
Abstract
Background:
A positive distraction is a significant environmental feature that introduces positive feelings by diverting attention from stress or anxious thoughts. Existing research has deemed the application of positive distractions in pediatric environments to be significant. This study investigated the essential positive distractions and the associated health benefits.
Aims:
The aims of this study were to validate and extend evidence on positive distractions and play opportunities in the design of the public spaces in pediatric healthcare environments, translate existing evidence into design suggestions, and identify research gaps in this realm.
Methods:
A four-phased literature review method was employed in the study, including literature search, literature screening and selection, literature appraisal, and thematic analysis and in-depth discussion. Eventually, 27 peer-reviewed publications were reviewed and discussed in detail.
Results/Conclusions:
The gathered materials were grouped into six themes of positive distractions: (1) art and environmental aesthetics, (2) spatial arrangement and atrium, (3) considerations of socialization patterns, (4) play and interactive technologies, (5) sound and lighting interventions, and (6) access to nature. The research indicated that positive distractions in the pediatric healthcare environment provide a series of health benefits for patients, including improved behavioral and emotional well-being, reduced stress and anxiety, enhanced healthcare experience and satisfaction, and facilitated medical procedures and recovery. Yet significant research gaps emerged between positive distractions and play in garden spaces and spatial design to accommodate interactive technology and socialization in the public areas of pediatric healthcare environments. This study organized the understanding on the components of supportive environments and its outcomes for pediatric healthcare design.
Research Background
Positive Distractions in Healthcare Environment
Since the 1970s, healthcare environmental research and design has shifted its focus from the reduction of negative effects of the physical environment to the creation of supportive environments that reinforce positive experiences (Shepley, 2006). The uninviting interiors and institutional organization of traditional hospital buildings isolated and disoriented their occupants, causing more damage to their psychological health, as such characteristics generated anxiety and stress (Ulrich, 1999). Following patient-centered care principles, increasing research on stress impacts within healthcare spaces led to the coining of the design concept of positive distraction (Ulrich, 1991, 1999). A positive distraction is an environmental feature or situation that evokes positive feelings, holds attention and interest, and eventually fosters beneficial psychological and/or physiological changes (Ulrich, 1991). Providing positive distractions in healthcare environments can reduce people’s stress and enhance their mood, thereby facilitating the healing process (Andrade et al., 2017; Ulrich et al., 1991).
Positive distractions have been shown to have a beneficial impact on patients’ well-being, both psychologically and physiologically (Ulrich et al., 2008). This concept is highly applicable to shared spaces such as waiting rooms, as they serve as an area of relief and recollection (Jiang et al., 2017). Therefore, positive distraction design features that allow and calm occupants can be effectively incorporated into the development of design processes, deviating from results of bare walls and little windows. Incorporating positive distractions could offer comfort and a perception of a supportive environment for patients and their families (Ulrich, 1997). Various types of positive distractions that are effective in general healthcare environments have been identified, such as color and artwork with positive meanings, nature, and technology intervention (Lankston et al., 2010; Nanda et al., 2011). Specifically, utilizing nature as therapeutic devices can soothe and encourage healing, reduce people’s stress, change their mood, and relieve their perceived level of pain in various healthcare situations (Cooper Marcus & Sachs, 2013; Jiang et al., 2017; Vincent et al., 2010).
Pediatric Healthcare Facilities and Patient Experience
Pediatric healthcare facilities are institutions dedicated to patients requiring sensitive care and unique needs. The influence of pediatric therapeutic environments on children—the healthcare facility’s most delicate patents—has been shown to be significant in the past research and practices (Sherman, Shepley, et al., 2005; Silvis, 2013). According to Piaget’s theory of children development, children think and process information from the physical environments differently than adults (Singer & Revenson, 1997). Frequently, visiting healthcare facilities for wellness check, acute care, medical procedures, and hospitalization can be emotionally and psychologically traumatizing for pediatric patients because they lack control of their environment (Lerwick, 2016). Children’s experience of helplessness, loss of identity and control, lack of social support, and accompanying fear and pain can delay important medical treatments, take more time to complete, and reduce patient satisfaction (Lerwick, 2016). Various psychological challenges during hospitalization could limit children’s cognitive development, which may result in the dysfunction of dealing with stress and anxiety in the long run (Eisen et al., 2008).
Play as Positive Distraction in the Public Spaces of Pediatric Healthcare Facilities
Play is essential to child development because it contributes to the cognitive, physical, social, and emotional well-being of children and youth (Ginsburg, 2007). By examining positive distractions through the lens of leisure psychology, play could provide exemplary positive distractions as such distractions share similar engaging experiences, such as relaxation, pleasure, enjoyment, and even the optimal experience of flow (Csikszentmihalyi et al., 2014). Various play opportunities in pediatric healthcare environments could help strengthen patients’ sense of control, reduce their stress, and promote their mood and positive experience while facilitating their healing and recovery from diseases. For pediatric patients’ healthy siblings, design features and settings for recreation play can ease boredom and calm their behaviors. Parents’ stress and anxiety could be alleviated through relationships with others, the ability to share emotions, and more relaxed interactions with other children (Corsano et al., 2015).
