
Abstract
Background.
Total ankle replacement (TAR) has developed rapidly during the last decades, and there is solid evidence that this is a good treatment for end-stage ankle arthritis (ESAA). Whether these improved outcomes have translated into a higher utilization of TARs compared with ankle fusions (AFs) in Scandinavia is unknown. The aim of this study was to report the incidences of TAR and AF in the Scandinavian countries and to report any trends in these incidences during the last 8 years.
Methods.
Data were collected from the official patient registries of the three countries for the period 2016-2023, using NOMESCO codes for TAR and AF. To evaluate the capacity for highly specialized foot and ankle surgery, data about triple fusions and calcaneal osteotomies were also collected. Trends in incidence rates were evaluated with negative binomial regression.
Results.
During the period, 5667 AFs and 2012 TARs were performed in the three countries, which gives an ankle replacement percentage (ARP) of 26% for the whole region. Denmark had a higher total procedure volume, a higher number of TAR, and a higher ARP than the other countries (38% vs 20% for the two other countries, P ≤ .001). There was an increasing incidence of TAR during the period in Denmark and Sweden, while there was a decrease in Norway.
Conclusion.
The incidence of TAR and the ARP vary between the Scandinavian countries, where Denmark has a much higher incidence of TARs than the other two countries. In the last 8 years, the incidence of TARs has been stable in Denmark, increasing in Sweden and decreasing in Norway.
“The incidence of total ankle replacement and the ankle replacement percentage vary between the Scandinavian countries, where Denmark has a much higher incidence of TARs than the other two countries.”
Introduction
End-stage ankle arthritis (ESAA) is a debilitating condition, and the standard treatment has traditionally been an ankle fusion (AF). Total ankle Replacement (TAR) has been an alternative for decades, but this treatment has been associated with a high risk of reoperations and revisions. 1 The main indications for TAR include primary osteoarthritis, post-traumatic osteoarthritis, inflammatory arthritis, and secondary arthritis from chronic instability or malalignment.1,2 In more recent years, newer-generation implants have been introduced, and the revision rate has been significantly lowered.3,4 Fixed-bearing designs are increasingly utilized.5,6 Outcomes have improved, and some authors question if AF still should be considered the “gold standard” for ESAA treatment,7,8 although there is still no long-term, high-quality evidence of any superiority of ankle replacement over AF, or vice versa. 9 A randomized controlled study between the two treatments showed no significant differences in the primary endpoint, but in a subgroup analysis, patients with a fixed-bearing TAR had a better Manchester-Oxford Foot and ankle Questionnaire walking/standing score than patients operated with AF after 2 years. In addition, patients with osteoarthritis in neighboring joints had better results with TAR than with fusion. 10
There is a considerable variation in the incidence of total ankle replacement worldwide. Although patients with ESAA have comparable PROMs both preoperatively and 5 years after the surgery to patients with hip and knee arthritis, 11 the procedure is not as readily available to patients as hip and knee replacement. In many countries, it is not available at all, while in the countries where it is available, the incidence varies considerably.12,13
In patients with ESAA, there is no general agreement on the specific indications for AF versus TAR. A decade ago, it was common to advise that TAR should be reserved for elderly persons with little deformity, low body mass index, and low functional demands, 14 but TAR is being increasingly utilized also in patients with large deformities 15 and in all age groups. 16
The proportion of ESAA patients treated with TAR will vary greatly between clinics, countries, and regions. Racial, socioeconomic, and insurance factors have also been described to influence the choice of treatment. 17 In this paper, we term the proportion of ESAA patients that are treated with TAR the “ankle replacement percentage” (ARP). The ARP is an interesting measure to compare between countries, regions of countries, or even between clinics, as it gives information about how widespread TARs are. As the level of difficulty in performing TARs increases with increasing deformity, expanding the indication for TARs also demands more experience and expertise. A high ARP is thus a sign of more advanced expertise in TAR surgery. Even if the role of TAR in the treatment of ESAA is still being debated, a very low ARP in a country or region may indicate that the treatment of ESAA patients may be suboptimal in this area. The “correct” level of the ARP is highly debatable, but it is of great interest to investigate the “real-world” epidemiology of ankle replacements, not only data from highly specialized centers.
The Scandinavian countries (Norway, Sweden, and Denmark) are generally viewed as very similar politically, culturally, and demographically. The health care system and population health in these countries are also viewed to be quite similar. 18 In all three countries, both AFs and ankle replacements are used to treat ESAA, but the incidences of these procedures have not previously been examined and compared.
The aim of this study was to report the incidences of TAR and the ARP in the Scandinavian countries, to compare these to other reported incidences and ARPs worldwide, and to report any trends in these incidences.
