
Abstract
The purpose of this literature review is to provide a better understanding of the impact that environmental design can have on the process of cancer prevention, diagnosis, treatment, and survivorship. Cancer is considered a chronic disease in the United States, and more than 1.6 million new cases are diagnosed annually. New strategies of cancer care propose patient-centered services to achieve the best outcome, and researchers have found that environmental design can be an important part of improving this care. Searches were conducted in the PubMed and Google Scholar databases as well as in specific healthcare design journals such as Health Environments Research & Design, Environmental Psychology, and Environment and Behavior. The criteria for articles included in the review were (a) English-language articles related to facility design, which addressed (b) the topics of built environment in relation to cancer diagnosis, treatment, and survivorship, and were (c) published in peer-reviewed journals between 2000 and 2017. Finally, 10 articles were selected, and the contents were analyzed. The selected articles demonstrate that environmental design is one of the critical factors for success throughout the whole continuum of cancer care from diagnosis to end-of-treatment. Some of the specific conclusions from the review are that “neighborhood-oriented” design strategies can be beneficial (by providing accessibility to all facilities along the patient’s path), that access to nature for patients, staff, and visitors alike is associated with better outcomes, and that provisions for natural lighting and noise reduction are associated with cancer patients’ well-being.
Cancer is one of the major concerns of society and cause of death in recent years (Berry & Mate, 2016; Gomez et al., 2015; Weiland et al., 2015). According to American Cancer Society (2016), 1.685 million Americans were diagnosed with cancer in 2016. Also, cancer prevalence and incidence rates are growing, and the problems and challenges associated with the high rate are increasing (Casarett et al., 2008). In spite of achievements in cancer diagnosis, treatment, and survivorship, it is still a heavy physical, emotional, and financial burden on patients and their families through the whole process (Casarett et al., 2008).
The cancer care continuum begins with prevention in society, which aims for reduction of risk and enhancement in cancer screening (Borosund, Ruland, Moore, & Estedt, 2014). Prevention has been the focus of many cancer models. Diagnosis is another step that can be combined with prevention and treatment processes. Survivorship is the last step in cancer care continuum and follows all other actions in cancer models. Cancer is entering an era of personalized medicine, which can lead to changes in the needs for the most appropriate future facilities (Borosund et al., 2014).
Berry, Wall, and Carbone (2006) categorized the perceptions of cancer services into three different groups: technical performance (functional clues), service provider behaviors’ and appearances (behavioral clues), and tangibles associated with service (mechanic clues). The whole cancer care continuum demands a sophisticated healthcare delivery system. This system encompasses various specialties, programs, faculties, supplies, and equipment (Wessels et al., 2010).
A subsequent amount of literature demonstrates that social and built environments impact the health of cancer patients (e.g., Gomez et al., 2015; Yen & Syme, 1999). The environment can be divided into social and physical dimensions (Yen & Syme, 1999). The social environment encompasses the groups that individuals belong to, the places they live, and policies of their lives. The built environment includes all the infrastructures around human beings, which can be divided into different scales from interior scale of the living to urban spaces (Bosch & Gharaveis, 2017; Lambert, Coad, Hicks, & Glacken, 2014; Peters & Verderber, 2017; Stern, MacRae, & Gerteis, 2003). It should be considered that physical and social environments are not segregated from each other, and any environment is the result of interaction between them (Yen & Syme, 1999).
Built environment design is a significant way to promote the patients and their families, staff, and society’s quality of life, which should be considered in the whole spectrum of cancer continuum. Advances in the service quality of cancer care are imperative (Berry & Mate, 2016). The service for cancer patients should be prepared by satisfying many factors including efficiency, patient and staff satisfaction, and customization (Berry & Mate, 2016; Casarett et al., 2008).
Built environment design is a significant way to promote the patients and their families, staff, and society’s quality of life, which should be considered in the whole spectrum of cancer continuum.
