
Abstract
Aim:
The aim was to investigate the content and quality of the governing documents created in the planning and design phase of new healthcare environments and in the related healthcare strategic and operational plans.
Background:
Quality deficits in buildings can often be traced back to the initial stages in the planning and design phase. Although large investments have been made to improve the process of planning new healthcare environments and linking the requirements to health service strategies, healthcare organizations rarely relate their strategy goals to the built environment.
Method:
A retrospective review of documents created in the planning and design stages of new healthcare environments and the operational plans of the target organizations was conducted.
Results:
The organizational operational plans did not contain any statements or information about the built environment or how a building could or should support the organization’s goals. Important information was frequently absent from the documents governing the planning and design of buildings. The documents lacked information about what and how to follow-up and what to measure once a construction project had been completed. There were no references to evidence.
Conclusions:
Poor documentation might undermine the quality of the planning and design phase and ultimately the opportunity to create environments that support health outcomes. Therefore, more emphasis must be placed on the importance of documentation but above all to strengthen and clarify the relationship between the healthcare organization strategy to achieve an effective and efficient care process and the intention made in the planning and design process.
Keywords
A global challenge today is the need to provide safe, high-quality, and effective health service in a context of ever-decreasing resources (Salonen et al., 2013). The built environment is an active and influential factor for health processes and should not be separated from executing organizations’ strategic goals to achieve service quality (Henriksen, Isaacson, Sadler, & Zimring, 2007).
Quality deficits in buildings can often be traced back to the initial stages in the planning and design process (Lindahl & Ryd, 2007). Documentation of decisions has previously been presented as a key to achieving quality in that process and as being required to communicate objectives for the entire subsequent building project (Ryd & Fristedt, 2007). However, documents have frequently not been used as a data source for learning about objectives and activities in the process of designing new healthcare buildings (Elf, Svedbo Engström, & Wijk, 2012). Recently, large investments have been made to improve the planning and design process of new healthcare environments. Special efforts have been made to ensure the link between healthcare goals, requirements, and strategies to the building project’s program (Ruohomäki, Reijula, & Reijula, 2017).
However, there is still a lack of studies on how the built environment is included and described in healthcare operational plans. In this study, we examined the content and quality of documents created in the planning and design process of new healthcare environments and in the related operational plans of the target organizations. This assessment was performed to explore how the organizations’ operational plans and planning and design documents are related.
Background
The built environment is increasingly viewed as a factor in delivering high-quality healthcare (Henriksen et al., 2007). Environments cannot only improve and influence health outcomes and efficiency but also contribute to problems such as the spread of infections, falls, and stress among patients, relatives, and staff (Ulrich et al., 2008). Poor design of public environments such as schools or libraries may cause dissatisfaction, inefficiency, or contribute to minor health problems; however, the consequences of an incorrect design in a healthcare context can be far more serious, including death (Becker & Parson, 2007). Thus, healthcare services must explicitly clarify in their strategic operational plans in what ways the built environment is expected to contribute to the quality of the healthcare.
Additionally, new concepts such as person-centered care and shared decision-making between patients and healthcare professionals are key requirements for healthcare today, and the built environment must reflect, match, and support these new models of care (Douglas & Douglas, 2005; Edvardsson, Winblad, & Sandman, 2008; Elf, Fröst, Lindahl, & Wijk, 2015).
With the increase in evidence-based data on the effects of the built environment on numerous outcomes, the link between strategic healthcare planning and planning of new buildings must be improved if the built environment should be a real support for the organization. New approaches and processes that integrate strategic visions and goals for healthcare and the planning and design of new environments must be developed (Zadeh, Sadatsafavi, & Xue, 2015).
Planning and Designing New Healthcare Environments
A building project is a complex process involving different conditional stages such as planning and design and construction and includes various stakeholders (Chandra & Loosemore, 2011, Elf, Eldh, Malmqvist, Öhrn, & von Koch, 2016). The early stages involve a series of iterative activities for collecting, analyzing, and synthesizing information needed throughout the building project for decision-making and implementation. In the initial stages, visions of the building project are established, and the goals are formulated, which, of course, should be based on healthcare service requirements. The desirable outcomes of patient care should be clearly presented, followed by how the work processes and the environment can support those outcomes. An understanding of the expected outcomes and an articulation of the project goals have been described as important factors for success (Becker & Parson, 2007; Wanigarathna, Sherratt, Price, & Austin, 2016). Decisions on environmental design will only be effective if such decisions support the overall goals of the intended healthcare services. The contribution from the built environment to the quality of care must be clarified in the planning and design stage. In the subsequent and more detailed project planning and design process, the goals are translated into technical descriptions of the environment in combination with architectural drawings (Lindahl & Ryd, 2007).
