
Abstract
Objectives:
In this work, we aim to have a better understanding of the impact of the architectural ambiance on patient well-being, by exploring patient’s perception of physical ambiantal factors in their rooms.
Background:
Perception of ambiantal factors is beginning to be relatively documented in space psychology, including health. There is no research in this field in Algeria; therefore, we would like to fill this gap and draw attention to the importance of the ambiantal physical factors in our hospitals.
Methods:
We conducted a practical study via a 19-item questionnaire at the neurology hospitalization department of two hospitals. This is complemented by in situ observations and reactivated observations. Descriptive, principal component analysis and statistical tests were applied on the responses.
Results:
Thirteen ambiantal physical items studied were all classified relatively medium with mean scores ranging between −0.55 < mean < 1.34, with SD 0.765, on a scale of −2 to 2. Patients therefore consider the room ambiance medium. Patients’ satisfaction and well-being results meet with findings about ambiantal physical factors. Neurological diseases affect patient cognition, which increase the importance of space-sensitive perception. The bad general condition of the building is negatively pointed in all testimonies of the questioned, especially spatial organization with multiple occupation room.
Conclusion:
The results indicate that reflection should be oriented on the design of single or double rooms, taking into account the emotional (sensitive) state of the patient, by integrating ambiantal physical factors (natural lighting variable, sound variable, thermal variable, olfactory variable), to contribute significantly to their well-being.
Our work focuses on the impact of the perception of physical ambiantal factors that combine and intersect with the field of social psychology and the psychology of space on the patient satisfaction and well-being in hospitals. Living space is a complex environment felt by our actions and movements. Because space is “sensitive” (Augoyard, 1995). To carry out our study, we therefore fragmented the perception of the spatial ambiance on each one of the senses to better understand the effect of the room design on the patients (Texier, 2007). Jean-Paul Thibault defines the ambiance as the continuous basis of the sensitive world. Crossing theoretical approach and methodological proposal, literary sources, and field surveys, the concept of ambiance is explored from a plurality of themes (Thibault, 2016). The ambient environment is then differentiated into many sensitive ambiances that specify the lived situations, whereas the characteristics of functional spaces do not reach us directly. They are modified by individuals’ motivations, which vary according to the induced activities. These activities are free or imposed by what holds individual’s attention. They are also transformed by cultural or personal specificities (Hall, 1971). Research has clearly established that the indoor environmental quality (IEQ) problems (thermal, acoustical, visual, and air quality) of a building have a direct effect on comfort, health, safety, and productivity of occupant (De Giuli et al., 2013; Pontip & Kandar, 2015).
Method
Study Participants
This work is part of the problematic of the architectural ambiance theory and proposes, through the approach of a space dedicated to the neuronal pathology, to understand the effect of the spatial ambiance of the structures specialized in the reception of adults with neurological disorders on their well-being. We choose neurology department since among the six major categories of pathologies supported by neurology, brain pathologies, pathologies of the meninges, multiple sclerosis, and stroke affect the control of our movements, emotions, social behavior, and all our functions: language, memory, and perception (Pfaff, 2018; Trabucco-miguel, 2008). These neurological diseases are at the origin of motor, neurosensory, and cognitive deficits, which deteriorate environment perception (Cofler, 2016). Our sample only concerned adults since children are not admitted in these services. The survey was conducted in two hospital accommodation units: the neurology service of the UHC Ibn Sina in Annaba and that of Benbadis hospital in Constantine. Constantine and Annaba are two of the largest cities in Eastern Algeria, each one drains the flow of patients from neighboring wilayas (territorial division of Algeria). The neurology service wilaya of Annaba accommodation unit has 19 beds spread over four bedrooms (one room for men and three rooms for women) aligned on one level (Figures 1 –5). It was built during the colonial period to accommodate a psychiatric hospital (Annaba Health Department, 2018, 2019; Baghriche, 2010).

Situation of the neurology department of the Annaba University Hospital. Source: Google Map 2020; Picture taken by Chawki Loucif Feb 2020; treated by Soundouss I. Talantikite, 2020.

Distribution plan for the accommodation unit of the neurology department of the Annaba University Hospital. Source: Soundouss I. Talantikite (2018), Software used Autocad 2016.

Photo of the neurology department building of the Annaba University Hospital. Source: Soundouss I. Talantikite (2018).

Distribution corridor for the accommodation unit of the neurology department of the Annaba University Hospital. Source: Soundouss I. Talantikite (2018).

Medical room in the accommodation unit of the neurology department of the Annaba University Hospital. Source: Soundouss I. Talantikite (2018). Note. We did not have the patient’s agreement to take a picture of the rooms, so we only took a picture of the bed while it was empty.
Originally a college then a convent for the Christian sisters, the building was transformed into a civilian hospital “Benbadis University Hospital Center of Constantine” in 1986 after a political decision (No. 86.298 of 16 December). Neurology service accommodation unit consists of 34 beds spread over 10 rooms (five men rooms and four women rooms, one women room is closed due to the collapse of the ceiling). Before hosting the neurological service, this building served as an asylum during the colonial period (Figures 6 –10; Baghriche, 2010; Constantine Health Department, 2018, 2019).
