
Abstract
Objective:
To describe the planning, development, and implementation of a structured video-based observational method that can be used to systematically examine and model the role of the physical environment within healthcare systems.
Background:
Direct observation methods are often used in healthcare to study complex healthcare systems. However, these observations often occur in real time, which predisposes the collected data to shortcomings such as time lags in recording of activities, overlooking events, or limiting the scope of information than can be collected. Video observation approaches eliminate many of these challenges and provide opportunities for researchers to understand and model the role of the physical environment.
Methods:
An approach to developing and implementing a structured video-based observational method to study and model complex health systems is presented.
Results:
A structured observational approach can be highly effective for collecting multiple layers of data necessary for understanding interactions between the physical environment and other systems components in healthcare settings. The proposed video-based observation method is effective in settings that have clearly defined environmental boundaries, limited number of people, are complex and fast-paced such as the OR, ED trauma rooms, and ICU rooms.
Conclusions:
Video-based observation is an effective complement to the traditional observational method for in-depth study of the built environment in health systems, enabling researchers to employ quantitative approaches to data collection and analysis, in addition to qualitative interpretations.
Healthcare environments are complex systems comprised of dynamically interacting components including people, the tools and technology they interact with, the physical environment of care, and the tasks performed by different people in the systems (Carayon et al., 2006). Understanding and modeling these complex systems is critical to identifying safety risks and developing effective and sustainable design solutions. Direct observation is a powerful research method for the direct study of behaviors, patterns, and collection of facts related to human–system interactions and is often used in conjunction with other approaches such as interviews and surveys that allow researchers to triangulate data from different sources (Carthey, 2003; Catchpole et al., 2017). Observational approaches are extremely valuable in understanding “work as done” (what really happens) in healthcare settings versus “work as imagined” (what designers, administrators, managers believe happens or should happen and often becomes the basis for the design of facilities, technology, and policies; Catchpole et al., 2017). While behavioral observation methods are used extensively in health services research as well as in environmental design research, the use of behavioral observation methods, especially video-based observation, to study the interactions between clinical work systems and the physical environment is not as clearly described. The purpose of this study is to describe a video-based observation method to study the role of the physical environment as part of complex clinical work systems.
An observational method traditionally used in the field of environmental design is behavior mapping, where descriptions of observed behavior are located spatially on a floor plan or other spatial representation (Ittelson et al., 1970). Behavior mapping often requires an observer to shadow a subject, keep a record of their behavior over time, and draw their path of travel on a map or a floor plan. The process of conducting a behavior mapping study includes determining the number of subjects under study; the intended activities or behaviors aligned with the goal of the study; the path, location, or space under study; and the amount of time spent on each activity and in each location. Data collection may occur by one observer or multiple observers. While several studies have used behavior mapping to understand the behavior of individuals in different settings, there are fewer instances of this approach being used in healthcare.
Observational methods are frequently used in healthcare for research, quality improvement, and training purposes (Bezemer et al., 2017). However, observations of healthcare settings are usually conducted in real-time and in-person, which predisposes the collected data to shortcomings such as time lags in recording of activities, overlooking events, or limiting the scope of information that can be collected (Asan & Montague, 2014; Bezemer et al., 2017). Due to the complexity of healthcare settings, some observational studies benefit from a more rigorous and systematic approach to account for simultaneous events and processes as well as interaction between different system components. This is particularly true in complex, high-tempo patient-care environments such as operating rooms (ORs) where multiple team members interact with each other, the patient, equipment, technology, and the workspace over the duration of the surgery (Joseph et al., 2017). Given the limitations of traditional in-person observational methods, various researchers are increasingly favoring alternative approaches such as observing video recordings. Observation of video recordings, like other observational methods, is applicable to different disciplines and allows collection of both qualitative and quantitative data (Andersen & Nielsen, 2013; Basil, 2011)
Using video recordings for observations reduces limitations associated with traditional in-person observations as it allows researchers to replay scenes as often as needed to capture information accurately (Basil, 2011; Bezemer et al., 2017). Additionally, videos, as opposed to other visual data such as photos, provide a more dynamic and self-explanatory type of data that can eliminate the need for field notes and allow immediate content analysis. Finally, video observation allows for time control and the accurate observation of scenes that observers may otherwise overlook when conducting traditional observations (Basil, 2011). Although widely used in various fields, there is little known regarding the application of video observations in the study of the healthcare physical environment. The purpose of this article is to describe a structured video-based observation approach for behavior mapping in the context of studying complex healthcare work systems. The approach described in this article is based on insights gathered by the authors while developing and conducting multiple video-based observational studies, most notably a multiyear study on ORs (Allison et al., 2021). This article is organized into different sections that describe the steps taken to conduct a video-based observational study focused on understanding and modeling complex work systems—defining the scope, video recording logistics, developing a coding scheme and observation protocol, analytical and modeling approaches.
Defining the Scope
Spatial Boundaries
Video-based observations of clinical work systems are highly effective for collecting data on behaviors of individuals in a well-defined and relatively small space. If the goal of the study is primarily to understand behaviors that take place within a geographically well-defined space (e.g. OR, patient room), then stationary video cameras can be set up to record activities within the space. Once the space becomes too large (e.g., a nursing unit), video cameras may not be able to effectively capture all areas within the defined space, and views may be obstructed by partitions or walls. This approach is also not recommended if researchers are interested in including behaviors and interactions that take place outside the scope of the video cameras. For example, in a study conducted on ORs, the researchers were unable to observe and understand the activities of surgical team members when they left the room during the surgery.