With an increased focus on patient-centered care, engagement of relatives, and increased requirements regarding staff effectiveness, the environment where patients receive healthcare increases in importance. The efforts dedicated to creating new built environments should therefore be viewed as a joint responsibility between healthcare and those in charge of planning and designing to achieve improved quality of care (Elf et al., 2015).
Documentation in the Process
In the planning and design process, multiple documents (often called briefs or programs) are created for different purposes to support an efficient planning process for healthcare environments. Documentation has been described as fundamental to expressing the intentions of new healthcare environments and how those intentions can be measured when a building is in use (Elf et al., 2012; Hamilton, 2017). Documentation is thus an important part of evidence-based design and quality improvement. Evaluation and measurement of predefined criteria and intentions associated with the built environment will answer the question regarding whether the intentions of the environment have been reached (Hamilton, 2017).
The documents created during the initial stage of the process are the medium for expressing or communicating intentions for a building project (Elf et al., 2012; Ryd & Fristedt, 2007). Documentation should, if created properly, contain background, visions, and goals applicable to a building project. However, few studies have examined the information contained in programs (Elf et al., 2012). Elf and Malmqvist (2009) reviewed information in documents created in the planning and design process for new healthcare environments and found that only a few documents provided clear, patient-oriented results that were measurable and had references to evidence. Fewer than half of the programs studied provided a clear description of the organization’s goals and activities that would occur in the planned healthcare environment. A follow-up study of the content and quality of documents during the initial stage of the planning process revealed the same pattern (Elf et al., 2012).
Evidence-Based Design
