
Abstract
Purpose:
This study investigates the relationship between environmental quality and medical sociology in hospitals and suggests a conceptual framework for understanding their interrelation.
Background:
Despite the importance of environmental properties in the sociological approach to users’ health and the role of medical sociology research in the design of hospital environments, few studies have been conducted in the field of hospital environments and medical sociology interrelation. Therefore, this article attempts to fill this gap in our knowledge.
Methods:
A systematic review was carried out in five databases (Scopus, Web of Science, Google Scholar, MEDLINE, and ScienceDirect) based on PRISMA guidelines to survey how environmental quality and medical sociology factors are related in the medical/environmental sociology research and the hospital design.
Results:
The search yielded the final 17 potentially relevant articles after finding 3,840 records, screening 1,295 nonduplicate articles, and reviewing 158 full-text articles. The findings revealed that four main aspects of medical sociology (physical–biological, psychological, social, and economic) and hospital environmental quality (physical, social, and psychological dimensions) influence users’ health and disease status. The hospital environment includes various social issues in medical sociology (like interactions, behavior patterns, lifestyle, work motivation, and culture). The physical and psychosocial factors of the hospital environment (such as spatial configuration, aesthetics, scale, privacy, and collective spaces) are associated with psychosocial aspects of medical sociology (like social class, behavior patterns, culture, and lifestyle).
Conclusion:
Environmental features and psychosocial issues should be considered to improve users’ health and experience in hospitals and to create a user-centered health-promoting environment.
Introduction
Built environment quality has an impact on human physical health (e.g., lower blood pressure, reduced heart disease, lower rates of respiratory disease) and mental health (e.g., less stress, less depression, and anxiety) (Hammink et al., 2019; Karanikola et al., 2020; Tsekleves & Cooper, 2017; Ulrich et al., 2018). Human health is one of the capacities that emerge from human interactions with the social and natural world (Fox & Alldred, 2016). Social and physical environments contribute significantly to users’ health outcomes and well-being (Arneill & Devlin, 2002; Suess & Mody, 2018). Sociologists are interested in the interaction between health and the environment and consider the impact of the physical environment on individuals from social and psychological perspectives (Brown, 2013; Capolongo et al., 2016). The different sociological perspectives on the “environment” address the interactions between the “environment” and “human health.” Some scholars have identified human health as being threatened by environmental factors. Others have noted that improving the built environment can provide sanitation and well-being (Fox & Alldred, 2016). As the healthcare environment provides a context for social issues, it is essential to consider the environmental quality to improve the social and psychological aspects.
Medical Sociology
Medical sociology is the study of health, disease, and medicine sociology, which considers the impact of social and structural factors on disease and illness processes along with the organization and delivery of healthcare (Table 1). These include factors such as culture (e.g., values, beliefs, normative expectations), organizational processes (e.g., hospital bureaucracy), politics (e.g., healthcare policy, political ideology), economics (e.g., capitalism, the stock market, healthcare costs), and microlevel processes such as socialization, identity formation, and group processes (Hafferty & Castellani, 2006; Monaghan & Gabe, 2022). One of the main questions in understanding medical sociology is “who people are.” Information such as age, gender, ethnicity, education, lifestyle, and socioeconomic indicators is essential because they are all involved and related to health status, health experiences, and the risk of death. Another question that medical sociologists want to know is “where people live” to investigate the geographical patterns of ill-health and to explore the relationship between the environment (area of residence, work, school, etc.) and health status. Different places can lead to differences in the health of their populations and are related to equity in healthcare and health outcomes (Monaghan & Gabe, 2022). Strauss (1957) divided the field of medical sociology into two parts: “the sociology of medicine” with a concentration on factors such as the organization, role relationships, norms, values, and beliefs of medical practice as a form of human behavior. This perspective emphasizes the social processes in the medical setting and their contribution to our understanding of medical sociology in particular and social life in general. “Sociology in medicine” focuses on the study of the social factors relevant to a particular health problem and the culture of the society in which the ill person lives and relates medical concepts, such as disease, illness, sickness, treatment, etiology, prevention, and so on, to sociological concepts, such as culture, society, economy, social structure, social class, social system, behavior patterns, personality, the family cycle, and sociobiographical factors including race, gender, age, and the constitution of the individual. Thus, sociology in medicine is applied research motivated by a medical problem rather than a sociological problem (Assi & Chima, 2020; Susser and Watson, 1971; Figure 1).