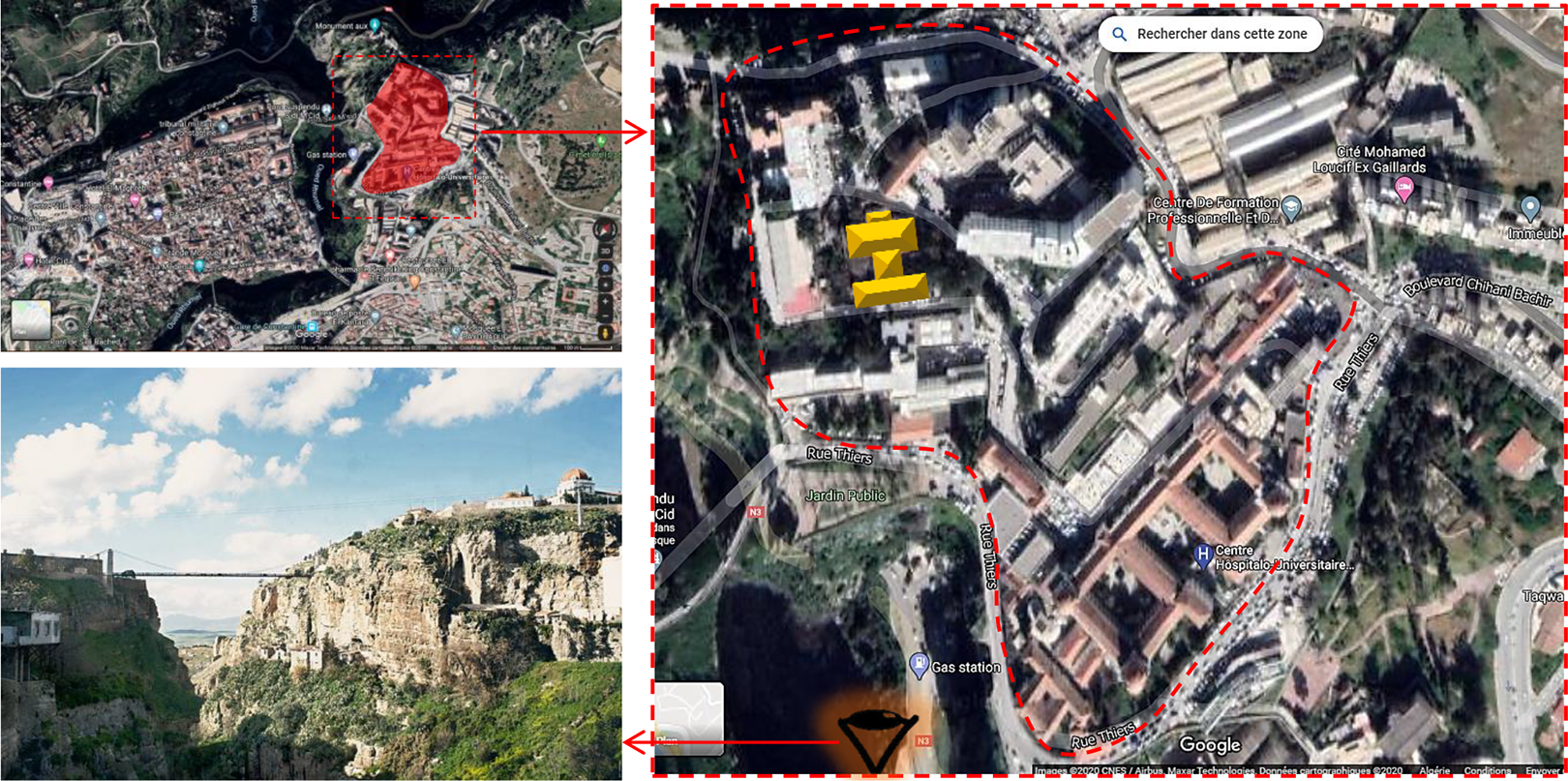
Situation of the neurology department of the Constantine University Hospital. Source: Google Map 2020; picture taken by Soundouss I. Talantikite, 2017; Soundouss I. Talantikite treatment 2020.

Distribution plan for the accommodation unit of the neurology department of the Constantine University Hospital. Source: Soundouss I. Talantikite (2018), Software used Autocad 2016.

Distribution corridor for the accommodation unit of the neurology department of the Constantine University Hospital. Source: Soundouss I. Talantikite (2018).

Women’s room (three beds) in the accommodation unit of the neurology department of the Constantine University Hospital. Source: Soundouss I. Talantikite (2018).

Men’s room (three beds) in the accommodation unit of the neurology department of the Constantine University Hospital. Source: Soundouss I. Talantikite (2018).
Despite the various renovations, these buildings are dilapidated and outdated, they do not respond to current safety standards for the construction of medical buildings and suffer from a lack of mismanagement equipment. The reception capacity is much lower than the flow of patients, the units lack space and beds (especially the neurology department in [Annaba]). The guided and commented visit by the head of the department also raised a major dysfunction of this department caused by poor management and spatial organization. We should note that the spatial organization has not changed since the colonial period. We notice the presence of bars on the windows used while the services were dedicated to psychiatry.
Ethical Considerations
Ethical approval of the study was obtained in two stages. First, approval was obtained from the Doctoral Council of the Faculty of Architecture and Urban Planning, Department of Architecture of University Salah Boubnider Constantine 3. Second, the research committees of the two participating hospitals approved the study. Oral consent was obtained for each interview conducted. The anonymity of the respondents was preserved. Approval to conduct the investigation at the Annaba University Hospital was granted on January 25, 2017, and that of the Constantine University Hospital on February 11, 2019 (in Attachment).
Questionnaire Development
The questionnaire instrument was developed in six stages, spread over 3 years.
Stage 1: A literature review of spatial atmosphere in hospitals allowed us to define 33 items that make up an architectural ambiance. A number of 335 references (Table 1) allowed us to define five ambient physical factors: sound, visual; thermal and olfactory comfort (an excel file of the database is joined), and eight factors concerning the socioprofessional characterization of the patient (MacAllister & Zimring, 2019). In addition, 25 items for patient satisfaction and well-being were extracted from a tool proposed by the center for health design, the clinic design patient survey, and clinic design section (The Center for Health Design, 2015).
First 48 Lines of the Literature Review Table.