Considering that environments today are viewed as part of a high-quality healthcare system and should support expected patient care outcomes and promote cost-effective healthcare, there is an increased demand for planners and designers to base decisions regarding the built environment on evidence (Hamilton & Watkins, 2009). Evidence-based design is defined as a critical and reflective process in which decisions on a new environment are based on the best available evidence, analyses, and experiences gathered from already built environments and a structured analysis of user experiences (Stankos & Schwartz, 2007; Stichler & Hamilton, 2008).
Evidence-based design is part of a continuous improvement in quality (Becker & Parson, 2007; Hamilton, 2017), which assumes that health goals are defined by the best possible research, knowledge, and experience and that clear goals can be presented at the beginning of a planning and design process to enable evaluation when a building is complete and in use.
Within this context, the aim of this study was to investigate the content and quality of the central documents created in the planning and design stage of new healthcare environments and in the related healthcare strategic operational plans.
The following specific questions were examined:
What are the content and quality of the documents created in the planning and design stage of new healthcare environments?
How is the built environment described in healthcare strategic operational plans?
Method
A retrospective review was performed on documents created for the planning and design stages of new healthcare environments and the strategic operational plans of the target organizations.
Sample
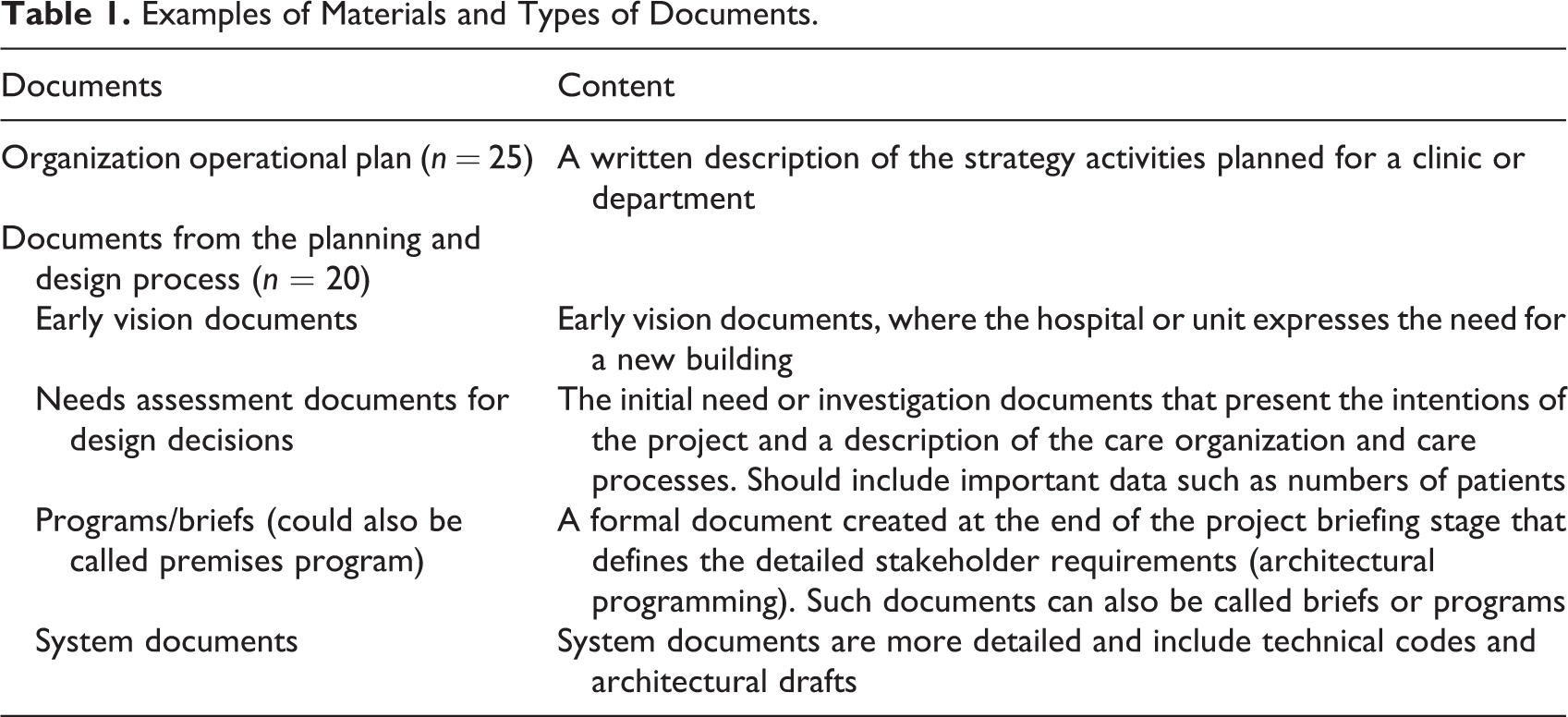
The sample consisted of documents from the planning and design process and the target organizations’ strategic operational plans. Overall, 45 various documents were reviewed (Table 1) from five building projects that had a budget of over SEK 50 million (US$5,493,000.00) and were executed between 2010 and 2014 in Sweden. The documents consisted of a combination of structured (tables, statements, etc.) and unstructured information (general texts, descriptions, etc.).
Examples of Materials and Types of Documents.
Sampling procedures
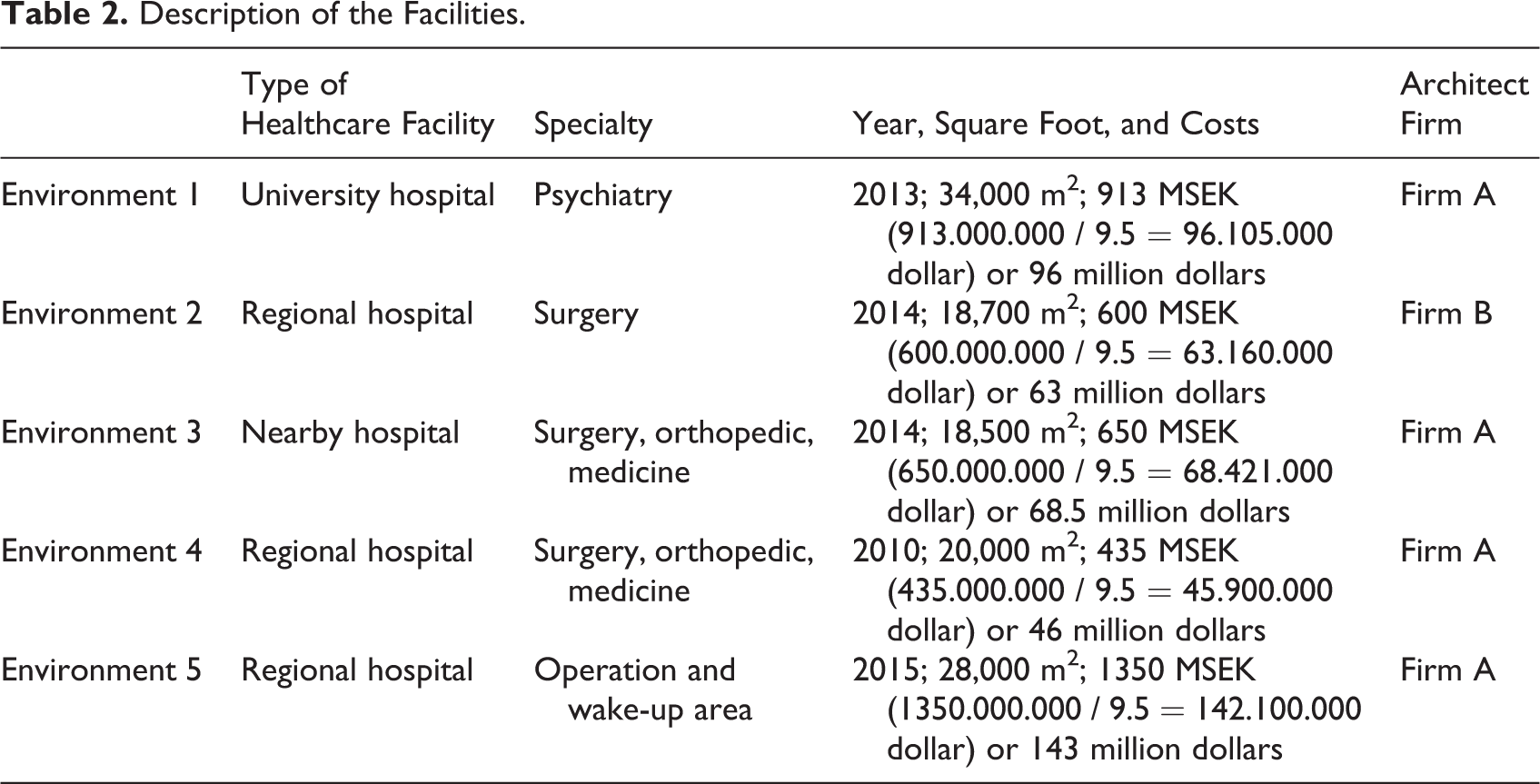
