
Abstract
Objective:
This article presents a pilot study that employed a user-centered methodology for evaluating and quantifying neonatal intensive care unit (NICU) designs based on the needs of the primary users.
Background:
The design of NICUs has begun to shift from open-bay to single-family rooms. Both designs present unique advantages and challenges that impact babies, families, and caregivers.
Methods:
One NICU design was analyzed using the functional scenario (FS) analysis method. For the FS, users’ needs were determined through literature review, interviews with NICU providers and parents, and a review of published design guidelines. Quantitative metrics were developed for each FS, so that characteristics of the NICU design could be analyzed to determine how successful they were in meeting the users’ needs. The results were graphically represented to visualize the success and considerations of the design.
Results:
A total of 23 FSs and 61 spatial metrics were developed. FSs for babies focused on infection prevention, minimizing exposure to environmental stimuli, and supporting enriching care activities. FSs for family members focused on direct access to the baby, and privacy and adequate space for daily activities. FSs for providers and caregivers focused on infection prevention, care activities, care zones, and visibility.
Conclusion:
Using an FS approach highlights design characteristics in the NICU that need to be addressed during the design process to more successfully meet the needs of the different users. Additionally, using this approach can inform design professionals’ decision-making by presenting them with the design characteristics that impact the needs of the user groups.
Keywords
Neonatal intensive care unit (NICU) design is at a critical junction as facilities increasingly shift away from traditional open-bay (OB) units to single-family room (SFR) layouts. However, there is little guidance available to advise the design community on how to build better, safer NICUs and how to balance the needs of babies, families, and caregivers in a way that meets all of their needs. Within the NICU exist opportunities to improve outcomes through an environment optimized to support the developmental and social needs of babies and families. In this study, we describe a methodology for evaluating NICU design from the users’ perspective that is informed by published guidelines and recommendations and the needs of the three users: babies, families, and care providers. This article presents a method to evaluate NICU design as well as design principles for consideration during the design process.
Background of NICU Design
Medical advancements have improved survival rates for babies born at decreasing gestational ages. The median length of stay of approximately 80 days has been reported for babies under 28 weeks’ gestation (Lee, Bennett, Schulman, & Gould, 2013; Stoll et al., 2010). Emerging evidence suggests that these premature babies are at an increased risk of long-term developmental problems such as cognitive deficits and learning disabilities (Altimier, 2015; Lester et al., 2014). These babies also have an increased risk of developing healthcare-associated infections, which can lead to adverse outcomes such as longer length of stay or death (Hooven & Polin, 2014; Sohn et al., 2001; Squier, Yu, & Stout, 2000).
Babies born prematurely continue to develop outside of the womb, making the NICU environment a critical component in their neurodevelopment. Recognition of the importance of the NICU environment is evident in programs of care such as early developmental care, which encompasses components of care ranging from noise, light, and parental involvement to positioning and other patient care activities (Haumont, 2014). This holistic and comprehensive approach to care is defined by the Wee Care Neonatal Integrative Developmental Care model, which identifies seven core measures for neuroprotective family–centered developmental care (Altimier, Kenner, & Damus, 2015; Phillips, 2015). These care models emphasize the importance of the environment, family involvement, and clinical processes for providing the optimum care to babies in the NICU.
NICU Design and Patient Outcomes
There is a shift in NICU design from the traditional OB layout to SFRs, which has fueled a debate within the literature. While there are advantages and disadvantages to both designs, SFRs are increasingly emerging as the optimal design configuration for patient- and family-centered care (Stevens et al., 2012; White, 2003, 2011). There is growing evidence that suggests that SFRs are correlated with a shorter length of stay, less time on ventilators (Altimier, Eichel, Warner, Tedeschi, & Brown, 2004), fewer apnea events, and increased rates of breastfeeding at discharge (Domanico, Davis, Coleman, & Davis, 2011). Improved physiological measures are reported in SFRs (Domanico et al., 2011; Lester et al., 2014; Stevens et al., 2007). Reducing the risk of infection is of critical importance to this vulnerable population, and studies have reported decreased rates of sepsis in SFRs (Domanico et al., 2011; Lester et al., 2014).
An important advantage of SFRs is greater control over the environmental conditions in the space, which is critical in reducing potentially damaging indirect stimulation from other babies, caregivers, and families in the OB NICU. This includes excessive exposure to light and sounds to which the premature babies have been shown to exhibit hyperreactivity such as increased heart and respiratory rates (Peng et al., 2009). SFR NICUs environments are advantageous over OBs because they offer reduced noise levels compared to OBs (Domanico, Davis, Coleman, & Davis, 2010; Levy, Woolston, & Browne, 2003; Liu, 2012). While it is critical to minimize high-frequency detrimental noises, such as alarms, it is also important to avoid creating an environment devoid of quality sounds such as speech (Lahav & Skoe, 2013; McMahon, Wintermark, & Lahav, 2012). Emerging evidence suggests that exposure to language (i.e., parents speaking) correlates with higher language and cognitive scores at 7 and 18 months (Caskey, Stephens, Tucker, & Vohr, 2014). SFRs, which promote rooming in (i.e., parents sleeping/staying in the room with the baby) and increased contact between parents and babies, can create a supportive environment for these babies developing language needs.
NICU Design and Family Experience
The literature overwhelmingly supports that family satisfaction is greater in SFR units with dedicated family spaces (Carter, Carter, & Bennett, 2008; Domanico et al., 2010; Stevens, Helseth, Akram Khan, Munson, & Reid, 2011; Swanson, Peters, & Lee, 2013). Families are reported to spend more time in the patient room, take on a more proactive role in the baby’s care (Altimier et al., 2004; Wigert, Berg, & Hellström, 2010), mothers are more likely to breastfeed (Domanico et al., 2011), and length of stay is decreased (Örtenstrand et al., 2010). This could be due to the increased sense of privacy and dedicated family space of SFR units as Harris, Shepley, White, Kolberg, and Harrell (2006) found. Dedicated family space with privacy is critical to providing patient- and family-centered care, which encourages family members to be more present. The provision of a family area is especially important for the NICU population as families may live long distances from hospitals, making visitation more challenging.
NICU Design and Staff Satisfaction
While NICU SFR units are reported to support patient outcomes and family experience, there are controversial findings regarding staff members. The perception of social isolation and increased workload is reported in SFRs (Bosch, Bledsoe, & Jenzarli, 2012; Domanico et al., 2010; Smith, Schoenbeck, & Clayton, 2009; Stevens, Helseth, Akram Khan, Munson, & Smith, 2010). Nurses report concerns about their ability to respond quickly to emergent situations in SFR units. This concern may be unsubstantiated, however, as technologies such as cameras are introduced to permit caregivers to remotely monitor the babies’ conditions. In addition, increased family presence means that there are more eyes to notice a change in condition.
