
Abstract
Objective:
The goal of this research was to understand the use of decentralized nursing stations (DNS), corridors, and huddle stations as places for teamwork and multidisciplinary care in the neonatal intensive care unit (NICU).
Background:
This article shares outcomes from a pre- and post-occupancy evaluation that assessed a NICU moving from an open-bay model to a new single-family room (SFR) unit comprised of six, 12-bed neighborhoods. This interdisciplinary research team draws upon the practical expertise of a NICU Patient Care Manager and researchers in Design and Communication to illuminate the research process, results, and lessons learned.
Methods:
A multi-methodological design, approved by the institutional review board, was employed that utilized an electronically distributed pre- and post-move survey of staff and observational counts of face-to-face interactions.
Results:
Survey results indicate NICU staff have statistically significant higher perceptions of job satisfaction, stress and well-being, and design satisfaction among a variety of professionals after moving to a SFR, decentralized unit design. Consistent with the literature, staff did not have significantly higher perceptions of the decentralized NICU relative to teamwork. Observations revealed frequency of conversations primarily at DNS followed by corridors and huddle stations. When examining the multidisciplinary makeup, outcomes were reversed with huddle spaces holding the largest percentage of conversations. On average, there were 2.72 individuals involved in these interactions, with the corridor seeing the largest average of group sizes.
Conclusion:
The outcomes of this study demonstrate that neutral spaces such as corridors and centralized huddle stations should be considered as locations for strategic collaboration and multidisciplinary care.
Keywords
Introduction
NICU Design
Neonatal intensive care units (NICU) contain some of the most fragile and vulnerable patient populations. Models of family-integrated care, couplet care, kangaroo care, and greater attention to circadian rhythms, infection prevention, breastfeeding support, and acoustics have led to the integration of single-family rooms (SFRs) and away from the historically constructed open or multiple-bed bays (Fay et al., 2020). Research continues to support the benefits of SFR units on patients and families citing improved quality of patient care, parent satisfaction, parent interaction, enhanced privacy, reduced level of infection, improved lighting levels, reduction in noise levels, and decreased length of stay (Bosch et al., 2012; Domanico et al., 2010; Hogan et al., 2016; Shahheidari & Homer, 2012; Watson et al., 2014; Winner-Stoltz et al., 2018). Although literature predominantly favors the SFR model for staff, Doede’s (2018) literature review reveals trade-offs including decreased interaction among the NICU patient care team, difficult interactions with families, decreased communication and perceptions of safety, and an increased perception of workload.
Review of the Literature
Teamwork and Multidisciplinary Care
As NICU care continues to become more complex, healthcare systems are responding with multidisciplinary care practices that include an array of caregivers including pharmacists, lactation consultants, dietitians, behavioral health specialists, and social workers. A key element to effective care lies within the team’s ability to communicate and collaborate with other professionals across the healthcare system. Effective teamwork in the NICU is critical to the delivery of high-quality care (Masten et al., 2019). Teamwork can be defined as “a behavioral process, wherein team members collectively accomplish specified goals efficiently and effectively, in the context of one or more patient care objectives” (Gharaveis et al., 2018). Multidisciplinary care requires the formation of social networks within the workplace to enable cross-disciplinary exchanges that challenge traditional medical domination of the care process and support informal learning opportunities for team members. Such exchanges can test team member assumptions, gather information, seek clarification, and provide input to collective decision-making processes (Carthey, 2008). Physical design can shape the social logic of nursing communication and teamwork in hospital workspaces (Real et al., 2018).
Job Satisfaction, Stress, and Well-Being
Awareness of healthcare professionals and their workplace design needs must come to the forefront of healthcare design as healthcare organizations face a staffing crisis that’s predicted to only get worse. According to data published by the Association of American Medical Colleges (AAMC), the United States could see an estimated shortage of between 37,800 and 124,000 physicians by 2034 (AAMC, 2021). The growing demand for both healthcare workers and services affect job satisfaction and healthcare quality (Obeidat et al., 2021). Work stress can negatively impact well-being and contribute to decreased morale, fatigue, and burnout; ultimately leading to job dissatisfaction and turnover. Research indicates that social support from others can settle work stress, reduce depression, and positively impact patient outcomes (Alvaro et al., 2016). Numerous studies have revealed that job satisfaction is influenced by work environment, unit layout, nursing care delivery model, organizational climate, and interpersonal relationships (Jimenez et al., 2019; Obeidat et al., 2021). Ulrich’s (1991) theory of supportive design grounds this in noting that the physical environment will reduce stress if it fosters perceptions of control and social support. The NICU comes with a range of potential stressors including the need for specialized education and training to adequately care for fragile newborns, working with new technologies to do so, and dealing with death and dying (Fiske, 2018). The physical environment of the NICU has been identified as a potential cause of physical and psychological stress for nurses due to concerns with patient visibility, walking distances, and decreased interaction and communication with team members (Fiske, 2018).
