
Abstract
Objective:
With the reactivating hospital concept, it is our goal to provide a more active stay in a hospital for patients by diverting the focus away from “lying in bed.” We want to achieve this by changing the spatial environment of the nursing ward. These new spatial interventions are aimed toward helping the patients to be healthier during and after their admission to the hospital.
Background:
When it comes to hospitals, we tend to have a mindset that is basically focused on disease, not on health. The whole hospital is geared toward illness, waiting, lying in bed: a passive attitude of the patient in this medical stronghold. Staying in a hospital has a negative influence on the body, especially for vulnerable patients. However, when patients remain active during their hospital stay, fewer negative effects occur. The risk of complications reduces, and patients recover better and faster. Research shows that only 15% of patients actually need to stay in bed. In order to enable hospitals and their patients to benefit from these insights, Gortemaker Algra Feenstra Architects introduces the reactivating hospital concept: a set of scientifically based practical interventions intended for a change in organization and spatial design of hospitals.
Design hypothesis:
How can spatial interventions to a geriatric department contribute positively to activating elderly patients during their stay in the hospital?
Research question:
What impact does providing areas for activation away from a patient’s bed have on the quality of the patient’s experience?
Method:
The reactivating hospital concept no longer revolves around “lying in bed,” but around the notion of “making patients stronger.” We are introducing a new rhythm of 8 hr of activation, 8 hr of relaxation, and 8 hr of sleep. This requires a different mindset of patients and personnel and involves a totally different interpretation of space. To tackle the problem at its roots, the bed will be solely reserved for sleeping and all other activities will take place elsewhere in the nursing ward. To encourage patients to remain active, we soften the transition from bed to room, from room to corridor, from corridor to department, and from department to the rest of the hospital. These subtle transitions invite patients to move around, thus remaining active. To test these methods, we use qualitative and quantitative research methods such as observation, conversations with focus groups, and questionnaires during the research.
Results:
Reactivating hospital concept is a concept and a design research in progress in collaboration with the existing Diakonessenhuis hospital and the Netherlands Organisation for Applied Scientific Research (TNO). In this setting, there are different scales of innovation. In the first phase, we have been working on a completely new bed department with a new typology. In the second phase, we are currently testing significant changes in a room, corridor, and department level, within the context of the existing department, and we are measuring and monitoring the results. The first research results show a positive effect on the state of mind of patients as well as the nurses. At this moment, we are researching the positive effect on the exercise and health of patients, and we are expecting the first concrete results to come in at the end of the year.
Conclusion:
The initial feedback we have received from the Diakonessenhuis hospital has been positive. Furthermore, we have noticed that the reactivating hospital concept is receiving more and more support. Lying in bed has a negative effect on patients, and a lot of hospitals are aware of this and are therefore looking for alternatives.
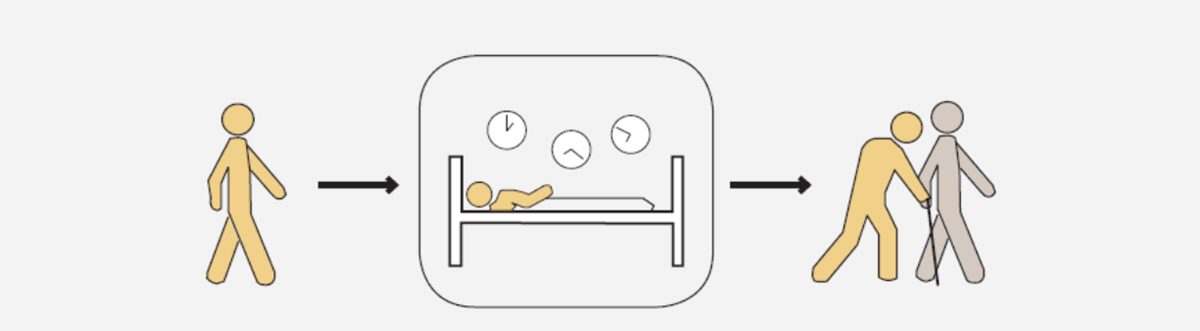
In our mindset, hospitals are very much focused on sickness, waiting, and beds, which results in a passive attitude from the visitor in this medical bastion. If we want to indicate the size of a hospital, we count the number of beds! You are lying in hospital! Why are we treating our patients so passively? There is a clear need for activation outside of the patient room in order to encourage patients to “get up and out of bed.” Especially for vulnerable patients, spending time in hospital has a strong negative influence on the human body and surgery worsens this influence (Figure 1). The overall physical state of patients worsens and their well-being and autonomy decreases (Gill et al., 2004). However, when patients stay active during their stay in the hospital, on the other hand, fewer negative effects occur (Dronkers et al., 2015). The risk of complications reduces, and patients recover better and more quickly (Arem et al., 2015). Physiotherapist J. Elings (2016) of Diakonessenhuis in Utrecht says that: “In our experience only 15% of patients should actually stay in bed during their hospitalization.” If research shows that hospitalization-associated disability occurs in approximately one third of patients older than 70 years, it’s of the utmost importance that we change the mentality of staying in bed too long. The average length of stay in the hospital is 5.9 days in the Netherlands (CBS StatLine, 2019). The average length of stay in the geriatric ward is 14 days (Leiden University Medical Center [LUMC], 2008). We know from these studies that inactivity has an enormous effect on the physical state of patients (Figure 2 and 3). As a consequence of their impairment in daily functioning, many of the participants became increasingly dependent and in need of help (Van Seben et al., 2019).
