
Abstract
Background:
Long-term care facilities (LTCFs) with compact, group-living arrangements have become COVID-19 hot spots during the pandemic. Systematic research is needed to understand factors associated with COVID-19 infections in LTCFs and the inadvertent effects of preventive measures adopted by LTCFs.
Objectives:
This rapid review identifies factors associated with LTCF residents’ COVID-19 infections and the impacts of the pandemic and the corresponding preventive measures on residents’ mental health and behavioral problems.
Methods:
Following the preferred reporting items for systematic reviews and meta-analyses guidelines, we identified and reviewed relevant literature in Medline, PsycINFO, and AgeLine.
Results:
Thirty-seven articles were identified and reviewed, including 30 reporting factors associated with COVID-19 infections in LTCFs and seven reporting the impact of the pandemic and corresponding prevention measures on LTCF residents. Results revealed four domains of factors associated with COVID-19 infections: facility physical environments, resident characteristics, facility management and testing, and community factors. The pandemic and infection control measures increased residents’ depression, anxiety, loneliness, and behavioral problems (e.g., agitation, hallucinations). Residents without cognitive impairments were more vulnerable to these adverse effects.
Conclusion and implications:
LTCF managers/policymakers and healthcare designers can help mitigate COVID-19 infections by (1) providing additional resources to vulnerable LTCFs; (2) enhancing the training of personal protective equipment use and guideline compliance; and (3) investing in amenities, such as sinks, quarantine rooms, and outdoor spaces. Digital activities and accessible green spaces can mitigate mental health and behavior issues. Future LTCF design can benefit from flexible spaces, natural ventilation, and reducing crowding.
Since the first confirmed case in December 2019, the novel coronavirus disease 2019 (COVID-19) has become a worldwide pandemic. During the first waves of COVID-19, certain population groups (e.g., older adults, persons of color, and individuals with impaired immune systems and comorbidities) were found to be at higher risk of severe complications of COVID-19 (Jordan et al., 2020). Long-term care facilities (LTCFs) are facilities with domestic-styled environments that provide 24-hr functional support and care and include nursing homes, assisted living facilities, care homes, and retirement homes (Sanford et al., 2015). They had disproportionate death rates from COVID-19 partly because their frail older adult residents are particularly susceptible to the life-threatening consequences of respiratory viruses. In the United States, it was estimated that as of March 2021, about 8% of the LTCF residents have died of COVID-19 (The Atlantic, 2021; COVID-19 Nursing Home Data, n.d.). The compact, group-living arrangements in LTCFs with close interactions among residents, staff, and visitors have been linked to greater disease susceptibility (American Geriatrics Society, 2020). Although many LTCFs adopted strict lockdown policies in the first pandemic wave, COVID-19 outbreaks in LTCFs continued to increase before the vaccination became available (Grabowski & Mor, 2020).
As COVID-19-related safety measures were mandated in LTCFs to control the spread of COVID-19, residents in LTCFs were increasingly isolated. These COVID-19 protocols inadvertently accompanied decreases in, or removal of, opportunities for social engagement, physical exercise, and emotional support, which are shown to worsen residents’ cognitive, behavioral, and physical condition and increased risks of anxiety, depression, and cognitive decline (Flint et al., 2020; Mok et al., 2020). With family visits playing an essential role in providing emotional/social support and monitoring the care quality, the quality of care within LTCFs declined during the COVID-19 pandemic as visits from family members were curtailed and staffing shortages became problematic (Gardner et al., 2020).
The vulnerable situation of residents in LTCFs raises questions about the planning and design of facilities to respond to COVID-19 and other infectious diseases. Relevant facility guidelines are being revisited to ensure that LTCFs are better prepared to cope with pandemics like COVID-19 in the future. The main objectives of this study are to review relevant literature to (1) examine how facility characteristics, policies, and community characteristics are associated with COVID-19 infections among LTCF residents and (2) understand the impacts of the COVID-19 pandemic and corresponding preventive measures on LTCF residents’ mental health and behaviors.
Method
Search Process and Study Selection
This rapid review employed the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines (Moher et al., 2009) for most of the review process. For the literature search, we selected three databases most relevant to this review for the timely completion of the search process: Medline, PsycINFO (Ovid), and AgeLine (EBSCO). The time frame of the search was from December 2019, when COVID-19 cases were first reported, to March 2021. Figure 1 shows the review process.