A pragmatic and purposeful sampling process was used to include a variety of building projects from different contexts (Tashakkori & Creswell, 2007). First, a systematic review of projects that matched the abovementioned criteria in all county councils in Sweden was performed. Finally, five building projects representing surgical, medical, and psychiatric care were selected (Table 2). Contact persons from the real estate department responsible for the building projects were asked to contribute all planning documents (vision documents, needs assessments, premises programs, etc.). Related organizations’ strategic operational plans were retrieved from the web (in Sweden, operational plans from the public sector are public) or requested from managers (n = 45; Table 1).
Description of the Facilities.
Measures
The documents were examined using an instrument for the analysis of the content and quality of briefs (content and quality in briefs—instruments—CQB-I; Elf, Svedbo Engström, & Wijk, 2012) and with the help of an established qualitative method for the content analysis of texts (Graneheim & Lundman, 2004).
CQB-I
The instrument measures whether there is a clear goal statement for a project based on user needs and the care activities that will occur in the new healthcare environment (Elf & Malmqvist, 2009; Table 3). Furthermore, it measures whether patient-related outcomes are specified and to what extent the information is evidence-based. A manual to support the assessment is available. The instrument has been tested and validated among experts (architects, facility planners, and researchers; Elf et al., 2012).
Results From the CQB-I Assessment.
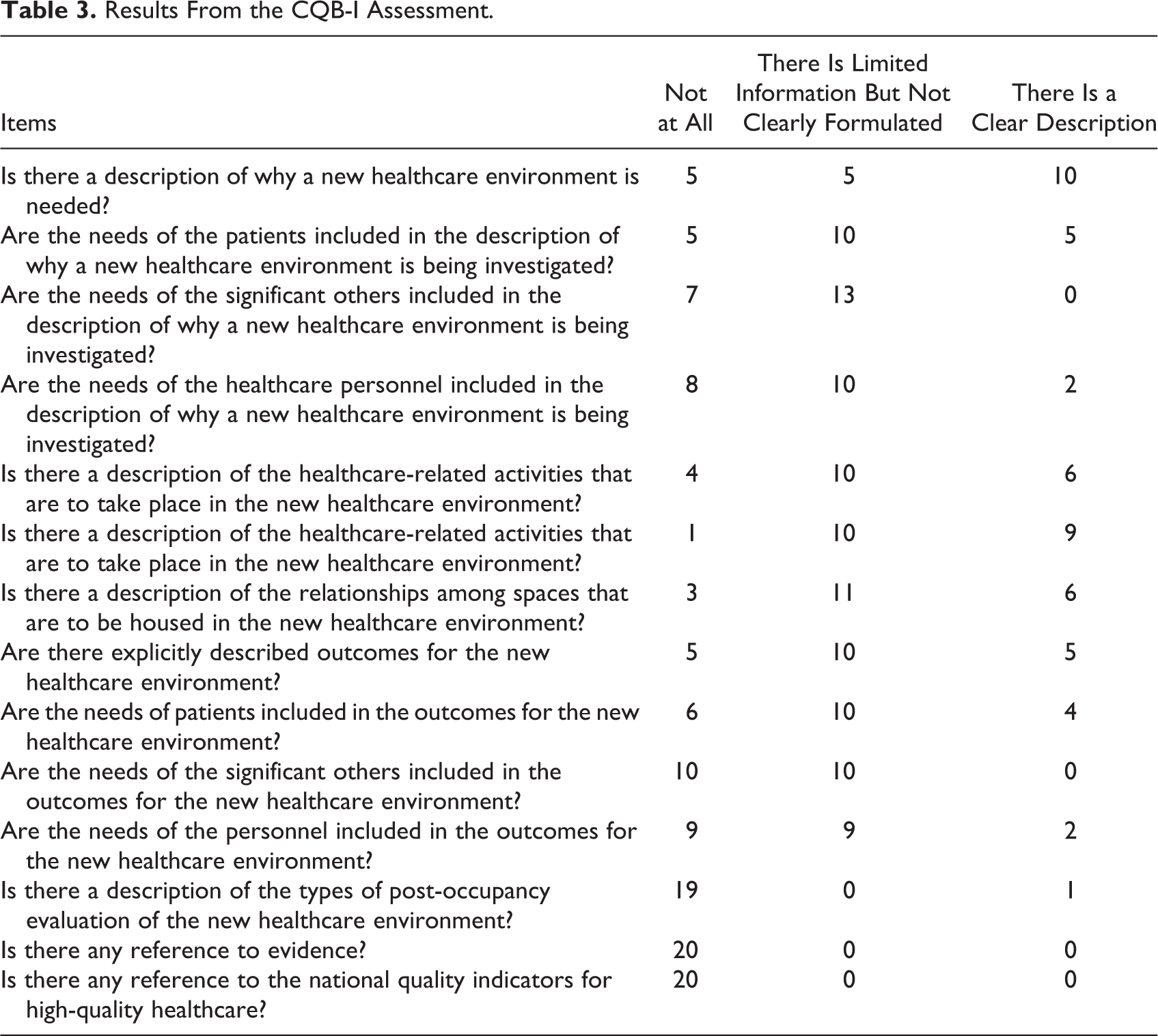
The framework for the instrument is Donabedian’s (1988) quality model and quality indicators for the Swedish healthcare system, which states that care should be safe, effective (and evidence-based), patient-centered, given the right time, and be equitably presented (The National Board of Health and Welfare [Socialstyrelsen], 2007). Donabedian described three types of factors required for quality improvements and evaluation: results, process, and structure. The result factors capture the desired results for the patients to be achieved (e.g., health, satisfaction, and well-being). Process factors are healthcare-related activities necessary for achieving the results (e.g., diagnostic procedures, treatment, and care), and structure factors include the basic physical and organizational qualities associated with