Source: Covinsky et al. (2011).
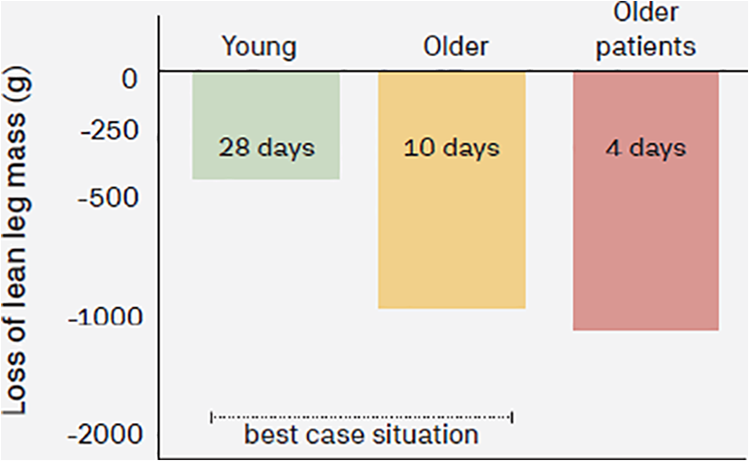
Source: Paddon-Jones et al. (2004), English et al. (2014), and Kortebein et al. (2007).

Source: Hulzebos et al. (2012).
For patients, hospitals, and other care institutions to gain from these insights, Gortemaker Algra Feenstra Architects introduces the reactivating hospital concept: A set of practical interventions meant to change the spatial organization in care institutions, which can initiate and support changing views of care processes toward reactivating patients during their stay in a hospital. As Marion Konijnenbelt (nurse department geriatric medicine) said: “With the new spatial organization and interventions, we as staff don’t have to organize the environment to be able to introduce movement and exercise for patients. This also motivates staff to activate patients.”
Background
Since the mid-80s of the last century, almost all facets of hospital organization have changed radically and fundamentally. This trend is not only influenced by technological and organizational breakthroughs but also by the changing characteristics of the patient population: Patients are getting older and more often suffer from chronic disorders and comorbidity. More and more, hospital care is turning into specialized care for patients who keep getting older. Along the way, this leads to new views about what health is and how to promote it.
Over time, more and more has become possible in and around beds in the nursing wards of the hospital, just to make sure that patients are not missing anything in terms of comfort while they stay in bed. In Dutch hospitals, everything is organized in and around the patient’s bed: a red button in the bed to call for nursing, the doctor comes to the bed to discuss the patient’s progress, the television is hanging over the bed, and family visits are facilitated around the bed. The patient rooms are located on one long corridor, a corridor that is mainly intended for nursing and is not designed to be patient friendly. The patients adopt a passive attitude and they are not expected to do anything else. In current developments, you see that hotel-like care is the trend in hospitals, but this is in fact a misguided development. By orchestrating everything around the beds and bringing everything to the patients, they are even less likely to get up out of their beds.
It would be very beneficial for hospitals if they would manage to shift their focus from the current process in nursing ward practices toward keeping the patients active during their stay in the hospital. Activity is important, but a meaningful activity that contributes to recuperation and rehabilitation is what the majority of clinicians strive for. For hospitals, shorter hospitalization and a lower chance of complications and rehospitalization not only mean an increased quality of healthcare but also increased efficiency. This is what many Dutch hospitals are striving for.
The reactivating hospital concept is based on a completely new daily rhythm and organization of the design of all nursing wards in hospitals. The reactivating hospital concept is not just about the hospital beds but also about the idea of “making patients stronger.” The reactivating hospital rhythm consists of 8 hr of activation, 8 hr of relaxation, and 8 hr of sleep (Figure 4). This requires a different mindset of patients and personnel and involves a totally different interpretation of space. To tackle the problem at its roots, the bed will be solely reserved for sleeping and all other activities will take place elsewhere in the nursing ward. This demands a completely different mindset from both the patients and the staff and an entirely different interpretation of the daily rhythm during hospitalization leading to a totally different interpretation of space. We have to change the care environment of patients. Beds are exclusively reserved for sleeping, while all other activities take place somewhere else in the department (Figure 5). To help encourage patients to stay active, we want to ease the transition from bed to room, room to corridor, corridor to department, and department to the rest of the hospital. These subtle transitions invite patients to stay active and keep moving. This is important for any type of patient who is physically able to move: both for long and short hospital stays.

The reactivating hospital rhythm.

Reactivating hospital provides different places to rest and activate in the nursing ward.
Research at the Hospital Diakonessenhuis
Aside from being a concept, the reactivating hospital is also a design research by Gortemaker Algra Feenstra Architects. In collaboration with Diakonessenhuis in the city of Zeist in the Netherlands and TNO, we have executed our first pilot project. The study took place in the geriatric ward, where people spend an average of 14 days.