SFR units, compared to OB arrangements, have been reported to be associated with higher staff satisfaction and lower stress levels (Harris et al., 2006; Shepley, Harris, & White, 2008). Nurses in SFRs reported higher job satisfaction, lower levels of stress, and more positive environmental satisfaction and perception (Shepley et al., 2008). Measures of staff satisfaction are more variable when shifting from OB to SFRs. Improved staff satisfaction and perceived quality of work environment is frequently reported after shifting to SFR units (Bosch et al., 2012; Smith et al., 2009; Stevens et al., 2010). Negative staff perceptions when switching from OB to SFR are reported to improve with time.
Summary
NICU environments must be intentionally designed to support all of the users’ needs. Evidence strongly supports that SFR units are better for babies and for family-centered care. With dedicated family areas, families can remain more involved in care and feel more comfortable in the NICU environment. While measures of job satisfaction and quality of work environment can improve, the transition to the SFR model can be challenging for care providers. Through thoughtful considerations such as visibility within and across spaces, the role of technologies to facilitate patient monitoring, and the spaces within a unit to promote staff interaction, the design of a facility can minimize these challenges.
NICU Design Guidelines
The NICU environment poses particular design challenges, especially in situations where design guidelines and recommendations are found to be conflicting. In this study, three primary users and their respective spaces or zones within the NICU are defined: the babies, the families, and the healthcare providers. The two primary resources for NICU design guidelines and recommendations are the 2014 Facilities Guidelines Institute (FGI) and the Journal of Perinatology Recommended Standards for Newborn ICU Design, eighth edition (White, Smith, & Shepley, 2013).
The 2014 edition of the FGI outlines requirements for NICU design, organized by spaces or special design elements such as NICU rooms, support areas, aisles, or windows (The Facility Guidelines Institute, 2014). When these criteria are combined with the needs of the NICU babies, the providers, and the families, conflicts may arise. For example, FGI guidelines state that all patient care areas must have access to natural light (i.e., a window), but it is also necessary to minimize the baby’s excessive exposure to light. Window shades should be neutral or opaque, but providers must have the ability to darken the room for transillumination. In another example, privacy is an important element for the patient- and family-centered care, as reflected in the FGI guidelines, which state that infants and family members should have visual privacy. This presents a challenge from a safety perspective, however, when also attempting to provide visibility to the isolette (an incubator for babies that provides a controlled environment) from the nursing alcoves. These examples demonstrate conflicting guidelines and recommendations and the importance of considering the needs of the three user groups (babies, families, and healthcare providers) when developing a design concept. From the design and layout of a facility to the material selections, the NICU environment must support a range of requirements including safety, infection prevention, and the developmental needs of the infants.
While the FGI guidelines serve as the building requirements for NICU design, they lack sufficient detail to aid in many design decisions such as the rationale behind why a recommendation is being included. The Recommended Standards for Newborn ICU Design aim to address the gaps in guidance by providing interpretations of the standards, which include contextual information for why the design features are important (White et al., 2013). Many criteria, however, are general statements that can be difficult to measure and turn into actionable design solutions such as providing families privacy. Consequently, designers and decision makers have little guidance to determine best practices for NICU design or to understand the implications of design decisions. In order to bridge the knowledge gap between the clinical and the design disciplines, this project begins to address the needs of users in a clinical context and translate those needs into spatial metrics using a novel approach called Functional Scenarios (FSs; Hadi, Lim, Patterson, & Zimring, 2015). This approach quantifies spatial affordances of users’ needs within a determined context to inform designers. This is expected to help designers maximize the user experience in their design. The goal of this article is to analyze design features of an NICU that prevent or support users and to determine how to better meet users’ needs spatially by evaluating a specific NICU design. This serves as a proof of concept for our methodology for evaluating NICU design.
Method
NICU Design
An NICU design was selected for analysis as it represents a model for evidence-based design. Floor plans for analysis were provided as a Building Information Modeling (BIM) Revit file. The plans included the dimensions of the space as well as the materials and brands of the equipment in the space. This allowed the analysis to include measurements of sound quality and workflow and to take into consideration various configurations of the space. The scope of this spatial analysis was limited to within the NICU room. While there are critical activities, needs, and design attributes beyond the room, such as the relationships between rooms and other spaces such as nursing alcoves or nurse stations, this study focused on the design characteristics and user needs inside the room itself.
This study received exemption as nonhuman subjects research by the institutional review board.
Functional Scenario Analysis
This research uses a novel approach to understanding spatial needs and quantifying spatial affordances that we term FS analysis (Hadi et al., 2015). This method has significant potential to improve the user experience by evaluating and revising designs before construction (i.e., a preoccupancy evaluation). The FS analysis follows multiple steps: (1) state FSs representing needs of users, (2) define spatial metrics that support or hinder the needs of users, and (3) analyze the design with the spatial metrics. The steps of this method are further explained below. This article reports the analysis of one design as a proof of concept for evaluating NICU designs through the eyes of users.
Functional Scenarios
An FS defines the needs and activities of the users. Three primary user groups were determined in the NICU: babies, families, and caregivers. Each of these users has specific needs that the built environment should support including neurodevelopmental, psychosocial, and care activities. In some cases, these needs are in conflict with one another. FSs are written in the form of “user needs x.” The goal of the defined FS is not to cover all the possible needs that a user might have but to describe critical needs and are affected by spatial design of NICU SFRs.
Developing the FS requires an in-depth understanding of user needs and activities in the environment that is being analyzed. We developed a set of 23 FSs based on peer-reviewed literature, visits to NICUs around the United States, nurse and provider interviews, discussions with NICU design experts (including former NICU moms) and published guidelines, as well as experience and information gathered over the span of 5 years discussing the topic with nurses, providers, and design experts.
Spatial criteria and metrics
Once the needs were defined, criteria for measuring the success of a design characteristic were developed, which link the FS to the built environment (i.e., how well the design characteristic meets the need of the user). The FSs are the user needs that need to be met, whereas the criteria are the attributes of the environment that will be measured and the metrics are the characteristics/levels/amounts of the attribute that are being measured. The criterion for analysis is the attribute that will be measured (e.g., sound), and the metric is how to measure that attribute (e.g., decibels). Some of these criteria are included in the FGI guidelines, such as distance between the sink and the isolette to reduce splashing and potential infection risk, whereas others, such as privacy, needed measurement metrics to be developed, so that they could be measured in a quantitative and defined way. The FS were translated into spatial metrics using literature, guidelines, additional online research, and field knowledge.