Definition of Medical Sociology in Studies.
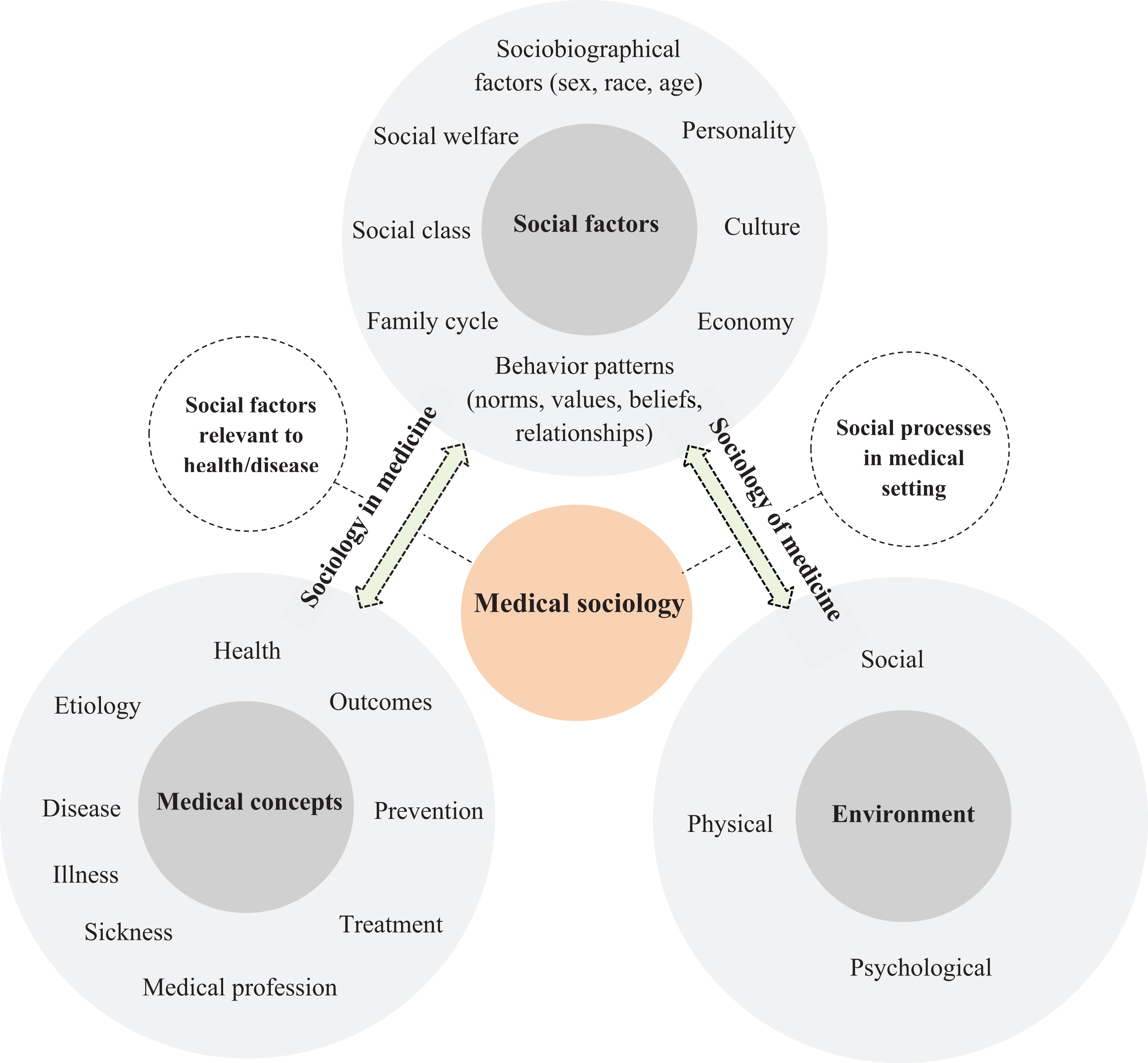
Hospital environment sociology concept. Source: Author based on Strauss (1957).
