
Abstract
Background. Venous thromboembolism (VTE) is a potentially life-threatening complication following orthopaedic surgery. While prophylaxis is well-established in joint arthroplasty, its role after Achilles tendon repair remains controversial. Despite being a soft-tissue procedure, prolonged postoperative immobilization increases VTE risk, with some studies reporting symptomatic rates as high as 7%. However, no prior studies have assessed whether pharmacologic VTE prophylaxis breaks-even in this population. Methods. A literature review and the TriNetX Research Network were used to identify symptomatic VTE rates within 30 days of primary Achilles tendon repair without pharmacologic prophylaxis. The cost of treating a symptomatic VTE was estimated from published data and adjusted to 2025 US dollars. Retail drug pricing was obtained from an online pharmacy database. A break-even analysis was conducted to determine the absolute risk reduction (ARR) and number needed to treat (NNT) required for aspirin (81 mg and 325 mg), warfarin (5 mg), enoxaparin (40 mg), and rivaroxaban (20 mg) to be cost-effective. A sub-analysis compared postoperative bleeding and transfusion rates in patients who received chemoprophylaxis versus those who did not. Results. Among 8935 patients undergoing Achilles tendon repair without chemoprophylaxis, 47 developed a symptomatic VTE (0.526%). Aspirin and warfarin broke-even across all VTE rates, with NNTs ranging from 9217 to 10 547. Warfarin still broke-even when including international normalized ratio (INR) monitoring costs. Enoxaparin and rivaroxaban only broke-even at the highest VTE rate (7.2%), with NNTs of 131 and 390, respectively, and required higher VTE treatment costs to be justified. Conclusion. In this study, we found that aspirin 81 mg, aspirin 325 mg, and warfarin break-even for VTE chemoprophylaxis following Achilles tendon repair. Enoxaparin and rivaroxaban failed to break-even. Chemoprophylaxis decisions should be individualized, weighing patient risk and economic considerations.
Keywords
“Aspirin and warfarin are cost-effective for venous thromboembolic chemoprophylaxis patients undergoing Achilles tendon repair.”
Introduction
Venous thromboembolism (VTE), comprising deep vein thrombosis (DVT) and pulmonary embolism (PE), remains a potentially life-threatening complication after orthopaedic surgery. While VTE prophylaxis is a well-established standard of care in joint arthroplasty, its role in soft-tissue procedures such as Achilles tendon repair is less clearly defined. Despite being frequently performed in otherwise healthy and active individuals, Achilles tendon repair often necessitates prolonged immobilization and non-weight-bearing postoperatively—2 risk factors known to increase thromboembolic potential.1,2
The optimal strategy for VTE prevention in this setting remains controversial. While specialty-specific guidelines from the American Orthopaedic Foot & Ankle Society and American College of Foot and Ankle Surgeons, as well as the International Consensus Meeting on VTE in Orthopaedic Surgery, do not recommend routine VTE chemoprophylaxis for isolated lower extremity injuries and note VTE rates are similar regardless of operative or non-operative management of Achilles tendon rupture, other studies have highlighted higher-than-expected rates of symptomatic VTE exceeding 7% following Achilles tendon repair—a population both societies recognize as elevated risk.2-6 In addition, a randomized controlled trial found that early mobilization does not prevent DVT in patients with Achilles tendon rupture due to postoperative pain and subsequent low weight-bearing. 7 Furthermore, in a recent survey study of orthopaedic foot and ankle surgeons, up to 98% responded that they use VTE chemoprophylaxis in high-risk patients, defined as a Padua prediction score ≥4. 8 Thus, there exists significant variability in clinical practice and decisions with regard to VTE chemoprophylaxis, which are often guided more by surgeon preference and perceived patient risk rather than by strong evidence or consensus guidelines.