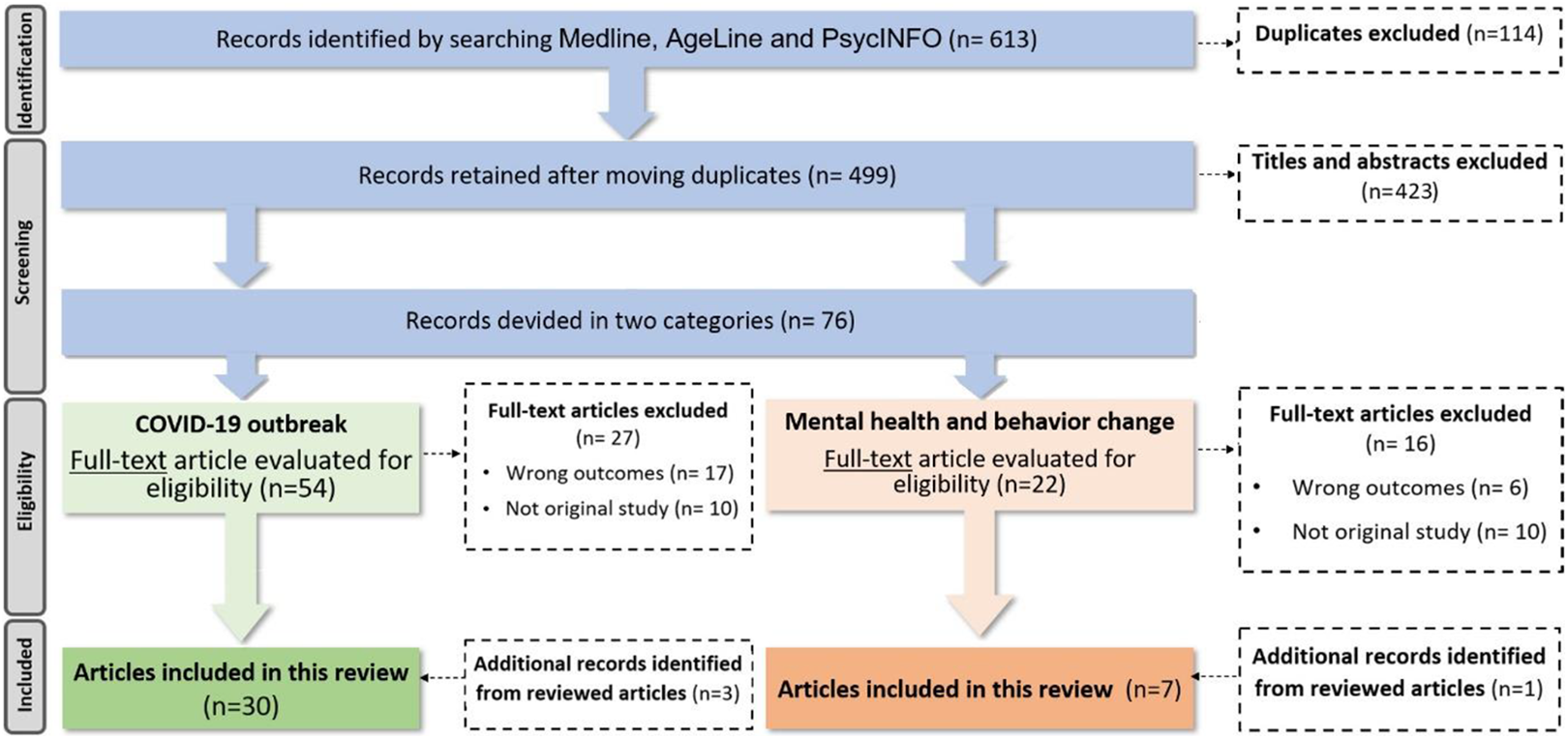
Preferred reporting items for systematic reviews and meta-analyses flow diagram describing study search and selection process.
We searched peer-reviewed empirical studies published in English between December 2019 and March 2021, which addressed (1) correlates of COVID-19 infections among LTCF residents or (2) impacts of the pandemic and/or corresponding preventive measures on LTCF residents’ mental health and behaviors. For the first topic, studies were included in the review if they examined the association between any LTCF characteristic, preventive procedure, or community characteristic and a COVID-19 infection outcome for residents in LTCFs. For the second topic, studies were included if they reported changes in LTCF residents’ mental health (e.g., stress, anxiety, isolation, loneliness) and/or behaviors (e.g., agitation, aggression, wondering, delirium, hallucinations) due to COVID-19 and/or relevant mitigation measures. Multiple combinations of key words were used to search the three databases selected for this study. The key words included wordings that capture LTCFs (“long term care facility,” “assisted living,” “nursing home,” “care homes,” and “aged care facility”), COVID-19 (“COVID-19,” “SAR-CoV-2,” “Severe Acute Respiratory Syndrome Coronavirus 2,” and “2019nCoV”), and residents (“resident,” “care receiver,” “elderly,” “seniors,” and “old adults”). Relevant literature review articles were also examined to identify additional studies that meet our eligibility criteria. Only articles written in English were included. Two reviewers independently screened article titles and abstracts and then reviewed the full text to identify eligible studies. A third reviewer was added to discuss and resolve disagreements when needed.
Data Extraction
A predeveloped data extraction template was used to organize the information gathered from the selected articles include (1) article title, (2) author(s), (3) name of journal, (4) research design, (5) study location, (6) sampling strategy and population, (7) data resources, (8) study period, (9) outcomes variable(s) and measures, (10) independent/confounding variable(s) and measures, (11) data analysis methods, (12) association between each independent/confounding variable and the dependent variable, and (13) study limitation(s). The data extraction was conducted by two researchers independently. Two researchers cross-checked each other’s extraction results to ensure completeness and consistency. The extracted data were reviewed, organized, and synthesized according to the two topics of interest.
Results
A total of 37 articles were identified, with 30 related to correlates of COVID-19 infections in LTCFs and seven related to the mental health and behavioral outcomes of the pandemic and corresponding mitigation strategies. Study characteristics are summarized in Table 1. The time frame of the data used in these studies ranged from January to September of 2020, covering the earliest waves of the COVID-19 outbreaks.
Summary of Included Studies.
