
Abstract
Purpose:
This article documents the development and implementation of a new approach for health facilities construction and maintenance planning, the use of a Facilities and Clinical Coordination (FCC) Council, at Walter Reed National Military Medical Center (WRNMMC).
Background:
WRNMMC is preparing for the largest and most complex renovation project in recent Department of Defense history. There is sparse documentation demonstrating stepwise frameworks for the implementation of effective and efficient health facilities maintenance management tools and techniques.
Method:
This study discusses the development and evaluation of the FCC Council. Clarity to the literature sources guiding the development of the FCC Council is provided, followed by the survey approach undertaken to assess Council efficacy based on participants’ perceptions. Data are analyzed using descriptive and inferential statistics.
Results:
Our study suggests routine cross-functional synchronous FCC Council meetings improve perceptions of safety and communication, encourage teamwork, and are more productive when conducted using synchronous rather than asynchronous communication. Clinician participants strongly supported the face-to-face meeting approach and considered such meetings more effective as they are perceived to maintain staff and patient safety as a constant organizational focus.
Conclusion:
The FCC’s perceived effectiveness toward improving healthcare facilities maintenance planning centers on engaged leadership, the inclusion of diverse subject matter experts, and structured group facilitation. Our results inform health facilities planners of the value the FCC Council brings to an organization by helping to develop organizational buy-in for major facilities renovation projects.
Keywords
Across the healthcare landscape, there exists a continued ambition for improving the environment of care. Zadeh and colleagues (2015) describe the healthcare environment consisting of increasingly outdated facilities averaging over 30 years old, which are costly and dangerous to both patients and staff. This case study shows how the facilities management process at Walter Reed National Military Medical Center (WRNMMC) evolved to meet constantly changing operational needs and trends toward evidence-based design (EBD) outcomes. There is sparse documentation demonstrating stepwise frameworks for the implementation of health facilities maintenance management tools and techniques for practitioners (Temel et al., 2019; Yousefli et al., 2017). In our discussion, we review the medical center’s historical process, then provide “blueprints” to integrate these tools and techniques into a formal process involving both facilities and clinical personnel, and conclude with the results of a preliminary assessment of the process.
Literature Review
The benefit as well as the need to conduct renovation and reconstruction is indicated through multiple studies, yet an ever-present question of how best to execute these tasks remains (Beauvais et al., 2019; Ulrich et al., 2008; Zadeh et al., 2015). EBD has emerged as a method for new construction and renovation projects with hopes to reduce safety incidents as well as improve patient and staff outcomes. On the premise of cultivating an environment of patient safety, implementing EBD can decrease hazards and risks such as patient falls (Zadeh et al., 2015). Patient experience, which is linked to bolstering clinical outcomes, can also be improved by incorporating EBD elements (Ulrich et al., 2008). Additionally, there is corollary evidence from the airline and hospitality industries to suggest patients may express greater confidence in organizations with more modern facilities (Goldman et al., 2010). Lastly, as staffing shortages continue to challenge healthcare executives, improving staff experience by updating the work environment can help with retention and recruitment (Hassmiller & Cozine, 2006). While there exists some leader hesitation toward making these large cash outlays for facility improvements, the relatively new Medicare & Medicaid Service Value-Based Purchasing (VBP) Program appears to incentivize hospital leadership to overcome their fears and make the investment to improve overall VBP performance (Beauvais et al., 2018). Considering the evidence suggesting the value of updating facilities, hospitals should ensure the planning process for these expensive renovation projects is effective and efficiently managed.
Management tools and techniques used within the health facility design and construction process are well established. One technique frequently used is the Big Room or Obeya concept, derived from Toyota lean manufacturing management strategies (Alves et al., 2017). The Big Room concept is an integrated project delivery modality intended to involve stakeholders early and aims to increase coordination, cooperation, and communication. Implementing the Big Room approach centers on creating a physical space in which a multi-disciplinary team of stakeholders will work from, throughout the duration of the project. The walls of the room are purposefully filled with detailed project information (Alves et al., 2017; Lean Construction Institute 2015). The colocation of team members facilitates frequent communication and decreases barriers to rapid problem-solving experienced in traditional project management methods (Alves et al., 2017; Temel et al., 2019).