Economic considerations further complicate decision-making. With increasing emphasis on value-based care, orthopaedic surgeons are tasked with balancing patient safety against the costs and potential harms of overtreatment. 9 Break-even cost-effectiveness analyses have emerged as a pragmatic tool for this purpose, identifying the threshold incidence at which prophylactic interventions become financially justified. 10 While such modeling has been applied to shoulder arthroplasty and total ankle arthroplasty, no prior study has explored this approach specifically in the context of Achilles tendon repair. 11
This study aims to evaluate the cost-effectiveness of commonly used pharmacologic agents for VTE prophylaxis following primary Achilles tendon repair, including aspirin, enoxaparin, rivaroxaban, and warfarin. Using a break-even analysis model informed by real-world incidence data from a large multicenter database and current drug pricing, we aim to provide an objective framework to evaluate the economic implications of VTE chemoprophylaxis and aid in the decision-making process. We hypothesized that low-cost agents such as aspirin and warfarin would break-even, whereas more expensive options such as enoxaparin and rivaroxaban would not break-even.
Methods
This study utilized a modified cost-effectiveness equation initially proposed by Hatch et al 10 to calculate the “break-even” VTE rate required for a prophylactic intervention to be cost-effective (Figure 1). The break-even rate was subtracted from the initial VTE rate to determine the absolute risk reduction (ARR) needed for cost neutrality. The ARR was then used to calculate the number needed to treat (NNT), representing the number of primary Achilles tendon repairs that would need to be performed with prophylaxis to prevent 1 symptomatic VTE event while remaining cost-effective. If the calculated ARR exceeded the initial VTE rate, the intervention was considered not cost-effective. In such cases, sensitivity analysis was conducted to identify the threshold for the cost of VTE treatment at which cost-effectiveness would be achieved.
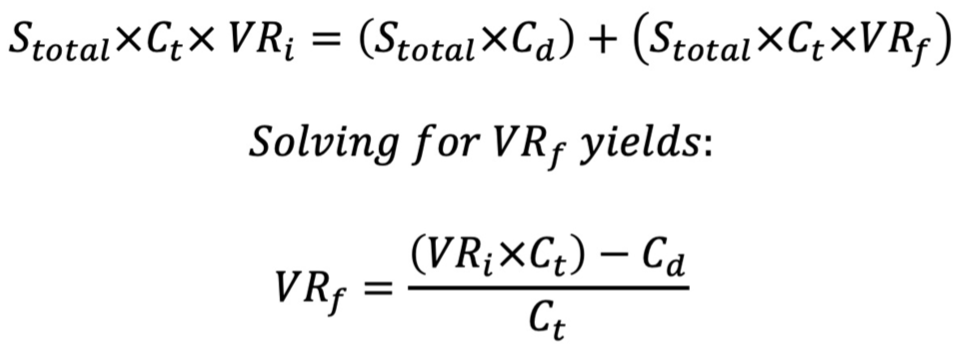
Equation for break-even cost-effectiveness model.