Nurse Stations, Corridors, and Neutral Spaces
Rashid and Zimring (2008) identify primary variables of workplace design to be interior design features including building configuration, floor layout, and functional distribution. Design layout is one of the most cited factors that play a role in healthcare teamwork. The spatial layout of a unit, including the location of walls, partitions, and furnishings can impact the frequency and quality of communication and interaction among staff (Gharaveis et al., 2018, Trzpuc & Martin, 2010).
Nursing stations are one of the predominant factors shaping healthcare unit layouts. The integration of decentralized nursing stations (DNS), or recessed alcoves outside the patient rooms, emerged with the design intent to position nurses closer to patient rooms and to positively impact visibility, response time, and enhanced patient care (Fay et al., 2018). However, research suggests that larger unit size and long corridors have led to unexpected negative consequences of reduced teamwork in decentralized units (Fay et al., 2018; Harvey et al., 2015; Pati et al., 2018; Real et al., 2017).
When considering unit design, corridors serve an important role as connective, flexible, multipurpose spaces (Colley et al., 2018). The value of a corridor should be considered as a setting that facilitates the interaction of multidisciplinary healthcare teams (Carthey, 2008). As such, some facilities are integrating extra-wide corridors to support interdisciplinary care (Fay et al., 2017). Face-to-face interactions have been found to be the most influential type of interaction within the corridor and can range from simple and unplanned social interactions to planned collaborative interactions (Gharaveis et al., 2018). Corridors have also been identified as an important space for care-related activities such as reviewing patient charts and preparing medications and supplies (Colley et al., 2018).
Neutral spaces, such as shared team rooms or huddle spaces, are traditionally not owned by one primary profession and have been reported to facilitate interprofessional teamwork (Peavey & Cai, 2020). Carthey (2008) notes the importance of adequately designed “neutral zones” for engaging in multidisciplinary exchanges. More specifically, Real et al. (2018) emphasizes the benefits of dedicated collaboration spaces for interdisciplinary caregivers located in units along with DNS as locations for support, mentoring, and social interaction. Hamilton (2017) cites a need for ICU designs to offer both close proximity of caregivers to patients and an environment where centralized elements for the clinical team are available to all.
The literature reveals a demand for further investigation of the SFR NICU work environment and its impact on staff. Designers should understand the components of teamwork and collaboration from a variety of health professional perspectives to develop enhanced designs and support improved healthcare delivery (Real et al., 2017). Designation of the various activities accommodated by DNS, corridors, and neutral spaces in the NICU should be recognized as important locations in the delivery of care (Carthey, 2008).
Aim and Purpose
An interdisciplinary team with members from healthcare, communication, and design conducted a multiphased pre- and post-occupancy evaluation of a NICU in an academic hospital that moved from an open-bay to a SFR design. The goal of this research was to understand the use of DNS, corridors, and huddle stations as places for teamwork and multidisciplinary care in the NICU. The study examined the use of these three spaces by physicians, nurses, technicians, therapists, visitors, and “other,” which included staff members such as custodial, lactation, and administrative, among other professions.
Three specific research objectives were identified for the study. First, to analyze the role physical design features of the NICU have in shaping multidisciplinary care. Second, to examine the use of DNS, corridors, and huddle stations by various health professionals. Third, to gain a richer understanding of the impact of the SFR NICU design on teamwork, stress, well-being, and job satisfaction.
Method
Study Setting
In 2018, the NICU moved from an 8,000 square foot open-bay model to a 36,000 square foot unit. The pre-move unit was comprised of nine, approximately six-bed pods home to a total of 50 beds and two neonate pods that had a total of 16 beds. The new unit includes six, 12-bed neighborhoods home to 72 beds. The majority of rooms in the new model are single occupancy with provision for family and visitors along with two twin rooms. Each neighborhood includes six DNS, a centralized huddle station, and an approximately 1,100 square foot corridor (see Figure 1). The decentralized stations are occupied by one seated nurse and provides a direct view to the patient headwall (see Figure 2). The neutral spaces which are referred to as huddle stations in this unit are primarily used for rounds, training, and grounding for staff (see Figure 3). In between adjacent neighborhoods are dual access medication, clean and soiled utility, nourishment, and equipment rooms. The new unit additionally includes staff spaces such as a workroom, lounge area, quiet room, and terrace that allow staff to work and rest while staying close to patients. For an overview of complete unit demographics, see Table 1.