Public spaces of pediatric healthcare environments, such as waiting rooms, hallways, and hospital gardens, serve as spaces for mere occupation, bringing to attention the necessity for constant sensory stimulation and entertainment for cognitive development in children. In the public areas of pediatric healthcare facilities, health professionals consider “play” to be an activity that helps children make better use of waiting times, decrease their anxiety and nervousness, and enhance interactions and communication with health professionals during the clinical visit, which is known as humanizing children’s healthcare (Corsano et al., 2015, p. 1067). Play and recreation can be therapeutic by giving children the opportunity to explore, express, and process their healthcare experiences in a safe, nonthreatening environment (Children’s Hospital of Philadelphia, 2017). Therefore, it is critical to design public spaces wherein children and youth can maintain a sense of identity and control through self-directed play activities. In particular, outdoor gardens could nurture and assist the healing process of ill children by enabling them to experience biotic, physical and climatic factors in nature and the diversity of forms, colors, textures, and shapes of landscape elements (Said, 2003).
A Brief Overview of Similar Studies
Yet studies conducted on the topics of pediatric healthcare design under the theoretical framework of positive distractions and play are limited. Compared with studies about the design of patient rooms, there is a particular dearth of documentation of positive distractions and the design of healthcare public spaces, such as shared hallways and gardens (Sherman, Shepley, et al., 2005). In an earlier literature review study, Sherman and colleagues (2005) identified 15 papers directly related to pediatric healthcare environmental design between 1997 and 2004, but the majority of the review papers were related to the newborn intensive care unit or pediatric intensive care unit. A few other literature reviews focused on games as distractions for distress among pediatric patients, but the spatial design features of the care facilities were insufficiently discussed or were not systematically reviewed (MacLaren & Cohen, 2005). Norton-Westwood (2012) reviewed the literature on the design parameters of pediatric healthcare environments published between 1980 and 2010, which did not include studies about emerging technology and ambient environment as a trend in current pediatric healthcare design. Given the importance of the topic and the lack of studies and documentation of the data, the current project aimed to systematically review studies conducted within the recent 20 years that are closely related to the design of positive distractions in the public spaces of pediatric healthcare environments.
Research Objective and Questions
This literature review study aimed to validate and extend evidence on positive distractions in order to determine the best methods and practices of incorporating positive distractions and play opportunities in the public spaces at pediatric healthcare facilities, including the overall facility aesthetics, and the sharable interior and exterior spaces such as the atrium, waiting areas, and gardens. In this study, “play opportunities” was used as a broad concept that included playful objects, places where recreational activities could happen, and design features that could arouse leisure experiences in a built environment. The following questions outline the goals of the literature review: (1) How do users perceive various environmental design features and play opportunities as positive distractions in the public spaces of pediatric healthcare environments? (2) What health benefits might positive distractions and play opportunities provide to occupants in pediatric healthcare environments?
Research Method and Procedures
A four phased literature review was conducted to identify and select relevant studies about positive distractions and play in the design of public spaces at pediatric healthcare facilities. The four phases included (1) literature search, (2) literature screening and selection, (3) literature appraisal, and (4) thematic analysis and in-depth discussions.
Literature Search
A combination of key words was used to search existing literature using mainstream medical and architectural databases. Key words groups included (1) pediatric, neonatal, children, youth, young patient, adolescent, and teenager; (2) hospital, healthcare environment/setting/facility, clinic, and pediatric center; (3) public space/area, waiting room/area, hallway, playground, playroom, and garden; (4) stress, emotion, anxiety, mood, behavior, perception, pain, distress, experience, and satisfaction; and (5) art, color, toy, play, image, video, game, distraction/distractor, and technology. A wide variety of databases were utilized, including the Applied Science and Technology Source, Art Abstracts, Avery Index to Architectural Periodicals, Incites Journal Citation Reports, Journal Storage, ProQuest Database, Springer Publishers, PubMed’s search engine, MEDLINE, CINAHL Nursing Journal Databases, Cochrane Library, PsycINFO database by the American Psychological Association, and Google Scholar. The Center for Health Design research repositories and International Academy for Design and Health resource library were also searched.
Literature Screening and Selection
Initial review results were screened by the investigator and two research assistants; irrelevant publications were eliminated after checking the titles and abstracts of the publications, which resulted in 49 publications, one book (Komiske, 2013), and two research reports (Almon et al., 2018; National Association of Children’s Hospitals and Related Institutions & The Center for Health Design, 2008) as candidates for the next round of review. The investigator further developed a series of selection criteria. Twenty-eight peer-reviewed publications were kept for the following round of review. The selection criteria were as follows: publication year/date between 2000 and June 2019, peer-reviewed publications in English language, studies focused only on private patient rooms and intensive care units were excluded, distractions not directly related to spatial design (e.g., handheld games/toys, parent/staff coaching programs) were excluded, and due to the high specialty in the research topic, studies focused on infection control in the pediatric healthcare environment were excluded, although some mentioned toys in a shareable space.
Literature Appraisal
It has been discussed recently in the field of evidence-based design that existing evidence should be appraised regarding the strength of recommendation for healthcare design. Stichler (2010) suggested a hierarchical strategy to rank six levels of evidence (Figure 1). The purpose of such critical appraisals was “not to develop a value judgment about the quality of the study or its findings, but rather to provide a tool to assist designers and healthcare leaders in determining whether statements about the effect of specific design features on outcomes are based on credible, reliable, and valid evidence” (Stichler, 2010, p. 6). Marquardt and Motzek (2013) developed two flowcharts to appraise and rank publications following Stichler’s framework, which was employed in the phase of literature appraisal (Figure 1). It was found that overall the 28 studies showed medium to high level of strength as evidence for healthcare design, with 19 publications ranked at Level 3, 6 ranked at Level 2, and 2 ranked at Level 1. One publication was excluded from this study since it ranked at Level 4 and discussed professional guidelines with studies and experts’ opinions to support such recommendations (Stichler, 2010, p. 7). Eventually 27 publications were reserved for the final round of review, thematic analysis, and in-depth discussions. Information about each publication’s level and citation frequency can be found in Table 1.
