as advocated by Lincoln and Guba (1985), was utilized to enhance transferability of findings. We recommend validating our recommendations with members of night shift and the particular hospital staff before implementing.
Strengths of the study include the data triangulation between ethnographic and architectural data components; an interdisciplinary approach to understand the intersection of nursing, human factors engineering, and architecture; and a deeper understanding between the intended use of space and the adaptation and meaning of space.
Conclusion
Results from this study support the intricate link between macrocognitive interactions and space syntax constructs within the HCBE. These findings help increase understanding of how to use the framework of mHCBE to improve design of new spaces or refine existing spaces or adapt interprofessional team practices to maximize formal and informal SMI opportunities. The findings lay the foundation to replicate this research to develop the mHCBE framework into a theory for future research to improve safety and quality for patient and family care and interprofessional teams.
Implications for Practice
Improve preplanning for space design to include all interprofessional team members, identifying corners, and potential islands. Support likely places where informal interactions among interprofessional team members (clinical, therapeutic, and operational) will occur, including in corridors, in front of PRs and near team rooms. Improve patient rounds by having colocated rooms with dedicated interprofessional team members. Use smaller neighborhoods to allow “eyes” on the patients and each other for better team work and detection of subtle changes in patients’ condition to improve patient care.
Footnotes
Acknowledgments
The authors would like to acknowledge Steven Langston, AIA, ACHA, EDAC, LEED BD+C, design director, Rogers, Lovelock, and Fritz, Inc., Orlando, FL; Judy Nordberg, education and clinical services librarian, University of Massachusetts Medical Center, Worcester, MA; Stuart Roberston, Ed.D. Robertson Educational Resources, NVivo specialist; Joshua F. Kilbridge, President Creative Director, Kilbridge Associates, for editorial assistance; and to all the Interprofessional Team Members working in this PICU.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.