Spatial analysis
Spatial metrics (e.g., distance, clearance, and visibility) were measured using AutoCAD 2016. Visual exposure and level of connectivity were measured using Depthmap, a stand-alone program performing visibility graph analysis (Turner, 2001, 2007). In addition to determining criteria and metrics, standards of measurement were determined to ensure interrater reliability and consistent analyses when used across multiple designs. The NICU floor plan was analyzed based on the defined criteria and metrics. The results of the analysis were also visualized graphically for clarity and ease of understanding, so that the results may be useful to those outside of architectural backgrounds.
Results
FSs were developed for each of the three user groups: 6 scenarios for babies, 6 for families, and 11 for providers and caregivers (Table 1). The FSs presented in this article represent a selection of user needs within the patient room. Each FS was measured using multiple spatial criteria to determine the design’s ability to meet the needs described in each FS: 13 criteria were determined for babies, 19 for families, and 29 criteria for providers. These criteria provide practical mechanisms for evaluating design components and spatial affordance. In the following sections, we discuss eight FSs that illustrate methods for evaluating how well the design meets the users’ needs.
Functional Scenarios From the Perspectives of Babies, Family, and Providers/Caregivers.
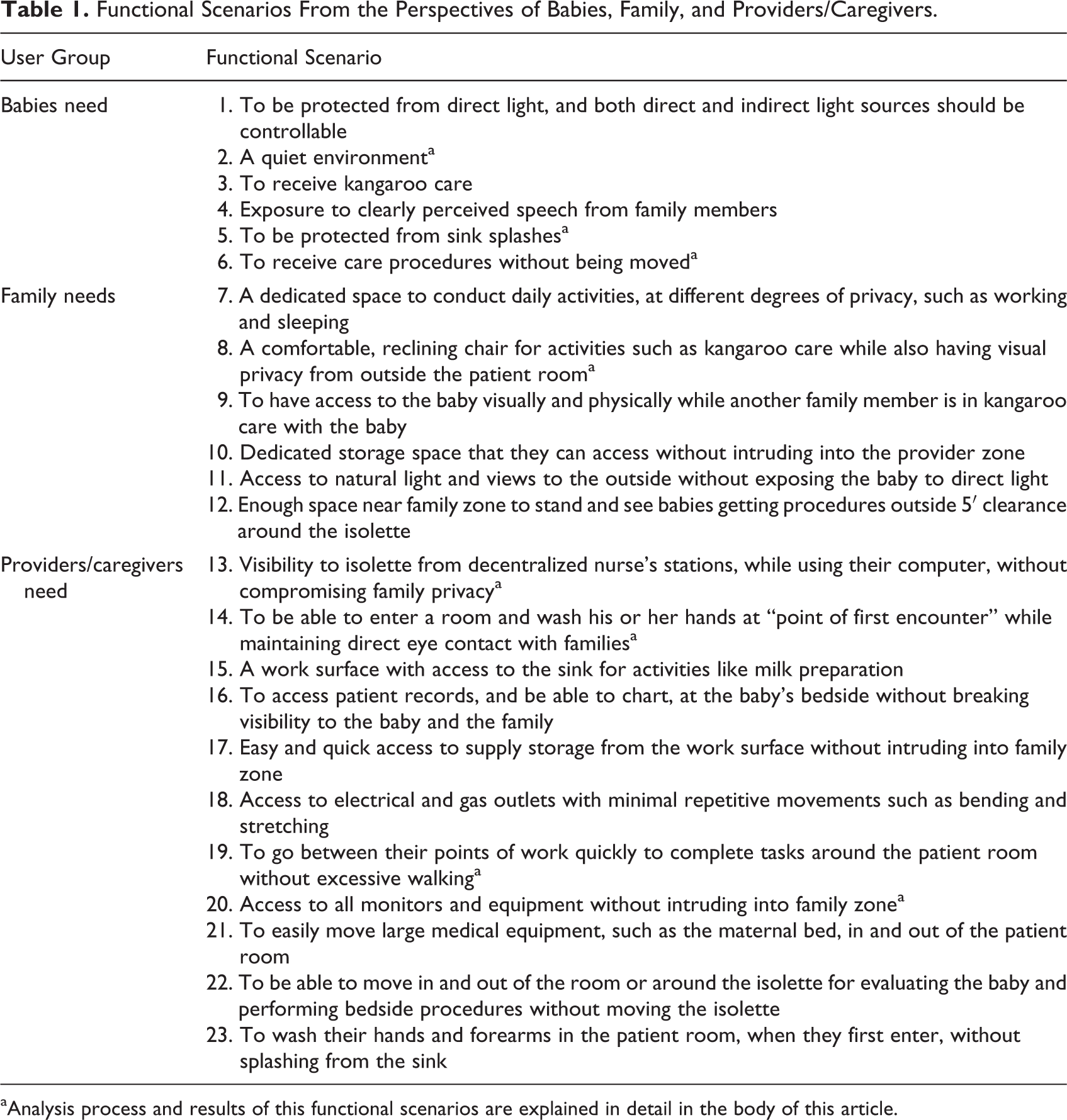
aAnalysis process and results of this functional scenarios are explained in detail in the body of this article.
Babies’ Needs
FSs for babies focus on three primary needs: (1) infection prevention, (2) minimizing exposure to environmental stimuli, and (3) supporting enriching care activities.
Infection prevention
For babies’ safety, infection control is a critical issue, and sinks can be main sources of infection (Squier et al., 2000). Therefore, babies need to be protected from sink splashes (one FS for babies). This can be spatially supported by controlling for the distance between the sink and the isolette. White, Smith, and Shepley (2013) stated that handwashing sink should be no closer than 3′ to the isolette, and this study adopted 3′ as a minimum distance between the sink and the isolette. The exact distance between two can be measured by calculating the distance from the faucet to the closest edge of the isolette. In the design that was evaluated in this study, the distance was 7′ and 8″ (Figure 1).