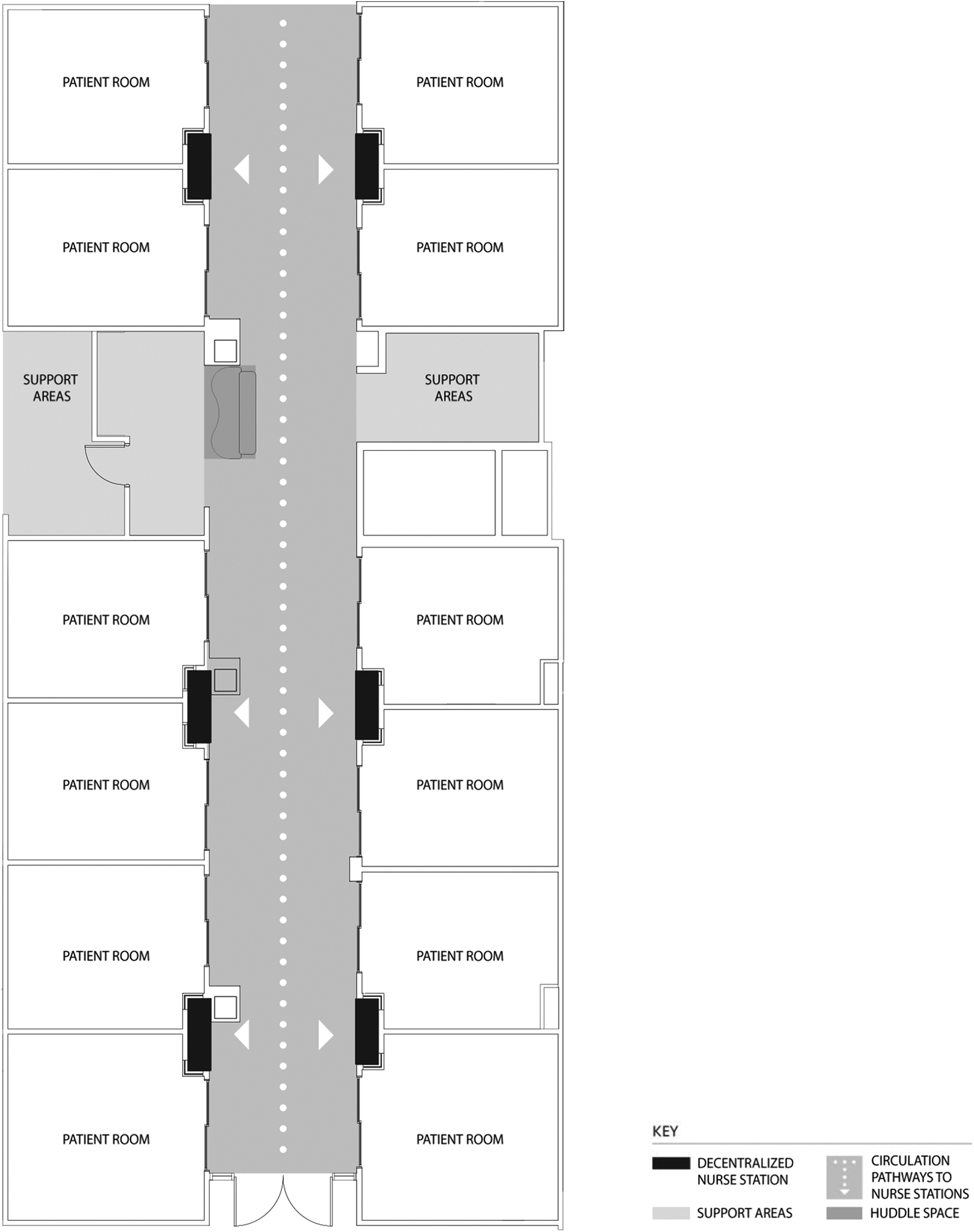
Post-move neighborhood diagram.

Post-move neighborhood.

Post-move huddle space.
Pre–Post NICU Demographics.