The need of different environments, to serve patients in different steps of cancer continuum, results in designing preventive, diagnostic, inpatient, outpatient, and urgent care facilities. These facilities are considered healthcare facilities and share many common principles with other inpatient and outpatient services. Healthcare environmental features can have notable effects on patients’ satisfaction, clinical outcomes, and well-being (Dijkstra, Conijn, & De Vries, 2006; Gharaveis, Shepley, & Gaines, 2016; Joseph & Rashid, 2007; Phelps et al., 2008; Ulrich, Berry, Quan, & Parish, 2010). Additionally, a systematic review by Ulrich and coauthors (2008) lists a range of general design considerations that can improve the chance of success in healthcare delivery including good acoustics, nature distractions, appropriate lighting, ergonomic design, family zone considerations, and improved floor layouts for staff.
The need of different environments, to serve patients in different steps of cancer continuum, results in designing preventive, diagnostic, inpatient, outpatient, and urgent care facilities.
Individuals who are categorized as having high risk of cancer or the patients who suffer from cancer may face specific challenges that may differentiate their needs (Weiland et al., 2015). Environmental design features for cancer facilities are listed within a different fashion including interior design elements (color, art, lighting, and furnishings), architectural design specifications (building design and layout), landscape design, and urban design factors (Berry & Bendapudi, 2003; Berry & Seltman, 2008; Shepley, Rybkowski, Aliber, & Lange, 2012; Ulrich et al., 2010; Wessels et al., 2010).These elements impact the healthcare delivery outcomes and convey many variables to promote the care delivery.
The changes in various cancer care models regarding healthcare delivery in patient-centered approaches, changes in technologies, which facilitate diagnosis and treatment, and improvements in resources lead to changes in trends for facility and space design. To understand the cancer care facilities’ special needs and explore design considerations, this systematic review was conducted. This article investigates the current state of knowledge regarding the impact of the built environment on cancer clinical treatment in healthcare facilities and warrants the implications for future design. This systematic review defines built environment as perceived and objective characteristics of physical surroundings in which human as users spend their time.
The changes in various cancer care models regarding healthcare delivery in patient-centered approaches, changes in technologies, which facilitate diagnosis and treatment, and improvements in resources lead to changes in trends for facility and space design.
Method
Identification of Literature
A systematic search of electronic databases was conducted in August 2017 to identify the most relevant studies focused on space and cancer care. The time span placed on this search was 2000–2017. The review of the literature failed to identify any systematic reviews on this topic. The search terms were finalized by team members before starting the process (Table 1).