To estimate the financial impact of treating a symptomatic VTE, a review of published literature was conducted. In February 2025, the PubMed database was queried for the search terms: “cost of treating venous thromboembolism” and “venous thromboembolism cost.” The most widely cited estimate, derived from Grosse et al 12 reported a cost of $15 000 in 2014 USD for treating acute VTE. This value was adjusted for inflation to $20 461.32 in 2025 USD. 13 Commonly used drug regimens were identified from a February 2025 literature search of the PubMed database with the search term: “venous thromboembolism prophylaxis drug regimen.” Drug pricing data were obtained from an online database (GoodRx; GoodRx Holdings, Santa Monica, California) that aggregates average retail prices for prescriptions. 14 Average costs for a 1-month supply of commonly used VTE prophylactic agents were obtained, including aspirin (81 mg and 325 mg), enoxaparin (40 mg), rivaroxaban (20 mg), and warfarin (5 mg). As warfarin requires regular international normalized ratio (INR) monitoring, which may range in cost from $6.19 to $145.70 per test, an additional analysis was conducted using the lowest reported monitoring cost to reflect a conservative estimate. 15
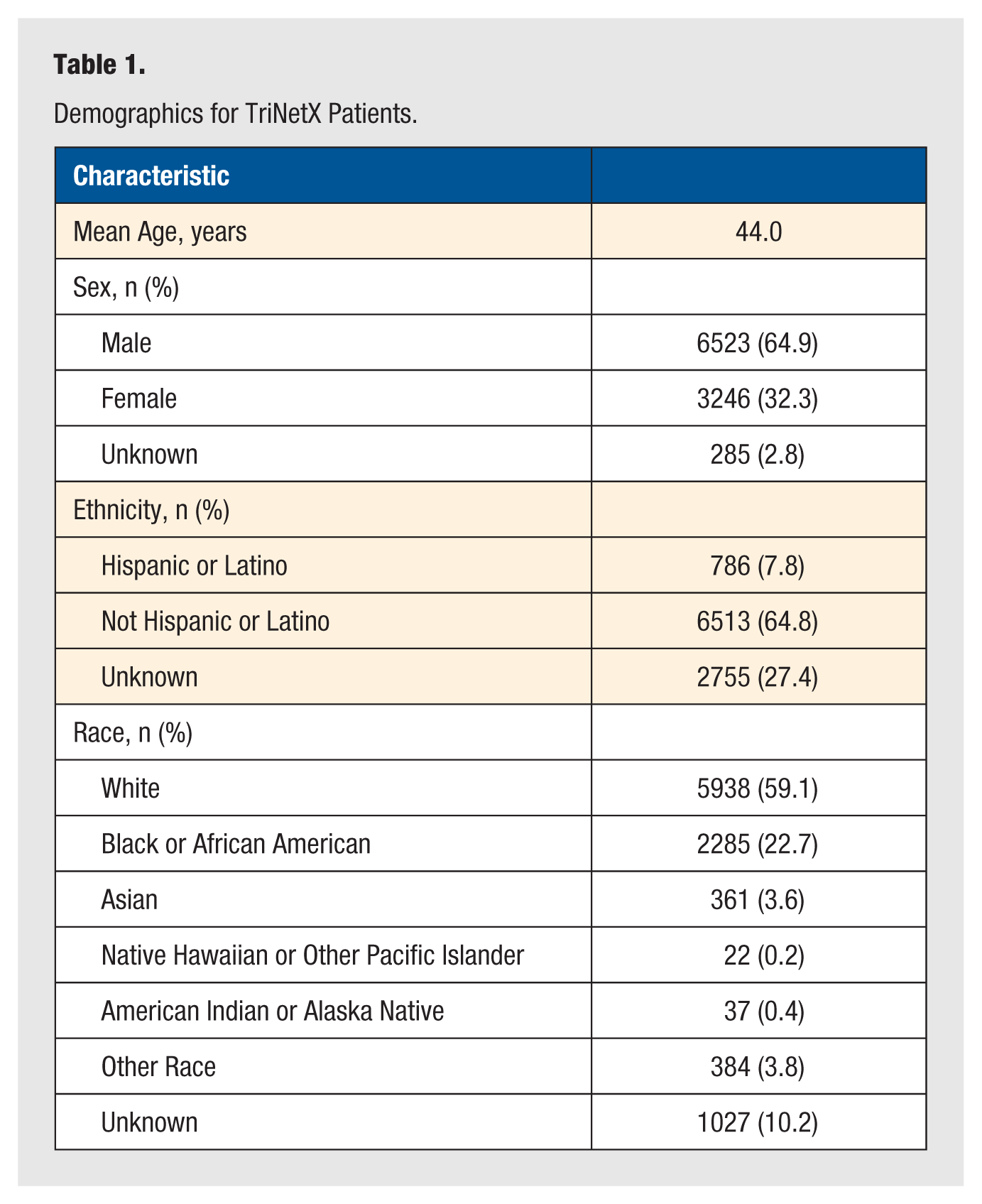
A literature search was performed to identify published rates of symptomatic VTE following primary Achilles tendon repair. In February 2025, the PubMed database was queried for the search terms: “achilles repair venous thromboembolism rate” and “achilles repair venous thromboembolism.” In addition, the TriNetX Research Network (TriNetX, Cambridge, Massachusetts)—a federated network of de-identified electronic health records from over 140 million patients across 106 health care organizations—was queried to determine the real-world incidence of VTE in patients undergoing primary Achilles tendon repair without pharmacologic prophylaxis. Patients were identified using the International Classification of Diseases-10 (ICD-10) and Current Procedural Terminology (CPT) codes associated with primary Achilles tendon repair (CPT: 27650, 27652) between February 2005 and February 2025. The VTE events occurring within 1 month of surgery were identified using diagnosis codes for PE (ICD-10: I26) and lower extremity deep vein thrombosis (ICD-10: I82.4). Patients with a prescription for VTE prophylaxis within 1 month after surgery were excluded. Three initial VTE rates were selected for the cost-effectiveness analysis: intermediate and high rates from the literature and a low rate derived from the TriNetX query to provide a conservative estimate of the break-even rate. Demographic characteristics of the study population are summarized in Table 1.