With this research, we wanted to get an idea of the acceptance, usefulness, appreciation, and effectiveness of the interventions. We also wanted to see which environmental factors have an influence and how Gortemaker Algra Feenstra (G.A.F) can take this into account in the further development of this concept.
This first image is important as a guiding framework for further concept development. The study also wanted to test the extent to which the research methods used are suitable for arriving at scientific evidence for effectiveness in the long term, once implementation has taken place in more places and on a larger scale. At the Diakonessenhuis hospital, we have tested significant spatial interventions on the design of the room, corridor, and department within the context of the existing department.
With our research at the Diakonessenhuis, we set the following goals: creating a more positive attitude for patients toward exercising during their stay in the hospital, offering more choice and variation in the activities on the nursing ward, having patients out of bed longer and more often, and having a more positive experience during hospitalization.
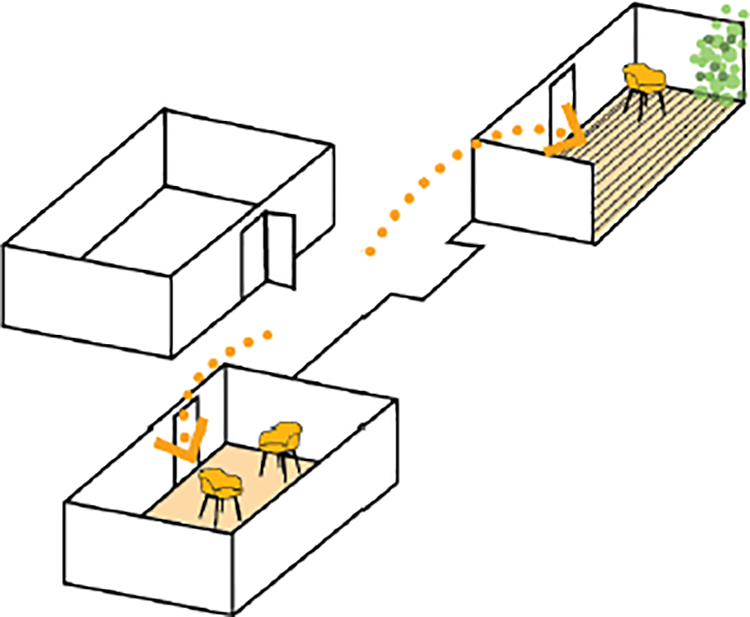
We have executed and tested several interventions last year. Our interventions were based on the theory of planned behavior (TPB), which explored how planned interventions can increase how much people move (Darker et al., 2010). We used this concept to place interventions of our own. At room level, we turned the room into a studio with a “living room” area (Figure 6). At corridor level, we implemented niches in the corridor to activate patients and every niche has its own theme: see, hear, write, and exercise. At department level, we provided a meeting room, a relaxation room, and a garden room in the department. The interventions are illustrated in Figure 7.

Interventions at Diakonessenhuis give patients a reason to spend time out of bed.

Interventions at Diakonessenhuis.
From Bed to Room
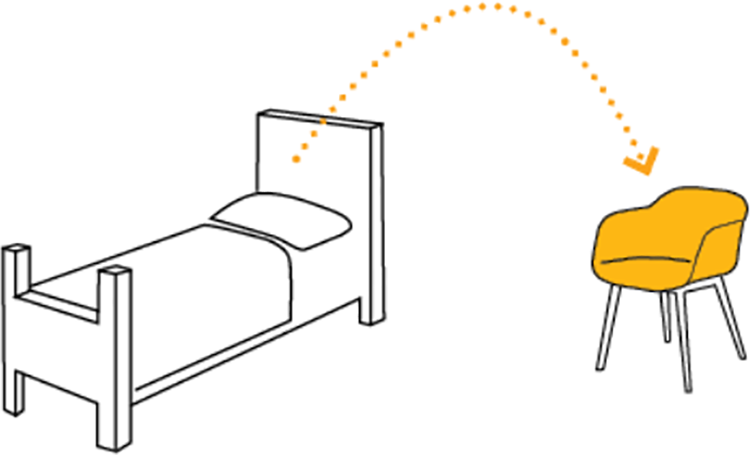
The first design intervention is in the patient room. Patients’ rooms are laid out in a way that the patients do not need to leave their beds. By providing the patient’s rooms with the initial motivation to leave their beds, we are expecting patients to be more active during their stay in the hospital (Figure 8).
From bed to room.
By adding a living room to the patients’ rooms, we want to provide patients with the initial incentive to spend time away from their beds (Figure 9). In this room, you will find a “dinner” table with chairs, a comfortable chair, and the TV will be located here as well, just like in a real living room. By decorating the room with homely accessories and changing the appearance of the floor and walls, we are trying to strengthen that home-like feeling.

From bed to room level.
Design Hypothesis 1
By creating an inviting area to hang out, visible from the bed, we are expecting the patients to spend less time in their beds. This is achieved and encouraged in many hospitals all over the world.