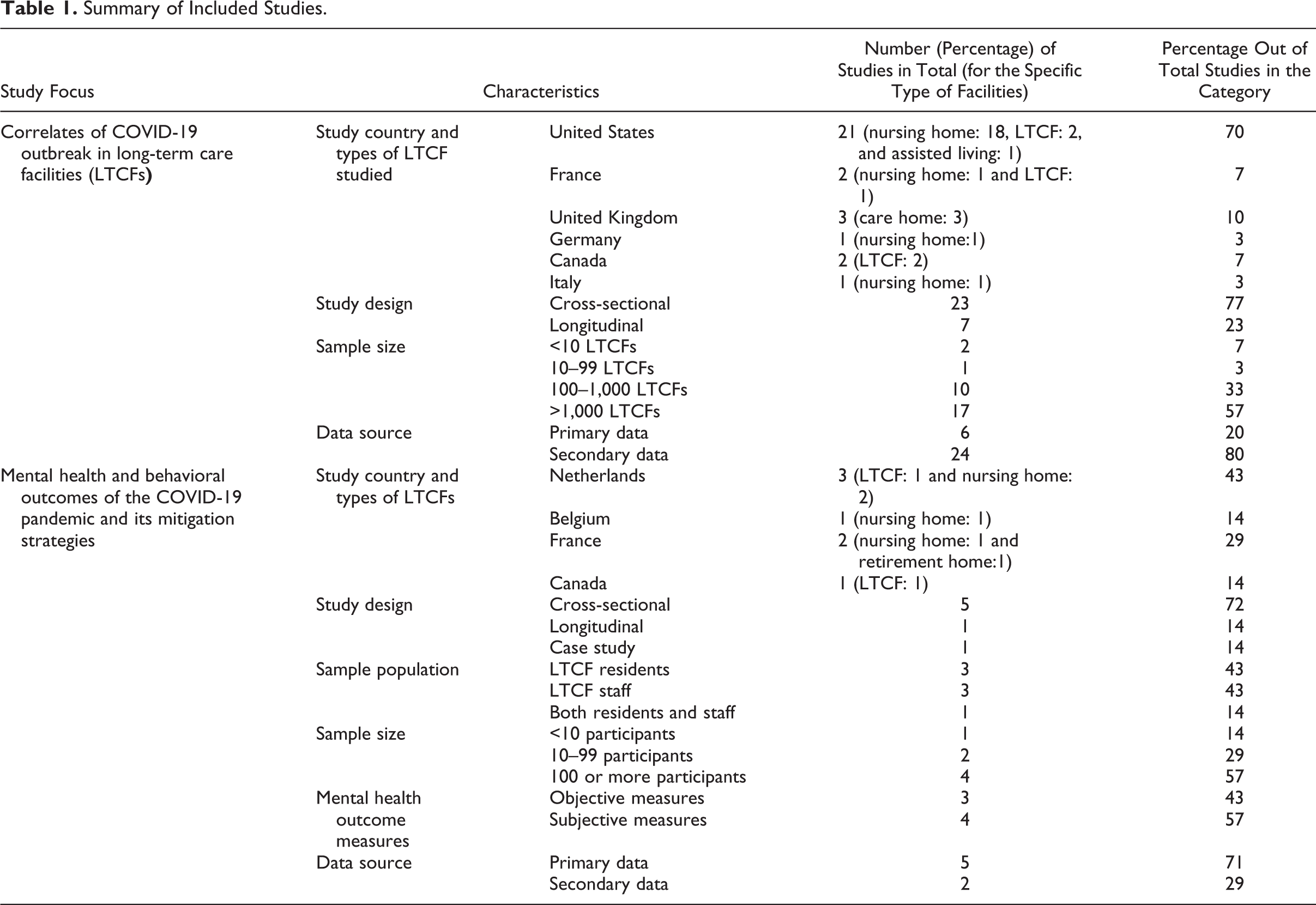
Among the 30 studies about correlates of COVID-19 infections in LTCFs, the largest proportion of studies was conducted in the United States (n = 21; 78%). All articles were quantitative and observational studies. For the sample size, half of the articles analyzed more than 1,000 LTCFs (n = 15; 50%), while three studies had less than 10 LTCFs. More than two thirds of the studies used secondary data (n = 24; 80%). Of the seven studies addressing COVID-19 impacts on residents’ mental health and behaviors, three were from the Netherlands, followed by France with two studies. Sample sizes ranged between 1 and 765 individuals, and over half of the studies (n = 4; 57%) had a sample size of at least 100.
Correlates of COVID-19 Prevalence and Presence in LTCFs
We identified 30 studies that examined the correlates of COVID-19 infections among LTCF residents. Correlates were characterized into four domains: (a) facility physical environments, (b) resident characteristics, (c) facility performance and management, and (d) community factors. In terms of the outcome measurements, these studies focused on either COVID-19 presence or COVID-19 prevalence. The outcome of COVID-19 presence was defined by having at least one resident case in the LTCF. The COVID-19 prevalence was measured as the percentage of infected residents or the number of COVID-19 cases among residents.
Facility physical environments
The correlates in the facility physical environment domain are shown in Table 2 and include facility type, facility size, number of certified beds, room type, occupancy, design elements, and facility age. A comparison of Green House and small nursing homes (typically with 10–12 residents, consistent staff assignment, and private rooms and bathrooms) with other larger, traditional nursing homes found that Green Houses and small nursing homes were less likely to have a COVID-19 outbreak (Zimmerman et al., 2021). Among the facilities with COVID-19 cases, the COVID-19 resident case rate in the Green House and small nursing homes was much lower than other LTCFs. The number of beds was identified as the most influential factor in multiple studies. A larger number of certified beds was associated with an increased likelihood of having a COVID-19 presence in 13 studies (Abrams et al., 2020; Brown et al., 2021; Bui et al., 2020; Chatterjee et al., 2020; Dutey-Magni et al., 2021; Gorges & Konetzka, 2020; Harrington et al., 2020; Lombardo et al., 2021; Shallcross et al., 2021; Stall et al., 2020; Sun et al., 2020; White et al., 2020; Zimmerman et al., 2021) and a larger proportion of COVID-19 cases among residents in two other studies (Travert et al., 2021; White et al., 2020).
Associations Between Facility Physical Environment Factors and COVID-19 Presence or Prevalence Among Long-Term Care Facility (LTCF) Residents.

a+ = positive association; − = negative association; NS = nonsignificant association.
bCOVID-19 presence means having at least one COVID-19 case among residents in the LTCF.
cCOVID-19 prevalence includes outcomes such as the number of COVID-19 cases and the percentage of COVID-19 cases among residents.
