
Abstract
Aim:
To investigate: (1) the types of health information, resources, and supports available to consumers in hospital outpatient waiting areas and (2) whether these are accessed by consumers.
Background:
Outpatient waiting areas commonly offer health information, resources, and supports to improve the health literacy of waiting consumers. It is not known what is available to or accessed by consumers in hospital outpatient rehabilitation waiting areas.
Methods:
A multicenter, prospective, observational, cross-sectional study was conducted in the waiting areas of two hospital outpatient rehabilitation services. Direct observations (in person and video recordings) of the waiting areas were used to describe what health information, resources, and supports were available and, if present, what was being accessed and for how long by consumers.
Results:
Fifteen hours of in-person and video-recorded observations were documented on purpose-designed instruments across the two sites during 18 observation sessions over 8 days. A total of 68 different health information and resources were identified. Approximately half were specifically for consumers (Site 1: 57%; Site 2: 53%). Only seven (10%) were accessed by consumers across both sites. Each resource (n = 7) was only accessed once. Health resources were used by consumers for 0.8% (3/360 min) of the observation time at each site. Health and social supports and use of other non health resources were also observed.
Conclusions:
Available health information, resources, and supports were infrequently and briefly accessed by consumers. Further research is required to explore what consumers want and need to improve the health literacy responsiveness of hospital outpatient waiting areas.
Keywords
The World Health Organization (WHO) recognizes health literacy as a priority area for global research and policy development to improve health outcomes, address health inequities, and reduce economic burden (Kickbusch et al., 2006; WHO, 2016). Health literacy influences health decisions and behaviors and in turn is associated with health outcomes (Dodson et al., 2017). Given this relationship, health literacy is recognized as a contributing factor to disease burden, poor health outcomes, and high economic cost (Eichler et al., 2009; Sheridan et al., 2011). Health literacy interventions can be targeted at multiple levels including at the health environment, health service, and systems levels (McCormack et al., 2017). Interventions at these levels aim to influence “health literacy responsiveness” which refers to “the way in which services make health information, resources, supports and environments available and accessible to people with different health literacy strengths and limitations” (Dodson et al., 2017). Targeting the health literacy responsiveness of health services represents an important philosophical shift away from “blaming” the health literacy ability of the individual (Frosch & Elwyn, 2014). Instead, this approach emphasizes the need to create person-centered healthcare environments (Frosch & Elwyn, 2014). Health literacy responsive environments that meet the health literacy needs of consumers may positively influence health literacy and have other benefits such as promoting equity and inclusiveness (Trezona et al., 2018). There is a growing international effort to create “health literacy responsive” health services and organizations (International Union for Health Promotion and Education, 2018).
Outpatient waiting areas are an example of a local health service environment that may have the potential to influence consumer health literacy through two key mechanisms. First, outpatient waiting areas commonly make health information and resources available for waiting consumers to access (Williams et al., 2019). This typically includes a range of physical items such as posters, brochures, and audiovisual displays (Moerenhout et al., 2013). Second, waiting areas offer opportunities for naturally occurring social support (Cohn, 2001). Social support may include sharing of health knowledge, advice, resources, experiences, and emotional support (Heaney & Israel, 2008). Social support can enhance health literacy and health outcomes (Heaney & Israel, 2008; Lee et al., 2004). Although the long-standing practice of making health information, resources, and supports available in waiting areas is widely accepted, it is not underpinned by robust evidence.
Little is known about what is available in hospital outpatient waiting areas to support health literacy. There is some evidence from general practice settings that a range of health information is often available in the waiting area, and when accessed by consumers, this has the potential to improve health literacy (Cass et al., 2016). Some studies from general practice environments, however, have cautioned that not all available information was accessible to consumers (Maskell et al., 2018; Protheroe et al., 2015). This highlights that outpatient waiting areas may offer health information and resources; however, these will only translate into improved health literacy if they are accessible to consumers. Issues affecting the accessibility of health information and resources could include language barriers, (health) literacy skill level, physical impairments (i.e. vision or hearing loss or mobility impairments), mental and social well-being, or technology barriers (Ramsay et al., 2017). In summary, there is a lack of evidence regarding (1) what health information and resources should be available in hospital outpatient waiting areas to support health literacy and (2) how to make such information and resources accessible to consumers.
Therefore, the aims of this study were to investigate (1) what types of health information, resources, and supports are available to consumers in hospital outpatient rehabilitation waiting areas and (2) whether these are accessed by consumers. This is the first step in a program of research exploring the health literacy responsiveness of outpatient waiting areas. Understanding these issues is a necessary precursor to a meaningful and nuanced exploration of whether the environment is responsive to the health literacy needs of consumers.