Environmental Sociology
The term “environmental sociology” was first used in 1971 by Samuel Klausner in his book On Man in His Environment (Klausner, 1971). Environmental sociology focuses mainly on the issue that “physical environments can have an effect on human societies and behavior” (Dunlap & Catton, 1979). Durkheim, the first social environment specialist, believed that the social environment was independent of the people who created it. Beliefs, thoughts, traditions, customs, and collective tendencies create a reality that is more than the sum of beliefs, traditions, customs, and personal tendencies (Durkheim, 1951). Social processes (discrimination, power, inequity, and collective activity) take place through the design and construction of forms and their use and maintenance (Gieryn, 2000). Therefore, space has elements that provide a context for social life, social activities, and social groups (Monaghan & Gabe, 2022; Prior, 1988). Physical and social environments are not independent of each other, and each is the result of continuity in the interaction between natural and human-built elements, social processes, and communication between individuals and groups. The place helps social life and historical changes with continuity of differences and social structure hierarchy, social interaction models through the creation of collective activities, and emphasis on norms and cultural values, identities, and untouchable memories (Gieryn, 2000; Table 2).
Definitions of Environmental Sociology.

Hospital Environment
In a hospital environment, positive experiences (psychosocial aspects) can play a significant role in patient’s well-being, healthcare quality, and a better workplace for staff (Barkan, 2021; Capolongo et al., 2016; Ulrich et al., 2008). Previous studies has demonstrated the impact of social determinants such as socioeconomic status, communication, gender, and the environment on health (Franz et al., 2019; Kendell et al., 2018). Ulrich’s (1991) theory of supportive design with the evidence-based design approach, attention restoration theory (Kaplan, 1995), and salutogenic design (Dilani & Armstrong, 2008) all emphasize the effect of physical and psychosocial factors on users’ stress reduction, health outcomes, and promotion in healthcare settings. The physical (air quality, light, cleanliness and maintenance, furniture, spatial configuration, ergonomic design, noise, color, art objects, spaciousness, thermal comfort, views, building aesthetics, and green spaces), social (privacy, care for social and organizational relationships [social support]), and psychological (safety, security, and positive distractions) aspects of the hospital environment can influence users’ experiences and health outcomes (Bromley, 2012; Martin et al., 2015; Mourshed & Zhao, 2012; Skinner et al., 2017; Ulrich et al., 2008). Hospitals, as complex organizations, focus on clinical relationships and curing patients’ illnesses. Recognition of social factors and their relationship with the hospital environment can benefit sociologists and architects to reconfigure the hospital for socialization and health promotion. Research and theoretical frameworks are needed to highlight the connection between the hospital environment and medical sociology.
Hospital Environment Sociology
Environmental sociology focuses on the interrelationship between the environment and the society. Sociology then moves from its primary perspective toward the environment to improve human health and well-being (Klausner, 1971). According to Klausner’s theory and Strauss’s view on the bipartite structure of medical sociology, the term “hospital environment sociology” can be used for sociology in the hospital environment which focuses on the study of social factors relevant to health and disease status (Gieryn, 2000) and sociology of the hospital environment with the emphasis on social processes such as social interactions in the hospital setting (Prior, 1988; Figure 1). An adequate sociology of healthcare architecture requires an appreciation of both the construction and experience of buildings exploring the briefs and plans of their designers, and observing their everyday use. Medical sociologists should complement these to extend our understanding of how the built environment can implicate and embed ideas, ideologies, and knowledge about health and medicine and in turn have consequences for those who use it (Martin et al., 2015).