Methods
All three countries have national patient registries: Norsk pasientregister (NPR/Norway), Landspatientregisteret (LPR/Denmark), and Socialstyrelsens patientregister (SPR/Sweden). In these, patients are registered with International Classification of Diseases, 10th Revision, (ICD-10) codes and the NOMESCO classification of procedural codes. The Scandinavian hospitals are funded partly by reporting the procedures that are performed, and it is vital for hospitals to report to these patient registries to get reimbursed for their operations. This means that there is a high level of accuracy in these data. ESAA does not have a unique ICD-10 code, and the patients were therefore identified by the Nordic Medico-Statistical Comitteee (NOMESCO) codes NHG40 (“Ankle fusion with internal fixation”) and NHB20 (“Uncemented ankle arthroplasty”). Since almost all AFs are internally fixated and all ankle replacement designs presently in use are uncemented, these codes will uniquely identify the patients.
The quality of the data in the public registries is considered to be good. The NPR is used as the “gold standard” for completeness in the Norwegian Arthroplasty Register 19 and in the Swedish ankle registry (Swedankle). SPR data are almost equivalent to Swedankle data for TAR, but SPR is more complete than Swedankle for AF. 20
It is conceivable that a lower ARP in one of the countries could be related to a generally lower capacity of highly specialized ankle surgery. To investigate this, we identified patients operated with two other procedures—calcaneal osteotomies (NHK55) and triple fusions (NHG42)—and compared the incidences of these procedures between the countries. These procedures are predominantly performed by specialized foot and ankle surgeons, and the incidence of these procedures serves as an indicator of the level of advanced foot and ankle surgery in the country, outside of the clinical field of total ankle replacements.