the care environment, such as physical space, regulations, staff, and organizational structure (Table 3). The instrument involves a systems-thinking approach and supports the planners in analyzing the project objectives considering the facilities being planned, activities that shall occur in these facilities and what possible facilities might suit the activities planned for.
Analysis of the qualitative data
To structure and deduce the content of the collected documents, a qualitative content analysis according to that reported by Granheim and Lundman (2004) was performed. Data from documents were organized into a matrix with five different levels of headings: meaningful unit, condensing meaningful unit, code, subcategory, and category, all of which aimed to capture a manifest content.
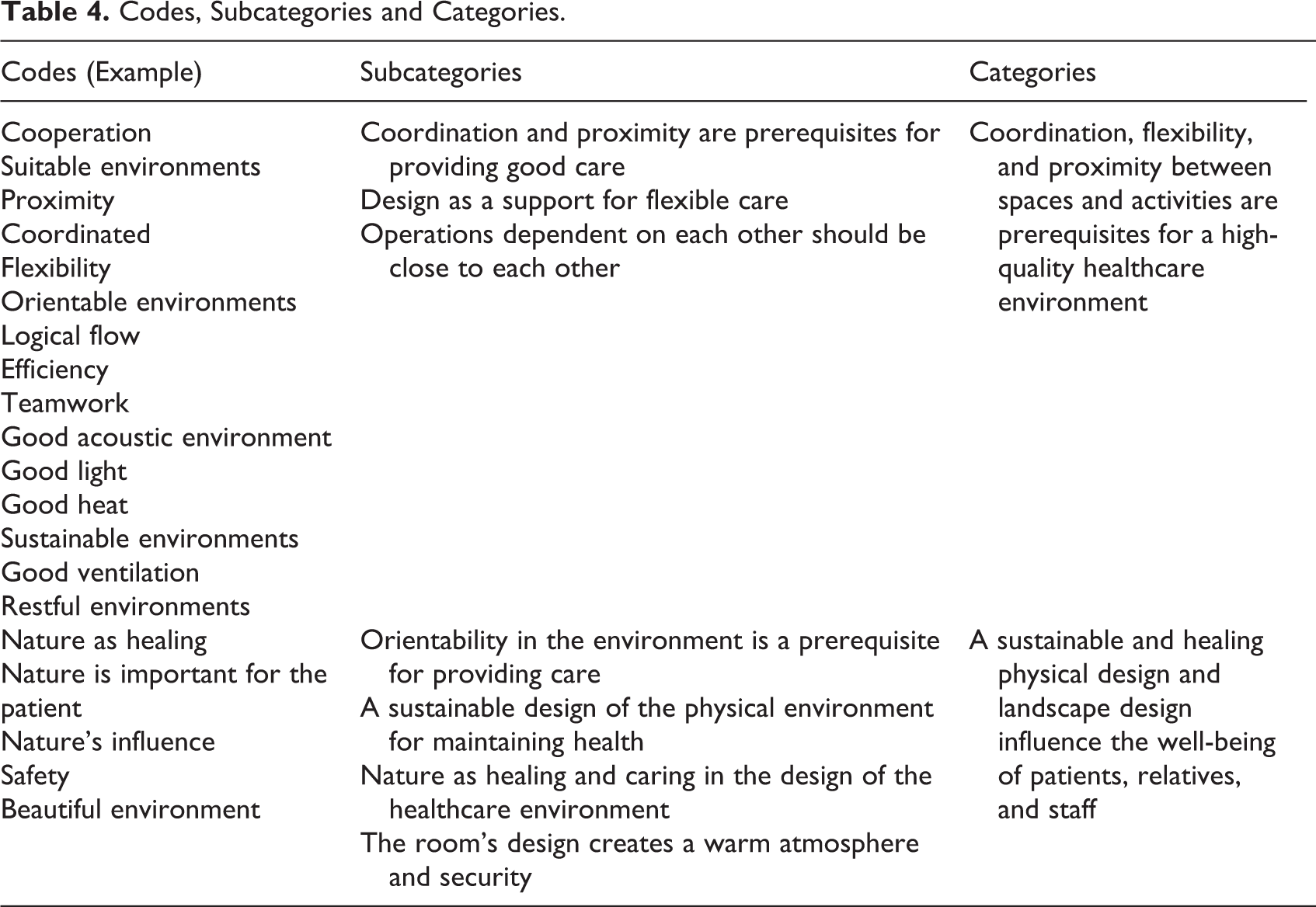
Key texts about the description of the built environment were highlighted as the meaningful units, which then were condensed and coded. In coding, the aim was to find meaning and clarify the content. The codes were compared based on similarities and differences and organized into subcategories and categories used to find patterns in the texts (Table 4).
Codes, Subcategories and Categories.
Results
CBQ-I Results
Most documents featured objectives formulated for the healthcare environment, but those objectives were not specific and measurable or expressed in desirable outcomes for what the new environment shall achieve (Table 3). In addition, the documents had no description or consideration of a post-occupancy evaluation of the completed environment. The results show that the objectives were not substantiated by references to evidence. In general, the documents expressed objectives that should have references to evidence or to experience-based knowledge.
Contents of the Planning Documents
The content analysis resulted in two main categories of objectives pertaining to the built environment (Table 4). These categories describe goals and what the built environment was expected to contribute to, as follows: Coordination, flexibility, and proximity between activities are prerequisites for a high-quality healthcare environment. The design of the built environment and exposure to nature affect patient health outcomes, relatives, and staff well-being.