Number of Subjects
This approach is most effective when there is a limited cast of characters within the observational area during the study. In clinical environments with a large number of individuals and equipment moving in and out of the space, researchers may find it challenging to observe and code all individuals accurately.
Legal and Ethical Considerations
Similar to any study involving human subjects, institutional review board approval must be obtained from the health system where observations are being conducted. Informed consent must also be obtained from individuals included in the observations. While video observation has many advantages, in that it is less intrusive and disruptive to clinical workflows, medicolegal implications may be more challenging to navigate (Asan & Montague, 2014). Most organizations have policies related to filming in clinical areas, but if there are no existing organizational policies, these will need to be carefully navigated. In particular, should an adverse patient safety event or near miss event occur, while the videos will enhance the analysis and learning from an event, they may also be legally discoverable, and thus potential evidence in subsequent litigation. However, at this time, there are no precedents of video research data being used in medicolegal proceedings. Research teams are advised to examine and evaluate existing policies within organizations and to have early and frank discussions with senior legal and risk administrators about any deviations (Asan & Montague, 2014). Additionally, certificates of confidentiality that protect the data from being released in the case of forced disclosure as part of a lawsuit may help in overcoming concerns about confidentiality.
In the OR study, all clinicians (surgeons, anesthesia providers, and nurses) and patients provided consent for the video recording of the surgeries. Surgical procedures usually have a small set of team members involved, and entry of individuals who are not associated with the procedure into the OR is often strongly discouraged. This makes it easier to obtain informed consent in an OR environment. Obtaining informed consent for video-based observations can be challenging in open clinical environments with many individuals moving in and out of the space. There will also need to be an agreed approach if someone who has not given consent becomes part of the video data or if individuals subsequently decide to withdraw. This could require the deletion of all video data featuring those individuals but might also be fulfilled with post hoc editing of the video to remove those sections in which the individuals appear. Conversely, some healthcare organizations record videos in care areas as a matter of course, which makes this process considerably easier to navigate.
Video Recording Logistics and Setup
Equipment Setup
In healthcare design research, in order to minimize interruptions to clinical workflows and to reduce perceptions of being observed, it is necessary to deploy cameras in a manner such that the natural flow of activities is not interrupted or obstructed. Cameras should be installed to capture a wide-angle perspective of the field under study, though there may be a trade-off between capturing the whole scene (such as the entire operating team) or the detail of one area (such as the surgical field or the anesthesiology monitors). High-definition cameras and careful placement can address these issues within the study objectives. Since understanding interactions with the physical environment is important in healthcare design studies, cameras must be positioned to maximize views of all spaces, people, and equipment such that key research questions can be effectively addressed. For example, in our OR study, four video cameras were mounted on poles in the four corners of the rooms so that the cameras were unobtrusive, out of the path of movement of clinicians and equipment, and enabled views of most objects, people, and surfaces in the room (Joseph, Neyens, et al., 2021; Mousavi et al., 2018; Neyens et al., 2018).
Selection of Equipment and Software
Video cameras and recording equipment should be carefully selected to support research activities. Many studies will benefit from the synchronization of video data from multiple cameras to enable multiple views of the same activity, so that multiple concurrent activities can be viewed and coded. In our OR study, the four video cameras were connected via wires that ran along the walls to a single laptop computer and controlled using software (Noldus Media Recorder) to synchronize the videos. Audio recording equipment was wireless and synced with the computer. In this setup, a researcher sets up the recording by assigning a unique session code to the observation and using a single button press to initiate and complete the video and audio recording. Other studies have used tablets (such as iPads; Joseph, Joshi, et al., 2021) and GoPro cameras (Joseph, Chalil Madathil, et al., 2021) to collect unsynchronized videos, which would then need to be edited and synchronized postrecording so that concurrent activities can be viewed simultaneously during coding. The options available for synchronous video recording are expanding significantly, and researchers should explore options for video recording equipment that meet their needs and budget.
Security of Equipment
Safety measures and precautions should be undertaken to ensure the secure installation of the cameras such that the equipment is not dislodged due to people or movable medical equipment such as booms, tables, or carts bumping into the camera apparatus. There may sometimes be concerns related to security of recording equipment after hours or when the facility is unoccupied. Protocols may need to be created to dismantle and store expensive equipment at the end of the day and to reinstall and recalibrate everything correctly before the start of the next set of observations. A researcher or coordinator located at the study site should be assigned to perform this task for the duration of the observations. In the OR study, the team was able to leave the poles and cameras in place at the end of the day. However, a research coordinator disconnected the laptop computer and stored it in a safe location at the end of each day of video recording.
Recording Video Observations
Once the video cameras are installed, the research team should test multiple viewing angles to ensure that the best (and least obstructed) views are obtained. The team should also pilot test a few observations to ensure that all video cameras and audio recorders are functioning properly and that the recorded videos are high quality and will allow observers to see all parts of the space clearly. The team should create a protocol that clearly defines the on-site video data collection process. This would include clear written instructions defining when a recording should start and stop. For example, in the OR study, we were interested in observing all behaviors that took place between patient entry into the room and the turnaround (cleaning and setup) of the room for the next patient. The research coordinator tracked the OR schedule and progress of individual procedures and ensured that they were available to start and stop recordings from the laptop computer. Other types of video recording equipment might need a different protocol for starting and stopping recordings. The research coordinator was also responsible for ensuring that all equipment was properly charged at the end of the day. The videos collected were stored locally on the computer using a unique identifier and then transferred to a secure shared storage location for access by the research team.