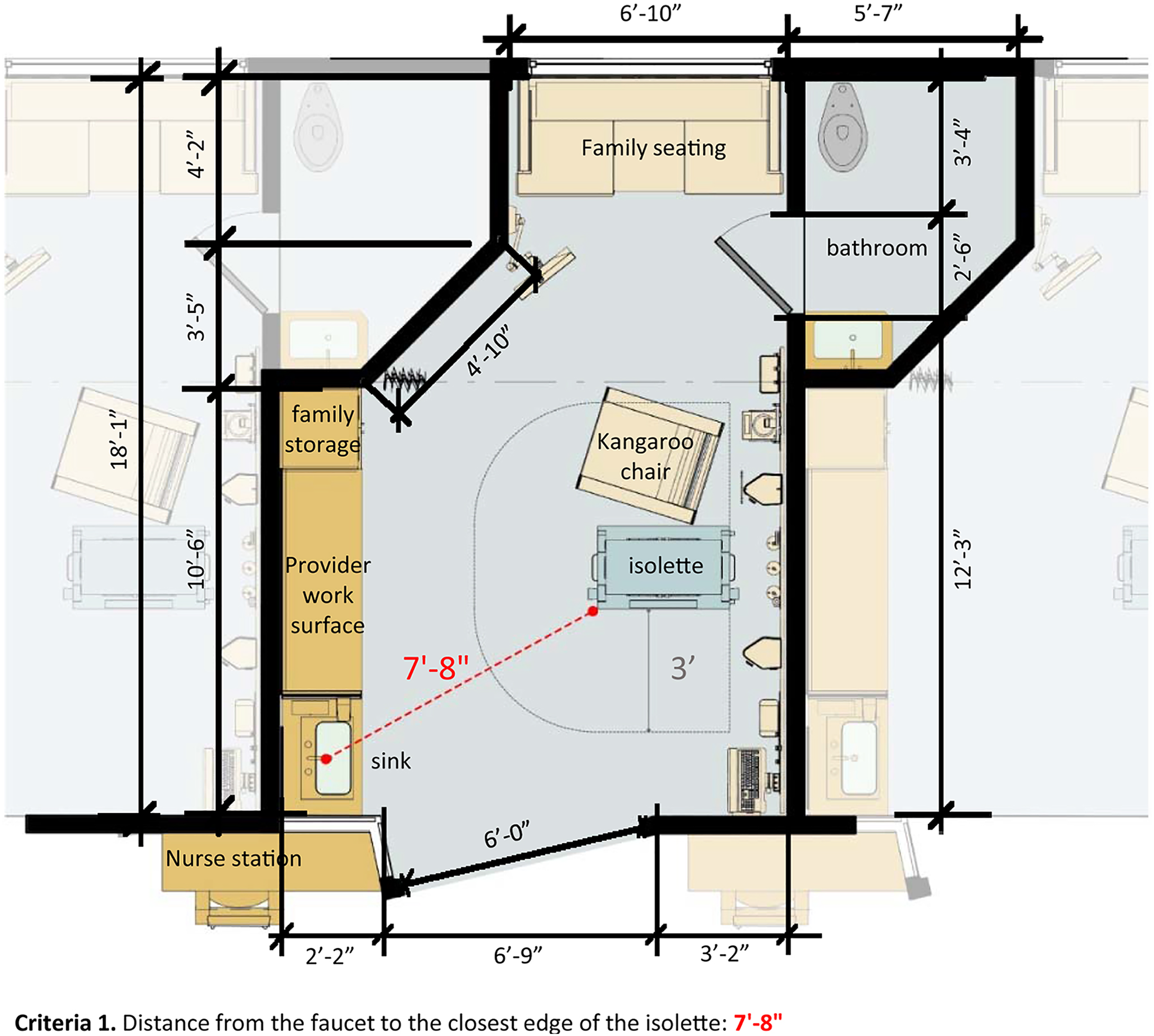
Babies need to be protected from sink splashes.
Minimize exposure to stimuli
As mentioned previously, babies need to be protected from environmental stimuli including light and noise. Figure 2 demonstrates how the abstract concept of a babies’ FS (needing a quiet environment) can be measured and rated using the established criteria and metrics. By providing the sound transmission coefficient (STC) ratings for various materials used within a space, designs can be directly compared to each other and evaluated. The NICU design in this study included the specifications for the wall and flooring materials that had high STC scores, which is optimal for the acoustic environment. Babies need a quiet environment.
Support care activities
FSs can also be used to measure how the space supports required care activities. It is undesirable for infants to be moved while receiving care. Sufficient clearance area around isolette where care activities can occur must be provided in order to avoid moving the infants. However, since there are no clearly stated measurements for the clearance area in existing guidelines, it was necessary to determine how much space was required during bedside procedures (Figure 3). Through interviews with NICU nurses and a review of NICU literature, it was estimated that approximately seven providers and caregivers would be present at the bedside during these procedures. Based on Edward Hall’s theory of Proxemics (Hall et al., 1968), 18 in. of personal space was allotted for each team member, and additional space was allotted for several pieces of equipment that were needed. This resulted in a 4-foot zone around the isolette.
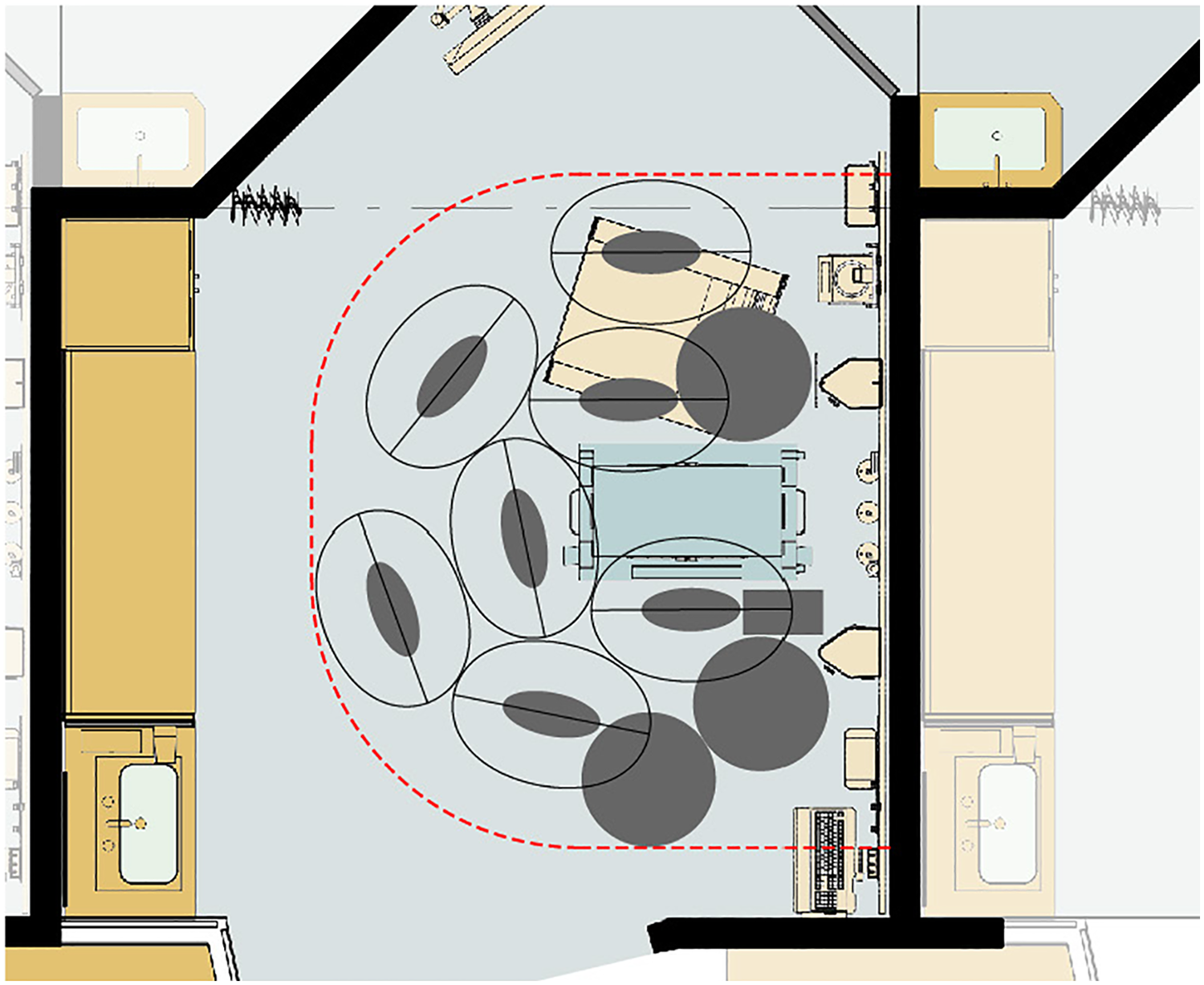
Isolette clearance. At least 4′ clearance is needed for seven care staff with 9″ oval around the person for personal space between people (providing 18″ personal distance) and equipment (a ventilator, three rolling stands for mounted IV pumps, a monitor, and a blender).
