
Abstract
Objectives:
This research aims to explore the perceptions of nursing staff regarding the effects of daylighting on behavioral factors including mood, stress, satisfaction, medical error, and efficiency.
Background:
In spite of an extensive body of literature seeking to investigate the impact of daylighting on patients, a limited number of studies have been done for the sake of nurses’ perceptions and behavioral responses.
Method:
A mixed-methods approach, comprised of qualitative explorations (structured interviews) and a validated survey, was applied and the results were compared and triangulated. Five nurses were interviewed and 156 nurses volunteered for a lighting survey from six departments of three inpatient facilities in Iran.
Results:
The findings of this study are consistent with the existing evidence that daylighting and view to the outside enhance nurses’ perceptions regarding satisfaction, mood, stress, medical error, and alertness, while reducing fatigue and stress.
Conclusion:
Patient rooms and work stations are the most crucial areas to provide daylighting from nurses’ perspectives.
A growing body of evidence supports the idea that environmental design considerations have been one of the major factors to promote occupants’ behavior (e.g., Bazuin, & Cardon, 2011; Gharaveis, Hamilton, Pati, & Shepley, 2018a, 2018b; Hamilton & Shepley, 2010; Ulrich et al., 2008). Daylighting has been regarded as an important environmental factor to impact building users. This impact can be divided into a wide range including physiological and psychological aspects (Andersen, Gochenour, & Lockley, 2013; Araji & Boubekri, 2011; Barroso & den Brinker, 2013; Boubekri & Wang, 2012; Gharaveis, Shepley, & Gaines, 2016). In this respect, the impact of daylighting on patients’ behavior including mood, stress, and satisfaction has been investigated and supported by previous studies (Alzoubi, Al-Rqaibat, & Bataineh, 2010; Gharaveis & Kazem-Zadeh, 2018; Hua, Oswald, & Yang, 2011; Joseph, 2006; Ulrich et al., 2008).
In spite of long hours of staff presence in healthcare facilities, most of the existing studies and design considerations with respect to the impact of daylighting and view to the outside on behavior have been focused on patients. Poor lighting impacts the healthcare workers’ performance and correlates with medical errors (Buchanan, Barker, Gibson, Jiang, & Pearson, 1991; Mahmood, Chaudhury, & Valenete, 2009). Stichler (2001) emphasized the impact of different elements on enhancements of staff as well as patients’ needs. Also, Joseph and Rashid (2007) found that a poorly designed physical environment has latent consequences including staff stress, fatigue, and burnout. In a systematic review, Ulrich et al. (2008) referred to the impact of lighting on staff mood. Furthermore, Salonen et al. (2013) stated a comprehensive list of daylighting effects on behavior, including reduction of stress, errors, absenteeism, depression, and fatigue as well as improvement of performance, attitudes, mood, and job satisfaction.
View to the outside is another byproduct of window presence in healthcare facilities. In a classic study, Ulrich (1984) found the content of view to the outside impacts different clinical outcomes, and this study was supported by the finding of a more recent study by Zadeh, Shepley, Williams, and Chung (2014). Gharaveis, Shepley, and Gaines (2016) conducted an exploratory study on the residents of two long-term rehabilitation facilities and found the positive impact of a view to the outside on long-term residents’ mood, satisfaction, stress, and perception. A related study was conducted in inpatient units regarding beneficial effects of lighting on treatment process and recovery time (Lo Verso, Aghemo, & Caffaro, 2016).
Significance of the Study
Despite the current healthcare design literature supporting the impact of daylighting and view outside on patients, this study addressed the gap in the literature for potential effects of daylighting and view to the outside on nurses in inpatient facilities—specifically in the nurse stations, staff break areas, and public spaces. The focus of this study was on the practical design perspectives of healthcare designers and planners. Daylighting is defined in this study as the illumination of buildings by natural light.
Research Questions
This article is based on the findings of the previous phase of this research, which was conducted by the lead author and the researchers’ experiences in designing healthcare facilities. This investigation is about the potential impact of windows on nurses’ perceptions about behavioral factors in inpatient facilities. The research subquestions were as follows: What is the most important reason for a window in inpatient units—access to daylight or having a view to the outside? Is there any difference between the needs for daylighting in intensive care and patient units? What are the most important places for staff to have daylighting? Is there any significant correlation between daylighting distribution and glare? According to the perceptions of the nurses, what behavioral factors are impacted by daylight: stress, fatigue, comfort, satisfaction, medical error, or general clinical efficiency? What is the best placement of windows with respect to the placement of patient beds?
Method
This cross-sectional study used a mixed-methods approach, including both qualitative and quantitative data. Daylighting and view to the outside were regarded as environmental factors, and nurses’ perceptions regarding behavioral factors (mood, alertness, stress, and comfort) were considered dependent variables. The study protocol was reviewed and approved by the Institutional Review Board at the home institute of the lead author.
Study Settings
Within the study’s targeted metropolitan area (located in Tabriz, East Azerbaijan, Iran), only one major healthcare system agreed to participate in this study. The system had three community hospitals with similar size patient and intensive care units (ICUs), and the participants were selected from the six departments (see Figure 1). Site 1 had seven ICU beds and eight patient beds. Site 2 had 7 ICU beds and 12 patient beds. Site 3 had 8 ICU beds and 12 patient beds. The selection of all the sites from a single system minimized the potential impact of other factors, since all the sites were operated by the same organization, located in the same geographical area, and had fewer logistical variations.