For the room type, Stall et al. (2020) suggested that the number of single bedrooms was negatively related to the likelihood of having a documented resident case. Another study identified that LTCF with more separate units was less likely to have a COVID-19 presence (Sun et al., 2020). Results about LTCF occupancy are inconsistent. Two studies showed that the occupancy level had a positive relationship with COVID-19 presence (Dutey-Magni et al., 2021; Sun et al., 2020), while the others found the occupancy rate to be insignificant for the initial outbreak but a driving factor for the number of infections in LTCFs (Bowblis & Applebaum, 2020; Brown et al., 2021; He et al., 2020). A study of 24 LTCFs in Atlanta indicated that LTCFs that implemented signages about droplet and contact precautions and had sinks in bathrooms and bedrooms had fewer COVID-19 infections among their residents (Telford et al., 2021).
Residents’ characteristics
Table 3 summarizes the results on the relationship between residents’ characteristics and the presence or prevalence of COVID-19 among LTCF residents. Nursing homes with older and more male residents were more likely to have a COVID-19 presence among their residents (Dutey-Magni et al., 2021; Temkin-Greener et al., 2020). Another noteworthy correlate of the presence and the infection rate were racial and ethnic minority status. Eleven articles found that LTCFs with a large population of Black, Hispanic, or Asian residents were more likely to have COVID-19 presence or greater prevalence among their residents (Abrams et al., 2020; Bowblis & Applebaum, 2020; Gorges & Konetzka, 2020; He et al., 2020; Li, Temkin-Greener, et al., 2020; Mehta et al., 2021; Shi et al., 2020; Sun et al., 2020; Temkin-Greener et al., 2020; Travers et al., 2021; White et al., 2020). Three studies showed that the higher percentage of Medicaid and Medicare residents was associated with an increased risk of COVID-19 presence (Abrams et al., 2020; Chatterjee et al., 2020; Temkin-Greener et al., 2020), while two other studies reported insignificant results (Bowblis & Applebaum, 2020; Li, Temkin-Greener, et al., 2020). Li and colleagues (2020) indicated that LTCF with more Medicaid and Medicare residents had higher infection rates (Li, Temkin-Greener, et al., 2020). Two U.S. studies found that the obesity rate among residents was related to higher COVID-19 prevalence (Mehta et al., 2021; Temkin-Greener et al., 2020). One study in England showed that receiving new residents during the pandemic increased the COVID-19 infected rate (Shallcross et al., 2021).
Association Between Residents’ Characteristics and COVID-19 Presence or Prevalence Among Long-Term Care Facility (LTCF) Residents.
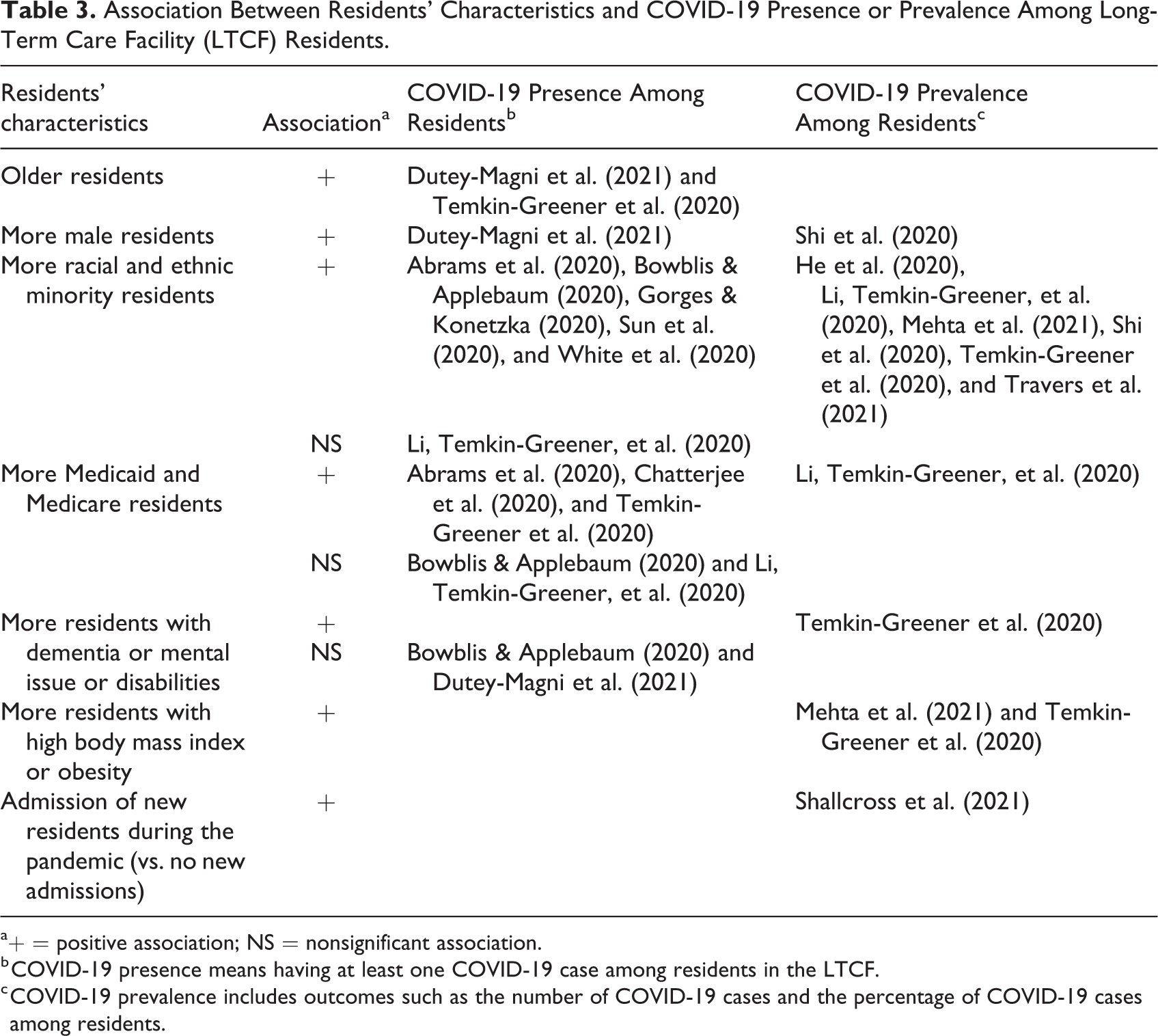
a+ = positive association; NS = nonsignificant association.