Data were collected and exported to Microsoft Excel where they were analyzed further. Annual incidences per 100 000 inhabitants were calculated using official population statistics for each of the years for each country. Trends in the number of procedures per year were evaluated with negative binomial regression in STATA version 17. Proportions were analyzed with chi-square tests. The statistical significance level was set at 0.05. No ethical approval was required for the study, as only aggregated and publicly available data are analyzed.
Results
Overall Findings
Between 2016 and 2023, 5667 AFs and 2012 total ankle replacements were performed in the three countries, which gives an overall ARP of 26% for the whole region. The number of procedures performed per year in the whole region is stable (Figure 1), but there were large differences between the individual countries (Figure 2A-C). There has been a decrease in the incidence of TAR in Norway (P = .002), while there has been an increase in Sweden (P < .001) and in Denmark (P = .04). The incidence of AFs is decreasing in Sweden (P < .001), stable in Norway (P = .2), and increasing in Denmark (P = .007).
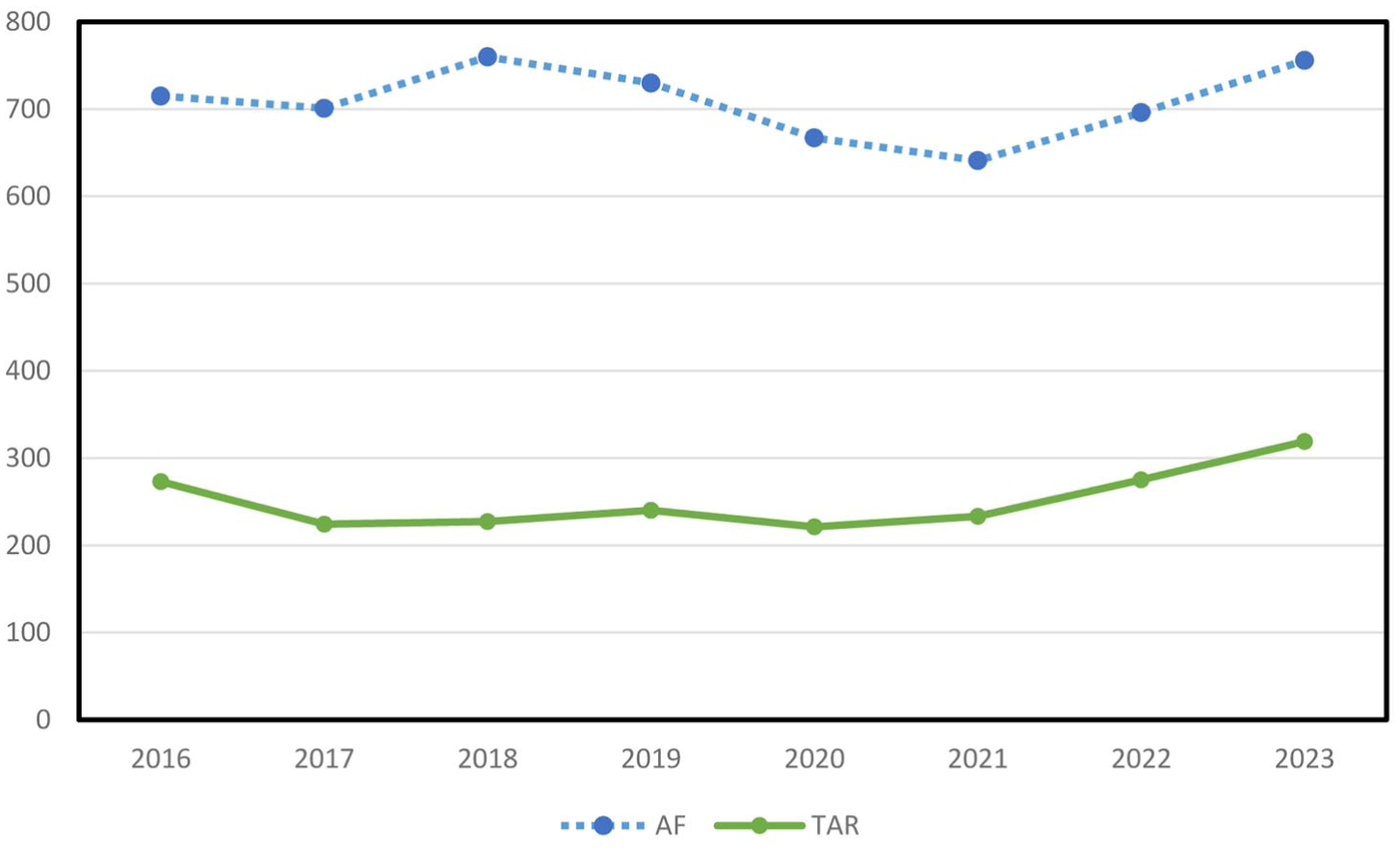
The number of total ankle replacements (TARs) and ankle fusions (AFs) performed in Scandinavia 2016-2023.
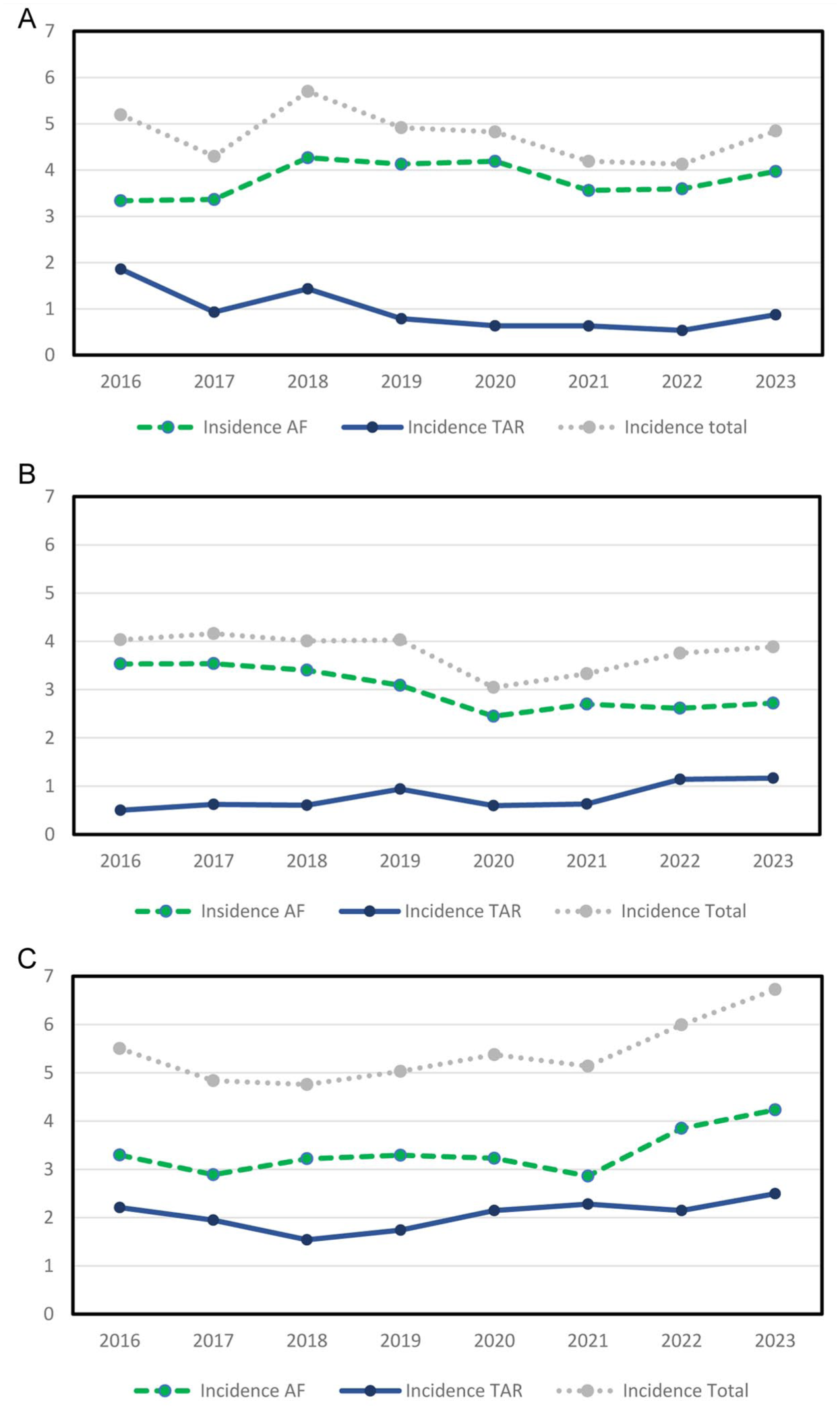
(A) The incidence (per 100 000 inhabitants/year) of total ankle replacement (TAR) and ankle fusion (AF) performed in Norway. (B) The incidence (per 100 000 inhabitants/year) of TAR and AF performed in Sweden. (C) The incidence (per 100 000 inhabitants/year) of TAR and AF performed in Denmark.