Coding Scheme and Observation Protocol
The coding scheme is the most critical part of any structured observation study and should be aligned with the study research questions. For example, the OR study focused on understanding how the design of the OR work system might contribute to safety. To understand the work system, the team focused on broad categories of tasks performed by different team members (defined by role), the location of these activities, and the impact of workflow disruptions on the activities of surgical team members. The team was also interested in understanding door opening behaviors (e.g., how often these took place, which doors were opened) since frequent OR door openings impact workflow and create interruptions (Mousavi et al., 2018). These research questions were informed by an in-depth literature review (Joseph et al., 2017). Further, we conducted several in-person observations in the OR to better understand the context. In-person observations were particularly helpful in validating the behavioral and environmental elements of interest and identifying any unforeseen elements that should also be considered. The coding scheme was thus developed based on the literature review, in-person observations, as well as building on existing taxonomies for studying characteristics of disruptions in the OR. The coding scheme should be supported by an observation training protocol or manual that details out all the steps involved in coding process as well as all codes, their simple definitions, and detailed descriptions such that coders have a reference document to support the coding process.
Coding Scheme
Healthcare design research studies will often focus on the utilization of the physical space by different team members for different activities. Thus, in addition to clearly identifying the study subjects, the coding scheme might include codes related to the physical environment and activities. Additionally, depending on the research questions, other elements could be included into the protocol, such as door openings, flow disruptions, the use of certain equipment, or other types of behaviors of interest.
Subjects
In any observational study, the research team needs to clearly identify both the individual subjects being observed and those who will not be observed. Some studies may also track the movement/placement of inanimate objects during the observation (e.g., movement and placement of trash cans during the surgery). In the OR, the number of personnel can vary greatly depending on the type of surgery and the type of facility. However, four main categories of personnel were identified in the OR study—anesthesia providers, circulating nurses, scrub nurses, and surgeons. These individuals were usually identifiable based on their location and activities in the OR. However, when the role of the subject was not clear, research team members with clinical backgrounds were consulted to confirm subject roles. The coders added descriptors to subjects (e.g., red cap) at the outset of coding so that subjects were easily identifiable to different coders.
Physical environment
Understanding the layout of a clinical space, its utilization for different functions, and potential challenges associated with different areas within the clinical space are important goals for a healthcare design research study. Areas or zones within a room can be defined by the activities occurring in them. The function of an area refers to the types of tasks that need to occur in that particular area. For example, the anesthesia providers in the OR usually work in a well-defined space at the head of the patient with specific anesthesia equipment. Other areas may