From Room to Corridor
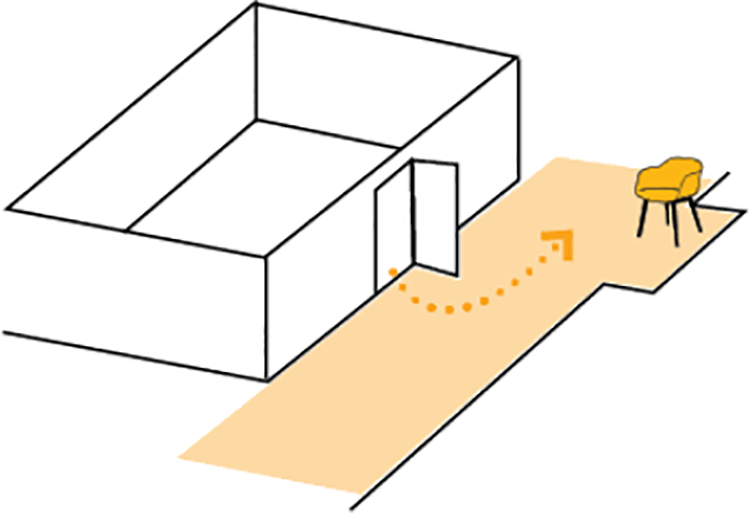
The corridors in a nursing ward are often very anonymous areas with not much place for activities by patients. This can often even create a barrier for older patients. Reducing this barrier by making the corridor a more accessible place for patients, we expect them to leave their rooms more often (Figure 10).
Room to corridor.
In the corridor of the nursing ward at the Diakonessenhuis, you will find a couple of niches. After discussing with the project team, we have chosen to use these niches to help activate the patients. Every niche will have its own theme: see, hear, write, and exercise.
Design Hypothesis 2
We are expecting to reduce the barrier to go into the corridors for patients, meaning they will spend more time outside of their rooms.
Design Hypothesis 3
The niches can help with the exercise program and contribute to the social interaction between patients and the nursing staff as well as patients and visitors (Figure 11 and 14).

Photo exercise niche corridor.
From Corridor to Department
If we want patients to spend more time out of their beds, we need to provide more options for activities and relaxation to the department (Figure 12). Currently, patients can already participate in joint activities in the living room at the department. Aside from offering activities, it is important for the target group to have an alternative for relaxation as well (Figure 13). Next to the shared living room, there is a room that is currently used as a meeting room for the nursing staff. For our research, we want to start using this room as a relaxation room. This room also connects to the outside area of the department, by using this room for relaxation; thus, opening it up to patients and visitors, these three common areas together can contribute to broadening the range of activities at the department, which in turn contributes to the activation of patients. In the pilot, we made use of the nursing room because it was being used for storage. It goes without saying that in future trials the interventions would not come at the expense of rooms that are being used for core functions such as nursing. This will have to be invested in the various departments and tailor-made.
From corridor to department.

Photo garden room.
Design Hypothesis 4
We are expecting to be able to activate patients more by offering a wide range of common areas. By realizing a relaxation room outside the patients’ rooms, we expect that the patients spend less time in their rooms.

Photo music niche corridor.
Research Questions
The impact of the four design hypotheses on patients and staff is further examined in one main and five subresearch questions that are the basis for evaluation of the interventions:
What is the impact of the applied changes to the spatial environment of the nursing ward on the activation of patients in the hospital? Do the interventions help patients to feel safer and more confident when getting up out of bed? Do patients feel like there are more choice and variety in the activities that are being offered? Do patients actually spend more time out of their beds more often? Do the interventions contribute to patients experiencing a more positive stay in the hospital? What are the effects for staff members?
Research Methods
Hinkema, M. J. (2018) of TNO was responsible for measuring the interventions of the department at Diakonessenhuis Zeist on behalf of Gortemaker Algra Feenstra architects. The research had a broad question and an exploratory character, which is well suited for a primarily qualitative approach, aimed at roughly mapping the full range of the subject. This qualitative exploration offers a framework in which quantitative research methods can be selected, contextualized, and determined during future research and implementations. In an early stage, we have been able to determine that we could not expect to achieve either statistical significance or that identifiable trends would pop up with the limited size of the experiment in Zeist when implementing quantitative research. Still, we have done some quantitative research on the side, next to the qualitative methods. This is because, on the one hand, we were curious whether we could derive anything in a quantitative sense, and, more importantly, on the other hand, to test the usability of the instruments that were implemented specifically for this research. The latter creates a foundation for the uniformity and comparability of follow-up research and validation.
The measuring research methods we used are focus groups (qualitative), observations of activities and interactions in the corridor and activity room(s) (qualitative), questionnaires based on the TPB (qualitative; Ajzen, 1991; Armitage & Conner, 2001; Godin & Kok, 1996), and structured observations of individual patients (quantitative). The TPB is a study whereby participants wearing a pedometer were measured to have an increased amount of walking, on average an extra 10 min per day, when they were in an environment with design interventions. These interventions became a determinant for walking, in other words, the interventions motivated the participants to move more (Darker et al., 2010).
Focus Group Discussions With Employees (Qualitative)
Two focus group discussions (of approximately seven of the eight persons) were held with employees involved in the department. The aim was for a multidisciplinary presence in both interviews: nurses, geriatricians, occupational therapists, physiotherapists, and activity guidance.