ARPs for Individual Countries
Table 1 shows the total number of procedures per country. In Norway, 409 TARs and 1627 AFs were performed, giving an ARP of 20.1%. In Sweden, the corresponding numbers were 643 TARs and 2476 AFs, also giving an ARP of 20.1%. The ARP was higher in Denmark, where 960 TARs and 1563 AFs were performed, giving an ARP of 38%, which is clearly higher than that in the other countries (P < .001). In Figure 3, the ARPs are plotted for each year for each country, showing that Norway has experienced a decrease in ARP during the period, while there has been an increase in Sweden. Table 2 provides incidences and ARPs from other countries for comparison.
Number of Procedures Per Country.
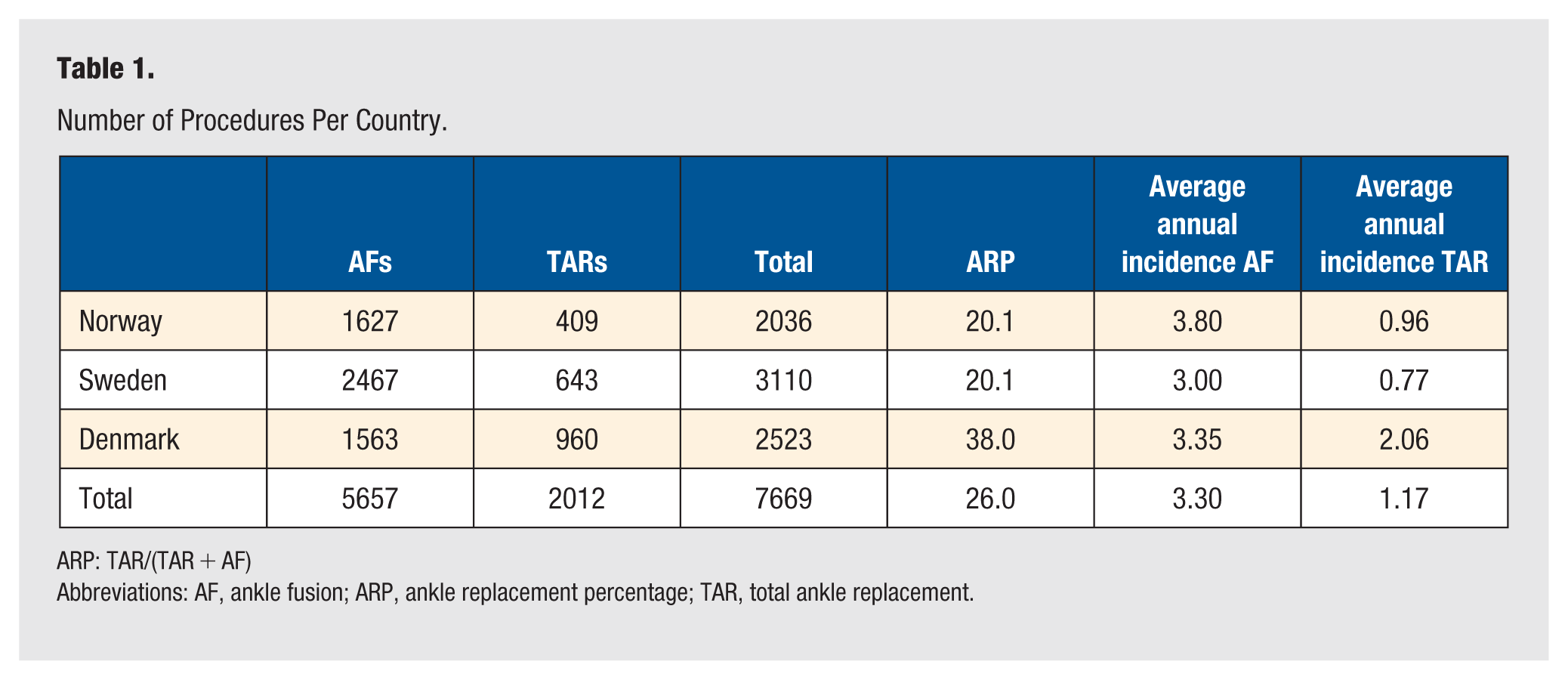
ARP: TAR/(TAR + AF)
Abbreviations: AF, ankle fusion; ARP, ankle replacement percentage; TAR, total ankle replacement.
