
Abstract
Objective:
The study fills a gap in the literature by examining the size of the art displayed and waiting time in an exam office on patients’ judgments of the quality of care they are likely to receive.
Background:
A body of research shows that the content of art in healthcare settings has an impact on patients’ well-being, yet no work has empirically systematically examined the size of the art displayed on perceived healthcare outcomes.
Method:
A fully crossed 4 ×2 between-subjects experimental design examined the impact of exposure to images in an outpatient exam room that varied in the size of what was displayed (a landscape scene: small, medium, large, and control—blank wall) crossed by the time waiting for the physician (10 vs. 45 min). The Dependent Variables were the reported anxiety and various measures of satisfaction with the healthcare visit.
Results:
The size of the art had a significant effect on the majority of the dependent variables; specifically, the large image had a more positive impact than the other sizes; longer waits were also negatively evaluated by patients and affected anxiety and judgments of room spaciousness.
Conclusions:
Identifying the recommended content of art displayed is necessary but not sufficient; the size of the art in its context has the potential to impact a range of important perceptions related to healthcare. When the size does not match the available wall space (i.e., the canonical size was not utilized), a variety of ratings of the healthcare environment (including the practitioner) were negatively affected.
Keywords
Research has demonstrated the healing potential of art in healthcare settings (e.g., Lankston, Cusack, Fremantle, & Isles, 2010; Nielsen & Mullins, 2017; Nielsen, Mullins, Fich, & Roessler, 2017; Ulrich & Gilpin, 2003), yet no research to our knowledge has systematically investigated the impact of the size of art displayed in the exam room. Research has demonstrated the negative impact of waiting on patients’ satisfaction with the healthcare visit (e.g., Bleustein et al., 2014) but also the potential for visual distractions to change behavior in clinic waiting areas (e.g., Pati & Nanda, 2011) and Emergency Room (ER) waiting rooms (Nanda et al., 2012). Might the positive distraction presented by art in an exam room offset the negative impact of a long wait for the physician?
The Impact of Art
Within the context of Ulrich’s (1991) theory of supportive design, the impact of positive distraction in the healthcare environment has received attention and is generally acknowledged and often utilized by healthcare practitioners (e.g., Frampton, Charmel, & Planetree, 2009). In general, patients prefer representational scenes of nature (Cusack, Lankston, & Isles, 2010; Eisen, Ulrich, Shepley, Varni, & Sherman, 2008; Hathorn, 1993; Hathorn & Nanda, 2008; Lankston et al., 2010; Ulrich, 1999).
Ironically, given the extensive body of literature on the content of the art displayed, the size of the display has been seldom considered, if mentioned at all. deKort, Meijnders, Sponselee, and Ijsselsteijn (2006) determined that viewing a 10-min film of nature on a large screen (72″) compared to viewing the film on a smaller screen (31″) had a more positive impact on physiological responses, but this research used an immersive display, not a static image as in commonly found in healthcare environments (i.e., images of nature hung on walls). Some suggestion about patients’ sensitivity to the issues of size, placement, and context emerged in the work of Nielsen, Mullins, Fich, and Roessler (2017). Qualitative data from interviews with 30 patients in hospital day halls in Denmark revealed that some patients noticed alignment, centering on the wall, and the relational size of the work (small paintings on larger walls were considered “out of place,” p. 320). Other research mentions the size of the images used without empirically assessing a range of sizes or focusing on size. For example, in research in a Dutch hospital by Beukeboom, Langeveld, and Tanja-Dijkstra (2012), posters of plants (90 cm × 60 cm; ∼ 3′ × 2′) were contrasted with real plants or no nature (control), but there was no indication of the dimensions of the waiting rooms themselves, making it hard to gauge the prominence of the posters.
In Hathorn and Nanda’s (2008) whitepaper on evidence-based art, they listed three criteria for the selection of art in healing environments: location of the artwork, the needs of special patient populations (e.g., palliative care), and the background characteristics of the patients (e.g., gender, age, ethnicity; p. 12). In addition, the authors comment that “art size, placement, and spatial relationships in the healthcare setting have not been studied in a scientific manner” (p. 12), noting, “there is a substantial scope to investigate the role of art in reducing perception of wait time….” (p. 14). Thus, there are numerous reasons researchers and practitioners should care about the specifics related to the installation of art in healthcare settings.
Perception of Size
While the context for this experiment is the patient-centered healthcare environment, it is relevant to include some work on perception and image size more generally. Research by Linsen, Leyssen, Sammartino, and Palmer (2011, p. 298) points out that people’s preference for an object is influenced by the size of the object as they experience it in the real world: “Canonical-size effects on aesthetic judgments thus indicate that people tend to prefer images in which the size of the object’s image within its frame fits their knowledge of its actual physical size.” The use of the term canonical is meant to communicate the idea of the basic form or perspective that reflects people’s experience of the object. Here, we are exploring what one might call the canonical experience of image display (i.e., the size of the image that is usually displayed on a wall in a given context, here, an exam room). Also, the real-world size of an object seems to be a property that is automatically accessed (Konkle & Oliva, 2012); it is part of our understanding of the object (perhaps its affordance; Gibson, 1979). Referencing Gibson, Konkle and Oliva (2012, p. 561) state “Every object in the world has a physical size which is intrinsic to how we interact with it.”