Coordination, flexibility, and proximity between spaces and activities are prerequisites for a high-quality healthcare environment
Key words found in the planning documents were associated with the coordination and proximity between spaces in order to establish effective routes between activities; for example, operations areas needed to be related to intensive care units. Coordination and proximity were also described as important for effective teamwork and possibilities for staff to interact between various areas during a working pass. The descriptions emphasized that facilities should support staff to easily move between various spaces and functions. The documents also describe how the environment should support increased co-organization between and within units and clinics. The proximity principle was applied in terms of the closeness between organizational units, between patients and staff, and among staff. For example, one of the planning documents described this concept as follows: “/…/ As there are almost daily emergency situations for the birth, it is important that all parts of the clinic are close to each other.”
Several planning documents described the built environment based on its adaptability and flexibility to support different types of care activities, collaboration, and teamwork between staff. A flexible healthcare environment was described as the one allowing the patient to be placed in the same room throughout the time spent at the hospital regardless of health status and that the necessary equipment and staff should instead transfer to the patient. One example of this reasoning found in the planning documents was as follows: “The premises should therefore be suitable for collaboration and teamwork. Patients should need as little as possible to move between locations and caregivers.”
The documents also described that the current healthcare service is characterized by development and changes in its activities and that this aspect must therefore be reflected in the environment as a built-in flexibility. New activities or altered activities should not automatically imply a new building, but the existing facility should be able to address these changes. Many of the planning documents addressed flexibility, for example: “Short-term locations designed to allow for both in-patient care and day care for both children and adults.”