Demographics for TriNetX Patients.
This study was determined to be exempt from Institutional Review Board (IRB) approval. All data used were de-identified and derived from secondary sources. No direct interaction or intervention with human subjects occurred. This meets the criteria for exemption under §164.514(a) of the Health Insurance Portability and Accountability Act (HIPAA) Privacy Rule.
Results
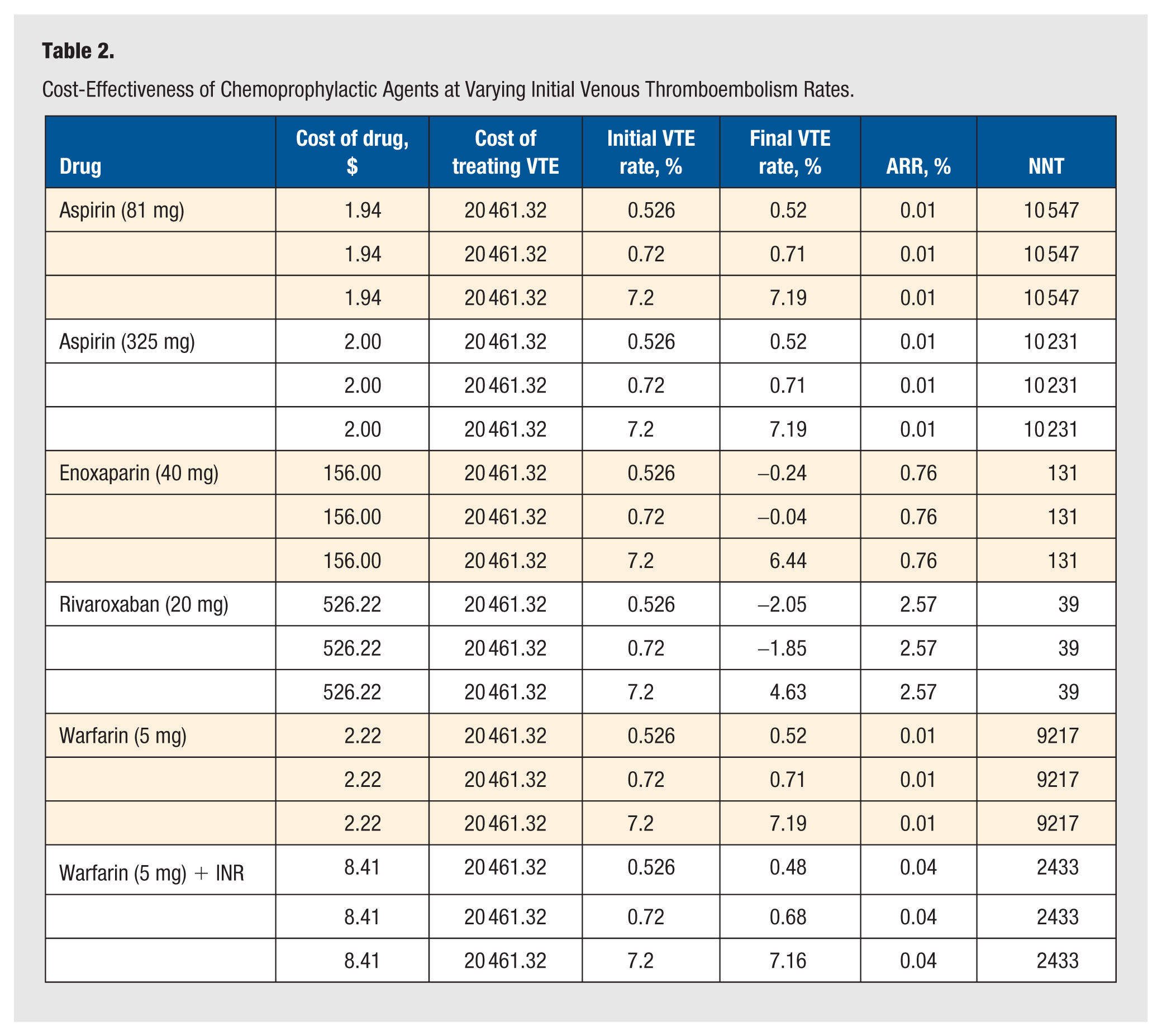
The product costs for a 1-month supply of once-daily aspirin (81 mg), aspirin (325 mg), enoxaparin (40 mg), rivaroxaban (20 mg), and warfarin (5 mg) were found to be $1.94, $2.00, $156.00, $526.22, and $2.22, respectively. The lowest cost of INR testing was estimated to equal $6.19, so the total price for warfarin (5 mg) plus INR testing was $8.41. These were the lowest prices for a full month’s supply that a patient could obtain if they used GoodRx. The cost of treating a symptomatic VTE was estimated to equal $20 461.32 based on existing literature. 12 The intermediate and high rates of symptomatic VTE obtained from the literature were determined to be 0.72% and 7.2%.2,16 Using the TriNetX Research Database, from 2005 to 2025, a total of 8935 patients underwent primary Achilles tendon repair and did not receive chemoprophylaxis. Of these patients, 47 (47/8935 = 0.526%) were identified with a symptomatic VTE.