The Impact of Wait Time
Advice to practitioners is that patients should wait less than 20 min from the time they are placed in the exam room to the time the physician arrives (McLaughlin, 2013). Allar (2018) reported that 20% of patients have changed physicians because of long wait times; 30% of patients report having walked out of the office because of a long wait. The average wait time in the United States reported in this article by Allar (citing Vitals’ ninth annual wait time report) was 18 min, 13 s. Patients consider the time spent waiting to be a component of the healthcare visit, and it negatively affects physicians’ ratings when patients have to wait, especially longer than 20 min (HIT Consultant Staff, 2016; Oostrom, Einav, & Finkelstein, 2017; Sanford, Weitz, Zahiri, & Park, 2020).
Importantly, a study documented that time waiting in the exam room was more negatively perceived (in terms of patient satisfaction scores) than in the waiting room itself (Bleustein et al., 2014). The authors speculate that the dissatisfaction may be related to (1) a lack of material to read, (2) the expectation that service will be quicker once you move to the exam room, and (3) having less comfortable surroundings. Because wait times negatively affect the confidence the patient has in the healthcare provider (Bleustein et al., 2014), it makes sense to consider whether aspects of the exam room might interact with wait time to improve perceptions of the visit and the quality of care delivered.
The Present Study
Thus, to address a gap in the literature, this experimental research examined the impact of exposure to images in an outpatient exam room that varied in the size of what was displayed (a small, medium, large landscape scene, and control—nothing displayed) crossed by the time the individual waited for the physician (10 vs. 45 min).
Specifically, we hypothesized that the medium and large images would produce more positive outcomes for all dependent variables than the small and blank wall conditions and that there would be an interaction between wait time and image size such that the longer wait condition (45 min) would be judged less negatively in the medium and large than in the small and blank wall conditions. We did not make a prediction about the difference between the medium and large images because the literature has not indicated when an image might be considered medium, when large. Consistent with the literature, we also predicted that those in the longer wait time condition (45 min) would have more negative reactions for all dependent variables than those in the 10-min condition.
Method
Participants
