
Abstract
Objective:
To assess the feasibility of quantifying variation in childbirth facility design and explore the implications for childbirth service delivery across the United States.
Background:
Design has been shown to impact quality of care in childbirth. However, most prior studies use qualitative data to examine associations between the design of patient rooms and patient experience. There has been limited exploration of measures of unit design and its impact on care provision.
Method:
We recruited 12 childbirth facilities that were diverse with regard to facility type, location, delivery volume, cesarean delivery rate, and practice model. Each facility provided annotated floor plans and participated in a site visit or telephone interview to provide information on their design and clinical practices. These data were analyzed with self-reported primary cesarean delivery rates to assess associations between design and care delivery.
Results:
We observed wide variation in childbirth unit design. Deliveries per labor room per year ranged from 75 to 479. The ratio of operating rooms to labor rooms ranged from 1:1 to 1:9. The average distance between labor rooms and workstations ranged from 23 to 114 ft, and the maximum distance between labor rooms ranged from 9 to 242 ft. More deliveries per room, fewer labor rooms per operating room, and longer distances between spaces were all associated with higher primary cesarean delivery rates.
Conclusions:
Clinically relevant differences in design can be feasibly measured across diverse childbirth facilities. The design of these facilities may not be optimally matched to service delivery needs.
Keywords
Across diverse clinical settings, facility design has been shown to impact patient safety, patient satisfaction, staff effectiveness, and overall care quality (Ulrich, Quan, Systems, Architecture, & Texas, 2004; Ulrich et al., 2008). While these impacts occur at multiple scales ranging from the patient room to the full facility, most prior research in childbirth has focused at the room scale (Aburas, Pati, Casanova, & Adams, 2017; Davis Harte, Sheehan, Stewart, Foureur, & Dip Clin Epi, 2016; Hauck, Rivers, & Doherty, 2008; Hodnett, Stremler, Weston, & McKeever, 2009). Research is lacking on how the design of the full clinical unit or facility impacts the way childbirth care is provided. For example, Birth Unit Design Spatial Evaluation Tool provides insights into the impact of design on fear, facility characteristics, aesthetics, and support for birthing individuals but does not attend to the impact of design on clinical decisions (Foureur, Leap, Davis, Forbes, & Homer, 2011; Sheehy, Foureur, Catling-Paull, & Homer, 2011).
Nonetheless, in other clinical domains, the unit scale appears to provide a compelling opportunity to understand the link between design and clinician workflows, experiences, and satisfaction (Foureur et al., 2010; Symon, Paul, Butchart, Carr, & Dugard, 2008a, 2008b). In a pediatric ambulatory surgery center, optimizing design to improve patient flow resulted in decreased nonoperative time in the operating rooms by 50%, surgical procedure time by 26–43%, and postanesthesia care unit time by 38–68% depending on the procedure (Pelly, Zeallear, Reed, & Martin, 2013).
In the United States, service provision and quality of care in childbirth varies considerably at the clinical unit level. Cesarean deliveries are one indicator of this variation. Cesarean delivery rates vary from 7% to 70% across hospitals, independent of patient preferences, sociodemographics, and comorbidities, indicating that characteristics of the facility where a woman delivers may be her greatest risk factor for cesarean delivery (Cáceres et al., 2013; Kozhimannil et al., 2014; Kozhimannil, Law, & Virnig, 2013). These characteristics could include the culture, management processes, and design structures of the facility upstream of the outcomes of care (Donabedian, 1988; Plough et al., 2017). Moreover, almost a third of all babies born in the United States are currently delivered via cesareans, far exceeding the World Health Organization recommendation of 10–15% (Martin, Hamilton, Osterman, Driscoll, & Drake, 2016; World Health Organization, 2015). The decision to perform a cesarean delivery requires complex analyses of time trends and clinical discretion that can make individual cases unclear in the moment, but at a population level, approximately half of these surgeries may be unnecessary in hindsight (Witt et al., 2014). These unnecessary surgeries can lead to substantial avoidable clinical and financial harm (Deneux-Tharaux, Carmona, Bouvier-Colle, & Bréart, 2006; Liu et al., 2007; Truven Health Analytics, 2013).
In a 1-year exploratory study, we aimed to develop and test a scalable method of collecting quantitative and qualitative design data at the unit or facility scale and to generate hypotheses about the impact of design on facility-level variation in low-risk cesarean delivery rates. We predicted that differences in facility design may not be related to differences in patient risk factors or needs; therefore, we hypothesized that some of the variability in design may contribute to unnecessarily high cesarean delivery rates among low-risk women.
