
Abstract
Purpose:
The purpose of this article was to explore how different types of mock-ups are being used in the healthcare design process and present a methodology framework for the process.
Background:
Historically, physical mock-ups have been used in healthcare design primarily to test construction techniques. Although this historic use of mock-ups assisted the design team in decision-making, newer forms of mock-ups have evolved that expand the input provided into decision-making. These newer techniques, rapid prototyping, early build-out, virtual reality, and enhancements to the traditional physical mock-up focus more on challenging the functionality of the space, testing new operational concepts, and increasing user input.
Method:
This methodology article utilized five case studies in which different types and combinations of mock-ups were used in the design process and then, the methodology compares the realism, immersion, and testability of each mock-up technique.
Results:
For each mock-up type, the case studies described the purpose of the technique, the advantages and disadvantages, the most appropriate phase for its use in the design process, the estimated cost, and the process logistics. These components are compared to assist in developing a methodology for a variety of design situations.
Conclusions:
The findings related to different mock-up techniques are a valuable tool for healthcare design teams to use in selecting the most appropriate mock-up technique and the proposed methodology will assist in executing the mock-up process.
Keywords
There has been an increased level of interest in experiential simulation models (ESMs), commonly referred to as mock-ups, being used to assist healthcare clients in developing, understanding, and refining a proposed design solution (Watkins, Myers, & Villasante, 2008). Mock-ups, particularly physical mock-ups (PMUs), have been a part of the manufacturing and construction process for a long time, most frequently used to test technical or material components such as sample brickwork or specific construction details. Currently, a variety of mock-up techniques are being used to help clients test and validate functional or operational components of a proposed healthcare space before it is built.
ESMs or mock-ups allow stakeholders the opportunity to experience a realistic model of the space and test patient care scenarios before the final design and construction are complete. For this reason, mock-ups have also been referred to as “interactive laboratories” by Watkins, Myers, and Villasante (2008) that provide an opportunity for participatory design, and testing of evidence-based design (EBD) strategies (Watkins et al., 2008).
As identified by Peavey, Zoss, and Watkins (2012), mock-ups provide multiple benefits to the users (clinical care team) and other design team members: (1) the information and confidence to make timely decisions related to the proposed design; (2) the opportunity to explore new operational concepts, to test the space by simulating patient care scenarios, and to verify the placement of equipment and furnishings in the space; and (3) the chance to identify issues before construction and find creative, cost-effective ways to resolve them, thereby, eliminating the inefficient and often unsafe work-arounds that develop postconstruction (Peavey, Zoss & Watkins, 2012).
Most often, mock-ups are developed for rooms that are repeated often in the design, such as inpatient care rooms, or expensive, high-tech spaces, such as operating rooms. But, an entire unit or department may also be mocked up to test functional relationships and adjacencies such as an inpatient nursing unit that will be repeated several times in a new bed tower (Williams, Greulich, Bodewin, & Hanzel, 2017). The purpose of this document is to illustrate how mock-ups are being used in healthcare design through five case studies and suggest a methodology framework for the mock-up process.
Types of ESMs or Mock-Ups
Within the category of ESMs, there are two major categories, physical mock ups (PMUs) and virtual mock-ups with several specific types of mock-ups within each category. As suggested by Peavey et al. (2012), all mock-ups can be compared based on the following characteristics: (1) realism: often referred to as high fidelity (very realistic) or low fidelity (less realistic); (2) immersion: the degree to which a participant perceives being within the space; and (3) testability: the ability to interact with the mock-up and test patient care scenarios (Peavey et al., 2012). By understanding each technique and the degree of realism, immersion, and testability it provides, the most appropriate mock-up technique or techniques can be selected to meet the specific goals of the healthcare planning team.
PMUs
Historically, PMUs have been the most common type of mock-up and are known for having a high degree of immersion and testability, but the level of realism varies by the type of PMU. The three main types of PMUs listed in order of increasing realism are as follows.