Participants were college students recruited through the institution’s participant pool (the average number of visits to exam rooms over the past 2 years was 5.98). A recruitment message was also sent to graduating psychology and behavioral science majors. Of 135 people who opened the link, 11 were the researchers testing the link, 12 were participants who did not start the survey, and 1 was a participant who stopped answering questions after the items dealing with perceptions of the clinic, reducing the sample size from 135 to 111. Participants were then retained only if they passed both manipulation checks, reducing the sample size to 83. All measures of internal consistency and dependent measures are based on this N of 83.
Measures
Visual stimuli
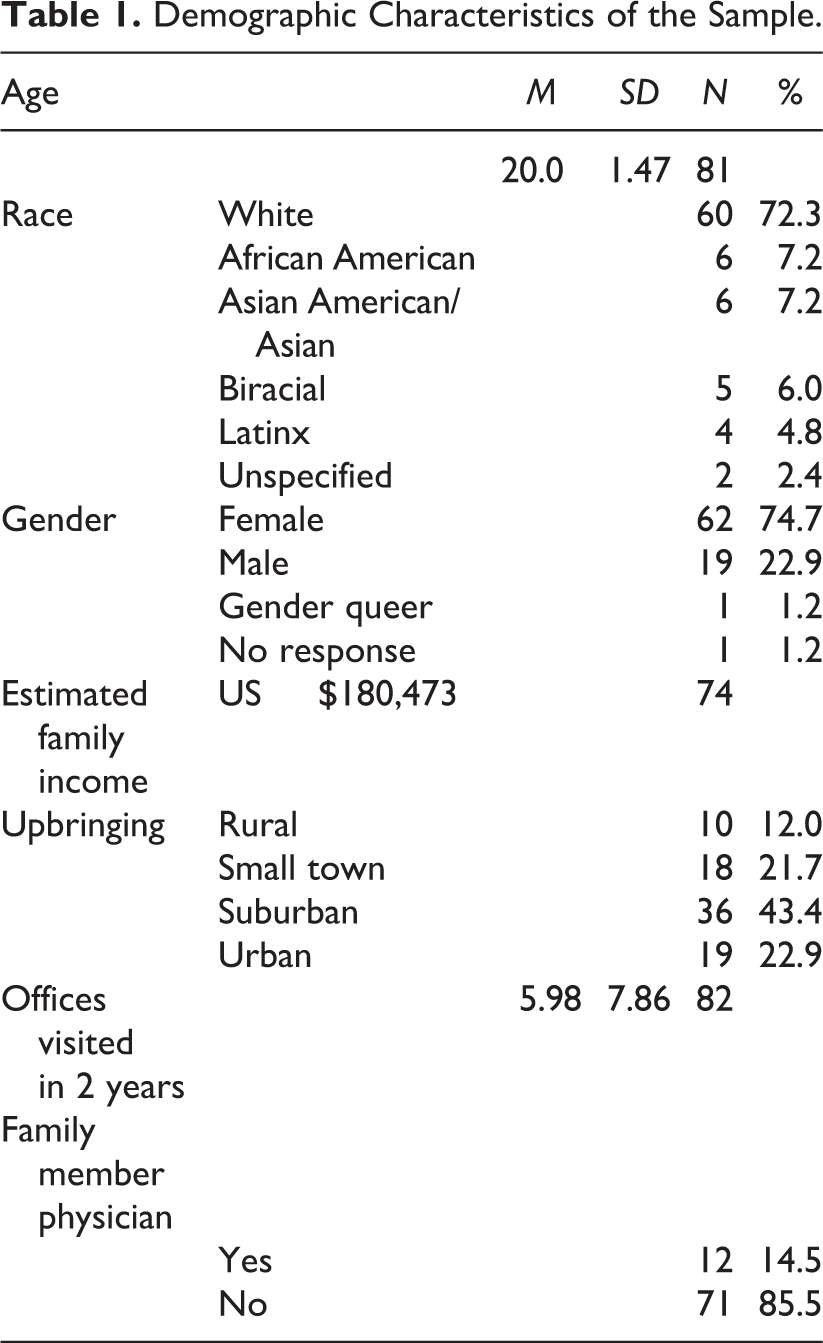
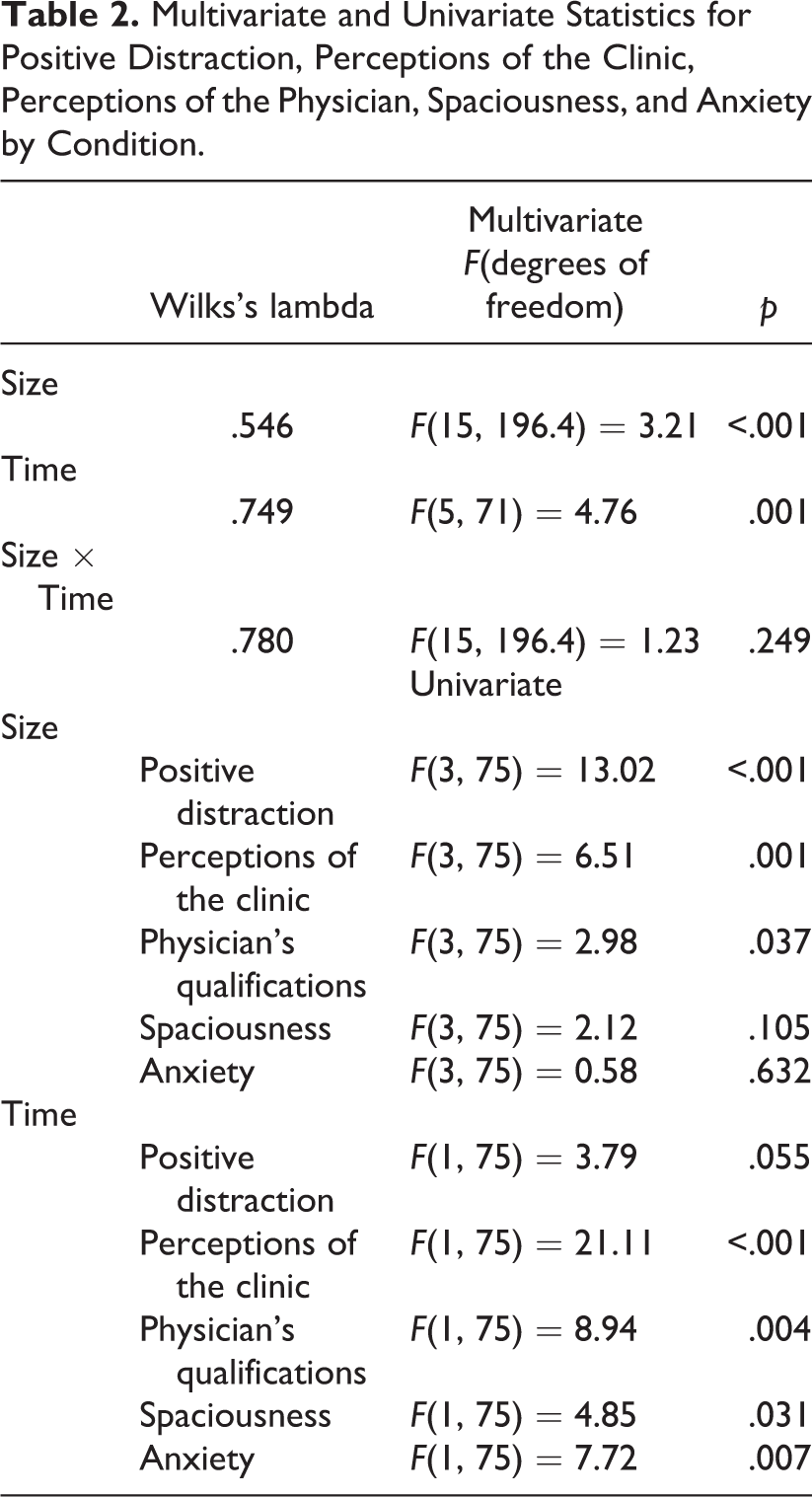
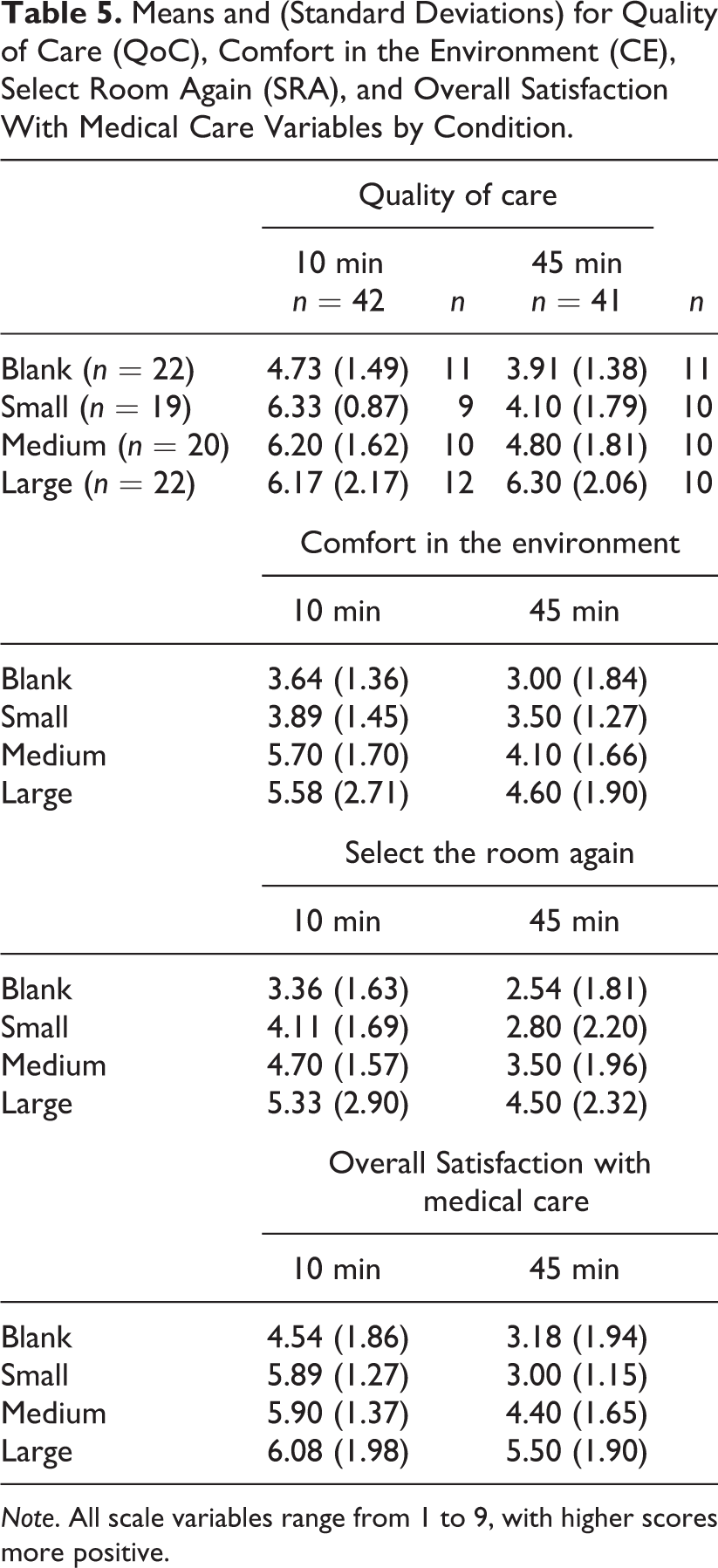
A photo of an exam room with a small image displayed (Lake Bled in Slovenia) and used in the study was manipulated using Photoshop to create three additional conditions (blank wall, medium image, large image). The exam room wall where the small photo was displayed was ∼ 9′ (W) × 12′ (L) × 8 1/2′ (H). The small image was 24″ × 16″; the medium image was 41.2″ × 27.5″; the large image was 80.3″ × 53.3″ (see Figure 1, which includes images 1–4).
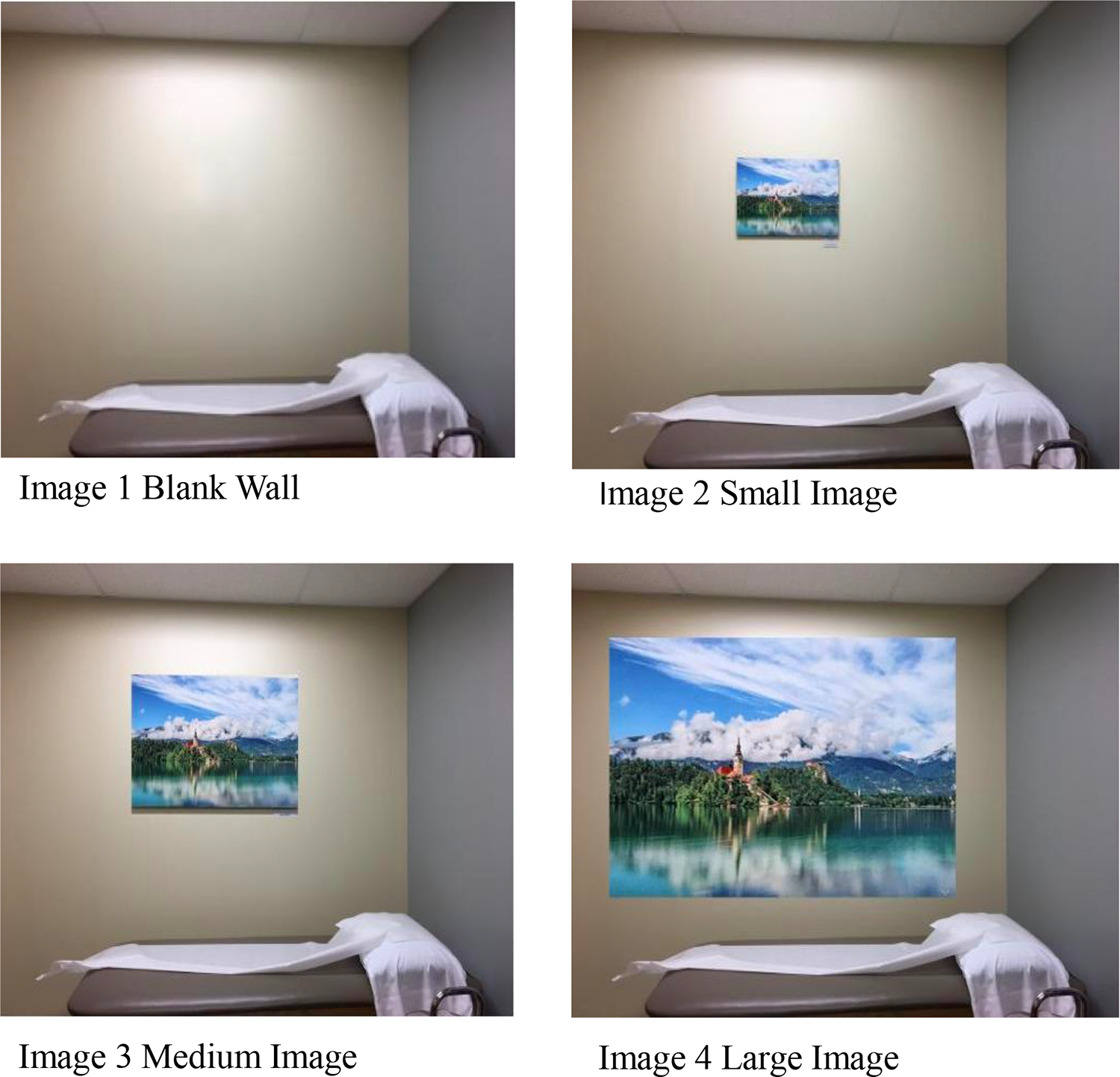
Images of the four photographic conditions.