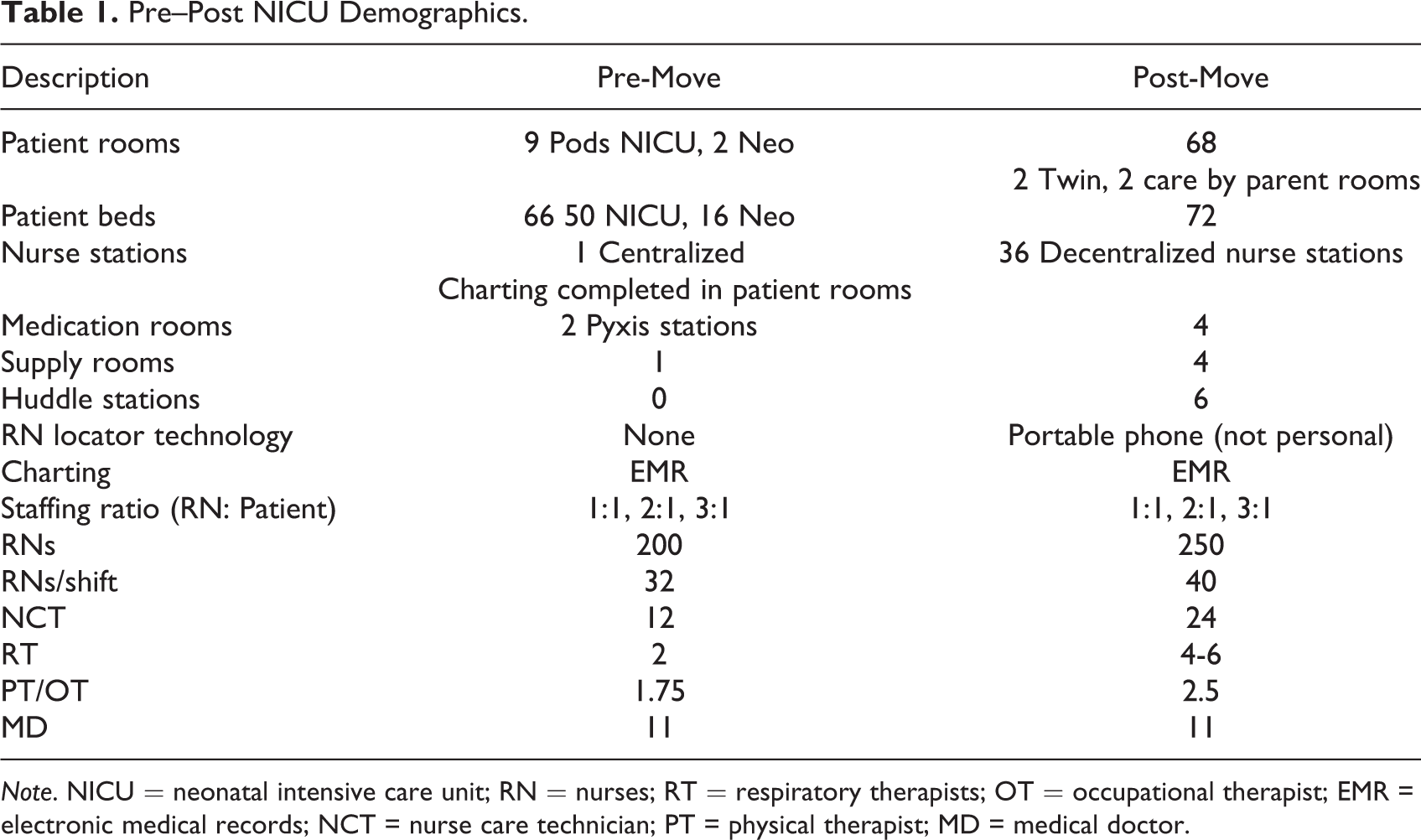
Note. NICU = neonatal intensive care unit; RN = nurses; RT = respiratory therapists; OT = occupational therapist; EMR = electronic medical records; NCT = nurse care technician; PT = physical therapist; MD = medical doctor.
Surveys
A multi-methodological design, approved by the institutional review board, was employed that first utilized an electronically distributed pre- and post-move survey of staff. The survey was piloted and utilized across two additional unit studies in the same facility before being implemented in the NICU study to ensure reliability and validity of findings. All staff members from the NICU service line had the opportunity to participate. The survey utilized 15 questions to assess teamwork, stress and well-being, job satisfaction, and satisfaction with design. Space was allocated for open-ended comments and demographic data were collected including gender, age-group, education, job title, years of experience, and years worked in the unit. Staff outcomes from the pre-move yielded 81 usable surveys while post-move yielded 131 surveys. Responses were recorded on a 5-point Likert-type scale, with 1 indicating strongly disagree and 5 indicating strongly agree.
Survey Analysis Methods
The survey outcomes were analyzed in a variety of ways. First, to test if perceptions were significantly different pre-move to post-move, t tests were performed to compare the mean categorical response rates of teamwork, stress and well-being, job satisfaction, and design satisfaction using the Bonferroni-corrected method. Second, a descriptive analysis was completed to quantitatively summarize individual survey items. For the descriptive analysis, percentage of agreement was calculated by determining the sum of Levels 4 and 5 responses (agreement) and degree of change was determined by calculating the difference between pre- and post-move responses.
Observations
In the post-move study, which was conducted 1 year after the unit moved to the new setting, six observers conducted 40 hr of observations collected over 19 days of 1 month by recording communication at DNS, huddle stations, and corridors. In total, 1,876 instances of observation were collected. Prior to obtaining data, human subject certification was obtained and training in the use of the observational instrument occurred to ensure validity and reliability of findings. Observations were completed using a paper instrument to document instances of face-to-face communication among occupants. Each observational period for communication documentation took place over the course of 2 hr. Observers positioned themselves at the end of each neighborhood, one observer per assigned neighborhood. Those staff who were recorded included physicians and residents (PR), nurses (RN), technicians (TC), therapists (RT), visitors and family members (VI), and other (OT) who were those badge-wearing staff members who were unidentifiable. Each instance of communication was defined as two or more people engaged in a face-to-face conversation. Any time a person entered or left a conversation denoted a new line of communication. The content of the conversation did not matter for this phase of the study and multiple locations could be circled per line (i.e., a staff member in the corridor speaking to another at a nurse’s station). The number of persons involved in the face-to-face communication was recorded by marking the number of people under each staff position listed.