be primarily used for circulation and may not have a defined function associated with an individual team member. Thus, a clinical space such as an OR or patient room can be roughly organized into these functional zones in plan for the purpose of mapping behaviors. For example, in the OR study, work zones (e.g., “Anesthesia zone,” “Circulating Nurse work zone,” and “Surgeons’ Workstation”) were identified because of their consistent utilization by a specific type of staff member, whereas supply areas and support areas were so named for their function of providing in-room storage of surgical supplies and surgical furniture/equipment, respectively. When multiple zones of one type are present or if the zone is large and the researcher wants to understand movements to different parts of this zone, the zone can be designated by number so that they are easy to differentiate while coding (e.g., Supply Zones 1 and 2; Support Zones 1, 2, 3, 4, and 5 in the OR study). Similarly, other functional and transitional zones should be clearly defined and designated so that all spaces within the setting are accounted for within one zone or another. Figure 1 shows the “location map” created as part of the coding protocol for the OR study with the location of different zones. In this study, once the definition of zones was determined by the research team, similar location maps were created for all ORs included in the study such that all observations could be coded in a consistent manner.
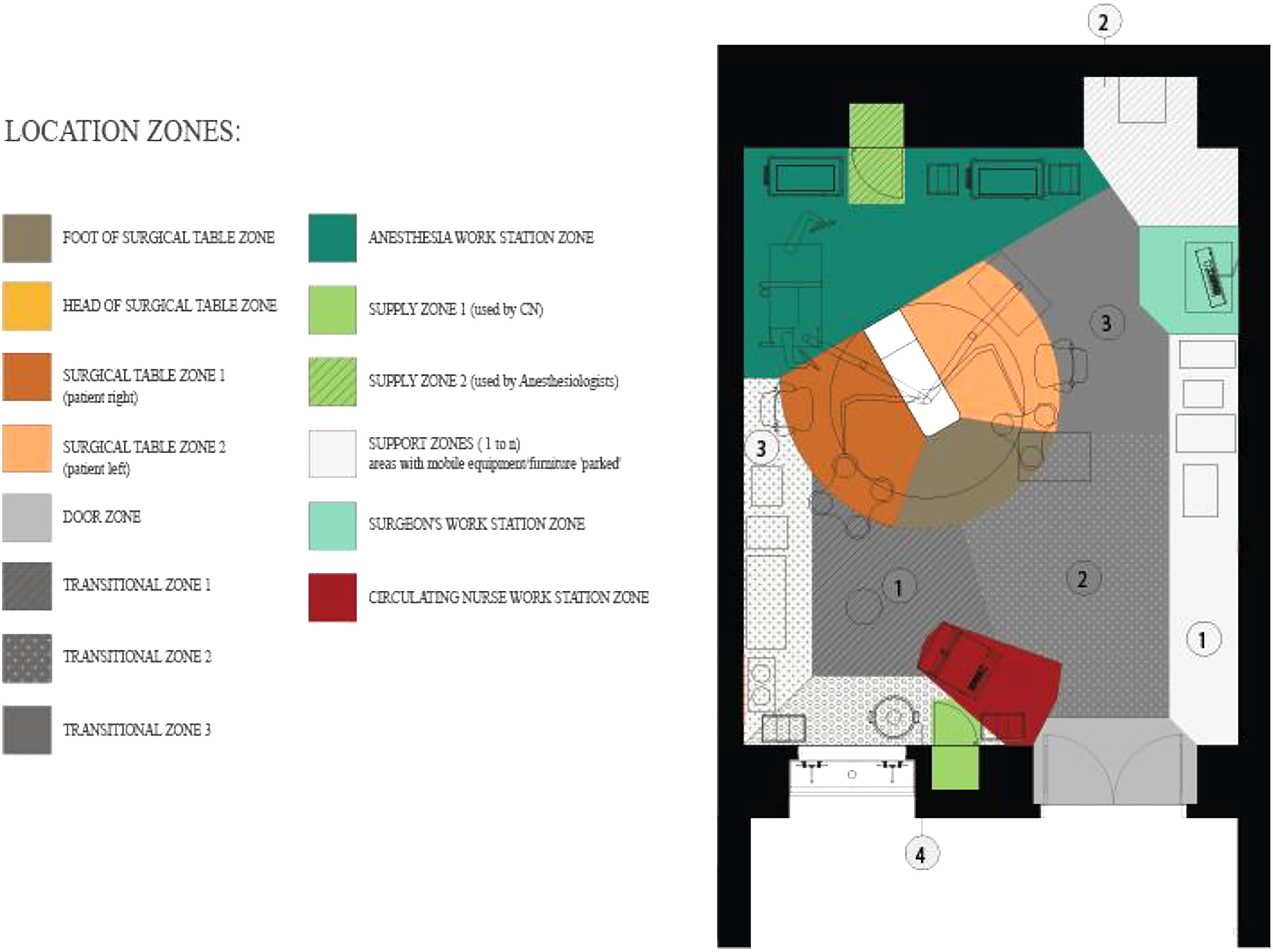
Sample location map.
Key activities/behaviors of interest
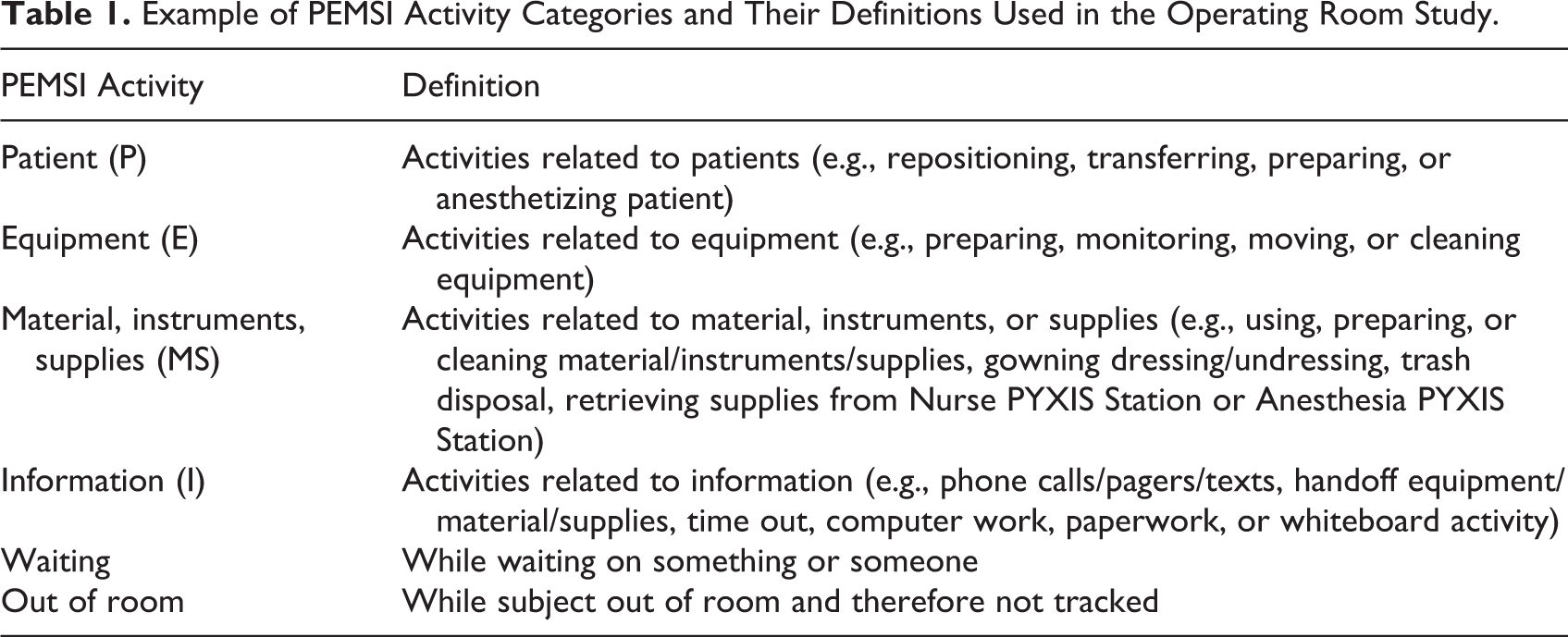
Many observational healthcare design research studies focus on understanding the relationship between physical environment characteristics and activities or behaviors of team members in the space. The behaviors or activities selected for coding are usually determined by the study research questions or study objectives. For example, a protocol for a study focused on nurse–patient interactions in the patient room may involve detailed coding of the many different interactions between patient and nurse (e.g., talking, lifting, checking vitals). In the OR, team members engage in a range of different activities depending on their role. For the purpose of simplifying the coding process and ensuring that coders could easily interpret and code activities based on observation, four broad categories of activities were created—those related to patients; equipment; material, instrument; and supplies; and information (PEMSI; Joseph et al., 2019). We further defined subcategories (modifiers) for each main category of behavior. PEMSI activities and associated modifiers were coded exclusively and sequentially. The coding of activities was associated with each subject (e.g., circulating nurse, surgeon), and the type and duration of the activity was recorded from the inception of the activity to the end of the activity by coding “start” and “stop” in the Noldus Observer XT coding scheme. Some activities are momentary, while others are longer in duration, and the coding platform can be set up to capture these different types of activities. In addition to PEMSI activities, we defined actions peripheral to the surgical process, such as “waiting,” “idle” (waiting without any identifiable reason). The actions that were not identifiable by coders were categorized into “out of room,” “obstructed view,” and “other.” At any point in time, every subject was coded as performing one of the activity categories and was coded as being located in a specific zone (or out of room). A list of PEMSI codes and related definitions used in the OR study are shown in Table 1.