The value of lean management techniques, such as the Big Room, is undisputed in the health facility design and construction process (Alves et al., 2017; Joshi et al., 2020; Temel et al., 2019). However, measuring the effectiveness of these approaches has been mostly anecdotal to date with the exception of the recently created Big Room Effectiveness Index (Joshi et. al., 2020). The BREI is “a quantitative framework used to assess the effectiveness of collaboration planning in a Big Room” (Joshi et al., 2020). The index ranks performance within four categories: (1) Collaboration, (2) Look Ahead Planning, (3) Knowledge Building and Tools Used, and (4) Continuous Improvement (Joshi et al., 2020). Within these categories are 10 distinct measurable parameters that are weighted based on importance to the successful execution of the Big Room concept, with collaboration weighted the highest (Joshi et al., 2020). Since the BREI attempts to measure collaboration using quantitative, objective measures such as commitments kept in the last month and number of training modules conducted last month, it lacks the ability to measure the sentiment of the participants. How individuals feel about their work environment directly impacts their commitment (Mowday et al., 1979; Rusbult et al., 1998). Thus, the inability to measure sentiment hinders the ability to explain or predict an individual’s commitment level, which Joshi and colleagues feel is central to effective Big Room implementation.
In 2017, Yousefli et al. conducted a systematic review of facilities maintenance literature. This review categorized the facility maintenance (FM) literature into three levels of maintenance management: strategic-level decisions, tactical issues, and operational aspects. At the strategic level, management strategies focused largely on describing maintenance management as determining the effects of planned “preventative maintenance” or unplanned “corrective maintenance” events and their impact on the end user (Jandali et al., 2018; Rani et al., 2015, Yousefli et al., 2017). At the tactical level, elements such as cost, equipment sourcing, and contract management are discussed in order to determine effective predictive measures to account for the total lifecycle costs, comprised largely (over 35%) of maintenance activities (Grager, 2012; Yousefli et al., 2017). The operational aspects consisted of resource allocation and risk management. Resource allocation aims to prioritize maintenance projects, seeking to focus more resources on projects associated with the hospital’s core activities (Yousefli et al., 2017), while risk management seeks not only to account for the primary impacts of maintenance on hospital operations but also for the third-order effects such as staff and patient safety along with satisfaction (Yousefli et al., 2017).
While each of these levels is logically created and executed well within their own respects, there exists a lack of planning techniques within the literature that allow for the ability to assimilate these three levels effectively within a single coherent strategy. While the literature points to the value of effective FM planning to incorporate EBD in an outdated environment of care, the absence of a formalized process guiding practitioners on how to seamlessly integrate these three levels of maintenance management limits healthcare leaders in their quest to ensure a clear path to optimize the environment of care.
The Case Setting
WRNMMC is a 244-bed facility providing patient care for over 1 million beneficiaries per year through a vast array of both inpatient and outpatient services. Conceptualized by Franklin Delano Roosevelt in 1939, the hospital expanded over the decades, and in early 2018, WRNMMC began its latest transformation through a series of major construction initiatives to improve the environment of care. Estimated to last over 7–10 years and at a cost of approximately $805 million, this project includes demolishing nearly one third of the existing aging infrastructure and the construction of new facilities within the demolished footprint, all while maintaining daily healthcare delivery operations. The ability to concurrently plan and perform substantial maintenance projects while ensuring patient and staff safety amid temporarily moving clinical space needed to be meticulously coordinated.
The Historical Process
Asynchronous Computer-Medicated Communication Versus Synchronous Face-to-Face (F2F)
The historical process to approve FM project requests at WRNMMC used asynchronous computer-mediated communication (CMC) among specific stakeholders relevant to a maintenance project. A digital FM request “project approval document” was emailed and routed to various stakeholders for input. Stakeholders either approved the maintenance request or voiced concerns. After the stakeholders annotated their comments on the digital form, the facilities management team reworked the proposal to mitigate any identified issues. The updated digital proposal was then resubmitted back to the stakeholders for a second review. The FM proposal was then approved or sent back through the resubmission process again until all concerns were addressed.