Rapid prototype
Rapid prototyping is a technique that allows participants to test and refine ideas using inexpensive, flexible materials. Typically, this type of mock-up is used early in the design process and allows users to rapidly test new operational concepts (e.g., universal room, dual entrance exam room) or the size and shape of a specific room. The end product is a very rough prototype, often created from cardboard, which is further refined as the design progresses.
Rapid prototyping, a common Lean technique for experimentation, is inexpensive and quick with a low level of realism, testability, and immersion, but, as such, the process encourages creative thinking and testing new ideas (Durham, 2014).
PMU
While rapid prototyping is often referred to as low fidelity, PMUs range from medium to high fidelity. The PMU may be created as early as the schematic design phase or later in the design development phase to test and validate the details of the room. It is common for this type of mock-up to be developed in an iterative fashion starting with the room boundaries and progressively adding more detail in each iteration (Bayramzadeh, Joseph, Allison, Shultz, & Abernathy, 2018). Often, members of the clinical care team simulate patient care scenarios to assess flow patterns within a room and the dimensions of the space. In addition, the clinical care team, construction team members, and sometimes patients or community members may view the mock-up individually or in small groups and, then, provide input via a survey instrument or interview.
The PMU is an expensive mock-up technique but provides varying levels of realism, immersion, and testability while it is still early enough in the design process to make changes. As a result, it remains a very common mock-up technique.
Early build-out
In an early build-out mock-up, once the building is enclosed, a key room, such as an inpatient medical–surgical room or an intensive care unit (ICU) room, is fully built-out before finishing the rest of the rooms so users can conduct progressive reviews of the space. The advantages of this type of mock-up are that the additional costs are minimal, and the progressive reviews will increase user confidence in the room design in preparation for the transition process. But, the disadvantages are that there are a limited number of changes that can be made at this point in the process, and access to the mock-ups are limited due to their location within a construction site.
Virtual Mock-Ups
The term virtual mock-up refers to computer-simulated virtual reality (VR) models. These virtual models allow users to experience the space via a computer screen or a special ocular headset which simulates the depth, scale, and distances of a proposed room in a format like a high-quality video game.
VR techniques allow users and members of the design team to visualize the proposed design early in the design process and, potentially, on a continuous basis throughout the process. It is a particularly good method to build trust in the users who may not be able to visualize a furnished and equipped three-dimensional space from a two-dimensional drawing. This technique allows clinicians and other users to view design simulation at a time convenient to them and submit individual comments or meet in a group to view the video simulation and discuss their findings in a structured focus group format.
Although less expensive and more flexible than a PMU, one disadvantage of VR mock-ups is that the testability of the space is limited, as users cannot simulate care delivery scenarios or test equipment and furnishings within the space.
Comparison of Mock-Up Techniques
Each of the mock-up techniques described is typically used in a different phase of the design process, as indicated in Figure 1. Although PMUs can be updated in several phases of the process, it is not as common or as easy as updating virtual models throughout the process.

Use of mock-ups during the design process.
In addition, each of the described mock-up techniques has different advantages and should be considered, as appropriate, in developing an approach to meet a specific client’s needs. Table 1 provides a comparison of mock-up techniques.
Comparison of Mock-Up Techniques.

Note. + = low; ++++ = high.
Case Studies: How Mock-Ups Have Been Used to Meet Specific Client Needs
The following case studies are examples of how mock-up techniques were customized or combined to meet the specific needs of a client such as providing input for decision-making, accelerating the design process, or developing new room types.
Case Study #1: Using Rapid Prototyping to Test a New Operational Concept
As part of a renovation project, an academic medical center wanted to explore the concept of a low-acuity emergency department (ED) cubicle that could expand using movable partitions from an individual cubicle sized to accommodate a single patient on a stretcher to a series of smaller cubicles that could accommodate patients in recliners or waiting in chairs. During the half-day rapid prototyping session setup in a conference room on campus, the group used sheets of cardboard, borrowed equipment, and readily available furniture to test their concept using group members as mock patients. With materials costing less than US$2,000, the half-day prototyping session resulted in a recommended size for the cubicle, several viable options for converting the cubicles to multiple occupancy spaces using movable partitions, a preliminary departmental layout, and equipment recommendations (see Figure 2 for an example of the rapid prototyping team testing the ED cubicle).