Method
Study Design, Setting, and Sample
A multicenter, prospective, observational, cross-sectional study was conducted in the consumer waiting areas of outpatient rehabilitation facilities at two tertiary hospitals (Melbourne, Australia) from May 2019 to July 2019. All sites had ethical approval (Melbourne Health Human Research and Ethics Committee, Approval number HREC/43635/MH-2018). The two hospital services were public-funded hospitals, and the waiting areas were for consumers attending appointments in the outpatient rehabilitation service (ambulatory care) which offers goal-based multidisciplinary therapy for consumers for a range of health conditions and injuries. Both hospital waiting areas had health information and resources available for waiting consumers which were selected and displayed by staff without consumer involvement. There were no participants recruited into this study; rather, this was an investigation of the environment and activity within these waiting areas. This study was reported according to the Strengthening the Reporting of Observational Studies in Epidemiology cross-sectional reporting guidelines (von Elm et al., 2008).
Measurement
The study was conducted in two parts. Parts 1 and 2 involved direct, semi-structured observations (Hanington & Martin, 2012). Part 1 involved direct observations of the waiting area environment and artifacts to describe what types of health information, resources, and supports were available. Part 2 involved direct observations of consumer activity in the waiting area to determine which health information, resources, and supports were being used, for how long, and what other activities were occurring in the waiting area. Health information is defined as information about illness, symptoms, treatment, or health services and healthcare more broadly (Ramsay et al., 2017). Resources are defined as tools that consumers can use or draw on to learn more about their care or to participate in their own care (Ramsay et al., 2017). Supports include social or peer support, which may include emotional or informational support, provided to consumers as they access services or make decisions about their care (Lee et al., 2004). Health information and resources are typically tangible (i.e. information displays or physical items), whereas supports are often intangible (i.e. shared through interactions or conversation). Any information or resources that were signposted for staff (i.e. with a heading over the display of “staff resources”) or were displayed with the primary intent for staff to read, rather than consumers, were classified as “staff-focused” resources. Examples of staff-focused information displayed in the waiting area included deidentified consumer feedback, detailed descriptions of local service and quality improvement projects, staff survey results, and hospital policies.
Qualitative observations allow the researcher to gain insight into the naturalistic environment of healthcare settings (Malagon-Maldonado, 2014; Pope & Mays, 1995). In particular, observations can capture the influence of the physical environment on culture, activity, and behavior (Mulhall, 2003) and subsequently inform evidence-based, person-centered health service design (Malagon-Maldonado, 2014).
Two semi-structured instruments were specifically designed for Parts 1 and 2 to guide observations and record data relating to health literacy. They prompted the researcher to observe the waiting area environment for artifacts, people, and activities which may influence health literacy. They also prompted observations of other activities or interactions to explore what else was occurring in the waiting area. The instruments allowed flexibility in keeping with the naturalistic paradigm while facilitating systematic and detailed data collection (Mulhall, 2003). The instruments were piloted to ensure ease of use, applicability, and clarity.
The timing and number of observation periods were purposively sampled as it was posited that the availability of resources and their use may fluctuate depending on the time of day and the number of consumers in the waiting area. For example, in “quiet” periods, it was hypothesized that there may be limited to no opportunities for sharing health information through social interactions. Alternatively, a higher number of scheduled appointments could result in a “busy” period in the waiting area. Quiet and busy periods were defined a priori based on the number of scheduled appointments: A busy period in the waiting area was defined as times when there were more than 30 scheduled appointments within the hour, and a quiet period was defined as less than 20 appointments within the hour. Six observations were conducted during quiet periods and 10 during busy periods. Direct observations were 30–60 minutes in duration. Data collection ceased once a purposive sample of 15 hours of direct, semi-structured observations over 2 months had been undertaken.
Part 1
In Part 1, three direct observations at each hospital site were performed by an independent researcher to provide a detailed descriptive account of what health information, resources, and supports were available to consumers in the waiting areas of each outpatient service. Each direct observation (six in total) ran for 30 minutes in duration. During this period, data were recorded in the purpose-designed instrument and in field notes. Data collected included health information, resources, and supports available in the waiting area—recorded in terms of narrative descriptions, numerical counts, and images (photographs). Health information, resources, and supports can be shared with consumers in many mediums such as verbal exchanges, written resources, or audiovisual media. Therefore, any medium that had the potential to increase health knowledge was included.