Example of PEMSI Activity Categories and Their Definitions Used in the Operating Room Study.
Observation Protocol
Coding template
Once all key observation categories (e.g., behaviors, locations, disruptions) and all the codes (e.g., PEMSI) within those categories have been clearly defined within the coding scheme, the next step is to develop a coding template for coding the recorded videos. If the codes are relatively simple, researchers could use a simple excel spreadsheet for tracking behaviors as they occur. However, if multiple subjects and multiple different types of behaviors are being tracked (like in the OR study), software platforms specifically designed to support behavior observations might be more appropriate (e.g., Noldus Observer XT, Noldus, 2020, observation software). This type of software has been used in numerous studies (Bezemer et al., 2017; Joseph, Chalil Madathil, et al., 2021; Quan et al., 2016; Zadeh et al., 2014) and is useful when coding video-based data. In the OR study, the observers/coders recorded the locations and PEMSI activities for all subjects. Given the complexity of the codes used in this study, coders recorded location data, activity data, and flow disruption data separately for each individual video recording. This allows quicker coding times because the coders are not having to consider multiple types (e.g., location, activity) of codes simultaneously. Figure 2 shows an example of a coding scheme developed in Noldus Observer XT for the OR study. Figure 3 shows the coding interface in Noldus Observer XT where multiple synchronized videos can be viewed simultaneously while coding at the same time. Coders are able to toggle between different videos to track the subjects as they move about the room.
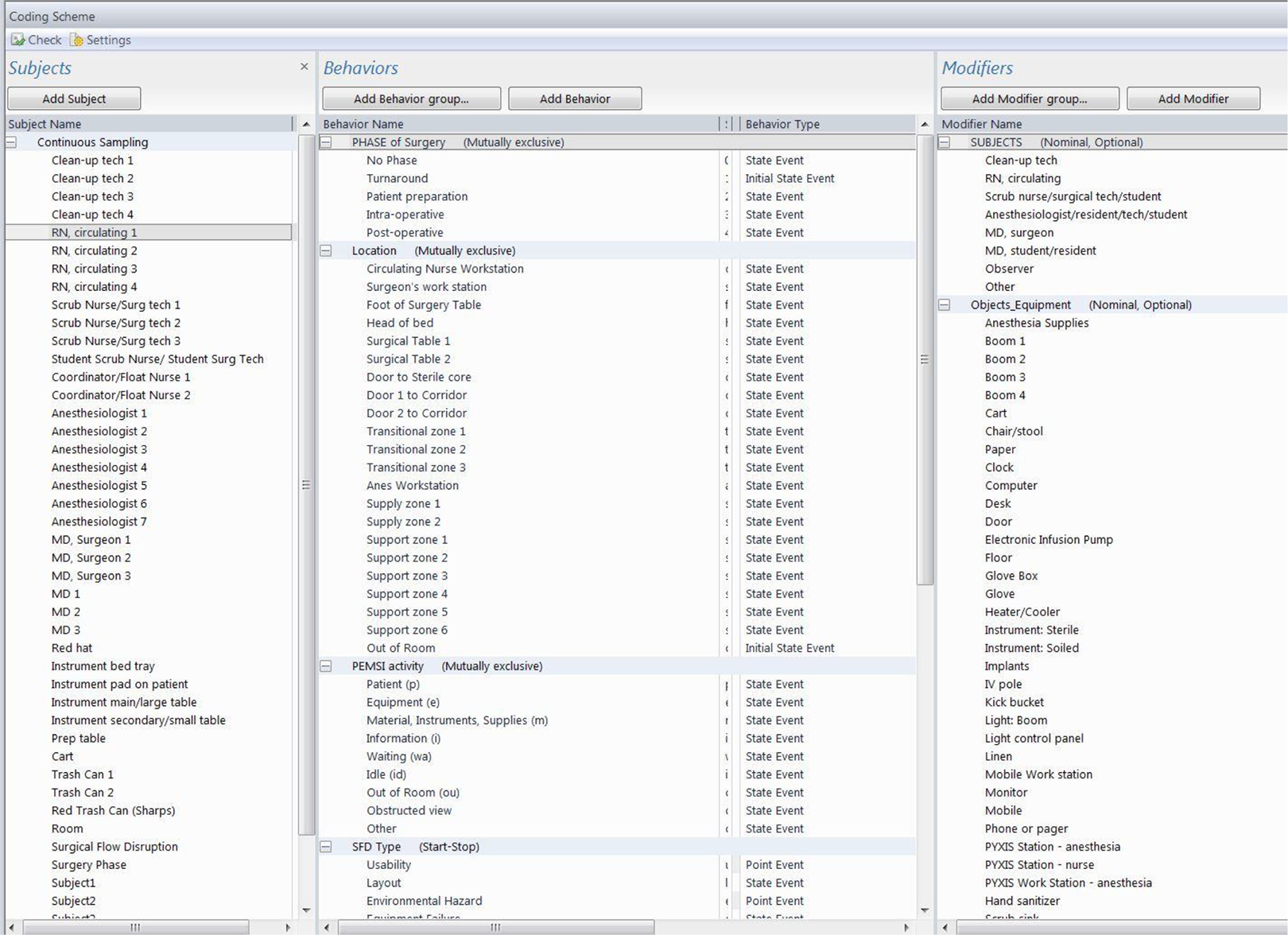
Coding scheme for the operating room study in Noldus Observer XT.