The prefabricated and flexible kit of mock-up parts allowed the team to assemble various mock-ups to test and vet the staff’s ideas. This was particularly useful as we were developing a design that is intended to adapt “on the fly” once constructed. (Facility Director of Architecture and Planning, mock-up participant)

Clinical care team testing their prototype of an ED cubicle.
Case Study #2: Using PMUs and VR to Accelerate the Design Process
The senior leadership at a community hospital wanted to accelerate the design process for a major addition, which included a surgery suite and bed tower by focusing on best practices in room design instead of spending significant user time in creating entirely new room configurations. This goal was achieved by developing a mock-up process that involved PMUs and VR models costing a total of approximately US$90,000.
PMUs
After the programming was completed, rough PMUs of key rooms, based on industry best practices, were constructed in a warehouse space. Users were asked to review the size and shape of the rooms and offer additional suggestions for improving the functionality of the rooms. This initial, very rough mock-up of the rooms provided the users with adequate information to validate the proposed size and configuration of the rooms, which, in turn, gave the team the confidence to proceed to the next step. Over time, the mock-ups were refined to provide more information to the users and support an ongoing approval process.
VR
Although the initial, rough mock-ups worked well for most room types, some users needed additional information to fully understand the space. For example, the surgery staff were used to old, undersized, and poorly configured operating rooms. A mock-up of a 625 ft2 operating room looked large but, due to the user’s frame of reference, it was difficult to envision how the room would be used. A VR mock-up was developed which allowed users to stand within the rough PMU of the OR and visualize, via a projected computer simulation or VR goggles, how the major equipment would be placed within the space. In addition to confirming the size and shape of the operating rooms, this added information allowed the surgical staff to provide input on other key issues such as where to locate the booms, placement of major equipment, and the optimum location of the circulating nurse’s workstation. Figure 3 illustrates how users can stand in the rough OR mock-up and using VR to visualize the layout of the finished OR space. The use of physical mock-ups afforded our clinical stakeholders the opportunity to spatially experience the various clinical rooms and confidently participate in their development and ultimate refinement. (Director of Facilities Planning, Design and Construction, mock-up participant)

Design team using a rough mock-up supplemented by virtual reality to study an operating room.
Figure 4 shows how a surgical staff member using VR goggles to experience a 3-D simulation of the OR within the mock-up. The use of the VR goggles helped me to see and think about how we could arrange the space to improve the comfort of our patients and make it easier for the clinical staff to care for patients. (Nurse, mock-up participant)

Operating room nurse using VR goggles to evaluate an operating room design.
Case Study #3: Using PMUs to Refine Room Designs and Generate Community Input
A community hospital used a unique mock-up approach to obtain input from users and to engage patients and community members in the design process. Mock-ups of the medical–surgical and ICU rooms were built in the lobby of the hospital, at a cost of approximately US$150,000. To obtain user input, department teams were asked to test the spaces using common patient care scenarios and their feedback was documented. This process led to shifting the location of the wall-mounted computers and a couple of other wall-mounted items as well as adjustments in the finishes. Due to the convenient location of the mock-ups in the hospital lobby, patients, families, and other community members were invited to tour the mock-ups and submit their feedback on a paper form which was reviewed by the design team. Although the mock-ups could not be left in the lobby long term, the members of the planning and design team felt this was a successful method to test the design and engage community members in the design process. The mock-ups made a huge difference. We caught things that saved us money and it allowed our staff and the public to participate in the process. I would never undertake a project of this size or magnitude without a mock-up. (CEO, mock-up participant)
Case Study #4: Creating Early Build-Out Mock-Ups to Obtain Final Sign-Off on Room Design
For a recently completed patient tower addition at an academic medical center, early build-out mock-ups of the medical–surgical rooms and the ICU rooms were developed after the building envelope was complete. Earlier in the process, key room mock-ups were constructed and evaluated in the construction trailer. The early build-out mock-up technique involved designating one medical–surgical room and one ICU room to be completed in advance of the other rooms on the respective units, thereby allowing progressive user reviews and final approval of the spaces. Because of this mock-up process, minor changes were made to the location of selected light switches and additional input was provided on the finishes. The additive cost to accelerate completion of these rooms was minimal, less than US$10,000, and the mock-up rooms became actual patient rooms in the completed facility. The advantage of the early build-out mock-up was providing the staff with the final look and feel of the room prior to finalizing hundreds of patient rooms. While the initial mock-ups defined the location for most items, it was not until the staff were in the actual, furnished patient room that they were fully able to envision the daily activities of patient care. This led to a couple of minor adjustments but, most importantly, it gave the staff the confidence that when they moved in, there would be no surprises. (Project architect, mock-up participant)
Case Study #5: Combining Rapid Prototyping and VR to Develop New Room Types
Similar to the initial rapid prototyping example, a comprehensive cancer center used the rapid prototyping process to define and explore two new room types being developed for its major cancer center project.