Observational Analysis Methods
Observational data were analyzed in a variety of ways. First, data were analyzed to understand the frequency of overall communication and multidisciplinary communication, or those conversations that included two or more professions, at the DNS, corridor, or huddle station. Next, the exclusive use of these spaces was calculated to determine use by individual profession. Lastly, data were analyzed to determine the use across locations including DNS to corridor, DNS to huddle station, and huddle station to corridor by profession.
Results
Survey results indicate statistically significant higher perceptions of job satisfaction, stress and well-being, and design satisfaction. NICU staff did not have significantly higher perceptions teamwork in the new unit (see Table 2).
Pre–Post Categorical Questionnaire Statistics.
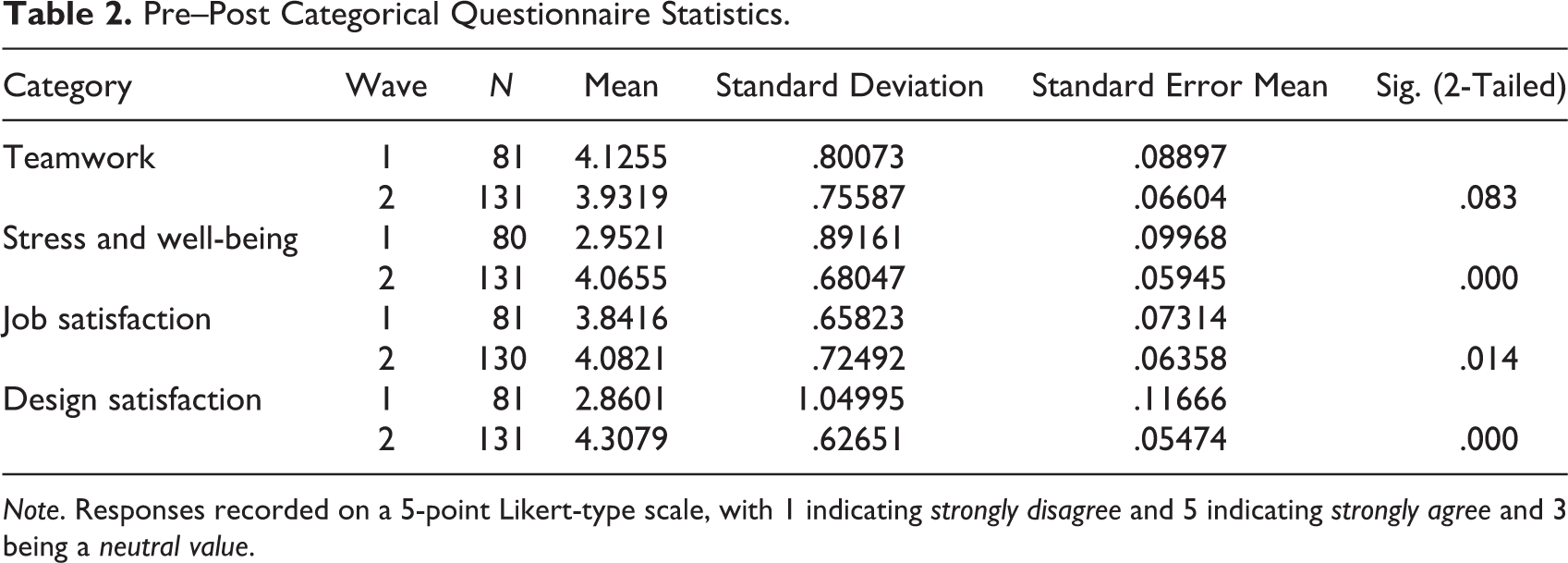
Note. Responses recorded on a 5-point Likert-type scale, with 1 indicating strongly disagree and 5 indicating strongly agree and 3 being a neutral value.
The descriptive analysis helps to further understand these outcomes by examining specific questions. In the category of teamwork, two related prompts saw a notable decrease in perception in the pre–post comparison: “I am satisfied with my ability to get assistance from coworkers when needed” and “I often feel near other co-workers in the unit.” In the category of stress and well-being, staff perceptions of stress saw the largest degree of positive change in response to two prompts: “The design of the unit helps to alleviate my stress” and “There are private places within the unit I can go to alleviate my stress.” The prompts under the category of job satisfaction also trended in the positive direction, though by a smaller degree of change. Lastly, the category with the greatest degree of positive change overall is design satisfaction with nearly 90% of all surveyed participants expressing satisfaction with the design of the unit, workspace, and physical layout of the NICU (see Table 3).