The first direct observation at each site was conducted when the outpatient service was closed (no consumers present) to focus on tangible resources. The second and third direct observation at each site occurred during a quiet and busy time, respectively, to focus on intangible items. The tangible, physical resources set up in the waiting area (i.e. posters and brochures) are unlikely to change (whether or not consumers are present); however, the intangible health information exchanges or supports (i.e. social interactions) may fluctuate depending on how busy the waiting area is at a given time.
Part 2
In Part 2, six observation occasions were conducted at each hospital site by the same researcher to provide a detailed account of how often and for how long health information, resources, and supports were accessed by waiting area users. The term “accessed” referred to engaging, reading, watching, or interacting with available health information, resources, and supports. “Waiting area users” may include patients and accompanying support people such as carers, family members, caseworkers, and friends. There was often no way to differentiate carers and support people from patients during the observations. Therefore, we have referred to them collectively as consumers in this study. Each direct observation ran for 60 minutes in duration, and observations were recorded at 1-minute intervals on a predetermined instrument and in field notes. Three of the direct observations at each site were conducted in person and three via video-recorded observation. Data collected included the number of consumers waiting, the number of consumers accessing resources, and the type and duration of resource use. These were recorded as numerical counts and narrative descriptions. Observations were conducted during busy and quiet periods.
For the video observations, an unobtrusive, portable video camera was installed to record the waiting area. A sign was displayed indicating when videoing was underway and the area being captured. The purpose of video recording the waiting area was to capture detailed data that may not feasibly be collected through in-person observation alone. For example, video recording affords the researcher the opportunity to rewind and replay footage so that data are not potentially “missed” which is a risk of an in-person observation (i.e. if interrupted or distracted during the observation). An additional purpose of the video recordings was to allow researchers to check whether their presence in the waiting area, despite efforts to be discrete, was influencing consumer behavior. Social desirability bias can cause consumers to alter their behavior when a researcher is present (Tashakkori & Teddlie, 2003). Observations recorded during video recording were compared to in-person observations as a form of triangulation (Higginbottom et al., 2013), incorporating the strategies of prolonged engagement and persistent observation into data collection by repeating observations using in-person and video methods (Morse, 2015).
Data Analyses
All data were analyzed through Statistical Package for the Social Sciences (SPSS) Windows Version 26.0 (IBM, Chicago, USA). Data were analyzed and presented descriptively. Data were assessed for normality using the Kolmogorov–Smirnov test. Nonparametric variables are reported as median and interquartile range, and parametric data are reported as mean and standard deviation. Categorical data are reported as minimum and maximum and/or frequency and percentage.
Results
Between May 2019 and July 2019, 15 hours of observation was completed during 18 observation periods. This involved six direct observation periods in Part 1 for a duration of 30 minutes each (total 3 hours). A further 12 observation periods in Part 2 were conducted for 60 minutes each (total 12 hours).
Available Health Information and Resources (Part 1)
There were 60 and 64 resources in total available in the waiting area at the two services, respectively (Table 1). At both sites, 34 of these resources (57% Site 1, 53% Site 2) were for consumers. These included brochures, posters displaying health information, signs highlighting health service information, handouts, business cards promoting the hospital’s telehealth service, feedback forms, and “other” resources (Table 1). The most common type of resource available at both sites was “posters” (50% Site 1, 38% Site 2).
Summary of Resources Available in Each Waiting Area.

Note. Resources are described in Available Health Information and Resources (Part 1) in the “Results” section.
a Brochures were defined as folded pamphlets or booklets with printed information.
b Handouts were defined as a single sheet or single page of printed information.
The resources displayed health information on a range of topics such as diabetes, hypertension, Parkinson’s disease, stroke, osteoarthritis, and dementia. They also advertised information on healthcare rights, peer support programs, other local health services and programs, elder abuse, health campaigns (i.e. influenza vaccination, benefits of exercise, smoking cessation), workplace injury, and transport accident claims. The layout of the waiting area environments and the location of information and resource displays are depicted in Figures 1 and 2.

Site 01 outpatient waiting area.

Site 02 outpatient waiting area.
During quiet and busy observation periods, naturally occurring social support was observed at both sites. Social interactions included the exchange of health information and recent healthcare experiences and general conversations. Social supports are described further in “health supports” and “other activities” in Part 2. Nearly half the available resources (43% Site 1, 47% Site 2) in each waiting area were for staff use (Table 1), and these were either posters or handouts.
Use of Available Information and Resources (Part 2)
The number of waiting consumers fluctuated at both sites. During quiet periods, no consumers were present in the waiting area. At busier times, most seats were taken with a maximum number of 22 waiting consumers present (Table 2). The turnover of consumers in the waiting area was constant during these busier periods. The researcher observed brief waiting times for consumers which may be one of the reasons for the subsequent findings.