The asynchronous CMC strategy continues to grow as a common technique for working groups desiring cost-effective ways to pull remotely located team members together and is most often used for FM planning (Hill, 2000). Additionally, within the healthcare industry, CMC is used to allow stakeholders, such as clinicians, to remain longer in their patient care roles. The thought is that in between providing patient care, clinicians can review the maintenance request and quickly provide feedback on any concerns from their perspective.
However, these perceived benefits of CMC are practically misguided. First, within the healthcare industry, key stakeholders, facilities maintenance leaders, and clinicians are often geographically colocated. Additionally, while CMC may appear as a cost-effective use of individuals’ time, it lacks multiple essential communication elements resulting in more “back-and-forth” needed to clarify ambiguity, delaying progress toward final decisions (Bergiel et al., 2008; Lean Construction Institute, 2015). The process of garnering feedback can be fragmented and protracted as stakeholders often report to different leadership structures in the organization causing distractions from competing priorities (Webber, 2002). The inefficiencies and prolonged process of gathering feedback makes the CMC strategy less appropriate for the healthcare environment.
A synchronous F2F meeting platform is the alternative to a CMC approach. In many cases, F2F meetings can be considered an outdated, inefficient misutilization of staff member time. Contrary to these beliefs and although F2F meetings can be costly and challenging to organize, it sends a message of executive leader emphasis on the organizational priority for the safety and satisfaction of both the patients and staff (Khanzode, 2020; Storper & Venables, 2004). As consistently demonstrated in the use of the Big Room concept, it is important to note the possible efficiency gained with having all stakeholders in the room at once if the meeting is executed well (Joshi et al., 2020; Khanzode, 2020). First, participants are more mentally present at a F2F meeting due to a decrease in workplace distractions. Second, ideas and friction points can be worked through faster by leveraging the benefits of F2F communication. Storper and Venables (2004) note “F2F meetings are particularly important where information is imperfect, rapidly changing, and not easily codified.” Last, F2F meetings result in less miscommunication among team members as compared to CMC methods (Blenke, 2013; Khanzode, 2020). These miscommunications can result in possible financial instability, since nonforecasted expenses are used to execute change orders after facilities projects are completed (Keys et al., 2016; Lean Construction Institute, 2015). The value of F2F meetings for healthcare facility projects is emerging as a strong communications strategy; the question still remains how those meetings should be conducted, along with who should attend. Additionally, strong consideration should be given toward deciding when to hold synchronous, virtual F2F meetings in the place of in-person ones in a post-COVID-19 world.
Essential Elements of the F2F Meeting
Leader engagement, psychological safety, and a structured agenda constitute three key elements of how a meeting should be conducted (Lean Construction Institute 2015; Malhotra et al., 2016). Leader engagement helps drive and sustain the progress of the decision-making process to ensure timely decisions. Skilled leaders are able to effectively garner good participation from team members to meet specific goals, help promote psychological safety, and encourage nonmajority functional team member participation (Lean Construction Institute 2015; Malhotra et al., 2016). Group members are increasingly willing to speak up, provide input, and disagree with others as they feel more psychologically at ease (Malhotra et al., 2016). Psychological safety enhances meeting effectiveness by gaining more diverse viewpoints. Meetings should be structured using a specific agenda and held to a specific time limit (Lean Construction Institute 2015). Structure, combined with a time limit, helps build predictability and aids in expectation management for participants.