NICU Questionnaire Individual Item Descriptive Analysis.
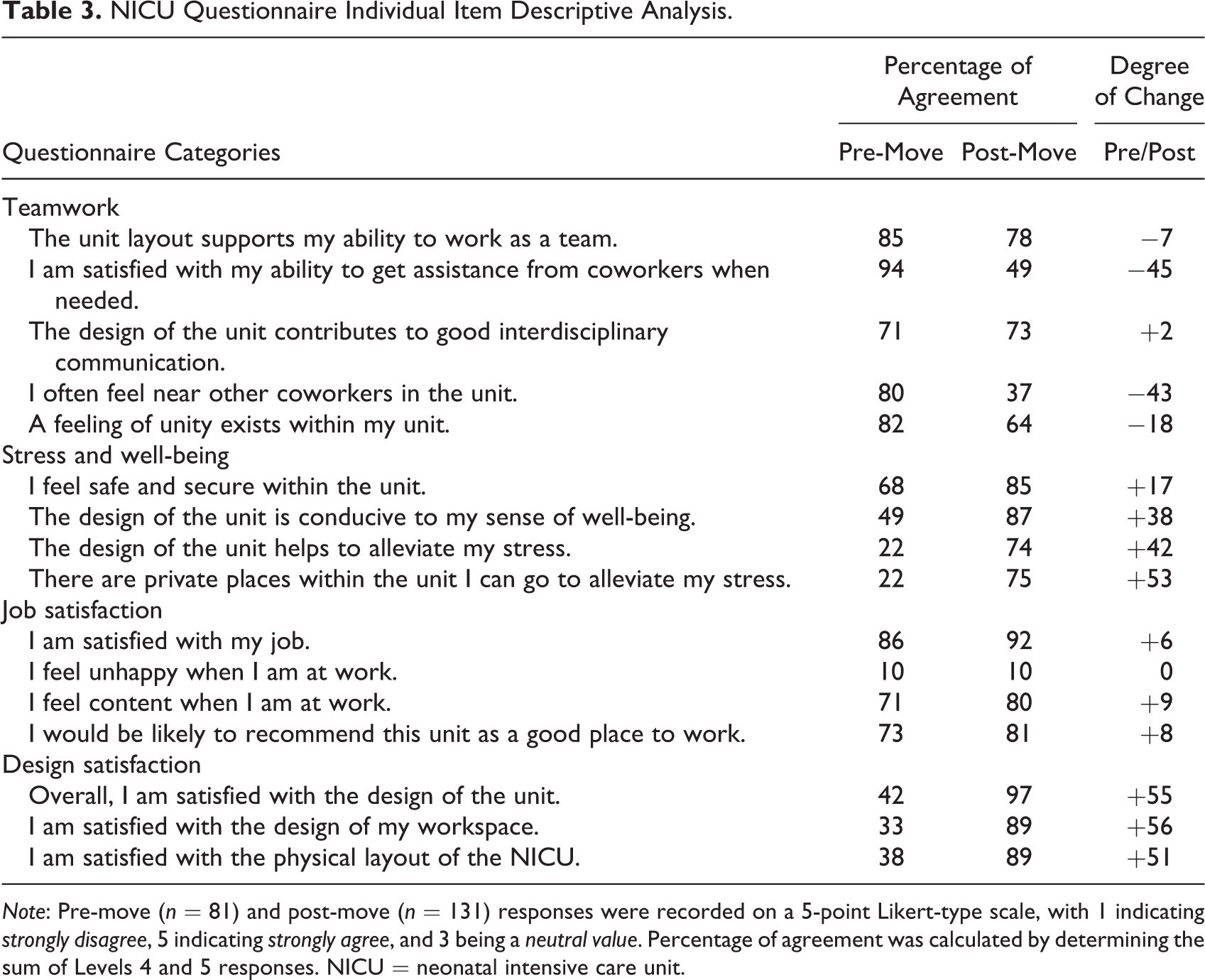
Note: Pre-move (n = 81) and post-move (n = 131) responses were recorded on a 5-point Likert-type scale, with 1 indicating strongly disagree, 5 indicating strongly agree, and 3 being a neutral value. Percentage of agreement was calculated by determining the sum of Levels 4 and 5 responses. NICU = neonatal intensive care unit.
The observational data build upon these outcomes. When examining all 1,876 NICU observations, the frequency of conversations was found to occur predominantly at DNS (54%) followed by corridors (46%) and huddle stations (18%), with some interactions occurring across locations and therefore resulting in a percentage greater than 100. When examining the multidisciplinary makeup of these conversations, or those conversations that included two or more professions, outcomes were reversed, DNS (37%), corridors (44%), and huddle stations (51%), indicating that corridors and centralized huddle stations should be considered as important spaces for multidisciplinary care. On average, there were 2.72 individuals involved in these interactions, with the corridor seeing the largest average group size of 3.08 but reaching a maximum of 12.