At the product cost obtained, aspirin 81 mg was found to break-even at the TriNetX, intermediate, and high rates of symptomatic VTE if the initial rate decreased by an ARR of 0.01% (NNT = 10 547). Aspirin 325 mg broke-even at all 3 initial rates with an ARR 0.01% (NNT = 10 231). Likewise, warfarin (5 mg) broke-even at all 3 initial rates with an ARR of 0.01% (NNT = 9217). In addition, warfarin broke-even when factoring in the lowest cost of INR monitoring (NNT = 2433) (Table 2). In contrast, the intermediate and TriNetX symptomatic VTE rates for enoxaparin (40 mg) did not break-even because the final VTE rate exceeded the initial rate. However, enoxaparin (40 mg) broke-even at the high symptomatic VTE rate with an ARR of 0.76% (NNT = 131). Similarly, rivaroxaban (20 mg) did not break-even at the intermediate or TriNetX symptomatic VTE rate. Additional analyses demonstrated that enoxaparin (40 mg) and rivaroxaban (20 mg) break-even when costs of treating a symptomatic VTE are higher (Table 3).
Cost-Effectiveness of Chemoprophylactic Agents at Varying Initial Venous Thromboembolism Rates.
Additional Cost-Effectiveness Analysis for Enoxaparin and Rivaroxaban at Varying Costs for Treating Venous Thromboembolism.