Method
Facility Selection
We identified potential facilities through a request for participation posted online and promoted via social media from December 2015 to January 2016. We received 63 responses from patients, clinicians, facility managers, and architects describing facilities with design strengths or weaknesses. We also considered facilities with existing relationships with the study team for inclusion. From the full set of 118 potential facilities, we selected three birth centers and nine hospitals to optimize our sample for diversity with regard to facility type, location, delivery volume, low-risk cesarean delivery rate, and practice model. All enrolled facilities signed participation agreements consenting to participation requirements and privacy protections for all the facilities and individual interviewees.
Design Element Selection
We used the pressure tank model to provide a theoretical framework for how the environment of the clinical unit may impact the decision to perform a cesarean. In this model, three types of factors can influence clinical decisions: (1) limited unit or facility capacity, (2) high workload, or (3) limited accountability for decision-making (Figure 1). Cesarean deliveries require less time and resources from the labor and delivery unit than vaginal deliveries; therefore, clinicians could theoretically use cesarean deliveries to increase the pace of patient throughput, freeing labor and delivery unit resources, and reducing their workload, in the absence of accountability for decision-making. The study team conducted a literature review to identify design elements that may impact processes and outcomes of childbirth care and categorized these elements based on the three dimensions of the pressure tank model. We also identified additional design elements that may impact the context or culture of care at childbirth facilities but did not fit clearly within any of the dimensions.

Pressure tank model.
We convened a 10-member expert advisory board, including key stakeholders and thought leaders in clinical obstetrics (obstetricians, nurses, and midwives), patient advocacy, facility management, health services research, architecture, and evidence-based design, to guide the development and execution of the project. Since many board members had multiple areas of expertise, we had one to three representatives from each discipline. The board members supplemented and confirmed the importance of design elements identified in the literature review and participated in a modified-Delphi consensus process to prioritize among the design elements. Before the meeting, board members completed a survey rating the relative impact of design elements on clinical decision-making during childbirth care and shared hypotheses on the mechanisms behind these relationships. During the in-person meeting, we presented the survey results to the board members and then moderated a discussion to explore areas of disagreement. Following the meeting, the board members repeated the same survey incorporating new perspectives raised by the interdisciplinary meeting discussion. The study team synthesized results from the two surveys and the meeting discussion to select the final list of design elements to measure and analyze across the 12 facilities (Table 1).
Design Elements and Metrics.

Note. All areas measured in square feet and distances measured in feet; low, medium, and high categorization used for qualitative measures.
Floor Plan Acquisition and Analysis
The study team created a two-page printed guide to assist facilities in submitting usable floor plans for analysis (Online Appendix A: Floor Plan Annotation Guide). The detailed instructions were designed for nondesigner health professionals and included advice about whom to contact for the required documents (usually the facility manager), the preferred file format (.dwg), and a list of annotations to add to the floor plans to allow for standardization and analysis. We maintained close communication by phone and e-mail with contacts at each of the facilities in order to ensure compliance with the instructions. In cases where floor plans were not readily available in the requested file format, we traced a .pdf file using computer-aided drafting software and a predetermined set of graphic conventions. In cases where annotations were not feasible, we used the architect’s original annotations or a phone discussion of the floor plan with a manager or unit leader to understand space allocations and functions.
We measured areas (square feet), distances (feet), and units (number) using built-in computer-aided drafting software tools to collect comparable metrics from our sample of facilities. Different drawing layers were used to visually group metrics corresponding to the different functional areas (e.g., nursing stations, minimum distance from nursing station to labor rooms).
During a second in-person advisory board meeting, we presented the design data from the floor plan analysis to the board members to refine our interpretation of the design metrics, continue refining hypotheses about how these design elements may help or hinder the provision of care, and discuss areas to explore further during our site visits and phone interviews based on these hypotheses.
Site Visits and Phone Interviews
Following the initial analysis of facility floor plans, we arranged site visits or phone interviews with all facilities. We selected six facilities for in-person site visits based on design characteristics and geographic location and conducted phone interviews with the remaining six. The site visits and interviews aimed to confirm details of the facility floor plan not clearly labeled or not well understood; broadly characterize the social, economic, and medical context in which the facility operates; and discuss how the design of the unit helps or hinders clinicians.