Calculating the use of DNS, corridor, or huddle station by individual profession clarifies whom utilizes the various workspaces (see Table 4). Data from 704 observations revealed 1,613 individuals involved in conversations occurring exclusively at the DNS with nursing staff involved in these conversations 80% of the time. Data from 531 observations revealed 1,650 individuals involved in conversations occurring exclusively in the corridor. This location was more equally utilized by physicians and nurses. Lastly, data from 277 observations revealed 430 individuals involved in conversations occurring exclusively at the huddle station. These outcomes confirmed this space as a multidisciplinary care location as physicians, nurses, technicians, and therapists all frequently utilized this space for conversations. The data across locations bring to light an important finding that staff, particularly nurses, most frequently engage in cross location conversations from the decentralized nursing station to the corridor.
Location of Conversation Participation by Profession.
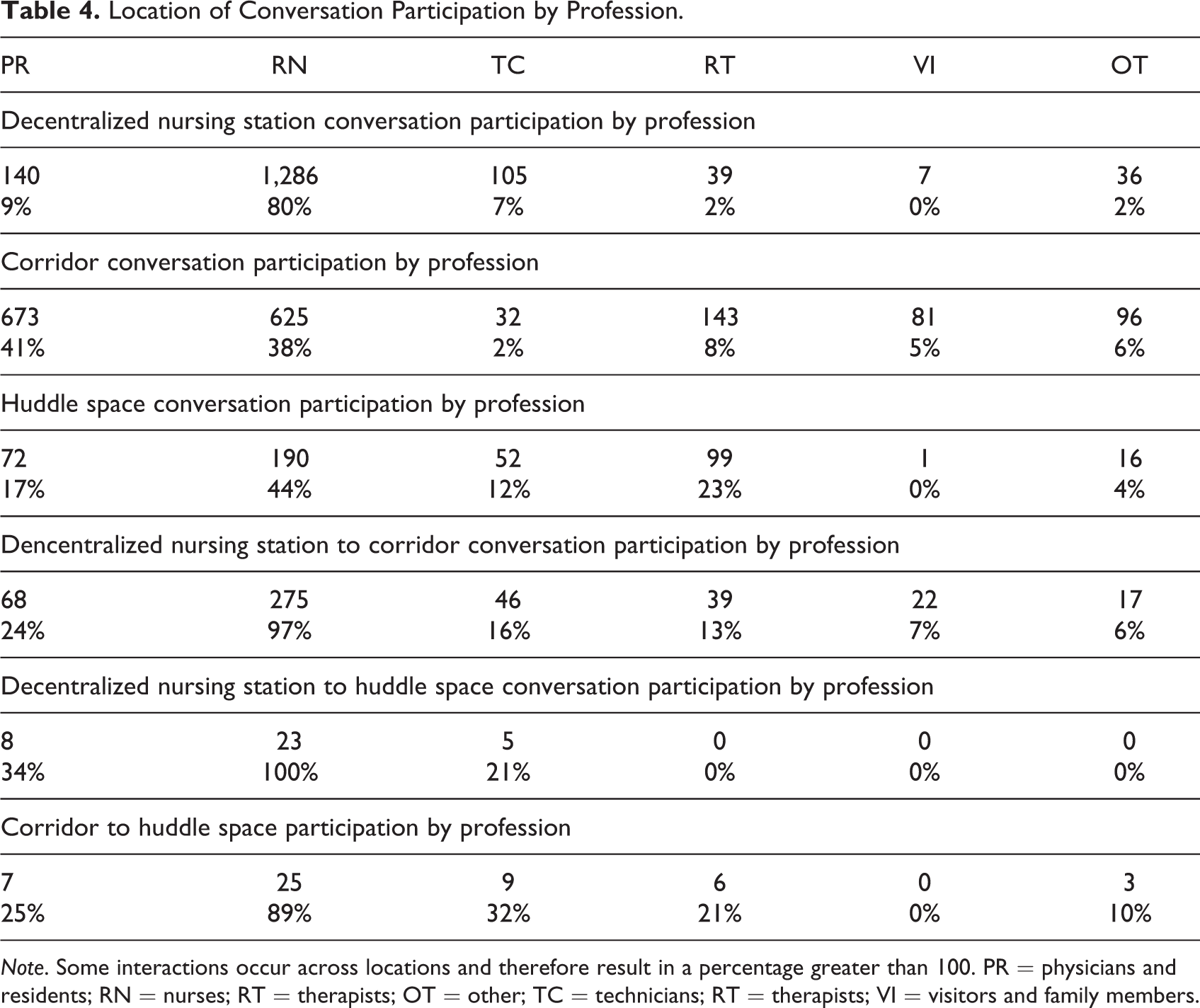
Note. Some interactions occur across locations and therefore result in a percentage greater than 100. PR = physicians and residents; RN = nurses; RT = therapists; OT = other; TC = technicians; RT = therapists; VI = visitors and family members.