Although most medical sociology studies focus on disease, health access, patients’ rights, occupational issues, and social aspects of users’ experiences and human communication, environmental sociology has not been sufficiently considered for the health aspects of environmental social movements. The relationship between the social environment and hospital users is less explored in this medical and sociological perspective. In addition, sociological studies have not yet been focused on understanding the significant role that hospital environments play in the social aspects of users’ health and well-being.
In response to this lack of knowledge, this article aims to review the literature on “medical/environmental sociology” and “healthcare environments” and to investigate how hospital environments and aspects of medical sociology are related to provide an understanding of the role of the environment in medicine and sociology interactions and the role of medical–socialogical research in hospital environments. This article proposes a conceptual framework based on environmental and social components in hospitals related to the medical sociology factors that affect users’ health. The research was conducted to answer the following questions: How is environmental quality related to medical sociology in hospitals? How do social aspects of medical sociology associate with the psychosocial and physical environments of the hospital? By answering these questions, this research will help architects consider social and medical factors in their design process and create health-promoting environments that provide positive experiences and satisfaction for users. Also, hospital managers and planners can benefit from the proposed model to integrate social and environmental issues into management policies to provide a healthy social organization.
Research Methodology
A systematic review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist (Moher et al., 2009; Figure 2). In the first step (identification phase), 3,840 articles were identified using five databases (Scopus, Web of Science, Google Scholar, MEDLINE, and ScienceDirect). The search key words were “hospital,” “environment,” “environmental quality,” “society,” “social,” “social environment,” “sociological environment,” “medicine,” “medical,” “medical sociology,” “environmental sociology,” and a combination of these terms such as “hospital” AND/OR “environmental quality,” “hospital” AND/OR “social environment,” “hospital” AND/OR “medical sociology,” “environment” AND/OR “medical sociology,” “medical” AND/OR “environmental quality,” and so on. The database searches that combined all three main terms (hospital environment, medical sociology, and environmental sociology) did not yield any relevant articles. The review included studies published between 1970 and 2022, as the term “environmental sociology” was first used in 1971 by Samuel Klausner in his book On Man in His Environment (Klausner, 1971). In the next step (screening phase), after removing duplicates, editorials, and abstract-only papers, the titles and abstracts were screened to exclude the out-of-scope articles. A number of inclusion criteria were applied: Full-text articles in English/Any original research published in a peer-reviewed journal, book chapter, or report describing environmental aspects of healthcare and medical sociology. The exclusion criteria were the following: Articles not related to the topic/Theses (masters and doctoral)/Conference proceedings and poster presentations/Articles with full text not available in English.