Summary of Health Information and Resource Use.
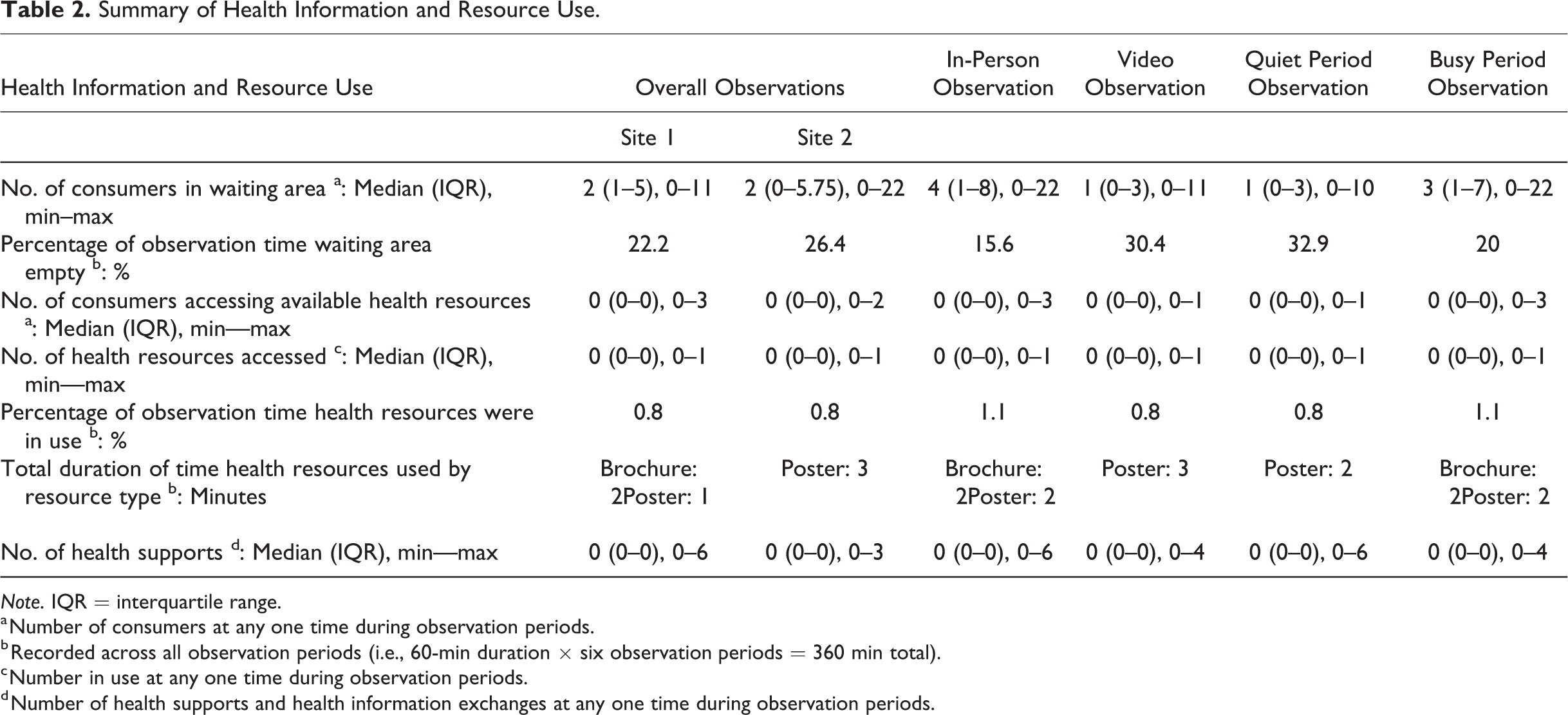
Note. IQR = interquartile range.
a Number of consumers at any one time during observation periods.
b Recorded across all observation periods (i.e., 60-min duration × six observation periods = 360 min total).
c Number in use at any one time during observation periods.
d Number of health supports and health information exchanges at any one time during observation periods.
Summary of Other Resource Use and Other Activities.