Dependent Measures
To measure positive distraction, 4 items from Andrade and Devlin (2015) were used. A sample item is “In this room, there are objects that attract my attention” (α = .884).
Four items from Okken, van Rompay, and Pruyn (2013) measured perceived spaciousness on a 5-point Likert-type scale from “strongly agree” to “strongly disagree.” A sample item is “I feel constricted inside this room” (α = .876).
For anxiety, the 21-item State-Trait Inventory for Cognitive and Somatic Anxiety (state version; Ree, French, MacLeod, & Locke, 2008) was used, which reflects the level of stress or anxiety an individual feels. A sample item is “My heart beats fast,” measured from 1 (“not at all”) to 4 (“very much so; α = .946).
To evaluate response to the clinic, the 17-item Person-Centered Climate Questionnaire—Patient Version (Edvardsson, Koch, & Nay, 2009) was used. This measure has a 7-point response format from “No, I completely disagree” to “Yes, I completely agree.” The stem is “I experience this clinic as,” and a sample item is “A place where the staff is knowledgeable” (α = .964).
Twelve items from the “Qualifications” dimension of the Physician Qualities Scale from Devlin et al. (2009) measured physician competence. Ratings use a 9-point bipolar scale. A sample question is “This person could be described as a 1 = high achiever to 9 = low achiever” (α = .961).
Next are 4 items about the room: a question evaluating the quality of care expected in the setting (1 = very low quality to 9 = very high quality); the degree of comfort expected in the setting (1 = not at all comfortable to 9 = very comfortable); whether participants would select the room again (1 = definitely no to 9 = definitely yes); how satisfied participants think they would be with the results of their medical care in the exam room (1 = not at all satisfied to 9 = extremely satisfied). Versions of these questions have been used previously in research by Devlin (1995) and Devlin, Andrade, and Lima (2014). Participants were also asked to indicate three aspects of the exam room that influenced their judgments and whether each aspect was positive or negative. Also included was a question asking how likely it was that the physician used the services of an interior designer for the exam room (1 = not at all likely to 9 = extremely likely).
Next were demographic/background questions: age, gender, race, estimated annual family income, and type of environment in which raised (rural, small town, suburban, or urban); number visits to an exam room in the last 2 years; and whether any family member is a physician (e.g., parent, sibling, aunt, uncle, grandparent).
There were two manipulation check questions. For the photo condition, participants were told “Below you will see four photos labeled A, B, C, and D. First look at all of the pictures; then select the letter corresponding to the picture you saw at the beginning of the survey.” Participants were then asked a follow-up question: “In terms of enhancing the experience of patients waiting in the exam room, which photo/image would you select (A, B, C, or D)?” For timing, participants were asked: “In the description you read of the exam room, how long did you have to wait to see the physician?” They were given the choice of 10 min or 45 min.
Procedure
The survey was created through Qualtrics (Qualtrics Core XM); participants who volunteered through the institution’s participant pool or responded to a mailing to graduating psychology and behavioral neuroscience majors received a link to the survey that included the informed consent (in downloadable form). Participants were randomly assigned to one of the eight conditions by Qualtrics. Participants read the informed consent and advanced the page to “consent;” saw one of eight conditions, and read the following description of the reason for their visit. The research had Institutional Review Board approval.
Scenario
“Imagine you have undergone an operation for a total knee replacement and are making your first post-operative visit to the physician’s outpatient office. You arrive at the office and are escorted by the assistant to the exam room you see in this picture. In addition to the exam table, there are two chairs, a work station, coat hook on the back of the door, and an adjacent magazine rack. You wait 10 [45] minutes before the physician arrives.” The photograph and text were displayed by a timing function for 35 s before advancing.
Results
Analytic Sample and Characteristics
Of the 111 participants, 83 passed both manipulation checks (74.8%) and were used in data analysis. Of these 83, a number of participants missed individual items and were kept in the sample if the number of items skipped was less than 15% of the total number of items for the measure in question. Missing cells were replaced with the sample mean. Across all dependent measures, 13 participants skipped 1 item, three skipped 2 items, and one skipped 3 items. See Table 1 for the demographic characteristics of the sample. We did a series of proportional analyses (χ2) to assess whether the participants randomly assigned to the size and time groups differed by upbringing, number of offices visited in the last 2 years, and whether any family member might be a physician; there were no significant differences (all ps >.05). This lack of difference provides some assurance that the groups were equivalent, at least for these demographic aspects.