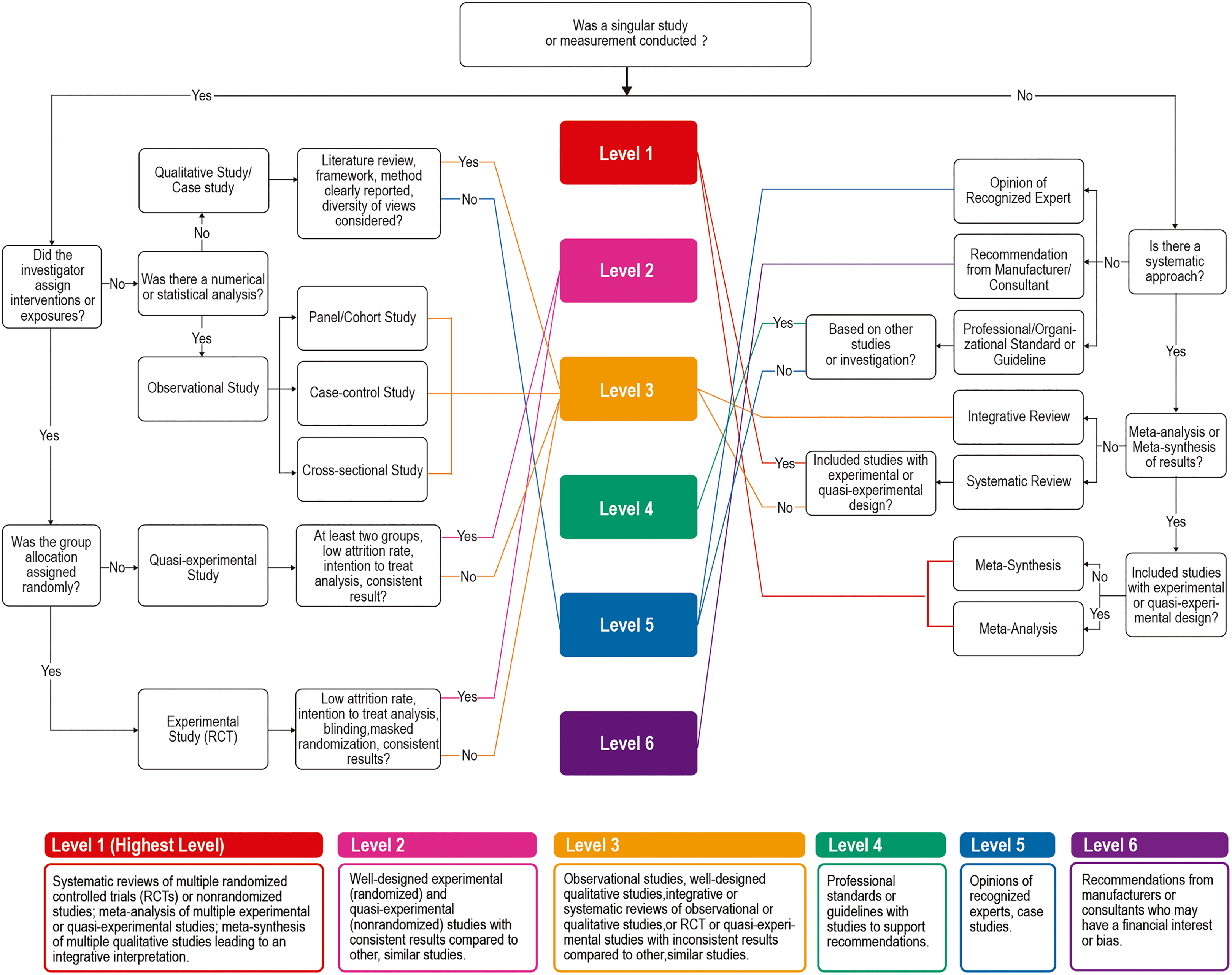
Research appraisal flowchart following Stichler’s (2010) framework, adapted from Marquardt and Motzek’s (2013) figure.
Detailed Content Review and Appraisal of the Level of Evidence for Healthcare Design of the 27 Peer-Reviewed Publications Included in This Study.

aNorton-Westwood (2011) paper was a literature review that mentioned multiple themes of positive distractions in pediatric healthcare design. It was categorized into Theme 1 in this table because art and environmental aesthetics aspects were the most discussed content in the publication. bThis article included multiple studies and measurements. However, since the article only introduced two studies without meta-synthesis of the results, it was categorized as Level 2 evidence. c Sherman, Shepley et al. (2005) paper was a literature review project that mentioned more than one theme of positive distractions in pediatric healthcare environment. It was categorized into Theme 5 because sound and lighting interventions were the most discussed content that were directly related to pediatric healthcare environment in the publication. dN/A means not applicable.
Thematic Analysis
The primary researcher (author of the manuscript) scrutinized the publications included in the final round of review and further categorized them according to the focused theme of positive distraction in each publication. Analytic notes were taken along the scrutinization, and codes and themes emerged from the concepts used in the publications. Conceptually similar themes were grouped together using the domain analysis as suggested by Spradley (1980): a series of themes were further grouped according to a semantic relationship such as “is a component of” or “is a type of” (Colorafi & Evans, 2016, p. 19).