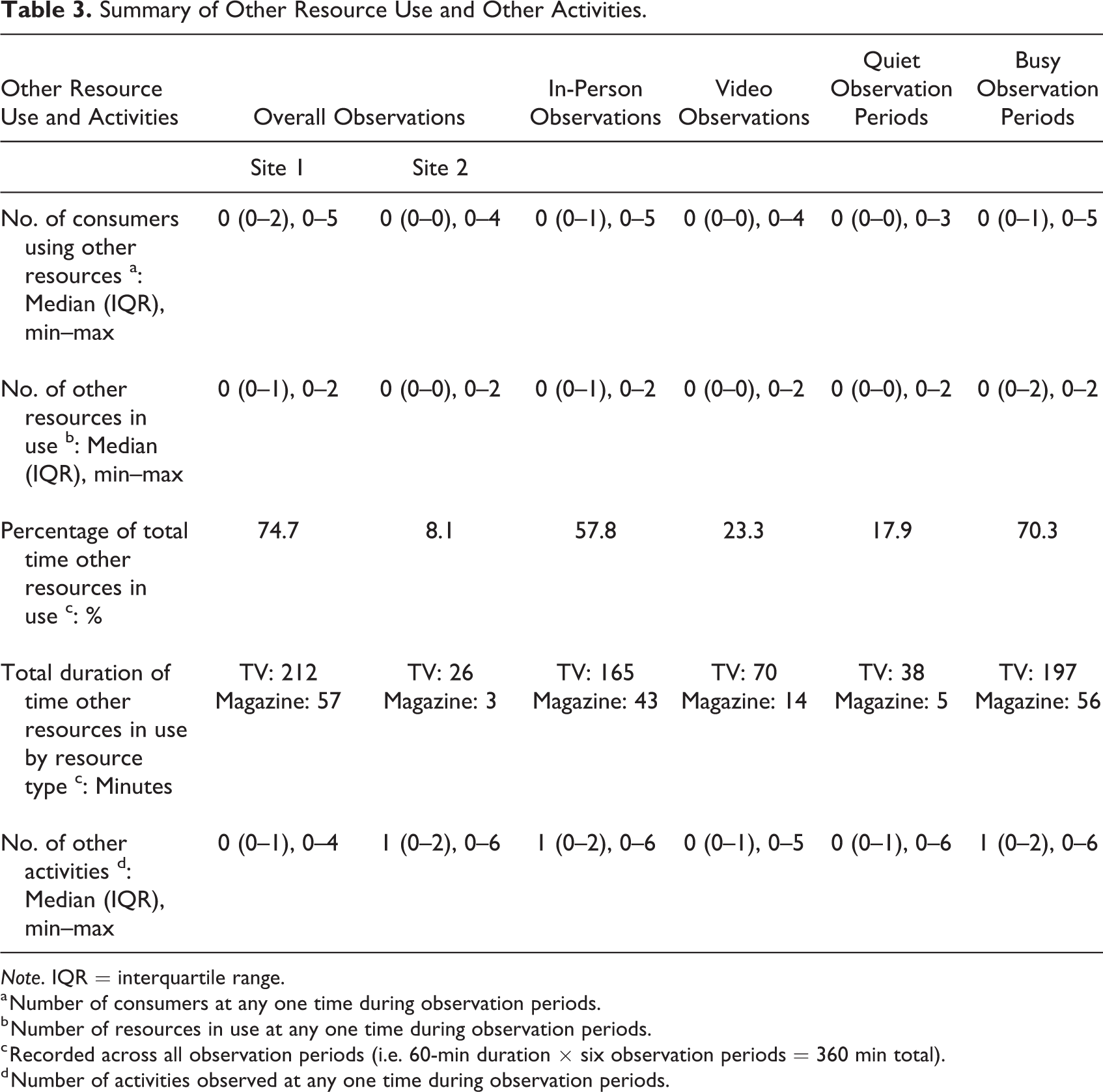
Note. IQR = interquartile range.
a Number of consumers at any one time during observation periods.
b Number of resources in use at any one time during observation periods.
c Recorded across all observation periods (i.e. 60-min duration × six observation periods = 360 min total).
d Number of activities observed at any one time during observation periods.
Use of available health resources
The number of consumers accessing the available health resources at any one time was very low (maximum number of consumers accessing health resources at any one time: Site 1 = 3; Site 2 = 2; Table 2). Throughout all observations, consumers were observed using available health resources infrequently and for short durations. The available health resources were accessed and used for a total duration of 3 minutes at each site across the 360 minutes of observation.