Care room
The “care room” was envisioned as a multiuse room in the outpatient clinic, allowing multiple caregivers to provide several types of care to the patient without requiring the patient to move to a different room or department.
Neighborhood infusion bays
In this concept, mock-ups were used to test a new operational concept in which the infusion bays are grouped into neighborhoods with a single care team and support areas rather than a large room with centralized staff and support areas. The goal of the mock-up was to test whether this concept would meet the patient’s needs and be more functional for staff. Two mock-up methods were used to assist the planning team in designing and testing the space and operations of these two new room types.
Rapid prototyping
Rough, rapid prototypes for each area were developed using semimovable walls, test furnishings, cabinetry indicated by tape on the walls, and accessories made from cardboard. Next, staff and design team members simulated patient care scenarios in the space to test the rooms. Ideas and suggestions were recorded with handwritten notes taped to the walls. At the completion of this exercise, the group had confidence that the basic design for both of their new room types would meet the needs of the patients and was operationally efficient. Figure 5 illustrates staff and design team members using rapid prototyping to test the care room.

Staff and design team evaluating a rapid prototype model.
VR
Next, to introduce a larger group of potential users to these new room types, the design team developed a VR experience that simulated walking into the fully furnished and equipped rooms. A total of 450 users were provided with low-fidelity VR goggles, made from a cardboard box with two lenses. Then, when the users inserted their smartphone in the cardboard goggles and watched the provided video, they saw a 3-D VR mock-up of the rooms. Users were encouraged to experience the VR simulation and, then, meet in small groups to discuss their impressions of the spaces and share ideas for improvement. The suggestions were evaluated, the necessary refinements were made, and the design progressed to the next phase knowing that many users had a realistic understanding of the operational model and space associated with the new room types. Figure 6 illustrates one of 450 pairs of cardboard VR goggles distributed to users to view the VR mock-ups. We are realizing the numerous dividends from the virtual reality process. (Administrative Director of the Cancer Center, mock-up participant)

Cardboard VR goggles used to view VR mock-ups.
Mock-Up Planning and Logistics
These case studies demonstrate the successful outcomes of the mock-up process; however, considerable planning and coordination are required to execute a successful mock-up process.
Key Tasks in Executing a Sucessful Mock-Up Process
Documenting client goals
Before deciding on a technique, the client’s goals or the information to be gleaned from the mock-up process needs to be determined. Then, this information should be used to select the most appropriate mock-up technique. The case studies presented illustrate the wide variety of client goals and, as a result, a variety of mock-up approaches.
Deciding what to mock-up
Typically, rooms that are frequently repeated such as inpatient rooms or high-tech, expensive rooms, such as operating rooms, are mocked up. Organizations that want to focus on medication safety may choose to mock-up a medication room, or some organizations may mock-up an entire department, such as a nursing unit or ED to study functional relationships (Williams et al., 2017). It should be noted that when an entire department is mocked-up, low-fidelity materials such as cardboard are typically used while individual room mock-ups may consist of higher fidelity construction materials.