Coding interface for the operating room study in Noldus Observer XT.
Coder training and training manual
The success of an observational study rests on well-trained and reliable observers. The training process involves clearly communicating the study purpose and describing the setting being observed, the roles of the subjects under observation, and the types of equipment, activities, and behaviors that coders are asked to observe. A training protocol or manual that incorporates the basic study information along with the steps in the coding process, all codes, definitions, and detailed descriptions is also recommended for a successful structured video observation study.
In the OR study, we conducted this training in different stages. During the first stage, research team leaders presented the overall goals of the project; an overview of key human factors issues, and challenges in the OR; and an introduction to the settings, subjects, equipment, and behaviors that coders would observe. During the second session, coders were trained regarding the coding process itself, which included an introduction to the software interface and the steps that would be necessary to initiate a coding session, how they would conduct the coding and save observations in a shared networked drive. All coders were given a set of “test” videos to code and were asked to identify any challenges with the process, the codes, and the descriptions provided in the protocol for recognizing different codes while viewing the videos. Based on the input from this phase, the coding template and protocol document were refined. The coders then pilot tested the coding process for a set of three videos. Inter-coder agreement (the extent to which different coders were consistent in coding a certain code) was calculated using the inbuilt inter-coding reliability metric (index of concordance) in Noldus Observer XT. Index of concordance values higher than 0.8 were deemed as acceptable. In cases, where values were lower than 0.8, discussion sessions were held to examine the areas of disagreement and develop consensus on the interpretation of the codes. This was followed by a second round of inter-coder reliability testing to ensure that consistency across coders was higher than 0.8. Codes that were less reliable were either removed or refined to ensure greater understanding by all coders. The training manual was updated to reflect any changes to the process or codes.
Once coders are trained and a process and time line are established for coding the videos, the team can commence coding all the videos. While video observation allows for replaying the same scene multiple times to accurately understand and record data, it can also be time consuming. The time taken to complete the coding process will depend on the complexity of the codes, length of the videos, and the number of well-trained coders available.
Data Analysis and Modeling
Data Analysis
The coding of the behaviors and their modifiers for each individual and entity in the video coding process in Noldus Observer XT results in a data structure that is based on the occurrences of events or behaviors. These event-based data are useful to quantify the frequency of individual events, but it is difficult to quantify the co-occurrences or the complex interaction of a series of different behaviors or events. In order to examine the timing and co-occurrences of events and disruptions, it is useful to convert the data from an event-based data format (as obtained from Observer XT) into time-based data. In the OR study, the event-based data were transformed into the time-based data using a program written in R (R Core Team, 2017) for each individual and entity coded in the event-based data. This transformation resulted in second-by-second data that mapped all of the individuals’ location, behaviors, and modifiers across each surgery video. That is, the data identified where the individuals were located and what they were doing across the surgical case. We could then identify the frequency of when two individuals were in close proximity, when and where they performed specific tasks, and what everyone was doing when a surgical flow disruption occurred. The transformed data allowed for statistical analysis and evaluating complex research questions (Bayramzadeh et al., 2018; Joseph et al., 2019; Neyens et al., 2018). For example, in Bayramzadeh et al. (2018), we are able to map sequences of tasks and locations to identify the specific associations with flow disruptions by utilizing the time-based data. The time-based data framework allowed connections between the individuals, tasks (behaviors), and tools (as modifiers in our data) and locations within the environment to facilitate systems analysis of the sociotechnical work system within the OR.
Modeling and Visualizing Work Systems
The time-based data set obtained from an in-depth structured video observation study, such as the one conducted as part of our OR project, can be extensive. This data set can not only be used to conduct complex data analysis but can also help in visualizing and modeling work systems. Coding location, time spent at a location (dwell time), and movement information provide a rich data source for visualizing how individuals interact with their environment in a more realistic setting. In the OR study, we used an agent-based computer simulation model (Khoshkenar et al., 2017) that enabled this visualization. First, a playback model was developed using simulation software to visualize movements of staff while adhering to dwell times and departure times from zone locations previously recorded. The model used the data to simulate the movement between zones, capturing data that could be used to assess the flow of individual OR staff (Bayramzadeh et al., 2018; Joseph et al., 2019; Joseph, Neyens, et al., 2021; Neyens et al., 2018). Through a social movement algorithm, interdependencies that accounted for collision avoidance were used to show how individuals are forced to walk around other staff members or objects in the OR. Another feature of the data set is the ability to create density or heat maps that illustrate the frequency of trips into a zone or the amount of time spent in a specific zone within the OR (see Figures 4 and 5). Such data can be captured dynamically during the simulation to show how activity changes during the course of an observation.