Coincidentally, the same total number of 68 consumer health resources were available, and similar trends of use were observed at both sites: Only four health resources were accessed by consumers at Site 1 and just three were accessed by consumers at Site 2. At Site 1, three different brochures and one poster were accessed. The three brochures were accessed on one occasion for 2 minutes by a consumer. Each of the three brochures contained information about different programs offered by a local community health service. The consumer read the brochures and took copies with them as they left the waiting area. The poster was read by a consumer for 1 minute. This poster displayed hospital “emergency procedure” information for staff. At Site 2, three posters were accessed by consumers. One poster displayed on a pinboard in the seated waiting area explained the signs of stroke. This poster was read by a consumer for 1 minute. Two consumers separately engaged for 1 minute each with posters displayed on the wall of the corridor adjacent to the seated area. The posters they stopped to read showed the local hospital “area wardens” and “occupational health and safety” displays, information that is displayed for staff. They did not engage with the consumer resources signposted and displayed nearby on the wall.
The in-person and video methods yielded similar results across most observations. Some differences between sites in video observation results were identified: (1) lower numbers of consumers were in the waiting area at any one time, (2) the percentage of time the waiting area was empty was higher, (3) the total duration of “other resource” access was lower, and (4) the percentage of time that other resources were accessed by consumers was lower. These differences can likely be explained by the positioning of the video camera at Site 2. At Site 2, the video footage focused on the corridor from the waiting area to the therapy area due to privacy concerns. Small numbers of consumers passed through the corridor at any one time. Majority of “health resources” were located in this corridor at Site 2; however, there were limited other resources (TV and magazines) located there.
Health supports
The types of health supports observed in the waiting area across observations at Sites 1 and 2 included exchange of health information, knowledge, advice, or experiences. Health support was observed between consumer–clinician, consumer–consumer, and consumer–administrative staff. Observed health supports in the waiting area were infrequent, typically involved only one to two consumers and were brief in duration (1–5 minutes). The most common health support in the waiting area at both sites occurred between consumers and clinicians. Health support between clinicians and consumers included the discussion of health information, health appointment plans, and progress with therapy. Health support between consumers involved the exchange of health experiences, knowledge of services, and suggestions for useful equipment.
Other resource use and other activities (not health related)
Other resources were defined as written texts or audiovisual displays that did not contain health information. This included resources such as magazines and TV shows on free-to-air channels. These other resources and activities were observed to determine what else was occurring and therefore better describe the environment and activities in the hospital outpatient waiting areas. More consumers accessed other resources than health resources during the observations; however, the number of other resources accessed at any one time remained low (Table 3). The TV was the other resource accessed for the longest period, with one consumer engaging with the TV continuously for 24 minutes. Watching the TV for this long was not common. The TV was viewed at Site 1 for a median of 2 minutes (interquartile range [IQR]: 1.25–5) and a median of 3 minutes (IQR: 2–5 minutes) at Site 2. Lifestyle and entertainment magazines were engaged with less frequently than the TV but for a longer duration on average. At Site 1, magazines were accessed for a median of 6 minutes (IQR: 3-8.5 minutes) and at Site 2 for a median of 3 minutes (IQR: 3–3 minutes).
Other activities were defined as conversations, reading, leisure, and use of technology that was not related to health or service access. The other activities observed at Sites 1 and 2 were similar and included making a phone call, looking at personal smart phone, reading a book, engaging in general conversation (not about health), looking at/typing on laptop, reading appointment documents/booking form, reading own A4 document, and reading a newspaper. The number of consumers engaged in other activities in the waiting area at any one time was low—usually one to two people at a time only. The most frequently observed other activity was consumers looking at their personal smart phone. This indicates that many consumers have access to a smart phone and use it while waiting for appointments.
Discussion
Health literacy responsive health services can improve health literacy and health outcomes. This study is the first to consider the health literacy responsiveness of hospital outpatient rehabilitation waiting areas. We found that a range of health information, resources, and supports are available, but these are rarely accessed by consumers. Approximately half of the available health information and resources are designed to build consumer health literacy, and the remaining resources are directed at staff. Of those available for consumers, only a limited selection was accessed by consumers, and when this occurred, it was for only a brief duration of time. Interestingly, we also found that consumers occasionally engaged with staff resources instead of consumer resources, and although not the direct focus of the study, no staff were seen to engage with resources (either consumer or staff ones) in the waiting area at any time during the 12 hours of observation.