Research Results and Findings
Six themes of positive distractions were identified: (1) art and environmental aesthetics, (2) spatial arrangement and atrium, (3) considerations of socialization patterns, (4) play and interactive technologies, (5) sound and lighting interventions, and (6) access to nature. The six themes were sequenced from interior features to outdoors, from general design features of the built environment, to design details and sensory stimulations. These themes of positive distractions were found to be associated with a variety of health benefits, including stress, anxiety, physiological arousal, pain and distress, levels of comfort and calm behaviors, emotional status, medical procedures and recovery, a sense of control or familiarity, socialization and social support, diurnal rhythms and sleep, waiting experience, levels of physical activities and contact with nature, patients’ perceptions of the environment, patient satisfaction, and the overall healthcare experience. Table 1 summarizes the details of the reviewed publications. Some publications examined more than one theme of positive distraction but were only categorized according to the original research intent and main research focus. Many publications explored more than one health benefit in association with certain positive distraction. Figure 2 illustrates the themes discussed in the publications and the associated health outcomes.
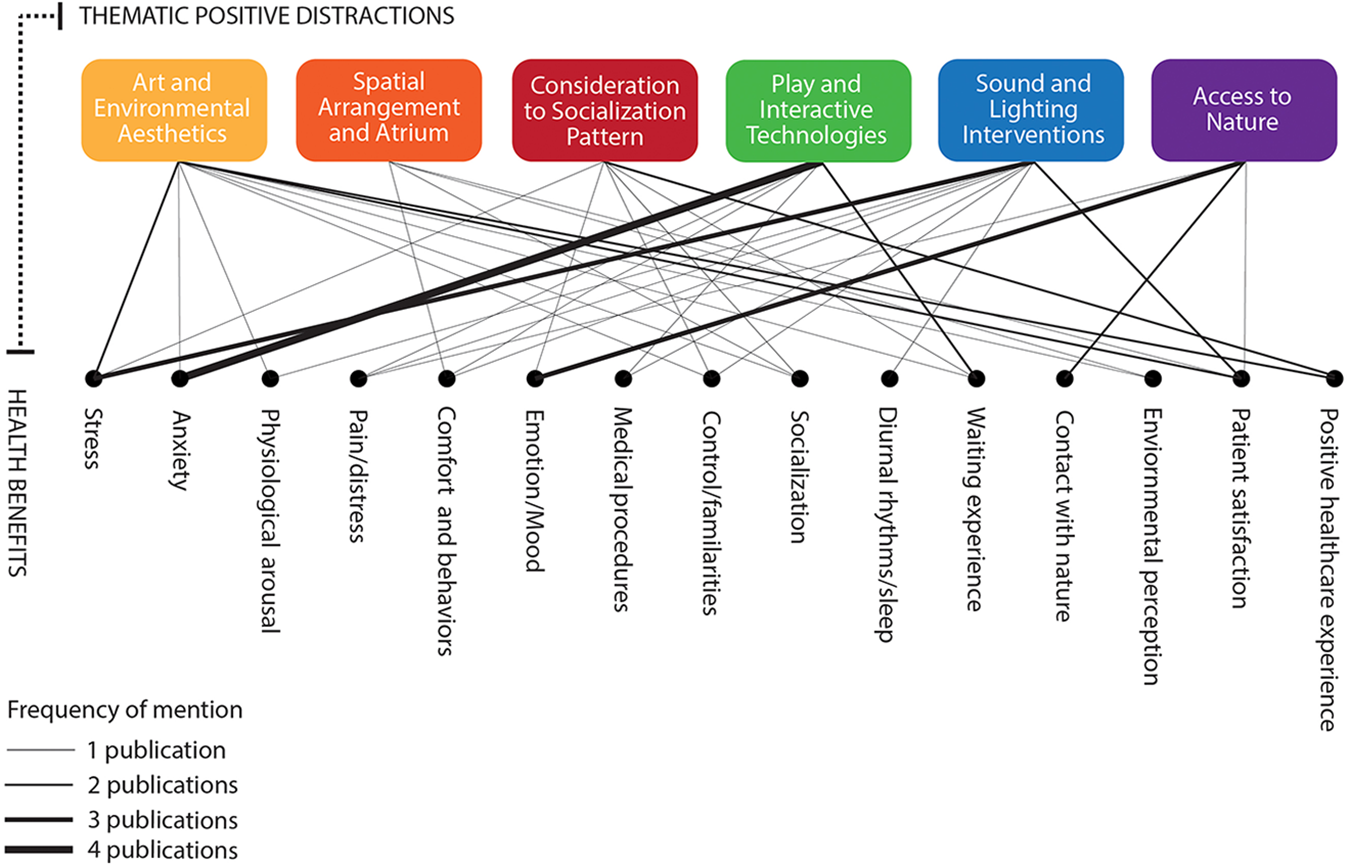
Themes discussed in the publications and the associated health outcomes.