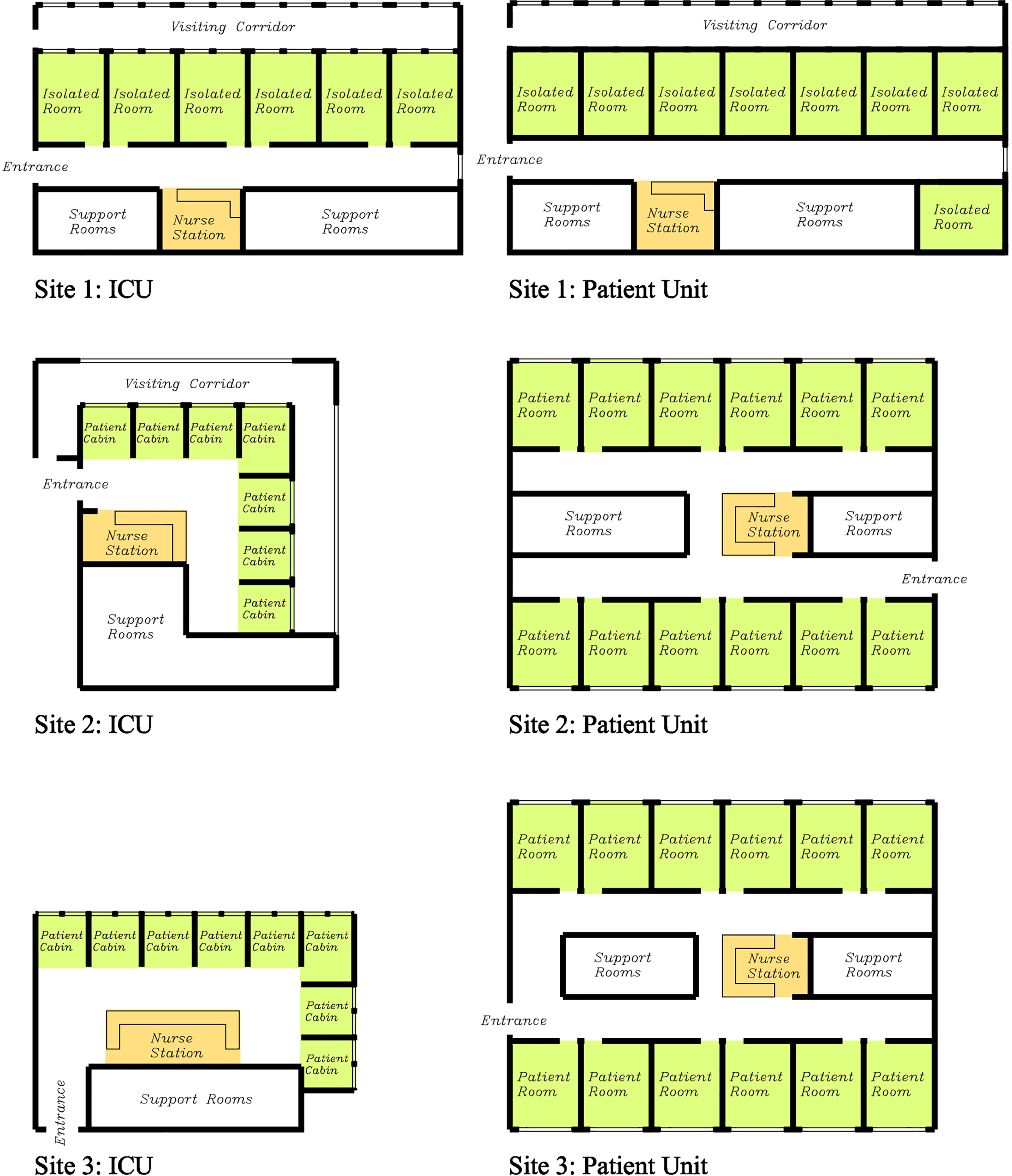
Study sites’ floor plans.
Daylighting was provided for all the patient rooms. Despite the similarity of patient room size (see Table 1) in all the departments, the accessibility to windows, size, and locations of the windows as well as the contents of view were slightly different (see Figure 2 and Table 2). No daylighting was provided in the staff area and public spaces inside patient unit and ICU.
Room Dimensions in Different Facilities.
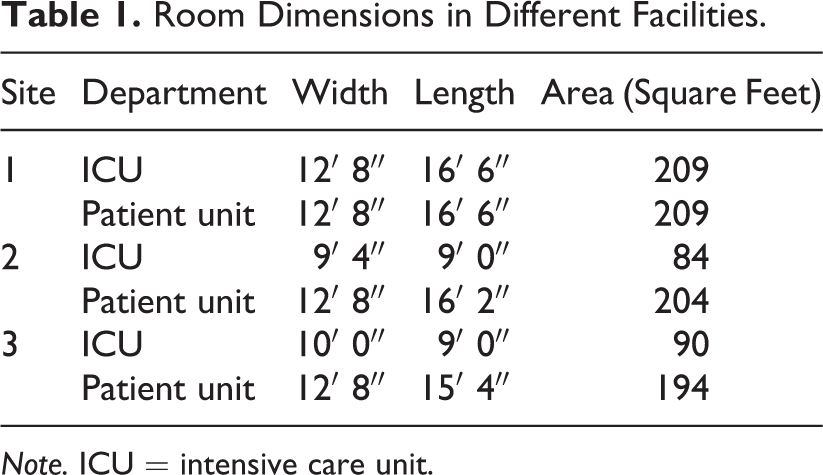
Note. ICU = intensive care unit.
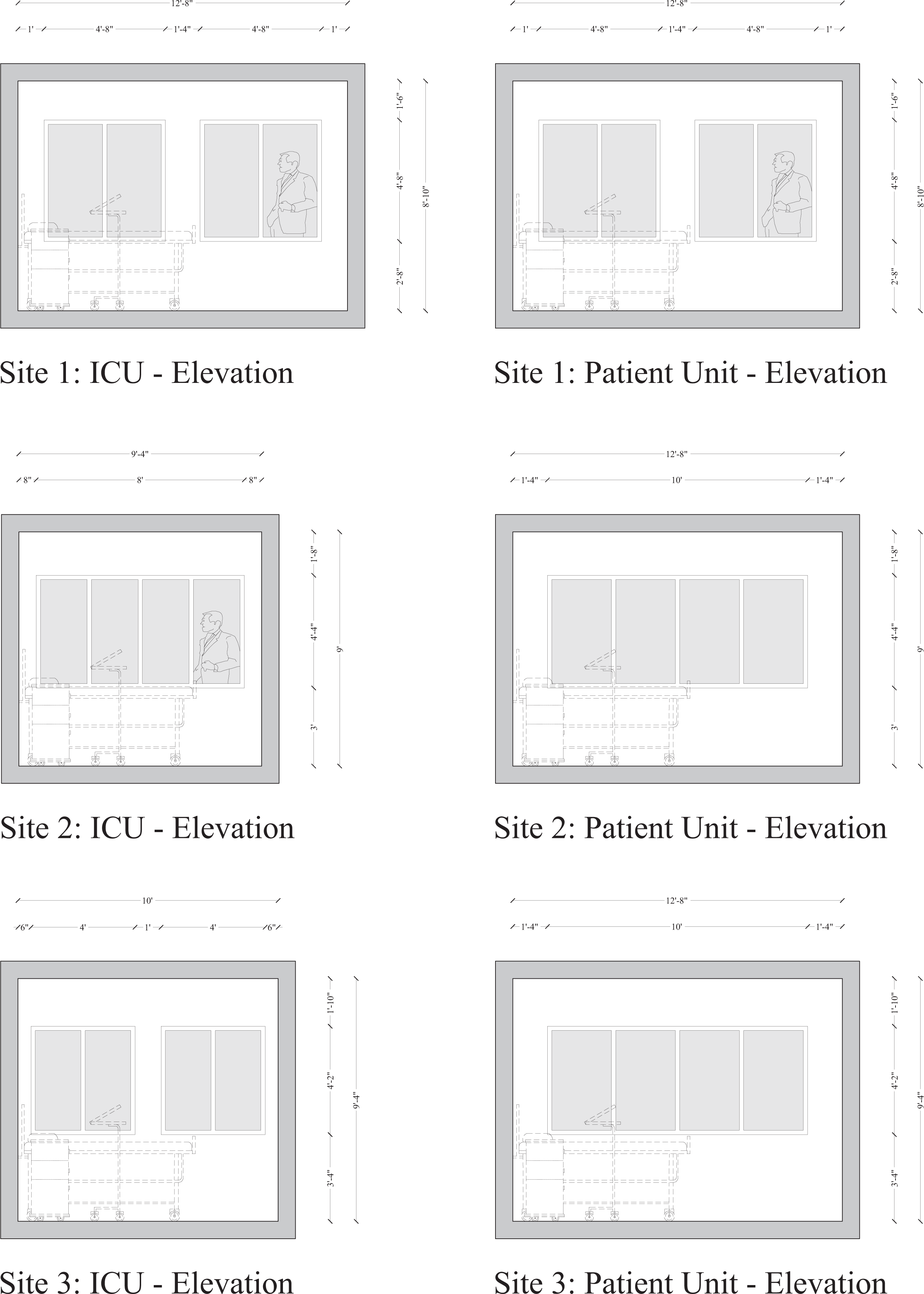
The study sites elevations.