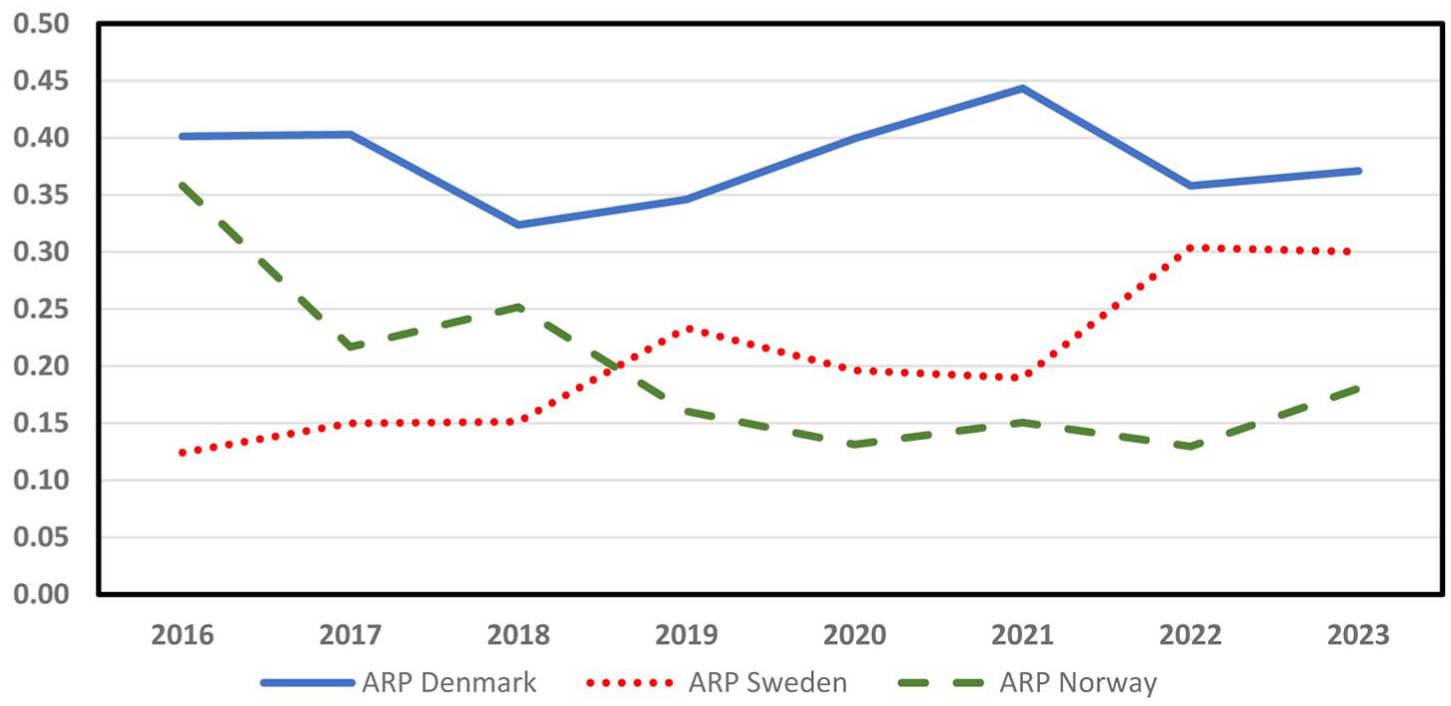
Ankle replacement percentages in the three countries during the period.
Comparisons With Other Countries.

ARP: TAR/(TAR + AF)
Abbreviations: AF, ankle fusion; ARP, ankle replacement percentage; TAR, total ankle replacement.
Capacity for Specialized Hindfoot Surgery
Triple fusions (NHG42) and calcaneal osteotomies (NHK55) were chosen as indicator procedures to investigate possible differences in the capacity of specialized hindfoot surgery. Figures 4 and 5 plot the annual incidence of these procedures per 100 000 inhabitants and show that while Sweden has the lowest incidence of triple fusions, it simultaneously has the highest incidence of calcaneal osteotomies, while Denmark has a high incidence of both procedures.