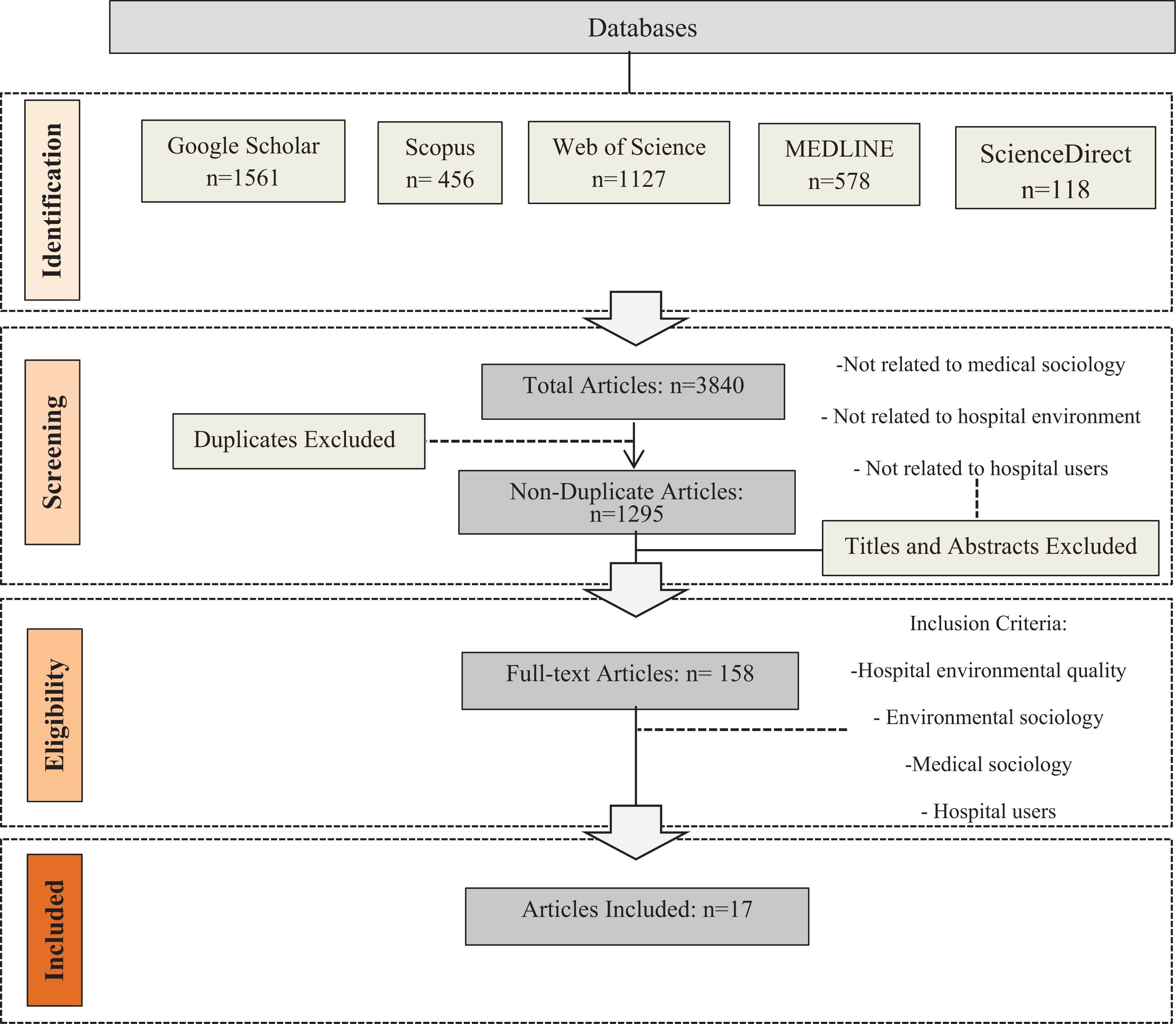
Selection procedure based on Moher et al. (2009).
In Step 3 (eligibility phase), studies were excluded if they did not relate to the hospital environment, medical sociology, and hospital users. A total number of 17 studies were selected for the full-text review (Step 4) according to the following criteria: (1) relevant to hospital environmental quality, (2) related to medical sociology, (3) relevant to environmental sociology, and (4) related to hospital users. Table 3 provides the details of the studies included in this systematic review. Finally, this review resulted in a framework representing the relationship between hospital environmental quality and medical sociology aspects.
Overview of the Selected Studies.