Making health information and resources available does not necessarily mean they are accessible to consumers. Further to this, even if accessible to consumers, health information and resources may not be understood or acted on. An integrative review of general practice waiting areas found that health promotion materials positively influenced knowledge, intentions, health service use, and behaviors of general practice patients (Cass et al., 2016). Similarly, a recent case study showed that consumers do engage with health information in general practice waiting areas (Williams et al., 2019). Our study found that hospital outpatient rehabilitation waiting areas may be set up to share health information and resources, but it is questionable whether the current approach is effective: Few of the available health resources were accessed by waiting consumers. There are several potential reasons that may explain this finding: the short duration of waiting time, poor-quality resources, insufficient quantity or range of resources, infrequent updating of health information, or familiarity with resources from previous visits to the waiting area. The exact reasons for this in hospital settings need to be explored. Drawing from the research in general practice settings, a range of potential barriers have been identified. An observational study conducted in 2017 found that many of the health information topics and resource types available in waiting areas were not accessible due to: poor quality, poor presentation, limited readability, out-of-date content, and limited inclusivity (i.e. no languages other than English represented; Maskell et al., 2018). Similarly, Protheroe et al. (2015) assessed the readability and content of written materials in waiting areas and found only 24% met the recommended reading-level criteria based on the average literacy level of adults. Although available, it seems health information and resources may not be accessible or comprehensible or applicable to many consumers in this setting. To satisfy their intended role in building health literacy, health service designers, managers, and clinicians need to consider all these factors when creating and sharing health information and resources in waiting areas.
Preparing and displaying health information and resources requires both a financial and time investment by health services which may be wasted if these are not accessed by consumers. Our study indicated that this issue may be relevant in hospital outpatient rehabilitation waiting areas. Although well intended, displays of health information and resources selected by staff may not be accessed by, engaging for, or useful to consumers. This aligns with moderate-quality evidence reported in a Cochrane Review that consumer involvement in the development of consumer education material creates more “relevant, readable and understandable material” (Nilsen et al., 2006). Consumer involvement is accepted as an important aspect of health service research and design but remains lacking in practice (Saunders & Girgis, 2010). This also reflects the advocacy by Pleasant et al. (2015) for a “paradigm shift” from simply providing “plain language” written resources toward considering and evaluating the actual use and effects of health information and resources on health and well-being outcomes. This study did not analyze whether plain language was used in the available information and resources, but future research should consider this. Based on the literature, consumer involvement appears essential to direct future reinvestment in accessible, responsive, and therefore cost-effective health information and resources for hospital clinical and service areas including waiting areas.
Learning experiences may be generated by consumers themselves in the waiting area. Consumers were observed engaging in supportive conservations and exchanging health information with each other in the waiting area. Given that social support between consumers can improve health literacy (Lee et al., 2004), future studies should investigate this relationship in waiting area settings. Similarly, design and environment attributes that promote social interactions and support between consumers should be explored.
Technology could be used to design effective and engaging learning opportunities in waiting areas. In our study, the other resource engaged with most often and for the longest duration of time at both sites was the television. The televisions did not display health information as they were tuned to free-to-air stations. This finding may suggest that consumers prefer to watch entertaining and non-health-related shows to pass the time while waiting. Alternatively, it may suggest that audiovisual displays are more engaging and therefore an effective mode of sharing information with consumers. Our observations also demonstrated that many consumers had access to their own smart phone device and used their phone while waiting for their appointment. This finding suggests that sharing or advertising online and smartphone-capable health information and resources in waiting areas may be very accessible to a high number of consumers.
Health information and resources should be carefully selected to optimize effectiveness and inclusiveness. An unexpected finding of our study was that a high number of staff-focused resources were displayed in hospital outpatient rehabilitation waiting areas. Displaying complex information useful only to staff in the waiting area may confuse or detract from the available information for consumers. It is not clear why staff-focused information is located here or indeed whether staff are aware of or engage with this information, and this warrants further investigation. We also found there were limited resources in languages other than English despite both hospitals servicing diverse communities. It is concerning that culturally and linguistically diverse consumers may be excluded from accessing health information as this may contribute to known health disparities and inequity (Chand, 2012; Sustainable Health Review, 2017).
Traditional educational interventions in waiting areas are largely passive in design (Cass et al., 2016); however, the literature suggests this should be challenged. Active learner participation is a key component of most adult learning theories, yet previous studies have used passive educational interventions in waiting areas (Freda et al., 1994). Likewise, most of the available health information and resources at our hospital sites were passive with the one exception of the aforementioned consumer health support and information sharing. Passive waiting environments (containing passive educational interventions) may have other unintended, detrimental consequences for consumers which reinforce the outdated biomedical model of healthcare delivery. For example, a waiting area environment which positions the consumer as a passive recipient of health information may impact on the consumer’s perception of the health service, their readiness to engage in their imminent appointment, and their perceived “role” as “consumer.” Protheroe et al. (2015) raised similar concerns about the influence of consumer information in general practice settings. Encouragingly, one interactive learning intervention was successfully trialed in a waiting area (Leong & Horn, 2014). Therefore, if the purpose of educational interventions in waiting areas is to promote learning and develop health literacy, evidence suggests that traditional passive approaches need to be challenged and replaced with active educational interventions.