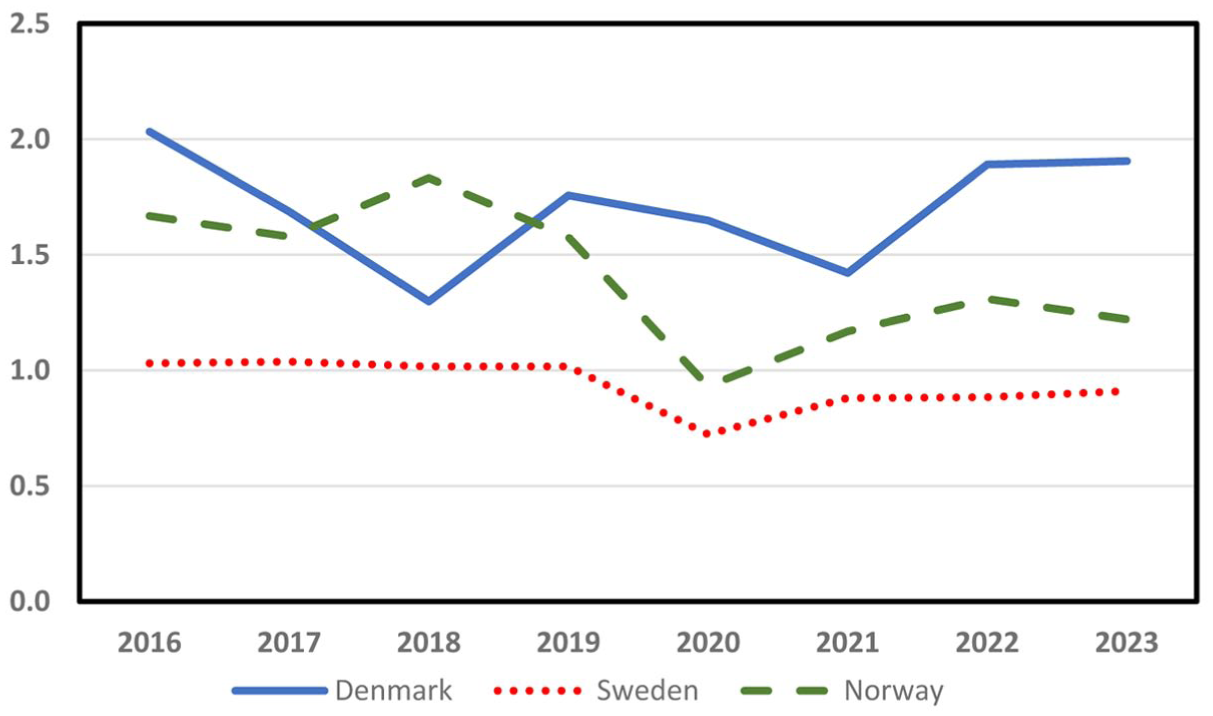
Incidence of triple fusions during the period.
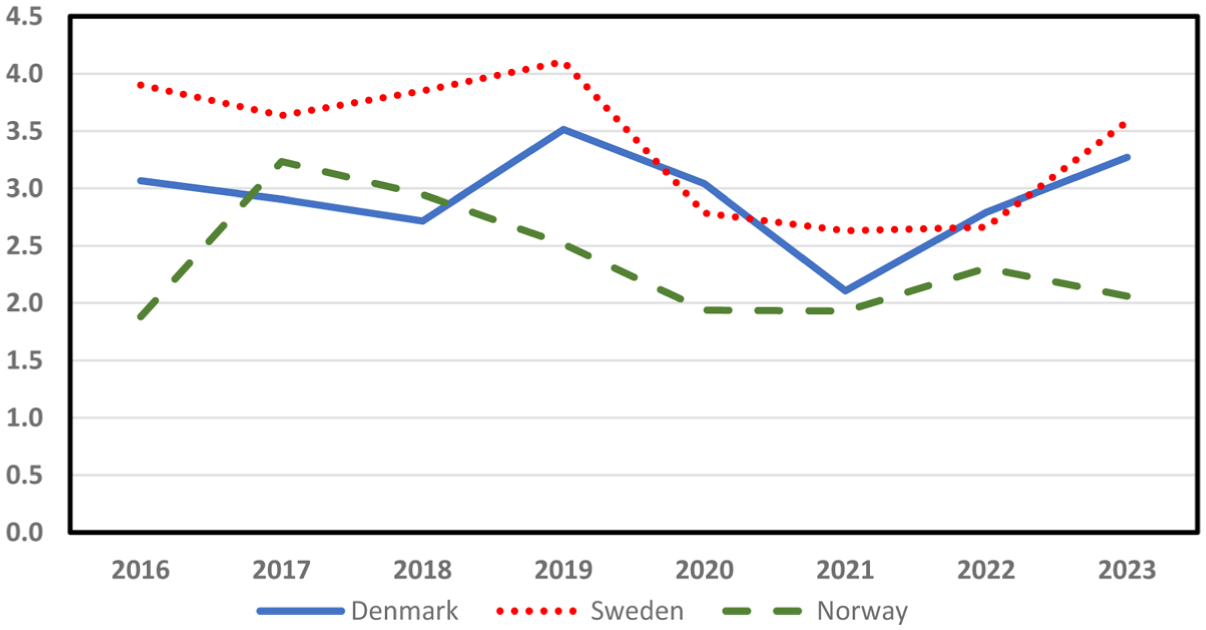
Incidence of calcaneal osteotomies during the period.