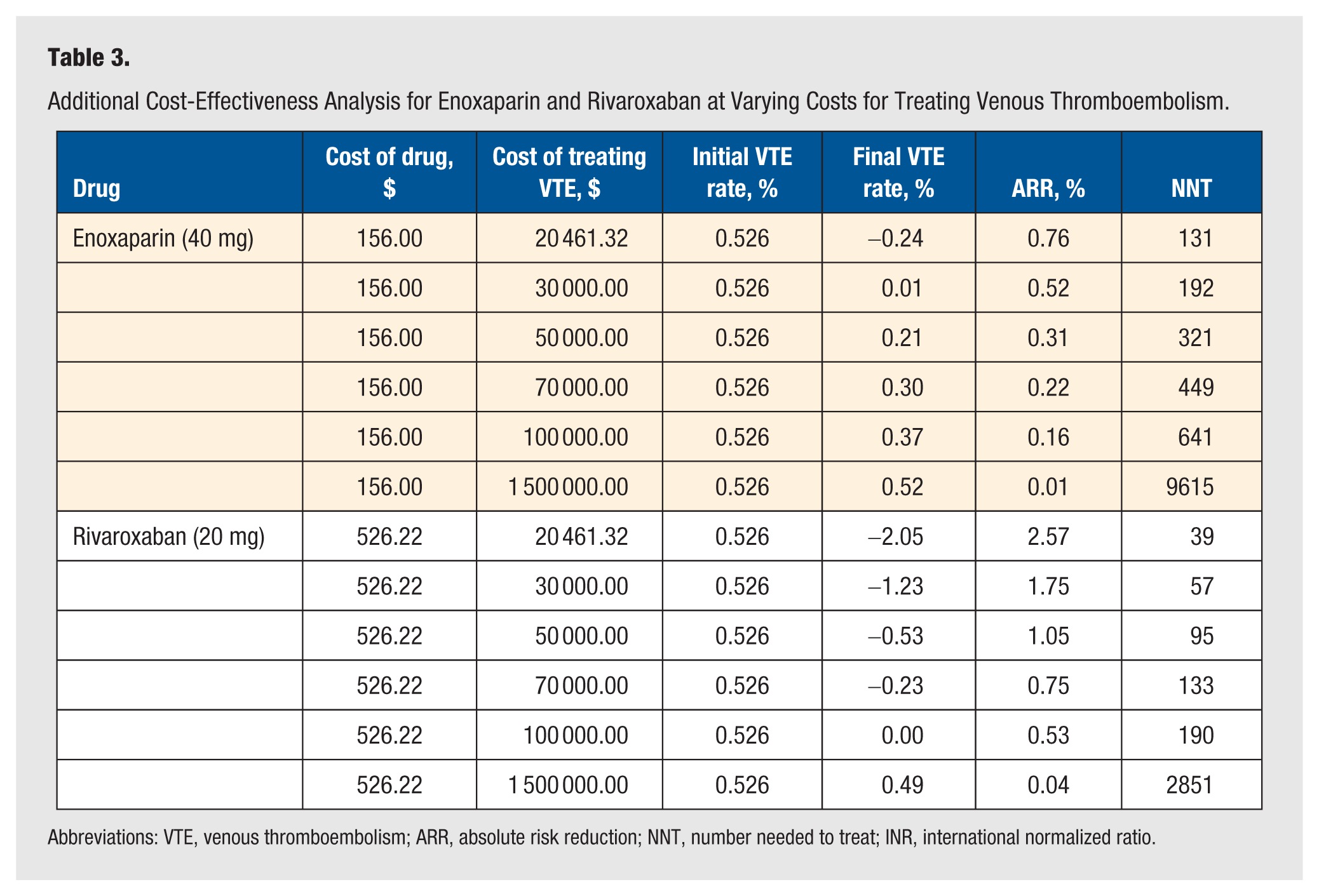
Abbreviations: VTE, venous thromboembolism; ARR, absolute risk reduction; NNT, number needed to treat; INR, international normalized ratio.
Discussion
In this study, we found that aspirin 81 mg and aspirin 325 mg daily are both cost-effective for venous thromboembolic chemoprophylaxis patients undergoing Achilles tendon repair at the TriNetX (0.526%), intermediate (0.72%), and high (7.2%) rates of symptomatic VTE. Warfarin 5 mg daily is also cost-effective at all 3 rates of symptomatic VTE, inclusive of the cost of INR testing. Enoxaparin 40 mg daily and rivaroxaban 20 mg daily are only cost-effective at the high symptomatic VTE rate. Enoxaparin and rivaroxaban only become cost-effective at higher costs of symptomatic VTE treatment ($30 000 and $100 000, respectively).