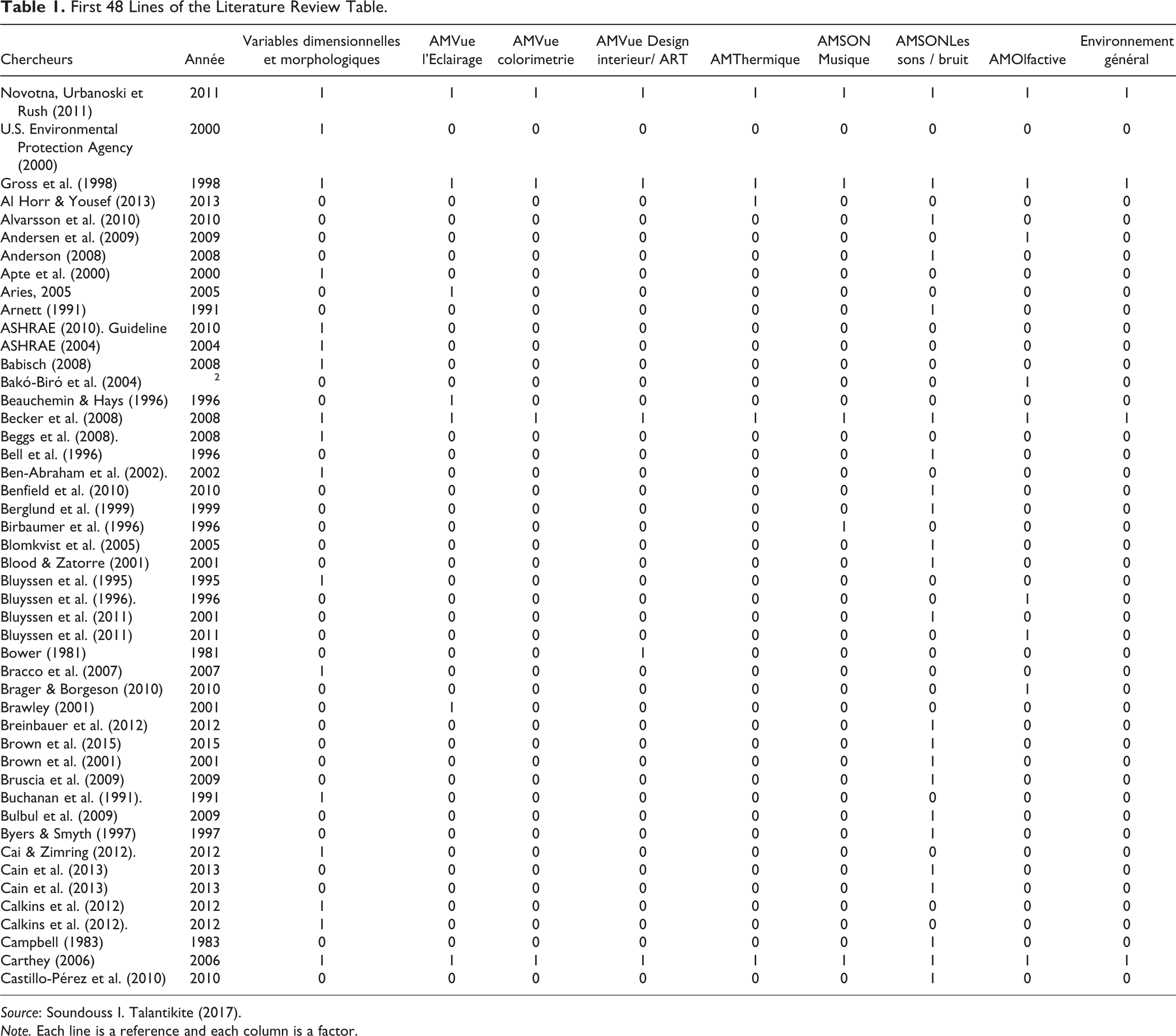
Source: Soundouss I. Talantikite (2017).
Note. Each line is a reference and each column is a factor.
Stage 2: A first investigation was carried out at the services in order to verify concordance of the ambient factors selected. We did semistructured interviews on 21 healthcare staff members, the heads of the two neurology departments, as well as the two heads of nurses, nine neurologists, and eight nurses divided between the two studied departments. The data collected are relating room ambiance and how it affects patient’s condition, also we asked for patient satisfaction during their stay.
Stage 3: Results of the two stages of investigations allowed us to develop a draft questionnaire (Figure 11). The questionnaire was written in French and translated into Arabic (national language) for those patients who do not master the French language. The draft questionnaire was then evaluated in a pilot test to analyze the comprehensibility and clarity of the items.
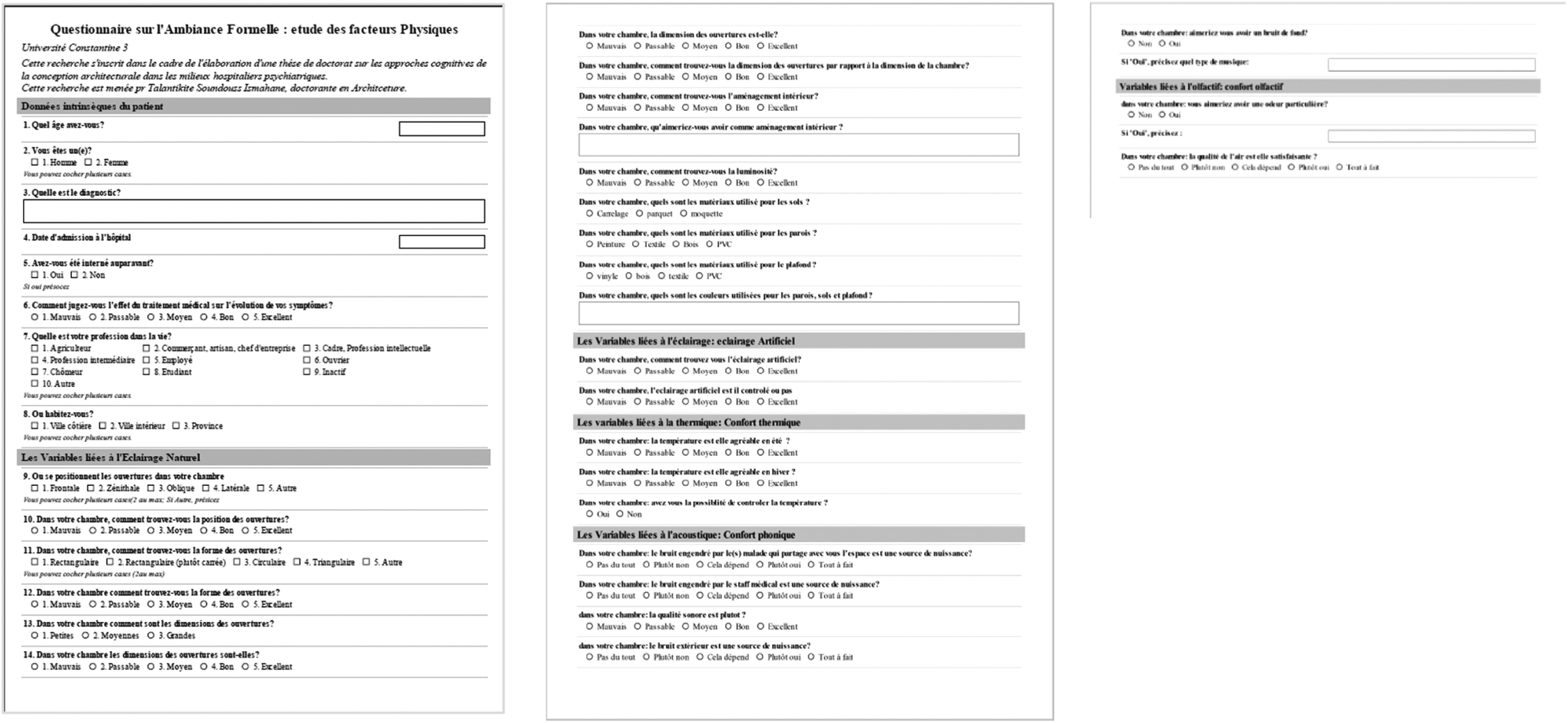
Overview of the draft questionnaire. Source: Soundouss I. Talantikite (2017).