b COVID-19 presence means having at least one COVID-19 case among residents in the LTCF.
c COVID-19 prevalence includes outcomes such as the number of COVID-19 cases and the percentage of COVID-19 cases among residents.
Performance and management
Facility performance and management variables related to COVID-19 presence and prevalence can be grouped into four categories: infection control policies, LTCF ownership, performance and deficiencies, and staffing (Table 4). Studies showed that screening and testing, and training on wearing personal protective equipment (PPE) were protective of COVID-19 spread (Krone et al., 2021; Shallcross et al., 2021; Telford et al., 2021). Observing protective care (e.g., wearing gloves, facemasks, and aprons) was a positive correlate of LTCF COVID-19 presence and prevalence (Shallcross et al., 2021). The authors stated that the most possible reason for this counterintuitive finding may be the cross-sectional design of this study not allowing to identify causality between variables. Therefore, it is possible that protective care practice may be in response to the high rates of COVID-19 prevalence.
Association Between Long-Term Care Facility (LTCF) Performance and Management and COVID-19 Presence or Prevalence Among Residents
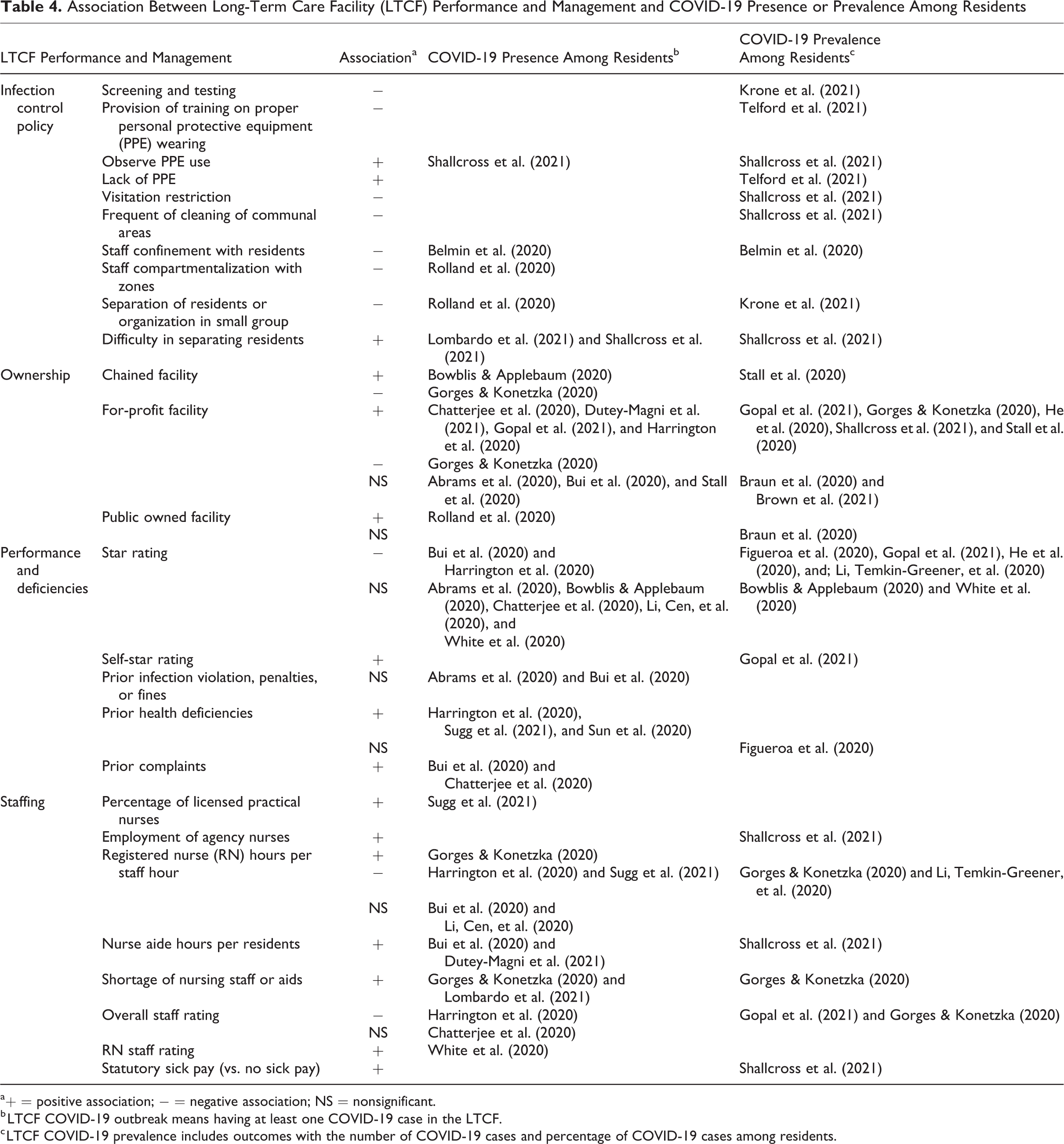
a+ = positive association; − = negative association; NS = nonsignificant.
b LTCF COVID-19 outbreak means having at least one COVID-19 case in the LTCF.
c LTCF COVID-19 prevalence includes outcomes with the number of COVID-19 cases and percentage of COVID-19 cases among residents.