Results and Discussion
The study of the effects of social conditions on health and disease is one of the bases of medical sociology. Medical sociologists seek to define the link between social, economic, and cultural factors with a disease such as the effect of age, gender, marital status, ethnicity, race, socioeconomic status (income and education), and religion on a particular type of disease as well as the role of social factors in people’s or societies’ encounter with diseases (Barkan, 2021; Fox & Alldred, 2016; Mykhalovskiy et al., 2019; Piątkowski, 2020; Wright & Perry, 2010). Health and disease include biological, psychological, and social aspects, which is called the biopsychosocial model (Masoudnia, 2017). According to the Oxford English Dictionary (Simpson & Weiner, 1989), the term psychosocial refers to the communication between behavioral and social factors and their effects on people’s minds or behavior. The vast health-disease continuum is, on the one hand, the result of a person’s links with the social environment, social groups, and social structures (economic, cultural) and, on the other hand, has a direct link with their characteristics from the point of view of personal conformity (in both physical and mental aspects). Since the social environment has a permanent connection with the physical environment, health and disease are simultaneously influenced by the physical and social environment (Armstrong, 2003). Three main notions in sociological studies are noticeable: Environmental characteristics are more than the sum of individuals; environmental features can strengthen or weaken social support and coherence and are essential for people’s health; and environmental–social properties are the result of characteristics such as socioeconomic status, public services, behavior, and culture. Also, sociologists seek to play an active role in hospitals by participating in modern care activities and the creation of new spaces (Franz et al., 2019, p. 7). Hospitals take different forms in different societies and cultures and are contexts for improving the values and beliefs of the culture of their society (Fox & Alldred, 2016; Van der Geest & Finkler, 2004, p. 1995). Humanizing medical practice and care in hospitals is inextricably linked to the environment in which that care takes place. Thomas McKeown, a professor of social medicine in the United Kingdom, emphasized that providing a healthy environment in hospitals requires architectural changes by reducing the scale of hospital buildings and introducing a variety of amenities along with hospital buildings such as shops, restaurants, amusements, and so on (Bates, 2018). In Prior’s (1988) study of 19th-century hospital architecture, these buildings represented historical beliefs about the causes, cure, and management of diseases and were more than just a context for sociomedical communication. At that time, the categorizations of patients were considered in spatial configurations based on their economic status, and a separate inpatient ward not only isolated patients from contamination but also separated them according to their ethnicity and social level (Brandt & Sloane, 1999, p. 285). Architectural plans are historical documents that contain the origins of medical science; for example, the construction of a pavilion hospital in the 19th century (with open corridors, windows to facilitate the airflow and light and toilets near the exits for the outlet of polluted air) emerged and was used to treat diseases caused by poisonous air (Martin et al., 2015). Burns and Wholey (1991) believed that the structural and organizational properties of hospitals such as size, type, and hospital ownership (private or public, educational or noneducational, and urban or rural) were associated with patient length of stay and death. Fox’s (1997) poststructuralism ethnography also demonstrated the effect of spatial configuration on the collective success of health and explored the role of nonhuman objects in this configuration. Brandt and Sloane (1999) examined the quality of the reflection of medical values in hospital elevations and spatial configuration, indicating that historical models of hospitals represent not only the perception of this unique building but a broader history of medicine, science, and dominant culture in the 20th century. Gieryn (2000) cited place-sensitive sociology in which a place becomes a space with the presence of people, activities, and objects and is not just an environment or background but a power with discernible and independent effects on collective life that plays an active role. In his article called “What Buildings Do,” Gieryn (2002) also presented a way beyond the buildings as limited structures or as meaningful through the interpretations of users, explaining the dual reality: Buildings limit activity and at the same time, despite their fixed appearance, they offer the possibility of interpretation and reconstruction. Therefore, although buildings confirm collective life, this confirmation is not complete and unchangeable. Sloane and Sloane (2003), in their book Medicine Moves to the Mall, considered the changes in hospital design in the contemporary era with economic priorities and in combination with the architectural properties of shopping centers, hotels, and houses. Street and Coleman (2012) recognized a hospital as a multilayered space in which different social groups have emerged. Bromley (2012) showed how architects and designers strive to consider hope, healing, and humanity by creating efficient and valuable buildings on a human scale concerning human-centered hospital design in the United States. Capolongo et al. (2016) addressed three main criteria for social sustainability in hospitals: Humanization focuses on four aspects of the hospital environment—safety and security, social aspects, well-being, and health promotion; comfort considers the microclimatic conditions in hospitals (indoor quality); and distribution concentrates on the impact of the organization of spaces, pathways, and so on people’s well-being. Providing lounges, day rooms, and waiting rooms with comfortable, mobile furniture arranged in small, flexible groups improves social interactions in hospitals (Ulrich et al., 2008).