Stage 4: The pilot test showed that the format of the questionnaires was inappropriate for the context, based on the literature, the questionnaire does not meet the accommodation conditions and building state of degradation, the results obtained were too scattered and could be inconsistent because of a sample of 15 patients, missing data, and contradictory answers. Several hypotheses can be advanced. The state of the hospital’s infrastructure and patients’ health condition could explain the disengagement of the respondent. For hygienic reasons, I had to wear a doctor’s white coat during “in situ” investigation. Consequently, the patients mixing with the health staff were able to answer in a diplomatic way to avoid any embarrassment. This first test allowed us to revise our questionnaire following the reality of the field and the sample.
Stage 5: A categorical thematic content analysis (Berelson, 1954) applied to the answers allowed us to build the questionnaire (Figure 12) following a satisfaction scale for the patient’s room through 19 items. The patient responds on a 5-point semantic-type Likert-type scale, gradually going from (−2) to (2), where six items concern patient personal characterization data (age range, gender, first hospitalization, socioeconomic level, living town, and disease), ambiantal physical factors consist of 13 items, and six items for patient satisfaction and well-being. The questionnaire contained an open-ended question to enable respondents to communicate their ideas on how to improve the physical environment.
Stage 6: The final questionnaire (Figure 12) was presented to some researchers who work in the faculty of architecture and some doctors who agreed to assess it and note if there are inconsistencies. The questionnaire was finally validated by all of the evaluations.
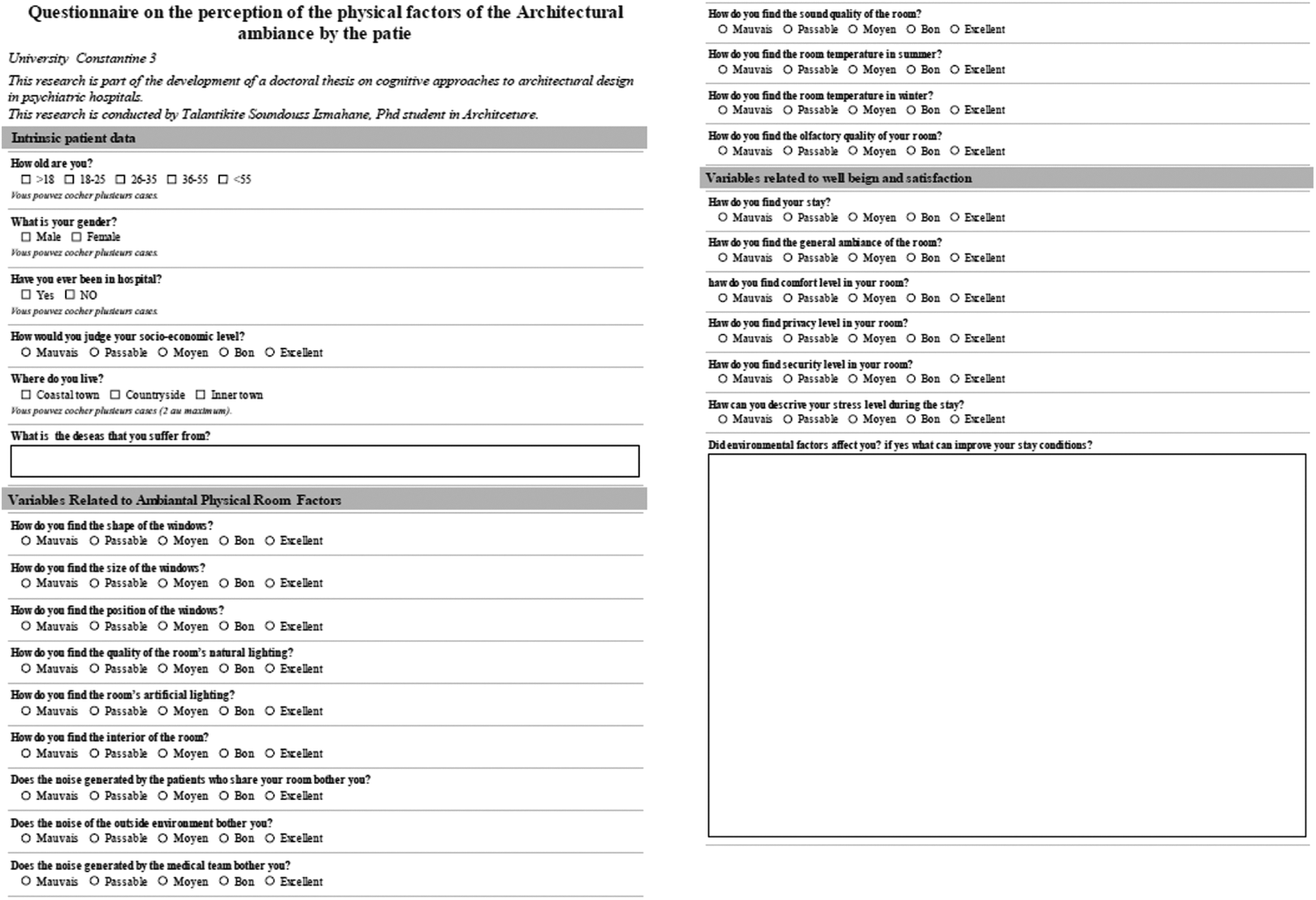
Overview of the questionnaire. Source: Soundouss I. Talantikite (2018).
Data Collection
Data collection took place during February 2018 at the neurology accommodation unit of Annaba and during February/March 2019 at the neurology accommodation unit of Constantine. The questionnaire was self-administered to all hospitalized patients (19 patients at UHC Annaba and 34 in Constantine). The administration of the questionnaire was done in the afternoon after lunch. We took great care choosing the right time and paying attention to the patient’s health. The collection of the completed questionnaire was done the same day. When the patients were unable to answer questions because of their health status, we referred to the nurses who accompanied them to obtain the necessary answers to our research. When the patient was illiterate (3.77% women, average age 64 years; 1.88% men, 75 years), we used a direct interview. In order to ensure that answers were not influenced by fear of retaliation, we used the techniques of direct (in situ observation) and reactivated observation (analysis of photos taken in situ) into our investigation. These techniques allow us to better grasp the reality of the field of investigation, without fear to collect testimonies from actors suspected of selectivity or reconstruction of reality (Arborio, 2007).
Data Analysis
The database was recorded by the Excel software, and statistical analysis was done by the IBM-SPSS Version 22 software. Descriptive statistics on the item and scale frequencies, percentages, means, and standard deviations were computed for the patient’s social characterizations. The test for differences of independent correlations was carried out. In this study, we employed principal component analysis (PCA) to identify the underlying structure characterizing a set of highly correlated variables for the 13 items dealing with the ambiantal qualitative physical factors. PCA was also performed for the six satisfaction and patients well-being items. The variance accumulation test commonly called “scree test” requires that a graph be drawn showing the size of the eigenvalues of the different components according to their order of extraction. Variance maximization (varimax), with Kaiser’s normalization, an orthogonal rotational strategy has been chosen for this study. Three summated indices were extracted from the 13 question items of the room’s physical ambiance factors: visual, thermal, and sound. And two components were extracted from the second PCA: satisfaction and well-being. To explore coherence, we carried out bivariate Pearson correlation test.