We designed a structured guide to standardize the site visits and data collection. Each visit started with an introductory discussion of the history of the building, patient demographics, baseline delivery data, and staffing and management practices with representatives from the facility, including clinical directors, nurse managers, and/or facilities managers. After the introductory discussion, we toured the unit or birth center to observe clinical, administrative, and staff areas. During the tour, an architect member of the research team photographed key areas and updated annotations to the floor plans. Following the tour, we conducted semistructured interviews with the facility representatives to discuss any elements of the site visit guide not covered on the tour.
Based on the highest yield information collected during the site visits, we adapted and condensed the guide to an approximately 1-hr phone interview. The phone interviews elicited information comparable to the site visits and demonstrated the feasibility of a more scalable data collection method for future research. A single member of the research team conducted interviews with a nurse manager and a facilities manager, if available, at all six remaining facilities. Interviewees were e-mailed a simplified floor plan before the interviews to help guide the discussion. As with the site visits, information from the phone interviews augmented data analyzed from the floor plans and enhanced our understanding of relevant themes and hypotheses about the way design impacts care.
Facility Profiles and Analysis
We developed detailed profiles for each facility including a floor plan highlighting different space uses, facility characteristics, and descriptions and/or pictures to illustrate key design themes highlighted by each facility. The profiles aimed to consolidate key information about each facility in a consistent way. We also analyzed the final design metrics data across facilities to assess the range of variation for the different design elements and graphed the design data with delivery volumes and low-risk (primary) cesarean delivery rates to identify associations between design element and care that could potentially be investigated in future work.
Results
Facility Characteristics
The selected facilities represented a diverse range of facility types, including freestanding birth centers, community hospitals, academic hospitals, and women’s specialty hospitals, located across the contiguous United States (Table 2). Annual delivery volume ranged from 175 to 300 deliveries per year among the birth centers and from 432 to 9,100 deliveries per year among the hospitals. Low-risk cesarean delivery rates ranged from 5.1% to 10.0% among the birth centers (reflecting patients transferred to hospitals for surgeries because birth centers do not have operating capabilities on site) and from 15.0% to 34.9% among the hospitals. Across the full sample of birth centers and hospitals, higher delivery volumes were associated with higher low-risk cesarean delivery rates.
Facility Characteristics.
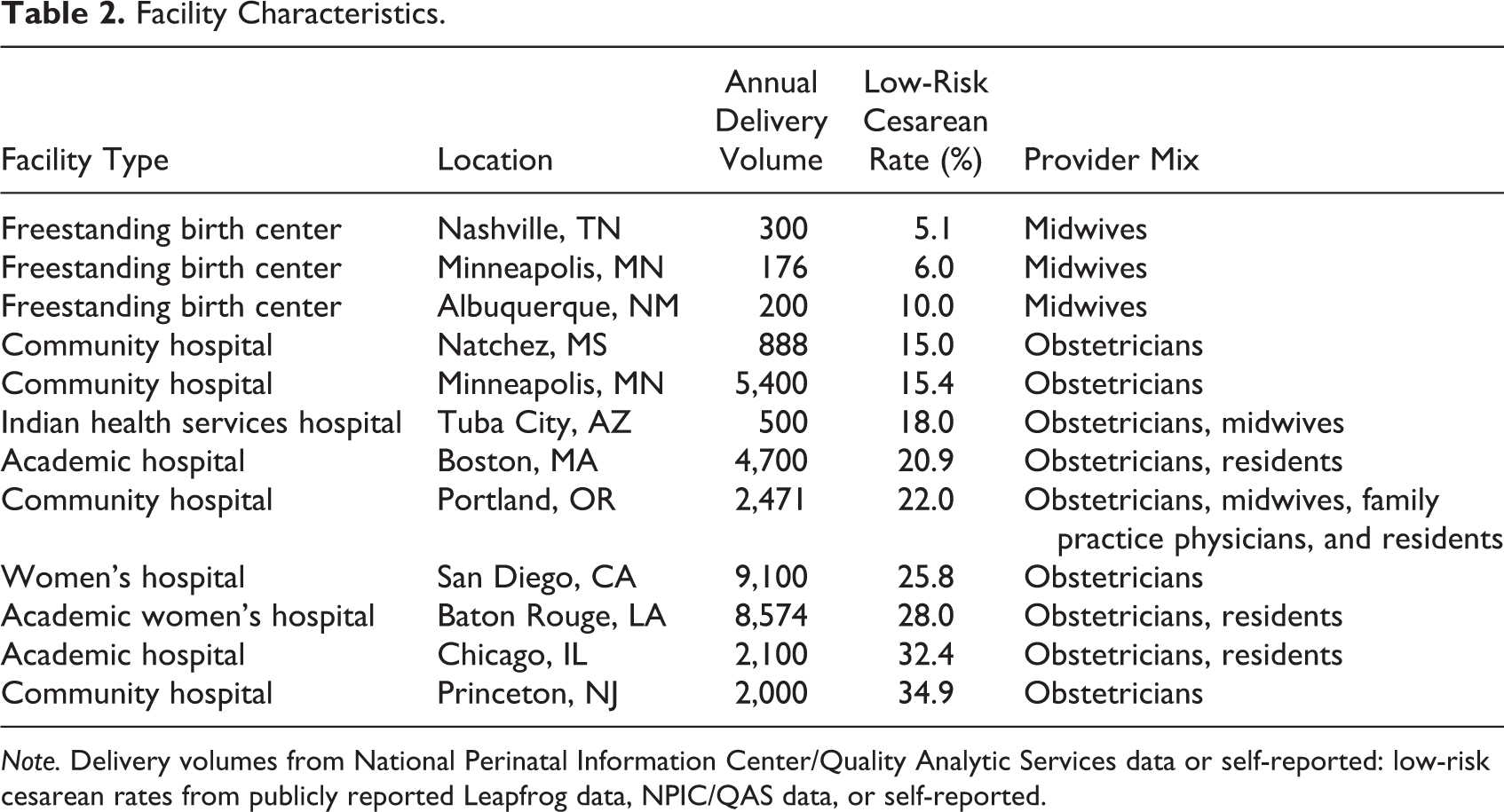
Note. Delivery volumes from National Perinatal Information Center/Quality Analytic Services data or self-reported: low-risk cesarean rates from publicly reported Leapfrog data, NPIC/QAS data, or self-reported.
Capacity Design Elements
Room demand and facility size
Room demand, defined as the number of annual deliveries per labor room, varied greatly between facilities ranging from 75 deliveries per room per year (less than 1 delivery every 4 days in each room) to 479 deliveries per room per year (more than 1 delivery per day in each room) across all units (Table 3). The facility size