Demographic Characteristics of the Sample.
Overview of Analyses: Impact of Image Size and Time Spent Waiting
Because we had a large number of outcome variables, we clustered these into two sets of conceptually related variables and then conducted analyses on these sets. To cut down on the possibility that a result would be significant by chance (i.e., Type I error), we used a multivariate approach, followed by analyses at the univariate level (i.e., for each outcome variable separately). The individual outcomes are the primary focus. The first set included positive distraction, perceptions of spaciousness, anxiety, perceptions of the clinic, and perceptions of the physician’s qualifications. The second set was the four quality of care variables: quality of expected care in the environment, the expected comfort in the environment, selection of the room again, and overall expected satisfaction with the results of medical care in the exam room. For each set of variables, we asked the question whether people in the four size conditions (blank, small, medium, large) and the two time conditions (10 vs. 45 min) gave different ratings to the outcome variables. We will first explain the impact of image size, then the impact of time waiting.
Image Size (Blank wall, small, medium, large)
Viewing the differently sized images made a difference in ratings of positive distraction; perceptions of the clinic; and perceptions of the physician’s qualifications. There were no significant effects of image size for spaciousness or anxiety. Specifically, when comparing the sizes against each other in follow-up tests, it was the large- and medium-sized images that provided significantly more positive distraction when compared to the blank wall. The large image also provided significantly more positive distraction than the small image. For perceptions of the clinic, viewing the large image produced significantly more positive scores compared to both the blank wall and the small image. For perception of the physician’s qualifications, the large image significantly enhanced the perception of those qualifications more than did the small image (see Table 2 for multivariate and univariate statistics and Table 3 for Ms and SDs).
Multivariate and Univariate Statistics for Positive Distraction, Perceptions of the Clinic, Perceptions of the Physician, Spaciousness, and Anxiety by Condition.
Means and (Standard Deviations) for Positive Distraction (PD), Spaciousness (S), Anxiety (A), Perceptions of the Clinic (PoC), and Perceptions of the Physician (PoP) by Condition.

Note. PD scale range from 4 to 20 (lower scores more positive); spaciousness range from 4 to 20 (higher scores more positive); anxiety scale range from 21 to 84 (lower scores more positive); perceptions of the clinic scale range from 17 to 119 (higher scores more positive); perceptions of the physician range from 12 to 108 (lower scores more positive).
Time (10 min vs. 45 min)
When looking at the individual outcome measures, the two time conditions (10 vs. 45 min) produced differences in scores. Those in the 10-min condition had more positive ratings than those in the 45-min condition for perceptions of the clinic, perceptions of the physician’s qualifications, spaciousness, and anxiety. The result for positive distraction approached significance (p = .055). Related to the initial hypotheses, while the result for the interaction between size and time for positive distraction was not significant, it was trending (p = .066), and an examination of the means suggests that the large image has the potential to offset the negativity of waiting 45 min. Refer to Table 3 for means and standard deviations.
Quality of Care Variables
Following a parallel strategy, we set out to determine whether the four quality of care variables (quality of expected care in the environment, the expected comfort in the environment, selection of the room again, and overall expected satisfaction with the results of medical care in the exam room) were affected by which image the participant saw (blank wall, small, medium, large) and for what length of time (10 vs. 45 min) the participant was told to imagine waiting. Of particular interest here, the size of the image significantly affected all four quality of care variables. As a pattern, the large image was viewed more positively. Specifically, when the image sizes were compared against each other, the follow-up tests showed significantly more positive ratings for the large versus the blank wall for both quality of care and for comfort in the environment. In addition, for comfort in the environment, the medium image was judged to be significantly more positive than the blank wall, and the contrast of the large versus small image approached significance (p = .061). For selecting the room again, the contrast of the large versus the blank wall was significant, and the large versus small approached significance (p = .094). For the overall satisfaction with the results of medical care in the exam room, the large versus blank wall and large versus small contrasts were significant, and the medium versus blank wall (p = .074) approached significance.
There were significant effects for Time for all four quality of care variables; means indicated that the ratings were more favorable when participants were told they would wait 10 rather than 45 min (see Table 4 for the multivariate and univariate statistics and Table 5 for means and standard deviations).
Multivariate and Univariate Statistics for Quality of Care, Comfort in the Environment, Select Room Again, and Overall Satisfaction With Medical Care (OSMC) Variables by Condition.

Means and (Standard Deviations) for Quality of Care (QoC), Comfort in the Environment (CE), Select Room Again (SRA), and Overall Satisfaction With Medical Care Variables by Condition.
Note. All scale variables range from 1 to 9, with higher scores more positive.
Interior Designer
Regarding whether participants thought the physician used the services of an interior designer, where 1 = not at all likely to 9 = extremely likely, there was a significant finding for size (p < .001), but not for time (p = .241), or for their interaction (p = .805). When the image sizes were compared against each other, the use of an interior designer was judged to have been significantly more likely in the large versus each of the other conditions.
Recommendations for Enhancing the Patient’s Visit
Regarding participants’ recommendations for which image size they thought would enhance the experience of patients waiting in the exam room, 60.2% (n = 50) favored the large image; 38.6% (n = 32) favored the medium; 1.2% (n = 1) favored the blank wall; and no one selected the small image.