Lastly, we incorporated the well-documented value of Freeman’s Stakeholder Theory principles in developing our cross-functional team (Atkin & Skitmore, 2008). Cross-functional teams are “a small collection of individuals from diverse functional specializations within the organization” (Webber, 2002). Within the facility design process, the proper mix of interdisciplinary stakeholders is critical (Mok et al., 2015). Malhotra et al. (2016) note equal representation of stakeholders facilitates the avoidance of dominance from one functional area, which is important for psychological safety and to facilitate organizational justice. The Lean Construction Institute highlights the need to periodically reevaluate the specific stakeholders based on the project being discussed (Lean Construction Institute 2015). While it is often thought of as inefficient for clinicians to attend these types of meetings, Keys et al. (2016) suggest almost all facility industry professionals value the input of direct care team members. Hence, the proper mix of clinical and administrative representation is required within these types of FM planning working groups to achieve the maximum productivity and effectiveness.
Development of the Facilities and Clinical Coordination (FCC) Process
In this section, we outline how WRNMMC developed and conducts the FCC process. The aforementioned literature and extensive documentation of lean management techniques served as the theoretical foundation for our approach. Using the Plan–Do–Study–Act (PDSA) methodology, WRNMMC started by conducting a systematic review of the historical FM planning process currently conducted at the facility (Christoff, 2018; Moser et al., 2020). Through multiple iterations of the PDSA cycle, the WRNMMC leadership needed to address three primary issues. First, the FM leaders identified a disjointed and overlapping asynchronous CMC FM approval process. Second, they found stakeholders were inconsistently informed of upcoming maintenance projects causing either disruption in patient care or delays in project execution. Finally, the current stakeholders in the approval process consisted mostly of administrators and facilities maintenance staff. After addressing these shortcomings, WRNMMC transitioned from primarily asynchronous CMC to a mixed methods approach relying heavily on the benefits of F2F meetings to gain maximum efficiency and effectiveness in the FM planning process.
Throughput became the next issue after developing the FCC F2F meeting. Figure 1 depicts the FCC process flow chart as compared to the historical process. On average, 65 projects are submitted weekly to the facilities management team at WRNMMC for review and adjudication. If the FCC was expected to review all of these, the system would quickly become overwhelmed. Efforts to decrease the volume of projects brought to the FCC for discussion led to the development of two prescreening processes. Annotated in Figure 1, the chief for Construction and the FM project coordinator first review the projects against the “FCC Trigger” criteria to determine which projects will move forward to the FCC Council. Broadly, the “FCC Trigger” criteria center on elements of patient or staff safety, critical infrastructure concerns, or a degradation of information technology capabilities. At this stage, typically 80% of the projects do not meet the FCC criteria and are reviewed through the historical asynchronous CMC process. The remaining 20% of projects are sent to a subject matter expert (SME) meeting, the second prescreening process, consisting of those individuals listed in Figure 2. The members of the SME meeting review the project and categorize operational risk categories as Low, Moderate, High, or Critical. There are clear instructions, with an intuitive methodology, depicted in Figure 2 as to how projects are categorized. Projects categorized with High or Critical operational impact by the SME meeting will continue to the FCC Council. These prevetting meetings are important to ensure only the necessary projects are reviewed at the FCC Council, since the organization values the time of clinical staff spent away from patient care.

The historical process alongside our new Facilities and Clinical Coordination process.

This risk matrix serves to help categorize projects based on assessed risk to the hospital mission which in turn helps practitioners determine which projects will be brought to the Facilities and Clinical Coordination Counsil.
In order to illustrate this process, we offer an example of a hospital’s need to replace a Fire Door. The FCC vetting process is flexible and guides the user through multiple questions regarding the project. These questions lead the user to explore the impacts to Patient Care, Quality Care, Patient/Staff Safety, and other measures important to the hospital, which are listed in Figure 2. The user will review the details of the project to include factors such as location (Is the Fire Door located within a patient care area?) and timing (Will the project be conducted during operational hours?). If, for example, the Fire Door replacement will occur in a strictly administrative/staff area of the hospital during nonoperational hours, it will not trigger the FCC process. In contrast, if the Fire Door replacement will occur within an Inpatient Area, which operates 24/7, it will trigger the FCC process because during project execution there would be major impacts to patient transport capability, emergency response times hindered due to trafficability around the project site, and other patient safety risk factors.