The Search Terms in Order to Search for Related Studies.
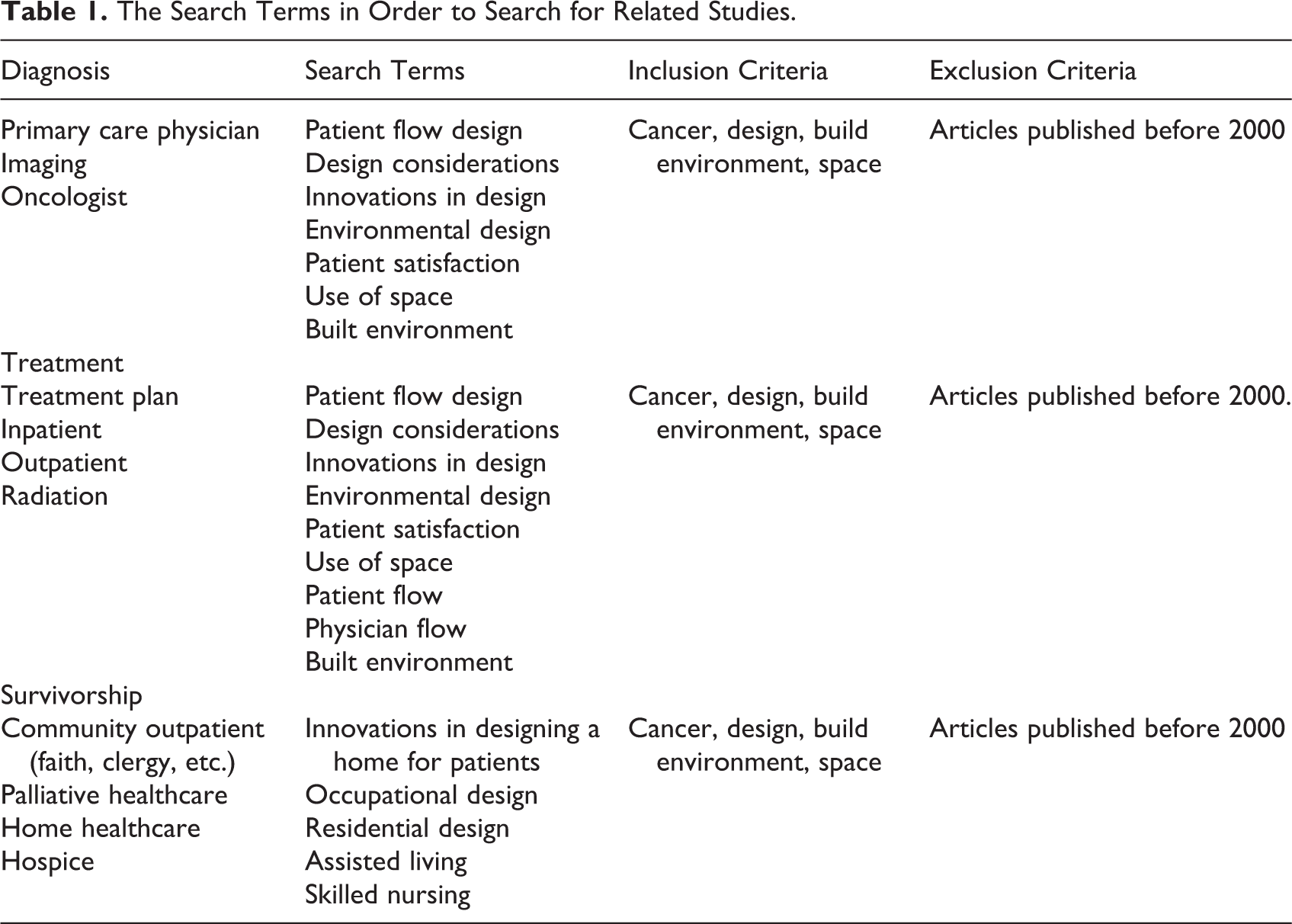
Google Scholar and PubMed databases and healthcare design journals including Health Environments Research & Design, Environmental Psychology, and Environment and Behavior were searched. Article search was limited to studies published in English. The sources provided related studies regarding cancer care from nursing, public health, psychology, and architecture disciplines.
Different combinations of search terms including patient flow design, design considerations, innovations in design, environmental design, patient satisfaction, use of space, patient flow, physician flow, built environment, and cancer were used to find the relevant and within reasonable limits peer-reviewed journal articles. The inclusion criteria were limited to design, build environment, and space.
Also, manual searches of mentioned journals were performed to identify the studies that were missed by the computer-assisted search. One of the team’s investigators reviewed all publication titles of citations identified by the search strategy. Potentially relevant articles were also selected for abstract review by one of the investigators of the research team, and the full articles were saved as the research team contemplated the relevance of the study to the research question. Sequentially, all the articles were manually and independently checked for inclusion criteria, and disagreements were resolved through consensus with the second investigator.
Inclusion Criteria
Inclusion criteria were the use of (a) primary studies (no secondary references) published in peer-reviewed journals (no anecdotal or opinion studies), (b) full-text English, (c) studies that were relevant to the healthcare setting with specific attention to cancer, and (d) research related to general environmental considerations and their impact on behavior. The relevance of the included studies was checked by the corresponding author, while the other author reviewed the final list.
This systematic review covered qualitative and quantitative studies without requiring the quantitative studies to be experimental. Also, there were no established appraisal tools used for the study. Since the sources of quantitative data were limited, statistical data analysis was not feasible to evaluate the findings. The studies that are incorporated in the final list were evaluated by the researchers to have acceptable method, measurement tools, research design, sampling strategy, and data analysis. The level of evidence of the final articles was graded based on the evaluating framework developed by Pati (2010). This evaluating tool categorizes articles into eight different levels in which one has the highest interval validity.
Data Extraction
The search results were transferred from databases to EndNote, and from EndNote, all the relevant information including titles, authors, purposes, methods, and findings of the studies were transferred to Excel. Analysis of the findings led to the latter step of the review, which was the full review of the related studies. Finally, 10 articles satisfied the criteria of the research (see Table 2), and the finalized studies’ references were explored to identify further relevant studies.