Window Dimensions in Different Facilities.
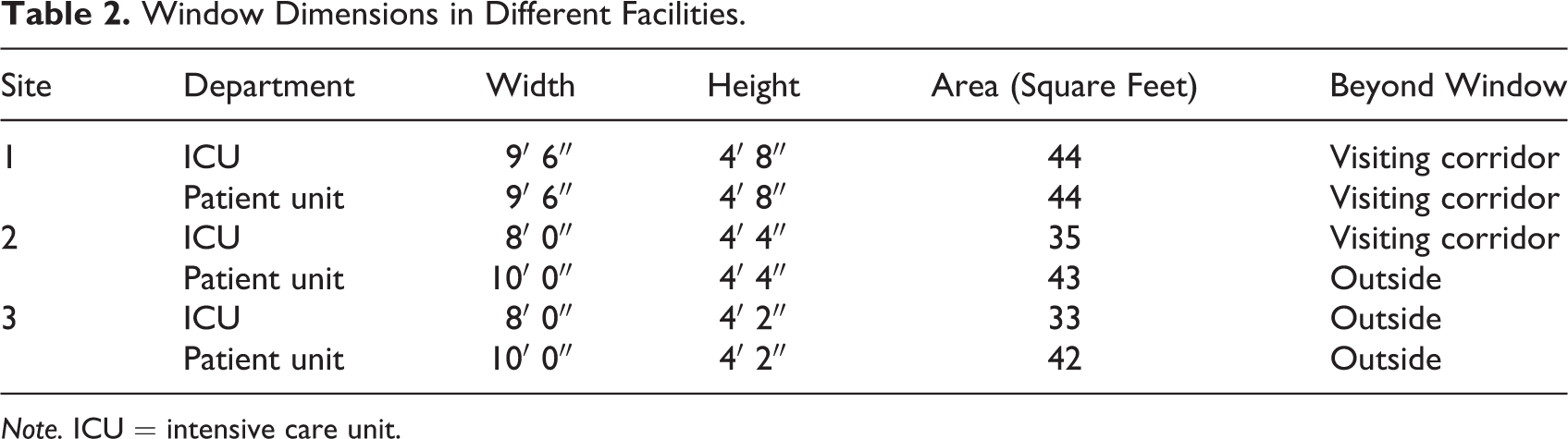
Note. ICU = intensive care unit.
Sources of Data
The questions for qualitative and quantitative components of this study explored similar concepts. Nurses from inpatient units (both patient and intensive care) were interviewed to provide in-depth insight and a better understanding of the research topic. The quantitative method (a written validated and psychometrically tested survey) was used to investigate the perceptions of the participants among a larger population sample.
Qualitative data
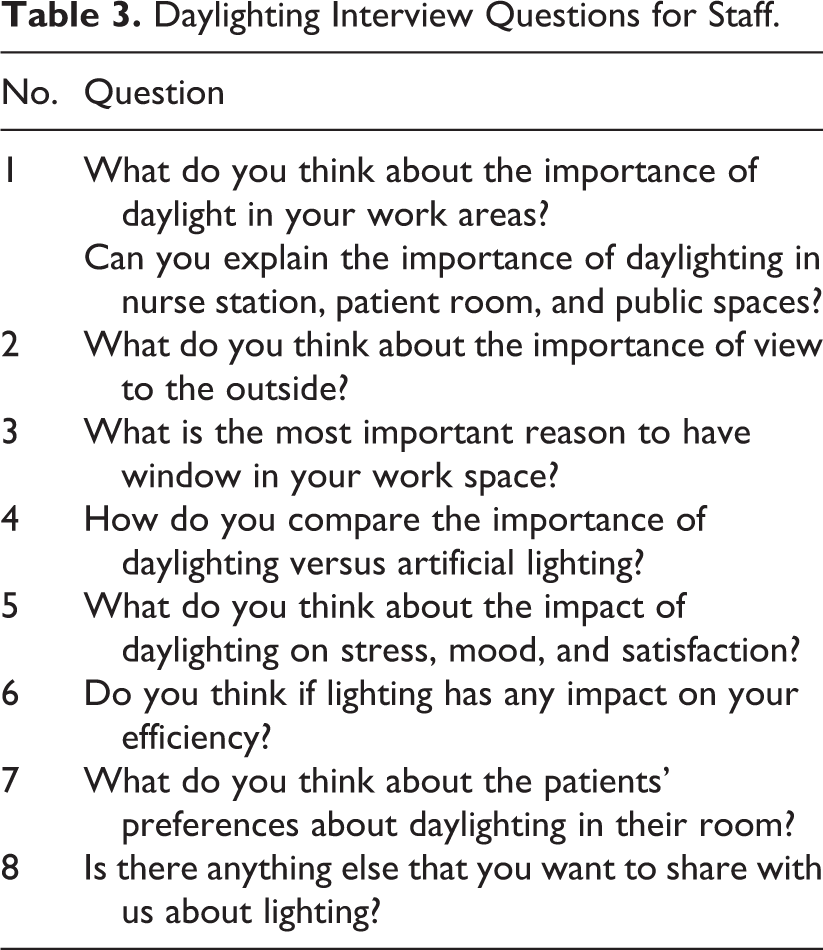
The interviews were conducted in a non-English language (Persian). Based on the lead author’s previous published study regarding patients’ perceptions, the interview questions were drafted according to the framework of this study (see Table 3). The interview questions were reviewed by all the authors for clarity. The changes were made before translating the questions to Persian. The translated questions were reviewed by three nondesigners. Finally, the interview questionnaire was designed with 10 open-ended questions to develop an in-depth understanding of (a) how nursing staff perceive accessibility to daylighting and view outside, (b) how they define their environmental needs/preferences with respect to their behaviors, and (c) their preferences in placement of windows.
Daylighting Interview Questions for Staff.
Quantitative data
The survey instrument used in this study was validated and self-developed in a pilot study in June 2016. The initial list of questions was based on a questionnaire that was developed by the lead author in a published work regarding patients. The questions were revised for the purpose of this study to explore nurses’ perspectives. A statistical analysis was conducted to verify the survey tool validity, applicability, and adoptability in healthcare facilities with the assistance of a convenience sample of respondents. The respondents included registered nurses with more than 3 years of work experience in healthcare facilities. A total of 15 nurses (3 male and 12 female, mean age of 39.21 years, mean job experience of 9.75 years) responded to the lighting survey. The feasibility of the survey forms was evaluated by examining the percentage of missing values. None of the questions were skipped by more than one respondent. The researchers examined the skipped questions and typing errors were found. A reliability test (the Cronbach’s α) was conducted based on the range of measurement to measure internal consistency and scale reliability. The Cronbach’s α was .88, which was in the acceptable range (viable scores on this test are generally considered to be anything greater than .70).