Once the project arrives at the FCC meeting, we used elements from the literature review to inform the best way to conduct an efficient meeting. Project overviews and information are provided to participants ahead of the meeting allowing for informed and thoughtful discussion. Disciplined leader engagement and expert facilitation synergistically provides psychological safety for the FCC members to voice opinions during the FM project review. These factors, coupled with timeliness in working through a standardized agenda, allow for a very efficient meeting and respect participants’ time.
The outcome of the FCC meeting are four possible decisions as depicted at the bottom right of Figure 1: approved, approved with contingency, disapproved needing an alternate plan, and disapproved needing more information. After a project is approved by the FCC, two critical events occur. First, prior to project execution, a strategic communication plan is developed and deployed through multiple modalities, including posting pamphlets in patient and staff areas for information diffusion and expectation management. Lastly, and arguably the most important, is the documentation of an after-action review (AAR) for the project, which is filed in the WRNMMC project management database. The FCC process is well suited for the healthcare environment because it provides organizations a predictable methodology to prioritize projects. The decision process ensures that only projects requiring cross-functional collaboration and a possible mission critical impact make it to the FCC Council.
Assessing the FCC Process
Method
FCC Council survey
A prospective written survey on a 5-point Likert-type scale (1 = strongly disagree, 5 = strongly agree) was used to measure the perception of FCC Council by participants. The survey and data analysis methodology mirrored the approach used by Pham et al. (2019). To control for recency bias, the survey was administered at the start of an FCC meeting (Offerman & Sonnemans, 2004).
Analysis and Results
The survey results were analyzed using descriptive statistics and independent t tests. We explored the relationships between participants’ staff type, work area, and whether or not they were in a leadership position prior to when the FCC was created. An α level of .05 was used as the threshold for statistical significance. All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS), Version 24 and Microsoft Excel 2013.
Table 1 highlights the demographic data of the 34 participants of the FCC meeting who were surveyed. The FCC is comprised of Military (56%), Government Service Civilians (32%), and Contractors (9%). Participants belonged to a variety of work areas: Administrative (59%), Facility Management (29%), and Clinical Care (12%). While 70% of the participants have been in their current position for less than 2 years, 65% of all participants have worked in the Military Healthcare System for over 10 years. The high turnover rate is not a striking finding within the military environment that moves active duty service members, on average, every 3 years. Lastly, almost half (44%) of the participants were at WRNMMC in a leadership role prior to the inception of the FCC Council.
Demographic Descriptive Statistics From the FCC Survey.

Note. FCC = Facilities and Clinical Coordination; GS = government service.
Table 2 shows participant perceptions of the FCC Council. The participants stated the primary benefit of the FCC is that it helps keep patient safety a focus within the organization (4.65 ± 0.54 on 5-point Likert-type scale). FCC members valued the F2F meeting verses the historical process of CMC (4.47 ± 0.79). The frequency of the meetings (weekly) was not found to be excessive, which is consistent with the previous literature (Lean Construction Institute 2015; Temel et al., 2019). Overall, the FCC was found not only to improve communication among all hospital staff regarding maintenance projects (4.52 ± 0.65) but was also perceived to be a good use of the attendee’s time (4.23 ± 0.56).
Mean Results With Standard Deviation From Each Survey Question.