The first meeting took place shortly before the interventions were carried out. In this conversation, they discussed their views on the following: the attitudes and abilities of patients, the degree of influence that professionals have, the amount of time the professional has in the daily range of tasks to activate patients, the degree to which the ward offers a protective and attractive environment in which to be active, and the degree to which patients are bored in the ward. The outcomes of the focus interview served to build up a good picture of the starting situation in the department, to map out expectations and points of concern, and to identify points for attention during the implementation of the research.
The second interview took place at the end of the research period and was more evaluative. In this conversation, the following questions were raised: How do we test the expectations of the effect of the interventions on patients? How can we test the expectations of the effect of the interventions on employees? What are the experiences and thoughts about the use and usefulness of each of the interventions? What are the expectations and ambitions for the development of the concept? Both interviews took about 2.5 hr. The findings of both interviews are integrated with the findings of the other qualitative research activities discussed later.
Group Discussions With Patients (Qualitative)
In total, two group discussions were conducted with patients. Both took place after the interventions were performed, in September and October 2018, respectively. Approximately five patients were present at each meeting. The purpose of the talks was 2-fold: To gain insight into the extent to which the patients were familiar with and made use of the interventions. To gain more knowledge of the characteristics, limitations, motives, health problems, and questions of meaning that play a role in the patients who are admitted to the clinical geriatrics department.
The interview was provided by the activity coordinators and hostess who worked in the department.
Observations of Activities and Interactions in the Corridor and Activity Room(s) (Qualitative)
Before and after the interventions were carried out, qualitative observations were made in the corridor and the activity room(s) of the department. Beforehand, observations were made twice for 4 hr (one morning and one afternoon). On four occasions, 4 hr was observed after the interventions were performed (two mornings and two afternoons). According to a fixed pattern, the observation was always 40 min in the living room and 2 × 10 min in the two corridor sections.
The observations looked at the degree and nature of activities that took place in this environment and the functional and social interactions that took place. Among other things, the degree of independence of movement and functioning of patients and the ease of use and quality of the facilities were examined.
The observations, in which a researcher was present in the ward for a longer period of time, were also used to collect informal impressions of how the interventions were experienced and appreciated by staff and patients. The observations were made in a free format. However, a framework has been developed of possible observable behaviors and interactions as a reference.
Questionnaires Based on the TPB (Quantitative and Qualitative)
The Holland Health House concept is not purely about movement in itself as an outcome measure but about changes in mindset, motivation, and well-being of patients and employees. It is therefore important to gain insight into the thoughts, perceived norms, and factors that promote or hinder active or nonactive behavior. The TPB is a suitable method to investigate this. Instruments based on this theory inventory the intrinsic views and beliefs of patients, the external (social) norms they experience, and the degree to which they experience control over the behavior in question. A questionnaire was developed for the study, which questions patients via 21 items (statements). Each statement is answered on a scale from 1 (totally disagree) to 7 (totally agree). The questions are about equally positive and negative (11 positive, 10 negative).
The questionnaire included the following questions: Patients like me do their best to stay as fit as possible, my family thinks it is important for me to exercise to be able to go home safely, I can move independently through the patient room, I often get lost in the hospital department, I like it when my stay in the hospital is as much as possible “just like at home.” (Figure 15 depicts the summary graph of “most confirmed beliefs, before and after” and main differences.)