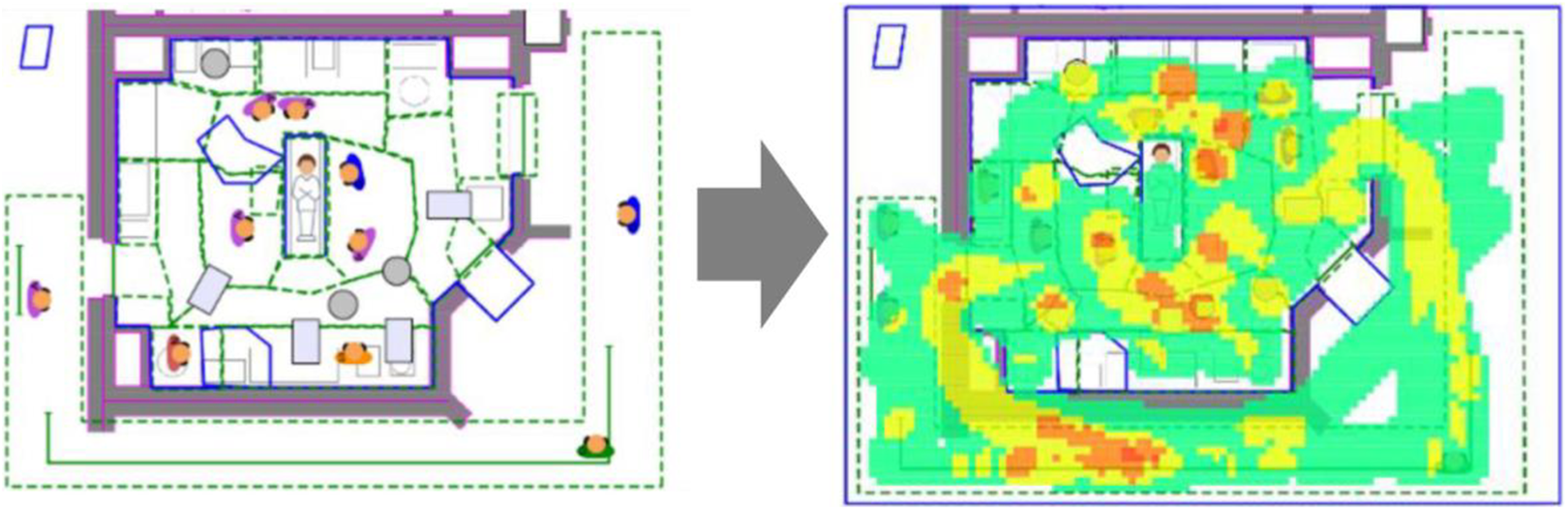
Animated computer simulation model (left: snapshot during intra-operative phase; right: heat map displaying density of activity).
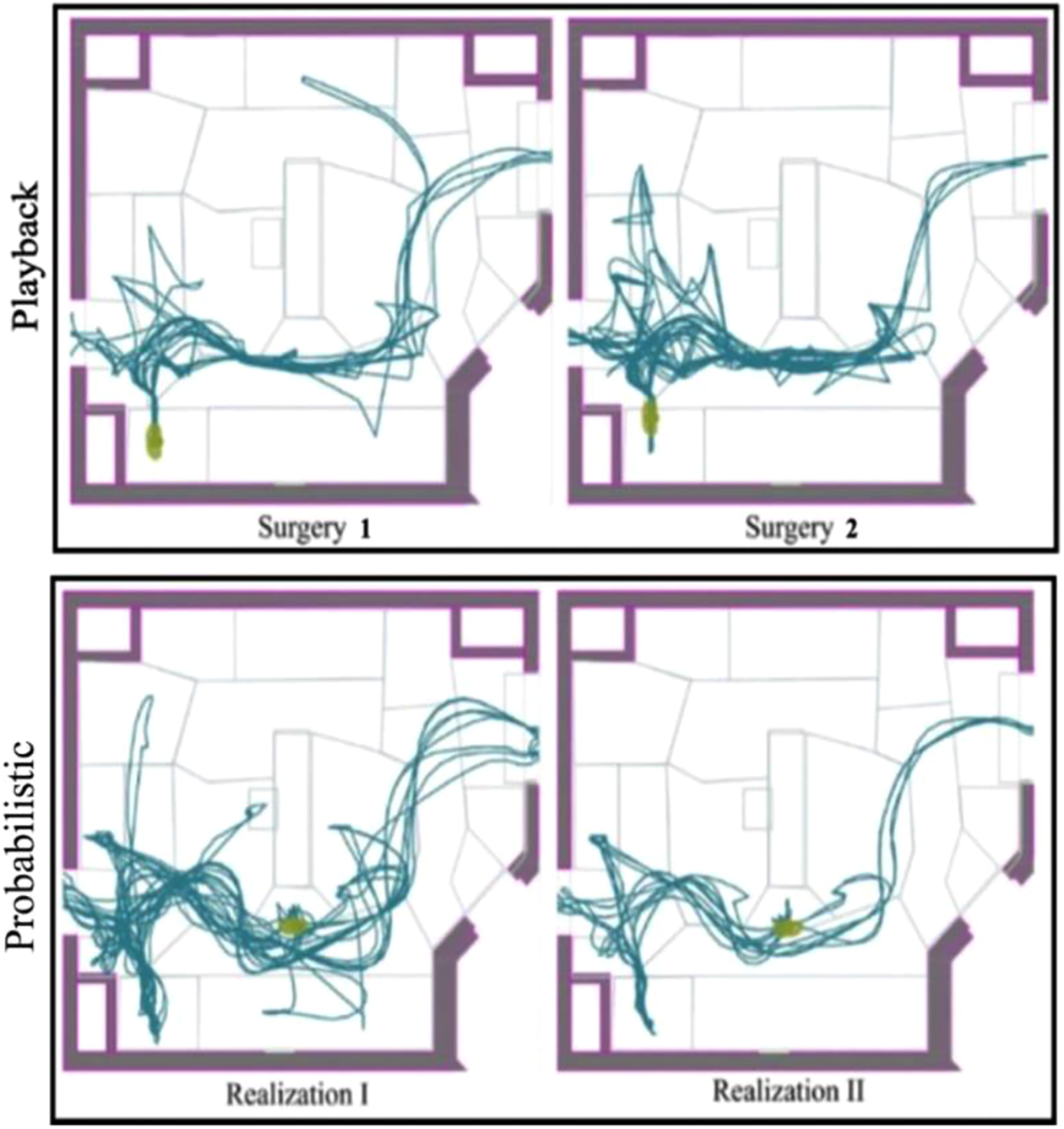
The movement patterns of a circulating nurse in both playback and probabilistic models.