Results and Analysis
Respondents’ Characteristics
Six variables relating to the patient’s intrinsic data were retained. Of our sample of 53 hospitalized patients, the average age is 39 years with a relatively high standard deviation of 14,582, 45.3% are in the age-group of 36–55 years. We note the presence of one child per service, these are exceptional cases of care given the seriousness of their cases. Almost a quarter of the sample (24.5%) represents the age-group of 26–35 years (Table 2). Women represent 50.9% of the panel compared to 49.1% of men. The social level is slightly below the average with a standard deviation of 0.678 and an average of −0.4; 34% of patients questioned have already been hospitalized, while it’s the first time for 66% (Table 2). Patients coming from inland cities represent 45.3%, 43.4% come from the countryside, and only 11.3% come from coastal cities. This is explained by the fact that the service of (Town Name 1) receives a flow from the inner wilayas, and also due to the fact that the service of (Constantine) has a greater capacity and is located in an inner city, drain a stream from the surrounding inner wilayas as well (Table 2). Patients in our sample are treated for the following diseases: stroke 28.3%, multiple sclerosis 24.5%, myasthenia 13.2%, subarachnoid hemorrhages 11.3%, myasthenia gravis 9.4%, myopathies 7.5%, and barred guillotine syndrome 5.7%, respectively (Table 2). A descriptive analysis of the questionnaire items is given in Table 3.
Background Information of the Respondents.
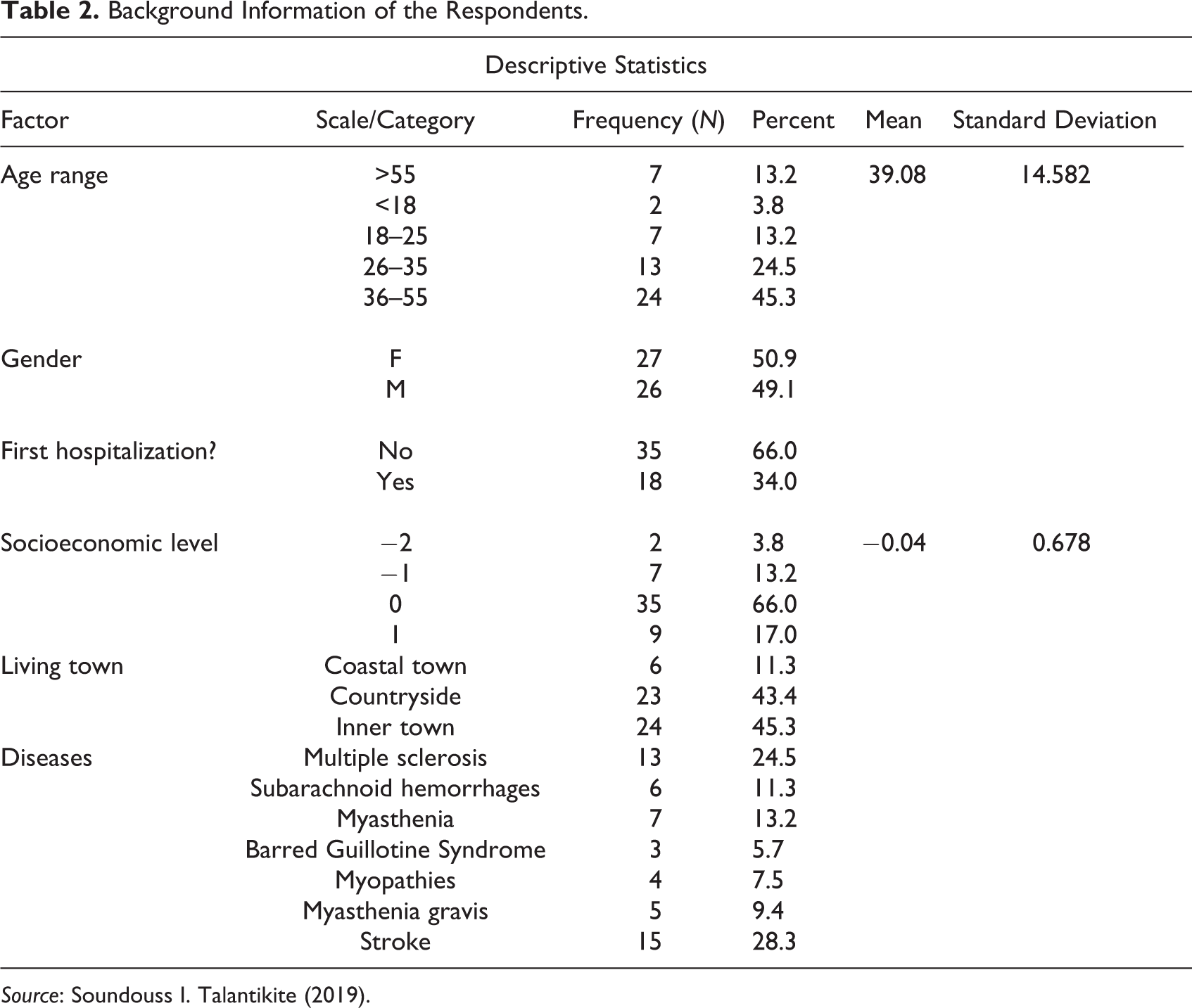
Source: Soundouss I. Talantikite (2019).
Descriptive Analysis of the Questionnaire 18 Items.

Source: Soundouss I. Talantikite (2019).
Note. −2 = bad; −1 = passable; 0 = Medium; 1 = good; 2 = excellent.
Ambiantal Physical Items PCA
Before performing a PCA, we ensure that the variables used are relevant, sufficiently correlated and that there are no cases of singularity where a variable is entirely defined by one or more other variables combined. To help diagnose problematic conditions in the correlation matrix, we analyzed the Kaiser-Mayer-Olkin measure of sampling adequacy which can be qualified as “average” (Kaiser-Mayer-Olkin measure of sampling adequacy = 0.584), and Bartlett’s Test allows us to reject the null hypothesis that our data would come from a population where the correlation matrix is an identity matrix (Bartlett’s test of sphericity sig = .000). The analysis of these statistics encourages us to pursue PCA.