Based on this 4-foot clearance area around isolette, the room could be evaluated as to whether the design was adequate in accommodating babies’ need to receive care procedures without being moved (Figure 4). Criteria 1 for this FS measures how much of this 4-foot area is obstructed around the isolette. In the design that was analyzed for this study, providers were able to access the isolette without any obstructions.
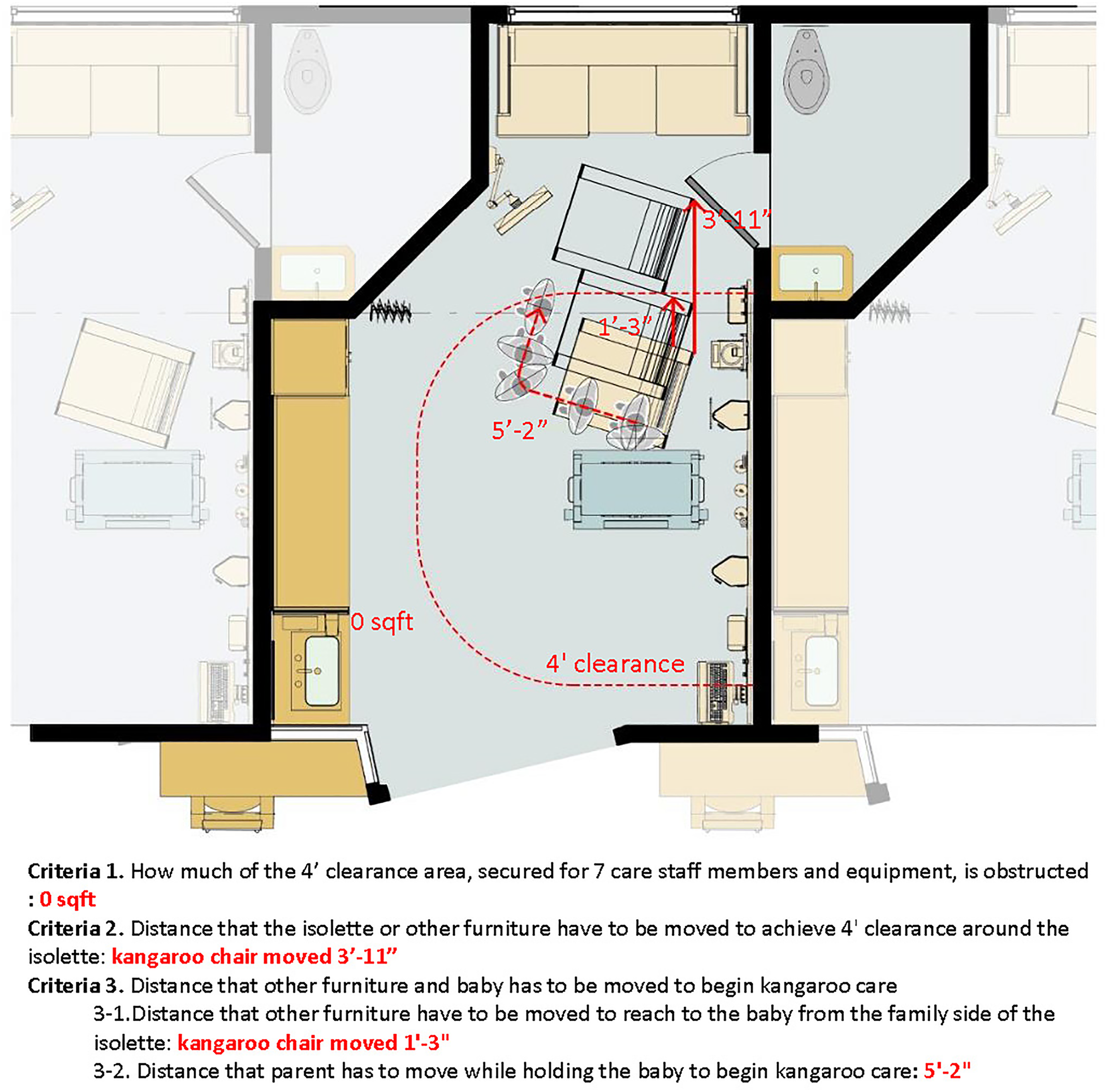
Babies need to receive care procedures without being moved.
Kangaroo care is increasingly recognized as a critical care activity and has been linked to better outcomes of babies (Feldman & Eidelman, 2003; Johnston et al., 2003; Ramanathan, Paul, Deorari, Taneja, & George, 2001). This care requires that parents spend as much time as possible with their baby on their chest with skin-to-skin contact. A reclining chair, commonly referred to as a kangaroo chair, provides a comfortable space for this kangaroo care. The kangaroo chair presented a challenge in this analysis as the chair was frequently in the way when analyzing the design using the FSs. The kangaroo chair is an essential piece of equipment in the NICU for kangaroo care, and yet it is frequently neglected during planning. These chairs tend to be bulky, but care teams must be able to shove them out of the way in urgent situations. Figure 4 shows how far the kangaroo chair must be moved, determines whether there is adequate space to move it out of the way, and how far away from the baby this subsequently puts the family.