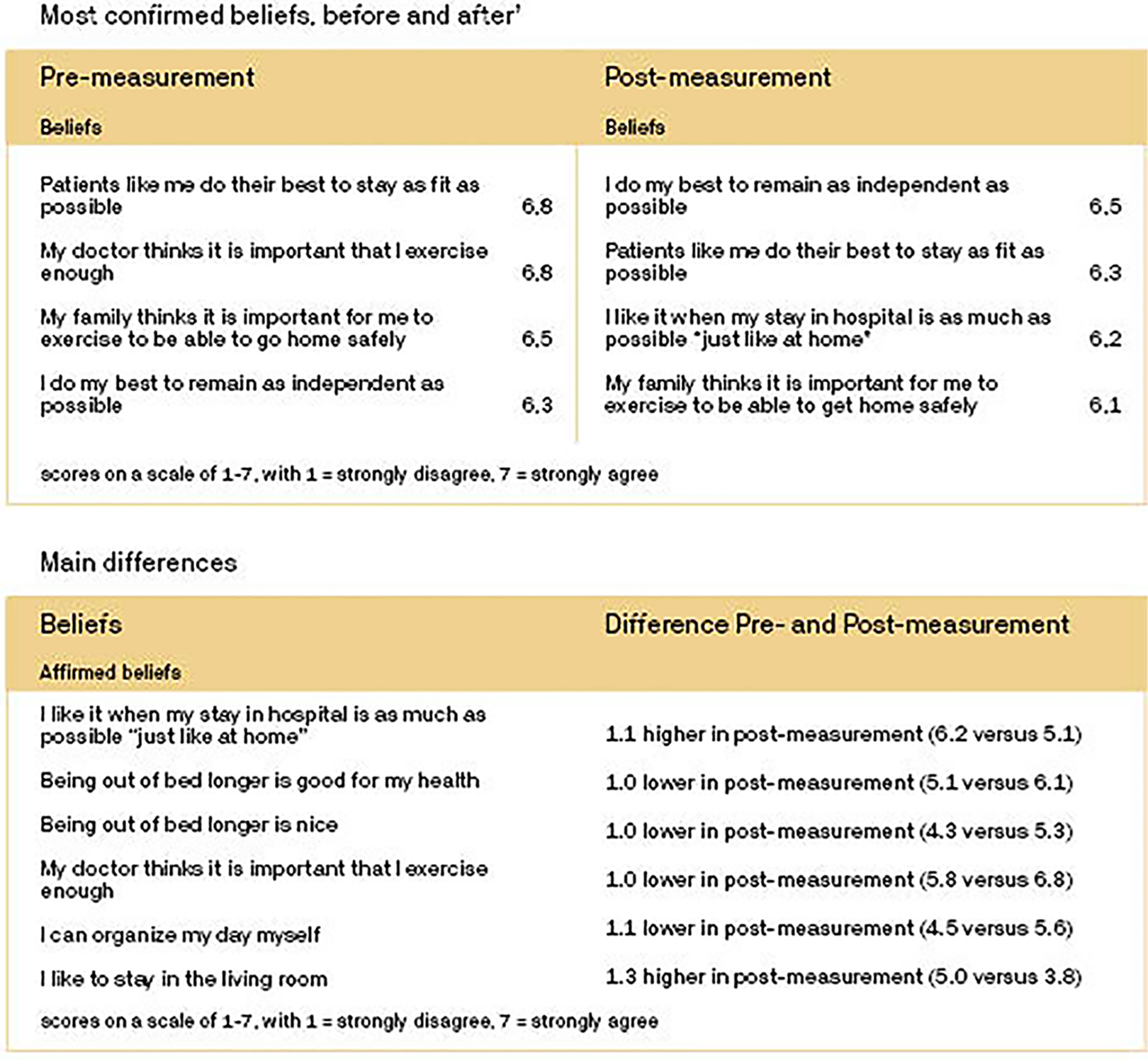
Summary graph of most confirmed beliefs, before and after and main differences.
In the second part of the questionnaire, the frequency of patients’ participation in activities during their hospital stay was recorded. These activities included relaxing/resting, eating, receiving visitors, planned activities, and physiotherapy/exercising. The environment in which the activity occurred was also recorded. These included the bed, a room, living room, and hallway. Finally, whether the activity occurred as a matter of choice (intended behavior) was documented.
The questionnaires were administered by nurses and activity coordinators from the department. Eight questionnaires were administered prior to the interventions and 10 questionnaires were administered after the interventions were performed.
The purpose of using the questionnaires was 3-fold: testing the usefulness and usability of the instrument for further research and validation, contributing insight into the motives, perceived norms, and perceived obstacles of patients, and the possible presence of differences in views and behavior between the “pre- and postgroups.”
Structured Observations of Individual Patients (Quantitative)
As part of the study, structured observational research was conducted in individual patients. For this, a method has been applied that has previously been used for research at the University Medical Center (UMC) Utrecht. The method is referred to as “behavioral mapping.” In this method, a patient is observed for 1 min every 10 min for a predetermined period of time (a number of hours, a half-day, or a day). With each observation, a fixed list of codes is used to note where the patient is, with whom they are interacting, the position of the patient, and the activity. This way of observing provides a detailed picture of the nature and degree of activity of patients. For application in the Diakonessenhuis, the protocol developed by UMC Utrecht has been slightly modified to better reflect the specific situation in the department in Zeist.
Behavioral mapping observations were performed both before and after the interventions. Before the interventions, a total of eight patients were observed for half a day (four in the morning, four in the afternoon). After the implementation of the interventions, a total of 15 patients were observed for half a day (7 a.m.–8 p.m.). About half of the patients observed after the interventions were observed in one of the patient rooms that were adapted for the experiment. The observations beforehand were carried out by nursing interns and the observations afterward by interns from the physiotherapy department.
When planning behavioral mapping observations, it was assumed that some of the activities would be carried out by students of the Hogeschool Utrecht. Unlike other years, there appeared to be no room for a practical study project at the Diakonessenhuis among bachelor students. Therefore, the behavioral mapping observations had to be done on (care) substantive grounds by experienced nurses and activity guidance. Due to the high pressure in the department, it turned out to be very difficult to plan this in addition to their regular work, partly due to pressure and staff shortages in the department. As a result, the number of observations was lower than planned and were scheduled at different times.
Preliminary Results
The question whether the interventions help patients think more positively about getting out of bed and being active can be answered with a careful “yes.” The staff members, for example, are experiencing that since these interventions were implemented, patients are more easily motivated to get up and do something. Additionally, reports and observations are coming in that patients are enjoying the usage of the interventions. Improving and enlarging the areas for group activities and shared meals as a prerequisite appear to contribute in this area. Especially these activities seem to stick out in dialogues and observations (as in the focus group discussions and observation of individual patients) as structural elements to which patients look forward to and that motivate them to become active.
Do the Interventions Help Patients to Feel Safer and More Confident When Getting Up Out of Bed?