An initial analysis was run to obtain eigenvalues for each component in the data. Five components had eigenvalues over Kaiser’s criterion of 1 and in combination explained 73,994% of the variance. This is the number of components that were retained factor loadings after rotation which are given in Table 4. The reliability of each attribute was examined by Cronbach’s α coefficient. The reliability estimates for the first three components were greater than 0.60 (Table 4), indicating a strong internal reliability among items with similar attributes. The Cronbach’s α coefficient for Components 4 and 5 is less than 0.6, consequently, the assumptions of the reliability model are not respected. According to the results, we will retain only the three first components for the final analysis, also, according to the results, 40,857% of the total variance was explained by Component 1 (it combines between visual factors, sound factors, and thermal factors). The rest of the variance was explained by the remaining four components.
Rotated Component Matrix of Questionnaire Ambiantal Physical Items.

Source: Soundouss I. Talantikite (2019).
Note. Extraction method: Principal component analysis. Rotation method: Varimax with Kaiser normalization.
a Rotation converged in seven iterations.
b The Cronbach’s α coefficient is less than 0.7. Consequently, the assumptions of the reliability model are not respected.
Satisfaction and Well-Being Items PCA
Like the first PCA, we analyzed the Kaiser-Mayer Olkin measure of sampling adequacy which can be qualified as “average” (Kaiser-Mayer Olkin Measure of sampling adequacy = 0.626), and Bartlett’s Test allows us to reject the null hypothesis that our data would come from a population where the correlation matrix is an identity matrix (Bartlett’s test of sphericity sig = .385). The analysis of these statistics encourages us to pursue PCA. Two components had eigenvalues over Kaiser’s criterion of 1 and in combination explained 47.402% of the variance. This is the number of components that were retained factor loadings after rotation which are given in Table 5. The PCA result suggested that Components 1 and 2 represented satisfaction and well-being, respectively.
Rotated Component Matrix of Questionnaire Satisfaction and Well-Being Items.

Source: Soundouss I. Talantikite (2019).
Note. Méthode d’extraction: Analyse en composantes principales. Méthode de rotation: Varimax avec normalisation Kaiser.
a Rotation converged in three iterations.
b The Cronbach’s α coefficient is less than 0.5. Consequently, the assumptions of the reliability model are not respected.
Relationship Between Personal Characterization and the 19 Items
Our 19 items will be correlated via six personal patient characterization (age range, gender, first hospitalization, socioeconomic level, living town, and disease) according to a specific categorization for each one. The study sample being relatively small we conducted a nonparametric test on 19 questionnaire items and reported them in Table 6. Results show that there is a significant difference in perception between patients with different diseases for the following items: natural lighting quality (p = .008), interior layout of the rooms (p = .000), windows dimensions (p = .015), room sound quality (p = .004), windows shape (p = .000), room temperature in winter (p = .000), and security (p = .023). For the gender characterization, we observe significant results with the following items: windows shape (p = .002), external noise pollution (p = .011), noise pollution caused by other patients (p = .004). Hospitalization and patients’ socioeconomic level characterizations have significant difference for the security item, respectively, in order p = .045; p = .023. No significant difference in perception was found for the other items.
Nonparametric Test Result.a

Source: Soundouss I. Talantikite (2019).
a Kruskal–Wallis test.
b Mann–Whitney U test.
*p < .05.
Coherence Test: Bivariate Pearson Correlation Test
This correlation is explored between the two components of satisfaction and well-being factors and the three components of physical ambiantal factors. Normality test results show that the dispersion of the variables is linear (Table 7). Therefore, we can proceed to the bivariate Pearson correlation test. This test revealed an average correlation for the comfort feeling factor at level .01 with the olfactory comfort factor (.386) and the room temperature in winter factor (−.370), the first correlation is positive in nature while the second is negative. A third correlation at the .05 level of negative nature is observed with the room sound quality factor (−.312). The safety factor is moderately correlated at the .01 level with the factor noise pollution caused by other patients, correlation is positive. For privacy factor, a weak correlation at level .05 of a positive nature is observed with room temperature in winter factor (Table 8). No significant correlation was found for other items, this may be due to the small number of the sample.
Normality Tests.

Source: Soundouss I. Talantikite (2020).
a Correction de signification de Lilliefors.
Bivariate Pearson Correlation test.
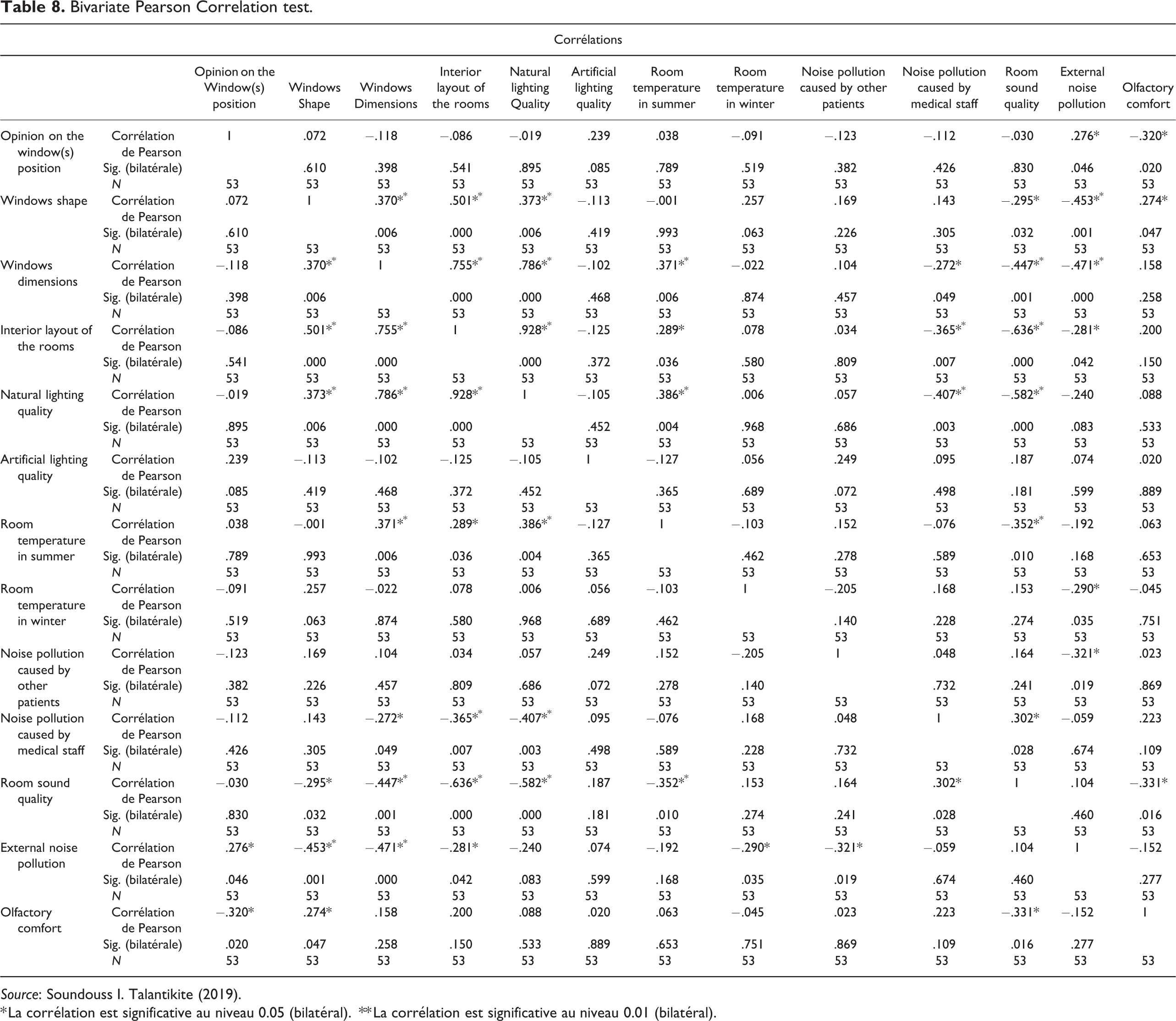
Source: Soundouss I. Talantikite (2019).