Theme 1: Art and Environmental Aesthetics
Existing studies found that patients’ perceived quality of care is positively correlated to the perceptions of their physical environments. The makeup of an aesthetically pleasing environment could reduce patients’ stress and anxiety and improve patients’ healthcare experience and satisfaction. Six papers addressed the theme of art and environmental aesthetics, including interior design style and art work as decorations. Art work depicting nature and in a realistic style has proved to be more favorable than abstract art among adult patients (Nanda et al., 2011; Ulrich, 1999), and this finding is consistent among pediatric patients as well, regardless of their cognitive development stages (Eisen et al., 2008). Specifically, the thematic design of nature, such as ocean and beach views, was a universal desire in hospital designs for children (Coad & Coad, 2018; Pearson et al., 2019). In Varni and colleagues’ (2004) study aimed at developing an evaluation tool kit of the built environment of children’s hospitals, it was found that facility aesthetics (e.g., the overall appearance and the decoration of the interior of the facility, color of the walls and pictures in the hallways, visual and sensory stimuli, the windows and daylight, and room furniture) were closely associated with the pediatric quality of life and parent and staff satisfaction.
Pediatric patients’ preference for environmental aesthetics vary among age-groups; childish decorations were actually disliked by adolescent patients who had already developed mature personalities (Tivorsak et al., 2004). However, the “fear” of medical equipment seemed to exist among all age-groups of pediatric patients, who had a desire to hide it (Norton-Westwood, 2012; Tivorsak et al., 2004). Some controversial conclusions about the color range pediatric patients preferred emerged: Children and young patients preferred pale to mid color ranges and mid blue-green colors (Coad & Coad, 2008; Tivorsak et al., 2004), although previous studies had suggested bright colors were preferred (Redshaw & Smithell, 2000). In general, pediatric patients preferred a rich variety of color, age-appropriate thematic artworks, and a sense of “not looking like a hospital” (Bishop, 2012, p. 83). Bishop (2012) further explored whether adding interactive art activities/tasks in the public pediatric spaces may promote the therapeutic effect of art, meaning it is not simply a graphic treatment but also functions in the ways that young patients “identified as being valuable in their experience of hospitalization” (p. 81). It is worth noting that using participatory design strategy and a children’s advisory group during the design of aesthetically appealing healthcare environments seemed to be an efficient approach for revealing children’s special needs and preferences (Coad & Coad, 2008; Koller & McLaren, 2014).
Theme 2: Spatial Arrangement and Atrium
Three publications addressed programming and spatial arrangement issues in pediatric healthcare environments, and two publications studied the same hospital atrium spaces in a contemporary Canadian pediatric hospital that has color, art, a water feature, and commercial venues as distractions. Adams et al. (2010) interviewed young participants about their perceptions of the central atrium spaces of a children’s hospital. The authors concluded that the architectural scale of spatial design impacts young patients’ perceived sense of the intimacy of the space. The public atrium enhanced opportunities to socialize and was associated with young patients’ emotional status. It was a place to see, be seen, and be involved in the social life of the hospital. The central atrium, with its memorable features, could ease navigation and improve wayfinding experiences. The atrium’s atmosphere of consumption (i.e., shopping mall) provided distractions for patients and families (Adams et al., 2010; Koller & McLaren, 2014). Ghazali et al. (2013) concluded that the design of pediatric healthcare facilities should focus on improving character and innovation, use, and access; understandable healthcare buildings and spatial arrangement could improve patient experience. Koller and McLaren (2014) also reported the absence of specialized spatial design for children, especially environments where play should occur, in the public open spaces within a children’s hospital.
Theme 3: Consideration of Socialization Patterns
Only three publications addressed the opinion that the design needed to include social spaces for young children in healthcare facilities, and two of them were by the same research team. Lambert et al. (2013) found that 5- to 8-year-old patients expressed a strong sense of isolation during hospitalization. They wanted to feel socially connected to the internal hospital community as well as the outside world. The authors concluded that there is a need to include “a diversity of readily available, independently accessible, age, gender and developmentally appropriate leisure and entertainment facilities seamlessly integrated throughout the hospital environment” (p. 203). Lambert and colleagues also stressed that today’s technology offers many opportunities to support children’s psychosocial well-being when in confined healthcare spaces; however, the implementation and operation of such services and systems require much further research in the areas of ethnics, facilitation, organizational impact, and evaluation (p. 195). In another study about waiting experience among young patients (7–15 years old) and their families, the young patients displayed a low level of anxiety and negative emotion (excluding boredom), whereas adults’ experience of waiting entailed boredom, anxiety, and concern for the health status of their children (Corsano et al., 2015). Pediatric waiting areas should be experienced by adults and patients as relational spaces (p. 1066). Design features and activities should support patients’ sense of control over their emotions and fears for the uncertainty. Patients and parents would like a waiting area with the presence of positive social and spatial distractions and entertainment activities. Adult parents’ stress and anxiety could be alleviated through relationships with others by sharing emotions and engaging in more relaxed interactions with the children (Corsano et al., 2015).
Theme 4: Play and Interactive Technologies
The theme of play and interactive technologies has attracted an increasing number of researchers’ attention in recent years. Previous studies criticized that traditional toys, whether plastic or metal, could be contaminated with potentially dangerous bacteria and might provide unnecessary risks for nosocomial infection in certain pediatric healthcare environments (Avila-Aguero et al., 2004; Bocchini et al., 2007; McKay & Gillespie, 2000). Therefore, positive distractions provided through digital displays (e.g., television [TV] screens) and nontouchable medium, virtual reality, and ambient environment emerged in the design of pediatric settings. Health benefits associated with play and interactive technologies included reduced pain and distress during medical procedures, reduced anxiety, reduced arousal, and calm behaviors and tranquility among pediatric patients. Pati and Nanda (2011) found that multisensory stimuli displays and ambient art could help calm pediatric patients’ behaviors and effectively hold their attentions when waiting. Virtual reality could be an efficient distraction during painful medical procedures (Wolitzky et al., 2005). Computer-mediated, augmented environments could efficiently assist with young patients’ rehabilitation process related to visuo-perceptual and motor planning skills (Chau et al., 2006). Furthermore, nature-themed content (e.g., nature, aquarium, animals, and zoo) positively distracts young patients’ attention and relieves anxiety relief (Biddiss et al., 2018; Pati & Nanda, 2011; Wolitzky et al., 2005). However, most existing studies examined the positive distractions as objects, and the spatial designs used to accommodate these play opportunities were rarely mentioned.