Once the survey instrument was validated, the bilingual researchers translated the survey to the participants’ language in the destination country (from English to Persian). For clarity, the translated survey was reviewed by three volunteers who were not architects and designers. The survey included 34 questions, both open- and closed-ended, divided into five sections: (a) demographic information including age, gender, job experience, and working department; (b) general lighting questions and accessibility windows; (c) perceptions about visual comfort; (d) usability in the clinical setting; and (e) improvement of lighting and view outside.
Sampling
Qualitative data
To identify interview participants, the researchers toured the facilities and discussed the research ideas with each department’s management. The sampling strategy to select participants was homogeneous convenient sampling. The initial inclusion criterion before the recruitment was to have worked at least for 3 years in inpatient facilities as a registered nurse. The research team prioritized the most eligible nurses, according to their years of experience. From 16 registered nurses who volunteered to be interviewed, 10 nurses from both inpatient units (5 nurses from patient units and 5 from intensive care) were selected. All the nurses were female and preferred not to disclose their ages. After conducting five individual interviews (two in person and three by phone), the researchers could not find any variations and new perspectives in the collected data—saturation was reached—and no more interviews were conducted (Saumure & Given, 2008).
Quantitative data
In regard to the survey participants, hard copies of the questionnaires were provided to the management system of all the sites. According to the data obtained from the management, 327 nurses were in six departments. Overall, 156 registered nurses (77 from intensive care and 79 from patient unit) from three facilities volunteered to take the survey (48% participation).
Data Collection
The data were collected for both methods concurrently and all the data collection processes were performed in January and February 2017. For interviews, upon the requests of the participants, no audio or video was recorded. The three researchers with a healthcare design background were taking notes during the interviews. After each interview session, all the interview notes were typed for further analysis. The content analysis was used to code and organize the data into mutually exclusive and exhaustive categories. With respect to the surveys, hard copies were provided to the management of each site, and the volunteers dropped off the filled-out surveys to the director’s office. The researchers inserted the collected survey values into Excel twice for consistency.
Data Analysis
Qualitative data
The investigators operated a word content analysis technique to collate ideas. The interview data analysis began after inserting all written responses into Excel 2016, and the content/theme analysis was based on the principles of naturalistic inquiry (Lincoln & Guba, 1985). Interview transcripts were prepared in the destination language for analysis after separating all the data units. A data unit was defined as “a piece of information in an interview that can stand alone and make sense” (Y. Lincoln, personal communication, February 27, 2015). All the units were read through twice by the lead author before coding. The statements were summarized to code the transcripts. The similar codes were clustered together to emerge themes. For more clarification, subthemes were created and titled based on different themes and subthemes. Finally, nonsaturated ideas and codes were deleted (Emerson, Fretz, & Shaw, 2011). Because the interviews were conducted in a different language, direct quotes were not addressed in this article.
Quantitative data
The statistical analysis of the quantitative data began using SPSS, Version 23, which involved the rating of options and preferences, using both descriptive and inferential statistics. Descriptive statistics clarified the nurses’ perceptions about the most important reason for having windows, the most critical places to have daylighting, and the impact of daylighting on the focused behaviors (mood, alertness, stress, comfort, and efficiency). Different ratings were compared and results were reported. For inferential statistics, since the collected data were normally distributed, parametric tests were performed for two purposes: exploring the similarities and dissimilarities between patient and ICUs by conducting a t test and investigating the correlations between the perception of light distribution and glare by regression analysis.
Results
Interviews
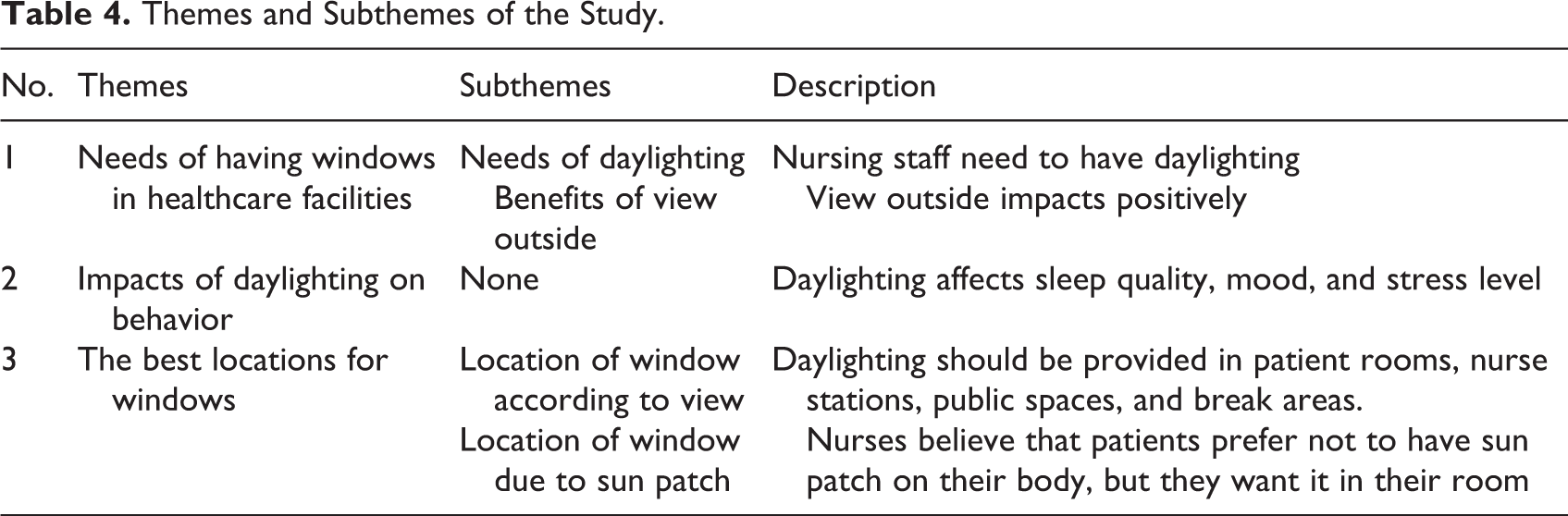
The study participants endorsed the value of accessibility to windows in healthcare facilities for both having a view to the outside and benefiting from daylighting with respect to their perceptions of behaviors. Three major themes and five subthemes were generated after categorizing different data units. Based on the research inquiries, respondents believed that having windows in healthcare facilities is a requirement and should be considered in different spaces that are used by staff. The participants shared the ideas regarding different behavioral effects of daylighting and view outside according to their preferences, perceptions, and experience. Visual accessibility to outside and benefiting from daylighting for nursing staff may lead to higher clinical and behavioral influences in healthcare facilities (see Table 4).
Themes and Subthemes of the Study.
Theme 1: Needs of having windows in healthcare facilities
Daylighting is required for staff, and nurses believe that it is critical for nursing profession. The nursing staff stated the needs of having windows in multiple locations of different facilities to have a view to the outside.
Subtheme 1: The impact of daylighting
Staff referred to different impacts of daylighting on their behavior and clinical outcomes (see Table 5). Many factors were referred to more frequently than others, which might show the importance.
Factors Associated With Daylighting From Staff Perspective in Inpatient Units.