Qualitative Aspects
While space limits the presentation of findings here, it is informative to examine some of the data regarding what features were judged positively or negatively. Looking at whether participants judged these responses to be positive or negative by size revealed significant differences. We used a series of χ2 to examine these judgments (positive vs. negative by the four sizes). For the first aspect mentioned, by size, the χ2 analysis was significant (p = .003). The pattern of responses was that as the size of the image became larger, the proportion of positive to negative responses grew: blank (13.6–86.4%), small (31.6–68.4%), medium (55–45%), and large (63.6–36.4%). These percentages show that for the medium and large sizes, the percentage of positive comments was larger compared to the negative; for the blank and small sizes, it was the percentage of negative comments that was larger compared to the positive.
In terms of content for Aspect 1, for the blank wall condition (n = 22), a strong theme was blandness, blankness, plainness, and lack of decoration, with nine (41%) people making such comments. There were only three positive comments, two for the magazine rack and one for the bed.
For the small image condition (n = 19), the picture was mentioned positively by five people (26.3%); one other positive comment was “similar to what I have experienced in the past.” For the negative aspects, nine (47.4%) mentioned lack of decoration or drabness, the wall color, having only one picture, including the comment “the picture on the wall seems forced and a half-hearted attempt to make the room more welcoming.” Three negative comments were about the exam table/bed, including the torn and crumpled paper on the exam table.
For the medium condition, n = 20, there were 10 (50%) positive comments about the picture; two mentions of the image (including the “wall”) were negative. There were also two negative mentions of the exam bed (messily placed paper); the doctor taking 45 min to arrive (2); two comments about the size of the space (cramped, small), the emptiness (1), but also one positive mention of the space.
For the large condition (n = 22), there were 12 (54.5%) positive mentions of the image (and two negative mentions—including a comment that it was too big). Other negatives included the (dark) wall color (3), the size of the room (1), the paper on the exam table (1), and relatedly the room not being neat (1). The physician arriving 45 min late (1) was negative. Across Aspects 2 and 3, the same kinds of comments were made (see the Supplemental Online Appendix for the complete set of comments broken down by Aspect, Size, and Time).
Discussion
This research is the first to our knowledge that systematically examines the impact of the size of art displayed in the exam room on perceived quality of care outcomes. The results of this experimental study find support for the hypothesis that the presence and size of an art image displayed in a physician’s exam room impact judgments of the visit and of the physician himself or herself. Specifically, the presence and size of the image displayed in an exam room can affect judgments ranging from positive distraction to perception of the clinic, the physician, and quality of care outcomes such as the overall expected satisfaction with the results of medical care in the exam room. In addition, the qualitative comments provide additional support that the size of an image can affect judgments of care.
We had anticipated that the medium and large images would both show benefits over the small image and the blank wall, but the contrasts involving the large image were more pronounced than those involving the medium image. As a theme, the larger the size of the image, the more positive the ratings were. In the qualitative comments, the χ2 analyses show that as the size of the image increases, so does the proportion of positive to negative comments. Regarding contrasts, it was the larger image that was judged to be more positively distracting than the blank wall; for this variable, the medium image did so as well. The larger image was also more positively distracting than the small image. The fact that the contrast between the blank wall and the small image was not significant for positive distraction is noteworthy, particularly as the small image was the one on display in the actual exam room. Ironically, no one recommended hanging the small image to enhance patients’ experience of waiting; the large image received over 60% of the votes. Further emphasizing the distinctiveness of this large size, it was only in the case of the large image (in comparison to the medium and small size and the blank wall) in which participants thought an interior designer had been consulted. The large image enhanced perceptions of the clinic and of the physician’s qualifications more than the small image, and compared to the blank wall, in the case of perceptions of the clinic. Clearly beyond a blank wall, but also beyond the display of an image at all, these results suggest that the size of what is on display has an impact. What these results demonstrate is that beyond the display of art in a healthcare setting, more attention should be paid to whether the size of the art “fits” the space available, echoing some qualitative comments from patients that emerged in work by Nielsen et al. (2017). Thus, as humans with experience in the world, we tend to have a canonical sense of the appropriateness of the size of the image displayed (Konkle & Oliva, 2012; Linsen, Leyssen, Sammartino, & Palmer, 2011).
The four quality of care variables (quality of care, comfort in the environment, selecting the room again, overall expected satisfaction) revealed a similar pattern in that it was the large image that was judged more favorably than the blank wall for all four variables, with the large versus small contrast approaching significance for two variables (comfort in the environment, selecting the room again), and significant in the case of overall expected satisfaction with results of medical care. While not to the extent of the large image, there was some support that the medium-sized image has the potential to have a positive impact, as it was judged more positively than the blank condition for comfort in the environment and approached significance versus the blank wall in the overall expected satisfaction with results.