* La corrélation est significative au niveau 0.05 (bilatéral).
** La corrélation est significative au niveau 0.01 (bilatéral).
Discussion
Descriptive Analysis of the Questionnaire 19 Items
Hospitalized patients have the best position to guide architects to design hospital service in general and in the design of the patients’ rooms’ architectural ambiances in particular. Their perception of physical ambiantal factors is based on their observation and space interaction during hospitalization. The 13 ambiantal physical items studied were all classified relatively medium with mean scores ranging between −0.55 < mean < 1.34, on a scale of −2 to 2. Patients therefore consider the room ambiance to be medium. A discomfort is pointed to the sound ambiance inside the room, indeed the mean score of the two items that represent it is negative: noise pollution caused by other patients = −0.55 and noise pollution caused by medical staff = −0.25, with a standard deviation considered minimal 0.503 and 0.705, respectively. These two scores are the lowest of the sample. The notation of the outside sound is diametrically opposite to the inside, it is considered good with a mean score of 1.34 for a standard deviation of 0.732, it is therefore the most appreciated among the 13 items. The second best noted factor is the quality of the natural lighting with the olfactory comfort: mean score 0.74; standard deviation of 0.902 and 0.56, respectively. The items related to the visual factor are all classified as medium, this confirms the positive appreciation of natural lighting. Thermal factor is also considered medium with a mean score of 0.23 and 0.26 for room temperature in winter and room temperature in summer, respectively. Interior layout of the rooms had the mean score of 0.42 with a SD of 1.167. The results obtained are rather logical and are consistent with the interior design and the privileged situation of hospitals. UHC Constantine and UHC Annaba are decentralized off the city. UHC Constantine is high and overlooking the city, while UHC Annaba is high and overlooking the Mediterranean Sea. The orientation of the different buildings is also a very important factor. Isolated position of the services, orientation, shape, and size of the windows limit external noises and provide good light quality and a pleasant thermal comfort.
Patients’ satisfaction and well-being results meet with findings of ambiantal physical factors. The six items studied were all classified relatively medium with mean scores ranging between −0.25 < mean < 1.77, on a scale of −2 to 2. General room ambiance perception and comfort level are judged medium, respectively, with 0.13 and 0.8 mean scores. Security level was judged near excellent with 1.77 mean score with a standard deviation relatively low 0.423. Patients are moderately satisfied by their general conditions stay (mean = −0.4, SD = 0.784), find that there is a lack of privacy with a negative mean rate −0.25 and their stress level is slightly lower than average (mean= −0.11, SD = 0.725).
Dating from the colonial period, rooms’ interior layout is outdated, so patients’ rooms do not meet current comfort requirements. All rooms are multiples, starting from three to five beds per room. This situation accentuates nuisances engendered by other patients; this explains why the rating of interior sound quality was quite low. Multiple bed rooms have consequences in other parameters such as privacy and air quality. So as for the air to remain healthy, it must be renewed. The lack of a mechanical ventilation system and the large number of patients per room induce the opening of windows to air, even in winter, which deteriorates the quality of thermal comfort in that cold season.
Correlation of Perception of Ambiantal Physical Factors; Patients’ Satisfaction and Well-Being With Patients’ Personnel Characterization
Correlation of the 19 items with the six factors of patients’ characteristics allowed us to identify some perception disparities. The most notable differences are found in patients’ disease and gender factors. The nonparametric test results show that there is a significant difference in perception between patients with different diseases in natural lighting quality (p = .008), interior layout of the rooms (p = .000), windows dimensions (p = .015), room sound quality (p = .004), windows shape (p = .000), room temperature in winter (p = .000), for ambiantal physical items, and security (p = .023) item for satisfaction and well-being items. Diseases that we have identified in our sample have symptoms such as muscular weakening going to paralysis (depending on the severity), ocular weakening or ocular disorders, and deterioration of cognitive functions (Cofler, 2016), for example, patients with subarachnoid hemorrhages develop an intolerance to light (photophobia) or noise (phonophobia). “Cognitive and motor disorders from which neuronal patients suffer make the immediate environment a high priority. Patients’ room must be carefully designed to positively support the patient during their stay, each ambient factor has to be improved to meet their needs.”
Women are more sensitive to noise and pay more attention to room details, they were more critical in rating windows shape p = .002, external noise pollution p = .011, and noise pollution caused by other patients p = .004 (Table 6). In Algeria, it is the women who take care of house interior design and the different domestic chores, this could explain their great requirement compared to the men.
The living town factor allows us to observe differences in relation to the thermal factor: room temperature in summer and room temperature in winter. The second difference relates to the natural lighting quality item (coastal town mean score=1.5, countryside mean score = 0.48, inner town 0.79). This is due to the difference in climate between the different areas studied. Annaba is a coastal city with a moderate climate all year round, with a humidity level that can be very high especially in summer. Constantine is an inner city with a cold harsh climate and a hot dry summer. Patients who are hospitalized for the first time are more critical in security (p = .045) than patients who have been hospitalized before. The field of patient satisfaction was defined by early research work (Sitzia & Wood, 1997). They defined patient satisfaction as a reflection of preferences, expectations, and the reality of care.
Impact of Ambient Physical Factors on Patient’s Satisfaction and Well-Being
The overall findings agree with researches on the impact of architectural ambiance in healthcare. The overall assessment of hospitalization care spaces considered moderately favorable. Patients are moderately satisfied of their stay, they find that general ambiance perceived and level of comfort are medium, also they rank level of security as good. However, they denounce the lack of privacy. Data analysis results of the two groups of items, ambiantal physical items and patient’s satisfaction and well-being items, are coherent and complementary. Ambiantal physical items allow us a better understanding of patient’s satisfaction and well-being items regarding the effect of ambiances on the patient.