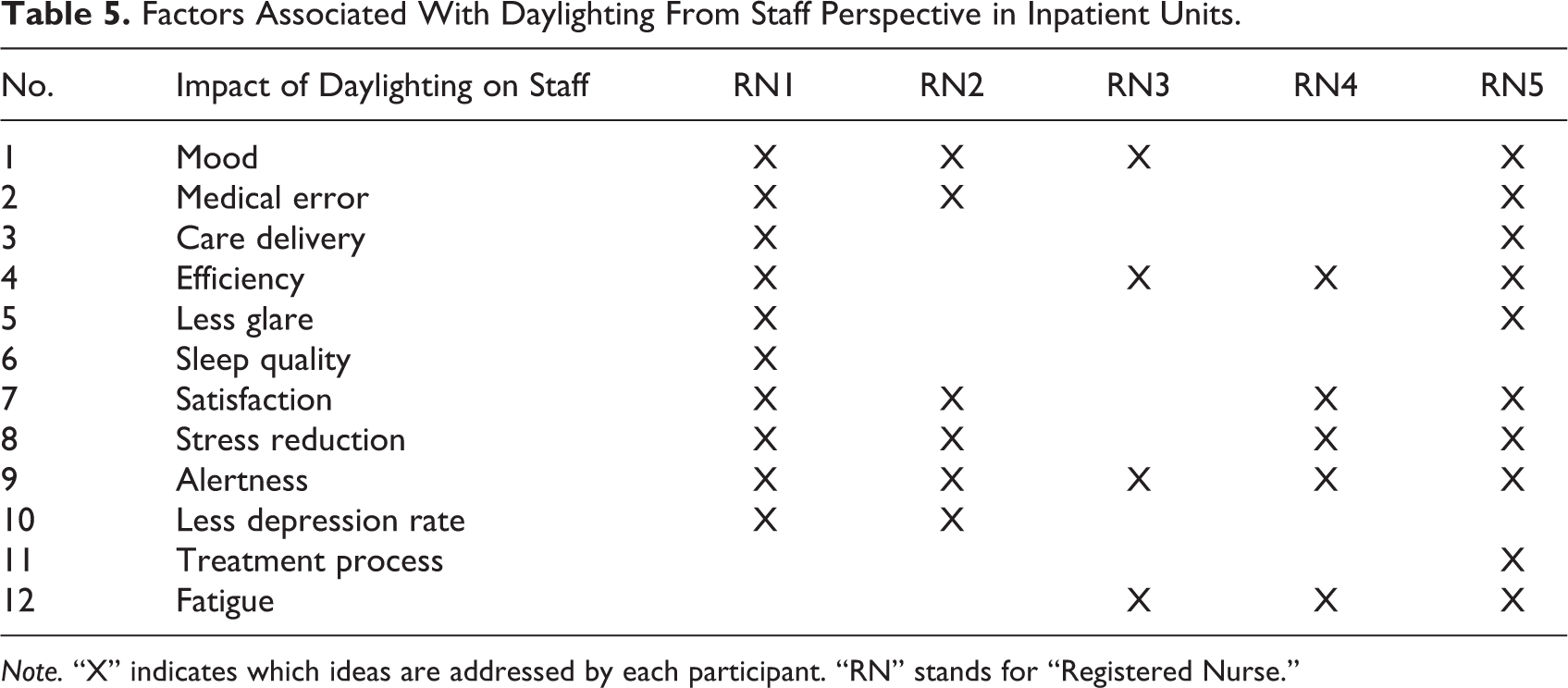
Note. “X” indicates which ideas are addressed by each participant. “RN” stands for “Registered Nurse.”
Subtheme 2: The impact of view to the outside
View to the outside in hospitals was important for staff, and they stated their perception of the importance for patients and their families. Three of the participants reported that view to the outside impacts both nurses’ and patients’ mood in healthcare facilities. One of the most functional reasons for having windows is the provision of view to the outside rather than just having daylighting. It was mentioned that staff mood can be promoted by having a view to the outside.
Theme 2: Benefits of daylighting for patients
Staff noted that insufficient lighting may lead to patient falls, stress, and high depression rates. In contrast, appropriate lighting promotes staff’s mood, satisfaction, and alertness as well as treatment process of their patients (see Table 6). Two of the nurses mentioned multiple behavioral factors of daylighting, while others only emphasized one. Additionally, participants believed glare would cause injuries to their eyes. So, lighting should be appropriate in order to promote efficiency.
Factors Associated With Daylighting on Staff in Inpatient Units.
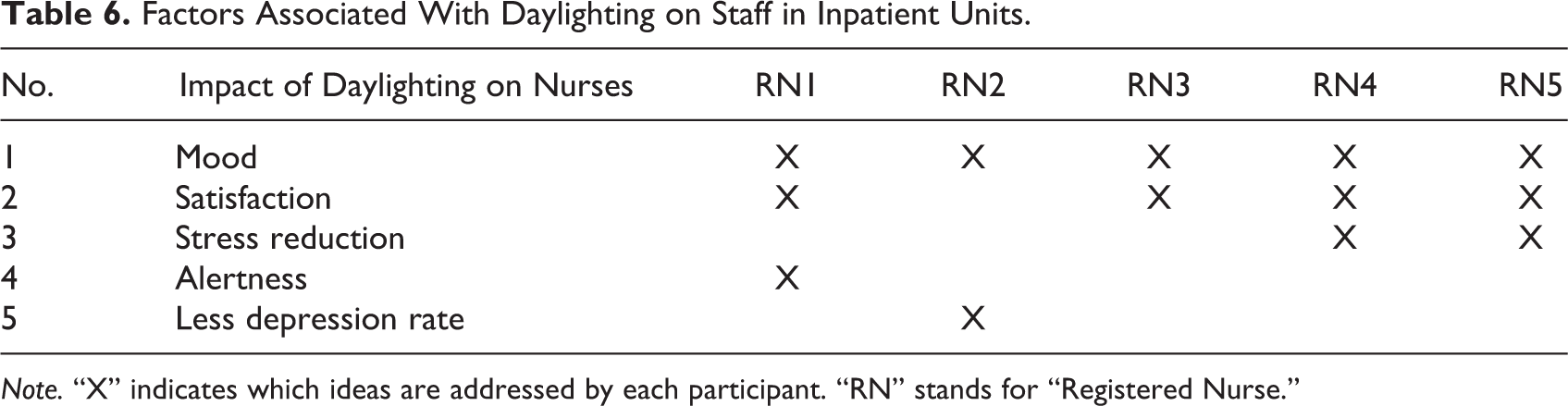
Note. “X” indicates which ideas are addressed by each participant. “RN” stands for “Registered Nurse.”
Theme 3: Window location in healthcare facilities
Having windows in all the spaces, if possible, was addressed in the interviews by the nurses. Also, specific locations of windows in patient rooms were noted by the participants to have a better lighting and view to the outside for both patients and staff.
Subtheme 1: Different locations of windows in healthcare facilities
Nurses asserted that they understand because of the complexity of healthcare facilities, providing daylighting in every space is challenging. However, they stated that daylighting should be provided in patient rooms, nurse stations, public spaces, and staff break areas. The respondents emphasized the significance of window presence next to the nurse station, since the staff stay there for a long time.