Identifying the right technique
There is no one right mock-up technique for a specific situation. Instead, it is most important to identify the right mock-up technique to evaluate the identified project goals or objectives (Bayramzadeh et al., 2018). Andersen and Broberg (2015) compared a full-scale mock-up to a low-fidelity tabletop mock-up in evaluating six ergonomic conditions. The findings demonstrated that the full-scale model was more successful in evaluating technology, tools, and space, while the rough tabletop model was more successful in evaluating organizational issues, thereby illustrating that the mock-up technique depends on the goals or objectives to be evaluated for a project (Andersen & Broberg, 2015).
Developing an evaluation process
Unfortunately, mock-ups are often used to obtain an overall like or dislike for the space as opposed to rigorously testing and evaluating EBD strategies (Watkins et al., 2008). To maximize the value of a mock-up, a very specific evaluation process must be identified for collecting, analyzing, and implementing the findings. A structured evaluation process prevents one person’s suggestion from being implemented without considering the overall project goals and the initial basis for specific decisions. Although obtaining information via individual comments or a questionnaire is acceptable, the following are examples of more robust, research-focused approaches: (1) questionnaires with closed questions and open responses followed by structured focus groups (Watkins, Kobelia, Peavey, Thomas, & Lyon, 2011), (2) observations supplemented with recorded interviews (Kasali, Nersessian, & Zimring, 2013), and (3) formal simulation of patient care scenarios conducted by staff which may be evaluated through videotaping or visual observation and, then, discussed in debriefing sessions (Bayramzadeh et al., 2018).
Planning the logistics
To reap the benefits of a mock-up, time needs to be invested in finding the appropriate space, assembling materials, inviting participants, and planning how the mock-up will be used. A well-orchestrated mock-up process will show respect for the user’s and design team’s time. It is important to pay attention to the particpants and make them feel comfortable by introducing them to each other and ensuring they are participating. After the mock-up session, participants should be provided with feedback and thanked for their participation (Durham, 2014). Table 2 compares the logistics to support mock-ups and summarizes these and other logistical considerations for the planning and execution of different types of mock-up evaluations.
Comparison of Logistics to Support Mock-Ups.
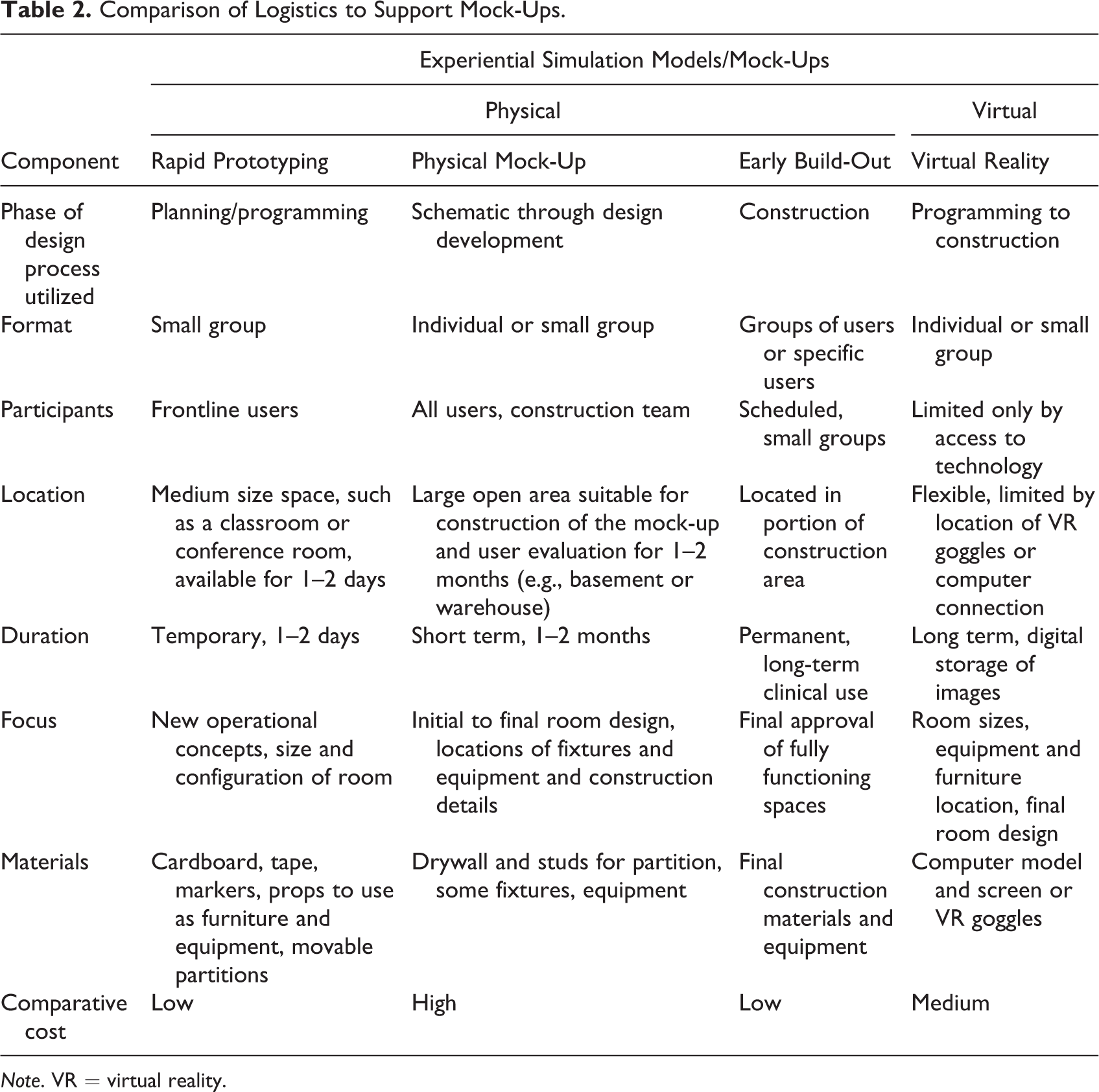