There are some limitations to this study. This is a cross-sectional “snapshot” only of the waiting areas. The time and number of observations were not powered to detect differences between groups as our intention was to observe and describe a range of busy and quiet times in the waiting areas at both sites using predetermined purposive sampling criteria. An outpatient rehabilitation setting may not be generalized to other outpatient settings, given the potential differences in consumer presentations (i.e. mobility impacting on access to resources) and features of the admission (i.e. frequency of appointments and duration of admission resulting in increased exposure to available resources). The video observations conducted at Site 2 were focused on the corridor only as previously described. Therefore, these three observation periods at Site 2 may have missed some use of resources in the main waiting area. A further limitation of the video observations was the poor quality of the recorded audio. As such, it could not be discerned if some of the consumer–consumer and consumer–clinician interactions related to health. When the topic could not be discerned, interactions were recorded as “topic unknown” and reported under “other activities.” As such, some health information exchanges may have been missed. Finally, during the observations, it was not recorded whether consumers were attending their initial or a review appointment. Therefore, it was not known whether returning consumers were familiar with the waiting area and had accessed the resources on previous visits. Given available health information and resources were updated infrequently at both sites, it is possible that consumers viewed them once and did not bother to review them at subsequent appointments.
A key strength of this study was the multicenter setting that enabled a deeper understanding of health information and resource availability and use across two similar rehabilitation services caring for diverse communities. Conducting the observations at quiet and busy times checked how the busyness of the waiting area impacted on consumer use of tangible health information and resources as well as intangible health and social supports. Conducting both in-person and video observations also allowed the researcher to check their presence in the waiting area was not altering consumer behavior. As mentioned previously, a couple of differences in the video findings are likely explained by the video setup and not due to the influence of social desirability bias. The primary researcher spent considerable time present in the waiting area. This assisted with sensitizing and familiarizing the researcher with the waiting area which has usefully informed a subsequent qualitative research study currently underway.
Conclusions
This study indicates that available health information, resources, and supports are infrequently accessed by consumers and therefore may not be meeting the health literacy needs of consumers. Further research is required to understand how waiting areas should be designed to promote and improve health literacy.
Implications for Practice
A range of health information, resources, and supports have been identified that are available for consumers in hospital outpatient waiting areas to improve health literacy.
Audiovisual displays were more frequently used by consumers than hardcopy items potentially indicating a preference for these mediums which should be explored further.
Overall, available health information, resources, and supports are rarely being accessed by consumers in hospital outpatient waiting areas. Further research should explore opportunities for optimizing the health literacy responsiveness of health service environments.
Multidisciplinary stakeholders including health service managers, clinicians, and designers should collaborate with consumers to understand their health literacy needs because it seems that without consumer input, available health information, resources, and supports may be not be accessible to or used by consumers. Following this, the impact of the health information, resources, and supports on health literacy, behaviors, and outcomes should be evaluated.
Given the current global pandemic, a shift away from shared physical resources may be required to address infection prevention. Perhaps this presents an opportunity for health services to share digitalized health information and resources that are accessible via personal smart devices. Although this study focuses on waiting areas, potentially other environments within health services (i.e. clinical areas) could also offer opportunities for sharing health information, resources, and supports with consumers.
Supplemental Material
Supplemental Material, sj-pdf-1-her-10.1177_1937586720954541 - Health Literacy in Hospital Outpatient Waiting Areas: An Observational Study of What Is Available to and Accessed by Consumers
Supplemental Material, sj-pdf-1-her-10.1177_1937586720954541 for Health Literacy in Hospital Outpatient Waiting Areas: An Observational Study of What Is Available to and Accessed by Consumers by Cassie E. McDonald, Louisa J. Remedios, Catherine M. Said and Catherine L. Granger in HERD: Health Environments Research & Design Journal
Footnotes
Acknowledgments
The authors wish to acknowledge the support of the following managers: Alana Jacob, Sandra Savy, Susan Cronin, Michelle Mews, and Gillian Dickman. They also wish to extend their acknowledgment and thanks to the following departments: Department of Allied Health—Physiotherapy and the Community Therapy Service at The Royal Melbourne Hospital; Western Health Department of Physiotherapy; and the Community Based Rehabilitation service at Sunshine Hospital. Finally, thanks to Alice Schenk-Green for creating the figures included in the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. Ms. McDonald is supported by an Australian Commonwealth Government Research Training Program Scholarship.
Supplemental Material
The supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.