Subtheme 2. Location of the window in patient rooms due to the location of sun patch
Direct lighting inside rooms may cause patient dissatisfaction because it heats up the room and causes glare. Staff believed patients prefer to have windows next to them to have a view to the outside without being in direct sunlight.
Written Surveys
Demographic information shows that 111 female and 43 male registered nurses volunteered in this research. The average age of the participants was approximately 34 years, while average job experience was 7.56 years in inpatient healthcare facilities. In regard to different questions, quantitative data analysis was conducted accordingly. Research Question 1: What is the most important reason for a window in inpatient units—access to daylight or having a view to the outside? All the nurses who took the survey responded to this question. Descriptive statistical analysis showed 98 nurses (63%) selected daylighting as the most functional reason for windows in their facilities, while 58 participants (37%) marked the view to the outside as the most important reason for providing windows. The responses in patient and intensive units were similar.
Research Question 2: Is there any difference between the needs for daylighting in intensive care and patient units? The data distribution was explored with the Kolmogorov–Smirnov and Shapiro–Wilk tests, and the results showed there was a normal distribution (p < .05). As such, the parametric test (t test) was performed to answer the research subquestion. The test results showed the difference in importance of daylighting in intensive care and patient units was statistically significant and the need in intensive care was higher (4.14 of 5 for intensive care and 4.12 of 5 for patient unit; see Table 7).
The Comparison Between ICU and Patient Unit in Three Facilities.
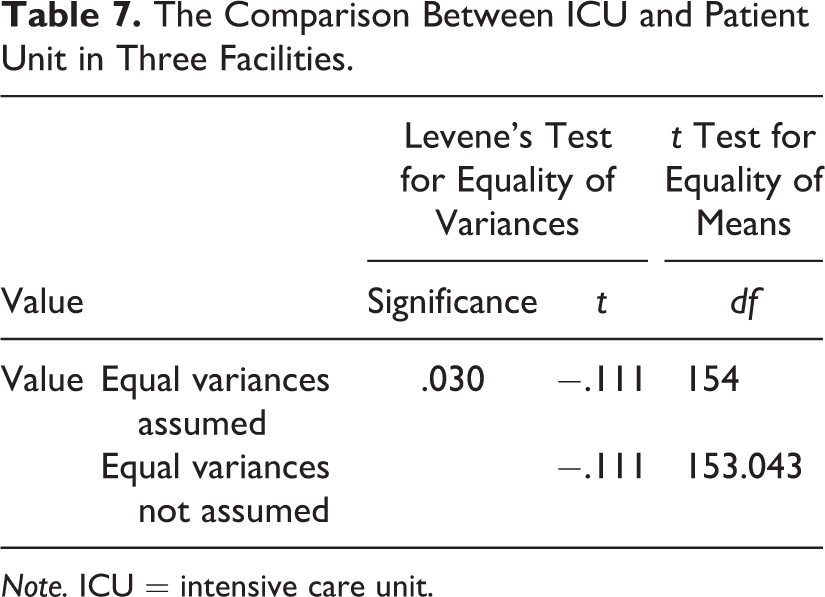
Note. ICU = intensive care unit.
Research Question 3: Where are the most important places for staff to have daylighting? Due to descriptive statistical analysis, the preferences of the nurses in three units were ranked. According to the nurses’ preferences, having windows in patient rooms had the highest importance. The second important location was near nurse stations and should be provided for the sake of nurses’ efficiency and preferences. The third preferred locations were the hallways and the places with task lighting sources (see Table 8).
The Importance of Different Locations’ Ranking in Daylighting Importance.
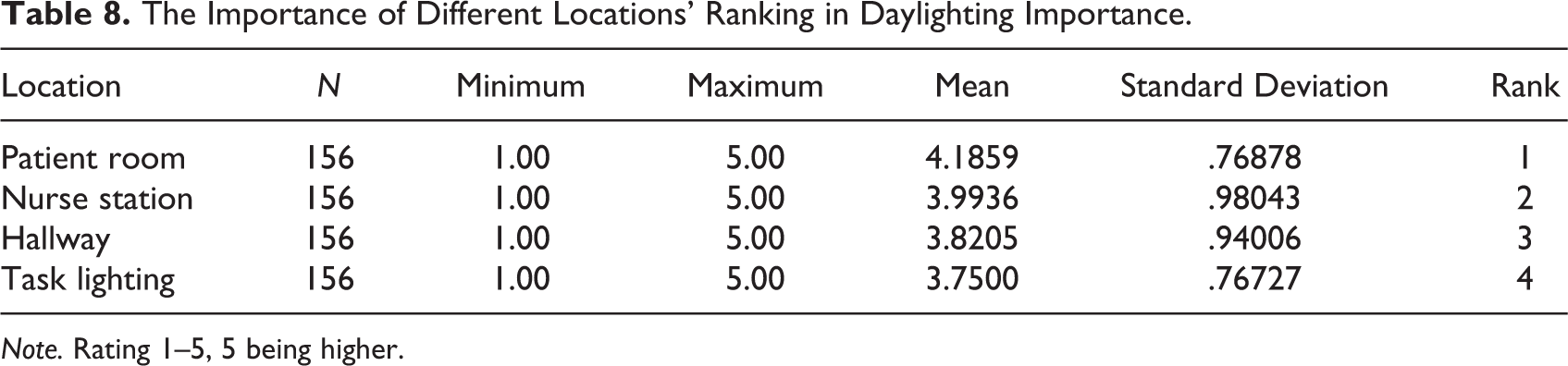
Note. Rating 1–5, 5 being higher.
The preferences for importance of view to the outside in different locations were asked from the participants. The most addressed places were (a) nurse stations (123 times), (b) patient rooms (71 times), (c) medication and supply rooms (57 times), and (d) charting spaces (43 times). Research Question 4: Is there any correlation between daylighting distribution and glare? In order to investigate the correlation between lighting distribution and glare in different departments and settings, the distribution of ratings regarding lighting and glare were explored by the Kolmogorov–Smirnov and Shapiro–Wilk tests, and data were normally distributed. A regression test was performed and the result showed there was a correlation between lighting distribution and glare with the p value of .000. The R2 value was .294 (see Table 9).
Regression Analysis Test Result.
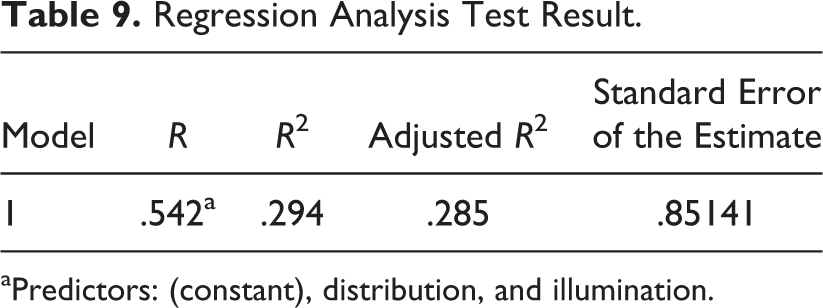
aPredictors: (constant), distribution, and illumination.