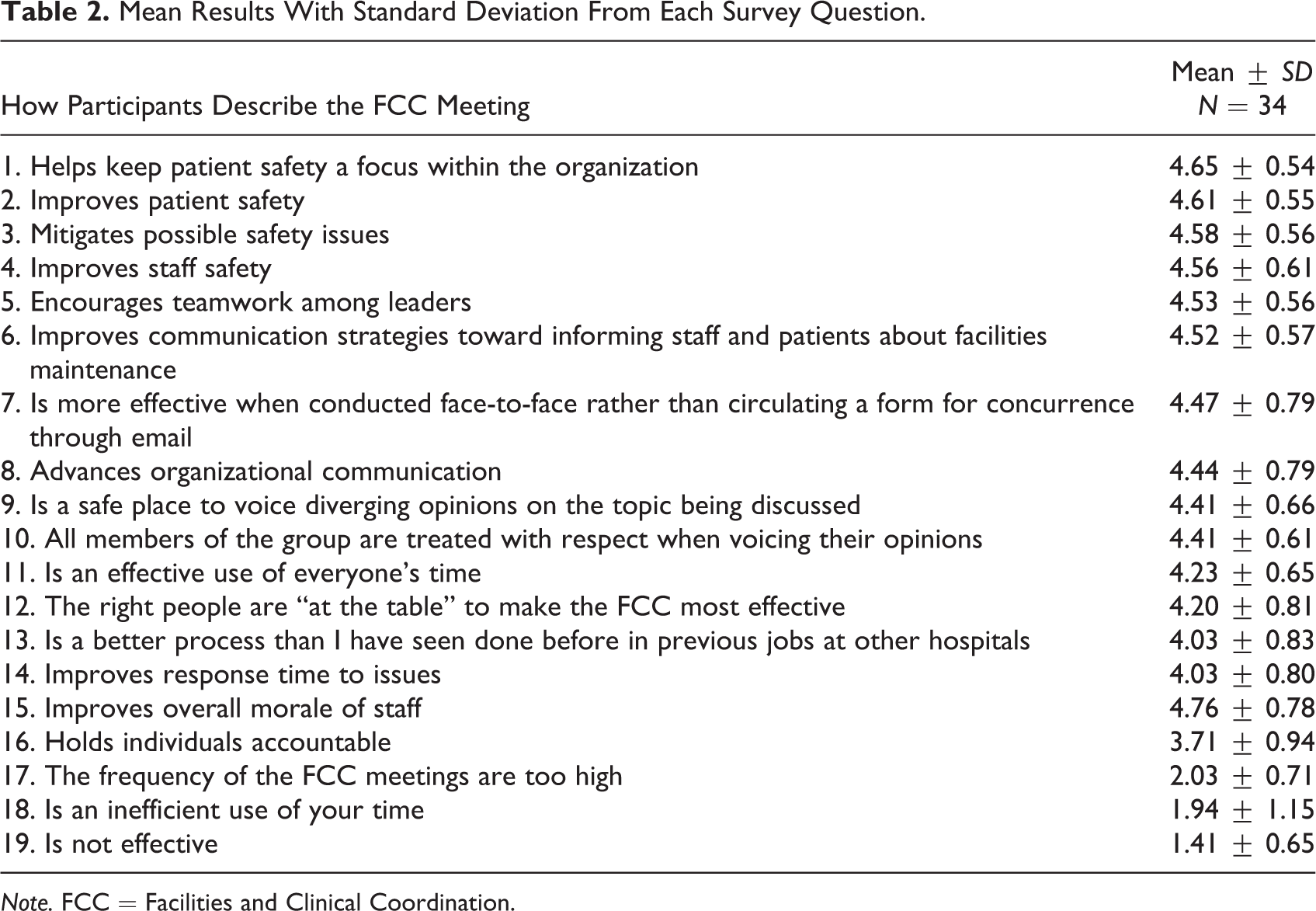
Note. FCC = Facilities and Clinical Coordination.
Table 3 illustrates the relationship between FCC Council subgroups with three key questions: (1) “Does the FCC help keep patient safety in focus within the organization?”, (2) “Is the FCC more effective when conducted F2F rather than via CMC methods?”, and (3) “Is the FCC an effective use of everyone’s time?”. There were no statistically significant differences between subgroups and their positive perception to the selected questions with the exception of one instance. While not statistically significant, All clinician participants found the FCC to help keep safety at the forefront of the organizational priorities (5.00 ± 0.00). Consistent with Reno et al. (2014), our research indicates clinicians prefer to be at F2F meetings, compared to asynchronous, because it allows them dedicated time away from patient care to think about the construction projects in detail, which avoids future environment of care issues during the project’s execution. The back-and-forth discussions also facilitate the prompt arrival of a shared understanding while considering multiple vantage points. Moreover, not only do clinicians want to be involved but also 98% of design industry professionals deemed user and clinical input vital to successful project outcomes (Keys et al., 2016). Intriguingly, our results suggest that contractors within our study perceived F2F moderately less effective than CMC as compared to the other subgroups (3.33 ± 1.15, p value = .01). We conducted a deeper review to define the contractor population and found that all who participated in the survey were managers within the facilities work area. A possible explanation for this finding comes from the fact that facilities managers spend tremendous time planning prior to the meeting and may feel as though their written analysis and thorough plans may negate the meeting’s necessity. This thought is further supported in our results, considering the contractors also scored the effectiveness of the FCC Council, in respect of participants’ time, lower than the other staff types.