Discussion
The study showed that there were considerable variations in the use of ankle replacements between the Scandinavian countries. Denmark had a higher incidence of both procedures combined than the other countries, and it also had a higher incidence of TAR surgery and a higher percentage of TARs. In Sweden, the percentage and the incidence of TARs have been increasing during the last decade, while in Norway, both measures have been decreasing. Monitoring incidences of surgery through national patient registries makes it possible for health authorities to evaluate whether countries or regions have the capacity to provide adequate services for their patients with ESAA.
Comparisons With Other Countries
In Table 2, the results are compared with recent findings from other countries.21-24 New Zealand has, for many years, had the highest recorded incidences of TARs in the world, 12 and Australia reports a rapid increase during the last few years. 25 In Italy, the rate of TAR has increased rapidly, but AF has remained at a low level, giving a very high ARP at 65%. 26 This increasing trend of the utilization of TAR is not a uniform phenomenon worldwide, as shown in the numbers from Norway in this paper and from a report from Germany where the incidence per 100 000 decreased from 1.75 in 2007 to 0.99 in 2017. 27 An analysis of results from registry studies prior to 2018 can be found in a review by D′Ambrosi et al. 28
Total ankle replacements are currently not available for the general public in low-income countries and most lower-middle-income countries due to its high cost.
Possible Explanations for the Differences Between the Countries
The incidence of a certain surgical procedure may be interpreted to depend on 2 basic factors: the demand for the procedure and the supply. Epidemiological studies of the incidence of ESAA or the main causes of ESAA (ie, previous trauma or injury, malalignment, instability, and inflammatory diseases) between the countries are lacking, but we have no reason to believe that there is more ESAA in Denmark than in the other countries, although it cannot be ruled out. The demand may also be influenced by the threshold of seeking treatment for ESAA and the perceived availability of the treatment in the population and among health personnel. The population demographic between the countries is similar, with a similar proportion of the different age groups. 29 This means that the reason for the differences most likely is to be found in the difference in supply of these procedures between the countries.
A likely explanation is that Denmark may have a higher capacity for advanced foot and ankle surgery than the other countries. This is difficult to quantify, as neither of the countries have a formal certification for foot and ankle surgery, and there are few formalized departments that are only doing foot and ankle surgery. Probably Denmark has a more centralized hospital structure, which may have multiple historical and organizational reasons; one hypothesis could be that the short traveling distances for patients in Denmark compared to the other countries makes centralization of advanced surgery easier. The incidence of calcaneal osteotomies and triple fusions can be interpreted to corroborate this, as Denmark has almost double the incidence of triple fusions compared with Sweden and a much higher incidence of calcaneal osteotomies than Norway. Sweden and Denmark have a similar volume of calcaneal osteotomies, however, and the variations in the incidences of these procedures may also be explained by a difference in surgeons’ preferences, not necessarily by the capacity or available expertise. The low number of triple fusions in Sweden may be also explained by the fact that many Swedish foot and ankle surgeons will rely on performing talonavicular and subtalar fusions and omitting the calcaneocuboid joint in many cases, thus not coding for a triple fusion. When informally counting the number of surgeons able to perform TARs independently at the end of the period in question, we counted 11 surgeons in Sweden and Denmark, and 6 in Norway. This corresponds to 1.8 TAR surgeons per million inhabitants in Denmark, while Sweden has 1.0 and Norway has 1.1 surgeons per million.
The short travel distances in Denmark compared to the two other countries may give differences in the (perceived) availability of advanced ankle surgery, as patients from remote areas in Norway and Sweden may be limited by the long travel distances to seek specialized treatment.
Norway
In Norway (population 5.5 million), the incidence of TARs has decreased during the last decade. This can mainly be explained by a decrease in the number of hospitals offering this surgery, 1 which decreased from 6 hospitals in 2016 to 3 hospitals in 2023. During this period, the vast majority of the procedures in the country and all revision procedures were performed by 2 ankle surgeons at the largest center (Sahlgrenska University Hospital) in the capital, while 3 to 4 other surgeons at other hospitals performed a few TAR implantations per year. There may be many reasons for the decrease in the number of hospitals performing TARs, but one hypothesis is that the disappearance of the clinical field of rheumasurgery in Norway may have had a large impact. In 2012, 10 hospitals performed TARs in Norway, most of them rheumasurgical centers. With the advent of biological treatment modalities during the last 20 years, the demand for rheumasurgery has declined, and with it the subspecialty and subspecialized departments. Other hospitals in the country are currently starting to do ankle replacements, but as there is a long learning curve, increasing the supply of ankle replacements in Norway will take time.