Lack of PPE was related to the increased COVID-19 infection ratio in LTCFs (Telford et al., 2021). Frequent cleaning in communal areas and visitation closing was associated with less spread of COVID-19 (Shallcross et al., 2021). Preventative actions related to decreased COVID-19 outbreaks included requiring staff quarantine with residents, compartmentalization with zones, and isolating or organizing residents in cohorts (Belmin et al., 2020; Rolland et al., 2020). Difficulties in separating residents because of the limited physical space or unwillingness of the residents to quarantine were associated with increased COVID-19 presence and prevalence (Rolland et al., 2020; Shallcross et al., 2021).
LTCF ownership has also been linked to COVID-19 outcomes in studies from the United States, England, and Canada. A national U.S. study found that LTCFs that were part of chains were less likely to have a COVID-19 presence than their counterparts (Gorges & Konetzka, 2020). However, Bowblis and Applebaum (2020) reported a contradictory result from their study among Ohio nursing homes, which showed chained facilities had a higher risk of COVID-19 presence. A Canadian study also showed that such facilities had more confirmed cases than facilities that were not part of chains (Stall et al., 2020).
The results about LTCFs under for-profit ownership were not consistent. Eight studies from the United States, United Kingdom, and Canada indicated that the for-profit status was positively correlated with the COVID-19 presence or a higher rate of COVID-19 infection among residents (Abrams et al., 2020; Chatterjee et al., 2020; Dutey-Magni et al., 2021; Gopal et al., 2021; Gorges & Konetzka, 2020; Harrington et al., 2020; He et al., 2020). But five articles from the United States and Canada reported a nonsignificant relationship between them (Abrams et al., 2020; Braun et al., 2020; Brown et al., 2021; Bui et al., 2020; Stall et al., 2020). One study from southwestern France found that public-owned facilities had a significantly higher chance of having a COVID-19 presence among residents (Rolland et al., 2020). Another study from the United States comparing the public-owned and private-owned LTCFs found no significant differences in COVID-19 prevalence (Braun et al., 2020).
LTCFs’ performance and deficiencies are strong indicators of care quality. The five-star rating system from the Centers for Medicare & Medicaid Services (CMS) was used to assess the care quality in U.S. LTCFs by comparing health inspections, staffing, and quality measures. Studies included in this review reported inconsistent findings on the associations of the five-star rating with COVID-19 presence and prevalence. For the COVID-19 presence outcome, five studies found no significant relationship (Abrams et al., 2020; Bowblis & Applebaum, 2020; Chatterjee et al., 2020; Li, Cen, et al., 2020; White et al., 2020), while two other studies found higher star ratings to be associated with lower odds of COVID-19 presence among residents (Bui et al., 2020; Harrington et al., 2020). In terms of the relationship with the COVID-19 prevalence, four studies reported negative associations while two reported insignificant associations (Bowblis & Applebaum, 2020; Figueroa et al., 2020; Gopal et al., 2021; He et al., 2020; Li, Temkin-Greener, et al., 2020; White et al., 2020). One study in California found that the LTCFs rating themselves higher than the CMS rating tended to have more cases (Gopal et al., 2021). Two studies concluded that prior infection violations, penalties, or fines were not associated with the COVID-19 outbreak (Abrams et al., 2020; Bui et al., 2020). However, the greater number of complaints from the residents was positively correlated with having a COVID-19 presence (Bui et al., 2020; Chatterjee et al., 2020). Three other studies reported that prior health deficiencies were associated with an increased outbreak in LTCFs (Harrington et al., 2020; Sugg et al., 2021; Sun et al., 2020).
In terms of the staffing levels, studies investigated the number of nurses/staff and nursing time. Sugg et al. suggested that LTCFs with more licensed practical nurses and nursing time were at a higher risk of the COVID-19 presence (Sugg et al., 2021). Shallcross et al. (2021) found that LTCFs that hire agency nurses tended to have increased odds of infection in residents and outbreaks (Shallcross et al., 2021). Several studies reported that higher registered nurse (RN) hours, staff hours, or aide hours per resident were associated with increased COVID-19 presence and prevalence (Bui et al., 2020; Dutey-Magni et al., 2021; Gorges & Konetzka, 2020; Shallcross et al., 2021). In contrast, two studies found that higher RN hours and staff hours were associated with reduced COVID-19 outbreaks (Harrington et al., 2020; Sugg et al., 2021), while another two identified nonsignificant impact (Bui et al., 2020; Dutey-Magni et al., 2021). LTCFs experiencing staff shortages or aids and failing to provide staff sick pay were associated with increased odds of COVID-19 presence and prevalence (Gorges & Konetzka, 2020; Lombardo et al., 2021; Shallcross et al., 2021). Lower staff ratings predicted the increased odds of having a COVID-19 presence and higher COVID-19 prevalence (Gopal et al., 2021; Gorges & Konetzka, 2020; Harrington et al., 2020). However, a higher RN staff rating positively predicted the COVID-19 presence in one study involving U.S. skilled nursing facilities (White et al., 2020).