Sociologists have considered the role of tools and objects in various studies. Some of these studies have noticed the importance of spatial and temporal trends in performing medical and nursing tasks in healthcare spaces (Lehoux et al., 2008; Mesman, 2009). Hospitals contribute to the change of medical activities’ models and professional situations to some extent linked to the development of architectural philosophies and building techniques (Martin et al., 2015). Therefore, medical sociology has been impressive in the hospital environment and its different spaces from physical, economic, cultural, social, and psychological aspects (Table 4).
Effects and Results of Hospital Environment Sociology.

Hospitals are changing and have major goals such as improving the health of society, enhancing patients’ experience, and reducing healthcare costs. Various programs in hospitals—such as collective gardens, crime decrease, work motivations, and programs for secure and suitable stay—are examples of sociological interests. The change of hospital activities toward a society-concentrated model benefits sociologists by reorganizing the hospital environment as a context for research on social standards and socialism developed beyond the hospital complex in the neighborhood and society (Franz et al., 2019). Generally, hospitals are social spaces where user-centered design for different users (patients, visitors, and staff) can be developed around environmental elements and configurations.
User-Centered Environmental Sociology Model
Social issues are one of the main concerns in complex healthcare environments. Medical and environmental sociology issues are linked because health and the environment affect our lives (Brown, 2013). However, few studies have focused on the association between the physical environment and medical sociology, and there is a lack of relevant research in hospitals. Furthermore, despite the significant role of the environment in social improvement and health promotion, inappropriate quality and ignorance of social factors in the hospital environment lead to undesirable experiences and user dissatisfaction (Dilani, 2001). Considering hospital environmental aspects and their associations with social factors from a medical sociology perspective is essential to provide more knowledge about the role of the hospital environment in medical sociology to create a healthy and desirable psychosocial place for different users. This study presents a systematic review of the relationship between environmental quality and medical sociology factors in hospitals and discovers the additional connections between environmental components and medical sociology and their impact on hospital users. The review of studies showed that medical sociology is the relationship between medical concepts such as health, disease, outcomes, prevention, medical profession, and social factors such as social class, behavior patterns, socio-biographical factors, economic status, culture, and so on. Therefore, physical–biological (age, gender, ethnicity, and race), psychological (personality, mental status, work motivation, safety, and security), social (social class, behavior patterns, culture, lifestyle, education, marital status, education, and religion), and economic (income, economic status, and healthcare expenditure) factors can be defined as the main aspects of medical sociology. The studies showed that these factors can affect the health and well-being of hospital users in behavioral and mental aspects. These factors can also influence the disease status and its prevention, outbreak, and treatment. In addition, hospital environmental quality includes physical (air quality, light, cleanliness and maintenance, furniture, spatial configuration, ergonomic design, noise, color, art objects, spaciousness, thermal comfort, views, aesthetics, building scale/size, and green spaces), social (privacy, care for social and organizational relationships, collective gardens, and amenities such as shops, cafés, etc.), and psychological (safety, security, and positive distractions) aspects that affect users’ health outcomes and their status on the health/disease continuum. These environmental features can lead to positive experiences, health promotion, comfort, and satisfaction. They can also enhance social interactions and communication, which influence users’ psychological responses and mentally engage with hope and the healing process. Accordingly, both the medical sociology factors and the environmental quality of hospitals can influence users’ health and experience. Besides, the hospital environment can impact the physical, psychological, social, and economic aspects of medical sociology. Hospital environmental factors (Figure 3) consist of social interactions, behavior patterns, lifestyle, work motivation, and culture (Bromely, 2012; Prior, 1988). Physical factors (noise, color, maintenance, access to green spaces, light, aesthetics, green spaces, and art objects) promote patients’ recovery and well-being (Dilani, 2001; Ulrich et al., 2008). Spaces such as collective gardens and facilities (shops, café) with social support can provide work motivation, behavior patterns, and