Note. VR = virtual reality.
Conclusions
Mock-ups require a significant investment of time and resources, but they are perceived as helpful and valuable. A study by Keys, Silverman, and Evans (2016) indicated that the groups included in the survey found mock-up process to be beneficial: architects found the mock-up process to be a critical communication tool that is best initiated early in the design process, clinicians found the repeated refinement and testing that occurs in a full-size mock-up to be valuable, construction and project managers enjoyed the interaction with the users and felt that even simple mock-ups such as tape on the floor were valuable, and hospital and nurse administrators felt the mock-ups process ensured the staff and the architects shared a common vision (Keys, Silverman, & Evans, 2016).
In summary, using numerous types and combinations of mock-ups in the process of designing healthcare spaces has been found to be very beneficial. The existing types of ESMs or mock-ups, both physical and virtual, have evolved over the last decade and will continue to do so as new technology and healthcare delivery methods evolve. As new mock-up techniques and utilizations continue to grow, it is hoped, as suggested by Watkins et al. (2008), that the use of mock-ups as interactive laboratories to conduct research studies will increase and, thereby, expand the healthcare design knowledge base (Watkins et al., 2008). Experience has shown that the findings from mock-up experiences increase user and design team confidence in the decision-making process and facilitates the successful execution of new operational concepts.
Implications for Practice
Successful mock-ups require significant, detailed planning, coordination of time and resources, and collaboration among professional end users, designers, and decision makers. Mock-ups have been perceived as beneficial in the translation of a design concept or idea to the physical or virtual realm making it easier for professional end users to understand, test, and revise the proposed physical space before construction. The type of mock-up used should be determined by the cost/budget, time/schedule, risk/benefit, and the level of detail required to make the best possible decision in the design of a space, unit/department, or entire patient care unit. Spaces that will be duplicated multiple times (patient rooms, patient care units) in a new facility or “expensive spaces” (operating room, imaging room) benefit from the mock-up process as it allows testing of the function of the room and validation of the details of the room prior to construction.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received support from SmithGroup in preparing this article.