Theme 5: Sound and Lighting Interventions
Noise can arouse stress. Noise in pediatric healthcare environments has been shown to be associated with increased stress and physiological arousal among neonatal patients (Sherman, Shepley, et al., 2005). Natural sound intervention has been found to be therapeutic by reducing noise, enhancing tranquility, and calming adolescent patients’ behaviors in waiting areas (Watts et al., 2016). Watts and colleagues (2016) also compared music and natural sound and found that music could play a role in well-being, but personal choice was an important factor that impacted the level of effectiveness of music as a positive distraction. In contrast, natural sounds, especially water sounds, were generally regarded as positive distraction (p. 140).
Technology has enriched the opportunities for sound and lighting interventions in the design of healthcare environments, such as using colorful ambient lighting to match the theme of animation and art. Quan and colleagues (2016) found that ambient lighting and animation interventions in a radiographic scan environment could help shorten the time of medical procedures, enhance parental satisfaction, and potentially reduce patients’ stress. Patients and adults experienced less stress, less pain, and higher satisfaction levels in ambient emergency departments with colorful lighting distractions and child-friendly animations projected on the wall (Robinson & Green, 2015).
Theme 6: Access to Nature
Five publications explored hospital gardens and user behaviors in pediatric healthcare environments. Three studies were post-occupancy evaluations (POEs) that employed methods including on-site observations and behavior mapping/tracing, interviews, and surveys. Whitehouse and colleagues’ (2001) seminal POE study brought the topic of healing gardens in pediatric healthcare environments to researchers’ attention. They found that the garden space was perceived as a place of restoration and healing, and garden use was accompanied by increased consumer satisfaction, enhanced emotional respite for visitors, and reduced pain and distress (Reeve et al., 2017; Sherman, Varni, et al., 2005; Whitehouse et al., 2001). Visitors who used the garden spaces appreciated the features and benefits provided by healing gardens, such as a place to get away, restorative experience, fresh air, sunshine, views, and fun and play (Reeve et al., 2017). However, the garden was not utilized as frequently and effectively as planned due to the low visibility (Whitehouse et al., 2001). Sherman, Varni, and colleagues’ (2005) study found that the largest garden in a pediatric cancer center with the most direct patient access was the most used space. Pasha’s (2013) study further revealed that a lack of knowledge about the existence of the garden, low visibility, and limited accessibility to the garden spaces were major barriers to garden visitation in a Children’s hospital.
Despite the child-friendly design of most pediatric gardens, staff and adult family members were the overwhelming majority of garden users, and only around 5% of the total garden users were children (Sherman, Varni, et al., 2005; Whitehouse et al., 2001). Adults mostly engaged in sedentary activities or simply walked through the garden whereas children engaged in significantly more interactive activities with play structures and natural elements (Pasha & Shepley, 2013; Sherman, Varni, et al., 2005; Whitehouse et al., 2001). Sherman, Varni, and colleagues (2005) also discovered an inverse relationship between the number of people in the gardens and the use of windows in ground-level patient rooms: As the number of people increases, fewer patients are likely to keep their window blinds open. The most popular garden was most likely to have closed windows, and the least populated had the most open windows (Sherman, Varni et al., 2005, p. 178). Design features that could potentially encourage garden usage by children included (1) a variety of high-quality seats and child-scaled furniture; (2) improved accessibility and circulation; (3) more trees, greenery, and shade; (4) a pleasant microclimate; (5) playful features that encourage play activities; and (6) security and privacy (Pasha, 2013; Pasha & Shepley, 2013; Sherman, Varni, et al., 2005; Whitehouse et al., 2001).
Discussion
Answering Research Questions
This article reviewed studies about the design of public spaces in pediatric healthcare environments, positive distractions, and the associated health outcomes by analyzing 27 peer-reviewed publications published in recent 20 years to answer the research questions stated earlier in the paper. The results indicated that environmental design features that young patients and family members in a pediatric healthcare environment perceived as positive distractions could be categorized to six themes: art and environmental aesthetics, spatial arrangement and atrium, play and interactive technologies, considerations of socialization patterns, sound and lighting interventions, and access to nature. A wide range of health benefits could be provided by appropriate positive distractions in the care environment, including physiological, psychological, emotional, behavioral, and social benefits. Young children and adolescents were found capable of perceiving their surrounding environments as well as expressing their preferences for and needs related to the design of the physical features of a healthcare facility. However, many publications reviewed in this study were passive observations of children’s behaviors or survey with adults. There is still insufficient knowledge about what constitutes a child-friendly hospital environment from young children’s perspectives.