Research Question 5: According to the perceptions of the nurses, what behavioral factors are impacted by daylight: stress, fatigue, comfort, satisfaction, medical error, or general clinical efficiency? The participants selected the behaviors that they perceived to be highly impacted by daylighting. According to descriptive statistical analysis, daylighting has been perceived to have the highest impact on mood (3.99 of 5). The second choice was the impact of daylighting on satisfaction (3.97). According to the data, daylighting had the lowest impact on comfort (3.93) and staff stress (3.80; see Table 10).
The Comparison Between Different Behavioral Factors (Satisfaction, Mood, Stress, and Comfort) in Terms of Being Affected by Daylighting.
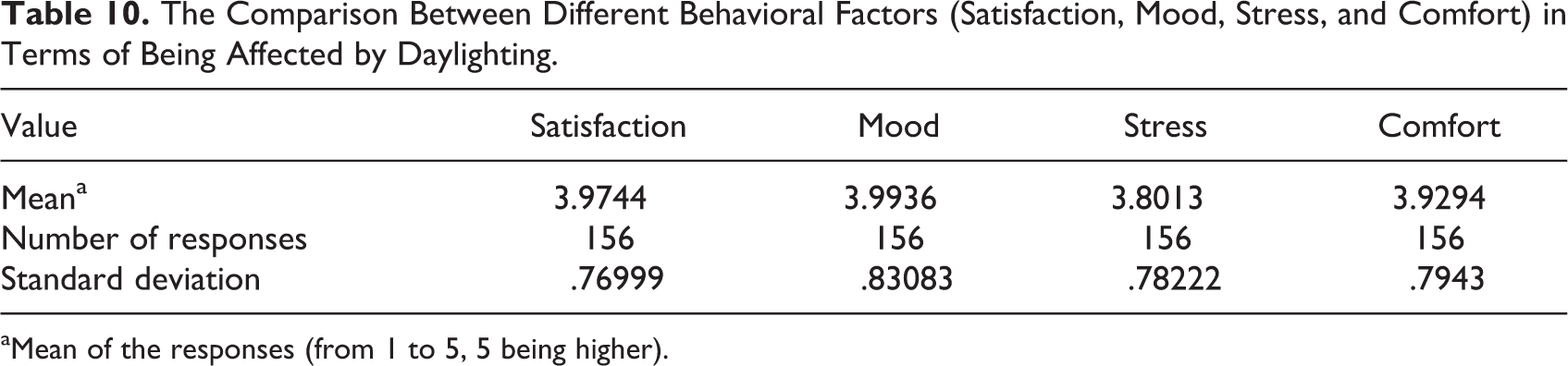
aMean of the responses (from 1 to 5, 5 being higher).
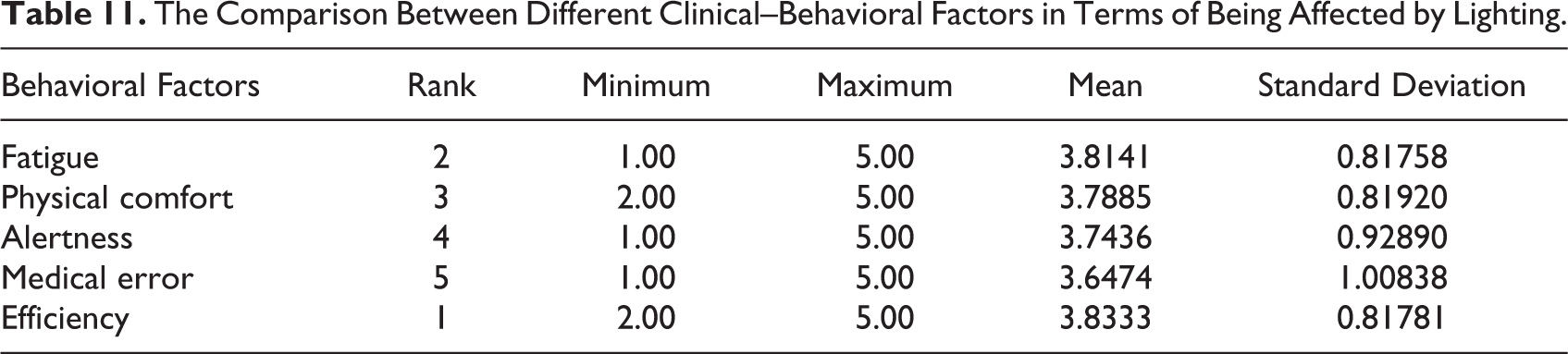
In a similar fashion, the staff were asked to select one among the behaviors (fatigue, physical comfort, alertness, medical error, and clinical efficiency) that they perceive to be impacted higher by daylighting. The results showed lighting had the highest impact on clinical efficiency (3.83 of 5) and lowest impact on medical error (3.65 of 5). For more details of the responses, see Table 11.
The Comparison Between Different Clinical–Behavioral Factors in Terms of Being Affected by Lighting.
Research Question 6: What is the preferred placement of windows with respect to the placement of patient beds? In order to investigate the best location of windows in the patient rooms, this study applied two approaches. First, respondents were asked about their preferences directly. In total, 155 of the participants responded to this question; 88 nurses (56.77%) perceived having windows in front of the bed would be the best location. Additionally, this question was explored in a different way by asking the nurses about their ideas regarding the placement of sun patch in the patient rooms. The majority of the respondents (75.44%) perceived having the sun patch off the bed is preferred (see Figure 3; Option B). This indicates the best location of the window is where patients have view to the outside while it would be close to the foot of the bed.
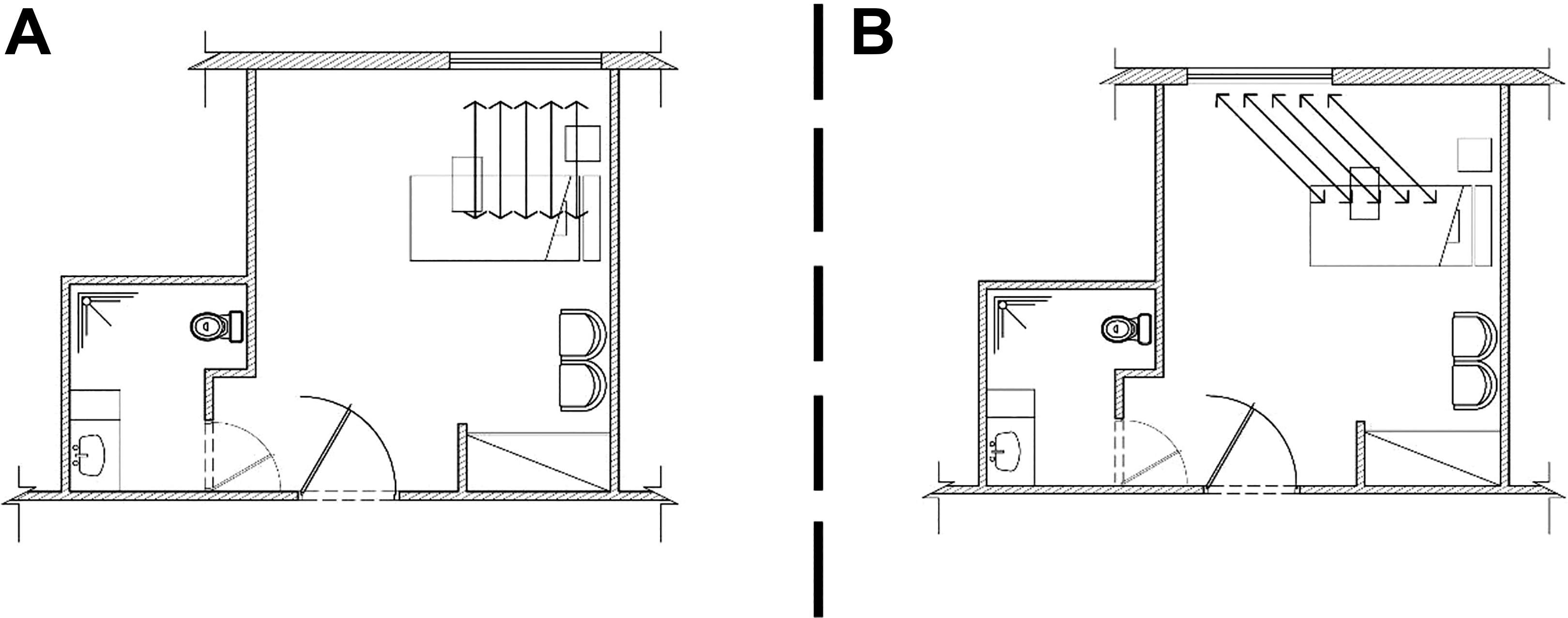
The placement of windows according to patient bed.