social interactions (Dunlap and Catton, 1979; Gieryn, 2000). Safety and security as psychological components in hospitals are critical to health outcomes, job motivation, behavior patterns, and social communication. As recognized by Bromley (2012) and Franz et al. (2019), hospital environmental sociology can influence the healing and health of societies, lead to positive experiences, and reduce healthcare costs. Medical sociology factors also influence the design and organization of hospital environment. Physical and social aspects of the hospital environment, such as spatial configuration, aesthetics, building scale, privacy, and collective spaces, can be influenced by social and psychological factors of medical sociology (social class, behavior patterns, culture, and lifestyle) (Franz et al., 2019; Gieryn, 2000; Martin et al., 2015; Prior, 1988). Sociologists need to consider social, economic, and cultural values in any hospital environment, and designers and planners should be aware of medical–social factors when designing healthcare environments to create a health-promoting environment, as the hospital space can influence user outcomes and health status. Medical sociology can shape our perceptions of how the built environment affects users’ behavioral and psychological health through physical, economic, psychological, and social factors (Figure 3).

Link between components of medical sociology–user–hospital environment.
Conclusions
The interrelationships between society and the health sciences have been considered in studies focusing on the social and cultural aspects of healthcare. Sociology researchers have emphasized the environment as one of the key factors in user health and outcomes. This research aimed to provide a holistic understanding of medical sociology and the hospital environment where social factors can influence health promotion. This study focused on how medical sociology factors are related to users and the environmental quality of hospitals. The review demonstrates that medical sociology factors in physical, social, psychological, and economic aspects can impact users’ health and disease. Environmental quality also affects the mental health status of hospital users. The results show that social and psychological determinants should be considered together with environmental features to improve users’ health and experience in hospitals and to create a health-promoting environment. The suggested framework addresses the relationship between environmental and sociological factors that may influence users’ health. Sociological research on the healthcare environment emphasizes the need for a remarkable role of environmental properties in human health and social factors in cooperation with environmental elements can improve this health status and outcomes. This research framework has implications for healthcare sociologists, designers, and managers to consider the role of social and environmental features in creating healthcare environments that can improve users’ health and to apply this perspective to practical action.
Limitations and Recommendations for Future Research
Similar to other literature reviews, this research has some limitations. The study includes English language articles, and studies in other languages were excluded. The studies between 1970 and 2022 were reviewed and those outside this period were not included in this research. This review highlights the need for future studies on the role of the environmental quality features on sociological factors in different spaces, such as inpatient wards, outpatient spaces, intensive care units, and open spaces, in addition to workplaces for hospital staff in healthcare environments. The future study can also focus on different users in hospitals (patients, staff, and visitors) and compare the association of environmental quality with sociological factors for these users in hospitals. Research can evaluate the effectiveness of different environmental elements in improving medical sociology factors and this association’s impact on patient and staff outcomes. Further investigation is required to examine the influence of the relationship between the hospital’s inside and outside environment and sociological factors on staff performance and patient health promotion.
Implications for Practice
Medical sociology considers the influence of medical and social factors, including the environment, on users’ health and disease status.
“Hospital environment sociology” provides insights into the role of environmental quality in users’ health from a medical–social perspective with a focus on social issues in hospital settings.
“User-centered hospital” can facilitate a health-promoting environment through strengthening hope, healing, and humanity. In this way, social, physical, and psychological aspects of medical sociology and healthcare environments help users’ positive experiences and well-being.
The reciprocal relationship between medical sociology and the hospital environment demonstrates that physical, social, psychological, and economic factors can influence users’ health outcomes in the social context of healthcare settings.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.