Venous Thromboembolism in Achilles Repair Patients
While multiple studies have demonstrated an overall low incidence of venous thromboembolic disease in patients undergoing foot and ankle surgery, most studies have found higher VTE rates in patients with Achilles tendon rupture. For example, in a meta-analysis of 22 papers including 43 381 patients undergoing foot and ankle surgery, Calder et al 17 found symptomatic VTE rates of 0.6% to 1% overall, but 7% in patients with Achilles tendon rupture. In fact, 1 study of 11 363 patients in the United Kingdom by Solan et al 18 demonstrated that Achilles tendon rupture patients are 6.5 times more likely to experience symptomatic VTE compared to those recovering from other foot and ankle surgeries. A retrospective review of 88 patients undergoing surgical treatment for an acute Achilles tendon rupture by Saragas et al 19 demonstrated a symptomatic DVT rate of 5.7% and a symptomatic PE rate of 1.1%. A retrospective study of 1231 patients from a single hospital in Australia with Achilles tendon rupture demonstrated symptomatic VTE incidence between 3% and 7%. 20 A prospective randomized controlled trial of 105 patients managed surgically for Achilles tendon rupture by Lapidus et al 16 demonstrated 35.2% radiographic DVT rate upon screening with color duplex sonography and 4.4% proximal radiographic DVT. Of note, there was no significant difference between those receiving dalteparin and those with no VTE chemoprophylaxis. In a retrospective study of 1172 patients, Patel et al 21 reported symptomatic DVT and PE rates of 0.43% and 0.34% following Achilles tendon rupture, and Pederson et al 22 reported a symptomatic VTE rate of 1.26% in a study of 28 546 patients. We observe a symptomatic VTE rate of 0.526% after Achilles tendon rupture repair, which is largely in line with the highest-powered studies in the literature.
Venous Thromboembolic Chemoprophylaxis
There exists conflicting evidence in the literature with regard to the efficacy of venous thromboembolic chemoprophylaxis. A follow-up audit study by Braithwaite et al 23 evaluating the efficacy of a VTE chemoprophylaxis protocol in Achilles tendon injury patients requiring immobilization demonstrated similar VTE rates in patients receiving aspirin 100 mg daily and those receiving no VTE chemoprophylaxis (6.4% vs 6.3%). Thus, the authors suggest that patients requiring immobilization following Achilles tendon injury should be given other forms of VTE chemoprophylaxis, such as low-molecular-weight heparin (LMWH). In a prospective randomized controlled trial of 105 patients managed surgically for Achilles tendon rupture by Lapidus et al 16 demonstrated no significant difference in VTE rates between those receiving dalteparin and those with no VTE chemoprophylaxis. In a prospective, double-blind, placebo-controlled trial of 440 patients who required immobilization in a plaster cast or brace for at least 5 weeks after a leg fracture or Achilles tendon rupture, Lassen et al 24 demonstrated a lower DVT rate in patients randomly assigned to receive reviparin for VTE chemoprophylaxis compared to the placebo group (9% vs 19%). The current study did not evaluate the efficacy of different VTE prophylaxis regimens. However, we did find that the 1-month supply costs of aspirin 81 mg ($1.94), aspirin 325 mg ($2.00), and warfarin 5 mg ($2.22) were much cheaper than enoxaparin 40 mg ($156.00) and rivaroxaban 20 mg ($526.22). Drug costs may be the dominating factor in complete cost-effective analyses when efficacy is unclear. Notably, the higher cost and greater anticoagulant potency of enoxaparin and rivaroxaban did not correspond to demonstrably superior clinical outcomes in the Achilles repair population, consistent with trial data showing no significant reduction in symptomatic VTE with dalteparin versus placebo. 16
“Break-Even” Analysis
In this study, we utilized a “break-even” analysis methodology that was first described by Hatch et al 10 in 2017. In doing so, we weighed the cost of various types of VTE chemoprophylaxis to the ARR of VTE in patients receiving this medication. Previous studies in the orthopaedic literature have utilized this analysis to evaluate whether different adjunct therapies break-even across various subspecialties.25,26 For example, Marinazzi, et al showed that VTE chemoprophylaxis breaks-even after total ankle arthroplasty. 11 While there exist numerous different cost-effectiveness methodologies, the type of analysis used in this study is advantageous due to its reproducibility and relative simplicity.