A sustainable and healing physical design and landscape design influence the well-being of patients, relatives, and staff
The planning documents also contained statements indicating that the built environment could affect health and well-being for patients, relatives, and staff (Table 4). Certain aspects of the built environment were described in greater detail than others; for example, good acoustic environments were emphasized in several documents. In general, the properties of the environment creating a calm, caring, warm, and secure atmosphere were raised as important qualities to achieve to support recovery.
Several documents emphasized both the importance of aesthetic characteristics such as shape, color, and art and functionality as a goal for the environment. Repeatedly, the documents stated that a beautiful environment affects good health and well-being; “As the patient spend most of the time in bed, thus the ceiling is a substantial part of the design of the room. A quiet white ceiling makes the room beautiful and soothing.”
There were descriptions of how a “healing environment” required a design providing an opportunity for closeness to nature and that the building design should integrate nature. Many documents emphasized that a natural and green environment has a healing effect. The documents described how the built environment should reflect the natural environment with plants and natural materials to create a lively and natural environment: “The nature can be a healing power needed to be recognized. The environment must be experienced natural and healing.”
Color and color choices in the environment were another common factor among the documents. Colors were reported to be important aspects for promoting a supportive and healing environment. Color was assumed to influence feelings such as safety, harmony, and peace. Moreover, colors were described to be used to support security, have a separating and guiding function, and support overall orientation: “In addition to creating security and harmony, the coloring must be carried out in a way so that it becomes easy to navigate in the building for patients and families.”
Much of the text in planning documents focused on technical descriptions of how the environment could support patient’s health. Often the statements indicated how the environment should be sustainable to be functional in the long term. Descriptions of acoustics were common “Great attention needs to be taken to a good acoustic environment since it contributes to patient recovery and a good working environment. An effective noise reduction is important in at the workstations in the corridor.”
Description of the Built Environment in the Organizations’ Operational Plans
The built environment was not mentioned in the operational plans of healthcare organizations. Thus, it was not possible to further analyze the content related to issues concerning the physical environment. The operational plans primarily described how the organization should develop means for reporting to different national patient registers and provide equitable care in terms of gender and ethnicity. The documents also mentioned goals focused on how to improve medical treatment and nursing and how to shorten queues and waiting times. Goals for ensuring the right level of drug use, values, and leadership were other important areas covered by the operational plans. There were no comments on how the built environment could or should support the goals in the operational plans.
Discussion
This is the first study of the content and quality of information contained in documents from the planning and design stage of selected building projects for new healthcare environments and operational plans from the related healthcare organization in Sweden. One interesting finding was that the organizational operational plans did not contain any statements or information about the built environment or how a building could or should support the organization’s goals.
A serious problem arises if those responsible for healthcare are not able to formulate their needs regarding the design of the environment for supporting care. Previous studies have shown that healthcare professionals can have ideas and requirements regarding design that are often not sufficient to support the needs of the design and construction process (Elf, Eldh, Malmqvist, Öhrn, & von Koch, 2015). The development cycles for healthcare are shorter than those for the built environment, a challenge that often results in arguments for flexibility rather than a high-level discussion of strategies and effects of the built environment. A gap between design intentions and the healthcare activities on which they should be based may result in refurbishment, inefficiency, and patient and staff frustration (Adam & Lindahl, 2017; Fronczek-Munter, 2016; Lindahl & Ryd 2007).
Furthermore, important information was frequently absent from the documents governing the planning and design of buildings; for example, the documents contained very little information about what and how to engage in follow-up and what to measure once a construction project had been completed. The result indicates that the care activities do not appear to be spatial at the strategic level, resulting in no or very few evaluation criteria noted in the documents that govern the planning process for the built environment.
Overall, intentions and goals pertaining to the proposed healthcare environments were expressed in most of the planning documents. This finding reflects the focus on capturing user or customer needs when planning for new environments. Today, stakeholders in a planning process are well aware of the importance of including project intentions and goals in the early stages of a project. Practitioners, architects, and planners as well as researchers have developed guidelines for a structured planning process in which the focus on expressing intentions and goals for the project has been central. This finding is also confirmed by many other studies in the planning and design field (Kelly & Hunter, 2005; Lindahl & Ryd, 2007; Vischer, 2009).
However, the results showed that even if the goals of a building project were stated in the documents, they were not written sufficiently clear to enable a follow-up at a later stage. For project actors, the documentation was not sufficient for follow-up. This situation is problematic as the possibility to conduct a credible and coherent evaluation after a building is completed and in use is very difficult without expected outcomes clearly described in the early stages of a planning and design process (Hamilton, 2017; Vischer, 2009).