The Studies About the Impact of Environmental Design on Cancer Care.
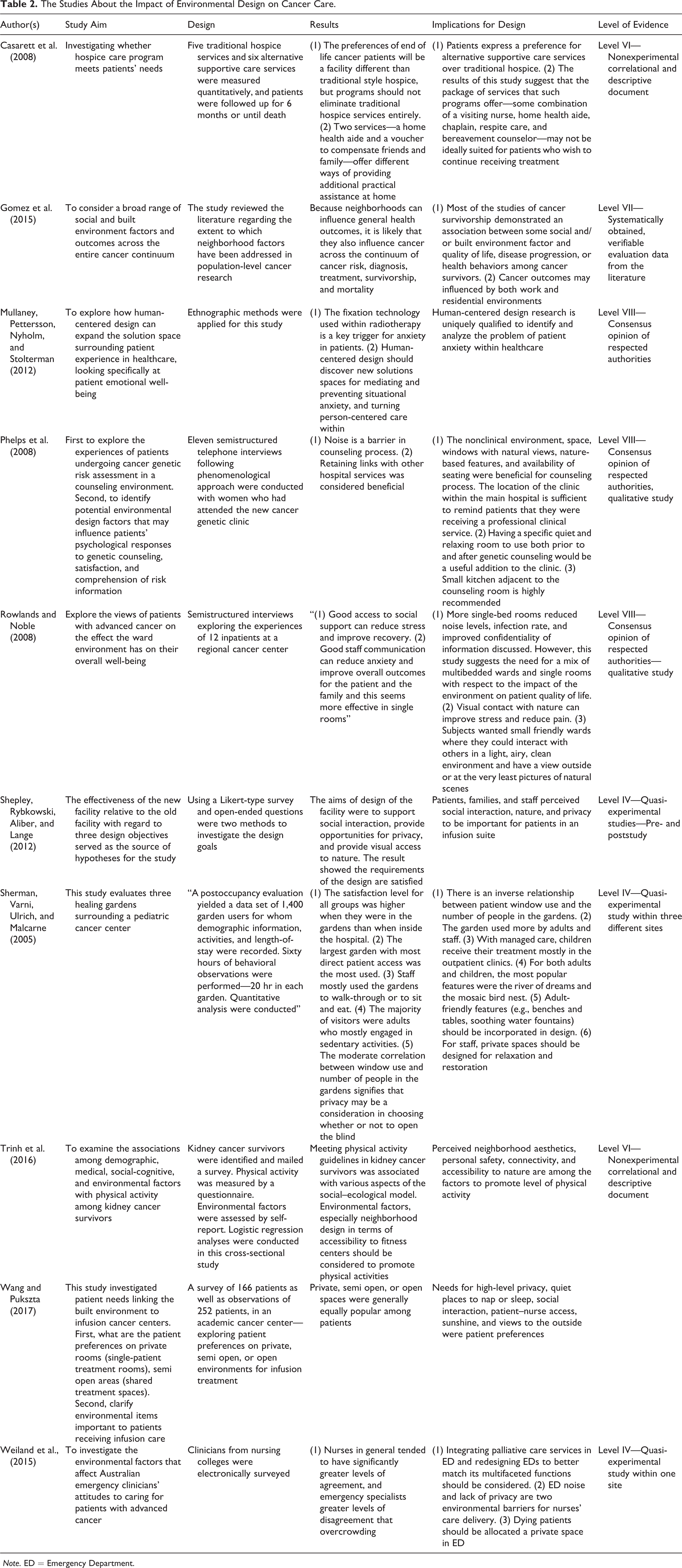
Note. ED = Emergency Department.
The included articles were reviewed by all of the team members for relevance. The content of the selected articles was analyzed by the researchers, and the specific aspects of design were coded in two steps and themes were generated, and related aspects of design were clustered together. The references of the final list articles were reviewed to explore additional sources. The final product of the review was drawn from the themes and presented as a narrative.
Results
Initially, 185 studies were found, and after the first round of review, 119 were selected for the second round of review, which included screening. In the third round, 32 studies were fully reviewed, and 10 articles were included in the final result of this systematic review published between 2005 and 2017 (see Figure 1).