That question can be answered with a “yes.” The niches in the corridor give the patients the option of taking breaks along the way to rest (Figures 15.1 and 16). This helps to reduce the barrier between staying in bed and doing walking exercises or going from their patient’s room to an activity room. Even for patients with the urge to walk, the niches accomplish that same purpose. Objectively, widening the living room and adding flexibility ensure that patients can move through the area more freely and easily at the least, and from observations, it seems that this is the patients’ experience as well (Figure 17). On top of that says Marion Konijnenbelt (nurse department geriatric medicine): the increased amount of possibilities in the living room and the lounge to regulate the number of stimuli make it so that especially those patients that are vulnerable in this regard feel more safe and confident, even when they are out of bed. Photo writing niche corridor. From room to corridor level. From corridor to department level.


Do Patients Feel Like There Are More Choice and Variety in the Activities That Are Being Offered?
It is not entirely clear whether patients are consciously aware of this. In addition, they are lacking the knowledge to compare the current situation with the “before” situation. For follow-up research, it would be interesting to collect data about how patients feel about this situation once they know it better and know how to optimally make use of the interventions.
The research data, so far, show that the interventions help to fill the large gaps in the offered activities in the evenings and the weekends: The lounge is frequently visited and used as a TV room, and the corridor niches are used the most extensively during that time as well. Staff members of the department note that especially during the weekends visitors have more options to give a positive and diverse spin to their visit. In the intervention rooms, various adjustments have been made, such as a separate seat with television and lounge chair, a table with two chairs where you can eat, more homely materials have been used, and a cupboard has been made around the hospital equipment. These interventions offer a wider scale of options to choose from during their stay in their own room, options that are actually taken advantage of in practice.
Do Patients Actually Spend More Time Out of Their Beds More Often?
For the patients staying in the adjusted patients’ room, that is definitely the case. Staff members clearly indicate that patients spend more time in the armchair and seating area than in their beds. Placing the TV in the seating area instead of above the beds was an immediate hit. Utilization of the lounge and the niches in the evenings and the weekends also indicates that patients are found out of their beds more frequently than before.
Although not as frequently, the niches and lounges are also being utilized in the daytime during the week. The qualitative observations give us the impression that the group activities are frequented slightly more than before and that patients stick around in the living room more often afterward. The meals seem to be drawing a bigger attendance as well. Keep in mind though, that the specific mix of people who were hospitalized in this department at this particular time could greatly influence the results. More extensive quantitative follow-up research (behavioral mapping) should be able to offer more insight into this.
There are a few striking differences between the pre- and postobservations. While patients are more often found lying in bed during the premeasurement (+4.1%), this is less the case with the postmeasurement (−14.9%). It is not entirely coincidental that the percentage of seated patients is lower at the pretest in the afternoon (−4.2%) but higher at the posttest (+7.6%). In the premeasurement, the number of patients reading, watching TV, or using a tablet or smartphone in the afternoon is roughly the same as in the morning (−0.8%); in the postmeasurement group, it is clearly higher in the afternoon (+7.9%).
On the other hand, the percentage of patients eating in the afternoon pretest group is clearly higher than patients eating in the morning (+9.2%). In the posttest, the number of patients eating is lower (−4.9%). As mentioned, this is probably due to the earlier start time of the afternoon observations at the premeasurement.
Do the Interventions Contribute to Patients Experiencing a More Positive Stay in the Hospital?
Receiving an explicit answer to that question is very difficult with this patient group because they often deal with complex problems and a multifaceted process of vulnerability, loss of functions, and loss of independence. It is hard to pinpoint how patients are experiencing their stay in the hospital within that reference framework, specifically for the patients themselves. Still, there are indications that the interventions are having a positive effect.
The increased range of possible activities at night and in the weekends ensure that patients are being distracted and are entitled “free” moments. Not only is that enjoyable in itself, but it can also contribute to keeping worrying and gloomy thinking, which are likely to strike during this time, at bay. Staff members have had a positive experience with the “hear” niche so far. Around the record player, spontaneous meetings happen in a positive atmosphere and its reach goes further than just its direct surroundings. Even in the rooms nearby, patients are able to follow what is going on.
The adjusted patients’ rooms seem to be making a significant contribution to the well-being of various types of patients: a living room in which patients can keep actively living “just like at home,” a safe space with tranquility and security to help take those first little steps on the road to reactivation for people.
By the observations, it is noticeable that patients in the posttest find it more important to be able to live like home. It is not clear from the figures whether this stems from goal-oriented ambition or, conversely, from an awareness of the loss of the ability to do so. The fact that people in the posttest think less positively about the usefulness and pleasure of being out of bed longer seems to be consistent with the assumption that the postmeasurement group is more vulnerable across the board.
What Are the Effects for Staff Members?
The effects of the interventions on the staff members are of great importance, as in addition to their role for medical care, they actively stimulate, guide, and channel patients’ behavior. For most patients, taking the initiative is a bridge too far in this case.
As such, it is pleasant to be able to conclude that staff members do indeed feel like they have more tools at their disposal to help patients become more active. The range of options is broad, there is more leeway to work with patients and provide tailored solutions to activate them. It has become easier to encourage patients because there is a reward on the other end, as well as specific incentives—such as the TV—put in place to tempt patients to leave their beds. The staff members, we have spoken to and seen during the research, were already extremely positive about working on activation of the patients’ daily rhythm, even before the interventions. In this regard, the interventions mostly worked as a reinforcement of that approach. We are under the impression that staff members view the interventions as recognition and encouragement for their way of working as well. In certain aspects, the staff members feel more capable of working proactively thanks to the interventions. Physiotherapists are very positive in regard to the exercise niche, activities under supervision profit from the larger more flexible spaces, and the option to regulate stimuli as needed (Figure 18).