Discussion
This study examined the use of DNS, corridors, and huddle stations as places for teamwork and multidisciplinary care in the NICU. While a significant body of research indicates the benefits of both decentralized nursing station and SFR NICU designs as beneficial to patients and families, the literature called for more research on the impacts of these design layouts on staff. From the research presented, it is evident that healthcare professionals perform their work in a range of spaces and that these spaces can have an impact on factors such as teamwork, job satisfaction, stress, and well-being. Consistent with the literature, the decentralized unit design of the NICU under investigation was not correlated with significant perceptions of improved teamwork. Furthermore, this study builds upon the evidence that DNS can lead to feelings of isolation from coworkers.
The uniqueness of the NICU under investigation, however, can be found in the neutral zones referred to as huddle stations. With the inclusion of the huddle stations, the post-move survey outcomes revealed statistically significant higher perceptions of job satisfaction, stress and well-being, and design satisfaction. The observational study confirmed the huddle station as a multidisciplinary care location as physicians, nurses, technicians, and therapists all frequently utilized this space for conversations. Numerous studies have revealed that job satisfaction is influenced by work environment and interpersonal relationships (Jimenez et al., 2019; Obeidat et al., 2021). Knowing that social support can both settle work stress and positively impact patient outcomes, the use of the huddle station as a location for multidisciplinary exchanges regarding care should be further examined (Alvaro et al., 2016).
The corridors of this NICU environment were home to the largest average group size. Thus, it is necessary to reframe the value of a corridor as an essential functional space that supports the delivery of care, particularly within an academic hospital where multiple observers are frequently participants of rounding groups. Healthcare facilities should consider corridors and centralized huddle spaces as important spaces for strategic collaboration and aim to design less hierarchical environments. From here, the challenge becomes to design neutral spaces and corridors in a manner that minimizes the negative aspects of clinical communication such as the compromising of patient privacy, increased acoustical disturbances, or the creation of blocked circulation paths. Providing a setting that encourages face-to-face interaction can lead to a more comprehensive approach to care and better support the breadth of the care team. Responding with spaces that promote both collaborative and focused work locations promotes the ability to deliver the highly specialized care required for a NICU environment.
Limitations
This is a pre–post study from a single academic healthcare facility and may not represent the majority of NICUs within the United States. The outcomes of the survey may represent selection bias because involvement was not mandatory. Past research suggests that a workforce immersed in a new work environment tend to progressively value performance of design features as the duration of exposure continues (Smith et al., 2009). To more clearly understand the impacts of the new design on teamwork, stress, well-being, and job satisfaction, a follow-up study should be performed. Additionally, the use of additional staff locations such as breakrooms, multidisciplinary office cubicles, and supply and equipment spaces could be examined to broaden the understanding of the healthcare workspace.
Conclusions
As NICU care continues to become more complex, healthcare systems are responding with multidisciplinary care practices that include an array of caregivers. The spaces where healthcare professionals work are key elements in creating an optimal patient experience and improving care delivery. The position taken in design guidelines relative to decentralized nurse stations, corridors, and neutral spaces must be informed by research findings. The NICU investigated in this study was found to have higher perceptions of job satisfaction, stress and well-being, and design satisfaction among a variety of professionals after moving to a SFR, decentralized unit design. The outcomes of this study demonstrate that neutral spaces such as corridors and centralized huddle stations should be considered as important spaces for strategic collaboration and multidisciplinary care as physicians, nurses, technicians, and therapists all frequently utilized these locations for conversations. Moving forward, designers should prioritize spaces for multidisciplinary teamwork and communication within NICU environments.
Implications for Practice
Healthcare facilities should consider neutral spaces such as corridors and centralized huddle stations as important spaces for strategic collaboration and aim to design less hierarchical environments.
Corridors should be designed with designated places for communication and offer ample space for large group sizes without compromising circulation, acoustical, and privacy needs.
Designers should prioritize multidisciplinary teamwork and communication in units designed with decentralized nurse stations.
NICU staff can expect both advantages and disadvantages when moving to a single-family room unit designed with decentralized nurse stations.
Supplemental Material
Supplemental Material, sj-pdf-1-her-10.1177_19375867221106503 - The Healthcare Workspace: Understanding the Role of Decentralized Nursing Stations, Corridors, and Huddle Spaces as Locations for Teamwork in a Neonatal Intensive Care Unit
Supplemental Material, sj-pdf-1-her-10.1177_19375867221106503 for The Healthcare Workspace: Understanding the Role of Decentralized Nursing Stations, Corridors, and Huddle Spaces as Locations for Teamwork in a Neonatal Intensive Care Unit by Lindsey Fay, Kevin Real and Shannon Haynes in HERD: Health Environments Research & Design Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.