Prisma 2009 flow diagram.
Table 2 outlines the finalized studies included in the review. One study was a review article and two of the studies used mixed methods. Three articles used qualitative and four performed quantitative data. Six of the studies were conducted in North America, three studies were published in Europe (two United Kingdom and one in Sweden), and one study was done in Australia. The final list included studies in which the environments regarding the whole spectrum of cancer care were explored, even though in some cases they were not the main focus.
Different themes emerged after the contents of selected studies were reviewed. The contents of the studies were focusing on general high-quality environment in different scales including neighborhood, healing landscape design considerations, and inpatient/outpatient facilities. Some interior design elements were also defined by this review in order to enhance the efficiency of buildings and productivity of the cancer models.
Theme 1: Neighborhood Design
Urban planning in general and neighborhood design in specific are the influential factors in individuals’ health directly and cancer care indirectly. The review results by Gomez et al. (2015) demonstrate that planning and design across the continuum of cancer mortality, risk, diagnosis, treatment, and survivorship would enhance the experiences of individuals and minimize the risks of cancer in society. Neighborhood social and environmental design considerations are not limited to residential buildings since neighborhood design of work environments is an influential factor in future developments.
According to the findings of Gomez and coauthors (2015), accessibility to different cancer facilities—which enhances convenience and minimizes expenses—is an important factor in the diagnosis of cancer, which may lead to prevention of late diagnosis and lower rate of mortality. Also, composition of neighborhood is another factor which is related to adjacencies of different functions. The risk of cancer can be lower in some neighborhoods considering activity level, housing/work environment quality, dietary habits, commuting characteristics, and market availability (Gomez et al., 2015).
Quality of life after diagnosis and cancer progression, which are parts of survivorship, can also be affected by neighborhood social and built environments. Wang and Pukszta (2017) referred to site planning and building orientation as important factors in providing appropriate window views and daylighting since open areas are more exposed to sun and view to outside. Wang and Pukszta (2017) identify site constraints as crucial factors in locating facilities and improvement of patients and staff experiences in cancer centers. In another study, Trinh and colleagues (2016) identify psychosocial, medical, and demographic variables as elements of physical activities of cancer survivors’ neighborhood design. This study determines the location of fitness centers, perceived neighborhood aesthetics, and the neighborhood’s safety as crucial neighborhood design (Trinh et al., 2016).
Theme 2: Accessibility to Healing Landscape
Accessibility to natural environments and gardens is a critical consideration in healthcare facilities to promote patient, visitor, and staff satisfaction. Staff and family members use the healing landscape more often than patients (Augustin, 2014; Marcus & Sachs, 2013). According to Sherman, Varni, Ulrich, and Malcarne (2005), the most popular features in cancer hospitals are benches, tables, water fountains, and paths to explore. Wang and Pukszta (2017) believe that patients’ accessibility to desired outdoor and natural environments during the treatment process enhances satisfaction and hope for future.
Sherman et al. (2005) found there is a reverse relationship between the number of people in the gardens and the usage of windows by patients. Additionally, private spaces that are segregated from patients and families should be designated for restoration and relaxation (Sherman, Varni, Ulrich, & Malcarne, 2005). In regard to the size of gardens, Sherman et al. mentioned the staff and patients use the larger gardens more frequently because bigger gardens provide different activities.
Theme 3: Inpatient Facilities
Design for cancer-related inpatient facilities is another focus of this literature review, which can be merged into general considerations for inpatient facilities. Similar to what has been discussed in regard to single-bed rooms in inpatient facilities (e.g., Ulrich et al., 2008), Rowlands and Noble (2008) found the similar preferences of cancer patients to reduce noise level, infection rate, and improvement in privacy and confidentiality. This study also suggested cancer patients’ visual contact with nature would alleviate pain and stress and the efficiency of small units in terms of social interaction because of their friendliness (Rowlands & Noble, 2008). Wang and Pukszta (2017) lists privacy, quiet places, accessibility to nurses, and view outside as crucial factors in design, which are adopted from the literature regarding inpatient facilities. The results of a study by Casarett and coauthors (2008) support the idea of having a package of services to offer a combination of traditional and innovative facilities. In this study, some of the cancer patients prefer to have different options of services including visiting nurse, home health aide, chaplain, respite care, bereavement counselor, and traditional hospice care (Casarett et al., 2008).