The most comprehensive and influential research on the impact of architecture on health outcomes is that of Ulrich et al. (2008), they tabulated their findings (p. 148), showing where empirical studies have found relationships between specific design factors and healthcare outcomes. They deduce that a design intervention improves a healthcare outcome. The analysis of the literature on the impact of light on outcomes in health facilities showed that increasing sunlight in patients’ rooms improves psychosocial health and reduces the use of analgesia, drug costs, and length of stay (Joseph, 2006). The effect of hospital sound environments on patient recovery process has been of interest since the 1860s (McCarthy et al., 1999). Thermal comfort is influenced by environmental parameters and personal factors (Katafygiotou & Serghides, 2014).
All responses (100%) to the open-ended question indicate the need to move to single or double rooms. The current rooms are multiple beds, and by adding family members, the room becomes overloaded. This distribution of patients causes discomfort among patients, and it is the origin of the bad sound ambiance. The general state of the room and the existing furniture is also questioned, patients request a deep renovation and new furniture. In Annaba service, 70% of the women ask separation from men’s room for safety and respect, this is explained by the social and religious factor of the Algeria population. Macallister (2014) highlights the importance of hospital design—and spatial layout in particular—for patient interactions in the room and, ultimately, for patient satisfaction. In terms of personal space, there is a preference for single rooms (Taylor et al., 2018); the satisfaction of the patient is linked to the perception of the comfort of the decor, the cleanliness, the courtesy of the household helpers, the temperature, and the noise (Schweitzer et al., 2004). “Results indicate that good reflection on the design of individual-type hospitalization rooms, which take into account the emotional (sensitive) state of the patient by integrating the physical factors (natural lighting variable, sound variable, thermal variable, olfactory variable), can contribute significantly to patient’s well-being.” The use of these results is a first step to better understand the role of the environment in patient satisfaction, which is not simply based on the quality of care but also on the perception of ambiances in care spaces and the immediate environment through the five senses.
Prescription of the Therapeutic Landscape as a Complementary Tool of Medical Treatment
Studying the notion of ambiance in healthcare settings should be combined with social and sensitive dimension of the occupied space. This approach has been developed through the notion of “therapeutic landscape” around “physical,” “social,” and “symbolic” environments (Mazuch & Stephen, 2005). Empirical studies deduced that a design intervention improves a healthcare outcome. Design factors contributing to positive health outcomes, highlighted in this study are natural lighting, view of nature, and sound quality for physical ambiantal factors. Regarding satisfaction and well-being, single bed rooms (related to privacy) and security of patients are pointed out. Other researchers are adopting the “Healing by Design” approach (Stichler, 2008), which reviews Planetree approach to architectural design, which in turn inspired Golembiewski’s reinterpretation of the salutogenic model (Golembiewski, 2010) introduced by Antonovsky (1996). “Nowadays, if doctors prescribe medicines for individual diseases, conditions, or injuries, they should also advise patients on the environmental factors they need to avoid in order to help their recovery.”
Limits of Research
The study has some limitations. The number of patients was relatively small considering the capacity of the services in which the study was carried out, and the unique nature of the study in Algeria did not allow to compare responses. The oldness of hospitals may have hindered research work. Buildings date back to colonial period and have rudimentary equipment. Patients’ responses may not be 100% reliable. Patients may have changed their responses for fear of retaliation, respondents may have been more diplomatic and evasive in their responses. Also wearing a white coat during the survey may have affected their response.
Conclusion
In this work, we aim to have a better understanding of the role of architectural ambiance in patient satisfaction and well-being, by exploring neurological patients’ perception of physical ambiantal factors in their rooms. Investigating through 19 items, this analysis demonstrates the sensitive relationship between the quality of architectural ambiance and the state of patient’s health. Indeed, the disorders inherent in neurological diseases could favor a particular relationship to space, which could either help as a complementary tool of medical treatment or further deteriorate these disorders.
The results indicate a lack of privacy due to multiple bed rooms, this distribution of patients causes discomfort among patients, and it is the origin of the bad internal sound ambiance. Reflection should be oriented on the design of single or double rooms, taking into account personal characterizations and emotional (sensitive) state of the patient, by integrating ambiantal physical factors (natural lighting variable, sound variable, thermal variable, olfactory variable), to contribute significantly to their well-being. Previous studies have shown that aesthetic factors such as rooms improved by renovations, affect the patient’s experience or room characteristics (Lorenz, 2007). Nowadays, if doctors prescribe medicines for individual diseases, conditions, or injuries, they could also advise patients on the ambiantal factors they need to avoid in order to help their recovery.
There is no research in this field in Algeria; therefore, we would like to fill this gap and draw attention to the state of hospitals in order to launch a dynamic of restoration taking into account the importance of the ambiantal physical factors. Many factors of progress are to be realized. A first approach is to develop tools and methods that fit Algeria case and helps architects and designers to integrate ambiantal factors in renovation and construction of health facilities and room in particular.
Implications for Practice
This study allows us to better understand the needs and expectations of Algerian patients, by proposing a space that combines the rigidity of the functional needs of health spaces and the personal needs of the patients, while integrating the sociocultural specificities of Algerian society.
The study carried out allowed us to precisely define the physical factors that influence the quality of the ambiance of these places, which will allow the prescription of precise and optimal ambiant conditions for the healing process, which in addition to be beneficial to patients will support the nursing staff in their task.
Establish, in collaboration with psychologists of the various units, a cognitive approach to the ambiant design of health spaces for the support of the patients during their period of hospitalization.
Propose specifications for the work to be carried out at Algerian hospitals in order to convince the authorities and officials concerned of the usefulness of creating a healthy space adapted to the needs of the patient. Indeed, we have noted a deterioration and dilapidation of these establishments, which date back to the colonial era.
Improve the hostile and unpleasant image known to health structures in Algeria.
Supplemental Material
Supplemental Material, sj-xlsx-1-her-10.1177_1937586720986106 - Effect of Spatial Ambiances on the Patient Satisfaction and Well-Being in Hospitals: The Case of UHC Ibn Sina Annaba and UHC Benbadis Constantine—Algeria
Supplemental Material, sj-xlsx-1-her-10.1177_1937586720986106 for Effect of Spatial Ambiances on the Patient Satisfaction and Well-Being in Hospitals: The Case of UHC Ibn Sina Annaba and UHC Benbadis Constantine—Algeria by Soundouss I. Talantikite and Meriama Bencherif in HERD: Health Environments Research & Design Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.