There is a risk that important goals beyond technical solutions will not be addressed or clearly defined and that planning and design decisions will focus on spatial or functional issues, such as number of beds and square meters, instead of users’ needs and requirements for supporting healthcare processes and reaching health. Previous studies have also revealed weaknesses in defining and expressing users’ needs (patients, relatives, and staff) and clarifying patient-related outcomes necessary for evaluation of the completed building (Elf & Malmqvist, 2009; Elf et al., 2012; Hansen & Vanegas, 2003; Wanigarathna et al., 2016).
Follow-ups have been described as a prerequisite for evidence-based design and successful continuous improvement of the planning and design process (Hamilton, 2017; Preiser, Rabinowitz, & White, 1988). Thus, it is important to gather information regarding how the built environment works, its effects, and how the people who work and use it experience it. One critique of the methods used to evaluate the built environment is that the focus has been on user experience and opinions rather than on predetermined criteria based on evidence (Stichler, 2010; Vischer, 2009). The criteria that must be investigated in planning of healthcare environments should be based on assessments of existing environments, evidence-based knowledge, and new technical and environmental requirements.
The absence of a link between the organization’s strategic documents and the planning documents is, of course, the most important outcome of the current study. The lack of this link indirectly reduces the precision of documents governing planning. This situation also challenges the ability to evaluate the quality of a new built environment for healthcare and whether the investment is cost-effective. Based on the present study, it appears that care has been developed without paying attention to the built environment space. A large amount of research has shown that the built environment plays a role in quality care and should be considered and described in all documents relating to care processes. There is a risk that ideas, knowledge, and experiences concerning the built environment will remain only in discussions in the planning process.
The documents studied contained almost no references to evidence of any type to substantiate the statements. The same was true even if the documents involved rather strong statements regarding, for example, the possibility of contact with nature and how that could influence patients’ health in a positive manner. This finding is worrying, particularly when considering the latest development and recognition of the importance of evidence-based decisions in planning and design processes. One possibility is that the design team in the projects studied collected, analyzed, and discussed evidence relating to design but did not document their efforts. For a reviewer of the document, it appears that decision-making in the actual building projects was based on ad hoc knowledge rather than a more systematic knowledge-based strategy. There were many vague descriptions of expected outcomes of the environment. Examples include “A good acoustic environment should be constructed,” “a good electrical environment should be constructed,” and “white ceilings have a calming effect.” Such statements were made without further explanation of why they were important or without references to research that could possibly support these statements. The planning and design process does not benefit from unclear anecdotes or subjective ideas about design without any references to evidence or established experience. Such poor documentation will also, eventually, undermine the professionals engaged in planning and design when questioned about outcomes.
Some limitations of the study must be discussed. First, the same architectural firm designed four out of five of the included building projects. However, the design team varied among the five projects. The planning and design process and the budget of the building projects also differed. Therefore, it is to some extent problematic to compare the documentation practices among these different settings. On the other hand, Sweden has developed guidelines for basic protocols and the documentation of the planning and design process. Thus, it can be assumed that the accuracy and completeness of the documentation in the planning process can be related to project managers, and their personal routines, and not to the system used to record information. The study reflects healthcare design practices in Sweden and cannot be fully generalized to other practices and countries. However, we believe that the insight gained into design methods and decision-making can help reflect on various practices in other contexts. The study was explorative, and a relatively small number of documents were studied. Therefore, further, possibly larger studies are recommended to develop knowledge about how grades and effects are handled from strategic documents down to guiding documents for planning and design.
Conclusion
Poor documentation may negatively affect the quality of the planning and design process as it hinders benchmarking, follow-up, and informed decision-making. In addition, insufficient and poor documentation today hinders knowledge exchange, effective communication between stakeholders, and neglects setting criteria for post-occupancy evaluations. Such documentation also makes the transfer of information and decisions between the different stages of the planning and design process difficult. Therefore, greater emphasis must be placed on the importance of documentation in the planning and design process to, above all, strengthen and clarify the relationship between a healthcare organization’s strategy to achieve an effective and efficient care process and the intentions of the corresponding planning and design process.
Implications for Practice
Linking operational strategic goals with environmental development is a key to conducting an evidence-based planning process for a new healthcare environment. Formulating outcomes derived from operational strategic goals early in the planning and design process provides an opportunity to understand the impact of design on care activities. Using documentation as a data source is key to the continuing development of the planning and design process.
Footnotes
Acknowledgments
The authors want to thank the Center for Healthcare Architecture (CVA) at Chalmers University of Technology, Forum for Healthcare Buildings and Dalarna University, Unit of Health and Welfare for Financial Support.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Swedish organization for health care buildings.