The age factor played a role in understanding children’s perceptions about various design features. Preliminary evidence indicated that spatial designs and features should accommodate different age-groups’ developmental stages (Tivorsak et al., 2004); infants need intimacy and loving personal contact, while the desire to have independent spaces, purposeful activities, and social interaction increased as children grew older (Olds, 1981). Including subspaces for different age-groups with age-appropriate thematic designs and decorations may fulfill different users’ needs (Zabloudil, 2017). Using a waiting room space as an example, Figure 3 compares a traditional waiting room to a humanized pediatric waiting room as adapted from previous theories (Olds, 1981). Designs to encourage social interactions are important for both young patients and their families. Hospital environments need to be designed not just to be child friendly in environmental aesthetics but to also respect children’s right to dignity, privacy, cognitive development, social support, and self-control.

Comparison between a traditional waiting room and a humanized pediatric waiting room as adapted from Olds’ (1981) study.
Nonenvironmental Positive Distractions
This study included positive distractions that are directly related to the physical environment of pediatric healthcare facilities. However, it is worth to point out that many nonenvironmental resources could also provide positive distractions to pediatric patients and families, especially to alleviate pain and distress associated with medical procedures. Through a meta-analysis, Kleiber and Harper (1999) confirmed that distractions had a positive effect on children distress behaviors and perceived level of pain. Nonenvironmental positive distractions examined by Kleiber and Harper (1999) included music/story via earphones, distraction with party blower, imagery, breathing pattern, toy, and nonprocedural talk by a professional. Koller and Goldman (2012) conducted a systematic review and summarized two domains and several subdomains of distraction techniques for children undergoing procedures to control pain, including active distraction (i.e., interactive toys, virtual reality, controlled breathing, guided imagery and relaxation), passive distraction (i.e., music and TV), and a mixture of active and passive distractions.
Organizations and nonenvironmental programs also play significant roles in providing positive distractions, such as the child life profession whose original goals were to improve healthcare experiences through providing play, preparation, family participation and educational programs (Association of Child Life Professionals, n.d.). Music therapy programs have expanded the wide acceptance of the practice in the pediatric healthcare delivery system. Resources such as the American Music Therapy Association and Journal of Music Therapy have documented a substantial amount of empirical studies about the various health benefits of music therapy in pediatric settings (Gooding et al., 2015; Millett & Gooding, 2017). Horticultural therapy programs, as an effective therapeutic modality that involves plants and horticulture to support an established treatment plan (American Horticultural Therapy Association, n.d.), have been implemented in a few pediatric healthcare settings, including the indoor garden suite at the UH Rainbow Babies & Children’s Hospital in Cleveland (Marolf, 2016).
Play therapy is a psychotherapeutic approach primarily used to help children with social or emotional deficits to explore their lives, solve problems, and freely express repressed thoughts and emotions through play (Association for Play Therapy, n.d.). Researchers promoted therapeutic play activities as far back as 1919 (Schaefer & O’Connor, 1983) in order to reduce children’s stress, express feelings of anger, cry, and ask questions (Erikson, 1963; Linn et al., 1986). For young patients who stay in a hospital longer, play can promote normal life experiences while maintaining and supporting the developmental, cognitive, social, and emotional health of the children thereby facilitating the development of hardiness and resiliency as well as the ability to master critical experiences (Bolig et al., 1986; Bratton et al., 2005). Usually such alternative therapy programs need dedicated spaces and specialties to assist with the process. However, it remains unclear that how spatial design and features could facilitate various therapy programs in a pediatric healthcare facility.
Research Gaps and Future Directions
To identify current research strengths and the knowledge gaps, Figure 4 demonstrated the themes of positive distractions, number of publications, and the different types of facilities/public spaces studied in the publications. Significant research gaps were identified through this literature review. There seemed to be a universal preference of nature among children; however, the garden spaces in many pediatric healthcare environments were not effectively used as intended by young patients (Pasha, 2013; Sherman, Varni, et al., 2005; Whitehouse et al., 2001). Gardens and nature are the ideal places to stimulate and nurture ill children’s senses as they can experience diversity of forms, colors, shapes of landscape elements, and dynamism of climatic factors (Said, 2003). With proper design and implementation, the hospital garden spaces can be made into therapeutic platforms for the children and their healthy siblings to play, rest, and socialize (Said, 2003). Future research should focus on how to promote longer stay in a garden space and how to engage children more actively with playful features.