Community factors
Previous studies also identified the community factors associated with COVID-19 outbreaks and prevalence in LTCFs (Table 5). The county- or state-level COVID-19 prevalence is positively associated with COVID-19 presence in LTCFs, as reported by seven articles (Abrams et al., 2020; Brown et al., 2021; Chatterjee et al., 2020; Gorges & Konetzka, 2020; Sugg et al., 2021; Sun et al., 2020; White et al., 2020). In addition, Shi and colleagues (2020) suggested if staff lived in communities with high COVID-19 prevalence, COVID-19 rates in those LTCFs would be higher (Shi et al., 2020). LTCFs located in a public health unit region with more cases were identified positive association with the presence of COVID-19 (Stall et al., 2020). Several studies found significant community-level demographic and socioeconomic correlates for the COVID-19 presence in LTCFs, including urban location, larger population, higher population density, larger black population, and more deprivation and unemployment (Abrams et al., 2020; Bach-Mortensen & Degli Esposti, 2021; Brown et al., 2021; Sugg et al., 2021; Sun et al., 2020; White et al., 2020).
Association Between Community Factors and COVID-19 Presence or Prevalence Among Residents.

a+ = positive association; NS = nonsignificant.
b LTCF COVID-19 outbreak means having at least one COVID-19 case in the LTCF.
c LTCF COVID-19 prevalence includes outcomes with the number of COVID-19 cases and percentage of COVID-19 cases among residents.
Impacts on Mental Health and Behavior of LTCF Residents
We found seven articles that studied LTCF residents’ mental health or behavior issues associated with the COVID-19 pandemic. To mitigate the rapid spread of COVID-19 in LTCFs, governments and facilities have implemented policies including infection prevention actions, restriction for visitors, and activity cancellations (Levitt & Ling, 2020; Sizoo et al., 2020). We examined these policies for their association with unintended consequences of decreased mental health conditions and increased behavior problems among LTCF residents.
Mental health concerns
The direct impact of lockdown on LTCF residents was associated with increased fear, loneliness, anxiety, depression, and sadness (El Haj, Altintas, et al., 2020; Sizoo et al., 2020; Van der Roest et al., 2020). In addition, loss of freedom, stimulation, autonomy, and social life were observed during COVID-19 (Kaelen et al., 2021). In two studies, residents with cognitive impairment (CI) were observed to have increased hallucinations and cognitive declines (El Haj, Larøi, et al., 2020; Sizoo et al., 2020). Another study indicated that residents without CI experienced more significant increases in depression and anxiety than CI residents (Van der Roest et al., 2020).
Problematic behaviors
During the pandemic, governments and LTCFs across the world enacted bans on visitations of LTCFs. In addition to limiting residents’ opportunities to interact with their family members, this ban increased staff workload, stress, and burnout (Low et al., 2021). Observed behaviors associated with the pandemic revealed significant differences between residents with CI and others. Although all residents exhibited more aggressive behaviors (e.g., agitation, aggression, and irritability) and less food intake (Sizoo et al., 2020), residents without CI seemed to be more severely impacted by COVID-19 than those with CI (Van der Roest et al., 2020). A study from Canada reported that residents without CI did not significantly change delirium and behavioral problems during COVID-19 (McArthur et al., 2021). Another study found that the residents with dementia had less agitation, aggregation, and wandering while exhibiting more apathetic behaviors during the lockdown period than those without dementia (Leontjevas et al., 2020).
Discussion
This rapid review examined factors associated with COVID-19 presence and prevalence among LTCF residents and the impacts of the pandemic on LTCF residents’ mental health and behaviors during the earliest waves of the pandemic. Knowing such factors can guide preventive measures in LTCF management and environmental design to help mitigate the detrimental effects of COVID-19. This work is especially timely and relevant, given the ongoing global outbreak and its continuing impacts on LTCFs, which are expected to be long-lasting even with vaccinations.
Thirty studies reported the correlates of the COVID-19 presence and prevalence of infections from four domains of factors: (a) facility physical environment, (b) residents’ characteristics, (c) facility performance and management, and (d) community factors. This rapid review identified LTCFs susceptible to COVID-19 spread as those of large size and occupancy located in high COVID-19 risk communities and those with larger proportions of racial minority or Medicaid and Medicare populations. However, as all the studies failed to collect the basic health conditions of residents in LTCFs, the finding on higher risk in nursing homes with more minority or Medicaid and Medicare populations may be due to the underlying health conditions associated with different racial and Medicaid and Medicare groups. In addition, community factors including high densities, large total and black populations, high deprivation rates, and high unemployment rates contributed to increased COVID-19 outbreaks in LTCFs.
Study results were consistent about the direction of associations for most of the correlates, except for the occupancy rate, LTCF performance, deficiencies, ownership, and staffing. Inconsistent results about the roles of occupancy rate might be due to the differences in the measurement methods used in the studies. For example, some studies used the daily occupancy rate based on licensed beds, while one study used a composite index created from the number of occupants per room and the number of occupants per bathroom. The two reasons can possibly explain inconsistent results for the LCTF performance, deficiencies, and ownership. First, studies were conducted in different states and countries, where different policies and other differential contextual factors might have led to different roles of the same/similar factors. Second, as time passes, LTCFs with lower star ratings and for-profit ownership might gain more experience handling situations by learning from their high numbers/rates of cases during early phases. This review concluded that the star rating was not significant in predicting the initial LTCF presence. Still, higher ratings had a significant negative relationship with the prevalence. However, its impact may diminish as the pandemic persists. Inconsistent results about staffing might be related to the complex and dynamic mechanisms underlying the spread of COVID-19. On the one hand, more interactions between residents and staff might provide more opportunities for cross-contamination and inflections if staff members carry the virus. On the other hand, staff shortage might lead to insufficient preventive/hygiene measures that can, in turn, increase the possibility for residents to be exposed to and contract COVID-19.