The effects of time were clear-cut and not surprising, yet they are important to consider. Waiting for a relatively long period of time has negative effects on a wide variety of healthcare-related outcomes, from quality of care and comfort in the environment to the perceptions of the clinic and of the provider. Moreover, waiting 45 min reduces the expected satisfaction with the results of medical care in the exam room. Further, it is noteworthy that the waiting manipulation affected anxiety scores; people reported being more anxious when they had to wait 45 min. Waiting also affected the perception of space (spaciousness), with participants perceiving the exam room to be more spacious (they felt less constricted in the room) when waiting only 10 min. The sense of boredom and constraint seems to increase with the length of the wait; keeping patients waiting that long in the exam room should be avoided. As mentioned earlier, Bleustein et al. (2014) suggest that the discomfort patients experience with this length of wait may relate to the lack of options for distraction in the exam room, coupled with the expectation that once you move to the exam room you are “ready to be seen.” They advise practitioners to keep people in the waiting room where there are typically more options (e.g., magazines, often television) if the physician is behind schedule. Relatedly, in this study, the availability of magazines (on a magazine rack) was one of the few positive aspects of the exam room (beyond the picture) mentioned by participants. One other finding is of note. As indicated previously, the Space × Time interaction for positive distraction approached significance, and the potential exists for the large image to offset the negative response to waiting 45 min. Further research with more participants should investigate this possibility.
While a significant amount of work has been done with regard to the role of art in creating positive distractions in healthcare environments, identifying the recommended content is necessary but not sufficient. This research shows that the size of the art in its context has the potential to impact a range of important perceptions related to healthcare. When the size does not match the available wall space (i.e., the canonical size was not utilized), as seemed to be participants’ judgment here, a variety of ratings of the healthcare environment (including the practitioner) were negatively affected.
Recommendations
What should healthcare practitioners take from this research? First, more attention needs to be paid to the size of the image displayed; in the case of this research, the image displayed in the actual exam room was a common size (24″ wide × 16″ high), whereas the large image was ∼80″ wide × 53″ high. An image that is 24″ × 16″ may fit a lot of spaces within an exam room (e.g., between a cabinet and the corner wall), but on a wall that is 9′ across, it appears “too small” for the space and seems to reflect a lack of consideration for the design decisions that are being made. As one participant commented in the small condition “The picture on the wall seems forced and a half-hearted attempt to make the room more welcoming”; and another commented “Mostly empty walls (minus the small photograph).” The results of the study suggest that art that leaves too much white space impacts how patients feel when waiting as well as their perception of the healthcare quality likely to be received, making the percentage of wall whitespace an important aspect to consider for healthcare exam rooms when decorating those spaces.
The qualitative comments that participants offered to identify point to some additional practical aspects of how time is spent waiting. Beyond the photo, the magazine rack was the most frequently mentioned positive item. The coat hook and the additional chairs in the room were also valued. There were a number of negative comments about the protective paper on the exam bed; because it was not “smooth,” it drew comments about quality: “torn and crumpled paper on the exam table.” As one participant in the blank wall condition commented, “The exam table had a misaligned/folded sheet on top of it. That signifies that the staff are not being careful and meticulous with their work.”
Limitations
Future research might recruit a more diverse range and a larger number of participants. At the same time, these college students had a reasonable amount of experience with healthcare settings (the mean number of offices visited over the last 2 years was nearly 6). A further limitation of the work is its basis in simulation; these were not patients experiencing a real office visit. While iconic simulation has been validated as a research strategy (e.g., Ulrich et al., 1991) and a meta-analysis by Stamps (1993) has shown the potential for color photographs to generalize to responses given on site, this work needs to be extended to patients in situ.
Future Directions
This research manipulated a single image on the wall, and future research might examine whether multiple images produce similarly positive effects. A second line of research involves whether the content of the image is “local versus global” and the potential advantage to using images of familiar local environments. The image displayed in this research was of Lake Bled, Slovenia, a relatively well-known (but international) location. A third direction relates to the circumstances under which medical content should be displayed in the exam room. In this study, one participant stated as a drawback “There were no posters of anything that involved the knee.” Here, the scenario described a patient who had undergone a total knee replacement, which is certainly a substantial but at the same time non-life-threatening procedure. Are there other circumstances (e.g., posters displaying cancerous skin lesions) in a dermatologist’s office that could be anxiety provoking for patients to see?
Implications for Practice
More attention needs to be paid to the size of art images displayed in healthcare settings. The content of art is a necessary but not sufficient criterion for selecting what is displayed.
The percentage of wall whitespace is an important aspect to consider for healthcare exam rooms when decorating those spaces.
Larger images (that utilize over 60% of the visible space on the wall) are judged positively by prospective patients.
Non-design variables such as waiting time have the potential to affect perceptions of design, such as room spaciousness. If waiting time is longer than expected, patients should remain in the waiting room rather than moving to the exam room.
Amenities such as magazine racks are valued, as are chairs for caregivers accompanying the patients.
Supplemental Material
Supplemental Material, sj-docx-1-her-10.1177_1937586719892602 - Magnitude Matters: Art Image Size and Waiting Time Impact Perceived Quality of Care
Supplemental Material, sj-docx-1-her-10.1177_1937586719892602 for Magnitude Matters: Art Image Size and Waiting Time Impact Perceived Quality of Care by Ann Sloan Devlin, Alaina Anderson, Sarah Hession-Kunz, Margaret Kelly, Lilly Noble and Amy Zou in HERD: Health Environments Research & Design Journal
Supplemental Material
Supplemental Material, sj-pdf-1-her-10.1177_1937586719892602 - Magnitude Matters: Art Image Size and Waiting Time Impact Perceived Quality of Care
Supplemental Material, sj-pdf-1-her-10.1177_1937586719892602 for Magnitude Matters: Art Image Size and Waiting Time Impact Perceived Quality of Care by Ann Sloan Devlin, Alaina Anderson, Sarah Hession-Kunz, Margaret Kelly, Lilly Noble and Amy Zou in HERD: Health Environments Research & Design Journal
Footnotes
Authors’ Note
Authors listed alphabetically after first author.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.