Theme 4: Outpatient Facilities
Most of the cancer treatment services can be provided in outpatient cancer centers. The recommendations and challenges of outpatient facilities are different than those of the inpatient cancer centers (Gharaveis, Hamilton, & Pati, 2017; Gharaveis, Hamilton, Pati, & Shepley, 2017). Wang and Pukszta (2017) address the significance of designing cancer outpatient facilities to provide a wide range of services for cancer patients who suffer from dramatic situations. Additionally, this study identifies the design of infusion centers, as they accommodate more than 50% of the chemotherapy treatments.
Shepley, Rybkowski, Aliber, and Lange (2012) investigated privacy, access to nature, and social interactions in infusion centers, which are regarded as outpatient facilities, by a pre- and postoccupancy evaluation study. The study addresses the crucial role of environmental psychology in cancer treatment because the patients with cancer are highly stressed. First, the findings support the idea that privacy is an important design factor in infusion centers. Second, staff–patient and patient–patient interactions are crucial in these units. The influential areas are the waiting and the café, and patients usually request a designated space for their interactions. Third, visibility from the nurse station to supervise patients and provision of spaces with more privacy in each unit have been addressed to be crucial.
Wang and Pukszta (2017) investigated some related research ideas. The need for privacy, quiet spaces for the sake of interaction or sleeping, patient–nurse accessibility and visibility, and view outside have been addressed by this research. The importance of visibility has been emphasized by Wang and Pukszta because of adverse consequences of some patients’ reactions to medications. Additionally, visibility in this study was mentioned as a design factor to enhance the patient’s sense of control, satisfaction, and comfort. Wang and Pukszta also explored the preferences for private versus semiprivate rooms and found private, semiopen, or open spaces are equally popular among patients. To describe the reason for not preferring private rooms, oncology patients described their wish to avoid isolation. Furthermore, this study found that window views and television provision would positively impact patients’ satisfaction (Wang & Pukszta, 2017).
Furthermore, specific design strategies should be regarded in outpatient facilities including nonclinical environments, natural views, accessibility of daylighting, and ergonomic considerations for well-located seats (Phelps et al., 2008; Wang & Pukszta, 2017). Phelps and coauthors (2008) also suggested locating counseling centers close to healthcare facility cancers, since adjacency bolsters the assumption of receiving professional healthcare services. Acoustic considerations for counseling purposes as well as relaxing environments are highly suggested by this study. A homelike environment that locates a kitchen next to the counseling area is convenient to improve user satisfaction (Phelps et al., 2008). Stressful devices should be limited in usage and ergonomic considerations should be improved in diagnosis and treatment stages for mediating and preventing anxiety (Mullaney, Pettersson, Nyholm & Stolterman, 2012; Wang & Pukszta, 2017).
Palliative care services should be integrated and multifaceted functions should be regarded in designing new emergency departments (Weiland et al., 2015). Weiland and coauthors (2015) also identifies noise and lack of privacy as environmental barriers for care delivery in emergency departments. Additionally, a specific and private space should be assigned for dying patients in emergency departments.
Discussion
The findings of this systematic review support the significance of environmental design to improve outcomes in patients, family, and staff. Design for cancer care requires specific considerations other than generic evidence about healthcare design while many studies warrant special aspects of design for cancer prevention, diagnosis, treatment, and survivorship. Design strategies cannot be limited to the application of ideas regarding inpatient and outpatient facilities and can be extended across the spectrum of the healthcare services. Some aspects of environmental design for cancer care have been explored by previous studies; however, there are some gaps to be addressed in the literature.
The findings of this systematic review support the significance of environmental design to improve outcomes in patients, family, and staff.
According to the findings of this systematic review, health-related strategies in designing neighborhoods should be regarded in new cancer care models for work and home environments. General policies in improvements of public health are applicable in design for cancer care models. Also, accessibility to healing landscapes is another way to promote the experiences of the patients, visitors, and staff, which associates with improvements in mood, satisfaction, and communication, while minimizing the stress level.