relative to delivery volume closely paralleled the room demand, ranging from 36 ft2 per delivery per year at a facility with one of the lowest levels of room demand to 4 ft2 per delivery per year at a facility with one of the highest levels of room demand. Across the full sample of birth centers and hospitals, both higher room demand and lower facility size relative to delivery volume were associated with higher low-risk cesarean delivery rates. When limiting the sample to hospitals only to account for the differences in patient risk levels and interventions provided in hospital labor and delivery units versus birth centers, there was no clear association between low-risk cesarean delivery rates and room demand, but there remained a positive association between low-risk cesarean delivery rates and facility size relative to delivery volume (Figure 2).
Variation in Quantitative Design Elements.

Note. All areas measured in square feet and all distances measured in feet.
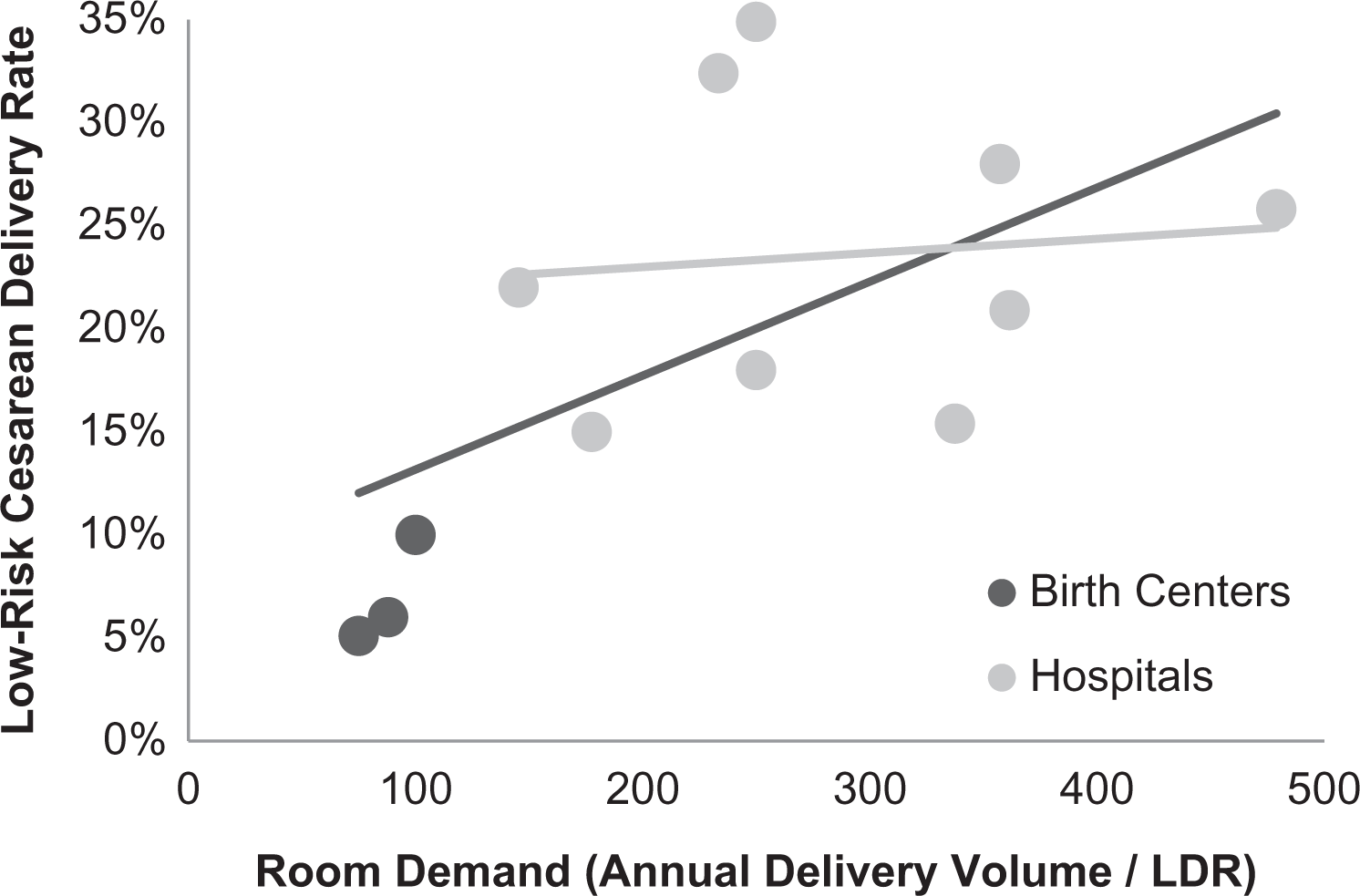
Association between room demand and low-risk cesarean delivery rates.
Overflow spaces
Facilities had varying abilities to accommodate surges in demand through overflow beds. Overflow beds are beds that do not normally function as labor beds but can be adapted to accommodate labor and delivery care when standard labor beds are occupied. The types of beds designated as potential overflow beds varied by facility, including dedicated overflow beds, triage beds, postanesthesia care unit beds, and operating rooms. Across the full sample of facilities, the ratio of overflow beds per labor room ranged from 0:2 at a facility without overflow beds to 5:1 at a facility with two labor rooms and nine potential overflow beds. Higher ratios of overflow beds to labor rooms were associated with higher low-risk cesarean delivery rates (Figure 3).