Family Needs
Parents in NICU are subject to significant stress and mental illness, which in turn can be detrimental to their babies (Hall, Phillips, & Hynan, 2016). In order to promote family presence and their bond with the baby, the family zone must be a supportive environment for family needs. Family members should have (1) direct access to the baby and (2) privacy and adequate space for daily activities (i.e., sleeping and working).
Access to the baby and privacy
The FS pertaining to kangaroo care describes two needs of family members: access to the baby and privacy. Figure 5 illustrates the family’s need for a comfortable, reclining chair for activities such as kangaroo care, while also having visual privacy from outside the patient room. Since kangaroo care requires skin-to-skin contact, visual exposure from the outside is not desirable for the family members during this activity. The design evaluated in this study has a kangaroo chair present with space for the chair to recline with minimal adjustment. In addition, this design provides visual privacy from outside of the room while seated due to the location of the isolette. This example implies that in addition to including the kangaroo chair in the NICU, the location of the chair, clearance around the chair to recline, and the visual exposure level of the chair should all be considered when designing the NICU.
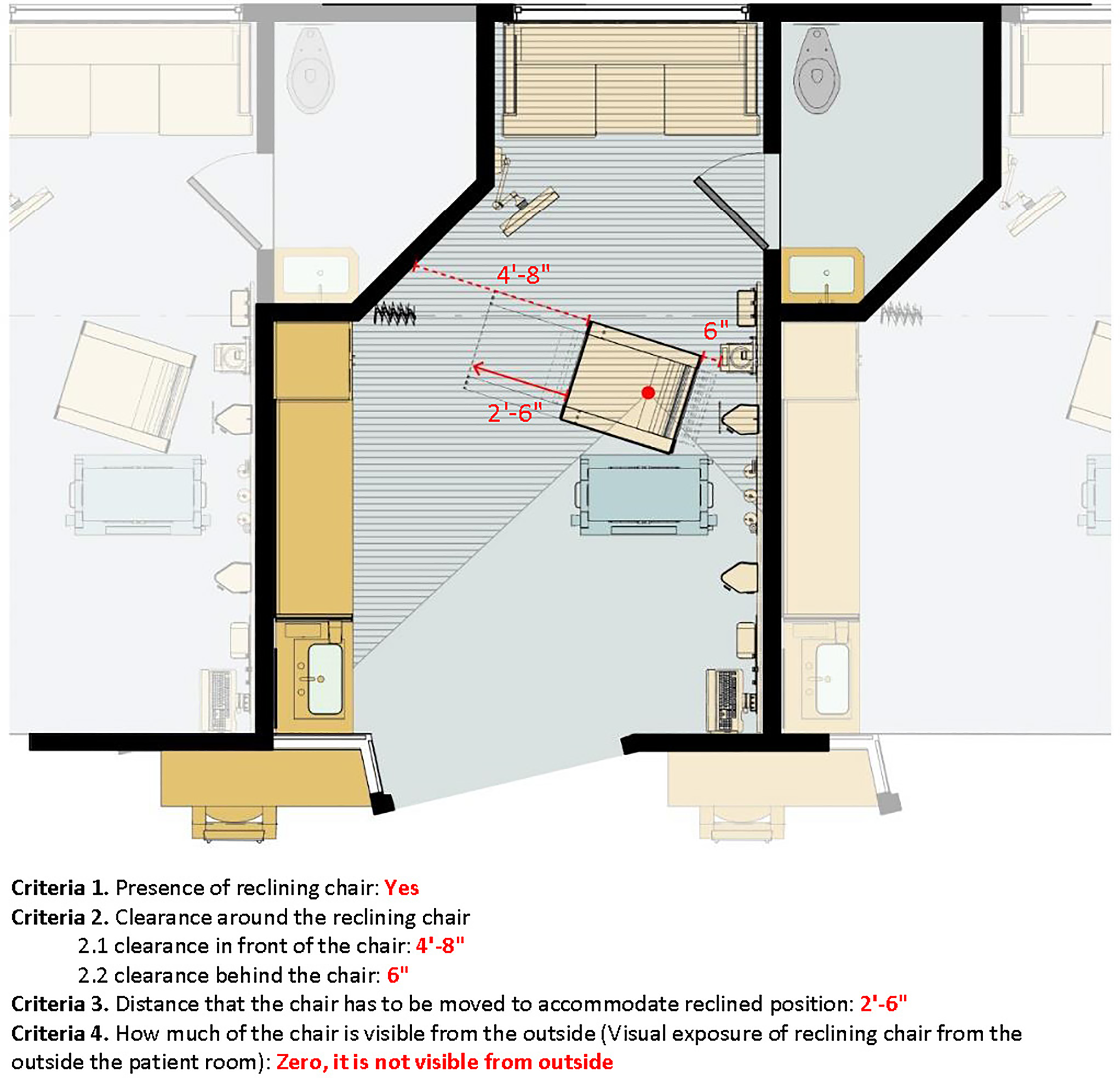
Family needs kangaroo chair with visual privacy.
Provider and Caregiver Needs
The NICU environment can facilitate patient care by supporting the needs of the care teams. These are described by the 11 FSs in Table 1 and include (1) infection prevention, (2) care activities, (3) care zones, and (4) visibility.
Infection prevention
Hand hygiene is the first line of defense against the spread of infection through contact. A common strategy for improving hand hygiene compliance through choice architecture is to include a sink at the entrance of the room to be accessible (Squier et al., 2000). One of the provider and caregivers’ FSs addresses an additional consideration for this design component, which is that the providers and caregivers should be able to maintain eye contact with families while washing their hands. Figure 6 shows the criteria for determining whether the provider can see the sink and the isolette at the point of entry, the distance to the sink from the point of entry, and how much the caregiver needs to turn in order to see the family while at the sink. While this might seem inconsequential, the degree that the care provider needs to turn is a way to quantify visual contact and the degree to which contact is broken.

Providers/caregivers’ ability to maintain eye contact at sink.
Support care activities
Room layout can greatly impact provider and staff’s ability to perform the functions of their jobs efficiently and safely. In order to evaluate the workflow pattern for this FS, we summed the distance between the primary touchpoints: the isolette, sink, work surface, computer monitor, headwall, and door (Figure 7). This approach takes into consideration every possible travel path by the provider/caregiver since workflow can be highly variable based on the tasks being performed. The summed distance and the shape of all connecting lines represent the possibility of working effectively with minimal walking, and it measures any intrusions into the family members’ zone. This pattern would be very different in a design in which these key touchpoints were at a greater distance from each other.