The seven studies reporting the impact of the pandemic on LTCF residents’ mental health and behaviors demonstrated that responses to the pandemic such as visitation closures, infection prevention measures, activity cancellations, and restrictions on social engagement were associated with an increase in depression, loneliness, anxiety, and fear, especially in residents without CI. Unexpectedly, the lockdown was associated with fewer reported behavioral problems in dementia residents, such as agitation, aggression, and wandering. In contrast, LTCF residents without CI were observed to have more aggressive behaviors. Studies further identified a significant decrease in food intake for all residents, while those with dementia were less seriously impacted. Residents with dementia had a lower level of impact or even a positive effect from lockdown, which may be attributed partly to the calmer atmosphere achieved with fewer visitors and more staff contact (Anderson & Blair, 2020). However, more research is needed to understand factors differentiating in the experiences of those with and without CI.
Conclusions and Implications
Gaps in the Literature
Published articles indicated a strong association between the LTCF and community characteristics and COVID-19 infection outcomes. However, studies in this review only covered the early waves of the pandemic, when the lack of testing, screening, and PPE, and deficiency in infection control management was more of the norm. As the testing capacity increased and protective supplies became more accessible later during the pandemic, factors associated with COVID-19 presence or prevalence could change dramatically. Therefore, future studies should address multiple pandemic waves to understand their dynamic and evolving roles and associations over different pandemic periods.
Compared to the studies focusing on LTCF infections, studies that examined the impact of the pandemic on LTCF residents’ mental health and behaviors were relatively few. Notably, in the United States, no study during our search period addressed this topic. Hence, this is a topic needing further study, especially to unravel whether and why those residents without CI seemed to fare worse in the initial studies.
In addition, this study focused on the direct impacts of the COVID-19 pandemic and corresponding preventive measures on the health and mortality of LTCFs residents. In future studies, it will also be essential to understand the secondary impacts of the pandemic and preventive measures on LTCF residents’ health conditions and mortality. A better understanding of both direct and secondary impacts can inform current and future efforts in responding to similar pandemics while balancing the physical, mental, and behavioral health of LTCF residents.
Study Limitation
This rapid review was limited to peer-reviewed studies written in English and excluded the gray literature and those published in other languages. Only studies published from December 2019 through March 2021 were included in this review. Given the rapidly changing nature of the pandemic, some critical information published later is also crucial for a better understanding of the topic. However, this particular study intended to provide insights into the early impacts of the COVID-19 pandemic. Besides, in the early stage of the pandemic, the infection data were not available for all the LTCFs. This might have been one of the reasons that limited the sample size in some of the studies and potentially introduced sampling bias. Data sources of the outcome measurements included the state or local public health departments, country-level health departments, individual LTCFs operators, Outpatient Standard Analytical File (SAF), and Hospital SAF. The different sampling frameworks in survey studies may impact the research validity.
Recommendations for Future Practice
Drawing from this review and from our past experiences in environmental design and public health, we suggest several best practices to help reduce the infection risks of COVID-19 and similar outbreaks in the future. To keep COVID-19 from entering and spreading throughout the facility, LTCF managers should strictly follow infection control policies, including training staff, enforcing proper PPE use, and using adequate signage. Policymakers are encouraged to allocate additional resources to vulnerable LTCFs including those with higher living density, more non-White residents, and located in high COVID-19 risk areas. Environmental amenities such as private sinks in residents’ rooms, designated test areas, and quarantine rooms should be integrated with the LTCF design and programming by designers.
Because some of the infection control policies inadvertently caused a reduction in social engagement and physical activities, LTCFs should provide alternative ways to meet residents’ social and mental health needs. Digital technologies can be introduced into residents’ daily lives, giving alternative mechanisms for social interactions with family members and friends, and connections to the world outside (Meneses Fernández et al., 2017). However, people with dementia may not be able to recognize or communicate with others via a screen. Temporary outdoor spaces setup to accommodate safe in-person visitations can accommodate their needs for social interaction in a safer and more restorative environment.
Suggestions for Future Nursing Home Design
Accessibility to frequent screening and testing was among the most influential factors in preventing the spread of COVID-19 in LTCFs in the early waves. We suggest that healthcare designers consider adding a built-in medical station in the facility for infection control and daily healthcare to perform various testing and screening activities. Reducing the size and density of residential units in LTCFs or subdividing large LTCFs into smaller units appear essential to prevent the spread of COVID-19. Building or remodeling more bedrooms with a private bathroom and sink could also prevent and/or reduce infections. Dedicated areas or flexible spaces for employees’ stay during the lockdown period should also be considered in the facility design. Natural ventilation helps reduce the concentration of pathogenic viruses in the air, as strongly recommended in the infection control guidelines (Wang, 2021). Other promising strategies include providing access to telemedicine facilities and the ability to implement ventilation equipment. To reduce the negative impacts of lockdown on the mental health of staff and residents, the quality of window views can be improved by more carefully orientating the buildings and designing the outdoor landscape. In addition, safe and accessible outdoor environments should be provided to facilitate and accommodate physical and social activities among the residents.
Many design features are being examined by groups monitoring LTCFs. It is important to recognize that some design features will be easy and less expensive to implement, while others will require more capital investment. Strategies also differ for retrofitting existing facilities versus designing new facilities. What is important is for LTCF designers, managers, and policymakers to be better informed about facility characteristics that either facilitate or impede the spread of infectious diseases.
Implications for Practice
Allocate additional resources such as PPE, access to test, and training to vulnerable LTCFs, including those with higher density, with more non-White residents, and located in high COVID-19 risk areas.
Enhance the training of PPE use and adhere to the relevant guidelines in LTCFs.
Invest in amenities such as sinks, clear signs, quarantine rooms, and outdoor spaces in LTCFs.
Provide flexible spaces, use natural ventilation, and reduce crowding in future LTCF design.
Implement digital social activities and provide accessible green spaces for LTCF residents.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially supported by the Innovation[X] Program at Texas A&M University.