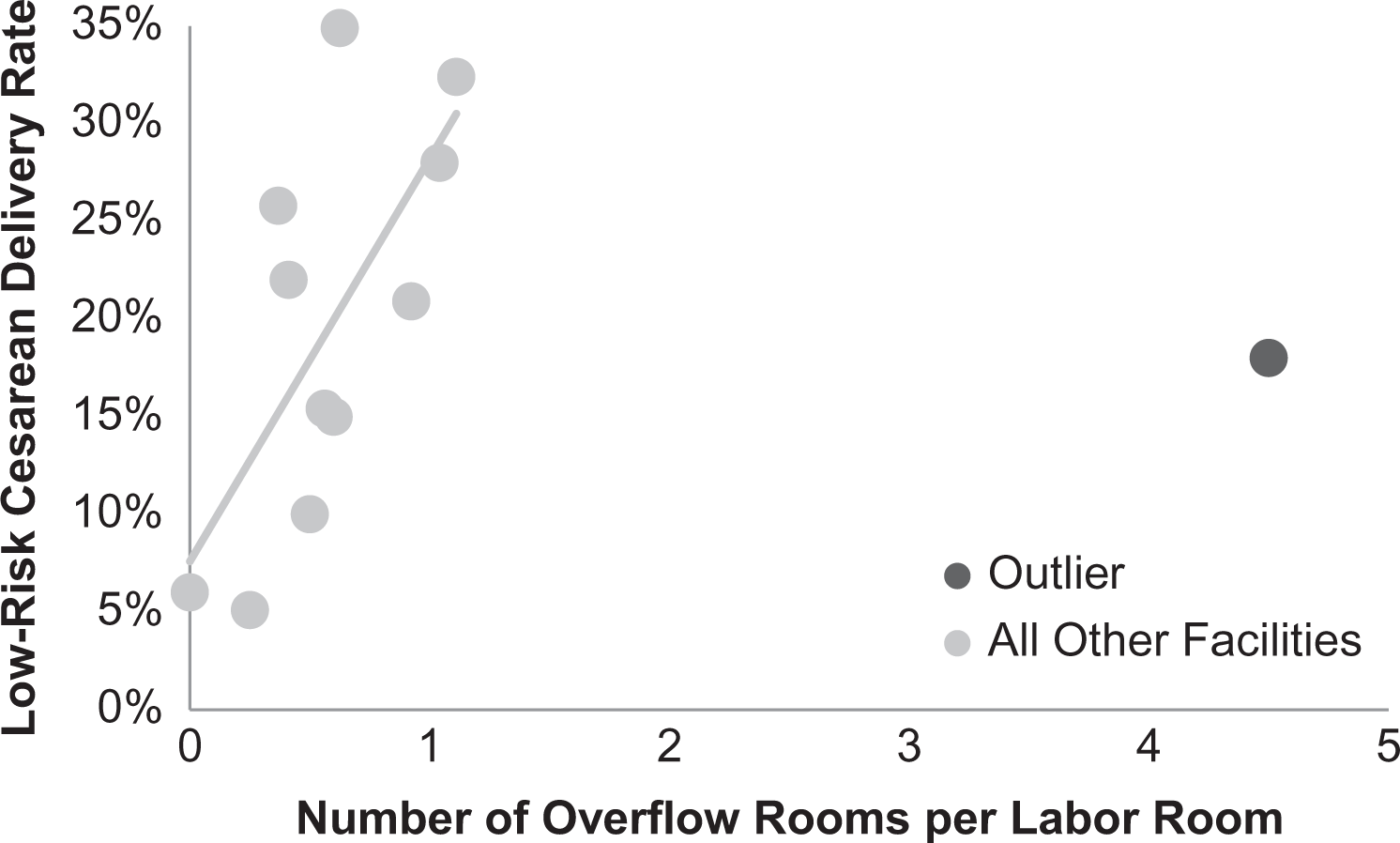
Association between the ratio of overflow rooms to labor rooms and low-risk cesarean delivery rates.
Operating room access
Birth centers provide care for a low-risk subset of patients and therefore, by definition, did not have operating rooms. All hospitals had operating rooms specifically dedicated to their labor and delivery unit. The ratio of operating rooms to labor rooms ranged from 1:1 to 1:9. Across all hospitals, higher ratios of operating rooms to labor rooms were associated with higher low-risk cesarean delivery rates.
Workload Design Elements
Distances to patient rooms
The average distance between labor rooms and workstations in each facility ranged from 23 to 114 ft across all units, and the maximum distance between labor rooms in each facility ranged from 9 to 242 ft. These distances were partly related to the overall size of the facility and partly related to the layout of the facility. In most cases, the distances increased with increasing facility size; however, one of the largest facilities studied had the shortest average distance between labor rooms and workstations because of their pod layout with sets of four rooms clustered around smaller, decentralized workstations. There was a positive association between low-risk cesarean delivery rates and the average distance between labor rooms and workstations and a positive association between low-risk cesarean delivery rates and the maximum distance between labor rooms (Figure 4).

Associations between distances between functional areas and low-risk cesarean delivery rates.
Standardization of labor rooms
Within the labor rooms, there were an equal number of facilities in each category of standardization (Table 4). All birth centers had unique labor rooms while hospitals had unique rooms, mirrored rooms (same headwall layout on different sides in each room), and same-handed rooms (same headwall layout on the same side in each room).
Variation in Qualitative Design Elements.