Relationship Between the Mean Responses of Three Select Questions Between Specified FCC Participant Subgroups to Demonstrate Their Sentiment Toward the FCC Process.
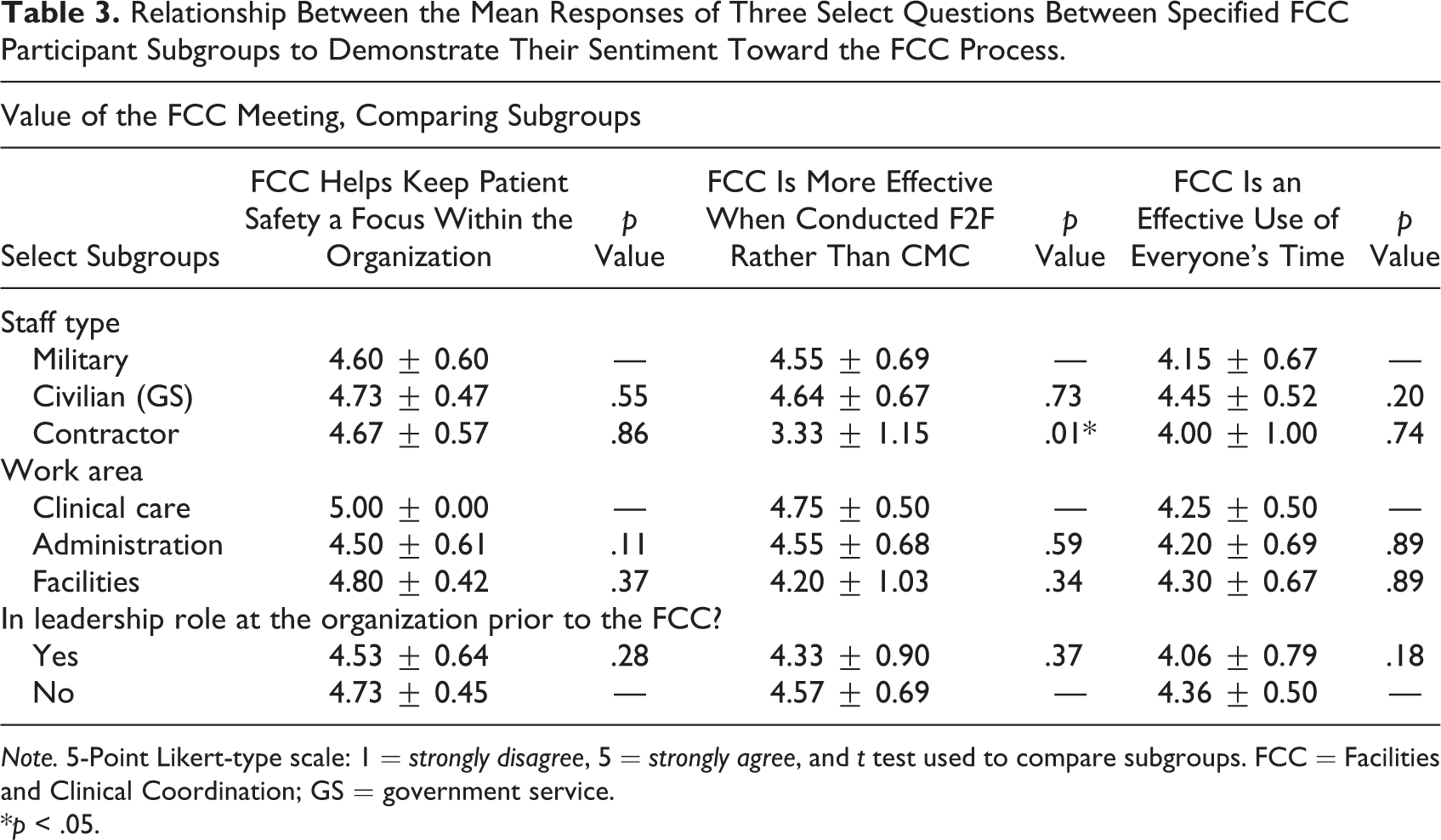
Note. 5-Point Likert-type scale: 1 = strongly disagree, 5 = strongly agree, and t test used to compare subgroups. FCC = Facilities and Clinical Coordination; GS = government service.