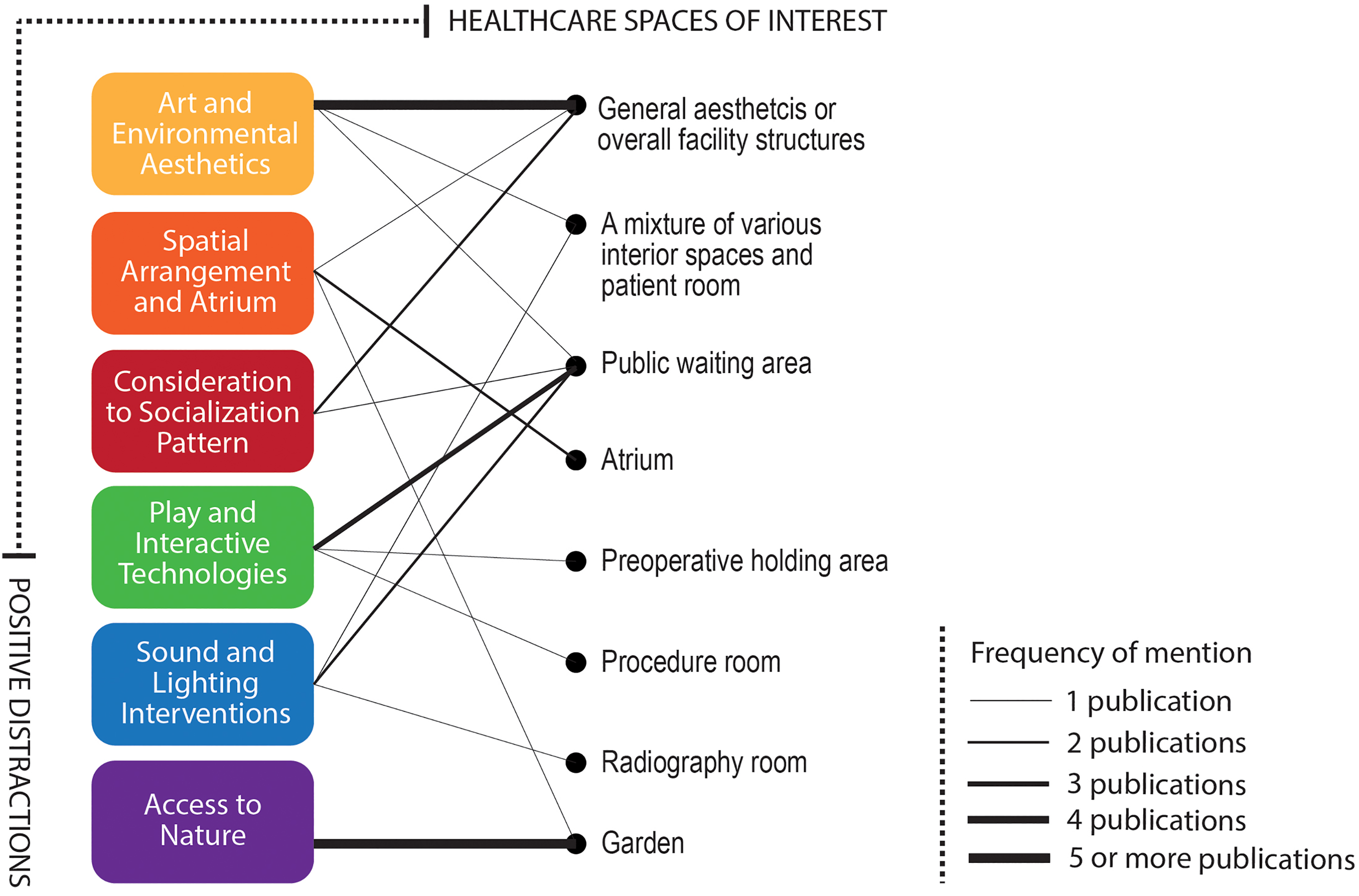
Themes of positive distractions, number of publications, and the different types of facilities/public spaces studied in the publications.
Play is the child’s language and toys are the child’s words (Association for Play Therapy, n.d.). Play could be an ideal positive distraction among children and young patients; however, existing studies examined the play device/opportunity only as an object, and very few discussed the spatial design to accommodate various play programs in a pediatric healthcare environment. Socialization patterns among pediatric patients require attentions when designing the physical environments of pediatric healthcare facilities. In-patient pediatric patients desire internal connections to the healthcare community, as well as external connections to their friends, the school, and a normal life. Such bonding between patients, family members, and caregivers could be promoted through play. Play in the realm of public health has consistently remained a research interest among researchers (Almon et al., 2018), yet play and spatial design for play seem to have been less studied in recent years, leaving a significant research gap in the realm of pediatric healthcare design.
Attracting children’s attention could be considerably more challenging than those of adults, especially those children with neurobehavioral development disorders and attention problems (Pati, 2010, para. 13). Interactive technology could effectively hold pediatric patients’ attentions. Ambient environment with multisensory stimulations and immersive virtual realities could calm behaviors, relieve anxiety, and enrich children’s enjoyable experiences during hospitalization. Technology is developing rapidly, but updates to physical features and spaces in a healthcare facility may not catch up in time. Designing flexible spaces that can easily be transferred to accommodate new technology may be a future direction in both practice and research.
Implications for Practice
A rich source of natural and thematic decorations should be integrated in the design of pediatric healthcare environments.
Spatial design should promote occupants’ play behaviors and hide “scary” medical equipment/supplies.
Strengthen social connectivity and provide opportunities for both children and adults to socialize in a shared space.
Interactive technologies, sound, and lighting interventions could be effective play opportunities and positive distractions.
Hospital gardens should be visible and accessible to all. Attractive landscape features, abundant shade, comfortable seating, choices of socialization or privacy, and guaranteed safety could enhance the usage of the garden spaces.
Children have the ability to identify multifaceted issues related to hospital design. Including a “children advisory board” could be an efficient strategy to understand the needs from young patients’ perspectives and involve patients in decision-making during the design of pediatric healthcare environments.
Supplemental Material
Supplemental Material, sj-pdf-1-her-10.1177_1937586720901707 - Positive Distractions and Play in the Public Spaces of Pediatric Healthcare Environments: A Literature Review
Supplemental Material, sj-pdf-1-her-10.1177_1937586720901707 for Positive Distractions and Play in the Public Spaces of Pediatric Healthcare Environments: A Literature Review by Shan Jiang in HERD: Health Environments Research & Design Journal
Footnotes
Acknowledgment
I thank my research assistants, Krisha Redillas, Yasmeen Juma, and Udday Datta, from West Virginia University, who provided assistance in the early phase of the manuscript development.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially funded by 2017–2018 U.S. Play Coalition Research Seed Grant and West Virginia University Research Apprenticeship Program.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.