The respondents were also asked to rate the importance of having additional windows in their facilities. The average of this rating was 4.16 of 5, which indicated the general preferences for having extra sources of lighting and view to the outside. In regard to the proportion of the windows, 36.12% preferred to have wider and 29.67% preferred to have taller, while 27.09% preferred to have the same size window. Only, 7.09% preferred to have shorter windows in their facilities. Overall, the respondents preferred to have larger (both taller and wider) windows to have higher quantities of daylighting and better views to the outside.
Discussion
This study focused on the potential impacts of windows in inpatient healthcare facilities on nursing staff. The perceptions of the nurses about the lighting impact on their behavior included mood, stress, satisfaction, alertness, medical error, efficiency, and fatigue. The findings of this study were partially achieved from qualitative data and mostly from the quantitative data. Both methods’ findings support the general notion that daylighting and view to the outside influence staff perceptions and behavior. The findings from interviews revealed that nurses prefer to incorporate natural views as well as accessibility to daylight in their departments. In spite of the focus of this study on the nurses’ perceptions and preferences about daylighting and view to the outside, many concepts regarding patients were discussed in the interviews. The researchers believe this is related to the nursing profession, in which nurses are more concerned for their patients’ preferences than their own.
This study also supports the existing literature about the impact of lighting on mood, stress, and satisfaction in healthcare facilities (e.g., Alzoubi et al., 2010; Gharaveis et al., 2016; Ulrich et al., 2008). Relatedly, research respondents rated the influence of windows in healthcare facilities as significant, as was hypothesized in prior studies (Araji & Boubekri, 2011; Benke & Benke, 2013; Hawes, Brunyé, Mahoney, Sullivan, & Aall, 2012; Salonen et al., 2013).
Among all the investigated factors impacted by daylighting—mood, stress, satisfaction, and comfort—nurses in the survey and interviews indicated that daylighting highly promotes resident moods in inpatient units. The findings support the previous study by Gharaveis et al. (2016), who reported that residents’ perceive mood as being affected greatly by daylighting. With respect to the comparison among different clinical–behavioral factors, this study reports that staff responded that daylighting impacts efficiency more than other factors.
View to the outside was found as another factor to be associated with higher levels of staff satisfaction and lower rates of stress. The findings support the idea that the most important reason for having windows in inpatient facilities is to have daylighting. The most emphasized areas for providing windows in both interviews and open-ended questions of surveys were the patient rooms, nurse stations, and staff break areas. These findings confirm other studies’ evidences (e.g., Gharaveis et al., 2016; Lo Verso et al., 2016; Pati, Harvey, & Barach, 2008; Zadeh, Shepley, Williams, & Chung, 2014). Among the potential places to have daylighting, the nursing staff rated patient rooms higher than other places, despite this was not the focus of this study. The second location was the nurse station, where the staff spend a significant amount of their shift. This was previously found by Zadeh et al (2014). The survey data indicated nurses’ preferences to have daylighting in addition to task lighting in their work areas. This is compatible with the findings of the study by Kamali and Abbas (2012).
Furthermore, this study compared the significance of nurses’ preferences in intensive care and patient units in terms of considering daylighting as an environmental factor. The results showed that nurses in intensive care rated the importance of daylighting higher. Also, the analysis results showed there was a correlation between lighting distribution and glare in inpatient facilities. Finally, the best placement of windows in healthcare facilities was explored by this research. The results showed having windows next to the patient, without disturbance of the associated sun patch, would be preferred. This is similar to what Gharaveis et al. (2016) found about resident preferences in rehabilitation facilities.
Limitations
Similar to all research activities, this study has limitations. The study included nurses in a singular geographical location, with specific cultural and behavioral considerations. As such, the findings cannot be easily generalizable to nurses working in other countries and other climate regions. Additionally, the use of self-reported data might have compromised the reliability/accuracy of the data and represented respondent biases. Also, the researchers of this study were not able to measure the quantity of daylighting and behavioral factors because of limitations in budget and time. Future studies can draw conclusions on more measureable aspects of daylighting. Furthermore, both the qualitative and quantitative participants of this study were volunteers, which may cause differences in results. Further research can address the limitations of this study. Conducting similar studies in diverse regions with various healthcare systems, cultural backgrounds, and healthcare systems may lead to further insights. Moreover, involving a larger number of survey participants and interviewees may provide a more complete understanding of effective design recommendations. Future research might also use alternative methodologies such as direct observation and outcome-based measurements to investigate staff usage, preferences, and other effects of having windows in inpatient units.
Conclusion
The results of both methods of this study suggest that accessibility to daylighting and view to the outside can bring significant direct benefits to nurses and indirectly affect the patients they serve. The results also support the proposition that specific environmental characteristics are potentially important for reducing fatigue, stress, and medical error, while enhancing satisfaction among nurses. Despite the differences in the importance of daylighting and view outside on different behavioral factors, the data collected from this study can provide new knowledge to help nurses, designers, and healthcare managers to promote the quality of lighting in facilities. This can also present specific policy and design interventions to make healthcare facilities more effective. Despite this study’s focus on the perceptions and input of the nursing staff, the nurse participants referred to the needs and preferences of the patients they serve.
Implications for Practice
This mixed-method study investigated the impact of daylighting on nursing staff in terms of mood, satisfaction, stress, and fatigue in inpatient healthcare facilities.
The main implications for practice: Environmental design is one of the critical factors for the reduction of staff stress successfully in inpatient facilities. Nurses prefer to incorporate natural view as well as accessibility to daylight in their departments. Nurses in the study selected daylighting as the most functional reason for windows in their facilities. This study founds daylighting impacts efficiency more than other clinical–behavioral factors.
Footnotes
Acknowledgments
The authors acknowledge the support of Dr. Mardelle Shepley: professor at Cornell University, Dr. Kristi Gaines: associate professor at Texas Tech University, and Michael Heath: adjunct professor at Southeast Missouri State University.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.