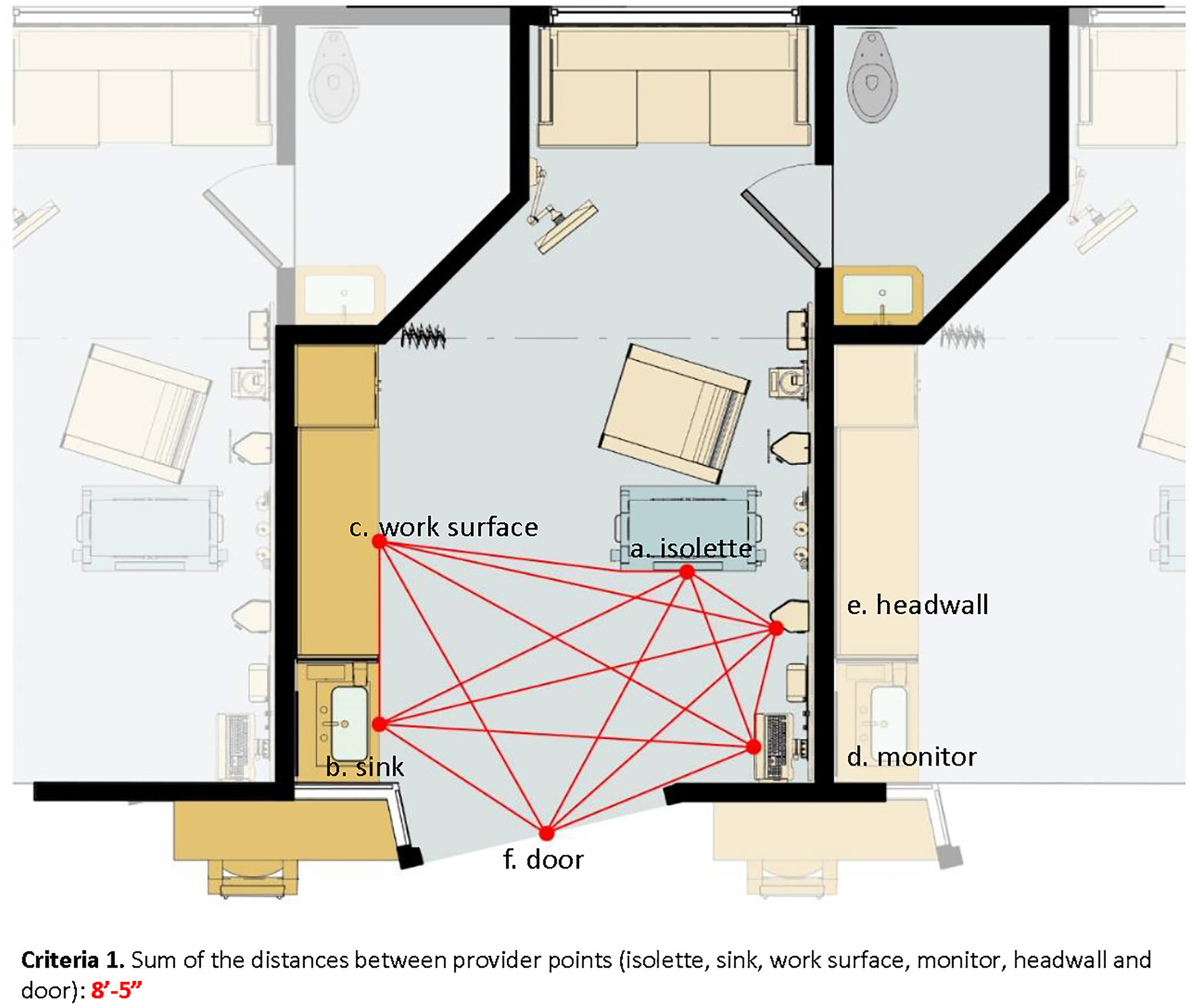
Providers/caregivers’ workflow pattern.
Care zone
This NICU design incorporates the concept of zones; the family zone and the provider zone are distinct and separate. Figure 8 depicts the integration of workflow and work zone for caregivers and shows that in this layout, there is very little intrusion into the family zone. This FS analysis also takes into consideration the area in which the two zones overlap one another. This approach allowed us to measure how much of the family/provider zone may be intruded into.
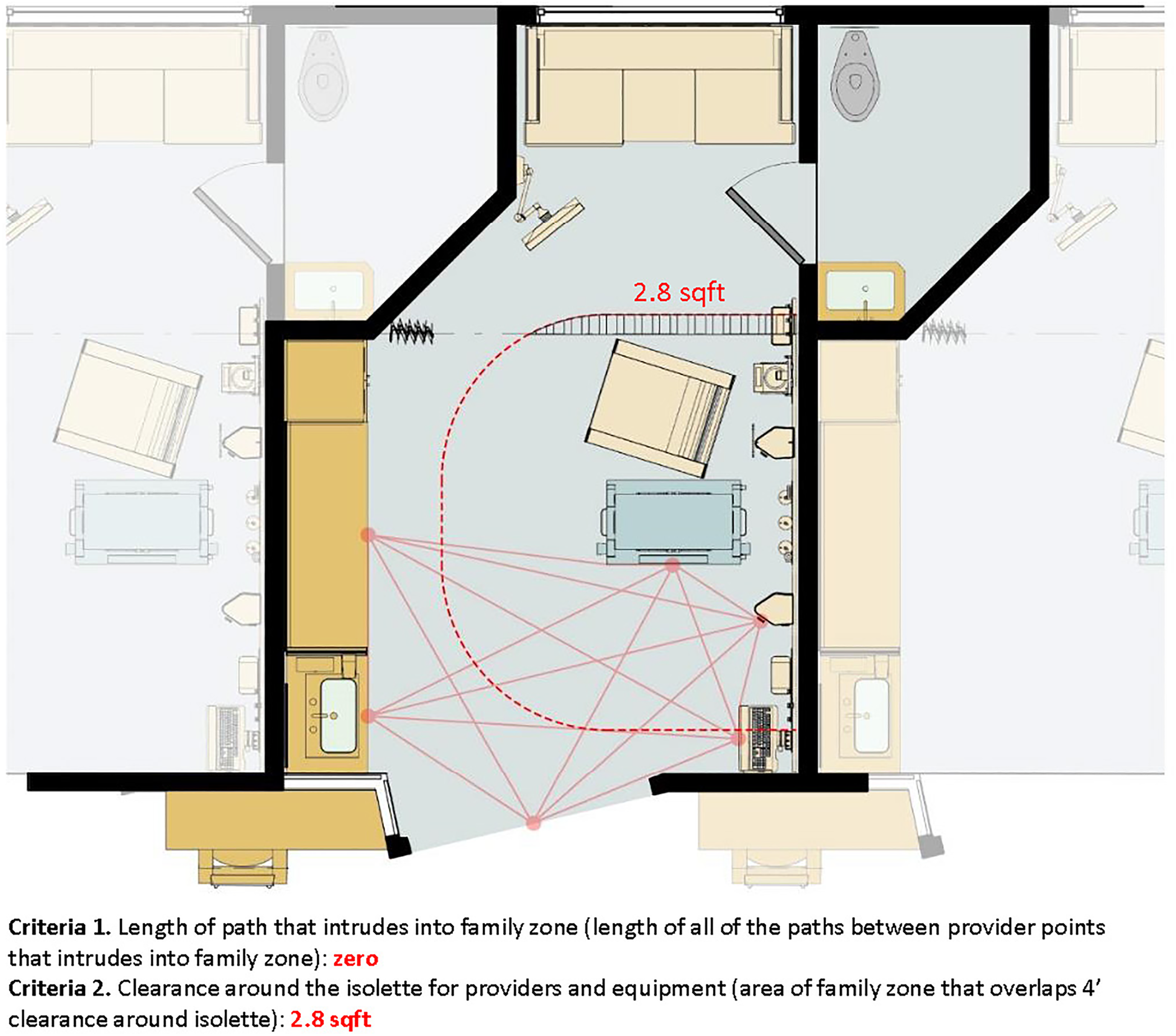
Providers/caregivers’ zone.