In addition to visualizing behaviors and interactions in multiple ways (e.g., heat maps, spaghetti diagrams) on a floor plan, this extensive data set can be helpful in proactively testing performance of proposed layouts. Taaffe et al. (2021) developed performance metrics for assessing OR movement and congestion and used a generalized modeling framework that could be used to test performance across a variety of room layouts and procedure types. In the OR study, we used this proactive simulation modeling approach to evaluate design configurations that differed by size, shape, and orientation of the surgical table (Taaffe et al., 2021).
Discussion
This article describes a unique video observational method that can be used to study and model the role of the physical environment within healthcare work systems. While several published studies describe how video observation can be used for research, quality improvement, and training in healthcare, to our knowledge, this is the first article to describe how this approach can be used to study the role of the physical environment as part of a more complex clinical work system. The approach described in this article allows researchers to collect multiple layers of data by coding the same video repeatedly. For example, in the OR study, we were able to obtain exhaustive data on the location of each individual subject and their activities, flow disruptions experienced by team members and the nature of those disruptions (e.g., location of disruption, severity of disruption, people involved), and door openings during each observation. The time-based data set obtained using this structured video observation method can be extensive and provides a range of information about concurrent events for each second of the observation. The combined data set obtained from multiple observations can be analyzed and modeled in many different ways to address a number of different research questions that allow researchers to understand and visualize complex system interactions. Further, this approach also allows for new layers of data to be added over time, provided that the videos collected as part of the original study enable exploration of new research questions, and that the subjects have given permission for secondary data analysis of the recorded videos.
Clearly, the structured video observational method addresses many of the challenges experienced in the field related to observer fatigue, delays in recording information, and inability to record multiple streams of information or activities simultaneously. Further, this method addresses the challenges associated with accommodating multiple observers in crowded healthcare settings. The COVID-19 pandemic has further highlighted the need to develop a less intrusive data collection approach in healthcare settings. While video observation methods have the potential to significantly enhance our understanding of complex healthcare settings, researchers have to be cognizant of the medicolegal implications of video-recording behaviors in clinical settings. Challenges can be overcome through effective communication with administrators and clinical teams about the intent of the study. The success of a structured observation study depends on careful and thoughtful planning during all stages of the study. Multiple rounds of pilot testing are highly advisable to ensure that high quality and usable video data are collected. Similarly, it is critical to develop detailed training manuals and to pilot test the coding scheme and process with observers to ensure consistent and reliable coding across multiple coders.
Although video-based observation enables researchers to record events and behaviors more accurately, it poses several limitations. Since videos are reviewed at a later time, it is often not possible to cross-check interpretation of events with those observed. In some cases, views may be obstructed due to the camera viewing angle or obstructions. Sight lines, the trade-off between wide-angle and detailed task-focus, lighting conditions in the OR, and audio issues need to be carefully considered, but all are resolvable with a thorough approach to equipment selection, study design, and pilot testing. While this approach yields a rich data set, video coding multiple layers of data is a time-consuming process, and research teams should budget for adequate time and resources should they decide to undertake this method.
Conclusion
Video-based observation is a valuable method of data collection compared to interviews, surveys, and other means of self-report, which rely on subjective and memory-based feedback of subjects. Videos provide an opportunity for careful examination of “work as done” by replaying recorded events as needed to observe key behavior and the impacts of the physical environment on these behaviors.
Implications for Practice
This study provides a practical approach to developing and conducting a video observational study of healthcare settings.
A structured observational approach can be highly effective for collecting multiple layers of data necessary for understanding interactions between the physical environment and other systems components in healthcare settings.
The video-based observation method is effective in settings that have clearly defined environmental boundaries, limited number of people, are complex and fast-paced such as the OR, ED trauma rooms, and ICU rooms.
While this method potentially yields a rich dataset, it is time consuming, and teams should allocate time and resources accordingly.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Agency for Healthcare Research and Quality [grant number P30HS0024380].