Note. Percentage of childbirth facilities with low, medium, or high designs as defined in Table 1.
Motivation and Accountability Design Elements
Call room accessibility
Among the 11 facilities with call rooms, the maximum distance between call rooms and labor rooms ranged from 88 to 661 ft. The one facility without call rooms was a birth center, which reported not having call rooms because midwives were expected to spend the majority of their time with the patient at the bedside for labor support. There was a positive association between low-risk cesarean delivery rates and the maximum distance between call rooms and labor rooms.
Staff support and collaborative spaces
Staff support areas, including call rooms, locker rooms, break areas, and staff restrooms, ranged from 14% to 26% of total unit area among birth centers and 3% to 13% among hospitals. Despite their smaller total unit areas and one birth center not having any call rooms, all three birth centers had greater percentages of total facility area dedicated to staff support than any of the nine hospitals studied. Within all staff support and work areas, collaborative spaces for multidisciplinary interactions ranged from 0% to 95% of total staff areas. There were negative associations between low-risk cesarean delivery rates and the percentage of total facility area dedicated to staff support and the percentage of total staff support and work areas designated as collaborative spaces (Figure 5).

Associations between staff support and collaborative space areas and low-risk cesarean delivery rates.
Context and Culture Design Elements
Accessibility of labor support equipment
Eleven of the 12 facilities selected had some type of labor support equipment available. All birth centers and two hospitals had the labor support equipment immediately accessible in labor rooms, while the other six hospitals with labor support equipment stored it outside of labor rooms. In some hospitals, rooms were not designed with sufficient storage space to accommodate labor support equipment in the rooms so centralized storage was necessary.
Prominence of technology
All three birth centers had less prominent monitoring technology with no central fetal heart monitoring, while all nine hospitals had monitoring screens both inside and outside labor rooms. Four hospitals only had central monitoring in staff work spaces and five had central monitoring in both staff support and work spaces. More prominent technology did not necessarily equate with more functional technology. In several units visited, there were multiple computer monitors that were nonfunctional or unused in the workspaces.
Nature and natural light in workspaces
Only two birth centers had views of nature and natural light in staff work spaces. The third birth center and all nine hospitals had neither views of nature nor natural light in staff work spaces. Some hospital units which had undergone recent renovations had moved staff areas toward the core of the building where access to windows was unavailable to ensure they had natural light in their added patient rooms.
Patient accessible circulation
The percentage of total unit circulation designated as patient accessible ranged from 27.6% to 100%. There was a negative association between low-risk cesarean delivery rates and the percentage of total unit circulation designated as patient accessible. The types of spaces available for patient ambulation also varied across facilities ranging from hospital corridors to a patient garden in one of the birth centers.
Discussion
Our study of 12 childbirth facilities demonstrated the feasibility of a scalable methodology for measuring meaningful quantitative and qualitative design data from diverse facilities. The architects on our team derived the quantitative metrics for this study from floor plans using computer-aided design software, but these measures could also be easily acquired through counts of different types of functional spaces and measurements of distances between spaces that could be performed by clinicians or managers at childbirth facilities. Through our measurements and analyses, we observed that the design of birth centers and hospital-based labor and delivery units varies substantially across the United States in ways that may be independent from service delivery needs. While some variation in design appeared to be intentional (such as a birth center selecting a space with a large garden for patient ambulation), much of the variation in design appeared to be arbitrary, rooted in unintended consequences of retrofitting existing spaces to fulfill childbirth care needs (such as a hospital labor and delivery unit with long distances between labor rooms and the nearest available call rooms).
Furthermore, our observations provide credible hypotheses of how design may impact care based on the theoretical framework of the pressure tank model. In the capacity dimension, we observed expected positive trends between low-risk cesarean delivery rates and room demand across the full sample of birth centers and hospitals; however, similar to the findings of Rowe et al. (2014) in 36 British obstetric units, we observed no associations between low-risk cesarean delivery rates and room demand when limiting the sample to the nine hospital labor and delivery units only. The limited association may reflect low sensitivity of room capacity to annual patient volume. Annual data can obscure dramatic variability occurring on an hourly or daily scale that is more likely to impact the pressures on clinicians and care in the unit. The associations could also be confounded by differences in organizational characteristics and clinical practice models that impact patient outcomes (Hodnett, Downe, & Walsh, 2012; Seibold, Licqurish, Rolls, & Hopkins, 2010).