Visibility of patients
Providers and caregivers need to have visibility of their patients from outside the NICU room in order to respond to any needs of the babies. However, the caregiver’s need for visibility and the family’s need for privacy can be challenging and in fact conflicting. Figure 9 depicts the visibility from the nurse alcove to the isolette and to the family area. While the nurse has 100% visibility to the isolette in this design, Figure 5 shows that the family maintains visual privacy from outside of the door.

Providers/caregivers’ ability to monitor the baby.
While this floor plan provides 100% visibility from the nurse station that is located outside the unit, it should be noted that this floor plan features a same-handed room design that limits the visibility from the alcove to only one room (the room analyzed in this study). In NICU settings where nurses are responsible for multiple babies, this layout would impede the visibility to a second room.
Discussion
The NICU environment is a critical factor for the short- and long-term outcomes of premature babies. NICUs should be designed to support the needs of all users including babies, families, and care providers. This article evaluated an NICU design using the FS analysis approach. It presented a list of FSs from the perspectives of babies, family members, and providers/caregivers. Spatial affordance for each FS was quantitatively measured and analyzed using one NICU design. The list of FSs and examples of spatial metrics and the results are expected to expand the understanding of the spatial needs of the actual users of an NICU and to inform future design of NICUs.
In the process of determining the criteria and the metrics, it was useful to examine design guidelines and standards as examples of how needs are met spatially. When an FS describes a need for performing an activity, the guidelines can be used for baseline measures or threshold limits for spatial metrics. More strictly defined metrics are preferable for the outcome of the FS methodology because they eliminate opportunities for misalignment and create standardization.
The NICU design that was analyzed for this project was developed by experts in the field of evidence-informed design, patient- and family-centered design, and NICU developmental care. It was intentionally designed to meet the needs of the three primary user groups. As such, it performed extremely well on most of the FS criteria. This floor plan was selected in part for that reason—it was designed to represent best practices in NICU design. In reality, hospitals are faced with constraints, such as space availability and cost, which could force compromises on some of the design recommendations. By applying the FS criteria to additional NICU designs, we can begin to understand the consequences of these design decisions.
Multidisciplinary teams are increasingly recognized as essential components of evidence-informed design, but effective communication among these teams can be challenging. One strategy to overcome these barriers is to translate outcomes visually into graphics to inform decision makers who do not have backgrounds in architecture or design. Conversely, the FS methodology provides the contextual information and rationale behind user needs that can help design teams understand the implications of their design decisions. The FS and design criteria developed in this project can be used to inform design by helping to understand the needs and potential trade-offs of design decisions.
Limitations
In this pilot study, only one floor plan was analyzed. This served as proof of concept for the FS methodology for evaluating NICU design. The list of FSs presented in this article represents a sample selection of the FSs developed in this pilot study. In order to extract design criteria that will be useful in informing designers on how to best meet users’ needs, multiple designs adopting different design strategies must be analyzed in the future research using the same set of FS, criteria, and metrics that are then compared. The analysis and comparison of multiple NICUs will enable us to understand variability of design properties and the effects of those elements on FS. Comparing the results of multiple analyses will shed light on how design characteristics affect one another and play a role in meeting the needs of users.
This study focused on the design of NICU room itself. As a result, there are some critical user needs that this study did not include such as staff members’ need to take adequate breaks, exposure to daylight, visibility to rooms from the nurse’s workstations, family members’ ability to interact with other family members, and so on. The study focused on the inside of an SFR. Future research exploring a broader range of spaces (including relationships between rooms and other spaces in the ward) and capturing critical needs of users beyond the room would provide a holistic picture of NICU design for better user experience.
Implications for Practice
Researchers can apply the FS analysis method on various architectural settings. Designers of healthcare settings can use this approach to assess the functional success or limitations of their designs iteratively to arrive at a design that supports its user groups. By representing the results of the analyses visually, the implications of the NICU design can be more effectively communicated across disciplines. Designers may more easily understand how design recommendations and decisions impact affordances offered to users of spaces. Similarly, caregivers and healthcare providers may more easily understand the spaces proposed by designers. Design guidelines for healthcare settings can be determined based on use scenarios and can include explanations for why a specific spatial threshold is being presented. Published design guidelines can be revisited and tested in tandem to highlight contradictions and misalignments that need to be addressed. This can serve as a bridge for medical professionals and designers in order to facilitate an understanding of each other’s perspective.
Footnotes
Acknowledgment
The authors would like to thank Tammy Thompson and the Institute for Patient-Centered Design, with help from subject matter expert Mardelle McCuskey Shepley, FAIA, DArch Professor, Cornell University, for cooperation in permitting the use of their neonatal intensive care unit design for this analysis. They would also like to thank Craig Zimring and Jennifer DuBose of the SimTigrate Design Lab for their support.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the College of Design at the Georgia Institute of Technology.