Regarding inpatient facilities, some ideas regarding the design of inpatient facilities are applicable, while specific aspects of cancer centers should be investigated separately. Reduction of background noise level, the chance of infection, and size of the unit have been addressed in the literature. Furthermore, this literature review found that enhancement of privacy, accessibility to nature, and view outside are crucial for inpatient cancer facilities.
Regarding inpatient facilities, some ideas regarding the design of inpatient facilities are applicable, while specific aspects of cancer centers should be investigated separately.
Cancer outpatient facilities and the needs of efficient center can be discussed more in future investigations. The current knowledge regards the infusion center as a type of outpatient facility, which can provide various services to patients who require chemotherapy. Privacy, accessibility to nature and daylighting, visibility from nurse station to the whole department, providing spaces for interactions and sleeping, and ergonomic chairs are highlighted in the studies to be influential in patient and staff comfort, sense of control, and satisfaction. For open versus semiopen environment, this review found that there is no-one-size-fits-all for the outpatient facilities, and a combination would be preferred for the cancer centers. Finally, future emergency department designers may consider having a palliative care section.
Limitations
This systematic review has limitations regarding the reviewed studies, search strategy design, and synthesis process. First, the final list of related studies only incorporates the documents related to cancer care environmental design, while another list could have been provided with respect to perception of cancer, challenges, and societal impacts from other disciplines’ perspectives. Additionally, the exact dates of the key word searches were not documented, which may hamper the replication of the systematic review to find more related studies in the future. Furthermore, the total number of experimental or randomly assigned studies has been limited, which makes the findings less comprehensive. This can be related to the limitation of the existing body of literature about the topic that has been explored by the current systematic review. Moreover, because the studies in the final list have not provided enough information, the statistics of different quantitative studies could not be pooled together to obtain a larger sample size and check the similarities of the findings. Finally, the search results were reviewed by two authors, while reviewing the materials by more researchers could have been reliable, because of the subjective nature of the inclusion and exclusion checking process.
Conclusion
Few high-quality studies have been published regarding environmental design considerations for cancer facilities in comparison with the depth of literature about cancer in different disciplines. This limited number of studies in the field of design can be related to the novelty of this field in healthcare delivery. This literature review warrants that in addition to the changes that are expected in technology, operational processes, and system-wide policies, designers and architects should provide the opportunities to transform the new models in cancer-related facilities.
The advancement of cancer prevention, diagnosis, treatment, and survivorship is only achievable by designing efficient facilities. Healthcare designers and planners should understand their crucial role in enhancement of patient experience, well-being, and quality of care through the whole design process.
Healthcare designers and planners should understand their crucial role in enhancement of patient experience, well-being, and quality of care through the whole design process.
Further rigorous research about environmental design considerations is required to compromise the future cancer models into design facilities. According to diversity in the nature of different cancer facilities, prevention, diagnosis, treatment, and survivorship, rigorous studies should be conducted to outline important design factors in each type. Current knowledge about inpatient and outpatient buildings and strategies about landscape and urban designing should be replicated for cancer-related facilities to clarify similarities and dissimilarities. A large body of existing literature may not be applicable for future developments because of the continuous changes in the field of cancer research.
Implications for Practice
This systematic review explored the current knowledge about the relationship between the design of the built environments and cancer clinical prevention, diagnosis, treatment, and survivorship in healthcare facilities by reviewing the relevant literature.
The main implications for practice: Environmental design is one of the critical factors for success of healthcare system regarding cancer care. “Neighborhood-oriented” design strategies can be beneficial by providing accessibility to diverse facilities in different neighborhoods. Providing access to nature and healing landscape would improve satisfaction and quality of life for patients, staff, and visitors. Spaces with natural lighting and controlled noise are associated with cancer patients’ well-being.
Footnotes
Acknowledgments
We would like to thank Mr. Mickey Heath, an adjunct professor at Southeast Missouri State University, for his sincere help and support in revising the writing of the article and would also like to extend my gratitude to Upali Nanda—the director of research at HKS Architects—and Dr. Bita Kash—an associate professor at Texas A&M University.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.