We also observed an unexpected positive trend between low-risk cesarean delivery rates and the ratio of overflow beds to labor rooms. Instead of representing a greater ability to flexibly accommodate surges in patient volume, a higher ratio of overflow beds to labor rooms may actually indicate an insufficient number of labor rooms. The Facility Guidelines Institute (2014) provides guidance on the minimum size of labor rooms, but there are no evidence-based or broadly accepted standards for the appropriate number of labor rooms for a given delivery volume. Future research should investigate the relationship between resource availability and patient outcomes controlling for potentially confounding organizational characteristics to develop evidence-based standards for childbirth facilities.
Across the other quantitative design metrics studied in the workload and motivation and accountability dimensions, we observed the associations between low-risk cesarean delivery rates and design elements hypothesized based on the pressure tank model, including a negative association between low-risk cesarean delivery rates and the ratio of operating rooms to labor rooms and positive associations between low-risk cesarean delivery rates and greater distances between functional areas. The negative association between low-risk cesarean delivery rates and the ratio of operating rooms to labor rooms may indicate supply induced demand where the relative quantities of labor rooms and operating rooms prime clinicians’ expectations about care based on the resources they have available. The positive associations between low-risk cesarean delivery rates and greater distances between functional areas may reflect increased use of low-risk cesarean deliveries as a lever to relieve workload pressures on clinicians created by the inefficiencies in the physical design of the spaces in which they work.
Collectively, these results should be interpreted in the context of our study design. We only analyzed 12 facilities and therefore, most likely underestimated the full breadth of variation in design among childbirth facilities in the United States. In a larger sample, we would expect wider variation and more notable associations between design and delivery of care. We also did not perform any significance testing or control for potentially confounding factors, such as patient characteristics or clinician staffing patterns, so we are unable to infer causality. Design may impact care; however, existing practice patterns in childbirth facilities may instead be driving the design of spaces in some cases. However, while design could be used as a tool to perpetuate existing models of care, design could also potentially be intentionally leveraged as a tool to instigate changes in practice patterns. This study also analyzed design elements individually, but clinicians, administrators, and designers aiming to use design to impact care should consider the way different design elements interact and modify the effects of each other.
Our work presents preliminary evidence for wider scale evaluation of the impact of design on clinical outcomes in childbirth and other healthcare domains. Evidence-based guidelines for the design of childbirth facilities are currently lacking. Nonetheless, childbirth facilities undergo a range of design adaptations that may offer opportunities to incorporate evidence-based measurement and design principles ranging from infrequent, large-scale construction to frequent smaller scale renovations of functional areas every few years. Future work should incorporate a larger sample size to investigate the interaction between design and other individual and facility characteristics in driving practice patterns. Future studies could also explore more granular data on the connection between design and practice patterns, such as the number of deliveries and cesarean deliveries per labor room or overflow room, to add further nuance to these hypotheses. These results can set the foundation for establishing best practices for architects, facility planners, and clinicians to coproduce childbirth spaces in order to ensure design and service delivery are well matched.
Implications for Practice
The design of childbirth facilities may impact the way care is delivered. There is a need for wider scale evaluation about the impact of design on clinical outcomes. Evidence-based guidelines for the design of childbirth spaces should be codeveloped by architects, facility planners, and clinicians in order to ensure design is well matched to service delivery needs.
Supplemental Material
Supplemental Material, HERD_Appendix_1 - Assessing the Feasibility of Measuring Variation in Facility Design Among American Childbirth Facilities
Supplemental Material, HERD_Appendix_1 for Assessing the Feasibility of Measuring Variation in Facility Design Among American Childbirth Facilities by Avery Plough, Deb Polzin-Rosenberg, Grace Galvin, Amie Shao, Brendan Sullivan, Natalie Henrich and Neel T. Shah in HERD: Health Environments Research & Design Journal
Footnotes
Acknowledgments
The authors would like to thank Emmy Ganos and the Robert Wood Johnson Foundation for funding this study; the advisory board including Jill Arnold, Bill Berry, Rosalyn Cama, Atul Gawande, Sue Gullo, Susan Haas, Elizabeth Howell, Michael Murphy, John Pierro, Chanel Porchia-Albert, Amy Romano, Susan Stapleton, and Jaynelle Stichler for providing expert input and guidance for the study; and Ani Bilazarian, Ana Inoa, and Olivia Orr for providing project support and coordination.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Robert Wood Johnson Foundation.
Supplemental Material
The supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.