*p < .05.
Limitations and Future Research
This case study has two primary limitations in regard to generalizability to other institutions. First, our work focused on a facility type consisting of a unique culture compared to the civilian healthcare system. Military members are acclimated to consistently changing work conditions, which could skew the perception of the FCC’s efficacy after changing from a CMC to an F2F meeting structure (Galvin & Allen, 2019). We hope our process would be considered at other healthcare institutions, then examined for its effectiveness. Second, we were limited in our ability to conduct meaningful comparisons among participant types due to a relatively small sample size. Future studies might consider pooling participant data in order to examine differences, conducting focus interviews, or examining the process over a longer period.
There are three main opportunities for future research. First, our process guides the organization through determining which projects benefit the most from FCC Council review. Considering an estimated 80% of projects will be processed through the historical asynchronous process, future research should focus on opportunities to optimize the historical approach. Second, we suggest future studies build upon quantitative methods of determining process effectiveness. It would be best to design a study exploring pre- and post-implementation utilizing our sentiment measures with the BREI and combine these with patient and staff safety as well as quality data (Joshi et al., 2020). Finally, in the current COVID-19 environment, virtual synchronous F2F methods have grown, allowing organizations to benefit from using technology to bring dispersed team members together while not losing the important communication elements found in F2F meetings. Future research should focus on the impact of the increasing prevalence of these new methods of communicating on the FCC process.
Conclusion
Our study supports and builds upon the body of evidence surrounding utilization of lean concepts, such as the Big Room concept, in facilities management. Our results provide a preliminary framework that appears to indicate the FCC process achieves perceptions of higher patient and staff safety. The FCC methodology is a programmatic way of (1) reviewing project details, (2) exploiting those details for known and unknown impacts to clinical and administrative operations, and (3) planning mitigations and communication cycles for maintaining safe, high-quality healthcare facilities. Our favorable survey results, among a very diverse set of healthcare professionals, provide some evidence for organizations to consider when deciding to adopt the FCC Council model within their facilities management and maintenance process. Based on the WRNMMC experience, the FCC process is a realistic solution that can be applied quickly within a healthcare facility.
Implications for Practice
The use of a Facilities and Clinical Coordination (FCC) Council comprised of both administrative and clinical personnel could enhance communication among the medical center workforce and increase stakeholder buy-in for the inconveniences that accompany major facility renovations.
The FCC could reduce mission impacts associated with major facility renovation and reduce negative interference with clinical operations.
The FCC could improve compliance with hospital accreditation requirements pertaining to facility maintenance and contribute to an overall safer construction environment.
The FCC could reduce nonforecasted expenses due to postconstruction change orders.
Footnotes
Authors’ Note
The views expressed in this article are those of the authors and do not necessarily reflect the official policy of the Department of the Army, Department of Defense, or U.S. Government.
Acknowledgments
The authors would like to acknowledge Dylan Hartsfield for his help in proofing and preparing the final manuscript for submission. Also, they appreciate Erin Palmer and William Lewis for their assistance in reviewing the article. Finally, they thank Mike Werner and Terri Lavoie for their work in helping develop the Facilities and Clinical Coordination process.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.