Reactivating signing.
The nursing staff notice the differences, especially in the evening and week shifts, moments at which they used to have a difficult time to keep the patients entertained. The extent to which staff members benefit from the interventions and act accordingly differs from person to person. When looking at the influence on professional conduct, the conclusion can be drawn that the effects so far are most noticeable on a personal level. This has nothing to do with a lack of goodwill; instead, it is a result of conditioning by education, professional experience, and the behavioral competencies that an employee can and wants to employ.
The staff members are aware that further steps are necessary to completely integrate activating work into the department processes in order to achieve the maximum benefits from the interventions. This is a relatively long winding process that demands the hospital to commit to a high level and for which the current experiment can function as a catalyst. It is important to note that the closely involved management and staff of the department have made a real effort within their capabilities to include their colleagues in these changes. The conclusions in this case mostly concern the further implementation and development of the concept.
Even before the interventions, the staff members had a positive attitude toward activating through action. Additionally, from our observations and conversations, we have gained the impression of a team of staff members that feels strongly involved in the department and the patients hospitalized there. From the aforementioned effects on staff members, it appears that they felt like they were given more tools by the interventions to concretely channel and utilize that ambition and commitment. It seems logical that this reinforces positive identification with the job. We see the verbal wish and ambition from the staff members to more sharply formulate and more explicitly convey the joint mission and more systematically work on adaptations of work processes and the structure of competencies and capabilities (see below) as a manifestation of this. The interventions have opened a door to further development of the department and the reactivating treatment approach.
Discussion
Out of necessity, the current research has been restricted to a mostly qualitative analysis of the early phase of implementing the interventions as well as trial runs with two tools for a more quantitatively aimed analysis. It would be useful for the analysis of the effects in the long term and for the gradual buildup of evidence if there could be a follow-up research of the quantitative instruments after a certain amount of time. It seems logical to wait with this until at least some practical improvements and some relatively simple communication measures have been implemented.
Points for Improvement and Development
The survey has revealed a number of practical areas for improvement. Some worth mentioning include the day storage for bedside tables, a visual separation between the bed and the sitting area, and signage, signs, and pictograms to increase the findability of niches and activity areas, to clarify the use of the interventions, and to add more mixed furniture to the lounge allowing greater flexibility of use.
In the field of information and communication, it has been found that the effectiveness of the interventions and the reactivating approach can be increased by the use of clear, recruiting means of communication tailored to the target group. This deployment should mainly take place immediately upon arrival, in places where patients, employees, and visitors interact with each other, directly at the activities, and with planned admissions already during the intake.
With regard to process and culture, it has become clear that employees advocate a planned effort with assurance on a high level in the organization in order to unlock the full potential of the reactivating treatment and the reactivating environment. This effort should primarily focus on the systematic analysis and development of change of work processes in the department and an inventory and action plan for the training and competence development of employees. It is clear that this process transcends the strength of a single department and its employees.
Conclusion
In the past 2 years, we have predominantly looked at activating patients during their hospitalization. The effect of the research is that people will also start to ask questions about the future of hospitals, whether hospitals will keep functioning in their current implementation, and how to change people’s mindsets (even when they are not patients) with respect to hospitals. We sometimes like to call it a health institution instead of a hospital. We have noticed that by adjusting the spatial environment, we can initiate change within people’s mindsets, even for nonpatients. We would like to further examine and develop this.
The reactivating hospital is not (just) a product but even more so a transformation in the mindset as well as a process. As a team, we have noticed that, by talking about the reactivating hospital, a dialogue has really started on a societal level within the healthcare industry but even outside of it as well. Naturally, the trend was already going in the direction of exercising more, for instance, in the office industry through a change in mindset: Sitting is the new smoking. Healthcare was still lagging behind, though there was a powerful sentiment coming through from physiotherapists that things needed to change within hospitals and that patients should not be lying in bed all the time. The implementation of this is mostly visible in the geriatric department. This societal dialogue is supported by our research. By utilizing the spatial environment, it suddenly becomes very clear that this is a different kind of hospital, expecting and supporting different behavior from patients, caregivers, and visitors. The research has contributed strongly to the dialogue about what hospitals should look like in the future.
Implications for Practice
Requires cross-sectoral cooperation between the different disciplines of architects, nursing staff, doctors, and facility employees in hospitals.
Introducing small steps: from bed to room, from room to hallway, and from hallway to department. As a result, the interventions that encourage patients to view multiple places are relatively easy to realize.
By offering different places in the department, this provides support to the care process and gives nurses handles to encourage patients to move. This provides relief for the care process.
The visibility of the interventions in the built environment is important to change the mindset of care, visits, and patients: In the hospital, you not only lie in your bed but also keep moving to stimulate your own rehabilitation.
Footnotes
Author’s Note
The reactivating hospital is a design research by Gortemaker Algra Feenstra Architects. In collaboration with Diakonessenhuis in the city of Zeist in the Netherlands and TNO, we have executed our first pilot project. Readers can contact the corresponding author (
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The part of the research was commissioned by RVO (Netherlands Enterprise Agency).