Currently, almost all TARs in Norway are performed with the Infinity implant (Stryker), with only a handful of TM-ankle (Zimmer Biomet) implants being implanted each year.
Sweden
In Sweden (population 10.5 million), there are large differences between the regions in the access to total ankle replacement surgery, as well as the availability of AFs. AFs have usually been performed by orthopedic surgeons without subspecialist expertise in foot and ankle surgery, in many different hospitals. TARs, however, have always been performed in highly specialized centers. Due to current trends in the Swedish health care sector, many orthopedic surgeons have left the public hospitals for the private sector. More complex foot and ankle operations are time-consuming and not economically well compensated for the private hospitals, and currently, very few TARs are implanted in private hospitals. The future for complex and highly specialized foot and ankle services in the private sector is unclear.
There is, at present, a clear shift in the treatment of ESAA in Sweden, where the ARP is increasing. However, TARs are not prioritized in the same way by the financial endorsement given compared to total knee replacements (TKRs) or total hip replacements (THRs) where the operating times often are shorter due to a larger need for associated procedures in TARs.
The majority of cases (almost 90%) are, at present, performed by or done in cooperation with 1 of 2 individual Swedish foot and ankle surgeons. The TAR surgery is now spreading to other hospitals, where one of these experienced surgeons is functioning as a traveling mentor. There are 9 other surgeons around the country that are able to do TARs independently, but currently in low numbers. Organizational problems within the Swedish healthcare system with low capacity, long waiting lists, and surgeons leaving for the private sector are viewed as the main obstacles for capacity-building and education of more high-volume surgeons. Clusters are currently developing for the cooperation between hospitals with few cases. Only 1 hospital (Sahlgrenska University Hospital) performed more than 20 TARs during 2023, with the Infinity implant being the standard prothesis. During the latest years, the treatment for ESAA at this hospital has been dominated by TARs, and in 2023, 9 fusions and 41 primary TARs were performed, which gives an ARP of 82% at this hospital. TARs were performed in 16 different hospitals in Sweden in 2023, with the TM-ankle (n = 85) and the Infinity TAR (n = 37) as the most common implants. 20 From 2024 onward, the number of procedures as well as the number of hospitals are likely to increase. Revision TARs are currently performed in a few centers and by a few surgeons. In total, 1838 TARs have been performed between 1993 and 2023, and 344 (19%) have been revised. 20
Denmark
In Denmark (population 6 million), there are 3 centers with 11 TAR surgeons that have the national health board’s permission to perform TAR. Two of the centers have been using the STAR prosthesis (Stryker) since the beginning of 2000 and still do so. In the third center, the Infinity prosthesis has been used by 4 of the 5 foot and ankle surgeons for the last 5 years, whereas 1 surgeon uses the Hintegra implant (Vilex). The number of TARs has, especially since mid-2022, increased sharply at Sahlgrenska University Hospital and now amounts to approximately 90% of all ESAA operations.
Currently, there are no private hospitals that perform TAR. The reason is primarily that the insurance companies will not finance ankle replacement surgery because they find the price too high and argue that it is considered a highly specialized treatment that should only be carried out at the 3 university hospitals authorized by the health authorities. As in Norway, the so-called rheumatic surgery departments have practically disappeared. This is because medical biological treatment is effective, and moreover, most rheumatological foot and ankle surgical conditions today can be treated like in other patients without rheumatoid arthritis.
Limitations
The study has the inherent weaknesses of registry studies. Procedures may be incorrectly coded or not coded at all, although correct coding has a high priority for the hospitals as this is necessary for their reimbursements from the governments. The completeness of coding from the private sector is unknown, although the number of procedures performed in the private sector is probably negligible. The considerations in the discussion regarding the perceived current situation in the three countries and the historical background for this are largely based on unpublished evidence and the personal opinions of the authors.
Conclusion
The incidence of TAR and the ARP vary between the Scandinavian countries, where Denmark has a much higher ARP and incidence of TARs than the other two countries, most likely due to organizational differences between the countries. In the last 8 years, the incidence of TARs has been increasing in Denmark and Sweden but decreasing in Norway. Ankle replacement surgery has proven its place in the treatment of ESAA, and ensuring capacity and competence to provide this treatment should be a priority for the health services in countries with the economical capacity to provide this.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: There has been no specific funding for this study, but the corresponding author has a part-time research position funded by the South-Eastern Regional Health Authorities in Norway.
Ethical Approval and Consent
Not applicable as the study is done on aggregated, publicly available data.
Data Availability
The data are public and can be provided by request.
Trial Registration
This is not a trial.