Patient-Specific Approach
Today, the prescription of VTE chemoprophylaxis in patients with Achilles tendon rupture remains surgeon- and patient-dependent with no clear broad consensus. A complete cost-effectiveness analysis of LMWH VTE prophylaxis in patients undergoing Achilles tendon repair found that routine chemoprophylaxis is unlikely to be cost-effective. 27 Multiple previous studies in the foot and ankle surgery literature have sought to risk stratify patients who are at an increased likelihood of developing a VTE. For example, Brennan et al found that advanced age over 65, diabetes, dyspnea, congestive heart failure (CHF), dialysis, wound infection, and bleeding disorders predisposed patients to developing a VTE in the postoperative period. In a retrospective study of 28 546 patients with Achilles tendon rupture in Denmark, Pederson et al 21 demonstrated 1.26% symptomatic VTE rate. Risk factors for VTE included hormonal contraception, previous VTE, older age, and male sex. Thus, the authors concluded that VTE prevention should be focused on risk stratification and preventative initiatives. Given the relatively high rates of VTE in patients with Achilles tendon rupture, future studies should focus on further elucidating the risk factors for VTE in this patient population. Our data support a patient-specific approach in the choice of VTE prophylaxis. Aspirin and warfarin broke-even at all VTE rates, while enoxaparin and rivaroxaban only broke-even at higher VTE rates, supporting the notion that prophylaxis may be more cost-effective for populations at higher risk.
Limitations and Future Research
This study has several limitations. This is a retrospective database study, so there could be significant heterogeneity in the data collection methodology over time and throughout the various sites of the study. In addition, we are relying entirely on CPT codes and ICD-10 codes for the procedures and diagnoses. Therefore, any coding inaccuracies could bias our findings. Also, rehab protocols, including postoperative immobilization and time to weight-bearing, may differ substantially between different sites and surgeons. Furthermore, we do not have any information related to imaging findings or surgical technique, both of which can vary significantly depending on the size and location of the tear.
Estimating the average cost of treating VTE is challenging and imprecise, especially as it does not account for the emotional and financial burden on families in cases of VTE-related mortality. Costs can vary significantly due to differences in the types and severity of complications, treatment settings, and geographic location. These variations can lead to inaccuracies, even when using the best available evidence. Similarly, drug costs incurred were modeled by GoodRx prices, which can be an oversimplification as patients may incur varying costs bound by insurance-covered pharmacies.
These findings are most applicable to the US health care system, where treatment costs for symptomatic VTE are relatively high. In health care systems with lower treatment costs, the break-even thresholds for chemoprophylaxis would increase, and some agents (eg, aspirin or warfarin) may no longer be cost-effective. In addition, this study is a break-even cost analysis and does not constitute a complete cost-effective analysis. Finally, the data reported in this study are predicated on a current literature review of the best available evidence. Future studies should be done evaluating the cost-effectiveness of venous thromboembolic chemoprophylaxis in other foot and ankle surgeries and the prescribing patterns of surgeons.
Conclusion
In this study, we found that aspirin 81 mg, aspirin 325 mg, and warfarin break-even for VTE chemoprophylaxis following surgery for Achilles tendon rupture. Enoxaparin and rivaroxaban did not break-even at all VTE rates. While there is no broad consensus on venous thromboembolic prophylaxis following foot and ankle surgery, most clinicians agree that VTE rates are relatively higher following Achilles tendon ruptures and that these patients should receive strong consideration for VTE chemoprophylaxis. Nevertheless, these decisions should be made on a patient-specific basis to achieve optimal outcomes. The cost analysis data presented in this study can aid in the decision-making process but does not impute a recommendation for or against the use of a specific VTE chemoprophylactic agent. These findings should be interpreted within the context of US-based cost assumptions, as variations in treatment costs across health care systems may significantly alter cost-effectiveness thresholds.
Footnotes
Author Contributions
Each author has participated in the design of the study, has contributed to the collection of the data, has participated in the writing of the manuscript, and assumes full responsibility for the content of the manuscript.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SL—AOFAS President, JAAOS Deputy Editor and MA—Consultant for Arthrex, Consultant for Zimmer Biomet, Consultant for Stryker, and AOFAS Committee Member.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
The Ethics Committee of Penn State University waived the need for ethics approval for the collection, analysis, and publication of the retrospectively obtained and anonymized data for this non-interventional study.
Consent to Participate
The Ethics Committee of Penn State University waived the need for patient consent for the collection, analysis, and publication of the retrospectively obtained and anonymized data for this non-interventional study.
Consent for Publication
Not applicable.
Data Availability
The data sets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.